Yves here. It is disturbing to watch the push to con the public into seeing remdesivir as the only promising treatment for coronavirus. Please circulate this post widely to inform people you know that established, lower cost drugs also show promise.
By Nevan Krogan, Professor and Director of Quantitative Biosciences Institute & Senior Investigator at the Gladstone Institutes, University of California, San Francisco. Originally published at The Conversation
The more researchers know about how the coronavirus attaches, invades and hijacks human cells, the more effective the search for drugs to fight it. That was the idea my colleagues and I hoped to be true when we began building a map of the coronavirus two months ago. The map shows all of the coronavirus proteins and all of the proteins found in the human body that those viral proteins could interact with.
In theory, any intersection on the map between viral and human proteins is a place where drugs could fight the coronavirus. But instead of trying to develop new drugs to work on these points of interaction, we turned to the more than 2,000 unique drugs already approved by the FDA for human use. We believed that somewhere on this long list would be a few drugs or compounds that interact with the very same human proteins as the coronavirus.
We were right.
Our multidisciplinary team of researchers at the University of California, San Francisco, called the QCRG, identified 69 existing drugs and compounds with potential to treat COVID-19. A month ago, we began shipping boxes of these drugs off to Institut Pasteur in Paris and Mount Sinai in New York to see if they do in fact fight the coronavirus.
In the last four weeks, we have tested 47 of these drugs and compounds in the lab against live coronavirus. I’m happy to report we’ve identified some strong treatment leads and identified two separate mechanisms for how these drugs affect SARS-CoV-2 infection. Our findings were published on April 30 in the journal Nature.
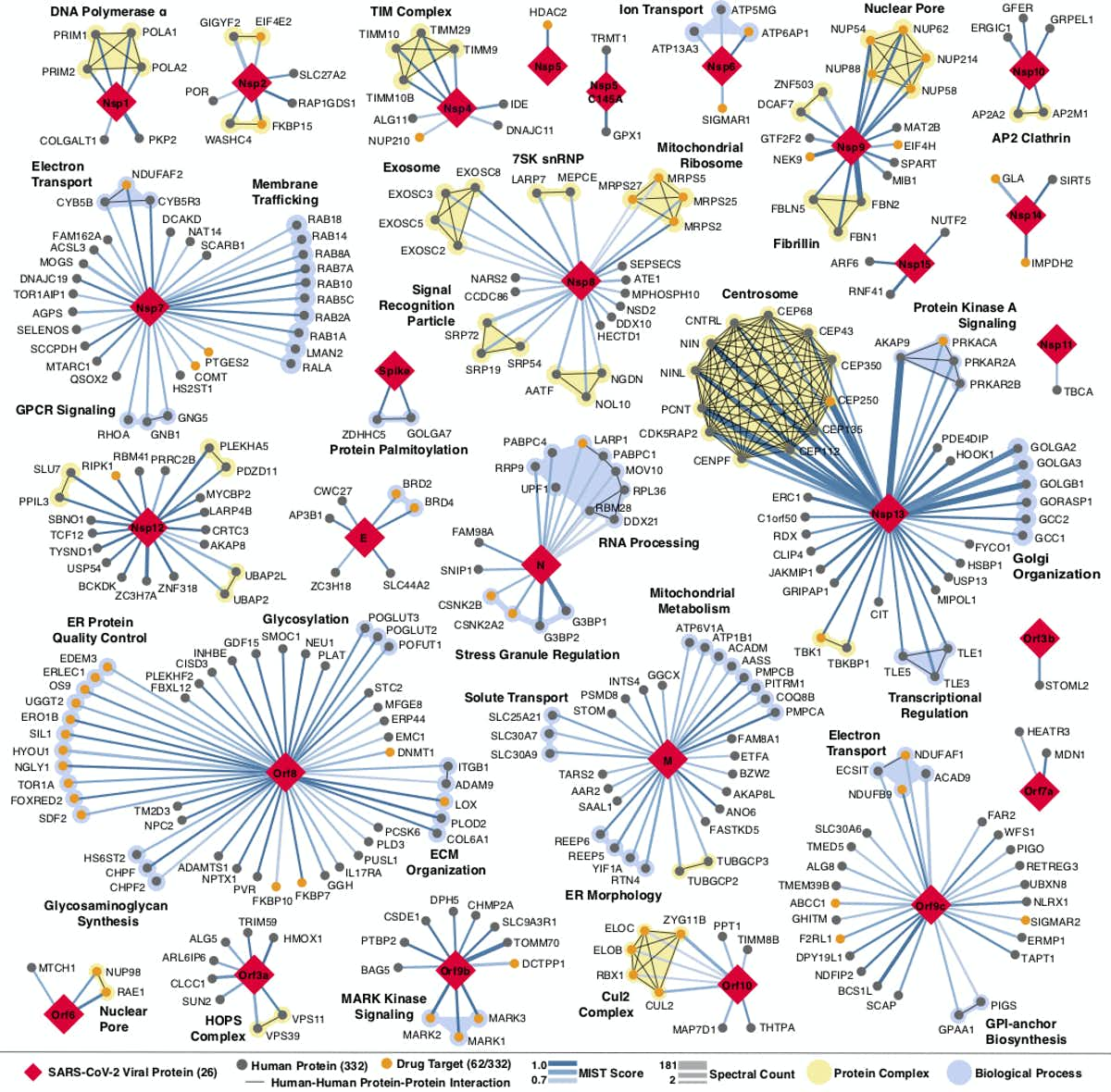
Every place that a coronavirus protein interacts with a human protein is a potential druggable site. QBI Coronavirus Research Group, CC BY-ND
The Testing Process
The map we developed and the FDA drug catalog we screened it against showed that there were potential interactions between the virus, human cells and existing drugs or compounds. But we didn’t know whether the drugs we identified would make a person more resistant to the virus, more susceptible or do anything at all.
To find those answers we needed three things: the drugs, live virus and cells in which to test them. It would be optimal to test the drugs in infected human cells. However, scientists don’t yet know which human cells work best for studying the coronavirus in the laboratory. Instead we used African green monkey cells, which are frequently used in place of human cells to test antiviral drugs. They can be readily infected with the coronavirus and respond to drugs very closely to the way human cells do.
After infecting these monkey cells with live virus, our partners in Paris and New York added the drugs we identified to half and kept the other half as controls. They then measured the amount of virus in the samples and the number of cells that were alive. If the samples with drugs had a lower virus count and more cells alive compared to the control, that would suggest the drugs disrupt viral replication. The teams were also looking to see how toxic the drugs were to the cells.
With dozens of drugs each needing full testing, to get results in four weeks required round-the-clock effort. Quantitative Biosciences Institute, CC BY-ND
After sorting through the results of hundreds of experiments using 47 of the predicted drugs, it seems our interaction predictions were correct. Some of the drugs do in fact work to fight the coronavirus, while others make cells more susceptible to infection.
It is incredibly important to remember that these are preliminary findings and have not been tested in people. No one should go out and buy these drugs.
But the results are interesting for two reasons. Not only did we find individual drugs that look promising to fight the coronavirus or may make people more susceptible to it; we know, at a cellular level, why this is happening.
We identified two groups of drugs that affect the virus and they do it two different ways, one of which has never been described.
Disrupting Translation
At a basic level, viruses spread by entering a cell, hijacking some of the cell’s machinery and using it to make more copies of the virus. These new viruses then go on to infect other cells. One step of this process involves the cell making new viral proteins out of viral RNA. This is called translation.
When going through the map, we noticed that several viral proteins interacted with human proteins involved in translation and a number of drugs interacted with these proteins. After testing them, we found two compounds that disrupt the translation of the virus.
The two compounds are called ternatin-4 and zotatifin. Both of these are currently used to treat multiple myeloma and seem to fight COVID-19 by binding to and inhibiting proteins in the cell that are needed for translation.
Plitidepsin is a similar molecule to ternatin-4 and is currently undergoing a clinical trial to treat COVID-19. The second drug, zotatifin, hits a different protein involved in translation. We are working with the CEO of the company that produces it to get it into clinical trials as soon as possible.
Sigma Receptors
The second group of drugs we identified work in an entirely different way.
Cell receptors are found both inside of and on the surface of all cells. They act like specialized switches. When a specific molecule binds to a specific receptor, this tells a cell to do a specific task. Viruses often use receptors to infect cells.
Our original map identified two promising MV cell receptors for drug treatments, SigmaR1 and SigmaR2. Testing confirmed our suspicions.
We identified seven drugs or molecules that interact with these receptors. Two antipsychotics, haloperidol and melperone, which are used to treat schizophrenia, showed antiviral activity against SARS-CoV-2. Two potent antihistamines, clemastine and cloperastine, also displayed antiviral activity, as did the compound PB28 and the female hormone progesterone.
Remember, all these interactions have so far only been observed in monkey cells in petri dishes.
At this time we do not know exactly how the viral proteins manipulate the SigmaR1 and SigmaR2 receptors. We think the virus uses these receptors to help make copies of itself, so decreasing their activity likely inhibits replication and reduces infection.
Interestingly, a seventh compound – an ingredient commonly found in cough suppressants, called dextromethorphan – does the opposite: Its presence helps the virus. When our partners tested infected cells with this compound, the virus was able to replicate more easily, and more cells died.
This is potentially a very important finding, but, and I cannot stress this enough, more tests are needed to determine if cough syrup with this ingredient should be avoided by someone who has COVID-19.
All these findings, while exciting, need to undergo clinical trials before the FDA or anyone else should conclude whether to take or stop taking any of these drugs in response to COVID-19. Neither people nor policymakers nor media outlets should panic and jump to conclusions.
Another interesting thing to note is that hydroxychloroquine – the controversial drug that has shown mixed results in treating COVID-19 – also binds to the SigmaR1 and SigmaR2 receptors. But based on our experiments in both labs, we do not think hydroxychloroquine binds to them efficiently.
Researchers have long known that hydroxychloroquine easily binds to receptors in the heart and can cause damage. Because of these differences in binding tendencies, we don’t think hydroxychloroquine is a reliable treatment. Ongoing clinical trials should soon clarify these unknowns.
Treatment Sooner Rather Than Later
Our idea was that by better understanding how the coronavirus and human bodies interact, we could find treatments among the thousands of drugs and compounds that already exist.
Our idea worked. We not only found multiple drugs that might fight SARS-CoV-2, we learned how and why.
But that is not the only thing to be excited about. These same proteins that SARS-CoV-2 uses to infect and replicate in human cells and that are targeted by these drugs are also hijacked by related coronaviruses SARS-1 and MERS. So if any of these drugs do work, they will likely be effective against COVID-22, COVID-24 or any future iterations of COVID that may emerge.
Are these promising leads going to have any effect?
The next step is to test these drugs in human trials. We have already started this process and through these trials researchers will examine important factors such as dosage, toxicity and potential beneficial or harmful interactions within the context of COVID-19.


Remdesivir news stories on the MSM! How promising! Fauci calls it “the standard of care” for Covid-19!
How corrupt. Flipping coordinated marketing campaign, as you say Yves, a “con”, what a damn gang of gangsters occupy power positions in the imperial parasite.
Incidentally, on the topic of greedy gangsters, in Canada, when interest rates went down, peoples’ HELOC credit line rates went down in lockstep – from 4.95% to 3.45%. Did this happen in the US of A? Not so much, from my experience – what have others seen?
After backing gain-of-function research in bat coronaviruses at the Wuhan lab, it’s very clever for Fauci to be a promoter of Remvesidir. He offers us both a problem and a solution. Such a good man. (https://www.newsweek.com/dr-fauci-backed-controversial-wuhan-lab-millions-us-dollars-risky-coronavirus-research-1500741)
Maybe Fauci likes it because he is financially linked to it? It’s more $ than hydroxychloroquine, both come w/ questions. That stated, I would take any of them if I needed to.
Still early days, but this is how researchers step up. Thank you for posting.
Here is a pretty good thread on how unlikely Remdesivir’s was in the first place, and how Gilead positioned it for promotion.
https://twitter.com/MarkHoofnagle/status/1256242036015063042
+1.
+2 Thanks a lot for this article with much meat on it to take a look.
I can actually cite a relevant case of a well financed and marketed effort being promoted in lieu of repurposing a cheaper already tested pharmaceutical. I had the privilege to work with the dedicated clinicians and researchers of the Boston University School of Medicine Amyloid Treatment and Research Center. They proposed repurposing a cheap NSAID (diflunisal) for treatment of hereditary Transthyretin Amyloidosis. Diflunisal was already on the market. A limited trial showed effectiveness. However, they were competing for aa small pool of potential trial participants with a well-financed company trying to develop and market a very expensive drug (tafamidis) that worked on a similar principle than diflunisal. A very difficult endeavour. I don’t think diflunisal was ever properly tested and tafamidis is on the market. I don’t know the whole story since I changed jobs during the whole affair.
oops. Correction. Should read “…expensive drug (tafamidis) that worked on a principle similar to diflunisal
Veblen’s idea that business sabotages industry.
It is interesting to note that Donald Rumsfeld was part owner/director of Gilead Sciences. It’s probably not a simple ‘coincidence’. I hope the truth is dared to be told by main stream media one day. Before it’s too late
for millions of humans at the mercy of the ‘experts’ who put their personal gains first.
Gilead produced Harvoni treatment for Hepatitis C. Saved my life. Strange to thank Don Rumsfeld for something.
I feel bad for the people who are currently dependent on those drugs. If one or more are successful in human trials, will the price not go through the roof (after what ever shenanigans to get and/or enforce a patent are implemented of course)?
> If one or more are successful in human trials, will the price not go through the roof
Don’t worry. People will be given “access.”
I would just like to point out the depressing reality that the researchers involved in this, and potentially the sites that report on it and in theory even nature magazine, all stand to have their social media accounts closed by tech platforms and search results delisted for spreading what is deemed by by officialdom/commentariat-consensus to be ‘misinformation’.
Big tech breakup when?
They have recognized places to publish their work. Twitter isn’t the place for this.
Yeah Twitter is not the route for FDA validation!
It works for Trump. Why not actual scientists?
I think the key messaging is that there are promising drugs out there but don’t believe the hype from certain podiums regarding certain teatments.
This type of information dissemination is useful to know that there could be a light at the end of the tunnel and it may not be an oncoming train. Part of my planning on social distancing and overall decision-making on activities over the next couple of years are potential timelines for doctors being able to treat this disease, vaccinations, or responsible government and corporate actions. I think the first one may be greatly improved by Labor Day, a vaccine might show up in 2021, but in general I have given up on responsible actions from most governments, especially federal, and many corporations.
Andy Grove wrote his leadership manual “Only the Paranoid Survive” over 20 years ago and both the title and content are very applicable today.
> Twitter isn’t the place for this.
I disagree. There are plenty of verticals that do very well on Twitter. In fact, the general public would not be apprised of #COVID19 advances were it not for Twitter. Which doesn’t imply that [glass bowls, this is a family blog] won’t ruin it for the rest of us.
Jeff Leek of the blog “Simply Statistics” writes:
” As a biostatistician at a very visible school of public health I have also had a number of media outreaches, but I’ve been hesitant to do any interviews or talk about COVID-19. The reason is that even thought I have a PhD in Biostatistics and I work in a School of Public Health I actually know very little about infectious disease modeling and response. I think if you aren’t really deep in the field, its difficult to know the difference between someone like me and someone with real expertise.”
And he goes on to post a “…brief list of people and organizations I find credible and have been following for good information in case it is helpful to others.”
https://simplystatistics.org/2020/04/29/amplifying-people-i-trust-on-covid-19/
Thank you, now I am following Derek Lowe (referenced by Leek) and his takes in vaccine development.
And D. Lowe on Remdesivir:
Not too promising indeed.
Excellent info. Thanks
Somebody sure has the hots for Remdesivir. Is it because it costs about a grand a dose? I read this morning that five hospitals here in Oz are going to receive it. Why, I have no idea because we are now down to only about 900 cases of which only 28 are regarded as serious. Would it not be better to conduct these trials where it can do more good? Places like New York, New Jersey, Michigan or Massachusetts? The need is certainly there-
https://www.theguardian.com/australia-news/2020/may/01/remdesivir-five-australian-hospitals-to-receive-experimental-coronavirus-drug
Gilead was part of Herr rumsfeld’s pension plan.
I remember tamiflu not really coming to the rescue (extra portfolio) in the last crisis.
I wonder what they have up their sleeve for the next one.
Looks like Japan is fast-tracking testing of this drug as well-
https://www.news.com.au/world/breaking-news/japan-to-fasttrack-coronavirus-drug/news-story/5d8cb480daf65607ab0471a15bf1f393
If you look at the annual reports of any of these zombie corporations, they have M&A driven by debt written all over them. The tech industry was never about development and always about control. The response to the virus was to separate people and insert technology in the middle, same old.
No one under 50 should have lost their job or their business.
(We sell those F35s for billions and can take them out of the sky for $5. That’s a feature)
Having achieved over 50, I’ve learned to be suspicious of any ‘problem’ whose only ‘solution’ is austerity for the working class.
My nomination for the article’s most revealing phrase:
a potential druggable site
That could be viewed as hopeful, to find cures and relieve further suffering, while also seen as indicating further investment, and to a subset of the audience as phenomenally lucrative, too.
Now that finance people are on record about cures not being good for business model sustainability, can pharma’s own version of product path dependency and cash flow stay out of the shadows any longer?
Great post. Encouraging for a number of reasons. I did want to highlight this part, in case anyone missed it:
Another interesting thing to note is that hydroxychloroquine – the controversial drug that has shown mixed results in treating COVID-19 – also binds to the SigmaR1 and SigmaR2 receptors. But based on our experiments in both labs, we do not think hydroxychloroquine binds to them efficiently.
Researchers have long known that hydroxychloroquine easily binds to receptors in the heart and can cause damage. Because of these differences in binding tendencies, we don’t think hydroxychloroquine is a reliable treatment. Ongoing clinical trials should soon clarify these unknowns.
I do remember a successful Chinese study that was done where they de-selected any patient that had a history of heart trouble because they were aware of the problems that could arise. I do not see any mention of zinc used in conjunction with hydroxychloroquine here which I wonder about. One US study said that it was useless but instead of using it at the beginning when the virus was just starting to take off and it was most effective, they were giving it to patients who were totally crushed by this virus so was of no benefit. Am I a hydroxychloroquine advocate? Nope. All I am saying is that they should be doing proper studies and then have them peer-reviewed to see what works.
Yes. Anyone looking at the chart above should realize that all of this is quite complicated to the Nth power. Each one of those nodes is a protein with probably hundreds of amino acids that fold up in a specific way, and have a 3D shape that is difficult to predict. Add on to that glycosylation, phosphorylation and other post translational modification and you have the shape of the thing. From form follows function. Drugs stick to cavities in the surface of the protein. If you stick to the right spot that changes the shape of the protein enough that it blocks the binding of the viral protein then you stand a chance of stopping or at least greatly slowing viral replication. The immune system will do the rest.
Many scientists will devote years or decades to the study of individual proteins and their role in the body. There are hundreds here. It will take the systematic effort from tens of thousands, in the hope that one or two will get lucky and have the stars line up in their favor with a good tailwind and the right people and instruments in the right places at the right time (with funding!) and all the biological facts on their side to arrive at a solution, but they will find one, probably.
Rather than spend trillions bailing out small or rather in practice large business, we could do more to help ourselves by providing emergency funding for the NIH and some fast track granting. Unlike business men with a fiduciary responsibility to pocket the cash and use it to reward shareholders, scientists will use the funds to do more research. Even if the money doesn’t go to coronavirus it will go to advancing human knowledge in some form — that is what they do — and leave us in a better position to handle this and future epidemics. It will also cost a tiny fraction.
Jobs are a bandaid. A cure is a solution. If you can use MMT to bail out our billionaires and mega banks, imagine what it will do for research.
One US study said that it was useless but instead of using it at the beginning when the virus was just starting to take off and it was most effective, they were giving it to patients who were totally crushed by this virus so was of no benefit.
Because there’s still not an agreed and properly tested with clinical trials treatment (imo) for Covid-19 yet, I’ll add this story (anecdotal evidence ) from Texas about early treatment with hydroxychloroquine. This is a Fox news story; at this point I’m listening to all news sources for information. Note that the doc in charge checked everyone’s heart daily with an ekg while administering the hydroxychloroquine, Zpac and Zinc treatment.
https://www.fox7austin.com/news/fox-26-gets-unprecedented-access-to-texas-1st-nursing-home-to-treat-covid-19-with-hydroxychloroquine
Very good article, thank you.
The federal government does not have to “negotiate” with a drug company CEO.
Just seize the company, make just compensation for its prior value, and go.
Any fear of that is the result of utterly corrupt government officials.
Re: “…its disturbing to watch the push to con the public into seeing remdesivir as the only promising treatment for coronavirus”
It that how you see it? a political con job? Wow.
The most important distinction to make about this post (which the author does) is the difference between in vitro testing and highly replicated double blind tests in humans. There are available drugs that might inhibit viral replication by, say, blocking protein translation (e.g. in text). Great results for the test with monkey cells in a test tube, but generally you don’t want to shut down all protein synthesis in the body. Ideally it needs to be specific for viral infection and replication. The drug might have been developed for patients with multiple myeloma at some dose (dosage is another important distinction that the author does not disclose), or may have become relegated to ‘experimental or compassionate use only’ after failing phase 1 tests in humans. New therapeutic development starts with testing drugs already developed before spending tons of dollars and time on discovery of new treatments. I’m sure some of these other candidates that show promise in in vitro tests will move into animal model tests and phase 1 tests in humans with time. I don’t see it as a con or a conspiracy by big pharma elites to profit off of remdesivir. When the entire public as some mortal stake in the development of therapeutics and vaccine I’d say the process is very likely to be transparent. Nobody is going to let granny be part of an experiment.
If you want an example of a big pharma con look at the negligent oversight and corrupt marketing promotion of Vioxx in the late 1990s.
there is a study on remdesivir at UC Davis a friend recently participated in. 20 patients on a 10 day study. she credits it with saving her life. her husband passed from covid-19 a few days before she began the treatment.
Women less likely to die than men. Over 3/4 of the people who get severe cases survive. And the study found that remdesivir made no difference in mortality.
Yves,
thank you for the info and response. that makes sense. she’s very religious so i’m gonna keep this to myself tho :) appreciate you.
It seems clear that this is not, not any kind of a miracle drug. I don’t see/hear anyone in the medical hierarchy, including Fauci saying that but I do see a lot people saying he said it. It’s a standard of care for people who are really, really sick. Full stop.
Yeah not so much.
(from dk’s link to Mark Hoofnagle)
Thanks, that’s quite a thread with much information.
> It’s a standard of care for people
It’s not a “standard of care.” Fauci doesn’t get to make that call, as an individual, and especially not based on a press release and data nobody else has seen. Worse, Fauci is implying that you can get sued if you don’t use remdesivir. Fauci’s behavior really stinks. Sadly, the liberal Faucigasm was all for naught, just like the liberal Cuomogasm…
I can’t really agree with Dr Fauci. Just saying that Remdesivir is the
“Standard of Care” does not make it so.
There are many clinicians around the world that are having
very good results with Hydroxychloroquine and Azithromycin.
This is another example of that.
https://aapsonline.org/hcq-90-percent-chance/
I find it abhorant that the medical community and the government are allowing
this grifting to happen while tens of thousands are dying. Remdesivir results haven’t been
even published and they are declaring it the “standard of care”, give me a break. This has been
in planning since they started ramping production of Remdesivir earlier in the year.
> This has been in planning since they started ramping production of Remdesivir earlier in the year.
To be fair, setting up parallel production lines hoping that one pans out seems like the right approach. Nevertheless, it is an enormous subsidy for Big Pharma.
Pharma companies all over the world have been ramping up on all sorts of drugs and vaccines related to the virus. Two reasons. A hope to cure the world, and money.
As more anecdotal stories about successful use of hcq + in the early stage of the disease are appearing, the Feds go after one doctor early to use the treatment in the US and publicize his results in an interview with Rudy Giuliani. I agree with a ‘don’t make false claims’ argument, but where is the data and the test results for remdisavir that’s being touted by Fauci and govt??
Doctor Who Promoted Malarial Drug Draws Scrutiny of Federal Prosectors
In an interview, Dr. Vladimir Zelenko said he was guilty of nothing more than sloppy wording.
https://www.nytimes.com/2020/05/01/us/coronavirus-doctor-zelenko-malaria-drug.html
The off label use of Plaquenil + zpak is useful for less severe patients, but not a standard of care. It is optional and not backed by science.
I’m a recently retired internist, and I gave my wife the above, and within 2 hours her supplemental O2 needs dropped by 50%!
But Remdesivir now has some good studies to back up its medical efficacy. It seems to reduce the duration of hospitalization with severe patients by one third. Not a home run, but a very big deal! And if further trials and the tincture of time continue to back up that claim, then it will become a standard of care for these select patients. Actually with the incredibly accelerated tract of accumulated medical information related to our virus, the drug is about already a standard.
Perhaps more hopeful, a study at Queen Elizabeth Hospital Foundation Trust mentioned on this discussion at 2:10 showed that people with normal Vit D levels (30microgr/mL) did not develop symptoms requiring hospitalization. Ditto for people with normal Vit C levels. The video shows the front page of an article about the Vit D study. It might be possible to find out more there.
Another Doctor (Mary Helen Hensley, Doctor of Chiropractic) mentioned that a major factor in how the virus affects people differently was the pre-existing degree of cumulative acidity in their body. This could also account for why older people were more likely to be hit harder–their bodies had accumulated oxidative stress from a range of sources (exposure to chemicals, wrong foods, stressful life events). She emphasized that people who might look “healthy” from the outside (not overweight, excellent physical condition, plenty of exercise, good diet) could be carrying a highly acidic load that is not visible from the outside, if they have a stressful lifestyle, relationships, thought patterns, etc. She recommended detoxing and especially examining the stress factors–i.e., it’s not just about food or toxins.
Your first graph mentioned normal levels of Vitamin D. That means staying inside is contrary to what a person would like to do, staying away from sunshine. Public policy doesn’t gibe with best practice here.
Another view of the snake oil show that is the Remdesivir Rollout.
Talk about regulatory capture, Wall Street has nothing on Big Pharma.
Fauci has peddled this as the “Standard of Care” on the basis of an unpublished study
that was terminated early and failed to meets its orignal end point.
https://www.zerohedge.com/health/remdesivir-probably-worthless-trauma-surgeon-exposes-drug-companys-shenanigans
Avaclor, active ingredient chloroquine phosphate, has very nasty side effects.
We took it as an anti-malarial on Sundays, and it ruined your day, you had to go to bed.
Diaprim, pyrimethamine, worked weii.
I don’t see the drug Ivermectin mentioned. My understanding is there was some excitement about it when it was shown (in-vitro) to kill coronavirus in 48 hours. Then, it was sort of dismissed because it was believed that the dose would have to be very high (and unsafe) to achieve the concentration that was used in-vitro. However, a recent observational study showed that even a one-time dose of the amount typically given to treat river blindness appears to have improved outcomes, even of those on ventilators: https://papers.ssrn.com/sol3/papers.cfm?abstract_id=3580524 .
It’s also used as heartworm medicine for dogs. It’s really dang cheap – maybe that’s why it isn’t getting attention?
One of the world’s leading infectious disease specialists, Dr. Didier Daoult, has treated 3,227 COVID patients with only 16 deaths. A fatality rate of less than 0.5%.
What is wrong with this treatment that has successfully treated thousands of patients?
One thing only…..HAADS…………hydroxychloroquine and azithromycin derangement syndrome.
Results published daily.
https://www.mediterranee-infection.com/covid-19/