By Lambert Strether of Corrente.
This post attempts to describe the state of play on AHCA/BCRA/ObamaCare replacement and/or repeal (a ginormous hairball of bad craziness that I’ll label “TrumpUncare,” which should not be taken to imply that Trump has taken a coherent position on anything, except violating his campaign promises). Since the state of play is inordinately complex, this post is inordinately long. However, its structure is simple, and it’s designed to show that the drivers for TrumpUncare’s success or failure are predominately local (and as a corollary, that most of the coverage you read in the Beltway press is worthless). Adding: The post is also inordinately late, for which I apologize, but I wanted to get the whole thing on the table immediately, since the Senate has now returned.
In the first section, I’ll look at the Senator, Jerry Moran (KS), who inspired me to take the approach I have taken. Then I’ll briefly review the math, and list the Senate Defectors who are standing in the way of TrumpUncare’s passage. In the next section, I’ll rule out a number of oft-bruited monocausal national explanations for TrumpUncare’s political difficulties, in the form of maps. In the final section, I will look — as best I can[1] — at the local pressures that the Senate Defectors face. I’ve numbered every section so you can skip over the boring bits. I’ll conclude with a few reflections.
(1) The Math, the Defectors (and Something Not the Matter With Kansas)
First, let’s look at Senator Jerry Moran (KS). From The Times, on July 6, as Senators left for their recess:
Unlikely Defector Underscores Challenge for Senate Health Bill
“Unlikely” to The Times and the Beltway, perhaps. Could it be that more locally focused coverage would have helped? More:
For about 90 minutes on a hot summer day, this tiny town in northwest Kansas, with fewer than 300 people, took on an improbable role at the center of the national debate over the future of health care. Mr. Moran did something that almost none of his Republican colleagues are doing over the Fourth of July recess: He stood in front of his constituents at a town hall-style meeting.
Mr. Moran faced probing questions about health care, exposing constituents’ deep concerns about the bill, though the gathering was notably polite. Dressed crisply in a suit, white shirt and red tie, Mr. Moran stood at the front of the packed room with the crowd of more than 100 spilling outdoors through an open doorway in the back.
Mr. Moran represents a state Mr. Trump won by about 20 percentage points. He won his own re-election by an almost two-to-one ratio. He does not have to contend with pressure from a governor who has been publicly critical of the bill, unlike colleagues from states like Nevada and Ohio. And yet he has become an unlikely Defector as Mr. McConnell tries to find the votes to pass the measure, starting next week.
In Palco — about halfway between Kansas City and Denver, and near where Mr. Moran grew up — the senator outlined how he was assessing the bill. Would it make premiums more affordable while still preserving coverage for people with pre-existing conditions? Would it help or harm the availability of health care in communities across Kansas?
“I am a product of rural Kansas,” he said. “I understand the value of a hospital in your community, of a physician in your town, of a pharmacy on Main Street.”
The debate over repealing the health law is playing out in a year when Kansas has been buffeted by political turmoil and blunt challenges to conservative policy making. After years of budget woes, state lawmakers voted to reverse course from the sweeping tax cuts championed by Gov. Sam Brownback, a Republican.
They also voted to expand Medicaid under the Affordable Care Act, driven in part by concerns about the financial viability of rural hospitals. Thirty-one states have expanded Medicaid under the health law.
Mr. Moran came out last week against his party’s plan to repeal and replace the Affordable Care Act.
Dozens of members of the Kansas Legislature, including numerous Republicans, signed a letter to Mr. Moran and Mr. Roberts saying that the repeal bill that passed the House in May would have “a profound negative impact on Kansas.” And hospitals, family physicians and other health care providers urged the senators to oppose the Senate bill.
But it remains to be seen whether Mr. Moran will stick with his opposition.
This article struck me forcibly because I hadn’t seen keeping rural hospitals open as a driver in “preserving” ObamaCare. But here it is, and as soon as you think about rural Kansas, it makes sense. (Keeping hospitals as such open is not a driver; hospitals are widely distributed, and aren’t necessarily a driver for other Defectors). Assuaging local concerns like this makes legislating hard. (Unless you’ve got the clout of a Max Baucus, and you can legislate single payer for one town in your state.) And the legislating is even harder when the bill is poised on a knife-edge, as TrumpUncare is:
While Republicans enjoy majority power in the upper chamber with 52 seats, the party can only afford two defections to pass the bill with Vice President Pence likely casting a tie-breaking vote.
And there are a lot more defections than two. The Cook Political Report summarizes the math, and the state of play:
[O]n health care, congressional Republicans are damned if they do and damned if they don’t. The fact that the initial plan from Senate Majority Leader Mitch McConnell’s (a pretty smart guy) had at least four Republicans (Ted Cruz, Mike Lee, Rand Paul, and Ron Johnson) who thought it didn’t go far enough in eliminating Obamacare, and at least five (Susan Collins, Lisa Murkowski, Shelley Moore Capito, Dean Heller, and Rob Portman) that worried it went too far showed that this was a matter of splitting the baby.
I think Cook’s two buckets are a reasonable shorthand, though it’s interesting he doesn’t label them “moderate” and “conservative.” In what follows, I hope to show there’s no single explanation for Cook’s buckets.
(2) Monocausal Explanations Ruled Out
(2)(a) Ideology
One thing I want to get out of the way is the “moderate”/”conservative” (“right wing”) dichotomy. Look at the voting records from FiveThirtyEight:
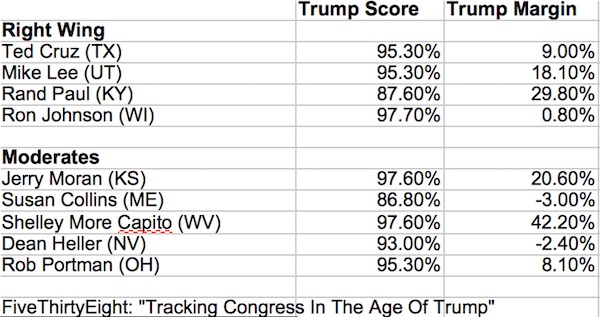
If there is a pattern here that shows who opposes TrumpUncare as a “moderate” and who from the “right wing” I’m at a loss to discern it. In other words, Cook’s “too far” and “not far enough” don’t map directly to “moderate” and “conservative,” since both buckets vote more or less the same. (Granted, the exceptions — there are always exception — are Rand Paul (KY) and Susan Collins (ME), but they are each sui generis, Paul on ideological grounds as a libertarian, Collins as a political icon and the last of the famously moderate and bipartisan “Maine Girls.”)
The names of all the Senators in the charts that follow are color-coded as follows:
Red (Cook’s “not far enough”)
- Ted Cruz (TX)
- Mike Lee (UT)
- Rand Paul (KY)
- Ron Johnson (WI)
Orange (Cook’s “too far”)
- Jerry Moran (KS)
- Susan Collins (ME)
- Shelley Moore Capito (WV)
- Dean Heller (NV)
- Rob Portman (OH)
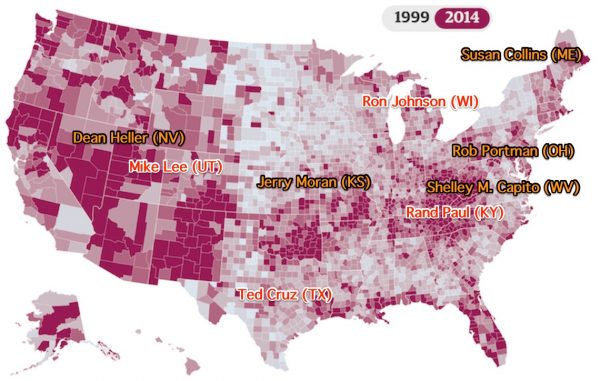
(2)(b) Medicaid Expansion
Granted, once people have a concrete material benefit, it’s hard to take it away from them:

However, with the single exception — there are always exceptions — of Shelly Moore Capito (WV), there doesn’t seem to be a pattern among the defectors, either: Ted Cruz (TX) and Jerry Moran (KS) both have light losses; one is in the “not far enough” camp; the other in the “too far” camp.
(2)(c) The Opioid Epidemic
It occurred to me that TrumpUncare’s Medicaid cuts might impact treatment for opioids, a very concrete material benefit:
Here again, I don’t see a pattern among the defectors. The (deindustrialized) Ohio Valley, for example, has a serious opioid problem, but Portman (OH) and Capito (WV) are in the “too far” camp, and Paul is in the “not far enough” camp. Both Utah and Nevada look like they’re in trouble, but Lee (UT) is “not far enough,” and Heller (NV) is “too far”).
(2)(d) 2016 Margin of Victory
It occurred to me that defecting Senators might be concerned about their re-election, whether in 2018 or later, if they take concrete material benefits away from their constituents:
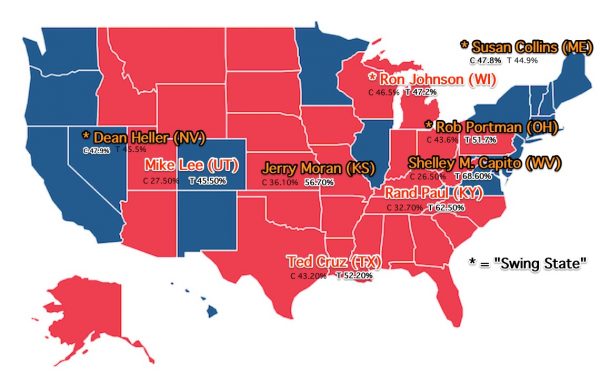
Here again, I don’t see a strong pattern. Of the four defector Senate seats open this year, Heller (NV, Clinton by <2%), Portman (OH, Trump by >8%), and Collins (ME, Clinton by >3%) are in the “too far” camp, and Johnson (WI, Trump <1%) is in the “not far enough” camp (though Johnson is unique). The others are all over the map.
(2)(e) 2018 Swing States
It occurred to me that defecting Senators in swing states might be especially susceptible to the pressure of party loyalty, especially from donors:
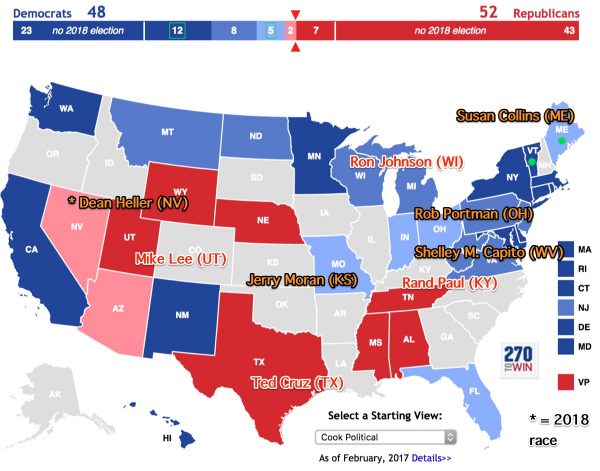
As it turns out, the only case is Heller, and if he’s suspectible to party pressure, it hasn’t shown up yet.
I imagine a professional, full-time politicians like Mitch McConnell solves a Rubik’s cube like this all the time. Beltway pundits, however, do not and cannot; although that humble bloggers can, by taking a look at the local state of play for each defector.
(3) The Local State of Play for the Senate Defectors
First, let’s look at the “too far” defectors:
(3)(a) Rob Portman (OH)
Rob Portman is a unique case, because he’s made himself a reputation as a leader in finding solutions for the opioid crisis, which TrumpUncare’s Medicaid cuts would affect. From the local Toledo Blade:
Sen. Rob Portman is the Senate’s leading authority on the opioid epidemic and his party’s leading voice of compassion on the matter in Congress. Killing funding for the fight has long been his line in the sand.
Mr. Portman, along with Republican senators Shelley Moore Capito of West Virginia and Susan Collins of Maine, has previously been adamant that any health-care plan should include significant funding for substance abuse treatment and prevention. He was targeting $45 billion over 10 years. The current Senate plan chips in $2 billion for 2018. That is a pittance and, combined with the long-term scale-back of Medicaid, could be catastrophic.
(More on Shelley Moore Capito below.) Portman also carries a lot of weight in his caucus. Politico:
As a former member of the House leadership and one-time OMB director who was reelected by a big margin in November, Portman carries a lot of weight among his fellow Republicans. It’s not that Portman controls these fellow GOP votes. It’s that with someone like Portman opposed, it makes it much easier for wavering Republicans to vote no as well.
And Portman is getting pressure from the health insurers and the hospitals (different from the pressure from constituents in Kansas about rural hospitals). From the Cleveland Plain Dealer:
Two days after Sen. Rob Portman announced that he couldn’t support the bill advanced by Senate GOP Leader Mitch McConnell, the CEOs of the MetroHealth System, UC Health, Summa Health System, Premier Health and Sisters of Charity Health System sent Portman a joint letter to thank him for his opposition and urge him to “remain steadfast unless our patients – your constituents – and the providers they trust to take care of them are better protected.”
Let’s not forget that opioid treatment is a profit center! And then, besides insurance company profit, there’s the prospect of more “good jobs” drying up. In Jefferson County:
[Here are some] effects the Republican healthcare plan would have on Trinity Health Systems, the hospital network that is by far the county’s biggest employer.
Trinity Interim CEO Joe Tassi told me the bill would translate to a loss of $61 million over 10 years, in the form of Medicaid funding cuts, which likely would lead to a loss of jobs and reduction in services.
“It’s not a closure situation for us, but it’s clearly a reduction impact on jobs,” Tassi said.
Why I wrote this: Plenty has been made of President Donald Trump’s economic message, and his promises to restore industry in places like Jefferson County. But the reality is today many of these communities rely on the healthcare sector to prop up their economies.
So much for those working class volatility voters? All this said, Portman doesn’t seem much for profiles in courage. Local blog Plunderbund:
Here’s a tweet from the AP at 1:48 PM today breaking the news that the GOP can’t find enough votes to support their awful health care bill
And here’s the tweet from Rob Portman, two hours and twelve minutes later, where he finally takes a stance on the bill.
Finally, it does seem that Portman has a price. From the Dayton Daily News:
Kasich, in D.C. for a board meeting with Siemans, told reporters at the National Press Club that he does not support the Senate bill as written. He said he had urged Portman not to accept “a few billion” to fight the nation’s opioid epidemic in exchange for drastic cuts to Medicaid, saying that the former would be “like spitting in the ocean.”
That Kasich thinks Portman can be bought off with a smidgeon of money for his signature issue implies to me that McConnell must think Portman can be rolled. Since Portman is said to be good at issuing “inkblot test” statements “that can be read any number of ways,” we may not know which way he jumps for some time.
(3)(b) Dean Heller (NV)
Dean Heller is a unique case, because got a tight race in 2018, in a state whose Republican governor Brian Sandoval is strongly for Medicaid expansion. (Portman’s governor, Kasich, is also for his Medicaid expansion, but Portman isn’t running and if he were he’d have plenty of margin.) The Hill:
Heller has served in the seat since 2011, when he was appointed to fill the seat of then-Sen. John Ensign, a Republican who resigned amid an ethics probe. He won reelection in 2012 by a 1-point margin.
Heller’s assessment (backed by Sandoval) is that taking concrete material benefits away from his voters is bad. Again Politico:
The previously uncommitted Heller stunned many Republicans recently when he appeared next to Sandoval at a Las Vegas news conference and ripped the GOP’s draft repeal bill, even saying supporters’ claims that the bill would bring down premiums are a “lie.” Sandoval was the first Republican governor to opt in to Obamacare’s Medicaid expansion in the fast-growing state, a move that netted more than 200,000 new enrollees.
Observers believe their best chance to get his support is reworking the way the bill rolls back Obamacare’s Medicaid expansion and puts the entire program on a budget, changes that would reduce federal Medicaid spending by $772 billion over a decade, according to the CBO. Sandoval has been critical of certain parts of the Affordable Care Act and says the law needs fixing, but he has railed against the GOP’s plans for Medicaid because of what they would mean for his state budget and its uninsured rate.
(And it’s hard to see how Cruz’s “Consumer Choice” amendment would “rework” “the way the bill rolls back Obamacare’s Medicaid expansion.”
Now, it is true that Heller faced both an air war from donors and primary threats from talk show hosts. However:
For Heller, the considerations about Medicaid expansion and repeal promises might all take a back seat to a more pressing reality. He’s up for re-election next year — a Republican in a state that has gone blue for the last three presidential elections.
But it seems Heller has made up his mind to defy both forces and hang on for dear life. Washington Times:
Nevada Sen. Dean Heller has found plenty of reasons this year to break ranks with fellow Republicans — including President Trump.
On everything from President Trump’s budget to the Obamacare repeal to the ultimate parochial issue of the federal government’s plans for a nuclear waste repository at Yucca Mountain — the classic parochial issue for a Nevada politician — Mr. Heller has balked at his party leaders’ plans.
He’s also the most vulnerable GOP incumbent heading into 2018, and Democrats are already pouring money into the state, looking to force him into a corner on the hot-button issues like health care.
That’s a lot of bridges to have already burned. What’s one more?
(3)(c) Susan Collins (ME)
Susan Collins is a unique defector, being impregnable in the state that likes to leverage its small size with Senators who can vote with either party, or at least be seen to. I have always wondered why the administration didn’t dangle a nice fat “good jobs” contract for destroyers at Bath Iron Works before her, and my current theory is that she told the leadership to back off. Why? Because she’s running for governor, and, like governors Sandoval and Kasich, thinks Medicaid in its current form is good for the state (and better than TrumpUncare). She’s certainly sending a strong message here:
“Never before, in the 15 times that I’ve marched in this parade, have I had people so focused on a single issue,” Collins told The New York Times while marching in the July 4 parade in Eastport, on a small island close to Canada. “I heard, over and over again, encouragement for my stand against the current version of the Senate and House health-care bills,” she told The Washington Post. “People were thanking me, over and over again. ‘Thank you, Susan!’ ‘Stay strong, Susan!'” Murkowski, parading in Wrangell, Alaska, said that most of the people who spoke to her at the festivities did not indicate “for or against” the bill. “They just say, ‘Make sure you’re taking care of our interests,'” she said. “In fairness for those that do the ‘for or against,’ everybody is pretty much [saying] they don’t think this is good for us.”
Note that Maine is not a Medicaid expansion state, so Collins’ constituents are worried about existing Medicaid and the existing ObamaCare marketplace.
(3)(d) Shelley Moore Capito (WV)
And finally, there’s Senator Shelley Moore Capito, who seems unique in any number of ways. First, recall that West Virginia, as shown in section (2)(b), suffers by far the most withdrawal of a concrete material benefit under TrumpUncare. Then, she seems be doing the very reverse of issuing Portman-like ink blots. Politico:
But if Capito is feeling the heat in a state that Trump won by more than 42 percentage points, she isn’t showing it. Back here in West Virginia, where more than 30 percent of families rely on Medicaid, she doesn’t hesitate at the prospect of casting the vote that kills the GOP’s repeal effort.
“I only see it through the lens of a vulnerable population who needs help, who I care about very deeply,” the 63-year-old lawmaker said in an interview. “So that gives me strength. If I have to be that one person, I will be it.”
“If I have to be that one person.” Hoo boy. And unlike Portman, she’s not going to be bought with opioid money. The Washington Examiner:
Sen. Shelley Moore Capito suggested Thursday that the $45 billion in funding to fight opioid addiction added to the Republican healthcare bill would not be adequate on its own to win her support for the legislation.
“We’ve been pushing hard for the extra opioid money and it’s critical,” the West Virginia Republican told reporters. “Is it enough to push me into the yes? Not at this point.”
Hoo boy. Capito doesn’t support the Cruz Amendment, either. From the local Gazette and Mail:
Since then, Republican senators such as Ted Cruz, R-Texas, and Mike Lee, R-Utah, have called for an amendment, “The Consumer Freedom Option,” that would allow insurance providers to offer coverage that does not comply with key aspects of the Affordable Care Act, so long as they also offer plans that do. However, Capito said she’s not ready to vote for a plan that takes away from some of the ACA’s most popular provisions.
Now, let’s look at the “not far enough” defectors:
(3)(a) Ron Johnson (WI)
Ron Johnson is a unique case. For one thing, “before his first Senate campaign, Johnson was a businessman whose company packaged medical devices.” For another, he’s “promised not to run again.” Also:
He is not politically indebted to the Senate GOP leadership, which actually reduced its planned ad buys for Johnson’s race last year when they (and many others) thought he was headed for defeat…. Nor is he all that indebted to President Donald Trump. …. But Johnson got about 74,000 more votes than Trump statewide because he did markedly better in Wisconsin’s most populous areas, including the GOP’s base counties in the suburbs outside Milwaukee.
Here’s a summary of the state of play in Wisconsin from the local Journal-Sentinel:
Caller after caller on his telephone town hall last Wednesday complained about the GOP proposal, including its Medicaid rollbacks, a part of the bill that Johnson supports.
Johnson told her that by his definition — the pure dollar amount being spent from one year to the next — Medicaid wouldn’t be cut. It’s a debatable definition, since the slower spending growth in the GOP bill, combined with inflation and population change, would result in fewer people being covered than under the current law.
Johnson feels like an outlier, to me: A classic Republican business type, with a bone-deep commitment to cutting back big gummint, and, if he is the sort to hold a grudge, the incentive to stick it to the Republican leadership. Although he’s faced protests, it’s hard to see how McConnell can bring pressure on him.
(3)(b) Rand Paul (KY)
Paul is a unique case, as a libertarian; he frames both ObamaCare and TrumpUncare as a bailout of the insurance companies. This story from over the recess, made a big splash in Kentucky. From the local Courier-Journal:
Paul met with community leaders in Shelbyville on Monday to hear their stories and concerns with health care, making a push for his association health care plan, which would allow people to join large groups for cheaper health insurance.
“We need to let everyone get out of the individual market for health care,” Paul said.
In addition to local government and community leaders, the crowd at the Farm Bureau Insurance building included several small business owners.
Mary Courtney, a farmer in Shelbyville, said her rates are sometimes $1,400 a month for health insurance because the family farm can’t enter into a larger group for reductions.
More on Courtney from local station WHAS:
While the government does not require the Courtneys offer health insurance to their seasonal employees, they say they represent a large group of Americans who need health care reform, young farmers.
We budget around $50,000 a year (on health care) and the reason for that is because we have a very high monthly premium, then we have a high deductible and it seems like, with a family of six, if somebody doesn’t have a health issue it seems like somebody else does,” Mary said.
She described being grandfathered into an insurance plan when the Affordable Care Act took effect.
That plan allowed one of their children to have required care from a specialist out of state. But as time wore on, the insurance company took away that option leaving them in search of a new plan.
“We did some digging”, Mary explained. “As much as it went against my core, to go on the state funded programs. But then we couldn’t get coverage for him if we needed it, out of state.”
So, first ObamaCare sent Courtney to HappyVille. And then ObamaCare sent her to Pain City. No wonder she’s upset. The Chamber of Commerce agrees. Local station WDRB:
Agreement seems to be in short supply these days when it comes to health care, but there’s one thing that kept cropping up at Sen. Rand Paul’s roundtable discussion at the Shelby County Farm Bureau on Monday.
“The rising cost for larger employers who are in a position to offer health care and for small businesses … it’s just out of reach for them,” said John Wheeland with the Shelby County Chamber of Commerce.
And Paul has a price. The Courier Journal once more:
U.S. Sen. Rand Paul said Thursday that he’d be “closer” to supporting the GOP’s health care bill if more language loosening association health plans found its way into the measure.
Association health plans allow certain organizations, like professional or trade groups, to offer insurance. In theory, then, small businesses, individuals or groups could band together and buy coverage, gaining bargaining leverage with more people.
“What’s great about this situation is that it doesn’t require a mandate. It requires liberalization of the law,” Paul said at an afternoon press conference in Louisville. “It doesn’t cost anything — we’re legalizing competition.”
(I’ve got to say that I immediately translated “associations” into the sort of heavily regulated private systems that countries like the Netherlands and Switzerland have; and that Paul and the Democrats should talk. Of course, Paul won’t accept heavy regulations, so talking to Democrats isn’t on. However, Pauls’ fellow Kentuckian Mitch McConnnell isn’t talking to Paul either; he is, however, talking to Ted Cruz.)
(3)(c) Ted Cruz (TX)
Ted Cruz is a unique case, as a once and future Republican Presidential candidate. To that end, he’s morphing from an ideologically-driven crusader into a compromiser who can “get things done.” The Texas Tribune:
Cruz paints a picture that he is now functioning as a cohesive force among Republicans. For Cruz to be speaking this way is no small matter. Over his first four years as a senator, he singled himself out as an immovable bulwark against moderates in his own party. That helped sour relationships with many of his fellow Republicans.
A little over a year ago, as Cruz and Donald Trump were the leading candidates in the hunt for the GOP presidential nominations, Republican leaders opted to not put up a fight against the unpredictable real estate mogul rather than back Cruz’s bid.
At the time, some operatives suggested Cruz should return to the Senate and focus on repairing relationships in the same way that U.S. Sen. John McCain did after he lost the GOP nod to President George W. Bush in 2000. And at least on health care, Cruz appears to be doing just that.
U.S. Sen. Lamar Alexander, a senior Republican from Tennessee, turned out to be the emissary and pulled Cruz into working on a repeal bill. Cruz is in deep enough in the negotiations that he has repeatedly hosted fellow Republicans in his own conference room to build the foundation for a deal.
The BCRA is now being rescored by the CBO, with and without the Cruz’s “Consumer Choice” amendment, which the New York Post summarizes:
The Cruz amendment would let any insurer who offers ObamaCare-compliant policies also sell insurance that doesn’t meet the one-size-fits-all mandates. That would let healthy, younger people buy affordable coverage — without subsidies, but also without forcing them to subsidize insurance for older folks.
Federal taxpayers as a whole would be directly helping the folks that most Americans believe should get assistance, while everyone else would be free to choose a policy that works for them, rather than one that satisfies a wish-list drawn up by Democrats in Congress nearly a decade ago.
The wee problem? From the San Antonio Express-News:
It’s that the entire individual market would fall apart under Cruz’s plan because of adverse selection — the idea that people with higher health costs will self-select into more generous coverage.
So, either McConnell believes throwing people with pre-existing conditions under the bus will fly, or he’s giving Cruz rope to hang himself:
McConnell is expected to place greater responsibility on Sen. Ted Cruz, R-Texas, to pitch his controversial amendment that would allow insurers to offer plans that don’t meet ACA requirements – provided they also offer some that do. McConnell could ask Cruz to speak to Republican senators as soon as Tuesday, according to a person familiar with his strategy. Cruz has often talked about his amendment in the senators’ regular Tuesday lunches, but the burden of building support for the bill could be left to the firebrand conservative.
(3)(d) Mike Lee (UT)
Finally, Mike Lee — who backs Cruz’s “Consumer Choice” amendment — is a unique case, simply because Utah is a unique state. By way of example, from the Salt Lake City Tribune:
When the Rev. Scott Dalgarno looks out at members of his Wasatch Presbyterian Church congregation on Sundays, his mind goes to what will happen to them if the Senate Republican health care bill passes.
Some are insured through the Affordable Care Act. Others are on Medicaid. Losing access to those services would wreak havoc on their lives.
These people “are worried about bankruptcy,” the Salt Lake City faith leader said Wednesday as he joined a group of about 30 Utahns who met with Sen. Mike Lee’s staffers at the Wallace F. Bennett Federal Building in Salt Lake City to voice concerns about the measure.
Sure, but why am I thinking the view of a Presbyterian “faith leader” — or protesters — might not carry great weight in Utah, given (for example) the Mormon supermajority in the legislature? (I’m not saying that Mormon religious views are the driver here — Harry Reid, pro-ACA and anti-single payer, is a Mormon, after all — but that the political terrain in Utah is unique (see here).
Conclusion
As readers know, I’m very reluctant to make any kind of call on TrumpUncare, because Republicans have been so very feral and focused on getting things done; the House bill, after all, ultimately passed. (And who knows? Maybe the same dynamic will play out here; in the game of “pass the parcel” for health care responsibility, perhaps the Senate would prefer that Trump be the one holding it when the game ends.)
With the caveat out of the way, passage of TrumpUncare as BCRA, as BCRA + “Consumer Choice”, or as a revised AHCA seems highly unlikely to me, as does the simple repeal of ObamaCare with no replacement. (Even if the repeal didn’t take effect until 2019, or even 2021, that would be a terrible look that proves Republicans are unfit to govern.)
First, a common but by no means universal explanation is that taking away concrete material benefits from people who already have them is politically hard. This is true in Maine, Nevada, and Ohio, although as background noise it’s present everywhere.
Second, it’s not clear what McConnell has to bargain with, even if he does have $200 billion in savings to throw away in the BCRA. My thought was always been to bribe the opiod epidemic states after backing out the tax cuts for the rich, but apparently $45 billion isn’t enough for Capito, and that’s a non-starter in Maine, was well. I can’t see the “Consumer Choice” amendment as doing anything other than burnish Cruz’s halo for 2020, if it even does that; every Senator will have gotten an earful about pre-existing conditions, and the magic of the marketplace will throw them under the bus.
Third, if you do the math and take each unique case into account, I read Heller as a solid “no,” since he’s bucking the leadership on everything else and he’s backed by his governor, I read Collins as a solid “no,” since not only does she — Lambert gets sentimental here — care about the constituents of her small, rural state, she wants to run for Governor, and I read Capito as a solid “no,” since $45 billion won’t buy her off; she wants more, but there’s no more to be had. McConnell can afford to lose two; that’s three. I’m pleasantly surprised by Moran, and he’s a bit like Collins, in that he too, seems to care about his rural constituents, and his state seems split, at the state level, between “too far,” and “not far enough” on issues like taxes. I rate Moran as a possible “no.” That’s four. I rate Portman as weak, so still four (depending on what pressure Kasich can bring to bear). And that’s before we get to Cruz, Lee, Johnson, and Paul. I might throw Paul in, since McConnell will not meet his price, bringing the number of defectors to five.
And now, we shall see! I hope I’m right. Which Republican will want to be the third?
Readers?
NOTE
Perhaps McConnell will end up working with Schumer on some minor fixes, and he and Schumer both will sell the deal as exorcising the dread spectre of single payer? Stay tuned!
APPENDIX
UPDATE Numbers to call:
“Too Far’
Jerry Moran (KS). DC: (202) 224-6521. Hays: (785) 628-6401. Manhattan: (785) 539-8973. Pittsburg: (620) 232-2286. Wichita: (316) 631-1410. Olathe: (913) 393-0711.
Susan Collins (ME). DC: (202)224-2523. Bangor: (207) 945-0417. Biddeford: (207) 283-1101. Caribou: (207) 493-7873. Lewiston: (207) 784-6969. Portland: (207) 780-3575.
Shelley Moore Capito (WV). DC: 202-224-6472. Charleston: 304-347-5372.
Rob Portman (OH). DC: 202-224-3353. Cincinatti: 513-684-3265. Cleveland: 216-522-7095. Columbus: 1-800-205-6446 (OHIO). Toledo: 419-259-3895.
Dean Heller (NV). DC: 202-224-6244. Las Vegas: 702-388-6501. Reno: 775-686-5770.
“Not Far Enough”
Ted Cruz (TX). DC: (202) 224-5922. Austin: 512) 916-5834. Dallas: (214) 599-8749. Houston: (214) 599-8749. San Antonio: (210) 340-2885. Tyler: (903) 593-5130. McAllen: (903) 593-5130.
Mike Lee (UT). DC: 202-224-5444. Salt Lake City: 801-524-5933. St. George: 435-628-5514. Ogden: 801-392-9633.
Rand Paul (KY). DC: 202-224-4343. Bowling Green: 270-782-8303.
Ron Johnson (WI). DC: (202) 224-5323. Milwaukee: (414) 276-7282, Oshkosh: (920) 230-7250.


Nicely done.
+100 Very helpful, Lambert.
Moreover, Trump doesn’t seem all that focused on this particular issue. Maybe they can pivot to war on the Korean peninsula to distract from all this mess.
My prediction: South Korean and North Korean leaders will soon announce that they will embark on formal reunification. It will be one of those out-of-the-blue surprises like Nixon’s summer 1971 announcement that he would be going to China in February 1972.
What will happen next? Well, the United States will be told that all of those bases will no longer be needed in the former South Korea, and, Yankees, it’s time to go home. Think Iraq not signing that status of forces agreement a few years ago, and you have the idea.
Reunification? In a word, it will be expensive. Just like the reunification of East and West Germany. Watch for the hissy fits on how much the whole thing will costs. Sort of like the Ossie vs. Wessie rivalry in Germany. That one’s still going on.
It would be nice to see your prediction come true soon.
I don’t think this is very likely in the near future. One of the huge differences between East Germany and North Korea is that the leaders of East Germany were sane. Sure, they had the oppressive Stasi, but the strangeness of the North Korean government is an order of magnitude beyond anything in the old East German government.
The strangeness of the government of North Korea is a tiny footnote to the strangeness of the government of the US.
McConnell has taken point on this, not Trump.
That said, I find it amusing to hear conservatives yammering about keeping their promises, when apparently Trumps’ campaign promises don’t matter a hoot (though in all fairness, perhaps
“Hope and Change”MAGA didn’t mean all that much to Trump himself).I find it odd that Trump has been fairly quiet on the policy front while busy starting Twitter flame wars. Initially I thought he was intentionally creating distraction but ultimately came to the conclusion that he’s just watching ratings and playing for attention. Governing is hard, starting a Twitter war is easy and far more emotionally rewarding.
I’m surprised you didn’t talk about Corker (TN), Cassidy (LA) and a number of others who have sounded pretty critical of McConnell’s bill. Corker talks a lot about needing to be assured that the bill will bring down premiums and deductibles (it won’t). Cassidy keeps talking about the bill needing to pass the “Jimmy Kimmel” test, i.e. newborns needing expensive care will get it (it won’t).
Well, I’ve got to stop somewhere! Frankly, that seemed like the most authoritative list to me, when I started.
As it turns out, FiveThirtyEight (in parallel) has the same list (except they add Murkowski. I wrongly thought she’d been sold, but apparently not).
Im pretty certain Murkowski is in deep with state level Republicans. Her father was Governor just 10 years ago. She’s still a Republican, but Im not under the impression she is a Paul Ryan level dullard (I could be mistaken; usually, the dullards jump out). Like Maine, I think the scale and economics of Alaska mean that if she wants to keep her seat she can’t directly harm her voters. Without the status of current Senator, Murkowski is a nothing which is what politicians hate the most. She has to listen to the state concerns in a way a larger state’s senator would find enough brown nosers to protect them.
Of course, I don’t think the Republicans expected to be in the position where they can repeal ACA.
Murkowski has absolutely nothing to worry about from her right flank. In 2010 she lost the GOP primary to a tea party nut job but won the general election as a write in….. Winning a write in with that last name means she has that seat for life and no one has leverage on her. She’ll vote how she wants.
https://en.wikipedia.org/wiki/United_States_Senate_election_in_Alaska,_2010
Cruz’ amendment is quite amazing. Let’s put all the healthy people in one cheap pool, and all the sick ones in a very expensive one. It defeats the entire idea of insurance.
Of course, the ideal pool size would be to include the entire population…..Medicare for All—MFA!!!
Cruz is a tool, but I’m pretty confident his ammendment is meant to appease his donors. Let that sink in, Ted Cruz donors. Much was made about Mitten’s famed 47% comment, but the real story was the questions Mittens faced from the GOP donors. Those people are barely connected to reality.
And help him run for Preznit [recoils in horror]!
I doubt his donors care about anything other than their tax cuts. I’d be more inclined to guess that the Cruz fan base (the entire idea makes me twitch) doesn’t like paying for sick people. I’ve seen that commentary over and over again, men shouldn’t have to pay for pregnancy coverage, why should we have to pay for your cancer, etc…
I think he’s trying to appease the hardliners who are thinking that their premiums will go down if they can stop having to cover all those damn sick people. When you see the words “lower premiums” that’s code for Let Those Sick People Die, Not My F(amilyblog)ing Problem.
Yes, and the solution for that is loss of what causes pregnancy. The Spartan women’s solution – a strike?
Is that a cutting remark?
What a quaint analysis, assuming that senators sincerely represent the interests of states, or groups of affected constituents, rather than industries!
I’d love to see the map showing the “health care” industry’s share of each senator’s political contributions. And, if possible, quantification of other personal ties (family, staffers…) to corporations that will be impacted by “health care” legislation. I bet that would be informative as to who “supports” or “opposes”…
But the real tragedy is that the only real debate going on is about which groups should be eligible for federal handouts (“subsidies” etc.), not the farcical economic structure of the system as a whole. It doesn’t matter whether Uncle Sam pays a few extra $billions/year for certain people to get “health care”, when the entire system costs $trillions a year more than any reasonable alternative, all for no net benefit. That’s a lot of human labor wasted, producing nothing of value.
The cost structure, driven by terrible incentives and insurance-middleman bloat, IS the problem. Given the national costs of this awful system, for those responsible to debate anything else is dereliction of duty at a level approaching treason.
Trump and the Senate should be thinking about how they could Make America Great Again by removing the trillion-dollar albatross of wasted labor that is holding down the U.S. economy.
I would make the same argument against monocausality in such a case. Perhaps I should have added another map, but I didn’t have current data. Open Secrets, with the same list as mine plus Sasse, Cassidy, and Murkowski:
I’d be the last to deny the existence of oligarchy or the corrosive effect of money in politics. However, I don’t think even Open Secrets can give a granular enough account of the votes in this case. We shall see!
Thanks for going the extra mile with the OpenSecrets data. 2012-2016 might not be the most informative time period, with the R half of the property party nominally in opposition to O-care. Could be worth rechecking it in a year or two, since sometimes the quid arrive after the pro quo! Also, there’s more than one way to deliver the quid. Where direct donations would be politically toxic, often the donor-oligarchs find other ways to line the senators’ pockets (or their friends’ pockets)…
Major organizations representing health care providers (hospitals, professionals) and insurance (AARP, Medicare managed care) don’t support the Republican bill.
https://www.forbes.com/sites/brucejapsen/2017/06/13/nationwide-blitz-launched-to-derail-trumpcare-in-senate/#607b24012bae
https://www.washingtonpost.com/politics/2017/live-updates/trump-white-house/gop-health-care-bill-the-latest-news-and-reactions/insurers-to-senate-proposal-could-harm-74m-on-medicaid/
The opioid addition treatment coverage is really a bailout for the insurance and ‘health care’ complex as pointed out in the article. Doctors and Pharma should be paying for the treatment because they caused the problem. Instead NIH and other government grants are funding research for a so called solution that the Pharmas will benefit from.
Nothing in the people’s interest; all for big business. Just like WR Grace company who socialized their liabilities in Libby, Montana, these big corporations like the corporate handouts.
Looking back to 2009, and the stunning realization that single payer was off the table, it’s interesting to find ourselves
a) still alive
and
b) with an American public that does not now want to retreat from what we’ve got.
It is an excruciatingly slow process, this “kindness” thing. Makes you want to find a record player and listen to Ronald Reagan warning us about the terrible thing called Medicare:
https://m.youtube.com/watch?v=Bejdhs3jGyw
Thanks, some great comments there.
I generally agree although I’m certain that “single payer” would mean that the oligarchs would control not only the pricing but also the checkbook used to pay their prices. That’s not a solution when the real issue is the absence of price transparency and meaningful competition due to the economically dysfunctional structuring of the supply side of medical care.
Next, we know from examples in other nations that we could have a better-performing system at $trillions/year less cost. Those $trillions are “employing” 10-20 million people (or more) who, in the current system, essentially produce NOTHING that we could not have without them, in a better-performing system with many fewer workers and much lower costs.
It’s no “kindness” to have 10-20 million Americans “employed” in the “health care” system who are demonstrably producing nothing of value, while others are still left without affordable care, all because the system has too many monopolies and too many middlemen. Create a better system and those millions of Americans could be taking care of everyone currently left out (for no extra cost!), Making America Great Again, or simply doing something useful and productive in life, liberty and the pursuit of happiness…
If you want to advance kindness, cut the crap out of the pricing of hospital care (same price for all), allow people to freely trade medical goods (so prices equilibrate globally), and figure out how to get the insurance middlemen out of the business (maybe a la Kaiser)?
Why are we assuming that accurate pricing for health care is possible, and why are we assuming that any market we can imagine setting up will achieve that? Please give a real life working example in health care of the policy you advocate, or else you’re just another ideologue experimenting on the health of the American people without their informed consent.
Accurate pricing may be possible if you bill for time spent, hours, not procedures.
The excess costs in the current system are mostly billing driven , which is based on bill-for-procedure.
If one does than one also has to address the cost of becoming a doctor in the US, which then requires an attack on university education costs…
Such a change would appear to pull the keystone out of the arch of the US’ rent extraction system….
I used to bill by the hour as a consultant, and, well…
Online price-comparison tool for drugs (health care goods):
https://www.discountdrugnetwork.com/drug-pricing/
Pricing at Surgery Center of Oklahoma:
https://surgerycenterok.com/pricing/
Also you should take a look at the burgeoning industry of medical tourism, with the relatively new trend of U.S. patients heading to other developed countries to get identical procedures at much lower costs, even after subtracting airfare etc.
For instance, here’s Wikipedia on growth in medical tourism to Israel:
https://en.wikipedia.org/wiki/Medical_tourism_in_Israel
“A patient with no health insurance who needs bypass surgery in the United States would spend approximately $120,000, while the same procedure performed in Israel would cost approximately $30,000. In vitro fertilization (IVF) is known for its high success rates and considerably lower costs. IVF costs $3,000-$3,500 in Israel, compared to $16,000-$20,000 in the United States.”
This is not ideological. Imagine if gas stations worked on the same business model as health care. You need gas? You’d have to go to just a couple of stations – no choice. If you needed gas right away (emergency) and couldn’t afford to wait, it’d cost twice as much “just because”. Oh, and the gas here in the U.S. would cost 2x-10x the same price as gasoline in Canada or Europe (not because of taxes), but you would not be allowed to import your own gas from overseas!
Why would anyone put up with that?
Who has the frigging time, knowledge, or connections to really do this? Especially if one is undergoing a medical emergency?
Count me skeptical
Here is Wisdom Seeker’s dream system at work:
(Originally from Dembot Site Lawyers, Guns, and Money, but still funny!)
http://digbysblog.blogspot.com/2017/07/how-to-survive-trumpcare.html
Step 1 – call Uber, not 911. Pay the peak pricing gladly – it still beats a fully loaded EMT response . Plus, if they don’t show up you get a $5 credit, should you survive
Step 2 – remember to not go comatose. Such lack of discipline at this critical pricing decision point could adversely impact your ability to make a rational decision on the services you may be willing to pay for and which supplier in your particular market you may want to utilize. You can ignore this if you live in a rural market and the nearest regional hospital with an ICU is 25 miles away.
Step 3 – direct the Uber driver to the nearest accredited hospital while you use your iPhone to solicit quotes from alternative medical retail establishments (hospitals, clinics, etc) don’t forget to read the reviews. At these times it’s also especially helpful to bring up your pre-defined Excel template that you cribbed from Consumer Reports to plug in the quotes as you are making your way to the first medical retail establishment in your itinerary for this medical emergency. Be glad you aren’t a rape victim so you can be sure that whatever fully informed facility and treatment path you decide on, the hospital won’t refuse to treat you according to your wishes. OTOH, the medical retail establishment might not treat you unless you can produce a current liquid net worth and credit score that meets their patient treatment scoring index. Subprime can lead to restricted options.
Amusing straw man, but not at all what I have been advocating. Suggest you stick it in your back yard.
FYI, Emergency medical services are a tiny fraction of health care spending (see elsewhere in thread).
P.S. If the relevant price/quality information was readily available, you’d know as a matter of daily life which hospitals in the area you liked, and so would your family. In fact, that’s how medical care used to work, back before HMOs and the like. Knowing where to go for emergency medical care is, or at least used to be, a basic part of family emergency preparedness, like having a plan for dealing with a fire, or an earthquake, or a tornado or hurricane.
” you’d know as a matter of daily life”
Osmosis.
“If the relevant price/quality information was readily available,”
So, then it follows then that it is NOT available. Why not? To whose advantage?
“Emergency medical services are a tiny fraction of health care spending”
The care that follows emergency medical care is the biggest portion of medical care spending, see above thread. Both of these, together, are what lead to Bankruptcy. See above thread.
all these government hand outs that are lauded as being good are in fact bad because they come about through robbery, a robbery the thieves call “taxation”
theft is amoral and perhaps the most devastating act against society, when a society votes for theft as public policy that society is doomed as surely as a man who eats only chocolate is doomed
healthcare can only work if it’s treated the same way the distribution of chocolate candy bars and lawn mowers is, by the thriving ingenuity of a market fueled by honest men and women engaged in gainful trade
reply below
> healthcare can only work if it’s treated the same way the distribution of chocolate candy bars
Why the [family blog] would you think buying candy bars is the same as buying health care? I think you must have gotten lost. You’re certainly in the wrong place.
Are you a second-hander Rander?
http://ideas.time.com/2013/11/01/why-so-little-candy-variety-blame-the-chocolate-oligopoly/
2017 bill to restrict medical insurance from being partly sheltered from antitrust law. Passed house, awaiting Senate action:
https://www.congress.gov/congressional-report/115th-congress/house-report/36/1?q=%7B%22search%22%3A%5B%22Gosar%22%5D%7D
Sounds like we need to break up the chocolatiers too…
Interesting, thanks. Vote was practically unanimous.
http://clerk.house.gov/evs/2017/roll184.xml
Here’s a bill that’s still in the House and would go a long ways to improve the “health care” system, by mandating open, public, transparent pricing, an essential component of a free, competitive market. This bill alone wouldn’t fix excess costs driven by miscoding, or rein in monopolistic price gouging, but at least it would shed some sunshine on the issue and raise awareness of how badly prices here are skewed vs. rest of world:
https://www.congress.gov/bill/115th-congress/house-bill/2569
“This bill requires entities that offer or furnish health care related products or services to the public, including health insurers and government agencies, to disclose the price for those products and services at the point of purchase and on the Internet. The entities must disclose all prices, including wholesale, retail, and discounted prices, that are accepted as payment in full for products and services furnished to individual consumers.”
I thank the Colorado Democrat who introduced this bill!
Where are the Senators who support “free markets” for health care? They need to sign up as co-sponsors!
Quick, give me the price list for the hospitals around here, I am having a heart attack!
It would be a Colorado Democrat. Probably pro-fracking and anti-Single payer, too.
Dale, your response is typical of those who totally miss (or want to deliberately deflect) the point. Most medical care is pre-planned, or at least offers enough time for a price-conscious decision. Even for emergency care, transparent pricing would allow honest journalists to engage in some well-justified cost-shaming of hospitals into some semblance of pricing sanity.
> Most medical care is pre-planned, or at least offers enough time for a price-conscious decision.
Evidence, please.
> Even for emergency care, transparent pricing would allow honest journalists to engage in some well-justified cost-shaming of hospitals into some semblance of pricing sanity.
Those stories have already been written. Hasn’t done much! Your faith-based approach to health care markets is touching. Even, well, “quaint.”
> Evidence, please
“Most surgeries necessary for medical reasons are elective, that is, scheduled at a time to suit the surgeon, hospital, and patient.”
https://en.wikipedia.org/wiki/Elective_surgery
Admittedly not a definitive source, so I looked further…
Various estimates cited in the link below place emergency medicine at 2-10% of all healthcare spending, as of 2010 or so:
http://www.politifact.com/truth-o-meter/statements/2013/oct/28/nick-gillespie/does-emergency-care-account-just-2-percent-all-hea/
From the structure of the health system, the main factors preventing price-conscious decisions appear to be insurance-driven limitations on patients’ choice of caregivers, and the obfuscation of pricing.
> Those stories have already been written.
“Evidence, please.” Heck, even for non-emergency procedures there’s no journalism. There are plenty of “hospitals charge outrageous prices” articles, but I’ve seen very few with data such as “Hospital X costs twice as much as Hospital Y for procedure Z”. Even for relatively simple elective procedures (insurance not needed), there’s very little price-comparison literature. Have you tried pricing out botox injections? About the only thing you can price are OTC medications.
The Free Market is a Wonderful God, isn’t it? Praise be It’s Holy Name.
Yes, why would we need what Europeans take for granted – simple and prominently posted price list for hospital services
I have no problem with transparency. Markets don’t function on transparency, AT ALL. In a market, everyone is trying to stick a shiv in the other guy, and deception, deceit, and deliberate misinformation (also known as lying) is the grease that spins the wheels.
What you want is a big police state that forces people to act in a transparent way, on pain of losing their ability to operate, and not in a more deceptive, more market friendly way where they get to do whatever they want as long they stick the shiv in far enough.
That you don’t already know this is just astonishing to me. Do you never leave the house?
> Do you never leave the house?
Only to buy candy!
What’s that phrase? “Like taking candy from a baby”?
But, seriously, I am totally in favor of a transparency bill. I’m also in favor of proactive price setting. I am not interested in romanticizing “the market.” The market is for residual crap that doesn’t matter.
It’s like do we waste our time applying for jobs that don’t state a pretty clear salary? People who rant on about the market hate the market as much as any other self protective person. Denial runs deep.
The next question is will Schumer be able to hold his caucus in opposition?
of course not. he won’t want to. mcconnell has now pushed back the time frame for passage to august. this gives him time to woo the usual manchin etc. group of dummycrats to ball everything up in some alphabet soup of details that muddies the idea of who will be responsible for the botched bill that finally passes to everyone’s disgust. anything but contrast obama/trump care to medicare for all. the dems would rather take the poison pill than abandon their donors. oh, yes, cory booker will be allowed to vote against the bill while making a lot of noise about it.
There is no Dem who is a threat to switch.
Manchin is neither the key to a GOP Senate majority as they already have one, and the GOP could probably beat him outright anyway given the state of Team Blue in WV. He’s the only one who really jumps out. A guy like Warner squeaked by Ed Gillespie. The GOP knows he can be beaten, and again, they don’t need him to run the Senate.
If Collins isn’t on board, Angus King is out. He has nothing to offer the GOP. Heitkampf can be problematic even by Senator standards, but this is too big an issue and too dear to voters to play around.
Schumer would love to frame holding the caucus together as an achievement of his “leadership”, but there is no reason for the Dems to not hold together.
Does he want to? I think Schumer would l-o-o-o-o-v-e to do a few minor repairs to ObamaCare, simultaneously sticking the shiv into McConnell and kicking the left.
Tom Tomorrow (cartoon courtesy here of The Nation) weighs in on the invisible hand of the free market as realized in both ObamaCare and the hopefully-D.O.A. Republican Plan:
https://www.thenation.com/article/wait-you-want-health-insurance-companies-to-cover-sick-people/
““The rising cost for larger employers who are in a position to offer health care and for small businesses … it’s just out of reach for them,” said John Wheeland with the Shelby County Chamber of Commerce.”
Which is why Rand Paul’s bid (for loosely regulated, no less) association plans doesn’t cut it. But at least he’s sane enough to know that the individual market has to go, (at least for most of us).
Creeping collectivism. I like it.
“I’m very reluctant to make any kind of call on TrumpUncare, because Republicans have been so very feral and focused on getting things done; the House bill, after all, ultimately passed.”
That’s true, but they also dumped it on the Senate to figure out. As for getting things done, it’s been six months.
Yep. So maybe McConnell will dump it on Trump to sign it, or not.
Single payer and 32 hour work weeks.
This is outstanding, really. +anything-one-cares-to-imagine
A few obiter dicta:
(1) Rural healthcare everywhere is decimated by BCRA. Richard Durbin spent one day of the July 4 recess (July 8) with downstate/rural healthcare reps and constituents. From his FB statement after the meeting: “Like the widely unpopular House bill, the Senate measure would cripple Illinois’ rural hospitals, families, and economy.” And it’s the same story everywhere – so yes, background noise, but a whole lot of it.
(2) The breakdown of reasons for possible defections was terrific. Another way to look at it, taking the longer view, which allows for (some) exceptions: this is in a sense a struggle among three parties, one solidly opposed (Dems), one very doubtful (trad Rs), and one raring to go for full “freedom” (from anything remotely social safety-net-related). The Rs haven’t (yet) been completely captured by the freedom fighters, thus the internal divisiveness (went too far/didn’t go far enough).
(3) I think Cruz has been outmaneuvered by McConnell here, in terms of pure political skill. If BCRA passes, McConnell wins (Hey! I got Cruz to bring us all together!) If it fails, McConnell wins (Hey! Don’t look at me, it’s his fault!). Cruz, not so much.
[OT: McConnell is really good, but he’s not quite as good as the Illinois house speaker, Mike Madigan, who will soon engage in a head-to-head confrontation with the Illinois Policy Institute for the soul of the state. Stay tuned: it’s going to be straight out of the Greek tragedians’ playbook.]
(4) In any half-rational political environment, a person who read through this analysis-discussion would conclude that it’s a compelling argument for single payer, period, full stop.
But of course we’re not living in a half-rational political environment these days.
RE (1). Moran has been getting an ear-full on rural hospitals. In Kansas, managers of these hospitals have been very vocal about just hanging on thanks to Obama Care, but under Trump care, would certainly go under. There was a report that in rural Kansas, if you have an emergency, it might take you 25 minutes to get to a hospital & then that hospital just might not have a doctor on duty.
On medical pricing, doesn’t Maryland cap what hospitals can charge for various procedures? Might be something to look at.
Think like an international investor ……
Investor maths:
The cost of living = housing costs + healthcare costs + student loan costs + food + other costs of living
Purchasing power = wages – (taxes + the cost of living)
The minimum wage must cover the cost of living.
Maximising profits requires low wages.
The cost of living is so high in the West, I need to invest in Asia.
The Western fools have had had real estate booms to inflate housing costs, the minimum wage and reduce profits.
The US has had it.
Look at their housing, healthcare and education costs.
Are they having a laugh?
What a dump, how does anyone make a profit there?
Even US investors prefer China and Asia, it’s so bad.
Anywhere else will do, the US is a complete waste of time for investment capital.
The US, unsurprisingly the world’s largest trade deficit nation.
A single light is left shining in the West, Germany.
With a high cost of living, they have a high wage economy where lots of value is added through high end manufacturing.
The importance of the cost of living was known to the Classical Economists of the 18th and 19th Centuries.
It was lost by the neoclassical economists of the late 19th and early 20th Centuries.
An unexploded bomb waiting to detonate under the West (apart from Germany) in the globalisation of the 21st Century.
You are obviously unaware of the basic accounting identity in which “U.S. trade deficit” implies “foreign investment in the U.S.”, and that as a result the U.S. is actually the largest destination for foreign capital?
That sort of impairs your thesis that foreign investors hate investing in the U.S. Or that U.S. investors are sending all our investments overseas.
On the other hand, we could be an even better destination for foreign capital if we cut healthcare costs and got more people working in ways that actually benefit the nation.
See e.g. https://fraser.stlouisfed.org/files/docs/publications/ERP/pages/8853_2000-2004.pdf
The money goes in to invest in financial products I assume.
Wall Street gains and Main Street gets nothing.
Trump seems to have made the same mistake as I have about the trade deficit, you had better let him know too.
Having a quick look on the internet.
It does look as though a lot of foreign investment capital comes into US manufacturing companies.
Do they in turn get that manufacturing done abroad for higher profits?
Refined with your comment taken into account.
Hollowing out the West and building the Asian Century.
The cost of living = housing costs + healthcare costs + student loan costs + food + other costs of living
Purchasing power = wages – (taxes + the cost of living)
The minimum wage must cover the cost of living.
Maximising profits requires low wages.
The cost of living is very high in the West, which makes it a home for high end business where a lot of value is added and high wages can be paid.
Everything else is more profitably done abroad apart from low end services sector jobs that must be done locally.
The cost of living effect is greatest in the US (where its very high) and the US is seeing its middle class disappear the fastest.
Like it!
High cost could be because of embedded inefficiency, or because of strong demand and limited supply. Paradise would be unaffordable to most. But the U.S. ain’t paradise, and a lot of the “high cost” is because we have some really stupid-inefficient economic arrangements.
On the plus side, major Asian nations have their own inefficiencies and the cost gap is closing. So the U.S. may not get too much more hollow.
Real estate booms are presided over by the economically incompetent in the West.
China is getting expensive but there are quite a few other Asian nations to choose from.
Excellent analysis, nothing to add. But I have the same question I have always had on this issue. Why doesn’t business support single payer? It would relieve them of the responsibility to facilitate (and partially pay for) health care for their employees. Surely General Motors recognizes that their products would be more competitive with Toyota if they did not have to bundle employee health care into the price of a car.
Congrats, Lambert. Well explained…
After Rand and Susan comes…
#3 and 4…Moran and Lee. One “too far”,one “not far enough”.
http://www.nbcnews.com/politics/congress/two-more-health-care-defections-dooms-current-gop-bill-n783926
It really is about the local pressures!