Yves here. This look at Covid-19 data shows how one needs to be modest in reaching conclusions, since much of the information bandied about (most importantly, confirmed cases) is of dubious quality and not comparable across countries.
Nevertheless, I’d add one consideration to the list: the stringency of the various “quarantines”. China’s was very tough, with people in cities not allowed to leave their apartment buildings if a temperature reading at the entrance showed a fever. It is an open question as to whether our halfway measures (closures of lots of businesses but no restriction on movement of people) will be good enough.
By Ignacio Moreno Echanove, an epidemiologist
I am analyzing the evolution of Covid-19 epidemics in three different regions of the world, identify the differences we can find, and speculate on how the disease spreads differently in these regions. The three regions are examples of full-blown epidemics managed with quarantines (mitigation).
I have not included data from South Korea since that can be considered a case of clever management during the contention phase.
The three regions are the province of Hubei (China Popular Republic, 58 million inhabitants) where all started, Italy (61 million) the country showing so far the highest toll, and Spain (47 million), following Italy’s path with a short lag in the development of the Covid-19 epidemics. I hope to provide some light in the development of the epidemics and provide a few hints on what to expect in other regions where the epidemics are developing now with some lag.
First, as a tracker of the epidemics, I don’t follow the number of confirmed cases as reported by every country. This number is in my opinion useless to track the disease for various reasons. I don’t want to belabor this argument but to have an idea of how an epidemic developed, what is needed is the testing of random samples large enough to give a significant number of positives that are representative of the true geographic distribution of the epidemic. In the early days of the epidemics this would be difficult and requires… what South Korea and South Korea alone has done.
There is an instrument that is used to track the epidemics of influenza, which very useful to decide each season what vaccines to choose (FLUNET). It may be have been diverted by some governments to track Covid-19 epidemics. I would certainly do so if I were in a position of authority! If has happened, it has not been publicly acknowledged as far as I can tell. However, according to a report from the WHO, this was done at least in Guangdong province in China.
Instead of confirmed cases I prefer to track the sad number of Covid-19 associated casualties. Mi hypothesis is that Covid-19 casualties are a much better reflection of the true extent of the epidemics. Probably very few are missed in reports and the cumulative number is an indirect indicator of the number of total contagions that had occurred in between 20-30 days before reflected the mortality data.
Remember that symptoms appear at about 5 days and disease development takes 2 weeks for mild cases and three for the severe cases. Cumulative casualties is a lagging indicator of course but after all more representative than reportedly confirmed.
The next graph shows the cumulative number of casualties in the three regions but synchronized starting the day when 6-8 cases had been reported in each region. The dates in the horizontal axis are valid for Hubei. Data for Hubei starting 21st Jan is from JHI web as reported by the WHO. Data for Italy (starting Feb 24th) and Spain (starting March 8th) are from Wikipedia. The initial lags are 35 days between Italy and Hubei and 13 days between Italy and Spain. The arrows indicate the starting day for general quarantines in each region. A blue ray (¿?) indicates the day when Hubei epidemics showed an inflection with daily casualties declining sharply: 31 days after quarantine start.
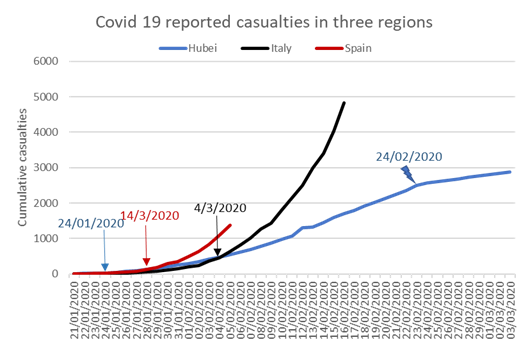
The Hubei epidemic is the only that so far shows the shape of a logistic curve, though compared with those of Italy and Spain looks nearly linear. It can be seen that the number of casualties dropped sharply on Feb 24th, coincidentally the first epidemic day shown in the graph for Italy. This sustained drop started 31 days after the start of the general quarantine. According to Zhou et al., (https://www.thelancet.com/journals/lancet/article/PIIS0140-6736(20)30566-3/fulltext) the median duration of Covid disease in severe cases is 20 days after symptom onset but on non-surviving patients median time to death is about 18.5 days.
In these curves the shape of the logistic curve will depend on the date of general quarantine start resulting in sharp reduction of RO and the development that should show up at about 5 days incubation period plus 19 days to death for a total of 24 days. The drop in Hubei, 31 days after quarantine start, exceeded by 6 days that of the disease development and it can be speculated that it could be due to chaos in the beginning of the quarantine, a spike in home contagions and some statistical mess. I would expect that this time “to sharp reduction of daily fatalities” could be somehow shorter in Italy and Spain. My experience is that the effect of emergency measures was quite sharp in Spain and I think it was the same in Italy after the Chinese experience. So one could expect to see some relief in Italy by the 31st of March and in Spain by the 10th of April, regarding the numbers of reported fatalities. I will refrain to project current trends publicly until those target dates but looking at the graph it is possible to understand that it can be quite horrible.
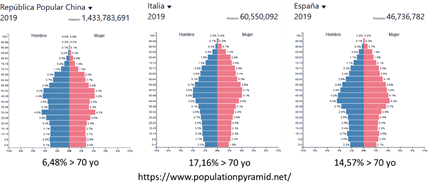
The starkest difference between these three curves is the slope of the regression, related with overall mortality rates. The slope is so far as twice as large for Spain (we have not seen the peak) and about four times larger for Italy. Why is this? One reason, given that the mortality rates are much higher for the elder, could be differences in the population pyramids of the three regions. Next graph shows a comparison of these pyramids that demonstrates the distribution of ages is less favourable for Italy or Spain. In particular there is a sharp difference in the proportion of 70 years old and elderly which is more than twice as large for Italy or Spain compared with China (assuming the distribution in China is representative of Hubei).
If this is the main reason explaining differences in slope, I would expect the slope in Spain would be somehow lower than the Italian one.
Another possible factor could be that quarantines were decreed in different moments on the evolution of the epidemics. The sooner, the lower slope. In this case Italy is again the worst case (11 days delay compared to Hubei) followed by Spain (4 day delay). These two reasons combined could explain the differences seen so far.
A third difference is that the exponential growth of the epidemics starts somehow sooner in Spain compared with Italy or Hubei by about three days. A possible explanation for this is that while in Italy and Hubei only one cluster was detected in the beginning, in Spain two clusters were simultaneously seen, one in Madrid and the second in the Basque Country. So, Spain is a tale of two close epidemic outbreaks. In my opinion those clusters expanding so fast out of control may have a common element: the so-called “superspreaders”.
These stories suggest a few things to be considered in other ongoing epidemics and for the future.
1) If “superspreaders” are involved in sudden outbursts, containment measures should account for this possibility and provide for intensive and extensive testing of the population around any given case. This could explain the South Korean success. In other examples where the epidemics still looks linear in the absence of such extensive testing, it may be the fortunate case that so far, no superspreaders have surfaced. Perhaps there was an undetected superspreader in Washington state. In France, UK or NY, the increasing numbers may be related with many individual contacts with Italy and now Spain (or Iran, SK) rather than a superspreader. The differences between NY and CA may reflect less direct contact with Europe in the latter case.
2) When containment has failed and uncontrolled spread is seen, the sooner quarantines are decreed, the better.
3) Other differences can be related with the intensity of social relations in large metropolitan areas like Wuhan in Hubei or Madrid in Spain (and presumably NYC?). Madrid accounts for about 60% of casualties in Spain. I think that NYC is now making a big effort to test everybody and this is good though a bit too late now.
4) Last but not least, the proportion of vulnerable people in a country will almost certainly affect overall mortality and contribute positively or negatively to the slope of the curve.


As the article mentions Basque Country, I have to say that the origin of the outbreak was a funeral, of mostly gipsy people, in Vitoria. With subsecuent outbreaks in Haro (La Rioja), Labastida, and Pamplona (Navarre).
You know that in funerals people gives lots of kisses and hugs. A superspreader? Maybe
On the other hand, in March 8th, tens or hundreds of thousands women were making demonstrations in all Spain cities, vindicating women’s rights.
I personally think it was an irresponsibility of the Spanish Government to allow it, when the coronavirus was already spreading in all the country.
Afterwards, the government took the right measures, but too late for containment.
Now we are quarantined, but just in a week, there have been 5000 calls to police by women, for domestic violence.
This crisis will be really hard at all levels.
I am afraid that I am very dubious about the origins if this virus being caused by random Gypsies and women protestors or a super spreader as suggested in this article. Chris Martenson, in one of his recent Peak Prosperity videos, mentions that Spain ignored the signs of Coronavirus and went ahead with several big festivals as they brought in a lot of money being so well attended. In fact, they doubled down and put in censorship to keep the story of the virus quiet. I saw one Spanish festival once and can imagine how quickly a virus can spread through them.
I know that this is likely as Oz also did something similar. In the initial stages of the virus, our government was dawdling as so much money came in from the tourist industry and even the visiting ocean liners brought in $1 billion a year. They wanted to rebuild the tourist industry which had been wrecked by the recent bushfires and wasted weeks reacting to the spread of the virus. So from this I can believe that something similar happened in Spain. Spain is paying for this now and according to recent figures, so will Australia.
Yes, we can talk about superspreaders and or “superspreading events” like that funeral. Then you go to one of the pet issues that current opposition is charging against the government. Why the demonstrations were allowed the 8th of march?. The number of casualties were beginning to creep up these days. Yet I see there a lot of “retrospective criticism” from people that did not say a word on this at the moment. Everybody has been surprised by the epidemics and, in the case of Spain, Italy was the warning signal that reduced reaction time. Unfortunately, both Italy and Spain, and I guess many other regions in the world have been reactive and consequently taken by surprise.
This makes sense Ignacio, thank you. I’m just witnessing the take off here (Utah). And in Oregon where my daughter lives. Here in Utah we ignored the initial take off – it was after a Jazz game among other things. The cases since the state went into lockdown (a week ago) have exponentiated. In Summit County from 2 to 50. We had one death yesterday, a patient over 60 who didn’t go to the hospital until he was 3/4 dead and died two days later. So that guy didn’t understand how serious the situation was because the state dithered about lockdown for 3 weeks. I’m afraid the entire nation is going to face this, because Uncle Donald (thank you Mr. Magoo) was in denial, taking sedatives, and acting like Pollyanna.
just now both our doctor appointments called to cancel until further notice… I’m guessing June
Yeah, but blaming a government for not suppressing a demonstration? They always try, and it never works too well.
This shows the cost when governments wantonly blow away political and social “capital”. If people had substantial trust in the government, the demonstrations would not have happened. Without substantial trust in the government, who’s going to believe them when they say that shutting up and dispersing is for the peoples’ own good?
“Honest. You have to stop for medical reasons. You’re hearing it straight from us.”
It’s not all that it may seem at first glance. The womans’ “demonstration” which included 120 000 people in Madrid, led by hard core feminists, was to celebrate world Womens’ Day. They were decked out in the purple colour of Podemos, the far left party led by leftist populist Pablo Iglesias who is the 2IC of Spain’s fragile coalition government. Iglesias was keen to show he was “proud” of Spain’s women. It seems the fragile government had little choice but to acquiesce.
All comments make sense and I accept them without any problem.
Anyway, none of my sisters and female friends went to the demonstration of March 8th, because they are in their 55+, 60s or older. And anyone can tell watching the photos of the demonstrations that there were lots of old woman less that in the last year demontrations,
Even the retired people demonstrating every Monday in Bilbao, decided to stop their demonstrations before the Government. I’m convinced that the Government avoided the quarantine a week before just to avoid prohibiting the March 8th demonstrations.
And yes, Rev, there still were people flying abroad to see soccer matches! C’est la vie!
My understanding is that the CCP is fudging the COVID-19 numbers by a number of means, including documenting its medical complication (such as pneumonia, organ failure, etc.) as the cause of death instead of documenting it as COVID-19 deaths, and not documenting most non-lethal COVID-19 infections.
Honestly I have a hard time believing any numbers from the CCP, considering there is a strong incentive to create the illusion of the CCP has successfully won the war against this disease in China.
And since experts predict a second COVID-19 wave to soon occur in China after lock down restrictions are lifted, the CCP has started to spread the narrative that new cases are now being brought in by travelers from outside China.
I am still shocked that governments outside China have not yet focused much angry against the CCP for allowing the unsafe conditions in their Wuhan wild animal wet market which allowed COVID-19 to mutate from bat to human, and then covering up this pandemic during the critical first 2 months when it could have been easily stopped. Globally the CCP has already cost many thousands of deaths which will likely climb to the millions, and cost many trillions of dollars in economic damage.
You are right. Any analysis based on numbers provided by CCP would be useless – as in garbage in garbage out.
In other words, we should disregard CCP data if we are looking for truth.
If we are really interested in knowing what’s happening in China, then analyse the data from other countries, and use them to estimate the situation in China. And in this case, Spain and Italy would be a good proxy for what is happening in China and Iran.
Different terrain, different people, different cultures, possibly different strains of the virus. Also eagerness to slag China as hate-China is succeeding hate-Russia as organizing political principle in Oceania.
You’re conflating China with the CCP.
I don’t think they are actively faking the figures – independent observers on the ground seem to confirm that the initial worst is over. However, even Chinese media is reporting that the method of calculation they government is using is different from everyone else – quite simply they only count new cases showing symptoms, not positive tests. Many people are still testing positive after being discharged from hospital and Caixin (an official newspaper) is saying that there are several dozen asymptomatic people being identified in Wuhan every day. South Korea counts all such cases.
The country is gradually getting back to normal – most industries are back operating and even public transport is filling up now according to reports I’ve seen. But it remains to be seen if they can prevent further outbreaks. The downside of course of such a sharp effective reaction is that if herd immunity exists, then most Chinese don’t have it yet.
I am surprised that nobody is mentioning the “hairy mammoth in the room”, North Korea! North Korea is releasing their data everyday, and to date, there is no Covid 19 transmission! In fact, no Carona infections, at all!
No infections, no deaths, no crowded ICUs! And this is in spite of sharing a border with China, and lots of back and forth movement?
Can anybody help me figure this out? I am totally flummoxed. It is a mystery wrapped within a mystery………What is there secret? Will they share it with the Leaders of the World?….(sarc)
Wet market means fish, crayfish is the local speciality in Wuhan and very good it is too. Wuhan is surrounded by large lakes and the Yangtze River, so fresh water fish produce, available live to ensure freshness, is very popular in the City. So it’s not a wild animal market by any means and wild animals are not generally sold there.
I am not defending Chinese practises with wild animals by any means, but just because cases were linked to the wet market one shouldn’t necessarily jump to the conclusion that wet market practises were to blame. Just takes one fool, maybe someone making Chinese medicine or something like that.
Thanks for this, very interesting overview. In all the chaos, I do hope that there are people in positions of power making this type of level headed analysis (there seems to be a huge variation between countries).
One factor I’ve heard commented on frequently is cultural differences. At the risk of indulging in cliches, Italians touch each other a lot and socialise in large groups, while, at the other end of the social behavioural scale, the Japanese and nordics do not. I wonder if this is a contributor in the somewhat surprising slow spread of the disease in Japan and some other Asian countries so far (although every Japanese person I’ve talked to says that the government is lying about cases).
I wonder if another factor could be to what extent the elderly and socially vulnerable live apart, or with families.
Just to add something to the confusion – this may be an element with some contradictions in the reporting of disease extent and impact – my niece, a hospital doctor, is saying that they are getting a surprising number of repeat visits from younger sufferers – after initially ‘recovering’ from bad flue symptoms after a few days, they are returning to hospital with chest and respiratory issues.
And another question – I wonder just how accurate some reported death rates really are. There is quite a bit of evidence that some countries such as Thailand have been deliberately or otherwise hiding deaths under ‘viral pneumonia’ or similar.
A lot of returns – my understanding is that the virus makes you bad for 2-3 days, and then a lof o people will have a remission. But after another 2-3 days it returns and is usually way worse than the previous one.
Re deaths – I believe Italy now tests all dead, and reports all who test positive as “CV dead”. I don’t believe that’s the case even for say Germany, and I know it’s not the case for the UK.
CZ had its first “CV death” yesterday. It was 95 year old with massive complications, and the officials said that while he was CV-positive, it was more of a case “died while infected by CV” as opposed “died because infected by CV”.
So as you say, the “deaths” are not a good measure either.
The usual duration of the disease is about 11-14 days after symptom onset in mild cases (no hospitalization required). Regarding those that showed remission of symptoms but then had to revisit the hospital looks like they had a mild upper respiratory track infection that was cleared fast (even before immune response) but the virus had managed to pass to the LRT where the infection progressed. The concentration of viral receptors is higher in the LRT.
It will be difficult to judge whether there’s a benefit going to hospital with mild symptoms, hanging around a long time waiting for service, and meanwhile being exposed to the other vectors in the same area.
Regarding accuracy, it may be the case that some deaths occur without previous or post mortem testing. But then you can say that, in Italy, March, Covid-like symptoms, covid-like progression, covid-like clinical chart, in must be Covid-19. I don’t think accuracy is an issue.
Thank you for the article, most enlightening.
Some thoughts:
The wet market in Wuhan has been a source of just over half the cases in the province, in around 40-45% cases there is no clear source. The Chinese researcher into coronaviruses suspects this source could originated from contamination of food by bat faeces, where food was grown near the caves with bat population. Would it be possible that some people in the province had already been ill without it being recognised as this infection?
Interesting, I didn’t know that. Do you have a source for that?
A recent paper* analysed genomes of the virus from patients, and showed that it most likely had a single origin in the human population. In other words, it most likely only jumped once from animal host to human host. However, after quick glance through the paper I couldn’t find how many genomes they included in their analyses, i.e. did they use all available genomes from Wuhan? If not, they might have missed something.
*) https://www.nature.com/articles/s41591-020-0820-9
summary here:
https://www.sciencedaily.com/releases/2020/03/200317175442.htm
IMO the wet market functioned as a “superspreading event” simply because it is a crowded space with lots of interactions and with closed spaces. The original site of human infection and human to human spread is, to my knowledge, not known. One article suggested that the use of bats in traditional Chinese medicine and the associated commerce of these could be the root cause. So far to my knowledge the closest virus found in bats is Bat coronavirus RatG13 (Pubmed accession number MN996532) from Rhinolophus affinis from Yunnan showing 96% identity in nucleotide sequence with SARS CoV 2
Thank you, Igbacio for this post.
Is it within the range when jumping species to have 96% identity, with one jump?
I would think closer identity, likev99%, but I’m not in that field. Just curious.
Appreciate the 5 plus 19 days guide.
California put in shelter in place on March 20. That makes it April 8. I will be checking around that time. Santa Clara county restricted a bit earlier…not sure by how many days. I dont live there, but maybe they improve sooner.
The 7 Bay area counties enacted shelter in place on March 16. Currently there are cases but we’re not at the point yet where everyone knows a victim. As of today, 321 confirmed cases, but per usual county officials estimate the actual tally is much higher: https://www.mercurynews.com/coronavirus-three-more-deaths-reported-in-santa-clara-county.
Santa Clara is kind of interesting because it seems there are quite a few independent cases rather than a single spreading event. If so I expect the growth rate in SCC might be higher than anything yet seen after a few days.
My family got sick back in late January. At the time I thought it was just a bad cold. Now I can’t help but wonder if it was mild covid-19.
Thank you Ignacio, for the article.
It is helpful to be reminded that a delay in the decline of the outbreak is to be expected. Quarantines and social distancing don’t show results overnight.
I think it is a good choice to look at the fatalities as that is harder to be missed, or supressed.
I propose we see the takeaways for the future (perhaps this coming Fall, who knows) as follows
1 as soon as a novel virus or bacteria is identified anywhere, screening, testing and tracking must begin immediately.
2 as soon as community spread is identified in a population quarantine is recommended
3 with a novel infectious disease, once a region has it under control, to keep it that way, continued screening testing and tracking efforts will be needed untill a vaccine or cure of some sort is available
I would be more confident if I am qualified as Virologist, rather than Epidemiologist. But… we are all now being introduced in the most crude way to the epidemiology of viral respiratory diseases.
Thank you for your post. A twitter thread from an MD and Yale prof, knowledgeable in virology and potential covid immunity post infection and recovery, is here. It’s an unrolled twitter thread so the images don’t load.
https://threadreaderapp.com/thread/1240689935557865472.html
And the longer thread on various aspects of infectious disease transmission, including the unrolled thread linked above.
https://twitter.com/NAChristakis/status/1239204599959093250
Thank you the paper on Covid-19 origin is quite good. Spoiler: not lab origin!
Ignacio, do you have thoughts about Sweden’s response to the pandemic? The Prime Minister gave an address to the nation last night (I didn’t see or hear it but my son did – he lives in southern Sweden) and from what I can gather and from what my son told me, Sweden seems to be continuing it’s herd immunity strategy.
There was an article in the Guardian covering it and the response in Sweden.
https://www.theguardian.com/world/2020/mar/23/swedish-pm-warned-russian-roulette-covid-19-strategy-herd-immunity
Chinese doctors flown to Italy were saying last week that Italy’s quarantine was way too loose. They may have tightened it up since then.
This goes to a polemic which has no easy answer. No one, including chinese doctors, knows what is the precise or desirable tightness of the quarantine and by how much the R0 is reduced given measures taken. In one hand there are some inclined to very tight quarantines, harsh quarantines, that in turn have other social costs. Once the quarantine has started it has to be said that its effects on hospitalization rates wont be noticed until perhaps up to 16 days or so (5 days for incubation and about 11 days for typical hospitalization) and any change in tightness won’t show up in hospitalizations in about a similar period. This means that in, for instance Italy, one could expect that the worst in numbers of hospitalizations is around the corner and might start to ease by the 25th of march. In Spain this might occur by the 30th of march. We will soon see how this unfolds. My personal opinion is that rather than harsh quarantines we should focus on protection of the most vulnerable.
Thanks very much Ignacio for this post and your comments here at NC.
It seems that Iceland has begun doing random sampling. Yesterday the public health agency here in Sweden said that they were going to follow their lead and test “a few thousand” people, which they say will give results in a couple weeks.
‘Thanks very much Ignacio for this post and your comments here at NC’
I would second that sentiment. Ignacio’s comments are always worth paying attention to.
Re: testing – a tidbit of info about UK response, and testing in general
The main type of test being used in UK for COVID-19 is genetic, and based on RT-PCR*, targeting specific virus RNA sequence. I believe this is also the case in other countries, see WHO information leaflet: https://apps.who.int/iris/bitstream/handle/10665/331329/WHO-COVID-19-laboratory-2020.4-eng.pdf
(serological / antibody-based tests should in theory be possible, but I’m not sure how easy those are).
The UK government is setting up a national testing centre in Milton Keynes. Last week, universities** have asked certain laboratory equipment (PCR and RT-PCR machines) to be loaned out for this purpose. On Friday, they were collected and transported with military escort to Milton Keynes.
In addition, a few days earlier, Public Health England have asked for volunteers from the research community to help with the testing effort:
A list of these regional labs is here.
I am not sure what the limiting factor in terms of time, and resources is for the diagnostic tests. Based on the above, there was a lack of PCR machines, and of people doing the wet lab work. Most of the chemicals are fairly straightforward off-the-shelf as they are being used for all kinds of genetic research, so should be easy to repurpose. The only Coronavirus-specific element of the test are the custom DNA primers, which need to be produced synthetically. But again, primer production for custom-designed DNA sequence is a standard run-of-the-mill production process already being used most molecular genetic research on a massive scale, so could presumably be switched rapidly to only produce Coronavirus primers.
As for time, a sample needs to be taken from a person, then RNA isolated, and added with other chemicals to molecular reaction tube, which goes into the PCR machine. According to this paper from January 2020, PCR reaction time is about 45 minutes, but presumably this can be cut down to maybe 25. For some variants of the method, the sample then needs to be run on a gel, which adds another 15-30 minutes. So, assuming perfectly organised sampling and logistic procedures, and testing in parallel, the shortest I envision this to take would be 40 minutes in total.
Does anyone know good sources of the ‘ten minutes tests’ I heard about from Korea? Perhaps they use a different procedure.
Finally, I wholeheartedly agree with the author that a portion of the testing capacity should be set aside for testing random samples across the population. That’s the only way to track the progress and geographical spread of the epidemic, including better estimates of key parameters (R0, mortality, etc).
—
*) Real Time or Reverse Transcription Polymerase Chain Reaction. This molecular technique tests for the presence of a particular RNA sequence in a sample (from nose or throat), in this case specific to the Coronavirus (and different from other viruses). Which exact RNA sequence to target is based on publicly available RNA sequence data from early patients in China. Such info is accessible in public databases (e.g. here: https://www.ncbi.nlm.nih.gov/nuccore/1798174254) which has been extended with sequencing of many more patients, in order to track mutations and estimate geographic distribution. A nice visualisation is here, https://nextstrain.org/ncov but make sure to read the caveats about geographic distribution.
In addition to diagnostic testing via RT-PCR, research universities** are also using DNA sequencing centres and laboratories to sequence the virus from as many patients / locations as possible (and have cancelled all other research).
**) My data point is one Russell Group university, but presumably this has happened across other research universities as well.
Forgot to add: the PCR reactions can be done in a massively parallel fashion. A single PCR machine can run 96, 192 or 384 samples at a time. So the average per-sample processing time may well be cut down significantly.
I don’ t know about the 10 min tests, most I heard were abut 30-40 mins.
I’dd add one thing to the above – the tests can be made so that they don’t need any real equipment to find positive/negative, as the chain reaction can be set to change the colour of the sample.
The real problem with RT-PCR tests is that because it’s a chain reaction test, it’s incredibly sensitive (in theory it can detect a single molecule of the relevant RNA sequence), and even the most trivial contamination of the sample can lead to false positives. This is often done by selecting more than one RNA sequences from the sample, and a hope that the cross-contamination won’t get all bits there, but say if you sample is handed by someone CV-positive, then it doesn’t matter.
Similarly as wrong reactants can lead to an entirely worthless test.
>The real problem with RT-PCR tests is that because it’s a chain reaction test, it’s incredibly sensitive (in theory it can detect a single molecule of the relevant RNA sequence), and even the most trivial contamination of the sample can lead to false positives. This is often done by selecting more than one RNA sequences from the sample, and a hope that the cross-contamination won’t get all bits there, but say if you sample is handed by someone CV-positive, then it doesn’t matter.
True. When I was doing lots of these (years ago, in a non-clinical setting), best practice was to include (on each 96 or 384 well plate) positive and negative controls, as well as a dilution series of a positive control (1:10, 1:100, 1:1000 etc). I suppose that including a sample of the lab person doing the test could also help.
Real time PCR is quantitative, so not just yes/no positive; it measures the relative concentration of the original RNA molecules. So a contamination with a few molecules would show up as a low-level positive, but not sure what the cut-off would be to distinguish from true positives.
Real time PCR data are monitored in real time on a computer (not on gel), read out optically from the plate using a fluorescent dye (e.g. SYBR Green) that binds to the PCR product, and whose fluorescence is a measure of PCR product concentration, which in turn is a measure of concentration of original virus RNA. A positive sample with high viral load will show up quickly, as the (exponential) curve of fluorescence will start to increase early.
Ten minute tests are serological tests. There are two types of serological tests: those that detect viral particles using anti-SARS Igs or those that detect immunological response and detect anti-SARS Igs. The latter are useful to analyse retrospectively the reach of the epidemics. These could show how many non-diagnosed individuals passed the disease. Real-time PCR testing needs sophisticated equipment and about 1 hour or less for results. Serological tests are much easier to deploy.
My understanding is that if you don’t really want quantitative data beyond a cut-off, then RT-PCR can be quite simple to deploy – but your propert test sensitivity gets quite worse because of potential sample contamination.
Anyways, many thanks for the post!
Thanks, that’s very interesting.
here are two types of serological tests: those that detect viral particles using anti-SARS Igs or those that detect immunological response and detect anti-SARS Igs. The latter are useful to analyse retrospectively the reach of the epidemics. These could show how many non-diagnosed individuals passed the disease.
Might it also show who HAD the disease but has now RECOVERED, and thus now has an immunity for some period of time? It would be useful to know who is now immune, cannot pass the disease on, and could return to work (maybe with something like a wristband a ‘passport’). imo.
I’ve been told here in Ireland from a hospital doctor that there is a 3 day lag in getting results – the bottleneck is the lab capacity – plenty of kits, just not enough lab personnel to do the work.
Korea has point of care antibody tests. US federal government is behind, which seems like a familiar pattern.
https://www.caltech.edu/about/news/tip-iceberg-virologist-david-ho-bs-74-speaks-about-covid-19
That’s very interesting. Is it specific for COVID-19, or does it measure a general immune response?
In the US I often hear that a shortage of “reagents” is the bottleneck in ramping up testing. I don’t know what reagents are. Would they perhaps be the DNA Primers of which you speak?
DNA primers are easily synthetised in amounts that allow for many tests. It could be that the reagents used to label the primers (and allow to measure their incorporation into DNA molecules during PCR) are in short supply.
Biologist, do you have a link for the call for volunteers? My wife is a biomedical scientist working out of a research company in Cambridgeshire, within commuting distance of the East of England PHE regional lab in Cambridge. Work has pretty much closed down in her laboratory because of the crisis, and so there are some very highly qualified research scientists with the right skills sitting and twiddling their thumbs at home who would jump at the chance to do something useful. That link would be a real help, if you have it. Thanks!
I don’t have a link, unfortunately, but I’m happy to forward you the emails if you want (not sure how to communicate privately through this site though).
These emails came from my research university, and it seems the effort is coordinated via research institutions / universities, for instance the Crick in London.
Perhaps your wife (or the management at her company) can contact the PHE regional lab and organise the volunteers from their company? Perhaps she has contacts at the Sanger or the University of Cambridge?
There’s also a new consortium that will sequence thousands of samples:
https://www.cam.ac.uk/research/news/cambridge-to-spearhead-ps20million-alliance-to-map-spread-of-covid-19-coronavirus
This article reports on testing in UK as well, read the end especially:
https://www.wired.co.uk/article/coronavirus-uk-testing-key-workers
Thank you, Ignacio. This does a great deal to clear up my understanding of the epidemic, and to simplify my thinking about it. What the US curve will look like next to these, I am afraid to find out …
Thank you Iganacio; well argued and documented. I particularly like point 3, once under control, […]continued scrreening testing and tracking efforts will be needed until a vaccine or cure of some sort is available.
In such a careful and specific focus, a great deal must be left unsaid, such as the political will and material and medical resources, economic conditions and how (the limits of a) global manufacturing structure fits in needed to support such measures, but your report makes it easier to logically move up and examine that chain of requirements.
Opps, sorry, wrong list, (just got up) though @thoughtfulperson’s list is indeed worthy of mention as well. Nevertheless, my point remains valid, your report breaks things down well and makes the larger issues involved clearer for analysis of approaches to be taken and weaknesses therein.
Thank you, Ignacio.
I wonder if the following fact could find a place in the analysis.
AFAIK until now the area where Covid hit more hardly in Italy has been the Bergamo province.
Some days ago a head physician’s hypothesis arrived to the Italian MSM : Feb 19, a few days before the start of the first lockdown measures, 45,000 Bergamo’s Atalanta soccer team supporters gathered in the stadium to see Atalanta against Valencia, and all the other supporters by the way gathered in homes , pubs, etc, then everybody celebrated for the Atalanta win. It’s been reported as well that a good number of Valencia players tested positive after the match.What maybe is missing to the picture is that I hardly believe that antihooliganism measures were so efficient to avoid any contact between the two teams’ supporters.
This indeed accelerated the epidemics in both countries. Many cases in Valencia associated with this event.
I understand that most people are concerned with the current state of affairs, but I guess that others have started to plan for the future
Governments world wide will appreciate this crisis for one in which ideal conditions – as far as it is possible to judge nearly every country and their population are passive dependent panicked and submissive – allow the development and testing of a variety of martial laws and surveillance systems a general re ordering of jurisprudence and judicial procedures, the further slicing and sectioning of the public according to a ‘indisputable’ new set of priorities into a new slew of sub groups, essential less essential etc : the re invention of a caste system
(let alone an ideal opportunity for careful re evaluation of the weaknesses on display country to country and the re configuration of war plans)
It looks like the Chinese government did contain to a certain extent did contain the virus, at the cost of a two months general shut down of society and the economy
Presumably with investment and more careful preparation (general hospital testing etc of the whole population twice a year, indefinitely, permanent and mandatory iphone ‘bug detector’ apps and tracking in real time) the outbreaks will be confined to a narrower spread and be shorter in length, perhaps one month no more and only regional shut downs, curfews and martial laws
This program to be adopted in every country – some may be able to afford and operate these large scale investments, many more will require massive inflows of capital and expertise and infrastructure, a form of re colonisation papered over as a new ‘alliance’
Or maybe the world wide consensus, to be formed by a new International Organisation perhaps, will decide that this program although laudable, must take second place to the combat climate change program, or indeed another
Or who knows there are those who claim that what appears already to be a recurring virus, or family of, can be prevented ‘with the right technology’ from occurring in the future, so obviate the need for future combat infrastructure
Or perhaps it may be possible to live with this virus and it’s future derivatives without having every time to fight them to the death ?
How can this be imagined possible ? Or why should it be more difficult to imagine this than any of the scenarios sketched above ?
If it is impossible for humans to get cleverer about their health, why assume or plan or hope that viruses will stay as relatively benign as this current one ? What does planning for the worst involve ? or is this impossible to imagine outside of full hazmat fantasies
Surely the current situation could be easily made much worse next time round
Another variable is Italy’s reporting system for deaths, which differs from other countries according to a Canadian Broadcasting Corporation (CBC Radio 1) report I heard yesterday. It stated that Italy records ALL deaths at hospitals with corona virus cases as corona virus, even if there are underlying conditions. This could be inflating the reported numbers, relative to places that don’t have the same criteria.
Ignacio, do you have any comment on the German experience so far. Their case fatality rate (0.3%) seems astoundingly low. They have more medical resources and a lower old age demographic, and don’t test post mortem, reasons offered for the contrast with Italy (9%). And they test a lot more than anywhere else in Europe.
This is one of the reasons I don’t look at number of confirmed cases. In each country there are different guidelines for testing that result in such large differences. Germany is testing much more than other European countries but they have not managed to contain the disease. They saw an early cluster in Bavaria and managed to control it. When the outburst was evident in Italy, new clusters were identified in Germany and not all could be traced to Italy. Following the number of casualties one can conclude that the epidemics in Germany has not been effectively confined but progressing in a relative slow motion. They still go with containment measures (meetings forbidden) but have not declared general quarantines. I guess they will continue to see the disease creeping up in a somehow slow motion. They are following the advice of Robert Koch Institute. Whether this strategy is working or will result in a larger outbreak later is something we will see. Such strategy must rely on Germans strictly taking all possible precautions while still trying to go on with their normal activities.
If you compare Switzerland and Austria, there is also a large difference and the epidemics is progressing much faster in Switzerland. Why? More international contact (more initial clusters)? A superspreading event?
Thank you for an interesting analysis, Ignacio. Might you comment on how the situation would progress, please? It is unlikely that herd immunity would be achieved after an intial lock-down. Thus, I’d expect a new ‘outbreak’ to start some time after a general quarantine is relaxed, especially given the presence of super spreaders and those with mild or no symptoms in a population where a majority of people might still have no immunity. I’d guess these repreated outbreaks to continue until some general level of immunity is established in the population. Do you think the population of China has now achieved herd immunity? What percentage of the population might now be immune?
Another question – at what point to relax a general quarantine to avoid catastrophic damage to the economy and also avoid a resurgent increase in the number of afflicted that would overwhelm the health care system?
If BBC is to be believed, CV19 cases are clocking up in earnest in Middle East and Africa. As of today,
Saudi and Qatar -500 cases each,
Egypt and Algeria – 300 each,
Somalia and Ethiopia – 150 each,
Nigeria, Burkina Faso, DR Congo, Kenya, Angola, Bangladesh -50 each.
For comparison, UK had 50 cases some fifteen days ago (time flies doesn’t it),
Given that reported cases are less than a tenth of real time figure, the way medical practices get implemented in those places, their governments ability (intellectually and physically) to prescribe suppressing measures, their citizens ability to adhere to such measures, I suspect that we will be witnessing events of an order of magnitude grimmer that what befell Chinese and Italians and Spaniards, in less than a month.
This article https://medium.com/@tomaspueyo/coronavirus-the-hammer-and-the-dance-be9337092b56 has very good information about the likely outcomes depending on which policies a country adopts. Let’s hope it’s not too late for most countries to make the right decision.