Yves here. One consideration that slightly ameliorates the downside scenario in this post is that China really has no other way of contending with a serious contagion like the coronavirus, whether it rises to a pandemic level or not, than quarantine and other methods to enforce greatly increased social distance. China has a woefully tiny modern health system relative to advanced economies, and still relies heavily on traditional medicine.
From an article sent by Troy P in Baldings World:
Delivery of high quality effective medical care and public health solutions in China suffers from a variety of problems. One of the most challenging is low levels of human capital in health care systems. According to one study, China has only 60,000 general practitioners or one per roughly 23,000 people. By comparison, in the United States there are 1,500 people per general practitioner. If all things were equal, this would mean Beijing one of the largest cities in the world would have fewer than 1,000 general practitioners. Nor are many medical professionals well trained. In community health centers, less than one fourth of doctors have a bachelor’s degree. Even as recently as a decade ago, only 67% of Chinese doctors had only been educated up to the junior college level, hardly enough under any reasonable standard to be a highly qualified medical professional.
The human capital deficiencies are compounded by government priorities. Buoyed by nationalistic support from Chairman Xi Jinping to traditional Chinese medicine, it occupies the second largest market share of the retail drug market behind chemical pharmaceuticals 29% to 43%. Leaving aside the weak evidence of traditional Chinese medicine efficacy in clinical trials, it diverts enormous resources from mainline medical service delivery and research at the altar of nationalistic sentiment. Addressing major public health challenges are better targets for public spending than boosting nationalist fervor.
Then oddly enough, health centers might be the only construction market in China to have missed out in the past decade. In 2009, China had 917,000 health institutions but by 2018 this number had only increased to 997,000 increasing roughly 1% a year. What has been happening however is a concentration of larger hospitals who are responsible for majority of growth in visits, bed space, and new institutions. This has led to wildly divergent health services. Primary level hospitals, the smallest hospitals in smaller towns, have bed occupancy rates of 57% while third level hospitals, which are the biggest and most advanced in bigger cities, register 98% in 2018 and 102% in 2014. In other words, in cities like Wuhan, hospitals the primary center of care for corona were already stretched beyond the breaking point.
These facts confirm our reaction when China rushed to construct a new hospital in Wuhan: so what? If you can’t staff it, what are you accomplishing? We had assumed it would be difficult to impossible to get qualified personnel (doctors with expertise in pulmonary ailments) to come to Wuhan even before we learned of the scarcity of medical personnel in general in China. Is the new hospital for show or merely to isolate people known to be sick? My understanding is that another constraint in any medical system, and it is bound to be much worse in China, is that the best hope of saving a severely ill coronavirus victim is to put them on a respirator…equipment not in great supply even in Western hospitals.
By David Llewellyn-Smith, Chief Strategist at the MB Fund and MB Super. David is the founding publisher and editor of MacroBusiness and was the founding publisher and global economy editor of The Diplomat, the Asia Pacific’s leading geo-politics and economics portal. Originally published at Macrobusiness
First the latest update from Beijing:
At 04:00 on February 8th, 31 provinces (autonomous regions, municipalities) and the Xinjiang Production and Construction Corps reported that 2656 confirmed cases (2147 cases in Hubei) were newly added, 87 severe cases (52 cases in Hubei) were newly added, and There were 89 deaths (81 in Hubei, 2 in Henan, 1 each in Hebei, Heilongjiang, Anhui, Shandong, Hunan, and Guangxi), and 3,916 suspected new cases (2067 in Hubei).
On the same day, 600 new patients were discharged from hospital (324 in Hubei), and 31,124 close contacts were lifted from medical observation.
As of 24:00 on February 8, according to reports from 31 provinces (autonomous regions and municipalities) and the Xinjiang Production and Construction Corps, there were 33,738 confirmed cases (including 6,188 severe cases), and a total of 2,649 discharged patients were cured (Heilongjiang reduced one) A total of 811 deaths have been reported, 37,198 confirmed cases have been reported (1 in each of Shanxi, Heilongjiang, Henan, and Hainan), and there are currently 28,942 suspected cases. A total of 371,905 close contacts were traced, and 188,183 close contacts were still in medical observation.
A total of 53 confirmed cases were reported in Hong Kong, Macao and Taiwan: 26 in the Hong Kong Special Administrative Region (1 death), 10 in the Macao Special Administrative Region (1 in cured and discharged), and 17 in Taiwan (1 in cured and discharged).
And the charts:
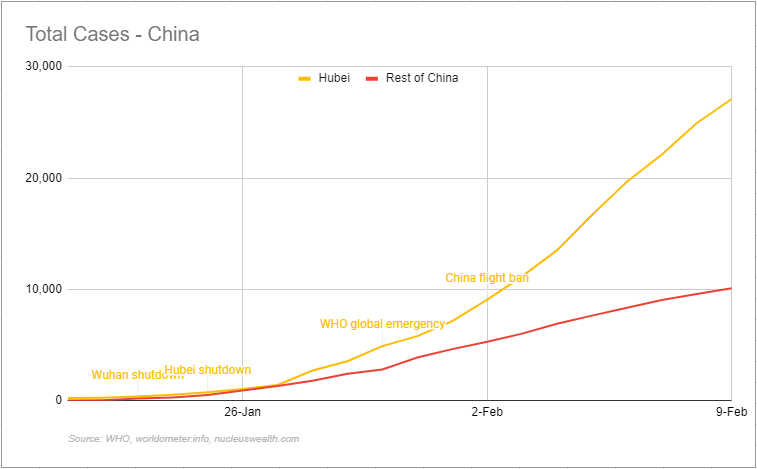
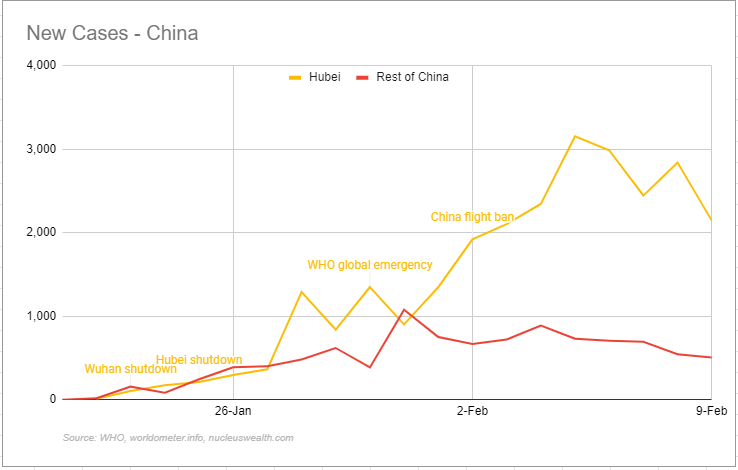
The most important news on the weekend was that Guangzhou (13m people) and Chengdu added draconian restrictions to their populaces and Apple assembly partner, Foxconn, was forced to close for another week.
It’s become impossible to track how many Chinese are now locked down. Most of the country to one degree or another. Some are reporting 400m. That is plausible.
The upside is that the shutdown appears, for now, to have slowed the virus spread in China. That’s great news. If you believe it.
The problem is, there are very good reasons to not do so. The epicenter of the outbreak in Hubei is clearly massively worse than is being made out. The number of deaths and other marginal indicators suggests 10x worse, via Bloomie:
The new coronavirus may have infected at least 1 in 20 people in Wuhan, the Chinese city at the epicenter of the global outbreak, by the time it peaks in coming weeks, according to scientists modeling its spread.
The typically bustling megacity, where the so-called 2010-nCoV virus emerged late last year, has been in lockdown since Jan. 23, restricting the movement of 11 million people. Trends in reported cases in Wuhan so far broadly support the mathematical modeling the London School of Hygiene & Tropical Medicine is using to predict the epidemic’s transmission dynamics.
That’s half a million people infected…
That discrepancy is indicating something else very important for the political response to the virus.
What’s Good for the CCP
The question is, what path is best for the CCP? Let’s not delude ourselves into thinking any other question matters, whether that of the Chinese public interest or our own. The CCP will do what best secures its power base amid one of the greatest threats to its rule since Tianenman Square.
At the moment it is caught between the need to defeat the virus and the vast ecomic damage being done by doing so. To date, it has managed this binary by lying about the severity of the virus and controlling the media narrative while deploying immense containment shutdowns. But with each passing day the economic damage makes this more difficult, right down to the basics of supplying food to 1.3bn people. It’s surely impossible for the CCP to sustain full lockdown for much longer without doing itself serious political harm.
It is probably true that the shutdown has limited the virus’ spread in wider China if not Hubei. But going back to work isn’t going to do that. And the virus is a long way from being eliminated.
This raises the prospect that, as virus containment and the economy come into greater conflict, the CCP may decide that its own best interest is served by letting the virus spread worldwide. Why? Becasue at least then it can throw its hands up and say “we did our best but this virus is beyond all human intervention”. An excuse that may wash with the Chinese people.
If so, it will allow its containment effort at home to slip while lying about it succeeding, and put a lot of pressure upon other nations to open their borders.
The Good of Other Nations
There is a problem if that’s the way the CCP is going. Most pointedly, Chinese authorites have inadvertently illustrated how best to combat the spread of the virus.
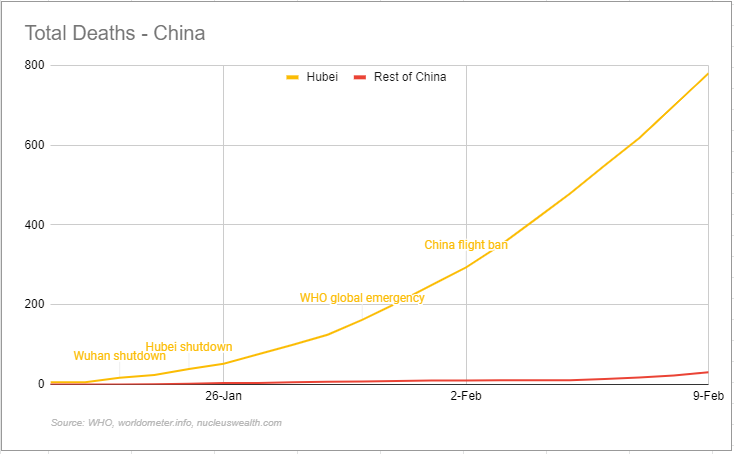
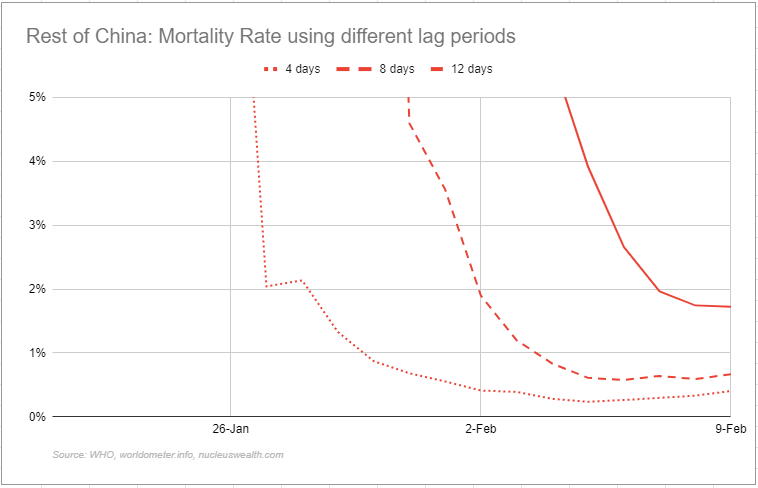
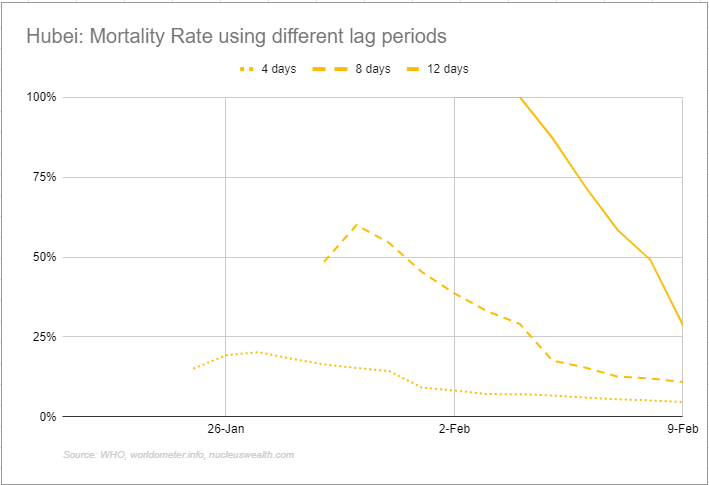
In Hubei, where authorities hid the truth and allowed the virus to spread, the mortality rate is massively higher than elsewhere. There are many reasons for this, not least being the outbreak began earlier and it has more cases. But perhaps the most important is that, once out, the virus proved virulent enough to overwhelm its public health system. Without proper treatment, the mortality rate skyrockets.
In short, the first order response for all nations is draconian quarantining of any outbreak so that any given health system can manage the outbreak at a pace it can cope with. If you allow the virus to spread unchecked even for a few weeks then it threatens a mass casualty event as it overwhelms response capacity.
Thus any government that opens up to China too early will find itself at risk of another outbreak, with the risk of higher deaths, versus the economic need to restore connections. Getting this balance wrong will trigger politically fatal allegations of killing citizens.
But any kind of ongoing isolation of China by other nations threatens the CCP. So it will ramp up pressure to release global clamps on its economy, and governments everywhere will find themslves caught between between Scylla and Charybdis.
The mind really begins to boggle when we consider the virus will likely get loose in less developed nations. There is some hope that it will not spread as fast in warmer climates but not enough to stop it. That could throw up an endless sequence of economic shutdowns applied piecemeal across the world as different governments respond.
It also raises the greater prospect of mutations and further pandamic waves.
The Upshot
There are no good outcomes. China has slowed but not contained the virus. It is very contagious and sending people back to work will bring it back on, jeoparding the CCP. Keeping them at home will jeopardise it even sooner.
The CCP is attempting to lie its way out of the conundrum. Other nations will be caught in the web. If so, nCoV will very likely spread globally, leading to a rolling shock of shutdowns all over the place.
Our base case is now a rolling shutdown in China for three-to-six months, rolling shutdown of contained outbreaks globally, with worse cases in EMs. This will hammer the global economy into recession and risk all kinds of financial contagion.
The upside risk case is no longer a SARS repeat. That hope is dead. It is that China contains the virus outside of Hubei over another few months as it incremantally opens up and stimulates wildly. This still delivers material damage to the global economy with a lighter recession held back by sporadic outbreaks of nCoV.
The downside risk case remains global pandemic and depression.


Just a point about medical systems – one curiosity about China (I don’t know the reason for this) is that doctors and nurses just don’t have the same status as in most other countries – its not seen as a particularly desirable profession. So with the exception of a dedicated core who have a genuine vocation for medicine (such as the brave whistleblowers in Wuhan, many of whom are now dead), the overall quality of medical staff in China is generally very poor. There is a reason you rarely find Chinese doctors or nurses in hospitals outside China, and even rarer to find ones trained in China. And there is a reason most Chinese who are sick fly to Thailand or South Korea or anywhere else for treatment if they can. If there is a medical system in the world worse than the US’s, its China.
Facts are available if you choose to look.
China – Infant mortality rate. In 2018, infant mortality rate for China was 7.4 deaths per 1,000 live births. Infant mortality rate of China fell gradually from 83.7 deaths per 1,000 live births in 1969 to 7.4 deaths per 1,000 live births in 2018.
During 2011-2013 (average), the infant mortality rate (per 1,000 live births) in the United States was highest for black infants (10.9), followed by American Indian/Alaska Natives (8.1), whites (5.1) and Asian/Pacific Islanders (4.2).
Searching on the net, I got a slightly different number from the 7.4 per 1,000.
That’s a minor point. The more relevant comparison, based on your comment, would be the Chinese Uyghur infant mortality rate, or of oother minority groups in China, of them there are officially 55, plus the Han.
I think its safe to say that no recent statistics coming out of China are reliable. I would venture to guess that in certain places, like HK, infant mortality is lower than 7%, but in the inner provinces, it’s much higher/not reported correctly/downplayed by the CCP. In the US, in 2017, infant mortality was closer to 4% in states like NY and CA, while most of the south, and, oddly, Rhode Island, had seven and eight percent mortality.
Silver cloud: after black death, European wages went up.
More seriously – Hubei mortality rate vs the rest-of-china seriously suggest that China is lying either on Huber, or rest of China, or both.
That’s why to me, the Diamond Princess, as unpleasant as it is for its passengers, is really a test case.
It has about 3.6k people onboard. Currently, there’s 136 confirmed cases, with not everyone tested. We can safely assume that most people were infected before the quarantine – Feb 4, 6 days ago, and that until then, it was “free for all”. The final number of cases on the ship will provide a good sample of how virulent it is, how effective total quarantine is and what is the progress – all items that the CCP held on tight leash so far.
It may even provide (unfortunatly) some insights into mortality – if the mortality is high (if it’s 1-2%, then the error will be likely too large for any good stats).
Good points, though I wonder about the Diamond Princess as a good “test case”. Many people are saying the ventilation system on the ship is really helping to spread the virus. I can’t evaluate this claim, but if it’s true, then this ship is tipping more towards a worst case scenario. Also if true, I hope the govt of Japan takes action sooner than later.
That makes it an excellent test case. If the virus can be spread through a ventilation system, then planes and office buildings become primary venues for transmission spread since most of those don’t have HEPA filters.
Since they have all these people bottled up in their rooms and presumably workers are squirting lots of surfaces with disinfectants, it becomes an excellent laboratory for understanding how risky this disease is for transmission. This is similar to the way that cruise ships have become floating experiments for norovirus transmission on a regular basis. They should be able to figure out if this disease is more or less transmissible compared to a norovirus since there are lots of test cases of that on cruise ships.
People travelling to and from China from the Western countries tend to have a fair amount of money, so if they are based in the West, they probably have good health insurance and enter the healthcare system readily. Also, flights are easy to identify and quarantine or track individuals from.
If this gets loose into the poorer areas of San Francisco, the Bay Area, or Florida, then all bets are off as the poor and the immigrants often want to stay off the radar screen and will probably not actively seek out healthcare until they have had lots of opportunity to infect others.
Southern California, and Seattle should be added to that list, along with the fact that many of the poor have no sick days and cannot afford to take off of work.
But also, I can imagine the doing just fine and the doing far better than most, also deliberately going under the radar when not feeling well; especially, if this is true, new research out of China notes that the incubation period could be as long as 24 days.
Additionally, San Jose’s Mineta International Airport has yet to institute screening like SFO, for some never explained reason; especially since Silicon Valley has quite a number of non Chinese Nationals who previously frequented China, along with ample private jet flights in and out.
I was going to ask, since the bans went into effect 8 days ago, what would it mean if we dont have any new cases here between now and this Sunday?
Maybe the question changes the date to the 26th instead of the 16th of this month.
The horse is so out of the barn that who’s to say how many new (or old, for that matter) cases there are, especially if the incubation rate is now suspected to be 24 days.
Prepare to lock yourself down for a long time at home:
Can anyone argue with this logic?
“There are two problems with this official assumption that house-arresting everyone from Wuhan will end the pandemic:
1. Given that Wuhan residents traveled freely around China for the month before the citywide quarantine, infecting people in other cities, there is now a pool of carriers who did not come from Wuhan, so quarantining everyone from Wuhan won’t stop these people from infecting others.
2. Much of the dirty, poorly paid work in China’s cities is done by “illegal migrants” from rural areas who don’t have official residency in the city….”
https://www.oftwominds.com/blogfeb20/wave-two2-20.html
Let alone illegal migrant workers in China, I’m bleakly ‘bemused’ by the lack of mainstream commentary regarding non Asians having carried the virus out of the country on private corporate jets, etcetera; especially when there are likely many Multinational Corporations, incorporated in Delaware and domiciled in Silicon Valley, etcetera, with International Headquarters in China. Or simply obscenely wealthy non Asian Us citizens who don’t need a jawb, vacationing for the New Year’s Celebration.
Anyone who’s ever had a ‘lowly’ job would agree that Private Jet owners and First Class Passengers would likely be economically intimidating and would be treated far, far more deferentially than the average person (at say, an airport), along with being able to pay quite handily for silence. If a Pandemic is to occur In the US, it might morel likely begin in a very wealthy community (perhaps named Samara), versus a food market where both the wealthy and poor might mingle.
No, the lack of official residency does not make migrants illegal. What it does mean is that in many (but not all) cities, migrants do not have access to free schooling and free healthcare, while residents do. Again, there are a variety of mechanisms for migrants to become residents. But Chinese cities remain similar to other cities around the world (including Japan), where newcomers (be they from the farm or mine, or from another country) tend to start at the bottom of the labor market.
Now in China incomes have risen much faster than the healthcare system expanded, so even residents have to wait in line (which wait can be expedited, for a fee). The system is evolving rapidly, but even in the US, we would not have enough unoccupied beds to handle an influx of the magnitude seen in Hubei. Ten years ago a new disease such as this might not have been spotted in the first 2 weeks, given relatively low mortality (small sample sizes make mortality rates a guesstimate, and bad air pollution means respiratory side effects are pervasive). This disease was “typed” and precise diagnostic tools developed in a markedly short time. Kudos to China’s reservoir of highly skilled medical professionals!
I suspect the first Santa Clara County case, who flew in through Mineta International on January 24th,, and was claimed to have immediately confined himself, may have been a non Asian passenger.
That case also resulted in five Good Samaritan Hospital workers being home quarantined (most certainly along with their family members and/or roommates?) for fourteen days (or now extended to 24?), after he visited there on the 28th of January:
Sorry, about that long link, I screwed up the end link html, and the preview function was temporarily not previewing:
That case also resulted in five Good Samaritan Hospital workers being home quarantined (most certainly along with their family members and/or roommates?) for fourteen days (or now extended to 24?), after he visited there on the 28th of January:
It’s lying, or more simply, not wanting or even not able to know the truth on Hubei and the other provinces. The incentives for such ignorance in provinces that host major hubs are even greater. Even more, those incentives might also be already in place in some other countries. Singapore has a true dilemma: quarantine herself would be like self-shooting both legs. Closing for tourism and business travel, rather than commerce, looks the most necessary if we want to delay the pandemic at least for this northern hemisphere high season. And the geographic scope of the closure should be more ample than just China according to recent developments.
Regarding the rolling shock of shutdowns foreseen in the base scenario, those will be increasingly difficult politically, and at some point simply useless. For instance, summer in Northern hemisphere temperate regions might relax vigilance. Disease spread could accelerate in Southern Asia during the dry season and in South America, South Africa and Australia when winter approaches in a few months. There are the summer reservoirs for next northern hemisphere winter outbreaks. Are we willing to quarantine whole hemispheres?
Winter is coming!
I’m wondering to what extent serious and fatal effects of the disease will manifest among persons of non-Asian descent.
Suggestive but hardly conclusive. If it turns out that particular populations are more at risk based on heritable and identifiable vulnerabilities, then we can focus resources on helping them if for other groups this virus causes nothing more serious than a common cold.
What happens aboard the Diamond Princess and in locations outside China should be revelatory. On NPR just now a woman who tested positive for the virus said in an interview that she didn’t even realize she was ill with anything other than a very mild cold.
Great! She can swan around giving the virus to the more vulnerable. Lock her up! Sorry, giddy silliness is one of my fear responses. I was once held hostage for several hours in fear for my life. I could hardly keep from laughing the whole time.
Before today, new cases on that particular ship referred to the original 200 plus samples (the first batch).
The plan has been that if there are no new cases (meaning in passengers or crew other than the first 200 plus) – and the results from that first batch were released over many days, giving a false impression of ‘new cases’ – then 14 days is the max., but any new cases reset the 14 day clock.
Are today’s 60 plus new cases from that original first batch?
(14 days now, though could be 24, according to one comment here).
It won’t be boring…
This article supposes that CCP may be trying to hide the extent of the outbreak by purposely underreporting confirmed cases in order to give the impression that their containment measures are working. It then further argues that this is likely to lead to other nations relaxing their travel restrictions, leading to outbreaks in new countries and new radical control measures implemented in those countries.
I feel rather mixed about these claims. I don’t doubt that the CCP would lie or otherwise manipulate the data to suit its perceived interests. I don’t even doubt that they would try to lie, even though it may do them more harm than good. What I doubt is that they could actually get away with lying. If containment is insufficient to control its spread, and especially in light of China’s woefully insufficient medical infrastructure, then the impacts to the country will be impossible to ignore. Furthermore, in time we will hopefully learn more about the cases in other countries, and if things look bad there, then I Would not expect any loosening of travel restrictions any time soon.
Looking at the data reported via the John’s Hopkins visualization system, I ran a new log-linear regression to estimate transmission rate using the last week or so of data. I only included the last week because the growth appears to be leveling off. (I also ignore the most recent data-point because it is missing cases that will be reported later in the day.) If these numbers can be trusted, then growth has indeed slowed. Confirmed cases only doubled every every 6 days or so. The trend suggests the rate of doubling as of today may be closer to 9 days as of today. This is a dramatic improvement from before, but it’s not yet clear if this trend reflects successful containment or merely a reduction in the rate of spread. If the latter is true, then growth may remain exponential. This would mean that the outcome in China would be the same, it’d just take longer to get there, which might actually be worse for the economy.
Likewise, it remains to be seen whether containment measures taken in other countries including the US have been successful. It may take another few weeks to knows for certain. My concern is that Acute Respiratory Distress Syndrome (ARDS) may be frequent enough under normal circumstances that it may require a few “generations” of infections (with long incubation periods involved) for a spike in ARDS cases caused 2019-nCov to register above the baseline. It would be very smart for the US CDC (and similar bodies in other countries) to advise that all ARDS patients be tested for 2019-nCov in order to catch it quickly in the event that containment is breached. Otherwise, we risk failing to recognize a new outbreak until it’s already very big as happened in Wuhan.
I’ll have more to say in a separate post.
Look at that data on a linear plot and you can see that the curve went linear a couple of weeks back, so the idea of exponential growth with a declining rate is misleading. The case curve seems limited now by the system capacity for testing. If you can only test 3K cases per day, you’ll see linear growth at that rate.
The FT has an interesting article today, on one family’s experience of the disease, that suggests the actual case numbers are far higher (10x or 15x?) than the official ones, just as the post today suggests. Again, they don’t count a case until they’ve confirmed it with testing.
Apparently over the weekend the authorities changed the criteria for what’s considered a confirmed case–against WHO guidelines. Now, even with a positive test result, if the patient is asymptomatic they are not counted as a confirmed case. This took 5k off the newly confirmed case list.
Yes. They are either goal seeking data or the numbers are completely dictated by the ability to test. Also, they recently changed their own protocol for defining a confirmed case, again indicating they are massaging numbers with a priority going to propaganda, not science.
On the topic of questioning their ability to contain the truth, note how effectively they have kept the Uighur narrative under control. In the west we underestimate how effective massive information control is. Almost everyone there relies on a single phone based social media and chat platform (WeChat). This provides an excellent bottleneck for central information control. Instant censorship of messages and link sharing is commonplace. I have seen it when sending info to friends, even ones sitting beside me in a cafe: send a news story link to a friend for interest and it just disappears.
The case for exponential growth is supported by theory of transmission dynamics early in an epidemic while most people in the vicinity of the outbreak haven’t been infected yet. The case for “linear growth”, more specifically the leveling off of daily new cases, is supported by the plausible proposition that testing capabilities are saturated. If we assume adequate quarantines are in place, than the growth may look more like a logistical model. Yet another possibility is that the data are complete BS and we’re wasting our time discussing it.
Honestly, I don’t think the data sheds light on any of this right now. Most insight will be gained in hindsight. I chose the exponential model because I believe it’s most informative in the early phase. With quarantine measures having been put in place, it’s reasonable to expect a leveling off of growth new cases, but this says nothing about whether containment has been sufficient and what the long-term outlook is like. And if containment is not sufficient, then the effect will be to merely slow the growth, prolonging the inevitable spread of the disease. Mind you, slowing growth can profoundly improve survivability and overall social stability if treatment infrastructure is not overloaded and should not be underrated.
About the information control. If the Chinese have something to hide, then they are surely in big trouble, and the *scale* of the disaster is likely to be such that they won’t be able to hide it much longer. This is directly impacting supply chains in the world economy, as has been discussed here repeatedly and is now acknowledge widely in the news. The fact that the stock market is acting like 2019-nCov is no longer a threat says more about their self-delusion than about China’s ability to control information. People will accept just about any “data-driven” conclusion if it is presented in graphical form and supports their pre-existing biases.
If 2019-nCov is as nasty as it looks to me, we could all be in for a whole lot of bubble bursting later this year.
I find it difficult to not want the bubble to pop. Twelve years of can kicking with TARP, QE, Twist, Repo madness. I just want to get to some price discovery in this damn market. I feel guilty about wanting it but I want the circus to end. Maybe because I didn’t buy every dip and I’m jealous, but my Gordon Gecko sense is tingling…
Here’s why they, and other Powers That Be, would lie:
https://www.oftwominds.com/blogfeb20/wave-two2-20.html
Hmm. https://www.theguardian.com/world/2020/feb/10/coronavirus-uk-declares-outbreak-serious-threat-to-health
The interesting bit on this is that one of the diagnosed was a doctor. Not a good news for Brighton.
One thing lost in all this is how the tremendous effort by the CCP is doing the world a lot of good by buying time. These sacrifices should be remembered.
Agreed. I’m not sure how well we would do in the west with such a threat. For the US that would be about 110 million people locked down, for the UK that would be about 20 million people locked down and for Oz that would be about 8 million people locked down.
And before anybody goes on about how great medical technology and facilities are in the west, consider the political leaders that would be in charge of such efforts in those three counties alone. So that would be Donald Trump, Boris Johnsone & Scotty from Marketing.
Yes, They .. and by extention, Their’s .. would be #thefrontoftheline … only the most efficacious anti-virals & top-of-the-line breathing machines for them. The Best of Care. I would include the many head municipal honchos and important oligarchy from coast to coast !
For us lowlies .. to loosely quote the Stewart of Gondor : “Go die in whatever manner suits you”….
Laughed out loud the hardest I have in weeks from your Denethor quote. +1
The West is democratic, meaning it could be messy, chaotic like what was observed of the turn of the century Austrian parliament.
We see that with travel bans, as people argue about them. ‘Won’t stop anything!’ They have been criticized here, and also by China.
Oz that would be about 8 million people locked down.
Snark: Historical Oz, or present day US: that would be about 8 million people locked up?
Well considering the quality of medical help available within the state(s) prison system and the priority given felons in general, this could relive “some” prisons over crowding. And if you consider latin America ( Brazilians prisons might rate their own separate considerations), if I am to believe what I have read about Mexico, Honduras prison conditions.
I wonder what would have happened if such an outbreak starts in, for instance, Italy. We would be blaming the Italian government for everything right now. It is our favourite game.
China’s top priority is saving and protecting Chinese citizens, as would any nation for their own.
Wuhan is sacrificed to save Shanghai, Beijing, etc., first and foremost.
Going back to work now vs continuing the sacrifices – that is the immediate question for many people in China now.
I bet the honchos in Beijing find it real tough to sacrifice the lives of people in Hubei (really, Wuhan).
I wonder how those in Hubei/Wuhan government come out of this. Those who delayed and lied and held huge public events after knowing about the virus.
Not to say there aren’t good decisions and bad decisions made in the response. But just as important as remembering is correctly ascribing agency to those responsible.
“According to one study, China has only 60,000 general practitioners or one per roughly 23,000 people. ”
Quite a claim and likely wrong. The number of GPs also says little about a health system that is build around clinics.
OECD statistics say that China has 1.7 practicing doctors per 1000 population.
https://read.oecd-ilibrary.org/social-issues-migration-health/health-at-a-glance-2015/practising-doctors-per-1-000-population-2000-and-2013-or-nearest-year_health_glance-2015-graph47-en#page1
WHO says 1.786 / 1,000
https://www.who.int/data/gho/data/indicators/indicator-details/GHO/medical-doctors-(per-10-000-population)
Commonwealth Fund says; “In 2014, China had some 173,000 licensed and assistant GPs, representing 6.0 percent of all licensed physicians and assistant physicians.”
https://international.commonwealthfund.org/countries/china/
I’d like to chime in here. People don’t go to GPs here like they do in the US. Instead, they go to hospitals and go to straight to a specialist. For example, my friend is a dancer with a joint problem. She went straight to an orthopedic doctor at the hospital.
However, if you have cold symptoms, you go to a doctor at the hospital and that person is probably going to be a GP. They would then send you to a specialist down the hall of need be.
In the US, the hospital is a place of last resort. In Asia, it’s often the opposite, a one-stop medical facility that will have a pharmacy on premise as well.
As for the emphasis on Chinese medicine… It’s baffling, but you can even get this at hospitals and it may be covered by your insurer. My local pharmacist always pushes these snake oil remedies on me along with whatever actual medicines they recommend.
Thanks, Japan is indeed similar. People do not have a personal physician, even in rural areas. Now this is partly an urban phenomenon – in rural areas in China local clinics may not have a doctor, only someone who does triage, and the training to treat everyday problems (cleaning / stitching wounds, handling kids’ ear infections, checking blood pressure and blood sugar). But the behavior is the same: you go to the local clinic/hospital, not to a specific person.
Again, given the rapid pace of urbanization (350 million people in the last 25 years or roughly the population of the US), urban services of almost every sort, from sewage treatment to schools to healthcare, have had a hard time keeping up. The ability to add beds quickly, and pull in professionals temporarily, has surely kept mortality lower.
For anyone interested in gaining facts, not fiction, about this virus and associated topics, may I point you to two very good YT channels….
Dr John Campbell and MedCram
https://www.youtube.com/user/MEDCRAMvideos
https://www.youtube.com/user/Campbellteaching
Respirator s require constant monitoring, beep or go off if patient moves at all. Patients are often kept on sedation, so become total care. This requires intensive nursing. Even large city hospitals only have a few ICU rooms, and two or three designed for TB with negative air flow, and staff tend to leave the doors open. I don’t see things going well here, either, in the event of a plague of pneumonia.
Relatedly, I read the article titled “Reporter’s Notebook: Life and death in a Wuhan cronoavirus ICU” (use search engine to bypass paywall) and the associated JAMA article. There is a lot of good information there, but not enough to get a good handle on mortality.
Among the helpful bits are the description of the case progressions. All studied patients were serious enough for hospitalization, which typically occurred around one week from the onset of symptoms. A subset of these required ICU, starting roughly around the end of the second week. A subset of ICU patients died around 3 weeks in. While some patients who are serious enough for hospitalization might survive without it, patients who need ICU will probably die if the resource is not available to them. Also of note is the cause of death appears to typically be multiple organ failure due to immune system collapse, particularly for those that progress to the ICU. It should also be noted that even patients who survive often need several additional weeks to recover. Many patients diagnosed at the start of the epidemic are still hospitalized.
Unfortunately, it’s very tricky to estimate what fraction of patients will tend to reach each stage of progression. Because of the long duration of the progression and the very short period of data collection in the study, naively calculated estimates (e.g. number of deaths divided by total cases) are likely to be overly optimistic. On the other hand, a lot of patients in this study may have been “front-loaded” within the study period simply because the hospital ran out of capacity quickly and had to turn people away later.
In any case, the fact that it takes a long time for death to manifest is startling. Assuming unlimited ICU resources and a 1-2 week incubation period, it could take 4-5 weeks for a new terminal case to actually contribute to the death count. Even where hospitals are overwhelmed and unavailable, the time to death after new infection may be 2-4 weeks. What remains unknown is how long it typically takes for a new case to become “confirmed”. Given the data I see, I’m leaning toward the assumption that most cases aren’t confirmed until they become serious and seek hospital care. That would further suggest that a lot of cases are not being accounted for because people aren’t getting tested.
Looking at just the numbers in this study and assuming (very charitably) that almost all the patients were hospitalized early in the study period, about 1/4 of those hospitalized require ICU treatment, and 1/4 or maybe a bit less of those who got ICU treatment die. A big open question concerns how many cases progress to the point that hospitalization is required in the first place. I don’t think we have any idea looking at the China data. Let me just pick 25% out of thin air here. If 25% of cases require hospitalization and if 5% of those die, then we have an overall mortality rate around 1.25%, which is quite serious if the disease cannot be contained. However, if the spread of the disease cannot be contained or slowed enough to prevent ICU resources from becoming exhausted, mortality may surge to 5-10% or higher which would have devastating consequences if on a global scale. Again, these figures follow from a number I pulled out of thin air, and hopefully data from other countries and that cruise ship will help us fill in the break here.
Lastly, I’m not inclined to take much away from the mathematical model that was linked in the article. The calculated results don’t even seem to fit the data well, what data there is. I think the conclusion that Wuhan infections will peak in mid-to-late February may also be overly optimistic, but a lot depends on whether containment measures are successful. As I already mentioned, if the containment measures merely slow the spread of the disease without actually containing it, then it could take a while to reach the peak.
I’m guessing that this sort of analysis is very effective communication in the globalized market. All our efforts to create a wonderful globalized economy will be ruined if we don’t establish effective medical responses and treatments for raging epidemics. Good health care is a prerequisite to a functioning market. That might be considered a silver lining to 5 million casualties – or it might be considered a no-brainer. But it probably won’t be ignored.
This is going to be a major test of the resiliency and robustness of the global supply chain. Auto and other companies had stocked up parts in inventory in anticipation of the Chinese New Year, but they did not factor in an extended shutdown afterwards. There is probably a couple of weeks when the manufacturing system gets really stressed due to lack of Chinese parts. If the internal China quarantines and plant shutdowns or slowdowns continue, then we will get to see how good the MBAs really were at planning and risk management. My suspicion is that they used models as effective as VAR (Value-at-Risk) and crises would develop fairly quickly.
It might end Globalization, not affording chances to ‘”create a wonderful globalized economy.’
Good health care should be for the sake of good health care of the people, and not for a functioning market.
Among the many concerning factors associated with this outbreak is that tests for the virus can come back negative even though the individual has contracted the virus. Just a few days ago, some of the quarantined Americans at Fort Travis in northern California displayed symptoms but tested negative and were sent back to join the others who are under quarantine.
Separately, now, the “Chinese National Health Commission has changed their definition of #WuhanCoronavirus “confirmed case” in their latest guidelines dated 7/2. Patients tested positive for the virus but have no symptoms will no longer be regarded as confirmed. This inevitably will lower the numbers.”
https://twitter.com/Trinhnomics/status/1226864221356359680?s=20
“Among the many concerning factors associated with this outbreak is that tests for the virus can come back negative even though the individual has contracted the virus.”
Link to show that? i mean of course NOT test is 100% sensitive. But where are you seeing that this test fails more than uncommonly?
Lack of sensitivity (i.e., a tendency for false negatives) is to be expected for a variety of diagnostics, arising due to a variety of reasons.
Lack of specificity (i.e., a tendency for false positives), which is what the Chinese National Health Commission may be responding to by not “confirming” people without symptoms. I don’t think we have enough knowledge to judge whether this is appropriate. If the true specificity is quite low, then the risk is that many healthy people will be exposed to the disease. However, lack of symptoms doesn’t necessarily mean the test was wrong or that the subject is not contagious.
Unfortunately, these are basic statistical concepts that even doctors struggle with, to say nothing of management, spokespeople, etc., many of whom heavily influence decision making. Most politicians and maybe lots of “technology” people too probably assume that a *test* yields gives a yes-or-no answer with 100% reliability and act accordingly to our detriment. Either way, we’re pretty much in the dark about these things without better data.
I am worried about both the food supply in China and the prices. My mother-in-law in Guangzhou told us that food prices (in particular, pork) were rising rapidly. For poor Chinese out of work, I could see their savings depleting rapidly.
Will more people in China want to emigrate after this is over (important to remain optimistic)?
As for now, Basic Income is one way to go.
I have to call this one out. The author is projecting a sinister narrative onto Chinese official motivation. If the vires escapes China (which it already has) we get to claim MIHOP (Made It Happen On Purpose.) He has no way of know what the Chinese are thinking, let alone how they will think in the future. The vires can just as easy escape out from genuine efforts to control the outbreak.
I confess I am both baffled and (to a lesser extent) cautiously optimistic.
The situation in China is clearly grave and unique. The population suffers from poor sanitation, water supply, pollution, poor quality medical services etc. And as others have noted there may be a genetic or racial element to infectivity.
I have spent a fair bit of time in Singapore over the last few decades (first visit: 1989) and to my mind it is an important test case. If the incubation (w/o symptoms) period is 7 to 14 days (or more) and given the Chinese New Year travel, there should have been quite a few infected individuals in Singapore over the last fortnight or so. Keep in mind that the foreign (Indian, Malay, and others) workers tend to live and work and commute in close proximity. And the popular food courts could be a beehive of transmission.
So if a number of infected individuals entered SG from China, and given the incubation period and alleged high rate of transmission, why haven’t we seen an explosion of cases in Singapore? Especially among the very low class, living in dormitory conditions and travelling to work crammed 10 or so in the back of a pickup truck?
I am probably just hoping for the best here. Let’s see what happens in Singapore over the next few days and weeks.
I’d like to see the Chinese statistics on how many people die from pneumonia as that seems to be the fall back case of death. If that has surged lately…
China…and still relies heavily on traditional medicine.
The explanation of why a particular herb is efficacious might sound like an explanation from the dark ages in Europe, but I don’t doubt the ability to analyze cause and effect.
Doing some mining in the traditional Chinese Medicine would probably spotlight some very useful treatments.
My father in law was emphatic that the Chinese Medicines could be effective, and were not as harsh as western medicines.
“the best hope of saving a severely ill coronavirus victim is to put them on a respirator…equipment not in great supply even in Western hospitals.”
It’s a virus. Even in Western medicine, treatment for viral diseases is mostly just supportive – like respirators,at the extreme. Desperately trying to keep the patient alive until the viral attack wanes.
So I wonder how much less effective Chinese traditional medicine really is, in this case. Biggest problem would be the lack of respirators or isolation equipment – and that can be just as much a problem in Western medicine, just because the need is so intermittent. (Cities around here don’t have much snow-removal equipment, either, just because they rarely need it.)
Chinese traditional medicine might be a good place to hunt for anti-virals, presently in desperately short supply. Naturopaths claim to have some, too; I have no clue how effective. But there’s something like a class system in what gets thoroughly tested. Known, traditional medicines can’t be patented.
Yeah, but if you can’t charge prescription level prices for them, then they can’t possibly help.
(sarc)
Just because pharmaceutical companies are criminal doesn’t mean wearing a mask and shaking a rattle is effective. There is no cause and effect relationship between the questionable ethics of big pharma and the dearth of evidence supporting countless traditional interventions.
Placebo has been proven effective and highly so, frankly. Sometimes I wish I believed in magic myself. Talking to imaginary supreme being is literally a proven positive health intervention.
This is a wonderful opportunity to stress why we need M4A:
“Sure you can afford the best doctors, but the people who are handling your salad, your food, your clothing, touching your children, may not.
Sure hope you are voting for Sanders…”
These viral epidemics are not one-off events. We will see these increase with the increase in human population. It would be reassuring to hear that WHO is making recommendations for these events that are sufficient and effective; that the UN is demanding all nation states submit to WHO directions in the event of an epidemic; that the quarantine rules be enforced at law with substantial penalties for disobedience.
I should also like to see social activities reduced. Many people work from home; teachers can teach from home; there is often a way of communicating these days that does not require face-to-face meetings. I should also like to see a governmental ability to regulate childbirth. China operated a one-child policy that was quite effective. We should revisit that. Our human population is getting to look like an infestation.
Humans are social animals, your suggested even further distancing (which has already been an utter Techno, forced human transience, disaster of epic proportions) is a dystopian death knell for humanity, in my small opinion.
Further, the one child per family policy was a disaster in China, which now has a huge overpopulation of males (33 Million plus) to females; as does India, even without any such requirement.
Good luck with that all male world, as I’m certain the one child only requirement would end up the same in other countries (including so called developed [Enlightened [White]!™] countries), female babies being aborted, and worse.
Frankly, if any population control is enacted, it should be on the filthy immoral rich – as in zero reproduction allowed.
The CCP needs to get better SpokesLiars™.
The falsehoods coming out of the CCP are either amazingly amateurish, or are DESIGNED to be recognized as false.
I believe today was meant to mark the end of the (extended) Lunar New Year holiday period. Apart from Hubei Province which is locked down, did the CCP ever give the green light for the mass migration of hundreds of millions from their home villages back to their cities of employment? I never seemed to hear about that taking place as yet.
I read that there are rather strict criteria in place in many provinces for factory owners to prove their workers are “healthy”, (or at least that bosses have taken the requisite quarantine precautions) before they are given the go-ahead to re-open, but I’m wondering what percentage of factory workers are still unable to work because they haven’t yet been able to make the trek back from holiday?
Just for reference, in 2018 Chinese urban mortality causes were as follows: #1 at 26% was due to cancer, #2 at 23% was heart disease, #3 at 20% was stroke (“cerebrovascular”) and #4 at 11% was respiratory. Of course seriously ill patients do catch pneumonia, so it is surely a more frequent proximate cause of death. There is no separate category for diabetes and complications thereof, it perhaps falls #6 at 3% under “endocrine, nutritional and metabolic”, with accidents #5 at 5.7%. Rural mortality is roughly similar, with stroke and heart disease a bit higher, and other causes correspondingly lower. Infectious disease in both is about 1%.