Readers, you know that word “access” pins my bullsh*t detector when used in the phrase “access to health care,” and many of you have picked up that same hypersensivity from me. Well, “access to health care” — the phrase, not the reality — is still ubiquitous, as I will first show. Next, I’ll give a quick look at what professionals mean when they say “access” (and raise a paradox, as well). Then I’ll look at an important new study from Health Affairs that raises the bare possibility that access to care means barriers to care and therefore, for many, no care. Finally, I (or rather Yves) will suggest that these barriers are not merely bureaucratic, or even financial, but part of the built environment itself. I will also do a little wandering through the sources in the notes, which you should not skip. But first, for the record, let me incriminate the guilty, something at which The Twitter is genuinely great:
Here is Democrat House Speaker Nancy Pelosi:
We must crush this coronavirus — and protect the Affordable Care Act to ensure Americans have access to the health care they need now more than ever. #FamiliesFirst @FaceTheNation pic.twitter.com/MZxYhJC2v4
— Nancy Pelosi (@SpeakerPelosi) October 4, 2020
You will notice that in Pelosi’s tweet, and in every tweet below, the words “access to” can be deleted from “access to health care” without loss of meaning (at least to a dull normal. People don’t want access to health care; they want health care!). So what is “access” doing? Hold that thought.
Of course, Democrat Party leader Obama:
Last night, @KamalaHarris shared how she will work with @JoeBiden to protect the Affordable Care Act and build on it so every American has access to quality, affordable care.
— Barack Obama (@BarackObama) October 8, 2020
Vice-Presidential candidate Kamala Harris:
Access to health care should be a right and not just a privilege for those who can afford it. pic.twitter.com/OcDiO7s5BP
— Kamala Harris (@KamalaHarris) October 4, 2020
Presidential candidate Joe Biden:
Obamacare was—and is—a big deal. As president, I’ll protect and build on it, lower health care costs, and give Americans the opportunity to choose a new public option.
We’re going to make sure everyone has access to the affordable health care they need. https://t.co/34NCSYhO2C
— Joe Biden (@JoeBiden) September 25, 2020
(In an enormous act of chutzpah, Democrats bait-and-switched the public option, itself a bait-and-switch!) And from the other side of the aisle, Kellyanne Conway:
My daughter, Claudia, is beautiful & brilliant. She has access to top doctors & health care & lives comfortably
Like all of you, she speculates on social media
Yet she’s 15
You are adults
We have COVID, but it’s clear who’s really sick
— Kellyanne Conway (@KellyannePolls) October 6, 2020
Note that Conway is the only one to indicate that there might be a class angle (“lives comfortably”) to any of this.
So what do health care professionals mean when they say “access to health care”? It’s complicated. It would take an intellectual historian with a grant to track down the history of “access to health care,” but here are a few hints derived from search. From “What does ‘access to health care’ mean?“, Journal of Health Services Research & Policy, 2002 (!):
Access is a complex concept and at least four aspects require evaluation. If services are available and there is an adequate supply of services, then the opportunity to obtain health care exists, and a population may ‘have access’ to services. The extent to which a population ‘gains access’ also depends on financial, organisational and social or cultural barriers that limit the utilisation of services. Thus access measured in terms of utilisation is dependent on the affordability, physical accessibility and acceptability of services and not merely adequacy of supply. Services available must be relevant and effective if the population is to ‘gain access to satisfactory health outcomes’. The availability of services, and barriers to access, have to be considered in the context of the differing perspectives, health needs and material and cultural settings of diverse groups in society. Equity of access may be measured in terms of the availability, utilisation or outcomes of services.
I tried to find out how the United States goverment operationalized “differing perspectives, health needs and material and cultural settings of diverse groups” in providing “access” to health care by searching U.S. Department of Health and Human Services and HealthCare.gov[1], but the best I could come up with was from HHS’s Office of Disease Prevention and Health Promotion (ODPHP), “Access to Health Services.”
Why Is Access to Health Services Important?
Access to health services means “the timely use of personal health services to achieve the best health outcomes.”1[2]
It requires 3 distinct steps:
- Gaining entry into the health care system (usually through insurance coverage)
- Accessing a location where needed health care services are provided (geographic availability)
- Finding a health care provider whom the patient trusts and can communicate with (personal relationship)2
And now the barriers:
Barriers to health services include:
- High cost of care
- Inadequate or no insurance coverage
- Lack of availability of services
- Lack of culturally competent care
And the ill effects, which amount to suffering and death, although this is America, so everybody is too polite to say that:
These barriers to accessing health services lead to:
- Unmet health needs
- Delays in receiving appropriate care
- Inability to get preventive services
- Financial burdens
- Preventable hospitalizations
Now let us return to our question: What is “access” doing? Again, people don’t want access to health care; they want health care! Look again at the list of barriers: You will see that “gaining entry” and “finding a health care provider” are not considered barriers at all! “Access” is conceived of as a frictionless, seamless process that connects patient and provider, and not — paradoxically — itself a barrier! So, this response to Speaker Pelosi:
“Access” erases the remaining financial barriers to health care after payment. A mere subsidy, even when achieved with the assistance of navigators does not eliminate co-pays, deductibles, network issues. “Access” also erases the enormous “tax on time” (as Yves calls it) of mastering complex eligibility requirements[3], finding the right policy, finding the right providers, handling the bills, and fighting with the insurance companies (generally while ill, or while caring for the ill). And of course the calls from collection agencies. Indeed, there’s an entire Twitter genre devoted to all the horror stories that “access” erases, and a fundraising site whose most numerous clientele didn’t get health care, even though they had “access” to it. “Access” to care paradoxically erases the enormous social cost determining who deserves “access” to health care, and if so, what kind and how much.
And so we come to the study I want to draw your attention to, from Health Affairs: “How Administrative Burdens Can Harm Health.” Imagine that! From the abstract:
In this brief, we detail how administrative burdens in our largest targeted social welfare policies may undermine health. First, we document the role of these social welfare policies in protecting health. We then define and conceptualize administrative burdens and detail how they limit access to these health-protective social welfare supports, all of which are critical in a major recession. Finally, we propose a research agenda to address the health implications of social welfare policy administration, especially the psychological and stress-related health impacts that may result from cumulative exposure to multiple administrative burdens.
I near spit coffee all over my keyboard at “research agenda”; see again footnote [2] at “generating theories”; it seems our system is Bourbon-like in its ability to “learn nothing.” That said, I’m happy to have everything that “access” erases made visible, so perhaps, under the lash and spur of the pandemic, we shall do better than we have heretofore. I’ll look only at the “administrative burdens” section, which begins:
The health benefits of social policies, however, are dependent on people accessing….
OK, OK…
…. them. The coronavirus-induced economic turmoil highlighted how hard it can be to access our largest social welfare programs. We provide a conceptual framework to understand people’s experience of this kind of onerous policy administration. Administrative burdens emerge in three subcategories: the learning costs of finding out about a program’s existence and benefits, determining whether one is eligible for the program and what benefits one might receive, and understanding how to apply for and stay on programs; the compliance costs of filling out forms, documenting one’s status, or responding to bureaucratic directives; and the psychological costs, including stress, frustrations, anxiety, loss of autonomy, or sense of stigma, that arise from interacting with these programs.
This is progress! Processes that the ODPHP (and before them, the Journal of Health Services Research & Policy, and before them, the Committee on Monitoring Access to Personal Health Care Services) treated as frictionless and seamless are now being treated as having real costs to real people. Here is a handy chart:
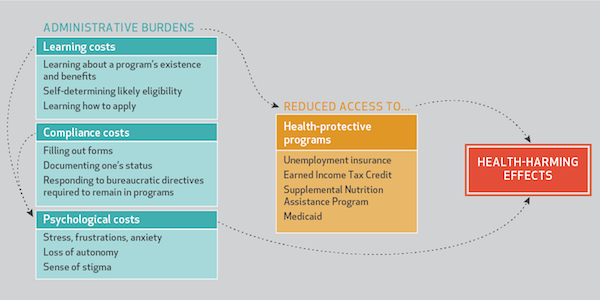
(Note that the chart applies to all social services, not just health care, which is also progress.) And — hold onto your hats, folks! — “onerous policy administration” is (dread word) political:
Burdens often have political origins and significant distributional impacts. Many are deployed as “policy by other means” to achieve aims that politicians otherwise struggle to acknowledge or enact, including rationing of benefits and services.
And profit for health insurance companies. More:
Although most people are familiar with cumbersome bureaucratic processes, it is easy to miss the scale, systemic nature, and intensity of the effects these processes can have. Moreover, they are often targeted at certain groups, including female, Black, poor, and disabled Americans.
Indeed, the working class generally. And it’s not easy to miss the “scale, systemic nature, and intensity” of these effects if you’ve had to deal with our health care system:
These burdens become magnified during major economic downturns, such as the COVID-19 pandemic-induced recession. Here, we detail health-harming burdens in our largest targeted social welfare programs, which also constitute crucial protections for those hit hardest by a recession.
The rest of the article covers unemployment insurance, the Earned Income Tax Credit, SNAP, and Medicaid, and is worth reading, but I don’t think adds anything on health care that readers don’t already know. The study concludes:
The previous section outlines how burdens may undermine health indirectly by reducing access to health protective programs. This section speculates about direct ways that burdens may influence health… pointing to a potential research agenda. Finally, although learning and compliance costs may affect psychological and physiological outcomes, how people are treated while they try to receive and keep benefits also likely matters. Psychological costs from stigma and discriminatory or belittling treatment may have long-term health consequences. Given evidence directly linking the experience of racial discrimination to poor health, it seems plausible that people who experience patterns of discrimination and negative bureaucratic encounters might also have worse downstream health. There is a need for more work examining the health implications of negative encounters with bureaucracies, many of which are patterned by race.
More study needed[4]. At least for health care, we don’t need a “research agenda.” We do not need to do “more work.” Canada, in what I have elsewhere called the largest natural experiment in the history of the world, has done the research and done the work. Canada — at least by the horrific and lethal example we have set — has made access a non-issue. We should follow their example. In my view, we should make health care free at the point of delivery for everyone. No co-pays, no deductibles, no in-network requirement, no eligibility determination, no billing. That entire bureaucracy of gatekeepers should be blown away[5]. How to do that is where the research and the work should be done.
Finally, there is one aspect not considered in any of the sources examined so far. It’s not enough to “find a health care provider” and “gain entry” to the system. The built environment in which care is deliverered matters too. Yves writes:
I happen to be spoiled by having insurance that does not limit me to an HMO or a PPO. I am getting a taste of what normal people go through via my mother.
She is in the HMO associated with the University of Alabama’s med school. Her doctor is part of the Kirklin Clinic, “one of the busiest outpatient centers in America.”
The place is a horrorshow for anyone with mobility issues. Whoever designed the space was fond of cavernous open areas. The parking is horrific and the parking lot is a huge walk (at least 1/5 mile) from the downstairs checkin. They claim they offer wheelchair assistance at the front entrance, but I wouldn’t trust it since even at airports (where everyone understands the passengers can’t be kept waiting too long) you can have waits for chairs. When you get upstairs to the floor where most of the MDs are, it’s another huge walk from the elevators to the exam rooms on the periphery. It’s a lot to ask a home health care aide to do as much pushing as is required for a visit. And I can’t go with her, since the distances are so large, I need a wheelchair too.
And it’s a Covid nightmare. A line to check in. Elevators to get to the MDs. Oh, and touch-screens to check in!
And it’s also managed on a Stalinist model. You can’t reach an administrator. You can’t even see a particular specialist even with a referral from your MD. The adminisphere determines which specialist you see if you need one.
We haven’t been since Covid and I don’t plan on her ever going there again. I am switching doctors because this setup is too patient hostile.
We have here concerns about “accessibilty”, but concerns that serve as a lens to focus light on the entire structure. It seems that problems for those who have mobility issues is a happy accident, the pleasing consequence of a fortress mentality designed with “defense in depth” against patients in mind. For all patients, the walks are long. Check-in is hard to do (and in the days of Covid, dangerous). You must wait for an MD (or an unknown specialist). And the administrators are behind the highest walls of all. One wonders at what point there will be armed guards at their doors. It would seem that the architecture of the building mirrors the power structure of the hospital. Have readers had these experiences and perceptions?
NOTES
[1] It wasn’t an easy search, because “accessibility” drowned out everything else on the HHS site; there may indeed by a definition of access at HHS and I just don’t know where to look. I did find this one manual for ObamaCare Navigators that has multiple uses of generic access (i.e., not for accessibility) but the term is not in the glossary. At HealthCare.gov, access is not in its glossary; a search on “access” yields 562 results, displayed 10 at a time. So, no. A search on “access definition” yields 10 hits, none obviously useful.
[2] Footnote 1 cites to the Institute of Medicine, Committee on Monitoring Access to Personal Health Care Services. Access to Health Care in America. Millman M, editor. Washington, DC: National Academies Press; 1993 (!). The National Institutes of health has a copy online. From the Introduction:
Access is a shorthand term for a broad set of concerns that center on the degree to which individuals and groups are able to obtain needed services from the medical care system…. For the purposes of its work the committee defined access as follows: the timely use of personal health services to achieve the best possible health outcomes…. The access monitoring indicators recommended by the committee are intended to detect when and where access problems occur in the personal health care system. They do not explain the exact causes of these problems, but they can provide a better basis for generating theories about why differences in access exist among populations.”
From a contemporaneous review:
This useful volume defines a set of national objectives and identifies indicators–measures of utilization and outcome–that can ‘sense; when and where problems occur in accessing specific health care services… The committee offers recommendations to federal, state, and local agencies for improving data collection and monitoring. This highly readable and well-organized volume will be essential for policymakers, public health officials, insurance companies, hospitals, physicians and nurses, and interested individuals.
Canadian Medicare was passed in 1966. 1993 – 1966 = 27 years. Summarizing with this handy chart:
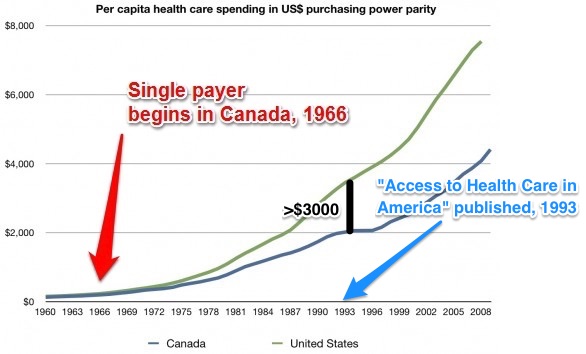
As the chart shows, even if all one cares about is “bending the cost curve,” Canada and the United States, had already diverged in per capita costs by at least three thousand dollars when Access to Health Care in America was published. One might have thought that “generating theories” and “improving data collection and monitoring” would not have been the order of the day, even in 1993. 2020 – 1993 is neatly symmetrical: Another 27 years! The rot in our health care system — our system generally — is very, very deep.
[3] In “The History of ObamaCare, 2013-2016,” I have an entire section (twelve posts) on “ObamaCare’s relentless creation of second-class citizens,” which details the many bureaucratic atrocities intrinsic to ObamaCare’s program design.
[4]. And more grants.
[5] From back in 2013. I don’t think I was far wrong:
Can’t quantify any of this, of course; but when ObamaCare apologists talk about how ObamaCare is going to become harder to repeal, I don’t think they mean that a grateful populace will get dramatically better access to health care; I think they mean that ObamaCare is going to develop constituencies based on a distribution of rents; and that many of those rents will flow to political class and “creative class” Democratic constituencies; people much like themselves. Not that there’s anything wrong with that. The opportunity costs, alas, will be dramatically better access to health care for everyone, besides immense waste of time and energy by well-meaning civil society groups of all kinds, as well as software engineers, project managers, architects, designers, etc. All of these people really do have better things to do….


Remember! You can get a FREE COVID-19 test.
And if you’re sick, it will only cost $35K to get treatment.
Total Cost of Her COVID-19 Treatment: $34,927.43
https://time.com/5806312/coronavirus-treatment-cost/
Time has been pretty good in chronicling the outrageous costs of US healthcare, as has Vox. In the end, however, the system just churns along, impervious to how ridiculously expensive it is. I first discovered some people’s response to it (medical tourism) about a dozen years ago, and nothing has changed since then, except it’s gotten much more expensive. Exponential growth is not the sole province of the COVID virus, apparently.
We live in a time of monopolies. I worry that their version of a public option will eliminate straight medicare and medicaid. More Big Healthcare negotiating with big insurance and big pharma on a national scale. All coordinated through DC. The final phase of a long term plan I fear. One big national privatized HMO. The astronomical deductibles in the ACA plans are the biggest barrier to access that I see…high deductible is basically catastrophic coverage for the middle class with higher premiums.
Agree completely. My thought as well. “Single payer” will be a form of privatized Medicare HMO Secure Horizons and that claptrap. Medicare has gotten oddly punitive over the years. If you are disabled and were eligible for Medicare B, but had alternative coverage and didn’t sign up for it, you must prove you had continuing coverage when you sign up for Medicare at age 66 or pay an outrageous ongoing penalty. My reaction was: “say what??” (Further, there was a time when the cost of B was frozen at what you would have paid when you first became B eligible.) Post-stroke, I have difficulty sorting these things out, even with a leg up, so to speak, as a former insurance lawyer. Unless raging capitalism changes in the for profit “health/illness” industry, private insurance selling empty benefits will not disappear. If you have a 5k deductible, with 3k out of pocket, pre-authorizations, claims people who are paid to say “no” – you know what I mean – you don’t have insurance. There is no place for CEO style profit templates for health care.
This is an excellent article. Thank you.
I don’t want any phrase to “pin” my bullsh$t detector. I want my bullsh$t detector much more robust than that.
OTOH, thanks in no small part to nc, my bullsh$t detector now generally goes “ping” when it encounters the phrase “access to” in association with almost any need we somehow aren’t actually getting (and in fact aren’t always even gifted with a glimpse of)….
Often all it takes is to read closely and look at what they’re really saying. An example from a few years back (which I can’t seem to track down) is faux self-reflection, something like this:
“We’ve noticed that there’s a perception among voters that we aren’t acting in their best interests, and we’re committed to changing that.”
What readers think it says: We haven’t been acting in your best interests. Sorry. We’ll start doing that.
What it actually says: Voters are stupid and don’t understand that we do all this for their own good. We’ll work harder at getting them to believe us and not their own lying eyes.
“We’ve noticed that there’s a perception among voters that we aren’t acting in their best interests, and we’re committed to changing that.”
Obama’s method was to keep on throwing PR at those voters until they were convinced that the dems were acting in their best interests, in spite of the facts on the ground saying the opposite. Just ask the people of Flint, Michigan.
When you get down to it, the word “access” is a qualifier word that has all sorts of conditions attached to it, usually based on class and money. I forget the details but Kamala Harris showed this line of thinking a few years ago when she made a political promise that was contingent upon a certain time frame and certain conditions being met for which she was roundly mocked.
Our French friends have a perfect phrase for being close but not close enough.
“Licking the glass.” lécher le verre
Patisseries and Charcuteries are involved.
Here stateside, alas, so is “health care.”
I think that what is being said is, “The voters don’t understand that no matter what was said, we are all acting in our own best interests.” In political terms, ‘i just want to be re-lected. Politics is a great free lunch.”
And maybe worse, “Access to affordable healthcare” which is a totally meaningless phrase!
As long as private insurance companies stand between us and Health Care, there is nothing affordable about it and access is exceedingly questionable.
I said “pin” the bullshit detector. I didn’t say “fry the innards.”
This issue melts the edges of my brain. I CANNOT believe it but this has been dominating my world since 1978. Fried innards — I’m getting there.
PS. This was a particularly great post. I’ve already read it 3 times.
ACA has been total bullshit from the beginning.
I lost my health insurance thanks to ACA. (At the time ACA went into effect, I had a group plan through my corporation. ACA redefined “groups” such that my corp was no longer qualified for a “group” plan, and the insurance company cancelled the policy at the next renewal. The alternatives were massively more expensive, both in premiums and out-of-pocket costs) and all had much smaller provider networks.
Shopping for insurance now, 70% of the choices I had pre-ACA no longer exist. The remaining policies are utter crap.
Current politics are a hobbesian choice between the Republicans who would repeal ACA and leave me with no medical care at all, or the Democrats who would expand ACA and have it continue to financially bleed me to death for health care.
Some choice.
And yet, I keep hearing the diminishing echos of “death panels” and “best healthcare in the world!!” I’m really God **** cynical nowadays, but really, just how do some of these supporters of the current deathcare provider’s system sleep at night? But then, we have the respectable Sacklers, illegal drug providers to the Disposables, multi decade child pimp to the elites Jeff Epstein, and Nancy Pelosi and Mitch McConnell, whose families made bank out of the stimulus legislation while giving token help to the unemployed.
Yes. The ACA made my very large group plan much much worse. Suddenly spouses and kids were now covered only at new exorbitant rates, co-pays went up, out of pocket went up, everything got more expensive for the employee and the employer, because what had been considered a pretty standard middle-of-the-road plan before the ACA was passed was now deemed a ‘Cadillac’ plan and options were narrowed accordingly.
” just how do some of these supporters of the current deathcare provider’s system sleep at night?”
In the words of Rainier Wolfcastle, “On top of a big pile of money.”
Admittedly for many of them that pile of money really isn’t all that big though. They’re just willing to sell their souls and see their fellow citizens suffer and die for very affordable rates.
When you look at the outlay totals for lobbyists, it’s quickly obvious from the ROI for the companies lobbying that government officials are woefully ineffective at collecting their fair share of the loot.
I think that differential is what elected officials use to convince themselves and their constituents that they aren’t actually corrupted. “See I only took 50 cents when I could have taken $10, I really do have your best interest at heart…”
Ah, there’s the choice of the lesser evil again. Good observation
Beyond the plans they destroyed early on, that “Cadillac Plan” was reminiscent of the failing school section of “No Child Left Behind”, it was designed to Catch them all. By basing it on cost not policy provisions and then not making any allowances for medical insurance inflation, it would make nearly every plan that provided more than the bare minimum of healthcare a “Cadillac Plan” in time. Eventually every employer provided plan, with few exceptions, would be high deductible, high coinsurance, low network policies. The exceptions being the same that decides who gets a golden parachute.
The greed, the class bigotry, and yes sadism that dripped off of the ACA was overwhelming. I keep expecting people to catch on that yes they got rid of preexisting conditions bans, they opened the door to make premiums, deductibles and copays so high you still couldn’t afford the treatment for those conditions after you paid for the “access” with the premium, employer provided or not.
There have been armed guards at my local hospital for ten years now. Nobody gets in without a wand screening. You are given a RFID badge that allows you to pass through some doors, but not others. (I imagine they can track your specific travel location in the hallways.)
Before you actually get hospital services you are required to sign a contract that stipulates you will submit any malpractice complaints to private arbitration. (Heads I win, Tails you lose.)
Even the critical care doctor who saved my life felt obliged to hurriedly inquire about my ability to pay immediately after being brought out of a week long medically induced coma. The very first question!
Medical care, even at the best hospital, is a crap-shoot.
–
I have noticed that some of the courts and police stations in the Bay Area have gotten more fortified over the past twenty years. Even those places that were around during the 60s and 70s were not fortified then, but only became so because “reasons.” More uncomfortable, confusing, irritating, and hard to use. The airports are the same as most of the “security measures” are security theater that are really profit centers that make flying even more uncomfortable for no good reason for the general public.
All of a sudden John Cornyn(R-Tx) is hawking a health insurance plan that will save medicare and reduce drug prices. Obviously trying to put on a halloween moderate costume.
Where to begin and what to winnow…
I accompanied a person to Kaiser Interstate for minor surgery, 50 miles away. Facility was vast and would be impossible for those who can’t hike. On the follow-up trip, we helped a man struggling to get from parking to entrance; we got a wheelchair and pushed him in. (He may still be there .)
A friend lost coverage through a slip-up while changing providers. During that month, she was diagnosed with breast cancer, which thus became a pre-existing condition. They sold assets, she died.
A diabetic friend had surgery followed by a several day hospitalization for removal of infected toes. He had good insurance through his large employer. He told us he would not live long enough to pay off his uncapped 20 percent and deductibles, some 30 thou, and he didn’t.
I won’t repeat comments I’ve made before about working in the industry. The data entry, computer, billing and collections, pricing and accounts receivable departments employed more people than the technical side.
> Single Payer begins in Canada, 1966. (chart)
Would Canadian healthcare costs have not risen as high and as fast as they have (since 1993) if the U.S. had adopted a Single Payer system in back 1966? In other words, has the exorbitant price inflation of healthcare in the U.S. dragged up Canadian cost as well?
It’s not a bad question and I have no idea if it’s possible. The US being such a powerhouse in healthcare spending inflates costs globally?
I’m just wondering why healthcare costs around the world escalated so quickly in 1rst world to 3rd nations since the late 70’s. I don’t think it’s just Canada but all around the world.
Changes to Canadian patent laws under the Mulroney government have also resulted in increased drug prices – it was sold with a promise from various big pharma companies that they promised to invest heavily in R&D in Canada. A non-binding promise of course so nothing really came of it. Drug prices ares still much lower but would have been lower still without this.
Considering Canada’s much lower population and how it is much more spread out over more territory it would seem to me that the US could, if single payer was implemented in a manner essentially identical to Canada, achieve the same health care outcomes as Canada does at substantially lower costs than we have here. “If single payer was implemented in a manner essentially identical to Canada” being the real trick. Even if a US administration and Congress ever do move to bring single payer to the US the grifters and con-artists will be hard at work trying to sabotage it.
> Considering Canada’s much lower population and how it is much more spread out over more territory it would seem to me that the US could, if single payer was implemented in a manner essentially identical to Canada, achieve the same health care outcomes as Canada does at substantially lower costs than we have here.
As I wrote in 2019, of the various proposals to do it like the Germans or the Dutch, much beloved of Vox-type policy wonks:
There’s a whole lot of motivated reasoning going on among the policy wonks; I hate to cast aspersions, but it looks like the motivation is preserving the private health insurance companies. Unsurprisingly.
Re the change to Canada’s patent laws: BIg Pharma did keep its word re investment for about 15 (?) years then broke its promise. Investment in R&D by Big Pharma is now less than it was when it made the promise in the late 1980s.
The reason patented drugs cost less in Canada now than in the US is because part of the quid pro quo by the Mulroney government to fend off attacks by defenders of our much looser patent laws was to introduce the Patented Medicines Prices Review Board (PMPRB). It reviews prices and sets the maximum price that can be paid measured against a reference group of countries and other criteria. The regulations are about to be changed and will soon be stricter, mostly by eliminating the US as a reference country. Drug prices will also be evaluated for effectiveness, a new, and excellent, provision.
I should note that even with no changes at all to patent laws and within the current very bad system for pricing, all countries can force Big Pharma to take lower prices by invoking their right to implement ”compulsory licences”. The fact this is rarely done, illustrates that prices are high due to a lack of political will to force them down.
I’ve been fortunate to have hmo kaiser in CA for nearly 40 years. No bills including when I went as advised to nearest (non Kaiser) hospital, modest co pays. Wife elected to switch to kaiser after retiring and before Medicare eligibility, so not cheap, 8k/yr. but she also satisfied.
You are assigned a gp, but we each chose to request switch to same sex, no problem. Ive had several health issues, once a little displeased had to wait for back surgery, but overall quite happy.
Obviously m4a, especially Jayapal bill better.
Just substitute the word “Air” or “Water” within the phrase to see how cruel it is.
“Steve Elmendorf, a registered lobbyist for United Health, sent invitations to a Pelosi fundraiser at his home for this past weekend. The asking price: $5,000 for PACs and $2,400 per individual – the legal maximum for each.”
https://www.change.org/p/tell-pelosi-to-return-donations-from-the-health-insurance-industry
I just want to call attention to another phrase “household income”
While my mother was living with us – a household with two working adults – she didn’t qualify for the local senior transport services because our “household income” was too high.
More recently, a 27- year old stepson has moved in with us for a bit in an attempt to reinvent himself in a new state.
You should see this coming, his options for affordable healthcare are based on “household income” meanwhile, he is too old to include as a dependent on existing insurance. His new low wage job does not have benefits – and we are all very grateful he has a job with a good employer.
How can anyone afford rent, insurance, phone, in this day? This has to be happening all over the nation, parents with adult children who don’t qualify for affordable insurance, let alone, the actual health care.
> I just want to call attention to another phrase “household income”
That’s an excellent point.
“No man is an island, but each person is a household.”
Some reason she has some moral obliation to tell the truth about your household income? “It’s so confusing”…”The website crashed”, “couldn’t get a live human on the phone”.
In other words, your mother should have lied. Corporations do, politicians do, why are we still following some outdated concepts of ‘personal responsibility’ that seemingly only applies to poor people?
Corporations obey the law to the point where they break it, or to the point where it’s actually enforced. We Americans should do the same when it comes to getting back what we and our ancestors have paid into the system.
Every senior that she knows in your town should learn about “self reporting” household income.
Great post! Thanks.
I remember when HMO’s first widely appeared in the late 80s here in large employer plans as a way to “reduce costs and increase access.” The modern HMO idea had been promoted by the Nixon admin in the early 70’s. The enactment of the Health Maintenance Organization Act of 1973 provided a major impetus to the expansion of managed health care.
Though some forms of group “managed care” did exist prior to the 1970s, in the USA they came about chiefly through the influence of U.S. President Richard Nixon and his friend Edgar Kaiser. In discussion in the White House on February 17, 1971, Nixon expressed his support for the essential philosophy of the HMO, which John Ehrlichman explained thus: “All the incentives are toward less medical care, because the less care they give them, the more money they make.”[6] Kaiser Permanente disputes Ehrlichman’s “secondhand, inarticulate paraphrase”, and presents a record of the briefs received by Ehrlichman and the White House.[7]
https://en.wikipedia.org/wiki/Health_maintenance_organization
The 1997 movie ‘As Good As It Gets’ made the HMO bureaucratic nightmare one of the plot devices. This was the scene that had audiences spontaneously cheering when the heroine cussed out HMOs.
https://www.youtube.com/watch?v=cGbhI11K6TU
The Medicare Part D plan was passed and drug prices started going up, in some cases by a lot. Then the ACA appeared as a way to “reduce costs and increase access.”… again. It’s only gotten worse, with PE getting in on the act and privatizing hospitals and clinics for shareholder value and pharma jacking prescription drug prices, and insurance companies raising premiums to-the-moon on the “affordable” plans, and surprise billing.
Here’s an old joke with an update:
“Hi, I’m from the
governmenthealth insurance company and I’m here to help you.”The Bismark model is one alternative to the Wall St model.
The Bismarck Private Insurance Healthcare System used in dozens of developed nations simply enables access to private affordable healthcare for all citizens by moving profits in the curve below from the boardroom to the Bedside
https://twitter.com/DermHAG/status/1311984991539286019
Interesting that there aren’t medical codes for the things the insurance companies don’t want measured.
Value based care can not be assessed unless @CMSGov
and the @AmerMedicalAssn
provide physicians with codes to document daily the 10’s of thousands of patient’s delayed, changed or abandoned care due to insurance prior authorization rationing or costs.
https://twitter.com/DermHAG/status/1312757057523798016
Read this whole thread. It contains this little known rentier mandate:
We physicians are mandated to lease EHRs to input data for sale by and to a myriad of companies with no clinical or financial ROI for physician’s and patients.
“Input date *for sale by and to a myriad of companies*” with no medical
Well, that’s horrible.
Not just “access”, but “research” should pin your bullsh*t detector.
In his book “The Politics of Pure Science”, Daniel S Greenberg has a footnote that has stuck with me for the more than 50 years since the book was published. On the topic of research, he says “The cult of research, pure and otherwise, holds forth research as the solution for many social ills that, in fact, have little or nothing to do with lack of knowledge. Jaques Barzan … brings to our attention the letter of a New York Times reader commenting on proposals for research on a 200 mile-an-hour rail service: ‘There is no need for another expensive foundation research project to begin railroad recovery. Any rider can provide expert advice, free of charge, to management. When it is cold, the cars should be heated; when it is warm, they should be cooled; when it says “No Smoking” the conductor should enforce it … where there is scenery, it should be discernible through the window … where there are rest rooms, there should be sanitation somehow comparable to a well-run stockyard'”.
Whenever someone responds to a policy question that “more research is needed”, you can pretty much guarantee they just want to kick the can down the road.
See footnote [4].
“Access” is the horse brought to water. You can bring a horse to a $1000 per sip fountain, but you can’t make him drink to save his own hide. Unless of course, he collapses into the water and gets his access to Emergency medicine and the inflated charges.
Really excellent piece, much appreciated.
“Research” on how other countries have gone about instituting universal health care of the type envisioned – there’s been quite a lot of that, hasn’t there? And perhaps it would be well to start at home, i.e. with how Medicare was instituted in 1965-1966. I’ve always been particularly struck by the fact that the entire 65-and-older population of the U.S. was enrolled in the program within a year, albeit in the absence of computer registration/enrollment/record-keeping.
The most important factor to make M4A a reality is to achieve political acceptance of what countries which provide universal health care hold as their core belief: health care is a human right, not an earned privilege.
THE MEDICARE LESSON FROM ITS BIRTH IS IMPORTANT: A UNIVERSAL SOCIAL INSURANCE PROGRAM FOR A DEMOGRAPHIC GROUP, WITH THE EXPECTATION THAT MORE WOULD BE ADDED: NHI BY AGGREGATION, AS WITH CANADA’S ADDITION OF SERVICES RATHER THAN GROUPS. BUT WITH SAME CONCEPTION OF SOCIAL INSURANCE, NOT SOCIAL ASSISTANTANCE.
> the entire 65-and-older population of the U.S. was enrolled in the program within a year, albeit in the absence of computer registration/enrollment/record-keeping.
I believe it was all done by punchcard
Lambert – did you mean to say “PINGS my bullshit detector” rather than “pins my bullshit detector”??
Back n the days of yore there was in your manual transmission truck or car an actual pin that stopped the gauge from spinning, so yes, pins is the correct verbiage…
Seemed timely (today’s Salon) and apropos. The pandemic has laid so many of these truths bare.
My sister died needlessly of COVID-19 — and bias
{hightlighting added}
An absolutely appalling story.
Hi Lambert,
A very quick comment re the graph in footnote 2 that reinforces the point made in the graph. The law enabling Canadian medicare was passed in 1966 but Medicare did not come into effect until January 1,1969. It was originally supposed to come into effect on Jan.1, 1968 but the Minister of Finance of the time (Mitchell Sharp) said fiscal conditions weren’t right so implementation was delayed until Jan 1, 1969.
Regarding your analysis of the expression “access”. It’s rather amusing because for us here in Canada arguing in favour of universal public single-payer Pharmacare, “access” is a term we use to counter Big Pharma/insurance industry arguments that almost everyone is currently covered by some prescription drug plan or other. This is correct but it ignores the hurdles imposed by deductibles, co-pays and the like, which wind up excluding 10-20% of people. So while they have coverage they do not have access.
Additional point: Canadian Medicare was not implemented all at once. It came into effect over several years as the provinces signed on to agreements with the federal government. So getting back to the graph in footnote 2, my guess is that the cost in Canada per capita began to drop almost immediately after Medicare was brought in, province by province.
>A very quick comment re the graph in footnote 2 that reinforces the point made in the graph. The law enabling Canadian medicare was passed in 1966 but Medicare did not come into effect until January 1,1969. It was originally supposed to come into effect on Jan.1, 1968 but the Minister of Finance of the time (Mitchell Sharp) said fiscal conditions weren’t right so implementation was delayed until Jan 1, 1969.
Thanks. That, the arrow in the graph is pretty fat…. Sounds like I have to surrender the pleasing 27-year symmetry though!
I don’t think what the political wordsmiths in DC mean when they say access to healthcare that matters. It’s what the public thinks they mean. That is the more relevant factor and that,universal healthcare,is where this country is going. And as for the higher premiums for upper middle class folks,you are not the group the ACÁ was intended to help. I ,as an employer have a number of employees who now have healthcare insurance which they greatly appreciate because being members of the bottom 50%, they wouldn’t have gotten insurance otherwise. Their biggest fear has always been having a catastrophic health event happen to them of their family. If I were to asks them how they define “access to healthcare,they would breakout laughing. What in the hell are you talking about…that’s what they’d ask me.
Health insurance isn’t health care… Maybe you should cut their pay enough that they are eligible for medicaid, or maybe that’s already the case and thus they are covered as low wage earners and it’s really a gift to you as the employers who now has covered employees at no cost to you. It’s hard to tell from your comment what their actual situation is. If someone asked me if I ought to go to a doctor I would certainly break out laughing.
I agree with your point that health insurance isn’t healthcare and this is exactly what my employees are discovering. I think that’s a good thing. They’re more likely to favor universal healthcare after having a taste of private insurance. My employees are not well paid tech workers but I have always paid them much more than they could make at other small manufacturing companies in rural areas such as we live in. I pay for their insurance fully. I also pay for counseling ,if they want it,at my own expense. I lend them money to buy cars or whatever at zero interest and no determined payback time. Some never pay me back. And..they don’t breakout laughing when they have an appendicitis,a broken leg or a broken jaw from an abusive boyfriend and have to see a doctor. They should be so lucky as you.
You should be so lucky. I make too much for medicaid and not enough to afford 300 a month and 5000 deductible so I’m in the “you’ll get nothing and like it” category.
I understand the predicament you’re in. I used to joke with certain of my employees that I could always pay them less if they wanted to be eligible for MediCal. They never took me up on it. If you don’t have insurance the deductible doesn’t matter…it is infinite.Many of my employees are single mothers with children and through the ACA I only pay in the $200 range per month. I’m guessing that you’re a single male under 40. If that’s the case, you only need catastrophic insurance. Under the ACÁ you could get that for around $100/ month. Well worth it.
Access to health care translates to: do you have the money to pay the premiums, the deductible, the co-pays, etc.? I was self employed and when my distributors went bankrupt, so did my company. Good-bye insurance. I also had developed several physical limitations while I was self employed that worsened after I no longer had insurance. They weren’t bad enough for me to qualify as disabled but they were bad enough to keep me from getting a regular job (plus I lived in the middle of nowhere and couldn’t drive at night or in bad weather). I did find other ways to make money but it still wasn’t enough for health insurance.
Until people find their circumstances drastically changed, they develop serious illnesses, and/or they have no health insurance or they discover the insurance they have is lousy, they do not understand just how bad the current system really is. I’ve had arguments with people on line because they do not understand how you can be poor enough to not afford insurance yet “rich” enough not to qualify for any help. And here we are in a pandemic, with millions more no longer with health insurance, and yet neither party will do anything to really help us. P.S. If it weren’t for Medicare, I’d be in real trouble.
I know that I am crying over spilt milk, but why do we think “health care” when what we are discussing is “medical care?” Nobody needs health care, almost everybody needs medical care at some time or other.
Maybe we should all stop thinking in catch phrases and start thinking in real language.
I’m with you, Dick, but the barn is a distant memory to that horse.
Maybe this comment will only show my ignorance. Should the word “pin” in the title really be “ping?”
My BS detector is often “pinged.”
Picture an analog voltmeter, the kind with a moving pointer. Such a meter is said to be “pinned” when the pointer hits the pin that limits its maximum travel.
Thank you.
SO, it is now apparently “open enrollment period” and as I sit here at my desk, my landline rings a couple times a day with friendly young people (I have Medicare) offering me options. I tell them “I wish I could subscribe to your lovely and valuable product, but my doctor has told me that I have only three months left to live.”
On the subject of bullsh*t detectors, one word that always raises my hackles is “stakeholders”, because it suggests that a compromise was achieved among disparate groups, some of whom may be extracting rent from society, and I would prefer to see these stakeholders burned at the stake.
One more thing. When a politician says “I want group x to have skin in the game”, it means “I gonna skin you first chance I get.”. As the Grateful Dead sang to us, “You know my uncle, he’s as honest as me, and I’m as honest as a government man can be.”
Speaking of access, what used to kill me about Boston and its famous hospitals is the way that those famous hospitals charged some of the highest parking rates in town. In that regard, the PNW, where I live now, is much kinder to patients and guests.
I’m a Forensic Pathologist. I’m salaried, and I’m happy. Coroner’s Offices are “socialized healthcare”, and we do a good job. Too bad the living don’t have the same equal and free diagnostic care. For the living, I’d even recommend equal and free treatment. I wish we more like Canada, France, Australia, Japan, England, Russia, Germany, China, etc., i.e. the civilized countries.