I’d like to start this article with a couple of disclaimers and a caveat. First of all, I am not a medical doctor. This article is not intended as medical advice. It’s a layman’s account of how an extremely cheap, safe and widely available off-patent medicine called ivermectin appears to be saving the lives of countless Covid-19 patients across Latin America and beyond. Yet hardly anybody is talking about it.
Here’s the caveat: The first section of the article, which was completed on Friday, is about Mexico City’s recent deployment of ivermectin in its fight against Covid-19. On Saturday, Mexico’s Ministry of Health jacked up its total excess death count due to Covid (for the whole country) by 60%, from 182,000 to 294,000. However, most of these deaths took place before Mexico City began using ivermectin as part of its its test-and-treat approach to Covid.
Covid-19 vaccines are reaching most emerging and developing economies in only drips and drabs, with a few notable exceptions such as Chile. In many countries, locking down entire cities or regions and paying millions of non-essential workers not to work while front-line doctors and nurses battle to contain the virus is not an option. There simply isn’t enough money available. This has left doctors and health authorities with little choice but to try out cheap, widely available generic medicines. Those drugs include ivermectin, a “well-studied, well tolerated,” (in the words of a 2013 FT article) off-patent anti-parasitical.
The results have been extremely promising, according to almost all of the clinical studies conducted thus far. Many of the studies took place in Latin America where around half of the countries in the region have used or are using ivermectin to some degree or another. A meta analysis of 42 clinical trials, involving approximately 15,000 patients, found that 83% showed improvements with early treatment, 51% improved during late-stage
treatment and there was an 89% prevention of onset rate noted. Yet the studies have received scant attention in more advanced economies — so much so that the vast majority of the people I talk to here in Europe have still not even heard of the medicine.
Bucking the Trend
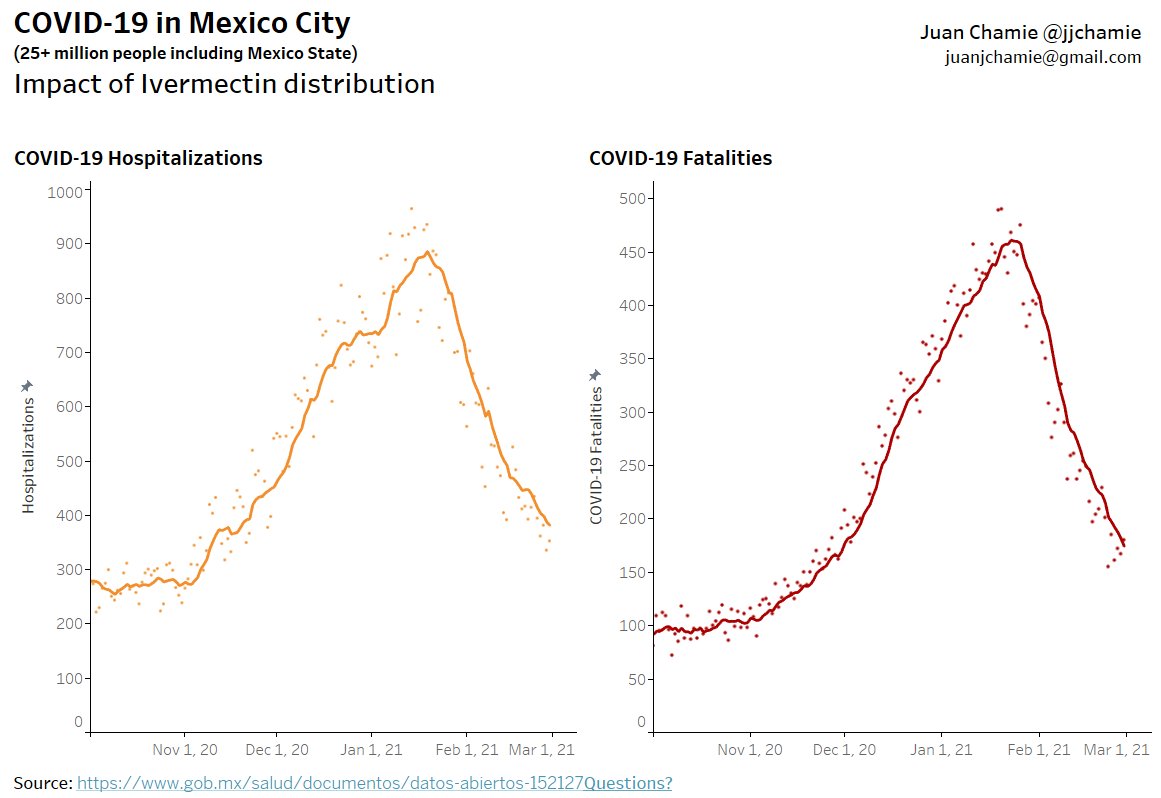
On December 29th of last year, Mexico’s Institute of Socal Security (IMSS) allowed ivermectin to be prescribed to outpatients with Covid. On the same day the Secretariat of Health of Mexico City and the State of Mexico decided to adopt a protocol in which anyone testing positive at any one of the city’s 250 rapid testing sites would be given ivermectin. As you can see in the graphs below, courtesy of Juan Chamie, a data scientist from EAFIT University in Colombia, based on data provided by Mexico City authorities, the number of hospitalizations due to Covid and excess deaths peaked shortly after the New Year and have been falling sharply ever since. They are now almost back to their prior base line.
Mexico City is the first major global city to adopt what amounts to a test-and-treat approach to covid-19 involving ivermectin. But it was the largely indigenous southern state of Chiapas that led the way last summer. In July 2020, as Mexico was buckling under its first wave of the pandemic, the state decided to distribute ivermectin as a Covid-19 treatment, having already deployed the medicine in its battle against mosquito-borne RNA viruses such as Zika and Chikungunya. Since October Chiapas has consistently occupied the lowest risk level on the federal government’s coronavirus stoplight map.
Thanks to ivermectin’s apparent success in Chiapas, IMSS allowed the medicine to be prescribed nationwide. It also helped launch the pilot program in Mexico City, for which it received a barrage of criticism. An official group of health experts argued that there’s no scientific evidence that the drug is effective, and called for the immediate repeal of its use. To their credit, both the Secretariat and IMSS have stuck to their guns.
Playing With Lives
Of course, there’s no way of definitively proving that the rapid falloff in hospitalizations and deaths, first in Chiapas and then Mexico City, is due to the use of ivermectin. Correlation, as we well know, is not causation. It’s also true that Mexico City authorities have introduced tougher social distancing measures and travel restrictions since December. But similar dramatic drop offs have been witnessed in other regions and countries where ivermectin has been used widely, including across the length and breadth of Peru and Iran as well as parts of Brazil, Paraguay, Bolivia, the Dominican Republic and India.
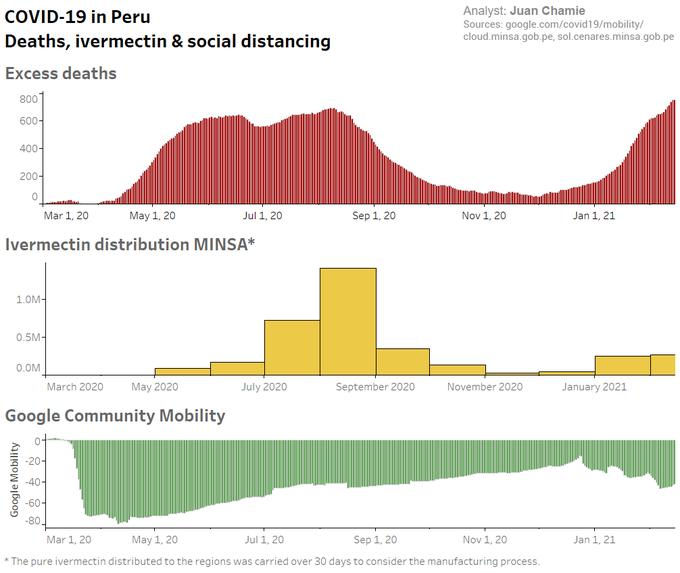
In Peru, ivermectin was used in eight states during the very early stages of the pandemic (May-July). Its use was then extended to the whole country except Lima, which did not start deploying the drug until months later. For the 24 states with early IVM treatment (and Lima), excess deaths dropped 59% (25%) at +30 days and 75% (25%) at +45 days after day of peak deaths. But in October, after the first wave had been brought under control, the new government in Peru took the inexplicable step of withdrawing a number of medicines, including ivermectin, from its treatment guide for the disease. Within weeks hospitalizations and deaths were soaring once again.
The following graph, taken from a study by Juan Chamie, Jennifer Hibberd of the University of Toronto and David Scheim of the US Public Health Service, shows the sharp rise, fall and resurgence in excess deaths (among the over 60 year-old cohort) in Peru as the virus waxed, waned and waxed again. Between August and December case fatalities dropped sharply in all states but Lima, yet six indices of Google-tracked community mobility rose over the same period, before rising once again. In other words, the treatment appeared to be working even as the country reopened.
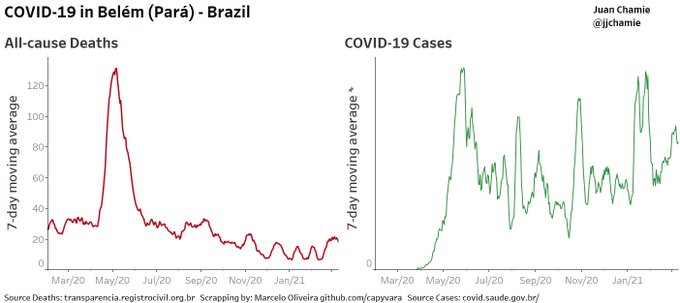
In the Brazilian city of Belem authorities began using ivermectin way back in June 2020. Since then the city has managed to escape the massive surge in covid-related deaths that has plagued Brazil since early November, as the graphic below shows. In another study a like-for-like comparison of cities in similar regions of Brazil showed that the cities that began distributing ivermectin in June last year were, by September, registering much lower case counts than those that didn’t.
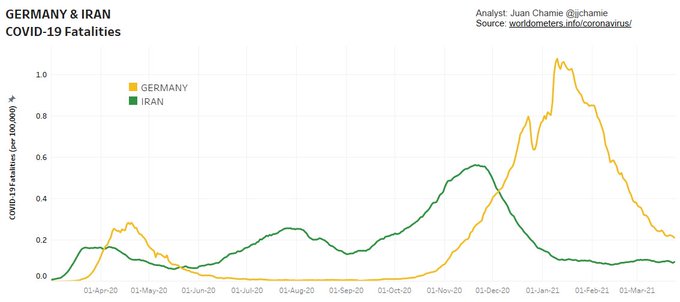
Iran has also seen a sharp fall in covid-related deaths since late November followed by a flattening of the curve. Earlier that month the country, with a similar population to Germany and an urban population density twice as high, succeeded in gaining the technical knowledge to produce ivermectin and began distributing it to hospitals in the country.
What is Ivermectin?
First discovered in 1975 and launched onto the market in 1981, ivermectin is a safe, broad-spectrum anthelminthic drug registered for the treatment of a number of neglected tropical diseases (NTDs) including river blindness (onchocerciasis), strongyloidiasis, trichuriasis, ascariasis, and lymphatic filariasis. It is also used widely in veterinary medicine. In recent years it has been discovered to have strong anti-viral properties against RNA viruses such as zika and yellow fever. In its use against river blindness in Africa it is estimated to have prevented 7 million years of disability.
The medicine is not only extremely effective in treating a broad range of illnesses, including RNA viruses; it is also well tolerated. To date, more than 3.7 billion doses have been distributed with an excellent safety profile. Most adverse reactions are mild, transitory and associated with parasite death rather than with the drug itself.
“The reason why this medicine is distributed in Africa not by doctors and nurses but mainly by volunteers is that it is extremely safe,” says Japanese microbiologist Satoshi Omura, who jointly with the Irish parasitologist William C. Campbell, led the team that isolated a strain of Streptomyces avermitilis that produce the anti-parasitical compound avermectin, the active ingredient in ivermectin. Omura and Campbell were awarded the Nobel Prize for Medicine in 2015 for their discovery.
Dr. Omura himself believes there’s already enough evidence of the benefits of ivermectin against Covid-19 for it to be granted approval as a therapeutic. One of its biggest benefits is that it appears to work in the early stages of the disease, he co-writes in an article published earlier this month in the Japanese Journal of Antibiotics:
“Currently, there are no therapeutic agents available for mildly ill patients who are being treated at home (or in self-isolating accommodations) or for moderately ill hospitalized patients. Nothing is as helpless as a disease without a cure.”
Anti-Viral, Anti-Inflammatory, Anti-Long Haul
Another major ivermectin proponent is the Frontline Covid-19 Critical Care Alliance (FLCCC), which has been trying to repurpose medicines already on the market for the treatment of Covid-19. In October it created the I-MASK+ protocol for prevention and early outpatient treatment, which includes ivermectin, vitamin D3, vitamin C, zinc, melatonin and quercetin.
The FLCCC believes that ivermectin is not only “one of the world’s safest, cheapest and most widely available drugs,” it is also the most effective against Covid. “The studies we presented to the NIH revealed high levels of statistical significance showing large magnitude benefit in transmission rates, need for hospitalization and death,” says Dr. Pierre Kory of the FLCCC, who twice gave testimony to the US Congress on Covid-19.
Besides the dozens of clinical studies conducted so far on the efficacy of ivermectin against Covid, the FLCCC also cites “natural experiments” in Peru, Brazil, Paraguay, the Dominican Republic and Mexico where ivermectin was distributed widely, with “large decreases in case counts … soon after distribution began.”
Another recent convert to the cause is Dr Alessandro Santin, a renowned cancer researcher who runs a large laboratory at Yale. Santin believes that ivermectin is a game-changer that could significantly reduce Covid’s toll on human health.
“The bottom line is that ivermectin works. I’ve seen that in my patients as well as treating my own family in Italy,” Santin said, in reference to his father, 88, who recently suffered a serious bout of COVID. “We must find a way to administer it on a large scale.”
In an interview with Italian daily Il Fatto Quotidiano, Santin explains why he believes ivermectin is so effective against Covid:
- Its powerful anti-viral properties: “The theory behind the main mechanism of action is that ivermectin attaches itself to Sars-Cov2’s Spike1 protein as well as at various strategic points used by the virus to bind and enter our cells. This is why it can also work against variants, unlike monoclonal antibodies.”
- Its anti-inflammatory activity: “Ivermectin has a powerful anti-inflammatory effect similar to that of cortisone. But unlike with cortisone, the effect is not immunosuppressive. Therefore the immune response of both T cells and B cells (producing antibodies) continues to function under ivermectin, acting on the transcription factor NF-KB (which informs our body to produce cytokines and causes a real cytokine storm when hyperactivated by Covid). This is why the drug also works well during the advanced phase of the disease”.
- It even seems to help long-haulers: “I have treated and am treating ‘long haulers’, including people who have been sick for a year and who do not breathe well, who have tried out everything to no avail. Within two weeks of starting them on ivermectin… these people have started to live again, with practically no side effects. The virus is an intracellular parasite; only if it enters our cells can it use the cellular machine to replicate. If it can’t get in and hack our immune system, then it stays out on the doormat and gets attacked by our immune system much more easily.”
More Evidence Needed, Say Regulators
Yet despite the growing body of evidence supporting ivermectin’s therapeutic effects against SARS-Cov2, national and supranational health authorities, particularly in more advanced economies, are dragging their feet. The European Medicines Agency (EMA) concluded this week that the available data “do not support its use for COVID-19 outside well-designed clinical trials”. The decision comes just two months after Slovakia and Czechia became the first EU countries to approve the temporary use of ivermectin against Sars COV-2.
In the US Ivermectin is not yet FDA-approved for the treatment of COVID-19, but in January the NIH changed their recommendation for the use of ivermectin in COVID-19 from “against” to “neutral”. This is a major step forward. As a result, doctors are at liberty to prescribe ivermectin for Covid patients.
But most regulators and expert panels insist that definitive proof is still lacking, despite the abundance of real world data, and have called for randomized placebo controlled double blinded studies. But that is time consuming and time is a luxury most doctors and their patients can ill afford right now. As covid continues to rage and patients continue to die, growing numbers of doctors feel that the risk of doing nothing, particularly in the early stages of the illness, significantly outweighs the risk of doing something — especially if that something has already been shown to work across multiple trials and real-world experiments.
“Clinical trials take time, but because of the abundance of overseas data, it may not be necessary to conduct clinical trials in Japan,” says Omura. “Experts have shown the numbers and announced that they are working. Therefore, I would like [the Japanese health authority] to grant it special approval. If you do not use it here, what is the special approval system for? Some people will die if they are waiting for a clinical trial.”
According to a WHO-sponsored review and meta-analysis of 18 clinical studies, the drug could cut the number of deaths from Covid-19 by as much as 75%. Crucially, some of the studies suggest that it is effective not only as a treatment in the early and later stages of the virus but also as a prophylactic. Yet the conclusion of the WHO-sponsored review is that more studies are needed.
Contrast this with the FDA and EMA’s mad rush to approve the anti-viral medicine Remdisivir for use against SARS-CoV-2 last October, despite the medicine’s lackluster performance in clinical studies and unproven safety record. On October 15, results from WHO’s Solidarity trial suggest that remdesivir does not even reduce mortality or the time COVID-19 patients take to recover. Yet a week later the FDA approved the drug for use against SARS-CoV-2 in the US, becoming the first drug to receive that status.
With a five-day course of treatment costing around $2,600 per person, there’s a lot of money to be made for remdesivir’s manufacturer, Gilead. Once remdesivir was approved in the US and the EU, it set off a cascade of approvals across the world, including in countries such as Brazil and Mexico whose public health systems cannot possibly afford to administer it on a large scale. In this case that is a good thing given how ineffective the drug appears to be.
Meanwhile, a Nobel-prize winning medicine that has been used extensively for four decades and costs just a few dollars per course of treatment could prove to be one of our best lines of defense again covid. Time and again it has been shown to work. Yet for the moment most health authorities in advanced economies — and quite a few in less advanced ones (South Africa, the Philippines, Peru…) — do not seem to be interested. In the coming days the World Health Organization is expected to come out with a definitive recommendation for or against ivermectin. If it opts for the latter, the pressure on doctors to stop using it will only increase.


[Edited: Just re-read the article & the WHO review mentioned could be the one I link to here….]
You may also be interested in the work of Dr Andrew Hill (of Liverpool University) who has been working with the WHO on drug repurposing (and has done for some time on all sorts of drugs) and produced this pre-print (see link).
https://www.researchsquare.com/article/rs-148845/v1
He’s on twitter @DrAndrewHill, but has gone quiet regarding some of his findings. Some twitter sources suggest that his current caution is due to pressure from his sponsors. He DMed me on twitter to say he’s still working on it though and there’s more in the immediate pipeline. I can imagine not wanting to get involved in Twitter to-and-fros could be a more simple explanation for his reticence.
Very interetesting and balanced look at the medicine.
I don’t know if this is intentional but the images are missing for me though.
Huh, I see them in Safari, Firefox, and Chrome, so I am at a loss to explain why they aren’t loading for you. Apologies.
I’m using Firefox and can see the images.
I’m using Firefox and have to right click on the word “Image(n)” then click on “view image” and it opens. Then use the back arrow to return to the article.
With respect, this article is far from balanced; it’s unabashedly pro-ivermectin. It does not even casually mention, let alone attempt to rebut, the case against using ivermectin, which is that it causes liver damage at higher doses, and it’s mostly higher doses that have shown promise for treatment of COVID-19.
The higher dose claim is false. The Lancet that found it was effective but what it contended was a high does was in vitro and on a sample of only 24! It’s a joke. And only a single dose when most MDs who treat early do more than one dose.
From an MD in a hospital system where he and other doctors have been using Ivermectin who was one of the readers we had review it in advance:
Drs. John campbell & Tess Lawrie have been conversing about the potential effectiveness with regards to covid & safety in general of ivermectin recently
https://youtu.be/vYF8bnmdQfY
A clinical trial research doctor doctor at University of California at San Francisco said Ivermectin trials were inconclusive, then said downsides were that oral dose necessary for antiviral effect was too high, and that because it was a veterinary medicine people were self-administering and overdosing (which I think is utterly irrelevant to question of whether it works when human formulations are administered by physicians.) I think she was probably citing Lancet study but don’t know. Seems overly negative to me, especially since the only safety concern she raised was about desperate people eating horse wormer.
https://www.youtube.com/watch?v=WXv8nBUdUSg
(32:20-34:45)
I will confess to not having watched the video. However, the use cases are as a prophylactic and VERY early in the infection process. Later is no good and the studies with negative findings are pretty much all on later stage use.
Look up Dr. Tess Lawrie and her meta-analysis of IVM.
She is an MD, PhD with a company that solely reviews research for accuracy and reliability (and has been employed by the WHO). She is stunned at how IVM is being ignored and lied about given what her meta-analysis has found.
https://www.facebook.com/watch/live/?v=290382055887781&ref=watch_permalink
You know the saying “the dose makes the poison”? Ivermectin, like most anti-parasitic drugs, is pretty hard on the liver. It’s only “well-studied and well-tolerated” at low doses for short courses–long enough to clear a parasitic infection.
The main counterpoint to using Ivermectin is that the (still fairly weak) evidence supporting its efficacy against COVID-19 suggests that it would require doses significantly higher than the currently-accepted safety threshold. It may well be worth the trade-off in some cases, but promoting it as a DIY treatment is deeply irresponsible.
As indicated above, that is not the experience of MDs who have been prescribing it for Covid. They have not had to use high doses to achieve results.
Another report by e-mail from a doctor late January:
This is not the same use case as for Covid but an HIV prophylactic would be unlikely to be at lower dosage levels than for Covid. It is hard to imagine that clinical trials would be authorized at a dosage level that would pose a danger to the liver….it would get knocked out at the safety phase.
There was an early in vitro study that found IVM had antiviral effects but at a very high tissue loading. Dr Kory addresses this in a video, IIRC with Dr Been.
The in vitro study was in chimp kidney cells. When it was re run with human lung cells, there was anti viral effects at a safe tissue loading.
And all the studies showing efficacy have been generally run at a known safe dosage level of 200mcg/Kg. One or two at 400mcg/Kg, still well tolerated.
Who is promoting it as a “DIY” treatment? All examples given in the article and Yves’ comments indicate that keen medical supervision is taking place when this drug is being used off-label to treat Covid-19.
No one in the article suggested a DIY treatment. We are simply exploring the FACT that its is apparently effective, cheap and easily distributed. So why aren’t we looking this way?
Bjorn, Perhaps you are playing Devil’s Advocate, and I appreciate that. However, let me respond to your comment “but promoting it as a DIY treatment is “deeply irresponsible”. That, of course is exactly what our CDC recommends if you “feel symptoms”. The CDC has been deeply irresponsible as of late and noticeably less effective than the 40 year use of Ivermectin has shown to be. Directly from the CDC’s guidelines: “Stay home. Most people with COVID-19 have mild illness and can recover at home without medical care.” “Stay at home” I read as DIY. Source: https://www.cdc.gov/coronavirus/2019-ncov/if-you-are-sick/steps-when-sick.html.
Regarding Hepatotoxicity AKA “liver damage”, the 1 (yes one) person with possibly associated liver damage, after 29 days, she was fine. Source from NIH/CDC Drug info. portal: https://www.ncbi.nlm.nih.gov/books/NBK548921/
Lastly, there have been no deaths directly linked to the use of Ivermectin in the over 3 Billion doses administered. That is a fairly large test group. As is often said, “Try it, you my like it.” That’s only possible if you can find it. Here in the US, lots of pressure is being put on doctors NOT to prescribe it, sadly. I can’t imagine why!
Bjorn; can you point to any studies of the current dosage being used for Covid 19 and liver disease? thanks
If ivermectin is so hard on the liver, why is it used as prophylaxis in nursing homes and prisons to prevent scabies? Note that like for covid, it is an off-label use, yet no one has questioned it.
It has been dosed throughout Africa for decades by non-medical professionals to prevent river blindness. Over 4 billion doses have been administered.
It has an incredible safety profile, with possibly two associated deaths related to parasitic treatment. Ibuprofen is associated with over 16, 000 deaths a year in the U.S. alone.
I fail to understand why people are so worried about giving it to the people most vulnerable to covid (nursing home residents) to prevent death, but never questioned its use on non-sick residents to prevent itching. Who is doing the risk-reward calculation here? How many people died alone, saying goodbye over FaceTime, because no one had the courage to use a cheap, safe, effective drug? And if not ivermectin, why not bromhexine, fluvoxamine, colchicine, etc?
There seems to be an Emergency Use Authorization induced blind spot. Apparently, in order to get their EUA, vaccine manufacturers have to show there is no effective treatment. It’s unconscionable that they couldn’t have adapted to a pandemic situation and changed the rules to allow therapeutics and EUA vaccines to co-exist.
Thank you Rob for your comment. Now I have insight into why everything that is not vaccine related is being so heavily challenged with made up statistics of lack of efficacy and safety concerns when years of use and tens of thousands or even billions of dosages administered showing efficacy and highly safety data instead. The falsely created studies published in the Lancet and JAMA were completely refuted and retractions printed within weeks that were negative about the use of HCQ, but the damage was done and the drug was removed from approved treatment by the US government FDA and never reinstated. Its the EUA requirement and money to be made by pharmaceutical manufacturers. We will never know the true numbers of the loss of life due to the almighty bottom line of profits. I’ve lost 14 family/colleagues (11 of which were MD’s and RN’s) due to COVID-19. The first was an ER physician treating positive patients and the most recent was my Mother who died without treatment before finally being admitted directly to the ICU to die 14hrs later.
Look up Dr. Tess Lawrie and her meta-analysis of IVM.
She is an MD, PhD with a company that solely reviews research for accuracy and reliability (and has been employed by the WHO). She is stunned at how IVM is being ignored and lied about given what her meta-analysis has found.
https://www.facebook.com/watch/live/?v=290382055887781&ref=watch_permalink
You are obviously reading from some misinformed articles as the dosages used are far within the accepted safety thresholds being used by medical doctors worldwide. Nowhere in the article implies using it as a DIY medication. Your whole response brings in to question your motives for posting except to discredit the research.
I respectfully disagree with your statements that it is pretty hard on the liver. If you read the primary literature, they describe any toxicities and the main one mentioned is headache. Furthermore, if you check Vigiaccess (the WHO approved toxicity monitoring site) you will see that ivermectin has a remarkably low number of incidences reported. The evidence supporting its efficacy is certainly not “fairly weak”. Tess Lawrie is a veteran meta-analyst with over 50 Cochrane reviews to her credit. She says that further “gold standard” trials will not shed any light on ivermectin’s efficacy because it is clearly efficacious; they could only give us better estimate of the magnitude of its effectiveness.
Ivermectin was mentioned multiple times in the Judicial Watch FOIA as an early treatment at the outset:
https://www.judicialwatch.org/wp-content/uploads/2021/03/DCNF-v-HHS-Nov-2020-00149.pdf
I did a search on ivermectin in that 302 page document and can find no mention. Admittedly my iphone search capability of a pdf may not be great (or it is only in images). Can you state at least one page on which it is mentioned? Thx.
You can’t get anywhere near the MIC [minimum inhibitory concentration] with a reasonable and safe systemic dose of ivermectin, but you can greatly exceed the MIC in the nose and nasopharynx by applying 1% ivermectin cream [Rosiver (Canada), Soolantra (US)] on a Q-tip deeply [3/4 of the length], so LOCAL application of ivermectin PROPHYLACTICALLY is about the only [maybe effective] way to use ivermectin in the context of Covid. I have been doing THIS twice a day for about a year now, because SARS-CoV-2 starts in the nose and nasopharynx, then [usually after a day or two] starts to move down into the lungs. I also rub ivermectin 1% cream on my eyelids twice a day, for what that is worth.
I have completely unrestricted access to ivermectin, but there is NO scientific basis for taking it systemically, and I certainly WOULD NOT do that!
Results from at least 5 randomized clinical trials are expected soon that might further inform the decision. NIH treatment guidelines still recommend against use of ivermectin for treatment of COVID-19, a recommendation I support pending further data — we shouldn’t have to wait long.
https://www.webmd.com/lung/news/20210309/fda-warns-against-using-ivermectin-to-treat-covid-19
I suggest you check the FLCCC site for their research papers and clinical results. Here’s a link to one paper pdf.
https://covid19criticalcare.com/wp-content/uploads/2020/11/FLCCC-Ivermectin-in-the-prophylaxis-and-treatment-of-COVID-19.pdf
The NIH guideline on ivermectic is Neutral, neither for nor against.
Recommendation
There are insufficient data for the COVID-19 Treatment Guidelines Panel (the Panel) to recommend either for or against the use of ivermectin for the treatment of COVID-19. Results from adequately powered, well-designed, and well-conducted clinical trials are needed to provide more specific, evidence-based guidance on the role of ivermectin in the treatment of COVID-19.
https://www.covid19treatmentguidelines.nih.gov/antiviral-therapy/ivermectin/
Thank you for this correction. It’s frustrating how much misinformation is out there. This neutral position is the same as for monoclonal antibodies and convalescent plasma, yet no one seems to question those.
“…there is NO scientific basis for taking it systemically, and I certainly WOULD NOT do that!”
So are you saying that the data cited by the FLCCC and others are worthless? If so, on what basis? Are they lying? Or is their evidence just not “scientific” enough? If the latter, what constitutes a “scientific” observation? A particular methodology? Or a particular set of authorities?
I am not dogmatically asserting a position on this issue; these are legitimate questions. This issue is extremely frustrating for those of us who have both an interest and some background in evaluating evidence, and yet continue to be confronted by such contradictory statements (often leveled with certainty). It is interesting to compare the FLCCC overview posted by Flora with the WedMD article. The latter strongly implies that (1) there is no evidence of Ivermectin effectiveness, and (2) it is potentially dangerous. The first conclusion is supported by one small study published in the JAMA. The second conclusion is based on the possibility that people will self-administer with horse pills. The author is not a scientist or MD, but a journalist.
Again, I am open-minded about Ivermectin. I have already received my first vaccination (it was Pfizer); I’m not some “fringe” anti-vaxxer. But the ferocious pushback on pretty much any treatment that looks promising by the medical establishment is quite striking. Especially when considering the few exceptions:
“Contrast [resistance to Ivermectin] with the FDA and EMA’s mad rush to approve the anti-viral medicine Remdisivir for use against SARS-CoV-2 last October, despite the medicine’s lackluster performance in clinical studies and unproven safety record. On October 15, results from WHO’s Solidarity trial suggest that remdesivir does not even reduce mortality or the time COVID-19 patients take to recover. Yet a week later the FDA approved the drug for use against SARS-CoV-2 in the US, becoming the first drug to receive that status.”
This COVID experience has been very depressing for many reasons, at many levels.
flora at 8:00 am points to a link at the FLCCC site. The FAQ on that site addresses many/most/all of the questions I have seen raised in comments to this post: FAQ: https://covid19criticalcare.com/ivermectin-in-covid-19/faq-on-ivermectin/
The FAQ includes the following interesting statement in response to a question about NIH recommendations:
“We are unable to identify a consistent approach to the strength and timing of NIH recommendations and/or updates to the recommendations …”
“but there is NO scientific basis for taking it systemically, and I certainly WOULD NOT do that!”
that seems a bit hyperbolic doesnt it given the numerous studies done to date? I admit they are not of the quality we would ideally see. But then we do see quality studies of remdesivir and i bet you would reach for that in an instant
As a microbiologist, I must beg to differ. There is in fact a lot of evidence from overseas and even in the US supporting ivermectin use, and for internal use. I am at a loss to understand where your claim about high dosage levels comes from.
I have read enough to conclude that ivermectin should be used for the following reasons:
It is well tolerated, with few side effects.
It is cheap and widely available.
Extrapolation from studies in vitro (in cells, not organisms) to conclude that effective dosage in patients would be too high is a stretch. The proposed mechanism of interference with proteins (importin alpha/beta1) that are required for viral replication is reasonable and supported by published evidence. As a cell biologist, it seems to me that such antivirals will be necessary to manage COVID-19. Yes, concentration matters. But a priori, this is not a reason to rule ivermectin out of court. Natural products do work! Artimisinin for malaria, for example. Known as a folk remedy for over a thousand years, not a drug of choice for malaria.
The evidence reported by physicians around the world supports continued use of ivermectin (IM Doc, for example). The drug doesn’t hurt and seems to help, a lot in some cases. This is more than “anecdata.” There is a proposed mechanism that makes sense, for example.
Thanks for that Nick.
This is likely not all that pertinent, but I was thinking about a relative a few days ago & how he only survived WW2 because he was fortunate in getting penicillin, which due to the huge effort made to develop the drug resulted in the saving of an estimated 80,000 Allied soldiers.
I had a gander on the Web to see if I could find out the details of the above effort & found an article by Roswell Quinn MD, PhD from 2013, in which he bemoans the lack of effort in research into new antibiotics to counter the growing immunity, while describing the effort that went into the drugs original development & use as a comparison to how things were done then & how the civic duty side of that effort has since been abandoned – Lister for instance chose not to patent his discovery.
It appears to me & much more venerable others that potential Covid treatments are being held back due to financial considerations – here is the Doc’s conclusion.
” Current policy efforts concerning antibiotic research and development overlook the relationship between intellectual property rights and the equitable distribution of scientific resources. Economist Michael Perelman notes that the free flow of information has been the hallmark of scientific progress, yet in recent decades corporations have curbed this flow by obtaining expanded patent rights, thus introducing inefficiency into the nation’s system of scientific production. In 1945 The history of penicillin demonstrates how the reverse can be true: by prioritizing scientific rather than economic goals, the penicillin collaborative spurred tremendous scientific innovation and industrial growth “.
In reminds me of the title from a song by Mtume that was popular in Manchester clubs in the late 70’s – ” It don’t have to make sense, just cents “.
https://www.ncbi.nlm.nih.gov/pmc/articles/PMC3673487/
Thanks, well stated… This is one place I got stuck…
“Yet despite the growing body of evidence supporting ivermectin’s therapeutic effects against SARS-Cov2, national and supranational health authorities, particularly in more advanced economies , are dragging their feet. ”
Why is it not stated as “more advanced countries”
Counties have citizens while economies have consumers?
My cynicism will be well rounded when pfizer comes up with a patented reformulation.
Look up the antiviral drugs they (Pfizer) are developing for treatment of SARS CoV-2, as well as Merck’s announcement last month of their new antiviral that is set to be released next month (May 2021). Interesting how the negative announcement by Merck’s hugely successful run with Ivermectin was put in the background as Merck announced it was unsafe for use and no pathway was known for its use in treating covid-19.
Piecing together some quotes from each source below suggests an interesting story behind the ascent of Pfizer:
“The History of Pfizer and Penicillin, and Lessons for Coronavirus
A ‘scientist general’ to coordinate private and public efforts can lead the medical response.” WSJ March 20, 2020 available at https://www.bahcall.com/wsj_oped-coronavirus/
“A BRIEF HISTORY OF PFIZER CENTRAL RESEARCH” Lombardino, Bull. Hist. Chem., VOLUME 25, Number 1 (2000) http://acshist.scs.illinois.edu/ bulletin_open_access/v25-1/v25-1%20p10-15.pdf
“Fleming’s discovery in 1928 that a penicillin mold killed bacteria lay dormant for a decade because he couldn’t isolate the active ingredient and make enough of it for testing.” (WSJ)
“In the 1930s, Pfizer was a small Brooklyn-based chemical company known mostly for making vitamins and the citric acid used in Coca-Cola.”
“Working out of an old ice factory near Pfizer’s offices in the Williamsburg neighborhood, they built a commercial-grade manufacturing plant in four months.” (WSJ)
“So Pfizer, in 1941, was asked by the US and British governments to accomplish large-scale penicillin production by means of deep tank fermentation. Merck, Lederle, and Squibb were also asked to join in this effort, with all the companies required to share their findings.” (Historical Chemistry)
also:
“Pfizer’s work on penicillin for World War II becomes a National Historic Chemical Landmark”
https://www.acs.org/content/acs/en/pressroom/newsreleases/2008/june/pfizers-work-on-penicillin-for-world-war-ii-becomes-a-national-historic-chemical-landmark.html
I didn’t see it mentioned in the article but India has also had success with Ivermectin. In Aug 2020 Uttar Predesh, India’s largest state added Ivermectin as a treatment and distributed it free to the populace for home care. The state of Bihar followed. By the end of 2020 these two states had the lowest fatality rates from Covid in all of India.
“Ivermectin prophylaxis leads to 73 per cent reduction in Covid infection: AIIMS-Bhubaneswar study” — This report in The New Indian Express from a few months ago is from the eastern state of Odisha:
BHUBANESWAR [the largest city in the state of Odisha]: In a significant finding, two-dose Ivermectin prophylaxis has led to 73 per cent reduction in COVID-19 infection among healthcare workers (HCWs), who are more likely to contract the virus given their nature of job.
The findings of the study conducted by AIIMS-Bhubaneswar between September 20 and October 19 is set to give a new dimension to the ongoing research on the behaviour of SARS-CoV2 and prevention and treatment of COVID-19….
https://www.newindianexpress.com/states/odisha/2020/nov/05/ivermectin-prophylaxis-leads-to-73-per-centreduction-in-covid-infectionaiims-bhubaneswar-study-2219438.html
Here’s and interview Dr. Campbell (PhD) did about 3 weeks ago with Dr. Tess Lawrie (MD & PhD) going over her Ivermectin research and other studies. It’s about an hour long.
https://www.youtube.com/watch?v=vYF8bnmdQfY
It’s also my understanding that several trials with ivermectin have been stopped. Not because they were getting bad results, but because the results were so positive that it was becoming unethical to continue to deny control patients the medication.
Thanks for this article. The same people who tell me to ‘trust the science’ seem mighty determined to ignore the science showing an inexpensive, off-patent drug has beneficial results used against a C-19 infection. The Netherlands, for example, will now issue high fines to doctors who prescribe Ivermectin for C-19. (You can run this link through google translate.)
https://www.medischcontact.nl/nieuws/laatste-nieuws/nieuwsartikel/hoge-boete-voor-artsen-die-onterecht-hydroxychloroquine-of-ivermectine-voorschrijven.htm
Have to wonder if the vehemence of the pushback has to do with the fact that the Emergency Use Authorization for the Covid vaccines requires that there be no effective treatments.
Another big issue is that it’s very hard to justify the high cost of funding clinical trials for cheap, off patent drugs. The math does not work.
A lawyer sent a similar comment by e-mail:
Interesting, thanks. Does anyone know if the same applies to the EU, i.e. EMA’s vaccine approvals?
This European Medicines Agency (EMA) website probably contains an answer to the question.
https://www.ema.europa.eu/en/human-regulatory/overview/public-health-threats/coronavirus-disease-covid-19/treatments-vaccines/covid-19-vaccines
You’d think under certain circumstances (like a pandemic) there would be an exception process..
I’d think that the Emergency Use Approval was such an exception process.
It was never never never intended to approve medications for mass use. It was meant for cases like “med is in pipeline and no red flags so far but some people who are very sick want it NOW” and the EUA is to allow what was until now a small number of people to have it.
As the “Masters of the Universe” like to say: “Rules were made to be broken.”
[Look where that has gotten us over the last decades.]
The way hydroxychloroquine was treated looked very strange. I had never seen anything like it. As if a PR company, or a bunch of them, were monitoring every post, every video, every magazine article around the world, and then massively trolling against any positive results. And as if someone was paying corrupt medical companies to produce fake studies that showed HCQ kills, and then get them into the Lancet.
Ditto the war now on the Astra-Zeneca vaccine.
And the war on Ivermectin is not so heated yet, but will ramp up if it starts to look as if it is being used.
Just “ordinary” people on FB and blogs and letter to papers, saying this is Dangerous, it will Kill, stuff like that. Getting doctors to say the same. Do doctors ever shill for money?
And so seeing this piece of info on EUAs and the caveat that nothing else must be available that treats, bingo!
The way HCQ was maligned was indeed remarkable. It has been shown to be effective when combined with zinc and used very early (within the first five days of symptoms). The studies using toxic doses in people with advanced disease to discredit its use were the equivalent of studying seatbelt use AFTER an accident and concluding that seat belts were of no use.
Yves
Why is the history of the Phizer/Moderna drug emergency approval a nearly unknown story? The successful War on HCQ is ramping up to be repeated with Ivermectin. Yet even among your much more sophisticated audience it receives only your short mention and one other note
.
FOLLOW THE MONEY– The first step in investigating any crime.
Two necessary conditions had to be created for the Phizer/Moderna non-vaccine genetic engineered therapy to gain emergency approval.
1- The applicants had to demonstrate that there were no other effective treatments for the target disease. Hence the War of HCQ consisting of fraudulent studies and data, many of which didn’t stand two week’s scrutiny. But with the massive censorship and disinformation campaign available to the Pharma Pushers, facts had little power.
2- The Gene Therapy developers, corporations, and executives required that they be granted total immunity from any future liability. What did they know and when did they know it?
How was the Pandemic Fear campaign organized, or did it grow organically once the gasoline and matches were introduced?
(as an aside, the Moderna Corporation burned through four billion dollars of investors’ money trying to develop a mRNA delivery system for rare and exotic diseases (of the type they could patent and charge $80,000 per year for) They failed to reach even the stage when they could begin to test it on humans because they couldn’t keep their animal subjects alive after being “vaccinated”. And then along came Corvid and suddenly they had millions of human guinea pigs eager to act as test subjects in order to be allowed to fly on airlines or return to work in the Land of the Free)
(Opinion) The mass casualties resulting from HCQ and Ivermectin suppression would put Dr. Melenge’s horror chambers to shame if there actually was justice available through a Nuremberg trial
(In the spirit of “Follow the Money”, dare any researcher dive down the Moderna rat hole. I suspect they wouldn’t need to go very far before finding financial connections to both Bill Gates and Fauci. Good luck getting it published!
We have seen fatally flawed studies being pushed in publications like The Lancet so I am now assuming that modern medicine has been compromised. Especially when you ask major organizations like the WHO and the CDC about things like masks and aerosol spread and they reply ‘Nah! It’ll be fine!’ Here is how it should work. You try a bunch of stuff and see what works. If something does work, you immediately follow it up with a view to deployment in mind. That is what they did in South America and I am here to say that an empirical approach to medicine is not the worse way that you can go.
Yes Rev, Dr. Pierre Cory during one of the FLCCC weekly updates a couple of weeks ago, through gritted teeth reported the fact that a peer reviewed trial had been rejected by the editors – this trial will now be available within the May issue of the American Journal of Therapeutics..
Obviously proper trials are important for medicines, but in any case should not substantial evidence based on observation at least be a basis for investigation ?
Perhaps it is also a case of having gone so far down the road of blocking the drug, they are in a situation in which they have to dig their heels in further, as if it were to become widely known that they have failed in at least examining something that could have saved many lives, it would likely not reflect very well on them.
For me, the big takeaway here is not whether or not Ivermectin is effective or not – I’m not qualified to judge. What is most striking is that more than one year into this pandemic we still do not have a clear set of comparative studies of the most common likely protocols and drugs to provide any good quality data on the best way to treat all stages of the virus. Medical authorities and individual doctors still have to pick their way through a massive thicket of competing and often very substandard (and frequently biased) studies. I would hate to be a doctor trying to work out the best way to treat my patients from the available data (doctors I know frequently tell me they are relying as much on personal intuition and experience as the latest ‘official’ recommendations).
This is a colossal failure of medical science and public health policy.
“we still do not have a clear set of comparative studies”
You are mistaken by a mile: 48 trials of which 25 randomized control: https://c19ivermectin.com
All the rest is Big Pharma disinformation.
See also for up to date commentary: https://covid19criticalcare.com
As and when all the Covid dots are connected, this will prove to be the biggest, deadliest fraud on humanity, ever.
It seems you abruptly stopped reading PK’s post.
Your (first) link does not speak to that.
With all due respect, this site is a lot better when it sticks to economics. The article mentions Mexico and Brazil, two countries widely criticized with disastrous handling of the pandemic, as some sort of example when it comes to ivermectin. I live in Brazil: aside from a few lunatic doctors, no one is seriously prescribing ivermectin. The only local adherents are the denialists who refuse to use masks and keep distancing, and use the fact that they’re on chloroquine and ivermectine as an excuse. And people are dying like crazy because of that. Those are the same people who’ve been taking veterinarian medicine and other crazy stuff as if there was a conspiracy to force them to vaccinate. The idea of a “silver bullet” is being sold to this crowd and bringing with it only death.
Our far right wing president changed Health Ministers three times already, and everytime he tries to put someone in charge that will defend these medicines as a way to “keep the economy open” despite the deaths. Local chloroquine supplies are low for yellow fever disease, which is the one use of it which is scientifically proven. The government delayed or downright refused offers to buy vaccine in the end of 2020 based on this stuff, resulting in our current record daily deaths. It only decided otherwise when an opposition governor bought them on the side and made them look bad. Higher ups at government openly accuse China of being responsible for the “comunavirus”. That’s the kind of people that defend chloroquine and ivermectin over here.
Data is data and it sure looks like you didn’t read the post and are wedded to your priors. The bit about Brazil is about one city, Belem, that has had markedly different results than the rest of the country. Did you not see the chart with the big, sustained fall in death rates since May, fer Chrissakes?
Ok. I hate that I respect you so much and love this site overall when it comes to economics but whenever someone disagrees with you you can’t help but take a condescending tone. But let me provide one example of why the guy’s video is based on partial/unreliable info at best:
When he compares numbers of cases from last year and says the reduction is greater on cities with ivermectin distribution campaigns, one element that is neglected is that, as I said in my previous post, no doctors are taking these “campaigns” seriously. They’re not prescribing, and the “campaigns” are falling on deaf ears. I live with people working in the frontline. There is absoluterly no evidence in Brazil of cities that are better off for making mass distribution of ivermectin because it is not being distributed massively at all. A few loons are the only ones taking it.
There are a lot of intervening factors to be accounted for that aren’t mentioned in these tables/graphs, the major one being that adherence and policing of lockdowns and distancing measures in Brazil vary WIDELY ” from city to city, not state by state, depending on whether the local government is a denialist or not. As an added example, one of the cities mentioned, Itajaí, for instance, is a coastal port city with a lot of turism nearby, being compared with a country city, Chapecó, which is far from turism centers and in which any lockdown/distancing measures would have a proportionally lower impact because, you know, they didn’t have that much outsiders going by in the first place, which can perfectly explain why one would have a greater reduction in cases than the other, without having to resort to ivermectin as an explanation at all.
Pairing by population alone two cities and comparing them is absolutely inadequate to produce any sort of serious epidemiological evidence in a complex situation like this. And, in this case, it leads to more misinformation which in turn costs lives.
While I appreciate the kind words about the site, you come on super aggressive with no factual backup and you expect not to get whacked for an almost entirely emotional comment? Come on. You attempt to dish it out and then you get all huffy when you get treated in kind.
You’ve only given a handwave with respect to Belem. Unless you can demonstrate that it had superior practices with respect to some other aspect of Covid management (lockdowns, mask mandates, quarantine enforcement) you have not disproven the thesis that Ivermectin had a significant impact there, particularly since the decline corresponds in time with Ivermectin uptake. A narrow claim was made and you haven’t come within hailing distance of debunking it. Ivermectin was a significant intervention there. Can you point to anything else?
Moreover, you have just contradicted your initial claim that Covid management all over Brazil is a train wreck. Now you are saying particular locations are doing a pretty good job. So which is it?
I’m sorry if I came across as agressive. Let me note that I started my “super agressive post” with “With all due respect”. Apparently, I’m being agressive if I state the opinion that this site is better when it keeps to economic subjects, which I fail to see as an agressive opinion by itself.
The fact that I mentioned other flaws in the video was a matter of ease of access of points to argue. Chapecó and Itajaí are in a neighboring state and I happen to know more about both to an extent. But before I get to Belém, let me note that you got nothing against the point I made about the inadequacy of the comparison of these two cities. That they’re even called “neighboring” when 530km separate them speaks volumes about the quality of the research by itself.
But let’s adress Belém. Belém is the capital of one of the poorest, worst quality of life states in Brazil. To be blunt, no one wants to live there and it is hardly an example for the rest of the country on absolutely anything. Social inequality in Brazil is huge and Nothern and Norhteastern states have the short end of the stick.
In a 3 minute search on google, I found three press articles about the improvement of the covid situation in Belém and the state as a whole. You’ll have to forgive me and trust my word on them because they’re in Portuguese.
https://agenciapara.com.br/noticia/20697/
This one is from a state agency. It mentions the fall in cases as a result of the significant increase in the availability and coverage of medical care in the state from the middle of May onwards. Several units were diverted in their purpose to treat covid patients. Maybe it isn’t clear for outsiders, but a lot of people die in Brazil due to missing healthcare, such as asfixiation due to lack of oxygen, and lack of spots on intensive care units. There is no mention of ivermectin there, and a government agency would have all the interest in making it known if it were relevant, to gain political leverage.
https://g1.globo.com/pa/para/noticia/2020/07/23/belem-diminui-casos-e-mortes-de-covid-19-mas-tem-taxa-de-letalidade-duas-vezes-acima-da-media-nacional.ghtml
This one is relevant because it also mentions that, despite the fall, at the time the lethality rate was still double the national average, hardly something to be proud of.
https://g1.globo.com/pa/para/noticia/2020/05/25/lockdown-em-belem-e-outras-cidades-termina-hoje-saiba-o-que-muda.ghtml
Finally, this one shows that a lockdown was put in effect in May in Belém and other cities, which, I think, makes it very clear that there is a solid explanation for the reduction without resorting to ivermectin. The graph does not mention this important detail.
Let me make one thing clear: I’m not a shill of Big Pharma, I hate them as much as the next guy. But the evidence for ivermectin in Brazil isn’t there. It’s easy for outsiders to look at a table and think they got the whole picture. What I hope to have demonstrated somewhat, whithin the constraints of the time I can dedicate to internet debating, is that there are a lot of other factors in play when you talk about real time epidemiological behavior, and making hasty conclusions about it by cherry picking cities under false assumptions is hardly sound science, and it’s also costing lives. I speak from the place of a person who has to reinforce daily basic measures amongst family, friends and in the workplace because I’m seeing people losing their loved ones mainly due to ignorance, and in the end they’d have a field day if they could read articles like this. And it would be disastrous.
“With all due respect” is a formula for signaling sharp disagreement and attempting to dress your interlocutor down.
Your lengthy discussion of Belem still fails to rebut the point made in the point: the rest of Brazil saw an explosion in cases in November and not Belem. Improving medical care and the lockdown explains the fall in May. The lockdown did not continue from May though now. It does not explain the failure to participate in the sharp rise, which by all accounts includes a troubling level of reinfections.
Ok, so the sharp fall in May means absolutely nothing in terms of evidence of ivermectin efectiveness. At least we agree on that. I think I’ve said everything I wanted on the subject. I showed that both brazilian arguments cited in the article (pairing cities without accounting for important differences and using the fall of cases in Belém after May as evidence of ivermectin efficacy) are shaky at best. I don’t have the time to dig evidence about november, though I’m sure it would end up going the same route with closer scrutiny, there are many intervening factors which could explain the difference.
It’s important that foreigners understand that we have a government that is currently more interested in stirring military interest in an autocoup (as it is predicting a loss in next years election) than doing what’s right for healthcare. Brazil is absolutely no example for anyone and people who cite whatever is being done here as some sort of example of best practice against the pandemic is terribly mistaken.
I had a long and detailed reply posted a few minutes ago and now it just vanished?
What was about it that you found worth of removing?
But let me try again in summarized form. Basically, nothing you mentioned counters the fact that the study compares two radically different cities that are 530km from each other and treats them as neighboring, which speaks a lot about the overall quality of the study.
I don’t mean to come across as agressive, though I fail to see what was agressive in my reply, which started with “with all due respect”. I thought this was an educated introduction of dissent in the US?
As for Belém, three press articles linked below say the city’s lethality rate dimished due to increase in health coverage in all levels (lots of people in Brazil die from covid related issues due to lack of intensive care unit spots to intern and even in some cases lack of oxygen) and a lockdown that was put in place in May to control the spread. No need to use invermectin to explain anything here.
https://agenciapara.com.br/noticia/20697/
Government one, makes no mention of ivermectin even tough it could get political leverage if it did.
https://g1.globo.com/pa/para/noticia/2020/07/23/belem-diminui-casos-e-mortes-de-covid-19-mas-tem-taxa-de-letalidade-duas-vezes-acima-da-media-nacional.ghtml
This mentions Belém still had at the time about twice the average lethality rate of the country.
https://g1.globo.com/pa/para/noticia/2020/05/15/lockdown-no-para-e-prorrogado-ate-24-de-maio.ghtml
This one mentions the lockdown.
I’m annoyed at the fact that half-assed studies are considered gospel sometimes when reality is a lot different. Real time epidemiological conclusions are very hard to come to and cherry picking cities under false pretenses or failing to acount for other factors definitely isn’t the way to make sound science.
People are dying daily here because of a denialist chlorochine-ivermectin-loving federal government. A few cities are doing something good, but overall the pandemic management in Brazil is atrocious, make no mistake. We’re a huge country, you have a lot of different realities going on at the same time here.
Makryu — I pulled your earlier comment into the backstage (where it is moderated, not deleted), because I wanted Yves to be able to deal with it on her own time. There are occasions where I feel (and the others will often agree) that Yves, Lambert, Jerri-Lynn, or guest writers should get a chance to react to a comment before it becomes an issue or kerfuffle for the entire commentariat. Please be respectful of our processes because their intent is to keep discussion maximally productive.
Perhaps you could site your sources. I cannot find any information or scientific studies about the use of chloroquine for yellow fever. The only effective treatment I’m familiar with is the prophylactic vaccine which is widely available in Brazil. I know there was a spike in cases in 2018 that resulted in a drive to vaccinate the entire country. I also know that there existed some amount of vaccine hesitancy at the time. If the vaccination drive was not entirely successful as a result, but it has been determined that chloroquine is an effective alternative, then that would be news to me. I am not dismissing the idea. Aside from malaria chloroquine is also used to treat amebiasis and has been found effective in treating rheumatoid arthritis and lupus, so there exists what is sometimes referred to as legitimate “off label use”. As far as covid 19 vaccines go it was publicly revealed in October of last year that the government of Brazil has a purchasing contract with AstraZeneca to pay U.S.$300 million even if the vaccine is never approved.
Sorry, I mistook from memory yellow fever with malaria, which is the disease chloroquine is used for.
Also, the Astrazeneca deal was pending approval and closed only under public pressure on the government. They refused deals of other companies, such as Pfizer, which would have delivered as soon as december. We don’t have even 10% of our population vaccinated so far.
https://www1.folha.uol.com.br/equilibrioesaude/2021/03/governo-negou-3-vezes-ofertas-da-pfizer-e-perdeu-ao-menos-3-milhoes-de-doses-de-vacina.shtml
The president has been speaking publicly against vaccination for months, amongst other stupidity such as promoting chloroquine and ivermectin. Federal government members say lockdowns “don’t work” because the virus is carried also by insects and animals and other such nonsense.
https://www.bbc.com/portuguese/brasil-56536892
Just a few examples.
With all due respect, what does the malign incompetence of the Brazilian federal government have to do with Ivermectin, beyond the coincidence that they are speaking well of it?
to restate a quote from an MD using the drug that Yves ran the piece by before she published it:
Is this MD engaging in stupidity, as you would have it?
Furthermore, this piece draws on data from other countries.
I have no position on this one way or the other. C19 is not really a medical emergency in my country right now. Consequently I am open to being persuaded one way or the other and am in no rush to take a concrete position. If your aim is to convince someone relatively neutral like me, though, that Ivermectin is a bad idea principally because your moronic president likes it, and by referring to its recommendation as a stupidity when the issue, it’s safe to say, is a bit more nuanced than that, well, that’s not very persuasive.
Thanks for this very relevant observation.
When I read this: “…aside from a few lunatic doctors, no one is seriously prescribing ivermectin. The only local adherents are the denialists who refuse to use masks and keep distancing…”
then I *know* that the information this person is trying to convey is not worth reading, because it is closed-minded dogma. “Lunatics” and “denialists” — clearly a smear meant to mislead the lay-person and link Ivermectin advocates with the worst “conspiracy theorists”.
It is possible to both respect professional expertise and reject dogma based on authority. Those of us with an academic background do both with regularity — or at least we should. As I have said elsewhere here, I am open-minded on this issue. Not an expert, but knowledgeable enough to know that the evidence in no way leads to the disdainful dismissal leveled by makryu — at least not yet. If you are indeed a medical professional, makryu, then I truly wish for a more open mind on your part. If you are a troll, then no sale here. Either way. if you want to be more persuasive I’d listen to Basil Pesto.
Read my other comments. Yes, the only people advocating for ivermectin here are denialists who don’t wear masks unless forced to do so, don’t keep social distancing and still insist in greeting you by touching your body. If I call them lunatics that’s because of what these other behaviors make them look like. I won’t hide that fact just because it makes people defending ivermectin look bad elsewhere. It is what it is.
That is absolutely false and a smear on Nick Corbishey, me, as well as on IM Doc, KLG, and other doctors who are experimenting with ivermectin. Take your tripe elsewhere. I’ve indulged you far more than I should have. You were arguing in bad faith and as predictably happens, you kept escalating rather than backing off or making narrower, substantiated claims.
and what it is is not remotely dispositive of the efficacy of Ivermectin. It tells us nothing about Ivermectin. It is merely a description of a group of dickheads. That doesn’t make people elsewhere who defend Ivermectin look bad, it makes you look bad for being susceptible to such poor reasoning. This is close to “Hitler was a vegetarian!!” territory.
Furthermore,
If you think Brazil’s a big place, try the world
Further to ChrisFromGeorgia’s comment below, it’s worth bearing in mind that, with regard to Pfizer and vaccines in Brazil:
That comes from this earlier story by Mr Corbishley, Pfizer’s sordid vaccine sales practices in Latin America could be a big boon for China and Russia
These are reasonable grounds to not deal with a company that go beyond simple vaccine denialism. In fact, they’re probably reasonable grounds to throw in a few choice words to said company’s representatives on their way out the door. If you were unaware of this action on the part of Pfizer in Brazil, it’s worth being aware of.
I’m not sure what happened with the AstraZeneca
deal so I can’t speak to that.
Well I see some dubious argumentative tactics employed here by the poster to assail the author’s work.
Guilty by association – just because some proponents of Ivermectin are also “right wing” or don’t believe that masks work, doesn’t mean they’re not right about Ivermectin. The “wrong kind” of people can be right even if by accident.
Factually dubious assertions – the reason Brazil and Argentina did not get the mRNA vaccines was because Pfizer and Moderna basically asked them to sign their countries away for purposes of indemnification.
I am sorry to say this, but I don’t read anything in your post that looks like science, more like a bad attempt to discredit a witness in a courtroom.
Since Chris said it first, let me just reaffirm his claim: “the reason …. Argentina did not get the mRNA vaccines was because Pfizer and Moderna basically asked them to sign their countries away for purposes of indemnification.”
If my memory does not fail me, Argentina was asked to sign over fishing rights, among other things, e.g.
in the space of 40 years ivermectin went from being a miracle treatment to hardly used for parasite control in livestock due parasite resistance. maybe something that should be of concern for covid treatment also.
40 years is a long time…..and I believe it’s still prescribed regularly for pets. There’s been tons of excessive drug use in livestock (most antibiotic resistance comes from the practice of giving antibiotics to healthy animals, it somehow helps in fattening them up for slaughter). I would not be surprised if ivermectin were similarly used widely as opposed to in cases of actual parasite infestation. Your language even suggests that: “parasite control”.
My dogs get ivermectin via their monthly heartworm pills, and we regularly gave it to our horses. I could go down to the feed store right now and find it on the shelf in the horse aisle.
The FDA recommends against using animal ivermectin! While veterinary grade is the same quality of manufacture as pharmaceutical grade, translating the animal dose into the human dose runs the risk of error. And the patient might also have conditions that argue against using it. “Generally well tolerated” absolutely does not mean “OK for everyone.”
Of course. I was just confirming that it is still being used for pets and horses.
When you cannot find a MD in your area who will prescribe Ivermectin for you, even when shown that the NIH has shifted their ‘recommendation’ to “Neutral,” you take what you can get.
So much of the Medical Complex is now “captured” by Big Pharma, one needs must ‘innovate’ in the acquisition of meds. That’s what we have had to do.
The math involved in translating the human dosing guidelines into “Veterinary Units” is a bit of a pain, but well within the capabilities of the average layperson.
As I have stated earlier, my cynical side tells me that Big Pharma will ‘approve’ of the use of Ivermectin only after a patentable, and therefore very expensive reformulation of the drug is developed and deployed.
When that happens, it will be time to start inflicting palpable pain on the heads of the Big Pharma organizations.
When you needlessly suffer from Long Covid, go long guillotines.
Agree. However, if you are run a big risk of dying from Covid and you have just been sent home with nothing, to live or get so sick its too late, then the motivation to do the maths correctly is very high.
I cannot argue with that.
This exposes a major flaw in the American “health system;” it’s ‘capture’ by avaricious entities.
I am quite puzzled by the “Left’s” lack of messaging concerning how the Pandemic is a perfect argument for a National Health System in America. That the so called “Left” in America is not in full on street demonstration mode over this subject is telling.
Even if you do the math to get the amount of active ingredient correct, might the tablets contain extra ingredients such as fillers that are not approved for human consumption? I’m no expert but just ask. If all the ingredients are listed on the box, then one should be able to answer that question.
I’ve used it for fleas in the past, but it’s safer for dogs than cats, for which I prefer selemectin (Revolution or Stronghold brands, for example) . BTW, don’t use pyrethroid, the synthetic on cats, but the natural pyrethrum (like from chrysanthemums, is usually safe. Cats are more sensitive to pesticides, especially synthetics, and I’m more careful now.
I’ve diluted selemectin, cheaper big doses for dogs, with ethyl alcohol, down to about .1 ml per pound for cats, applied topically, since I had many to treat for fleas. I spent a fair bit of time researching the subject.
What I have heard over the past months is that ivermectin is not promising at all and it’s use is not supported by research. https://www.microbe.tv/twiv/twiv-730/ podcast (time 24:23), ‘clinical update’, with Daniel Griffin PHD MD, is a recent discussion of it, and links to recent research (March 4) at https://jamanetwork.com/journals/jama/fullarticle/2777389.
This is one study and it is not the use case for the MDs that have found it to be effective.The big aim is to prevent hospitalization. The data in the post above (admittedly correlations in large real world settings but quite a few) plus tests run in hospitals (“Team Ivermectin” versus “Team Placebo” so these were real studies, admittedly small-ish scale) points to a real impact in enough different settings to suggest that there is a there there.. Selecting for mild cases means ones on track to hospitalization were excluded.
The other use case is as a prophylactic. That again isn’t what was tested in the one study linked to, which seems to be the basis for the podcast.
That podcast refers to the one paper, but there are many others. Tests in hospitals are not clinical trials, nor scientifically valid, with proper control groups of sufficient number. Other repurposed drugs have been and are being used, such as antiviral drugs, steroids, and anticoagulants (including aspirin), given in specific time frames, and even use of proning to help breathing (which Dr. Griffin was an early proponent of).
You say in the intro “First of all, I am not a medical doctor. This article is not intended as medical advice. It’s a layman’s account of how an extremely cheap, safe and widely available off-patent medicine called ivermectin appears to be saving the lives of countless Covid-19 patients across Latin America and beyond. Yet hardly anybody is talking about it. “.
Griffin is a medical doctor, actively involved in clinical work, as well as a PHD. Racaniello is professor of immunology, Barker a professor of immunology, and the other have similar qualification, not to mention the qualifications of the various guests. These are anything but laymen, or even run of the mill doctors, but top experts and researchers (including some who have done the original research on the virus and disease, and don’t refer to sources because they ARE the sources) who present podcasts which are listened to, and advise medical doctors. That’s why I have been listening to these podcasts for the last year: this is the best source I’ve found for reliable information.
Actually, I’ve hearing people talking about ivermectin for quite some time, and have seen much material about it, and despite being a layman, I have done a fair amount of research, including going through some course material on the subjects, having spent a few hundred hours going through it, and have a fairly well informed opinion about the pandemic, the virus, and the drugs and treatments — but with no comparison to the experts I’ve listening to, as referenced, who have spent decades immersed in the subjects. Don’t listen to me — listen to them.
Again, the studies I have seen that are negative were without exception not on the recommended use cases: 1. prophylactic and 2. very very early, at symptom onset. Later use is not/not very effective.
Yes, DRs. Racaniello, Griffin, et al, have said the real trouble with sar-cov-2 is not so much the virus itself but the immune reactions to it, and that includes long covid well after the infection is cleared. Same story with the convalescent serum and monoclonals or cocktails: they need to be given early while the viral load is still increasing.
The big problem here is that, in America at least, testing is an entirely slip shod affair. Finding a testing source that will do the testing without an MD approval is almost impossible around here. Thus, the issue of financial ability comes into play. You have to pay for the doctors ‘visit’ first, and then, around here at least, pay for the test and hope for reimbursement later. Many people here cannot afford even that level of expenditure.
It’s a perfect example of Neo-liberalism Rule #2 in action. [Go, die.]
Many, many people resort to DIY medicine in this case because that is their only feasible action.
The whole health care industry (can we call it a system) in the US is in shambles, and this pandemic is emblematic of that. When an empire collapses it takes a lot with it, but capitalism is as naked as the emperor with no clothes now. The economy, and medical care and research, is like a factory where the machinery is never maintained, or a farmer who never waters of fertilizes the crops — and then blames others who succeed in their businesses. We can see the results all over, and it’s not from just one party or something recent.
I understand vaccines and support vaccination generally, but I don’t trust the corporations, politicians, or media, since they all lie constantly about everything.
If I could get a Russian vaccine I’d jump at it right now, but mostly stay home, hesitate, to see how all this goes down — if the narratives and what is being said stands up over time, or if it’s like the unemployment figures, the propaganda against Russia, China,Venezuela, Iran, Iraq, etc. Even scientific and medical professionals can be fooled or lied to, as can the journals with the plethora of writing paper with bad research and preprinted without decent review, and the trash talk from those with financial or ideological agendas. I’ve become very cynical and skeptical over the years, living in a country where deception and greed rules, and corrupts most everything.
Yes, we do have an urgent care center nearby where you can get the antigen test (the fast one) IF you get there before they run out of tests for the day!!! WTF?!?!
And as most here know, the PCR test typically takes 48 hours for the test center to provide results, and during that window, the infection, if you are infected, can have made a considerable advance. So I agree with a separate concern, that our generally crap testing makes it hard to intervene early even when that might work.
Given the extensive compelling evidence of efficacy outlined here, the result in the Colombian study of no effect is puzzling. The explanation in the article about why the study was limited to “mild” cases (although “mild” in this case could include hospitalized persons not receiving oxygen) is this: “Viral replication may be particularly active early in the course of COVID-19, and experimental studies have shown antiviral activity of ivermectin in early stages of other infections.” Also, the drug was administered for five days–did the doctors who found IVM worked use it for a longer period with more severe cases? The Colombian study is the only one involving ivermectin that has received coverage that reaches the non-specialist reading public (such as me), so it gets little further attention while pricey alternatives do. I speak as a lay reader who is trying to follow these things.
The use case is prophylactic and early use, basically as soon as someone is found to be infected. Sorting for cases far enough along to be able to judge that they are mild looks to be largely too late.
We will now prepare for an avalanche of RCTs in hospitals followed by a establishment chorus of “It doesn’t work!”
From the JAMA article in your comment:
So I don’t think this one passes the Mandy Rice-Davies Test.
I wish somebody would do a RCT on study results that took conflicts of interest into account….
oh there are studies like that. Poke around. you WONT be surprised
That is a piss-poor excuse for a scientific study. Besides the obvious bias of the authors and their admitted conflict of interest.
Note that they were amazed at how well BOTH sides of the study performed. They were expecting the control side to be 5 times worse than they tested. Hmmm.. wonder why they had such mild symptoms.
Yes, they admitted many of the controls were given ivermectin instead of the placebo. But when they discovered that those were excluded from the results. Well, what if others also got ivermectin but it wasn’t ‘discovered’ by the pharmacist?
Then, they never used a matching placebo. The people could know from the taste if they were getting ivermectin or not. And in a country with a high use of ivermectin, those knowing they were not getting the real thing could get it on the side so they would be protected.
And finally, the coup de grace, they ALLOWED people with a recent history of ivermectin use into the placebo group! by design!
while we do not know how long ivermectin provides protection from C-19, we do know that people are protected from river blindness taking it once in 3 months or more often, once a year!. Cessation of taking ivermectin 6 days before the trial began invalidates the study while providing the evidience as to why the placebo group tested so well.
This was an ivermectin versus ivermectin trial. It is no wonder the end results were so similar for each side.
Here come all the naysayers. Three in a row so far.
Dr Pierre Kory pleading with TPTB:
https://www.c-span.org/video/?c4930160/user-clip-dr-pierre-kory-senate-hearing-ivermectin-100-cure-covid-19
The FLCCC protocol: https://covid19criticalcare.com/
Watch the video and read through the FLCCC website. These are quite obviously competent, caring doctors practicing evidence-based medicine. The people who don’t see this are the wack-jobs.
That is the main thing that has struck me about those who are trying to get Ivermectin at least to be given a chance in the sense that the Doctors & the data analysists involved obviously know their jobs & are not going to make a killing out of their efforts. The only real Cui Bono in all of this potentially applies to patients.
and the inverse, Eustache de Saint Pierre? if patients are NOT the beneficiary, who is and what is systemically keeping patients at a disadvantage, and how is this potential charade being maintained?
The FDA article, Why You Should Not Use Ivermectin to Treat or Prevent COVID-19, features a picture of a horse, to make their point, I assume, that humans should not take a veterinary medication prescribed for a horse—-makes horse sense to me. The drug’s approved uses in humans is, to my mind, downplayed.
The main thrust of the article is that the drug, for whatever reason, has yet to be adequately evaluated and for that reason is not FDA approved. Given the time that has passed and, according to claims by Dr. Kory and others, the great amount of data that have been generated showing the drug’s efficacy, it does cause one to wonder if perverse incentives, during this period of late stage parasitic capitalism, have wormed their way into the FDA.
So the FDA doesn’t want people to take dosages appropriate for animals? Fine with me…
To me, the real question is why our medical establishment has not already rushed to investigate Ivermectin.
And why the people doing the RCTs through peer review find it impossible to get them published.
Here is Dr Tess Lawrie saying “I’ve never seen a commit to publish rescinded, maybe for fraud, but this is not that…”
https://www.youtube.com/watch?v=y2FWPQm6sxw&t=2s
Dr Kory can’t get his published either.
As flora pointed out early, the NIH is officially neutral on Ivermectin. The FDA posts raising alarms are about attempting to self administer with veterinary Ivermectin. Other readers pointed out you do want an MD to prescribe since there could be drug interactions.
After seeing Dr Kory’s heartfelt and authentic feeling testimony to Congress it became even more clear to me that prevention and treatment options were NOT being given the attention expected if this was indeed a serious risk to humanity.
other links: https://dryburgh.com/ivermectin-pierre-kory/
https://www.hsgac.senate.gov/imo/media/doc/Testimony-Kory-2020-12-08.pdf
I, for one, applaud this site for addressing this issue. If what is happening isn’t economics I don’t know what is – and I value the critical and thoughtful attention and dialogue to this important topic. Kudos to Naked Capitalism.
I will add this question which I ask myself regularly and keep coming up with similarly depressing answers to: why do so many of our human societal issues appear so similar from a higher or integrated level, and get systemically dealt with in a similarly and apparently ineffective way? Who benefits from this (cui bono). iIt’s regularly not me or people like me.
> heartfelt and authentic feeling
Since authentic feeling is all-too-easily simulated (we have a word for that: “acting”) I’d prefer to leave it out of consideration altogether.
appreciate the sentiment. the facts looked to speak for themselves, yet crickets.
One can also refer to https://www.microbe.tv/twiv/twiv-691/ for discussion (by top experts, and with links to source material) from last December (time about 1:29:30) , or search on ‘ivermectine TWIV’ and find other podcasts.
Sorry, discussions are opinion. I want to see studies. With studies you can see if what was tested is the actual recommended use case.
And more important, I don’t see the basis for this vehement nay-saying. The NIA is pointedly not recommending against it (not recommending for it either). Standard established doses will not be toxic. So what is the harm of taking it if you think you will be in at high risk (like on a long flight) or were exposed to someone who got Covid and you are pretty sure it was when they were shedding the virus? At worst, this falls in the “can’t hurt, might help” category like taking Vitamin D.
The discussion are expert opinions, but the studies are linked to, and are often those who discuss it are the same people who did the studies and authored the various papers.
Which is another typical sign of quackery.
You got some kinda problem with Mexican doctors, champ? Sheesh.
It’s plenty harmful if you think it will substitute for a vaccine or it makes you immune. Which seems pretty common on the Internets.
This one still quacks like a duck for me. The comments of true believers “using ivermectin successfully” are more likely to be confirmation bias than anything else. Every wonder drug that doesn’t work out follows the same pattern this one has: amazing anecdotes not backed up by research (here the too low concentration for results) and studies from far away that are impossible to confirm.
“Big Pharma is immorally obsessed with profit” is a truism, but it is a terrible rule of thumb for determining if drugs work. Big Pharma doesn’t suppress orphan drugs, it buys them up and jacks the price up 1000x.
Or like Merck is currently doing – it does everything it can to badmouth and torpedo older drugs like ivermectin – so its new upcoming anti-COVID drug has no competition. Replacing the 8 dollar drug with a 2000 dollar drug.
The fact that you are bad-mouthing research from other countries is exactly what some of us are talking about – the studies are coming in from all over the world – and are very similar in their findings for the most part. To dismiss this off the cuff, in my opinion, is an extreme form of racism and first-worldism. We may all find out very soon what our arrogance as a nation will cost us.
Just a solid head nod and virtual hand shake to IM Doc.
I’m also a medical professional and I’m with you.
So many posters are talking without knowing, only quoting what they’ve been fed.
I’ve spent hours weekly reviewing the Ivermectin data and it’s a no brainer that if the USA really cared more about health and death they would at the very least have had instigated trials on IVM. This is becoming a stain on the US medical conglomerate.
We are in a pandemic and imo we have enough data to promote and use IVM to save lives, and keep people out of the hospital.
Sadly, I fear money and ego are the obstacles.
Well that modus operandi doesn’t work so well when the drug in question is off-patent. Even Iran figured out the manufacturing process (not to diss Iran, I realize they have a lot of really smart folks but the sanctions have certainly put them at a huge disadvantage.)
The vaccines do not make you immune….
The potential harm in trying an “alternative” treatment is that the patient may be diverted from reliable, effective conventional treatment.
A second consideration is that an “alternative” or “supplemental” therapy may interact badly with reliable, conventional assessment and/or treatment [eg by way of drug-drug interaction, side effect, etc.]
So, alternative and supplemental “therapies” are not always benign.
What would “reliable, effective conventional treatment” be in this case?
Regarding interactions or side effects, in the case of ivermectin these seem to be pretty well-known, so I’m assuming this knowledge is available to physicians. As far as I can tell, no one here who is advocating open mindedness on ivermectin is encouraging people to go to the veterinary supply story and self-medicate.
I am not doubting your sincerity. But linking this issue, the way it is laid out in this article, to some sort of dubious “alternative medicine” treatment is a rhetorical device, whether conscious or not.
I asked you above what would constitute a “scientific” observation in this case. I meant that as a legitimate question. I’d like to know why this inquiry is illegitimate.
To your point, my MD, who is the antithesis of a right winger, just prescribed it. I told her I’m coming to NYC and am concerned about exposure to variants. She agreed it was in the category of “can’t hurt, might help” for use around the time of the travel.
This is not “alternative medicine”. Help me. This is an “off label use”. Tons of medications are prescribed on an off-label basis, like thorazine (a super potent anti-psychotic) to people with severe pain who aren’t responding to opiates. Or your favorite, Botox, which in fact has never been approved for its main use, partly paralyzing facial muscles for cosmetic purposes. See here to confirm: https://news.abbvie.com/news/press-releases/fda-approves-expanded-botox-onabotulinumtoxina-label-for-treatment-pediatric-patients-with-spasticity.htm
I keep an emergency medicine kit against covid-19 in case. I live deep rural, and I keep a generator and a freezer and plenty of dry goods in rodent-proof storage also. Because a three-day power outage happens at least once every winter (last year it happened twice) and what if, for example, I get covid-19 and the local hospital (25 miles away) is full? So here it is:
Vit C; Vit D; zinc (childrens size); low dose aspirin; NAC; Gingko Biloba; quercetin; astragalus and echinacea. These are daily items. I keep a stock of veterinary ivermectin (for emergency use only!!) – it’s used as a horse wormer – one dose for a 1000 lb horse yields about four 40 mg daily doses. I know that taking veterinary medicine is not recommended, but I’m convinced ivermectin is effective and will use it if infected with covid-19, and: 1) my doctor won;t prescribe it (which is unfortunately likely tho he will prescribe the almost useless remdesivir); and 2) if I have to treat myself because the hospital is unavailable.
Thanks for this article, Yves. You folks are a beacon in a dark time where it seems all our institutions have been corrupted. When the Sainted Fauci publically stated that remdesivir was “the new standard of care” against covid-19, and suppressed ANY other treatment including ivermectin, I concluded he and his institution were corrupt actors. Sad to say, we are on our own in this when the NIH and CDC would rather advance the profitability of an at best marginal drug over a cheap remedy that is widely available.
I would note that Gilead has studiously avoided testing GS-441524, which is very similar to Remdesivir but less toxic and easier to make, because it has less time left on its patent.
There is a thriving black market for GS-441524 to treat Feline Infectious Peritonitis, (FIP) which is caused by a CORONAVIRUS.
I’d like to see tests of the drug.
Remenber when Fauci ramped Gilead’s stock based on the remdesivir press release? Good times.
Why yes, yes I do.
When people wring their hands over the general public not believing in experts, they always cast it as ignorant people thinking that they are smarter than experts.
It’s not it’s people, both ignorant and otherwise, believing that the so-called experts are corrupt and self-serving.
Any review of medical literature retractions over the past decade shows that the experts are bought and paid for.
From the Jerusalem Post: “Sheba researcher: Antiparasitic drug [ivermectin] reduces length of COVID-19 infection”
An Israeli tropical-disease expert says he has new proof that a drug used to fight parasites in third-world countries could help reduce the length of infection for people who contract coronavirus. Prof. Eli Schwartz, founder of the Center for Travel Medicine and Tropical Disease at Sheba Medical Center in Tel Hashomer, last week completed a clinical trial of the US Food and Drug Administration-approved drug ivermectin, a broad-spectrum antiparasitic agent that has also been shown to fight viruses….
https://www.jpost.com/israel-news/antiparasitic-drug-reduces-covid-19-infection-exclusive-658949
John Day, M.D., “Treat Your Own COVID” — article in The Automatic Earth:
… Ivermectin has a remarkably broad safety profile, and has been served up about as many times as McDonald’s hamburgers, to man and beast alike, for various forms of worms and parasites. It does cause birth defects in rats, when given at high doses, so don’t use it in pregnancy, please. Like most medicines to treat coronavirus illness, ivermectin does different things against the virus, than it does on regular days. Ivermectin inhibits the transport of the viral RNA into the cell nucleus, where it would be transcribed, manufacturing new viruses. It does other things, like reduce inflammation during cytokine-storm, in the second and third weeks of illness, helping the people who get really badly sick. Ivermectin is effective in prophylaxis, in early illness and also in later, severe illness, and through multiple mechanisms. Ivermectin is what I prescribe since last August.
Ivermectin is now available mail-order from India, and from a reliable source. https://www.medicinesdropshipper.com/antiparasitic-drugs.html#iverlast-12mg-tablet
The preventive, “prophylactic” dose of ivermectin is based upon body weight, and it can be taken weekly, once an initial level inside of the cells is established. Ivermectin leaves the cells very slowly, so it can just be topped-off once per week. There are some slight variations on this, but I’ll describe the one I prescribe. It uses the same body-weight dosing that you will find wherever you look up ivermectin dosing for humans or animals. For every 5 kg, or 11 pounds of body weight, a person takes 1 mg of ivermectin at that dose. For most people I treat, that is 12 to 18 mg of ivermectin per dose. For COVID-19 prophylaxis, this dose is taken Day #1, Day #2 and then every seventh day after that. If you forget, take it when you remember, and get back to the original schedule after that….
https://www.theautomaticearth.com/2021/02/treat-your-own-covid/
I learned about ivermectin’s use for Covid from Chris Martenson at Peak Prosperity at least six months ago. Through him I also became aware of Dr. Pierre Kory and Paul Marik at Frontline Covid-19 Critical Caregiver’s (FLCCC). They were using ivermectin clinically and were having great success. Dr. Tess Lawrie at Evidence-Based Medical Consultancy in Bath, England became aware of ivermectin when she watched Dr. Kory’s testimony at a Senate sub-committee hearing. She and her staff took it upon themselves to do a meta-analysis of ivermectin and found that it was significantly effective for all stages of Covid and as a prophylaxis. At the same time, the World Health Organization hired Dr. Andrew Hill at the University of Liverpool to do a meta-analysis of ivermectin which is now completed. WHO is supposed to be issuing a statement concerning ivermectin shortly.
I visit Naked Capitalism everyday and would notice an occasional article about ivermectin in the Links or Water Cooler. But I was disappointed that no major article on ivermectin was forthcoming. Until today. Nick’s article is excellent. The cat is now out of the bag. Evidence from around the world is showing that ivermectin is safe and effective against Covid-19.
> Dr. Tess Lawrie
Lawrie article (not peer-reveiwed) and video interview. Here is Lawrie’s company.
I believe this post and the comments are perfectly emblematic of unfortunately where my profession is and where my country is. I have to admit, I would have never dreamed this possible just 10 years ago.
I will start by quoting one of my medical professors years ago when I was an intern….You have to imagine it in a very hard Danish accent….”Young man, if research or scientific findings make you angry in any way, you must immediately examine yourself. You are by definition not practicing science or medicine, you are practicing dogma. You must put down your test tubes and go to the nearest closet and in private examine your soul.”
I have thought of this old man often this past year – and the tenor of some of these comments have brought him yet again to mind.
We have created a world where every side has their own facts. Unfortunately, I believe we are all going to find the hard way that science is not going to work like that.
We have done everything possible to politicize medicine and science this year in this country – and look where it has gotten us. People not just here but all over Twitter and our media screaming at one another about things they have no clue about – just because their side says so. It has been a revelation.
I would also like to echo one of the above commenters – decrying the fact that most practicing physicians have just been cut loose to flap in the wind. Trust me – there are many days when I feel just like that. We have not had time for science in this pandemic to give us real answers – but the more unfortunate thing is that our national agencies have not even tried. The minute that these overwhelmingly positive studies were coming in from other countries about Ivermectin – our NIH and other agencies should have immediately been on the ball – working on our own rigorous studies. They have been nowhere. That has led physicians like me to use the drug despite our own credulity in the beginning (Lice pills? You have got to be kidding!) – guess what – it seems to be working to keep people out of the hospital. And it is not nearly as scary as the other option, monoclonal antibodies (MONOCLONAL ANTIBODIES, WTF?) to keep people out of the hospital. And I remind you – the monoclonal antibodies are on an EUA just like the vaccines – and are considered the same status as Ivermectin by the NIH. This is a safety no brainer – and yet my profession and our country seems hell bent on laughing off the 8 dollar a month safe 40 year experience pill for something that is equivalant to a dose of chemotherapy – with really no strong efficacy numbers to balance out the risk. And they are thousands of dollars a dose.
Our nation’s medical leadership has been all over the place this year – wear masks – don’t wear masks. 3 foot social distance – 6 foot social distance. You all know exactly what I am talking about. Instead of leadership, they have often gotten on national TV to fear monger and even cry like yesterday.
Meanwhile, there are thousands of physicians like myself in communities all over this country doing our best to hold it all together for our patients. Not just the COVID patients, the countless others who have lost jobs and livelihoods and lifelong businesses. We are seeing all kinds of vaccine complications – while the media and medical elites are screaming that they are 95% effective and perfectly safe. I am praying every day that the vaccines work – and it was worth the risk – the backlash if not will be unforgiving.
That is where I am today. I will continue to use ivermectin to keep people out of the hospital. It seems to be as effective as any other modality we have right now. I will keep my eyes peeled for studies and evidence about this issue. Antivirals are going to be as critical going forward as vaccines.
And for those questioning why doctors are remaining anonymous ( a trend that was never dreamed of during AIDS) – you really must be dense. Look at the cancel culture in which we live. We as a country need some serious introspection when good faith questioning leads to job loss and career suicide.
To Yves and Lambert – like everyone else – you are not 100% right all the time. The definition of humanity. But you have given thinking people a forum to discuss and learn. For that we should all be eternally grateful. You are doing a great service to our world.
“We are seeing all kinds of vaccine complications ”
Could you be specific? Maybe I missed prior posts of yours.
Also, just wanted to say “thanks” for your contributions.
Reactions by those with autoimmune diseases. Multiple reports from people who are one degree of separation removed from me of a significant worsening of symptoms after getting the Pfizer and Moderna vaccines, and that not abating over time.
Just an anecdote but good to know from someone with an autoimmune condition. I have been worried about this and can’t get any information from doctors or the internet. I figure I have to wait a year until the shit hits the fan (or not) to see what shakes out. So frustrating.
What am I seeing?
The most fascinating problem that has no obvious explanation is a surprisingly large number of patients that get sick and are COVID positive within hours/days of their first injection. I have heard all kinds of lame excuses why this may be happening – but none of them really ring true for the numbers that are occurring. I would predict this is going to be an interesting story when the full story of COVID comes out in a few years. By the way, they tend to be WAAAAY more sick than a regular COVID patient. No hospitalizations yet.
I am seeing blood clots in both venous and arterial systems. This is happening mainly to younger people. I have 4 so far – an unexpected DVT, a PE, a very strange problem in a young healthy man having unstable angina with positive enzymes within hours of his first shot, and a young woman who clotted off the main artery to her arm on the injection site leading to a compartment syndrome. None of these patients have died – and all are doing well now. But it was scary when it was happening. No proof the vaccines did it – but the timing is very concerning, especially in the last 2. I would reiterate that the PCPs of the world are flying blind in this regard. We have no guidebook of completed and well-done trials to guide us with what are common problems. We are literally just taking it all in as we go along. I will reiterate – in a decades long career – these things I have just outlined are 3 times as many severe complications as I have seen after giving 10s of thousands of other immunizations. This is the truth.
A handful of patients with sudden flares of their dormant autoimmune syndromes – one of which is turning into something possibly bad. Multiple patients with COVID negative and severe URI symptoms. And multiple severe issues with lymph nodes almost to the point of being bubos. I have also seen a severe Ramsay Hunt syndrome in an elderly woman and one episode of anaphylaxis.
That is all I can remember off the top of my head. Maybe these all have nothing to do whatsoever with the vaccines. The timing, however, is very suspicious. And please note – this is a handful of severe problems in probably 1500 to 2000 vaccinated already. The number of people with fever, chills, flu-like illnesses, etc has been very high, just as predicted in the protocols. But the vast majority of patients have no obvious long-term problems. It is my contention that the patients of the world should have had this presented to them correctly – and we would all be better off emotionally. But alas – it is what it is. Younger people seem to be having a much worse time with side effects – now that we are moving into the younger age groups, I fear this is going to become a much more significant issue.
> the patients of the world should have had this presented to them correctly – and we would all be better off emotionally.
It does seem that, at least at the top level of the public health establishment, lying to the public to achieve an acceptable outcome is considered best practice (see Fauci on masks). Those lying must not perceive the practice as maladaptive from a career perspective, so one shudders to think of the state of the institutions through which they rose.*
* “Everything is like CalPERS.”
Actually we have precedents for the observation you mention on cases cropping up early from other vaccine trials and we now have DATA from two vaccine studies for this vaccine that document what you are saying.
I adopted a rescue dog from coastal North Carolina in 2012 that had a bad case of heart worms. The universally accepted treatment is a dangerous (and very expensive) two-dose injection of arsenic to the dog’s spine followed by cruelly immobilizing the dog in a tiny crate for six weeks. The shots leave many dogs with permanent paralysis and many more die from blood clots formed by rotting masses of dead heart worms which die off suddenly from the injections. A small town Vet in North Carolina who was very skeptical of the cruel and high-risk injections tipped me off to a University of Georgia study where dogs were successfully cured of heart worms using a standard prophylactic dose of Ivermectin and intermittent Doxycycline. I ran the idea by my very caring, intelligent and open-minded Vet in Manhattan and after reading the study said he was willing to try the alternative treatment. The one-two punch of the Ivermectin and three-cent-a-pill Doxycycline worked like a charm and my dog was heart worm free after six months without being cruelly confined or running the risk of paralysis or sudden death. The vet was amazed and swore he would never recommend the standard heart worm treatment again. I saved myself about $3000 as well, and while the amount was significant to me, that was just icing on the top not the prime motivator for seeking an alternative treatment. However, for many pet owners, that sum could be the difference between seeking treatment and letting a dog slowly succumb to parasites. I researched the dangerous and expensive shot and why it was universally accepted in the United States as the only legitimate cure for heart worms and the answer seemed to be strategically placed board members among prestigious Veterinary Schools and a quite few lavish Marlin Fishing junkets funded by the pharmaceutical company producing the arsenic shot. Yes, veterinary medicine I know, but from what I’ve learned Veterinary medicine and Human medicine operate exactly the same in the US. Never treat anything with a pill that cost pennies if you can use a shot that costs thousands, even if the more expensive treatment paralyses and/or kills the patient – large profits are far more important to the functioning of the system than curing disease or minimizing harm. When it comes to medicine trust no-one receiving payment, do your homework and plan on advocating for yourself at every turn.
This story is heartwarming, but it’s no proof ivermectin is a good covid treatment.
It’s amazing how skeptical folks are of Big Pharma’s PR, but how incredulous they are for “heartfelt anecdotes.”
Never said my story was proof Ivermectin is a COVID miracle drug. Just a real world example of how Ivermectin has been dismissed as a treatment option by the (Veterinary) medical establishment due to a Capitalist preference for a more expensive, but less desirable treatment. Furthermore this isn’t a ‘heartfelt anecdote’ but a firsthand account. I think the treatment regime I detailed has gained a bit more acceptance for heartworms now, but it was virtually unheard of in 2012 despite published research showing efficaciousness dating back several years. The other parallel of my story is the economics and availability of the preferred medicine of western doctors in highly developed countries frequently mean nothing to those without the financial means to obtain the treatment, and in some countries the drugs simply aren’t available to people, necessitating alternative treatments and experimentation, which most I think most would agree is preferable to dying. I have no dog in this fight ( pardon the pun ) but I do have experience with Ivermectin being sold short as a drug by credentialed medical experts in the pursuit of profits.
*** crickets *** in response…
Reminds me of Doris Cully talking about ivermectin talking about river blindness and allowing time for clearing the parasite from the eye — about 14 minutes into the podcast. Sounds like the mass of dead worms you mention.
About 3 minutes in Doris Cully relates her background working with ivermectine when it was discovered.
forgot to give link https://www.microbe.tv/twiv/twiv-599/
Thank you for this and your other comments. I watch for and greatly value your insights and revelations offered through your view from the trenches of medical practice.
Before the Corona pandemic I had been growing pessimistic about how Humankind would respond to Global Warming and the impending limits to growth, and about what prospects the future held. After a year of the Corona pandemic observing the incompetence, greed, and cruelty of the US Government, and organizations, agencies, authorities, and disciplines that once held my highest regard, mishandling the pandemic and the ongoing economic disasters it created, my pessimism nears fatalism regarding prospects for the future of Humankind, myself, and my children.
A recent addition to the FLCCC website is a page “How To Get Ivermectin” offering a list of physicians who will prescribe ivermectin.
https://covid19criticalcare.com/guide-for-this-website/how-to-get-ivermectin/
Thank you very much for this valuable information.
I grew up stock farming in the great Ivermectin boom when every farmer was recommended to drench his cows (forced oral administration) with it against liver flukes and the like.
Ivermectin, IIRC, is notorious in the organic farming community for producing “plastic cowpats” – cowpats that do not degrade and support insect populations but dry into frisbees. The difference between organic cow manure and intensively farmed is profound.
So, if you do take it off-label, just be aware your microbome might need some serious restoration of your commensal bacteria and parasites. Low parasite loads are linked with many autoimmune diseases and gut disorders.
I still think the data on Ivermectin justify proper randomised clinical trials. The examples and counterexamples are just too noisy. Even the argument about effective concentration is not clear: in vitro is not in vivo because compounds exhibit preferences for different tissues (volume of compartmentation), which is why chloroquine reaches effective blood cell concentrations on low regular doses and, after many years, can lead to blindness because of the effects of high retinal concentration.
> I still think the data on Ivermectin justify proper randomised clinical trials.
They do indeed (though many of the RCTs for HQ seemed almost designed to produce a negative outcome, not being designed to test for prophylaxis).
However, given the givens, I think the threshold could be — is, obviously, already in many countries — lower than RCT. Zeynep Tufecki writes, of RCTs and masking:
So far as making public health decisions in a pandemic, I don’t see why the enornous natural experiments listed in the post aren’t enough to go forward on, RCT or no RCT.
To do it right, studies for all the possible drugs should be funded, and research funding, which is pitifully stingy, should have been ongoing for decades, including genomic research and such into possible vectors for zoonotic diseases, such as bats. This is a constant complaint among researchers (corona virus among deer mice, for one example I heard). We seem to be too preoccupied with finding new ways to blow ourselves up for that however.
Reality check from the CDC’s Mortality and Morbidity Weekly Report: “Among 148,494 U.S. adults with COVID-19, a nonlinear relationship was found between body mass index (BMI) and COVID-19 severity, with lowest risks at BMIs near the threshold between healthy weight and overweight in most instances, then increasing with higher BMI. Overweight and obesity were risk factors for invasive mechanical ventilation. Obesity was a risk factor for hospitalization and death, particularly among adults aged <65 years.”
Body Mass Index and Risk for COVID-19–Related Hospitalization, Intensive Care Unit Admission, Invasive Mechanical Ventilation, and Death — United States, March–December 2020 | MMWR
https://www.cdc.gov/mmwr/volumes/70/wr/mm7010e4.htm?s_cid=mm7010e4_w
AKA: If you are already “ill” (Obese) it take less effort for disease to kill you.
That’s not a surprise.
I suspect there is a causal link between Obesity, Air Conditioning and Driving, as both air conditioning and driving appear to eliminate exercise appear to promote obesity (through lack of exercise) and its attendant ills.
I used the site AmericasFrontlineDoctors which takes you to speakwithanMD.com to get my 80 year old father ivermectin. After the consult, they sent him hydroxychloroquione/zinc instead, and they have not responded to any of my emails/texts inquiring if that was done due to possible interactions with my father’s other medications.
From my reading, and I’m not an MD or biomed person, I believe there are a few ivermectin contraindications – like pregnancy and liver disease – and drug interactions – like Warfarin and coumadin. Don’t take my word. This is one reason it’s so important to talk to your doctor about whether it’s an appropriate med for your medical condition.
It’s infuriating the US pharma/med/govt nexus is trying to stop your local MD who knows your med history from prescribing ivermectin when appropriate.
> I used the site AmericasFrontlineDoctors which takes you to speakwithanMD.com to get my 80 year old father ivermectin. After the consult, they sent him hydroxychloroquione/zinc instead, and they have not responded to any of my emails/texts inquiring if that was done due to possible interactions with my father’s other medications.
Well, so much for them! (One of the disadvantages of being an outsider is lack of resources, and one of the dangers is zealotry.)
So why do you trust “America’s Frontline Doctors” over Big Pharma?
Or is this organization NOT selling you something?
As alternative treatments always do, this reeks of “we care, not like horrible Big Pharma!”
Great bedside manner is the entire foundation of a quack’s practice. A great mild example is Cancer Treatment Centers of America. Expensive, but they support you with alternative treatments! And there survival rates look great! Must work, right?
They get those rates by not admitting folks with low survival probabilities. It’s much money for a kinder, more pleasant environment. Which feels “healing.”
“Well, it can’t hurt..”
Sorry, TANSTAAFL applies. The cost may be low, but there is a cost. Quackery crowds out resources for real treatments.
Ignoring the actual evidence in the post entirely. But you do you.
TANSTAAFL is Libertarian code speak for Neo-liberal Rule #2.
(Here we go again!)
Update: Yay! It worked! I have no clue as to why the previous comments were eaten by the Internet Dragons. Oh well. Perhaps the “gods” are trying to teach me something about the quantum nature of reality.
Since there is now an article dedicated to this subject, here is a related link from an MD who specializes in bioweapons: https://anthraxvaccine.blogspot.com/2021/01/first-country-bans-ivermectin-lifesaver.html
She first came to my attention after the anthrax mailing scare years ago as a skeptic against the official narrative. I thought of her again when Covid started and I’ve been reluctant to post anything from her here before, since she is once again going against the official narrative. I have no idea how she is regarded within her field, she does get tend to hyperbole a bit in the link above, and I don’t know nearly enough about medicine to evaluate what she says in this and other posts of hers I’ve seen across the interwebs over the last year. That being said, while I’m not a regular follower of her blog, I have checked in over the years when microbes are in the news and she does seem to have a lot of knowledge in her field and comes across as a genuinely decent human being. Also, she is from Maine!
Her other writings on the coronavirus topic, including what I thought was decent argument debunking a study claiming chloroquine was not only ineffective but dangerous (she said it is dangerous when they drastically overdose people like they did in the study, but not when used in proper dosages) can be found with a quick search for anyone interested. Or you can just read more on her blog linked to above, but the blog may not have the most detailed and scientific arguments compared to other writings.
I would be genuinely interested in what others with a better understanding of virology/vaccines make of her take.
Of so many tragedies to come out of the COVID-19 pandemic, one of the saddest to me – and probably the one with the longest-reverberating consequences – has been its wholesale discrediting of our health science institutions.
Here we are, over a year into this pandemic, and we cannot get a straight answer on whether or not this relatively cheap and safe drug saves human lives from COVID-19 or not. Worse, we can’t even seem to properly investigate it. All questions bring hysterics, or hardly-believable obfuscation, or (informed?) outrage, no matter what authority we turn to. The fallout in my own life from watching all this unfold has been… dramatic.
I don’t trust what the CDC says. I don’t trust what the WHO says. I don’t trust what the FDA says. I don’t trust Pfizer and the rest of the pharmaceutical companies any farther than I can throw them. I look with suspicion on my own scientist acquaintances, wondering if they are really following the data, or if they are clinging to a chosen worldview that science in America still works, oh god it still works, oh god it hasn’t been completely discredited, no it cannot be, my life work must have meant something, it must still work, it must still work….??
None of this means that ivermectin works–or for that matter, that it doesn’t work. It means that I have realized, slowly and then all-of-a-sudden, that I cannot know. Nor can any other layperson. We are alone, our economy is collapsing in slow-motion, and our lives are at stake. Or so we think! If we doubt so much, how much more should we really be doubting? I believe, for what it’s worth, that COVID-19 is real and that these experimental vaccines probably won’t kill us. At least… not that many of us.
But I wonder now, in my darker moments, whether the claim of those who don’t believe such things that refusing the vaccination is a “Darwin’s test – pass it and survive” have grokked something that was beyond me, in my previous worldview. How could it have come to this…? And if I am feeling like this, how must people with less scientific background (I attended a science magnet school) be feeling about it all??
Will my children be safe from measles, etc in the years to come? I have vaccinated them with the whole slate, and feel fine about that choice, but will the fallout from this debacle mean the end of herd immunity in America, as trust in the ‘health experts’ collapses into dust? How can we get it back, then – at gunpoint? With all that would imply… is it even worth such a high price…?
NC is doing the Lord’s work in finding the high quality news sources it continually brings forth for our viewing. But – pardon me – this isn’t something that should need to be be argued over in the comments section of a news site. This isn’t something that laypeople should have to suss out, with their own lives on the line. That it has come to this is a shame, and a shame so complete, that every time I really contemplate it I get the shivers. Our government has failed us. It has failed us. Yet we elected it. Oh, the shame…!
Is it my fate to live the rest of my life ashamed, utterly ashamed, of my own country? There has been no feeling reoccurring more regularly over the course of this past dreadful year, than that one. When, if ever, will the day come where I can live free of that dreadful emotion, attacking me every time now when I catch a glimpse of that flag flapping in the wind…?
I could not have expressed many of my same feelings better. Thank you. And I am a medical professional. You should not feel alone in the chaos. Anyone who has a brain and the ability to reason has felt the same way all year.
My feelings echo your despair.
> Is it my fate to live the rest of my life ashamed, utterly ashamed, of my own country? There has been no feeling reoccurring more regularly over the course of this past dreadful year, than that one.
I have had the same feeling all this year, too.
My first comment from a long time reader. This heartfelt comment is exactly what has concerned me throughout this year. I thank you for so eloquently speaking what I consider truth.
Here’s another “Amen” from a healthcare person who is feeling dazed and confused by this year and is having a bit of an epistemological crisis — I feel much the same about the organizations you referred to.
As for the original post, I could hardly believe the vehemence of the reaction against hydroxychloroquine last year, since in my experience it’s not known to be overly dangerous. But I thought, “Ok, well, Trump Derangement Sydrome, Plus, it’s probably bad news to give it to someone really old who’s critically ill and
has a bunch of electrolyte disturbances etc..”
Now the pushback against Ivermectin. I have to wonder where it comes from. Who knew there was such widespread simmering emotion about a drug that most wealthy Westerners never encounter in their lifetime!
I don’t know. I’m probably just internet-poisoned but this whole thing stinks and now my question-everything paranoia directly affects my work life, so now I can’t get away from it. Argh!
I am so glad I am not having to administer the AZ vaccine yet! I’m supposed to be able to give patients an intelligent recommendation on these things, but I mostly feel like an idiot.
You have captured the essence of the New American Experience.
It feels like what someone losing a life long religious conviction must experience.
Are we going to have a “Lost Generation” like the West did after World War One?
Regardless of whether ivermectin works or not, it’s promotion seems heavily connected with promoting “lockdowns are the real killer” narratives, and it seems to be popular with the just offering hypotheses to Questions bunch.
Much like HCQ.
I’d ask my parents who believe that Fauci created covid what they think of it, but I don’t have the stomach for it.
I’m sure creating an interest in a drug that commonly comes in a dosing for horses that is the equivalent of a few dozen human doses is completely harmless. Not like anyone OD’d on Vitamin A and required hospitalization…..
The dose makes the poison.
How did you conclude that consideration of Ivermectin is connected with promoting “lockdowns are the real killer”? Ivermectin is used for treating horses, and treating pets for worms and mange, and for treating human diseases like river blindness. Its use as an antiviral comes as a surprise to me, but so does the idea of using a compound exuded by a greenish cantaloupe mold as a powerful antibiotic.
True the dose makes the poison. I have read that distilled water in sufficient quantity is a poison as is carrot juice.
The folks heavily invested in PROMOTING this alternative treatment(and all the others) seem invested in that narrative.
If you look at this epidemic and many others, “this isn’t really happening” and “wonder cure” are narratives often pushed by the same folks, even if they conflict with each other. But nothing goes so well with belief in a CT as beliefs in more CTs.
A true unbiased researcher would go where the data lead. If it leads to a conclusion that makes them uncomfortable, because it puts them outside of “polite company”, then so be it.
A big part of why we’re in such a hole in this country is that folks cannot separate out two things that can be simultaneously true. Like, Ivermectin might be an effective therapeutic drug in some use cases, and some of the people who are vehemently saying so are a bit off the mark in other areas (like mask wearing, or lockdowns.)
At any rate, it sure would be nice if our government that is swimming in Federal Reserve play money (or a wealthy individual with no soft money conflict of interest) would do a large scale RCT and publish the results. Then we might actually get to have some “science” to go by.
A big part of why we’re in such a hole in this country is that folks cannot separate out two things that can be simultaneously true. Like, Ivermectin might be an effective therapeutic drug in some use cases, and some of the people who are vehemently saying so are a bit off the mark in other areas (like mask wearing, or lockdowns.)
Bingo. This is basic logic. It’s in very short supply these days.
That is absolutely false and is Making Shit Up. You have no evidence of your contention.
Did you not work out that there’s no money to be made in recommending old, off patent meds? Your argument doesn’t even pass the smell test.
In fact, the mainstream media is refusing to discuss these treatments even though the advocates do not in fact have an ideological agenda, contrary to your assertions. From an e-mail I got late in 2020:
> Because of the mainstream media censorship of our position that early outpatient treatment is safe, successful, inexpensive and would largely solve the pandemic without necessity of or even better than vaccines, most of our messaging has appeared on the political right.
What Operation Warp Speed should be faulted for is a heavy orientation toward vaccination as oppose to treatment (which did get funded, though in lesser amounts).
> I’m sure creating an interest in a drug that commonly comes in a dosing for horses that is the equivalent of a few dozen human doses is completely harmless. Not like anyone OD’d on Vitamin A and required hospitalization…..
Do consider reading the post. Serious, genuine medical professionals are using Ivermectin and getting good results with it, as documented here and in three studies I put under “Healthcare” in Water Cooler today. These are not cray cray late-night telemarketers, despite your stereotyping,
Countries like Mexico are looking at Ivermectin because our insane, rentier-driven health care system is producing medicines they cannot afford, and they need to save lives. Given that most of Flyover in this country is approaching Third World status, we would do well to follow their example.
Countries like Mexico are looking at Ivermectin because our insane, rentier-driven health care system is producing medicines they cannot afford, and they need to save lives. Given that most of Flyover in this country is approaching Third World status, we would do well to follow their example.
— Right on, Lambert!
I read this post, and a few others on the same subject you have posted. I keep waiting for one of them to go off script of the typical Quack Miracle Cure narrative.
Quack medicine is not often originated out of malice. It often arises from caring and competent (as technicians) folks trying something out, and confirmation bias does the rest. Other folks not finding effects is Big Pharma/They did the experiment wrong/etc. All studies finding effects are great, no matter what, and even if analysis is done in a small echo chamber.
Then power of confirmation bias to create belief is amazing.
You seem rather impervious to data.
Your ‘Quack Miracle Cure narrative’ trope can certainly come off as just as unhinged as any “it’s from big pharma so it must be bad” prejudice (and in fact I share your disdain of blanket prejudicial dismissal of any and everything that comes out of the established medical world, or whatever you want to call it). I’m all for scepticism and criticism but yours seems just as tossed-off as any ~alternative~ talking points. Do you have anything of substance to show us, besides general observations of How Quackery Happens?
None of the phenomena you describe apply to the post, which is carefully written and evidenced. This isn’t Natural News. Go away. I do admire your tenacity in sticking to your talking point, good job
For those interested, I added three Ivermectin studies to the “Healthcare” section in Water Cooler.
Sorry guys, this is a BS
https://www.ema.europa.eu/en/news/ema-advises-against-use-ivermectin-prevention-treatment-covid-19-outside-randomised-clinical-trials
weak tea, Phill
“this is a BS” is not a sensible conclusion to draw from that link. It’s pretty equivocal stuff.
> Sorry guys, this is a BS
Says the dude with a throw-away email address who also doesn’t know “BS” does not require an article….
Well, in his defense, he is trying to discredit an ‘article.’ /s
Imagine what other news has been suppressed by leftist media? No one talking about this? Media blackout is why. As so many informed readers have commented, there are accounts of ivermectin effectiveness in third world countries but any doctors speaking about are crucified.
It’s not “leftist”. It’s “liberal” which = mainstream pro capitalist with idpol decoration.
True leftists are also denigrated by the MSM. Look at Sanders, who isn’t at all left wing by non-US standards, he’s a social democrat, and Europe is full of mainstream social democratic parties.
The data look quite promising! But possibly irrelevant if there’s no big money to be made; consider me cynical about Pharma. The “can’t hurt, might help” approach works for me, however.
I don’t know if any of you had small children that brought home (from school) the harrowing gift of…pinworms! But the whole fam takes ivermectin! That was so long ago, my guess is Merck still made it. Anything that is at all helpful for early Covid, mild Covid, new strains, etc that is safe, should be seriously tested and considered and not be excluded simply due to our never ending quest for huge pharmaceutical profits.
As far as off label drug use, I perused the piece on Botox for muscular dystrophy. I can attest that Botox for spasticity (particularly spasms that are contractures) is nothing short of miraculous. But the cost is astronomical.
FLCCC site has list of human Ivermectin suppliers.
https://covid19criticalcare.com/guide-for-this-website/how-to-get-ivermectin/
Interesting complication to the story, as I just learned listening to https://www.microbe.tv/twip/twip-193/
It may be that a factor with ivermectin use is not that it combats covid, but rather a secondary infection which may arise from the use of steroids used for covid, which suppresses the immune system and dormant allows a parasite to become active — strongyloides in the case presented in this podcast. Use of ivermectine handles the complications of infection from the parasite. If this is the case we should also expect to see different results of trials depending on where it is done, and what the prevalence of secondary pathogens is.
In biology, nothing is so complex that it can not be complicated even more.
In politics, nothing is so complex that it can not be complicated even more. In medical politics, everything is so complex that it can not be complicated even more.
As an engineer I see this whole arena filled with multiple feedback loops nested in feedback loops.