Michael Olenick unearthed an anomaly that is so extreme that it raises doubts about the numbers that the Department of Health and Human Services is reporting for Obamacare signups and enrollments to date. He writes:
Following up about the rightfully maligned healthcare.gov website, and the software which underlies it, I can verify the program appears significantly sicker than anybody admits. As a Florida resident using the Federal exchange, I was never able to view plans despite working feverishly at it for over a month. I finally reached a worker at healthcare.gov who told me the site simply doesn’t work. She heard that state exchanges were better but verified that she has never personally seen anyone from Florida able to move past the last screen to view or purchase plans.
Yet the Department of Health and Human Services boasts about their signup success. Lambert pointed me to this October 26 statement by Kathleen Sebelius, What’s Working in the Marketplace: The Data Services Hub, which proclaims:
The Social Security Administration has reported 4.2 million transactions involving individuals or households who have elected to establish an account… The highest numbers of transactions continues to involve individuals and households in the following states: Pennsylvania (323,000), New York (310,000), California (290,000), West Virginia (240,000), and Washington (135,000).
Yves here. This extract from Sebelius is a remarkable confection of disinformation.
Let’s start with a basic issue: What exactly is a transaction? Normally, you’d assume that means signing up for insurance. My trusty desktop dictionary defines a transaction as “an instance of buying or selling something; a business deal.” But here in a typical Obama Orwellianism, that’s redefined to something, but we’re not sure exactly what, that prospective insurance customers do after the’ve managed to set up an account. So it’s clear they aren’t even within hailing distance of the conventional use of “transaction” which would be a completed enrollment (or in Obamacare speak, a clean, unique 834 transaction). We know those numbers are tiny for the Federal exchanges, hence the desperate effort to point at anything that looks like progress, particularly if you can attach big impressive-sounding numbers to it.
But the simple layperson way to think about this is that a transaction in this case means some sort of interaction with a database. This is Oracle’s definition:
A transaction is a logical, atomic unit of work that contains one or more SQL statements. A transaction groups SQL statements so that they are either all committed, which means they are applied to the database, or all rolled back, which means they are undone from the database. Oracle Database assigns every transaction a unique identifier called a transaction ID.
Lambert adds:
So for example you could have a number of SQL statements to set up an account, each with it’s query, like one for the name, another for family members, another for income, and so on. It would seem reasonable that ALL the fields to create an account would be a transaction, because that’s what you would want to be able to roll back. I think there would be a minimum of two transactions: 1 for the account, 2 for the plan. But there’s probably tons more, to save state between sessions, or to roll back incomplete file transmissions, say.
In other words, this figure is just as meaningful as the “hits” figure they gave us at first.
Let’s notice a second layer of misdirection: the mention of the Social Security Administration as the source. Um, the Social Security Administration subcontracted this all to Experian. And unlike outsourced call centers where the folks who answer the phone follow scripts that give the customer the impression that they are dealing with a company employee (“This is Sarah with Podunk Catalogue. How can I help you?”), there’s been no effort to hide the fact that Experian is running this gig. This practice didn’t start with Obamacare; it started right out of the box when the Social Security Administration contracted out its web access to Experian last January.
And remember, merely setting up an account was a process that took weeks of daily attempts for Olenick, a computer professional, to complete.
Olenick continues:
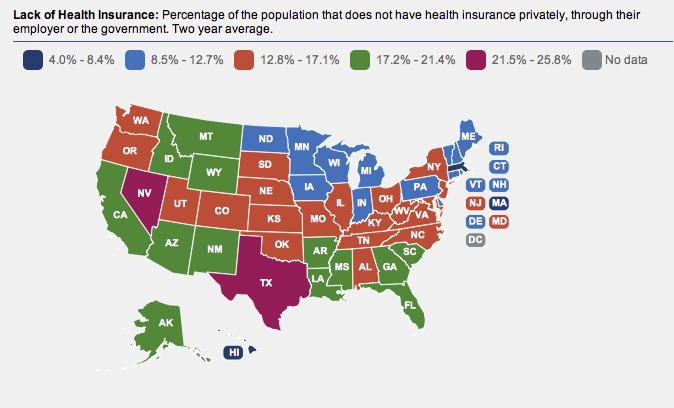
Wow, that’s a lot of accounts I thought, though then I did a double take at the numbers. California has 38 million people and about 20% are uninsured, according to the census and the Henry J. Kaiser Family Foundation, whose numbers are used for this type of analysis. So CA has 7.6 million uninsured people. Texas is the second most populous state with 26 million people and leads the nation with 24% uninsured, for six million uninsured people. My own Florida has 19.4 million people and 20% are uninsured, making for 3.9 million uninsured Floridian’s.
In contrast West Virginia has 1.86 million people of which Kaiser says 14% are uninsured, so there are 260,000 uninsured West Virginians. But according to HHS those quarter million West Virginians created almost as many accounts as the 7.6 million uninsured Californians and more accounts than the six million uninsured Texans or the 3.9 million uninsured Floridians…
I believe it is fair to infer that HHS/CMS – who did not respond to a written inquiry – is busted. They’re either outright lying about the number of accounts created or they somehow made it easier for people from West Virginia to use the federal exchange for testing. Either way their figures are grossly misleading.
I don’t mean to make an example of Olenick, but look what happened. He’s a careful reader, since he caught the significance of the numbers. Even so, we have an IT professional who works a lot with databases and hence more likely to be sensitive to what “transactions” might really mean per the HHS who was nevertheless taken in by Sebelius’ misdirection. He read her statement and took it to be referring to account creation, and not some mystery activities that take place after that point.
Nevertheless, his conclusion is correct. The figures are implausible, even more so than he suggests, as we will demonstrate.
This image underscores the point Olenick made, that despite its conventional association with moonshine and Appalachian poverty* (and West Virginia is indeed poor and rural), the state is middle of the road as far as the proportion of uninsured is concerned:
In December, as quoted by Associated Press (hat tip Lambert), “Tomblin administration officials estimate that between 37,000 and 60,000 people would seek coverage through this new marketplace.” So that 240,000 “transactions” for West Virginia is 4 times the highest number of individuals that state officials expected to sign up.
Pull out a calculator. The HHS number might be read to be making the bold claim that 92.3% of the entire uninsured population in West Virginia has signed up (240,000 divided by the uninsured population of 260,000). But uninsured individuals does not equal the number of accounts that would be created to insure them. Uninsured children and spouses would all sign up as part of a household; in fact, one of the most annoying and difficult parts of the Federal exchange account creation process is apparently telling the system who in your family is going to be signing up with you and identifying their relationship to the person creating the account correctly.
So take that 260,000 and divide it by the average household size in West Virginia, which per the Census Bureau, is 2.43. That might slightly understate the number of parties that might seek accounts (unmarried couples would apply as individuals) but it’s closer to the mark. You have roughly 110,000 uninsured households as the total universe.
Now remember, Obamacare (plus expanded Medicaid) was never was intended to cover them all. Nationally, over 30 million people were expected to remain uninsured, some because they weren’t eligible, others because they opted out (either by choice or necessity, as in the plans were too costly even with the subsidies). The CBO estimated that 14 million of the 48 million now uninsured will become covered as a result of Obamacare. That ratio is 29%. So, making some crude assumptions, you’d expect 30% of West Virginia’s households to sign up, which is 33,000. This is generally consistent with the state government’s estimates of 35,000 to 60,000, because those higher figures are for the number they expect to “seek insurance” which will include people who find they aren’t eligible or opt out once they look at the policies. Some subset of that set up accounts and has engaged in 240,000 “transactions.” Given how hard Olenick found it to be to establish an account, one has to believe that the number who have accounts is way lower than the 60,000, which is the highest estimate of the relevant universe we have so far, and that mean the average number of transactions per account in West Virginia is therefore considerably higher than four.
The wildly disproportionate level of transactions relative to the eligible population is even more ridiculous once you do more digging. You’d expect West Virginia to have its enrollment level as a percent of its uninsured population to be considerably lower than that of other states. Why? 35.9% of the population has no Internet connection anywhere, and over 20% does not have a computer at home, according to the Census. And yes, the Census was smart enough to capture people who don’t have either a computer or Internet access at home but use the Internet elsewhere; that’s an additional 5.0% of the total. And you can be sure those with no Internet access would be overrepresented among uninsured households, since both would skew poor.
And it’s not as if outreach could explain this difference. The Administration’s outreach efforts are targeting the “young invincibles” and Hispanics, who aren’t heavily represented in West Virginia.
Why are we harping on these numbers? Because the Administration is trying to turn a metric of failure into a badge of success. More transactions per person is not a good outcome. In this context, it likely means (among other things) difficulties finding information the prospective buyers found relevant (like “is my doctor part of the network?” or “are abortions included?”), trouble with subsidy information, and hangups in completing the enrollment.
The West Virginia outlier in theory could result from the fact that its exchange is a bastard child, a “partnership marketplace“:
A state that partners with HHS may assist HHS with certain functions, such as making qualified health plan recommendations and conducting aspects of consumer outreach and assistance.
But there’s no obvious reason why in practice it should be any worse than the Federal exchanges. Per Forbes (hat tip Lambert):
In a state-federal partnership, states will divide obligations with the federal government. For this partnership model, as well as the state-state partnership option, there is no requirement for a 50-50 split of labor. The states are actually more of a façade, whereby the consumers (individuals and employers) merely interact with the state. The federal government, on the other hand, will essentially perform all functions of exchange management except customer service and plan management. Moreover, states have the choice to take responsibility for only one or both of those functions.
And Sebelius is taking ownership for the West Virginia results and including it in her “hub” success stories, so the Administration acts like it owns the results no matter what the branding is.
None of the plausible explanations are flattering.
1. The HHS numbers are as utterly error-filled as everything about Obamacare, but no one cares about accuracy if the PR message is good
2. The Administration is just plain lying and assumes no one will catch it (“There’s a lot of black lung in West Virginia, so of course people in that state will sign up in droves!”)
3. The Administration has come up with some highly technical definition of transaction (as in particular types of database queries) so that their figures are technically correct even if by any commonsense standard the related declarations are lies
Given that the Administration has highly competent technologists working with the NSA, one would have hoped it would enlist them to cut the healthcare.gov Gordian knot. It now does look like the HHS types have called on the folks at the NSA, but only the ones who are experts in misleading wordsmithing under fire.
____
* I am permitted to say that sort of thing about West Virginia since I was born there.


Transactions is a meaningless measure, as you say.
If we are talking about transactions against a content database then we are talking multiple transactions everytime you view a page. E.g. one transaction for each image and text content used to construct the page.
Alternatively, if we are talking about transactions against something like an account database, then we are talking many fewer. Even so, it’s not clear what granularity we are talking about. Is every page view one transaction? Or logging in? Or changing something in your personal data?
Without that definition, “transactions” is meaningless.
The question then is why would someone quote such a meaningless number? From my experience, the obvious answer is that the real numbers are too embarassing. But there is also the possibility that the person quoting the numbers has no idea what they are talking about. I would guess both are true: the real numbers are awful and Sebelius has no idea what “transactions” refers to.
Dump em all
Yves, and thru all of this, nothing has been mentioned about the cost of the plans. For example, my current plan may now cost $400 a month (including vision and dental). When I finally get signed up, and search thru plans, what will upset me most is that I find a plan with marginal improvements in “care/services”. Yet the cost is still $400. Or, even worse, it’s $401 or higher. And the experts can brag all day about subsidies. But I still don’t know how I am supposed to provide my 2014 gross income per my 2014 tax return. And then, if my understanding is correct, I won’t get the subsidy until 2015’s tax return. So I have to pay higher premiums for 17 months (u always pay your insurance a month ahead) and then hope that I am not accused of fraud when my gross income is different by $1.
Good detective work! Obviously the drones who whipped up these flaky figures (on HHS’s high-powered electric adding machines) are innumerate, and assumed that their credulous little ‘consumers’ would be too.
Maybe they meant ‘Virginia,’ or ‘the Virginias,’ or just ‘barefoot hillbillies in general’ (I’m permitted to say that, having earned a degree in Arkansas).
To paraphrase from the 1985 cautionary tale of New Coke, as reported on Wikipedia:
An IT legend in her own mind …
Correct me if I’m wrong but isn’t it the only state that isn’t blue in the one’s listed? Red states are loving and signing up for Obamacare too ….
The only word I can think of to describe the US healthcare system is “surreal.”
It is a perpetual profit machine which is unrelentingly self-serving. It is Adam Smith, bowdlerized of any of that foolish talk about “moral sentimens,” on steroids.
Mexico spends about 1/6 per capita what the US does on healthcare, and according to the UN’s objective and measurable metrics ranks about the same as the US does in quality of healthcare.
I ventured onto the healthcare.gov site last week. What a shocker! I’m 61 years old and in good health. I was presented plans that cost anywhere from about $400 per month to $900 per month, with $6000 deductibles and anywhere from 10% to 20% co-pays.
The problem is that here in Mexico there are cheap generic drugs. I take drugs for both high blood pressure and high cholesterol. These run about 10% of what they do in the US, so I buy them outright for about 1/2 what my 20% co-pay in the US would be.
If I get a cold or some sort of throat or respiratory infection, I go to my pharmacy where there is a doctor on duty. For about $3 or $4 he will examine you and write a prescription, which again runs a small fraction of what it would in the US. The total cost usually runs about $8 or $10. And my personal experience has been that the drugs they prescribe work just fine.
If I have to go to a specialist, the cost for an appointment is about $40.
I recently had to have two new crowns installed on a couple of teeth that had disentigrated. These cost about $80 each.
I’ve not had any major surgery. My friends who have say the cost here in Mexico is a small fraction of what it is in the US, probably not much more than what the 20% co-pay in the US would be. I have one friend who doesn’t trust Mexican hospitals. He’s had several major surgeries, so he flew to Thailand for them. He says the care there is far, far superior to what he received in his native New York, and a fraction of the cost. He says he prefers first-world healthcare, and the extraordinary patient care, like that available in Thailand, over the third-world healthcare available in places like his native NYC.
I went back to the healthcare.gov site this morning to review the various healthcare plans I can buy in the US. The site seems to have lost all the original data I imputed, either that or I can’t figure out how to get back to the page where my various healthcare plan options are displayed.
I sure hope, being an expatriot and having far better healthcare options, that I can qualify for some sort of exemption from ACA and escape the entire US health”care” prison.
Good luck with avoiding the dragnet. While the weaving on the social safety net is becoming more open, the revenue collection side of things is becoming a 600-knot-per-inch envy-of-the-best-Persian-weavers dense.
Very helpful comment. The whole HC issue here in America is surreal because we don’t understand that we live in a very sophisticated semi-totalitarian regime. We don’t have massive Gulags, we don’t have information churned out by a central government bureaucracy but we have a virtual Ministry of Truth that carefully monitors the information the masses have been receiving and is now beginning to break down just a bit by the internet and additional news cable networks (Al-Jazeera, RT) who offer other perspectives.
The point is that what you experience in Mexico and what other expats experience around the world is virtually unknown and unreported on in the United States where people are programmed to program themselves to ignore the truth, to not see the elephant in the room through the techniques of misdirection–as the old Subgenius slogans go “pull the wool over your own eyes” and “relax in the safety of your own delusions.”
Virtually no one knows anything about other cultures in this country and people are usually stunningly uncurious. I find people at all levels of education largely uninterested in how health-care issues and healing modalities are handled in other societies.
“We don’t have massive Gulags, we don’t have information churned out by a central government bureaucracy…”
Of course, the irony is that trying to find an extreme which we don’t have, even this stuff we do essentially have, from the criminal justice system to the national security state to higher education to stenographer media.
CPI, TARP, FISAAA, drugs, abortion, oil spills, prisoner abuse, wars, take your pick – choose a policy area where secrecy and lying is not the approach of the central government bureaucracy.
“Virtually no one knows anything about other cultures in this country and people are usually stunningly uncurious. I find people at all levels of education largely uninterested in how health-care issues and healing modalities are handled in other societies.”
That’s actually rational of course. They don’t live in those other societies (though some can cross the southern border depending on where they are in the U.S.) and even a plane trip to Thailand may be out of the budget. And they see no hope of actually sucessfully reforming the U.S. healthcare system (and of course they are pretty much correct or Obamacare wouldn’t even exist).
I don’t buy this excuse for American insularity for one second.
Pull out a map. Australia is further from ANYWHERE than the US is. Four hours flight to Bali, roughly 9 hours to Hong Kong and Singapore, 12 hours to LA, 21 hours to London. Yet every Australian I met, even ones from modest backgrounds, had traveled abroad, most extensively. And this was when the Australian dollar was weak. They’d stay in B&Bs or hostels, use train passes to get around, etc.
By contrast, I was friendly with a partner at PWC, which in those days had a big management consulting arm. He said only 30% of the firm’s partners in the US had passports. Their not traveling had nothing to do with money, it was sheer lack of interest and perhaps even dislike of the unfamiliar.
“We don’t have massive Gulags…”
Yes we do.
http://www.amazon.com/Sick-Justice-Inside-American-Gulag/dp/1612344879/ref=la_B000APTJ4S_1_2?s=books&ie=UTF8&qid=1383771492&sr=1-2
You nailed it. We live in a virtual island of slanted information, all designed to support the existing (captured) power system favoring massive wealth expansion for those who already have it.
Mexico, I believe you are exempt; see Consumer Reports here; they have a useful continuing series on ObamaCare questions.
That’s good news.
Thanks for the heads up.
For the sake of future reference, are his fears about Mexican hospitals justified? And how would one go about arranging treatment or surgery in Thailand?
Time to claim your Mexican citizenship, I think. Or do they not want you?….
I think we are seeing misdirection going to new heights because the right-wing has shown how easy it is to make people believe the most stunningly idiotic things. Americans are looking to believe things–if someone they like says something then it’s true whether it’s Sarah Palin or the President. If they fly the right tribal colors then they are right and correct.
As Uncle Walter [Cronkite] once said, “America’s health care system is neither healthy, caring, nor a system.”
“I’ve been asked a lot for my view on American health care. Well, ‘it would be a good idea,’ to quote Gandhi.” ― Paul Farmer, medical anthropologist and physician, best known for his humanitarian work providing “first world” health care for “third world” people
“It is very expensive to give bad medical care to poor people in a rich country.” ― Paul Farmer
“Obamacare was almost the perfect example of politics in the Bubble Era, where the time horizon for anyone with real power is always close to zero, long-term thinking is an alien concept, and even the most massive and ambitious undertakings are motivated entirely by short-term rewards. A radical reshaping of the entire economy, for two election cycles’ worth of campaign cash – that was what this bill meant. It sounds absurdly reductive to say so, but there’s no other explanation that makes any sense.” – Matt Taibbi, Griftopia: Bubble Machines, Vampire Squids, and the Long Con That Is Breaking America
More Griftopia on Obamacare @ http://www.scribd.com/doc/97838653/Griftopia-on-Obamacare
“White Liberals think all the world’s problems can be fixed without any cost to themselves. We don’t believe that. There’s a lot to be said for sacrifice, remorse, even pity. It’s what separates us from roaches.” – Paul Farmer, Mountains Beyond Mountains: The Quest of Dr. Paul Farmer, A Man Who Would Cure the World
Those who believed the administration’s numbers have just landed at JFK or LAX. This administration deserves a Nobel for splitting the famous Fog of War into constant fog and constant war. Way to go guys!
About the healthcare.gov software system: almost everything read and heard about it is wrong. As Michael Olenick rightly says the condition of the system is grave. Experience tells us that when systems that large get that bad, the fasted and cheapest solution is to start all over again. I once worked on a financial software system that had about 400 known bugs, i.e. problems, when I was called in. The industrious programmers solved most of them in a week. Alas, the following week we had 400 new bugs. This beauty continued for several months. The wise CEO scrapped the system. He saved millions.
The gov still sets the end of November as system is ready for prime time. Since we don’t know anything about the system except that it doesn’t work,(all other information, media/interviews/experts, is nonsense.), the chances of that date are slim but not none. I would gladly bet on none.
“Experience tells us that when systems that large get that bad, the fasted and cheapest solution is to start all over again.”
You speak the truth here, if the system is bad enough it’s faster and cheaper and more efficient and likely to yeild better results to start all over from scratch. And I’m just talking software, just the time and intellectual effort needed to understand bad code. Though if one were to generalize that to our political and economic system haha …. maybe we also should start all over from scratch.
“Though if one were to generalize that to our political and economic system haha …. maybe we also should start all over from scratch.”
Three-quarters of state legislatures can lawfully elect to do so any time they like. Eventually they may have no other alternative.
Gee, it sure is odd that “punch list” isn’t public.
Agreed. So can the Gov’t go from concept to completion in 30 days time, to finish by the end of the month? That’s quite a raging hackathon.
The fact that an account is created does not exclude the possibility that it is a duplicate account. The account creation problem was one of the earliest to be found as almost all people initially could not log on the accounts they had just created.
The major bug was in the enrollment process itself. And likely that was because not all of the private insurers had completed and test their end of the interface that had to be created because CMS could not depend on using the already defined HIPAA 834 data transaction; it had not been implemented as a uniform data transaction across all insurers even after a decade.
Transactions is an apples to oranges comparison when looking at difference implementations.
Maybe the developers in WA did a great job and only called the APIs that access the SSI database once and cache the data in their database while the Federal contractors call the API every time they display plan. Heck, maybe there’s a bug in the Federal site that calls the API passing in WV data when anyone hits the Federal site from say TX (or everywhere).
No, Sebelius is talking numbers all in the Federal exchanges. Even though West Va. is a “partnership”, the information I’ve found suggests that they are in fact running on the Federal exchange platform.
NY is supposed to be a completely separate exchange, so why is Sebelius quoting NY numbers?
I’m inclined to believe something closer to the usual business definition of “transaction” is operative here, for two reasons. It’s the counter that would most likely appear on the C-suite dashboard as a number of interest to management, rather than internal middleware stats that don’t have a direct relation to the business. Also, the “multiplier effect” of a large number of transactions per actual conversion jibes with the reports of multiple spurious 834s (+n) and corresponding cancellations (+n) for each new policy (+1?).
Of course, the dashboard is still not the road…
A problem with Obamacare that has not gotten a lot of coverage is what it is doing to the career paths of doctors. It is nearly impossible to sell a physician practice now to any entity except a hospital. The time tested practice of the older physicians selling out to the younger physicians when they reach retirement is gone–instead they sell to hospitals, because the hospital is the only buyer.
BTW, I am not involved in medicine. I hear about the changes in business practices from friends who are. Please correct any misunderstandings I have if you know more than I do.
In five years, hospitals will own most medical practices, because the ACA requires practices to belong to an ACO, accountable care organization, if they’re going to get re-imbursed by medicare or medicaid. It also requires steep expenditures on IT, in order to generate information for the government to analyze to determine whether an organization gets bonuses or penalties for their medical or cost containment outcomes. This sounds to me like a recipe for corruption and indifferent patient care, particularly since the ultimate beneficiaries of the payments are hospitals, the people who brought you the $60 aspirin tablet.
In any case, this is all about the referral stream. While theoretically a doctor in a hospital owned practice can refer anywhere, in practice, they will be referring within the organization, and woe be to the physician who doesn’t go along. They will be unemployable.
That stinks. So doctors will be wage slaves now too? Oh well I extent the solidarity pipe to them then :). Solidarity forever … one of these days.
Well, life for young dentists is a horror show. They graduate, get picked up at a corporate dental farm, where they are forced to abide by the profiteers’ borderline malpractice assembly line milk the patients rules.
They then get a series of crappy reviews on the internet, and if/when they move off the corporate dental farms and into their own practices, they have to live down their bad reputations.
I know this because I recently had to look for a new dentist, and I felt as bad for them as I did for me.
I then picked someone with an established private practice, and it’s worked out fine.
But, my, what a mess. Talk about having to run the gauntlet.
Awesome write-up again.
It’s been pretty clear since the 2008 campaign and the Dem convention language and the OFA bus tour and everything else that Obama’s actions on healthcare have been fraudulent.
But it’s still fun seeing that described in way more words.
The blizzard of BS numbers from HHS has only begun. The true enrollment numbers must be catastrophically bad.
I can’t remember where I read it, but someone who was doing investigations of the federal website mentioned that he got far enough along in the process that his “application” was submitted even though he hadn’t finished it. I wondered about week ago whether or not the application process was submitting everything anyone entered to processing, and that this might be the origin of the multiple 834s that some insurance companies were reporting up to the meeting with Jarret a couple of weeks ago. This could also explain the huge numbers of “transactions” processed by the IRS and SS. I have never gotten passed the verify identity process, but I wonder if I am responsible for hundreds of transactions just by myself.
I realize that in the Republican House everything is a scandal and therefore grounds for dismissal or impeachment.
Is there a legitimate case for Sebelius to step down? Besides the ACA website fiasco there’s the Frontline report
[ http://www.pbs.org/wgbh/pages/frontline/hunting-the-nightmare-bacteria/ ] pointing out (1)CDC has no authority to force hospital to report outbreaks, (2) little attention is being paid at the highest levels of government.
Sebelius oversees both CDC and NIH. The report left this viewer questioning the zeal government is putting into it.
Capitalism has all but abandoned new drugs to fight NDM-1
and other resistant bacteria. This is the wrong time to be
pinching austerity pennys in an agency charged to deal with global pandemics. Is it time to take off shoes and pound the podium? Again the true scope of the problem in the US is unknown because reporting is not required.
You have to remember Benghazi when it comes to accountability. The GOP elite loved the idea of knocking over Gaddafi to dole out new contracts for multinationals as well as arms contracts.
The GOP isn’t holding hearings on standards we might have had for handing over weapons or whether we overstepped international law by targeting Gaddafi in a ghost town because they like those things, but they hate the Democrats.
A U.S. ambassador was killed, and I think the GOP thought this would be a foreign policy embarrassment especially when support for the Libyan intervention was limited and largely derived from long term dislike of Gaddafi from the 1980’s within the population at large. I don’t know anything about the whole situation. I don’t care. The ambassador was in a war zone for a war he helped create. Good riddance to bad rubbish, but the GOP’s complaints about the death of the ambassador don’t attack the system perpetuated this war which is American imperialism and the demand for non transparent government contracts to the MIC.
You are pointing out practical reasons why Sebelius should be fired/removed/resign in disgrace, but the GOP would have done it the same way. The GOP wants to hurt the Democrats without attacking the Democrats for what they want to do which is run government for private profits just like the Democrats. Everything our current government does is about short term profits of top industries.
There may be grounds for various actions, but Sebelius will only bother the President and Democrats when she becomes a political liability among Democratic partisans or challenges Dear Leader. The Republicans won’t attack her in a realistic manner because they don’t want to attack the profit making schemes much like Benghazi/Libya.
sounds sensible to me. thanks for that coherent exposition of the issue.
As for Sibelius, of course she should resign–but officials seldom resign over policy failures in this country because they don’t want to give the false impression that anyone is accountable. Sibelius says she takes “responsibility” then resign! But that’s not the way the game is played everyone takes responsibility but there are no consequences for upper tier managers in an increasing number of organizations.
Let’s say that everything is a cluster—- and the ACA is doomed to failure and needs to be repealed. Then what? Nothing. Nothing will happen because the conservatives/tea party/rwnj types in Congress will see to that. We will go back to our old system; a system far worse than the ACA. Millions of young adults will lose insurance. Millions with pre-existing conditions will be denied insurance…I could go on.
What do you think will happen? I agree universal health care is the only realistic plan to help all but is it realistic to think that will pass in this political climate? I read this blog everyday and what do you propose the Dems do that has a remote prayer of passing? Let’s face it, the reps will do nothing and so it rests on the Dems to come up with something.
Don’t get me wrong: reporting problems is fine but what solutions are there?
The first step is to acknowledge the problem. One major problem with ACA is does nothing to undermine the system of hospital cartels which is the primary problem with healthcare delivery and costs in this country.
Deflection isn’t a solution, and pretending we aren’t in a healthcare crisis is absurd. ACA was never the best product which could be achieved, and pretending the President and the Democrats acted in good faith is absurd.
I’m going to ask what are the problems with healthcare and ACA because your comment seems to be a nicer way of saying, “shut up be nice to Obama.” What are the problems?
As for solutions, one stop giving money to right wing Democrats. As Alan Grayson specifically and Dean’s 50 state strategy candidates demonstrated, Democrats can win in Republican districts when they actually run as Democrats. Rahm Emmanuel’s pro-gun, anti-choice, pro-corporate candidates couldn’t even in 2006.
The second step is Democrats are in need of new leadership. Pelosi and that punch drunk Mormon convert have had their time. They and their underlings have to go.
The third step is running on a comprehensive plan to solve the healthcare crisis. Yes, that means attacking the hospital cartels, and before you say the GOP will be mean, the Democrats did the bidding of the health-rentiers and lost in 2010.
Let the GOP vote against good policy. Despite the debt ceiling fiasco, Democrats actually improved their polling when they did the upstanding thing, unlike their summer performance of advocating for more war and militarizing the border while providing faux-amnesty to con rubes when their polling numbers down. I would love to see Republicans vote against heating assistance for poor people instead of some generic cloture vote, but why don’t the Democrats do that? Why don’t the Democrats make the GOP vote against extending the Bush tax cuts for the middle class while ending them for the rich?
It takes time to fix things because Democratic enablers denounced critics as racists and unserious people while they championed poor policy. Not only do we have to fix the policy, we have to get the GOP out of the House which was lost because minorities and the young didn’t vote for Democrats in 2010, not white liberals who showed up, and we have to convince the people who are getting hit with the ACA every day to take another chance.
The best step you could take is stop deflecting for the Democratic elite and let them take their lumps. Why aren’t you demanding reform from the Democrats?
It was President Obama who proposed a budget with funding cuts to LIHEAP (low income energy assistance program) from just over $5 billion to $2.5 billion. Ultimately, Congress and the White House reduced funding to LIHEAP by 25%. Do I trust the Democratic Party or this President to do the right thing for the people, NO.
I am aware of the President’s and Democratic malfeasance, but the solution to GOP obstruction is to make sure they have individual records voting against good legislation, not bad legislation they once proposed.
Admittedly, it takes time because trust is hard to rebuild, and Democratic partisans have spread so many lies rebuilding the brand in the eyes of people who have been turned off politics all together and the people who will be harmed in the near future is a gargantuan task largely created by Democrats who whined about liberals not slavishly lauding the President for treating everyone in the country like shit.
Solution: Single Payer Healthcare System!
Yes, our status quo healthcare system is very broken for the vast majority of people in the United States. But, the solution is not to make the health insurers and pharmaceutical companies even stronger ensuring this inhumane system for an even longer period of time which is what Obamacare does. The question you should be asking…why are we allowing a system in which HEALTH insurance companies would even be able to practice if they are the “only game in town” and yet can bump people for “pre-existing conditions”? Why AREN’T all young adults provided access to healthcare? And, why are we as taxpayers going to transfer and “subsidize” further the insurance companies which is exactly what Obamacare does.
As for the Democratic party, it should be obvious by now that they will do nothing for the people that doesn’t help the corporations and their campaign contributors first. Replace every member of Congress (regardless of party affiliation) in every state until they get the message that corruption is no longer an option for them.
Something that’s very simple and concrete is removing the requirement that states wait until 2017 to get “waivers” from HHS to “experiment” with single payer systems; it’s only thanks to Kucinich that the waiver is there at all, but why must we wait ’til 2017 to move to system that we already know works? Maybe we’ll strike it lucky, Saskatchewan-style.
Every time an Obot goes “I really love single payer but–” suggest this minor fix to them and watch them start stumbling about, eyes bleeding.
About problems and solutions, one needs to understand that there are symptoms associated with problems. It is very important to cure a problem and not a symptom. Message there is be sure you sort the problem out of all the symptoms.
Well…..
History tells me……
A general strike………
And, in this case a general march on Washington DC…..
Pushing a gallows……
Just saying………
To get all conspiratorial: maybe the website not working is the plan. It’s a way to delay Obamacare even more, even though the planned start of the exchanges already had a built in delay of years from when Obamacare was first passed. Because if the program is going to suck anyway, might as well keep delaying actually delivering it, and keep selling empty promises of a wonderful healthcare system instead. Maybe it’s Obamacare itself that is vaporware.
The 11-dimensional chess theory… I’m pretty foily, but I doubt this. The optics on the rollout are really bad, and Obama does care about optics, if nothing else.
One fundamental Emperor’s-New-Clothes/Elephant-in-the-Room question that I’ve never seen discussed, a question which my pea-sized brain thought fundamental to the capitalist system, is, “What value does the Obamacare system add to health care?”
Just curious.
If anything, it extracts value (if we conceive of human health as a value, not just the rents). As does the health insurance industry, which also adds no value, being 100% composed of parasitical rentiers.
Ah, just as I suspected.
Ps. Love your work and am touched by the personal response and the fact that comments towards the end are indeed read.
No reply to your reply necessary.
It’s always interesting to notice the hugely different evidence people require to know they are being lied to.
Some see the lies before the fact. Others only after. ‘Funny thing is that those who haven’t a clue until it’s too late are those who also credit their own superior intellect as self-evident license to order other people around.
Krauthammer recently got off a one-liner to describe this sort: “Liberals don’t care what you do as long as it is mandatory.”
Transactions are the new hits.
From what I gather, about anyone that’s healthy and who looks into it, being mandated to buy corporate insurance, gets sticker shock when they finally see it. They can’t afford it and besides, it’s not worth it. And upon learning that the IRS withholding is much much less, without any real penalty, that is what the masses are going to decide to do.
So what are the ramifications?
New payroll tax witholding rules to see to it that the penaltax is covered, maybe. Low-wage workers not uncommonly view the income tax refund as something like a Christmas club account. Taking a one or three hundred dollar bite out of that payout would make their situation more precarious if anything.
Ironically, the self-employed are the most likely to avoid the penaltax. But how hard is it for one to get a passport with a grand or two in delinquent Federal tax debt on the books?
Well the penalty, when it kicks in, is only 1% of income. Yea, the IRS can keep that as a tax. It’s going to pale in comparison for anyone but those that have enough money it doesn’t matter. I don’t think that bite is a deterrent.
But it seems to me that we are going to be seeing self-employed among that 5 percent drop off from paying into the system, at the same time people that are very poor, with a laundry list of ailments, come onto the system. How would that not in turn make the insurance companies raise rates even more on what’s left of the 5 percent?
I also do not buy into the notion that the good 20-30 something uninsured Obamabots are just gonna start chucking their dollars at the government. It doesn’t fit their profile. They too, are counted on to foot the bill.
Maybe I’m missing something that plans on keeping this death spiral at bay.
Being a West Virginian, I’m not really surprised, nor am I suspicious of a whitewash. I really do think West Virginians are different when it comes to government service. 1) we’re quick to sign up. 2) we’ve been neglected by the insurance industry for years, 3) we’re old, 4) we’re sick, and of course, mostly importantly, 5) we’re uninsured. Also, I’ll note that Obamacare had a heck of an ad rollout in the state prior to the care coming out. We’re actually stoked about Obamacare here.
My only choice, as a small business owner before, was a Blue Cross policy with a $3,000 deductible. Next year it will be $1,000 for me and my employees, cost less, and provides more coverage than we had before. My dad, who owes another small business (we still have these in WV) signed up on the individual exchange. He was told he qualifies for $542 in subsidies. The local blue cross gold plan with the $500 deductible cost $502 a month. Pry that out of his hands!
The animosity on this blog to Obamacare is really overblown. This product rocks when your living in WV.
Yep. A lie. Small, rural, isolated, not well known; people will believe almost anything about WV. When the curtains roll back you will be surprised, not by the number of sign-ups, but by the number willing to pay the fines.
The number of people who are going to make the local news over billing disputes not being covered by Obama is going to be shocking.
I predicted the ACA software would have to be replaced wholesale over a month ago.
It was an easy prediction. The people in control of the project were careful to avoid even reasonable practices, much less best practices.
You know something is terribly wrong when you can’t sign up because the forms come back with somebody else’s personal information, which makes any attempt to use the site an invitation to identity theft.
Or worse.
I won’t even try and cover the details of how f#cked up it sounds.
It’s a system dependent on:
1) Transactional integrity when it is connected to a somewhat local database. (commit or rollback of data and a “record” – whatever is designed to be an important “transaction” in the overall workflow – like in this case identify user, create account, collect the rest of user data…etc – move thru the next steps of verification, obtain further info, present applicable plans to a user- which is supposed to end up as a commercial “transaction”.
2) Like most systems, ever since IBM built the second mainframe, the data isn’t all in one place. We’ve been moving it around ever since then. I won’t bore everyone with the details but sometimes it’s real time methods (probably with Experian) and some times it’s batch processing methods.(some sort of batch file transfer, or nowadays it might be a “web service”)
During all of this data transfer, processing, and moving around activity, the system has to check that everything has proceeded correctly with good data. The software industry has built in “database transaction managers” into web severs, middleware and databases to simplify the task of commits and rollbacks for application programmers/system architects, but you still have to write the code yourself when interfacing with third parties.
I guess what’s her name could have told us how many people successfully signed up for O Care – using provider sign up data.
But she played the techie card and read us the Oracle transaction sum report. Haha*
* This is how Bill Gates and Larry Ellison used to race databases. But you have to be a data base racer to understand it.
‘… Given that the Administration has highly competent technologists working with the NSA, one would have hoped it would enlist them to cut the healthcare.gov Gordian knot. …’
http://www.gocomics.com/tomthedancingbug/2013/11/01
always interesting what the MSM takes notice of, in light of the gaping hole of what it does not.
http://news.msn.com/us/the-hidden-marriage-penalty-in-obamacare
Uh oh. Exclamation point.
Rumor has it that the ACA website has already been hacked by several parties besides the NSA, CIA, FBI, Homeland Securty, and assorted unnamed contractors.
Did you really suppose virulently hateful wingnut pubs wouldn’t be highly motivated to pay for ways to attack it?
A lot of people are disgusted, but an unmanageable number are freaking out, and some people are really, really pissed off. Imminent developments are unlikely to be positive, given the skills of foreign operatives who do not like the U.S. very much.
Failures in the ACA program overall have the potential to disrupt the general population significantly. Many people have committed themselves to a dysfunctional system and can be expected to spend rather a lot of the rest of their lives try to straighten it out.
All very bad. I think we’ll find that the overall result is about what you expect when an intrusive, national-scale software and systems project is run by ignorant, greedy, disconnected, self-dealing, self-interested, and otherwise clueless politicians who are desperate for bigger and better ways to fuck over the general population but aren’t remotely qualified to actually pull it off.
[Quietly backing away from the blast zone . . . ]
This CP article shouldn’t be news to NC readers (in fact, Yves is quoted within), but the truth cannot be repeated enough:
The Truth About ObamaCare
http://www.counterpunch.org/2013/11/05/the-truth-about-obamacare/
“It’s not a government takeover of medicine. It’s the privatization of health care. If you took George H. W. Bush’s health plan and removed the label, you’d think it was Obamacare. If you thought a single-payer advocate would say these words, you’d be wrong. It was Republican lobbyist Tom Scully speaking to a room of fifty large Wall Street investors as quoted in a recent article by Wall Street-funded business journalist Adam Davidson,[1] in the New York Times Magazine.”
Isn’t this a bit of turd-polishing?