By Lambert Strether of Corrente
The nation’s — some say the world’s — premier public health agency continues to butcher its messaging on how Covid is transmitted. I read their Covid FAQ the other day (Updated May 25, 2021) and nearly stroked out. Here from the Covid FAQ landing page is the second item, “Spread.” I have helpfully highlighted a few of the offending passages:
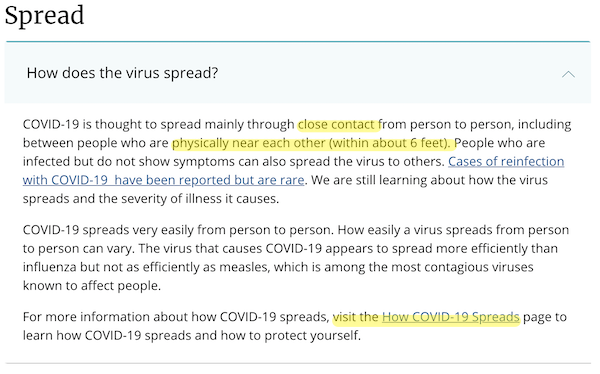
First and foremost, “close contact” should be expunged from Covid discourse entirely. Proximity is not transmission. A “close contact” model would permit infection by brainwaves, odor, visual cues, and so forth. CDC then compounds its initial error by repeating the 6-foot rule; readers know that Covid aerosols spread to fill a room, like cigarette smoke; social distancing is necessary but not sufficient. A busy school superintendent could read the FAQ and conclude that moving desks apart was sufficient to protect students; it isn’t (and lives could be lost because of CDC’s feckless and Romanov-like bureaucratic ineptitude).
To be fair to CDC, I visited the link highlighted above (“How Covid-19 Spreads”). Here it is:
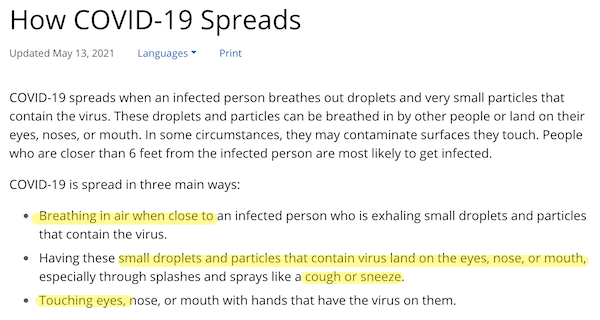
So, one level down, CDC is still reinforcing “close contact” with “breathing in air when close,” and “coughing and sneezing.” They also introduce fomite transmission, with “touching eyes.” First, the risk of fomite transmission[1] is small (“Exaggerated risk of transmission of COVID-19 by fomites“). Second, mere breathing (aerosols) is also important, perhaps more than coughing and sneezing, so they at least deserve a mention (“COVID 19 can spread through breathing, talking, study estimates“). See generallly “Ten scientific reasons in support of airborne transmission of SARS-CoV-2” in the Lancet.
To continue to be fair, when I finally arrived at the CDC’s section on ventilation, I found it to be pretty good:
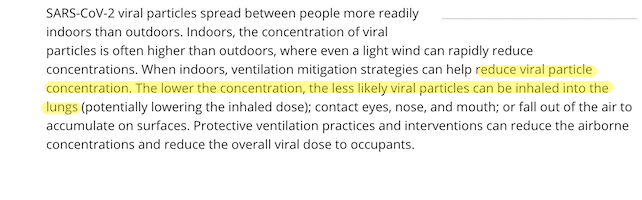
(I continue to see CDC’s “layered approach” as driven by institutional imperatives; everybody gets a slice of budgetary pie, even the fomite people.) They even get the idea that reducing concentration reduces the dose. Note, however, that this is true because aerosols fill indoor spaces, like cigarette smoke, which the “close contact” and “cough and sneeze” models do not support. Concentration affects all the people in a room regardless of “close contact.” So we see that the means of transmission here in CDC’s ventilation section completely contradicts the means of transmission presented earlier in the FAQ. In other words, CDC has no agreed upon means of transmission. How can we fight a pandemic if the world’s premier public health agency can’t get its story straight on how the germ that causes the pandemic is transmitted? Not well. Obviously. (Of course, if we simply vaccinate everybody, we don’t have to worry about such details.)
As a palate cleanser, CDC does have a lot of well-thought-out suggestions on ventilation, even if the content of the “Spread” and “How Covid Spreads” sections mean that nobody will read them:
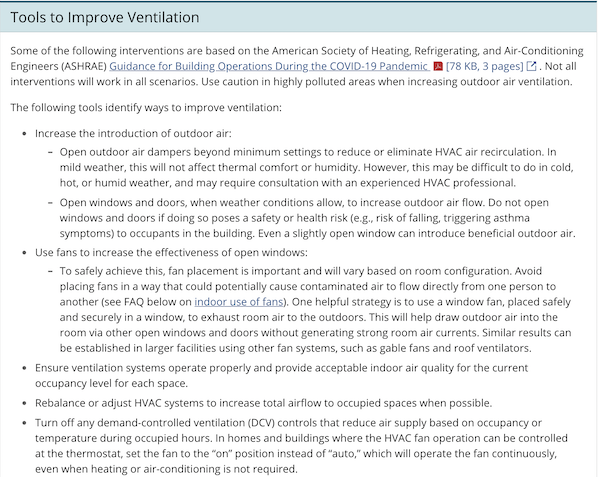
That final bullet point on “turn off any demand-controlled ventilation” sounds practical and helpful (though I defer to HVAC mavens in the readership.)
Now let’s turn to the CDC”s data collection on breakthrough infections. The New York Times describes the policy decision on May 25:
Earlier this year, the agency was monitoring all cases. Through the end of April, when some 101 million Americans had been vaccinated, the C.D.C. had received 10,262 reports of breakthrough infections from 46 states and territories, a number that was very likely “a substantial undercount,” according to a C.D.C. report issued on Tuesday.
Genomic sequencing could be done on only 555, or about 5 percent, of the reported breakthrough cases.
Contact tracing, apparently, was not even an option.
Over half of them involved so-called variants of concern, including the B.1.1.7 and B.1.351 variants.Some 995 people were known to have been hospitalized, and 160 had died, though not always because of Covid-19, the new study said. The median age of those who died was 82.
The agency will carry out vaccine effectiveness studies that include data on breakthrough cases, but only in limited populations, such as health care workers and essential workers, older adults, and residents at long-term care facilities, a spokeswoman said.
The essential point:
“The C.D.C. is a surveillance agency,” [Ali Mokdad, an epidemiologist at the University of Washington who spent many years as a senior scientist at the C.D.C.] said. “How can you do surveillance and pick one number and not look at the whole?”
That’s a good question! Here is the CDC announcement:
As of May 1, 2021, CDC transitioned from monitoring all reported vaccine breakthrough cases to focus on identifying and investigating only hospitalized or fatal cases due to any cause. This shift will help maximize the quality of the data collected on cases of greatest clinical and public health importance.
(We have seen throughout this pandemic that the spotlight is fixed on hospitals. This is true whether we ignore essential workers who can’t make it to the hospital in the first place, or on mask studies that apply hospital results to the general public, despite the fact that hospital ventilation systems change the air umpty million times a minute.) Like Mokdad, I’m unclear on why CDC would wish to blind itself in this “See No Evil” fashion. From The Atlantic:
If a variant were to consistently pop up among the vaccinated, researchers would need to understand why. A new version of the virus might be more efficient at infecting people, or have a new way of eluding the immune system. To tease out those possibilities, researchers need data, the more comprehensive, the better. “Asymptomatic, mild symptoms, hospitalized, passed away—all that information is important,” says Ryan McNamara, a virologist at the University of North Carolina at Chapel Hill, where he and his colleagues are sequencing samples from breakthrough cases across the spectrum of severity. “If you’re asking what variant is driving worse clinical outcomes, you need both ends of the data,” he told me.
Many public-health laboratories at the state and local level have been diligently tracking breakthroughs of all kinds for months, and are unsure of whether to mirror the CDC’s shifting priorities. “Previously, labs were sequencing all the breakthrough cases we could get our hands on,” Kelly Wroblewski, the director of infectious disease at the Association of Public Health Laboratories (APHL), told me. “Now states are scrambling, trying to sort it out.” Some states, such as Illinois and Tennessee, quickly followed the CDC’s lead. Others are hesitant. For now, “we’re not changing what we’ll be sequencing,” Myra Kunas, the director of Minnesota’s state public-health laboratory, told me.
You can bet that any state with budget problems is going to follow CDC’s lead in gathering less data. Further, CDC is gathering less data at just the wrong time:
In recent weeks, several college and professional sports organizations that had for months implemented routine testing for athletes and staffers announced that they were cutting back on screening for the immunized.
Programs like these might have otherwise revealed some breakthroughs. But hunting for these cases has other drawbacks. Earlier this month, the New York Yankees, a team that continued to regularly test its fully vaccinated personnel, recently reported nine positive tests—most connected to asymptomatic cases. Many experts framed the detection of mostly symptomless infections as proof that the shots were doing their job, but worried about rote reliance on testing as a security blanket, and wondered about the possibility of false positives. Vaccinated people are so unlikely to catch the virus that administering a bunch of tests wastes resources and increases the likelihood for errors, says Omai Garner, a clinical microbiologist at UCLA Health. Chasing constant reassurance about infections after vaccination could also send the wrong message, Saskia Popescu, an infection-prevention expert at George Mason University, told me. “If we’re telling people they can be unmasked and we’re still [frequently] testing them, what’s the signal we’re sending?”
This creates a strange bind for public-health officials who depend on the data that testing programs yield. As collective immunity around the nation builds, finding its weak spots is becoming harder. “We’re running into this potential of losing our pipeline for studying variants in the population,” Wroblewski, of APHL, told me.
So why the decision?
The CDC’s revised guidelines on monitoring post-vaccination infections could, in some ways, be seen as pragmatic. More severe sickness is relatively straightforward to tabulate, and hospitalizations and deaths lend themselves to a more comprehensive census.
Much as the drunk looks under the lampost for their keys. But here, I think, is the kicker:
The agency’s decision to shunt attention away from quieter breakthroughs could also help normalize mild or silent coronavirus infections—ones that have been effectively tamed by our suite of lifesaving shots—as a typical experience in the era of COVID-19 vaccines. Though the pandemic will eventually be declared over, SARS-CoV-2 is not exiting the human population anytime soon. Periodic liaisons with the virus will remain a part of everyday life; they might even remind our dormant immune cells to stay on guard.
The CDC is really sending two messages here: (1) The vaccines don’t confer sterilizing immunity (i.e., you can still catch Covid even after you’re vaccinated), and (2) Covid is now normalized. I mean, how do we know mild stays mild? As we see, CDC[2] is no longer in the surveillance business. As we saw in the first part of this post, CDC is not in the epidemiology business. CDC is not in the test kit development business (they butcher it). CDC is not in the software development business (they butcher that, too). What business is CDC in, exactly? The “See no evil” business?
NOTES
[1] Even though I am aware of no documented cases of fomite transmission, I still think cleaning surfaces in a non-obsessive manner is a good idea; after all, the aerosolized particles that bear the virus have to land somewhere. But if I were a school department strapped for cash, and had to choose been disinfectants and fans, I would choose fans, because aerosols are the primary means of transmission, not fans.
[2] To be fair to CDC, there are good people there, and some science is done. But institutionally? Charlie Foxtrot’s in charge.


Great stuff Lambert, as always.
Is it me, or does the international capitalist order just seem like they are throwing up their hands in the air and say “eff it”.
Let’s disaster capitalist this thing, funnel the funds to our pharma friends, and who cares if people get long-term symptoms, patients that need treatment are profitable patients.
If the goal of the vaccines was to return to “normal” – it sure doesn’t seem to be working. I mean, places are opening up now, but lots of new cases of Delta are in Germany…
https://twitter.com/dm_ms/status/1405056137758756877
The October waves might be pretty impressive…
Where “eff it” is concerned–will there be further efforts to develop tested and more reliable vaccines now that “emergency approval” will no longer be the thing? I know there are other inactivated type and hybrid vaccines being tested in France, China and India, and I am sure other places. I will be looking for the results of these trials, but not much hope of availability in the U.S.
So new questions are:
1. What percentage of vaccinated, asymptomatic individuals are carrying live virus?
2. How infectious are vaccinated, asymptomatic individuals who are carrying live virus?
3. How long do vaccinated, infected, asymptomatic individuals carry live virus?
4. Can the virus mutate in vaccinated, infected, asymptomatic individuals? (like the Kent variant apparently did in the UK, in a long term infected individual(but not vaccinated)).
5. How effective are the new vaccines compared to vaccines for other illnesses (eg do the Covid vaccines allow breakthrough Covid infection at greater rates than say the measles vaccine allows breakthrough infections for measles?)
All of this data is crucial to understanding and containing the Covid virus.
I hope someone somewhere has the funding to do this research.
Because the last thing we want are vaccinated, long term infected, asymptomatic individuals brewing Covid viruses that mutate to neuter vaccines.
“Vaccinated people are so unlikely to catch the virus…” jumped out at me. Isn’t that a giant unwarranted assumption? It looks like a predetermined outcome searching for supporting ‘evidence,’ or lack thereof.
We’re not letting our guards down just yet.
I’ll say. A friend from Connecticut wrote the other day that eight friends, all fully vaccinated, gathered for lunch–sort of an end-of-lockdown celebration, I gather. She was invited, and though also fully vaccinated, her daughter has a severe autoimmune disease so she declined the invitation, just remaining extra cautious. All eight friends tested positive for Covid following the luncheon. Don’t count on seeing this data in VAERS, or even your local newspaper.
Did the 8 friends get tested because they were experiencing symptoms?
Good question. It would also be good to know if they were infected with variants of concern.
She didn’t say–it was just a quick email. My guess would be one or two experienced symptoms and they alerted the others to get tested.
Testing via PCR is still a mystery. CDC recently specified CT for vaccinated should be <28 an appropriate level to detect illness. But CDC also said CT for non-vaxed should remain 40+, obviously to keep fear train rolling by coming up w more false positives that feckless msm would trumpet as new cases. Instead of mass heredity, we have mass hysteria coupled with unparalleled censorship of top docs & scientists attesting efficacy of early treatment rems which as matter of law, make experivax EUAs improper at best. FDA recent approval new alzheimers drug over objections of its own investigative committee shows how corrupt they are from top to bottom. Asymptomatic spreading another canard to add fear to the populous notwithstanding very few documented cases. C19 will go down as biggest, deadliest con of all time and high efficiency of Goebbels Big-Lie technique. Disgusting.
more details? 8 out of 8 seems crazy among the fully vaccinated.
It reminds me of the issue with kids and covid last year. How do you know they aren’t catching or spreading it when you refuse to test them?
Another breakthrough anecdote:
A “fully vaccinated” couple I know in their early 30s recently went to a (presumably largely unmasked) wedding in a western state. Both got symptomatic covid, as did many others at the event.
If one assumes the 95% protection number, the chance of someone getting it is 1 in 20. The chance for two people from the same exposure is 1 in 400.
I believe in vaccination and am vaccinated.
I don’t believe the 95% figure.
“If one assumes the 95% protection, the chance of someone getting it is 1 in 20.”
That’s not what the 95% means. It means that, compared to an individual who is unvaccinated
and has not had covid and is being exposed to the same environment, the risk to a fully vaccinated individual is reduced by 95%. Outside of a clinical setting [1], attack rates for even unprotected people are going to be a lot less than 100%,
and so the rate for the vaccinated is going to be a lot less than 5%.
[1] … or a choir practice. Or a mosh pit. Or a 160,000 ton net weight floating Petri dish. Or a …
Yes, “protection” means “when compared to an unvaccinated person”.
Or, one can say risk of an individual contracting covid is 0.05 * attack rate for unvaccinated.
For a given event, for two vaccinated people to both get covid, the odds are 0.0025 * attack rate for that event.
This is pretty small odds, and yet there is the anecdote. This would not have been reported to the CDC since they were both quite sick but not hospitalized.
If the true efficacy is, say, 70% the odds are considerably less unlikely.
A possible explanation:
mass transmission events are not independent in the sense of probability,
so the probabilities don’t get multiplied.
If N people, all vaccinated or all unvaccinated,
sit next to each other in the same environment for a long enough time,
either the dosage they all get from the aerosol in the air
will be sufficient to catch covid, or it won’t be.
This wouldn’t necessarily be the case for short exposures
to a contaminated environment,
but seems a reasonable model for a long exposure.
So, if the people are HVAC-downstream from a superspreader, the probability
of them all getting it might not be much less than the probability that
just one of them sitting there would get it.
Just a guess.
Listening to CDC give advice is an exercise in hermeneutics, where there isn’t a straightforward relationship with truth.
It’s almost bipolar advice, with apologies to people who are bipolar. But the advice swings from one end of the factual to the other depending on which spokesperson is talking (deputy vs dept head), who they are talking to (Congress, media, layman), the time of day (Monday press conference, weekend shows), and what the political situation is at the exact moment.
Nobody has time for this kind of silly BS, except the bureaucracy at the CDC that swims in it.
I think if I were the parent of an under-12 child, I’d want them in a school with fully-functioning windows, sitting near one, and with fans in the classroom blowing air towards the doorway(s) from the windows. Alas, many of our public schools’ windows don’t open – either because of decrepitude or because they’ve been sealed for insulation purposes.
When the first super-spreader event (that choral practice in Washington state) became public, I just sort of intuited “aerosol spread.” I’ve been masking up and avoiding indoor spaces accordingly for 15 months now.
But hey, that’s just me.
My sister is a retired nurse and teacher of nursing, she is almost overwhelmed with grief and rage about the way the CDC has handled the pandemic.
It’s a betrayal of everything she dedicated her life to for decades.
I stopped talking to her about Covid some months ago due to the pain it causes her.
She is someone who naturally trusts authority and I am a natural skeptic whose attitude has been reinforced by brutal experience, I am saddened and disgusted but not surprised.
As an aside, those who are wearing chin diapers are actually following CDC guidance in that they are both wearing a mask because it is absolutely essential to do so and totally unnecessary.
chin diapers… lol
I think anybody who uses the phrase “chin diaper” needs to take a look at how natural their skepticism really is.
I didn’t rewatch the clip so maybe slightly nsfw
Its a reference to South Park and how people maybe don’t master wearing masks properly.
The CDC’s lack of interest in tracking breakthrough cases is stunning. The only figures I’ve seen so far is that the CDC says there were a total of 10,262 breakthrough infections reported in the U.S. as of April 30, at which time 101 million people had been vaccinated.
That number is most likely an absurd undercount.
Let’s look at a state that is tracking breakthrough cases to see why.
As of June 5, there were 3,641 cases of COVID-19 among 3,500,011 fully vaccinated people in Massachusetts, according to the Department of Public Health. That works out to about 1,000 breakthrough cases per million vaccinated.
Extrapolating that breakthrough rate nationwide, there could be something in the range of 130,000 breakthrough cases out of the 130,000,000 fully vaccinated folks, at the very least.
According to the Massachusetts Department of Public Health, their number of breakthrough cases jumped 20% from May to June — from about 3,083 breakthrough cases on May 5 to the 3,641 breakthroughs cases on June 5 I already mentioned.
So either Massachusetts is an insane outlier, with nearly a third of all known breakthrough cases in the U.S., or the way the CDC defines breakthrough cases (i.e., hospitalization or death) undercounts the number of breakthrough cases by more than ten times the true number.
Since we don’t really know how infectious breakthrough cases are, this could be setting us up for more trouble.
I’ve been looking at these numbers too. Mass is now reporting 4000 breakthrough cases as of yesterday. https://www.bostonherald.com/2021/06/16/nearly-4000-fully-vaccinated-people-in-massachusetts-have-tested-positive-for-coronavirus/
Another big jump. Since we number as of May 5th we should be able to do a crude estimate how what percentage of total cases in Mass? N
I did a bit of a survey among states that are making some attempt to track breakthrough cases.
As covered above, Massachusetts has a breakthrough rate of around .1%. They seem to be tracking symptomatic cases as well as those people who are hospitalized or die.
Washington State – Appears to track symptoms, hospitalization and deaths.
As of June 12, it had 2,039 possible breakthrough cases that meet criteria out of 3,975,979 fully vaccinated people. That’s a breakthrough rate of about .051%
Nebraska – Appears to use the CDC definition of breakthrough cases (hospital or death).
As of 6/16, 631 possible vaccine breakthrough cases out of 866,030 fully vaccinated people. Breakthrough rate of about .072%.
California – Not clear what type of breakthrough cases they are tracking, but the article linked below does say that the state health department did not have information on hospitalizations and deaths attributed to breakthrough cases. Who knows what they are measuring.
Anyway, as of April 28, there were 3,084 breakthrough cases out of 12.9 million fully vaccinated. Breakthrough case rate of .024%.
Now we come to the vaunted expert on all of this, the CDC.
The CDC claims that on April 30 — the last day they collected data on all breakthroughs, not just hospitalizations or deaths — there were 10,262 breakthrough cases among 101 million vaccinated. That is a breakthrough rate of .01%.
I can’t find any more recent reports of breakthrough cases on the CDC site, but I’d be interested to see any if they exist. Right now it seems like the findings on the breakthrough case rate are all over the map. I would think that gathering and sharing this information would be a priority.
These rates are over a short period immediately after vaccination (when immunity is at its strongest) and against the background of decreasing cases overall.
There will be a lot more of them once cases start rising again even if immunity did not wane, but all the evidence points towards immunity waning and boosters being needed, probably annually.
So a registered breakthrough rate of 1 in 1000 fully vaccinated already at this point is not all that good at all. In reality there are probably 10 times that many such infections, and then there are all the factors I listed above.
Good points.
I would also note that Variants of Concern are being reported at high rates in breakthrough cases.
In Nebraska for example, variants of concern represent 232 (91%) of the 256 breakthrough specimens that have been successfully sequenced.
A recent study currently in pre print titled Variants of concern are overrepresented among post-vaccination breakthrough infections of SARS-CoV-2 in Washington State found that 100% of infections in the 20 breakthrough cases in the study were due to variants of concern.
Authors of the study defined Variants of Concern this way:
“Variants of concern (VOCs) are those strains that show evidence of increased transmissibility, more severe disease, reduced neutralization by antibodies elicited by past infection or vaccination, reduced efficacy of treatments, or failures in diagnostic detection.”
0.1 is if if vaccinated people. It’s the wrong denominator. We need to know what percentage of cases during a given period are breakthrough cases.
That number feels like it is… a bit high in Massachusetts already.
Not sure what you are asking.
As it says above in the original post:
As of June 5, there were 3,641 cases of COVID-19 among 3,500,011 fully vaccinated people in Massachusetts.
That works out to about .1%.
I understand, I’m saying the denominator of 3,500,011 vaccinated people is the wrong denominator to use because it doesn’t say anything about the prevalence of Covid, which is relevant. The right number to use to understand the efficacy of the vaccines is to know for the period of, say may to June, how many people who got covid were vaccinated. The denominator should be the total number of people who got Covid during that period, not the number of vaccinated people. That will you something.
Okay, so, for example, did a quick and dirty sum from NYT of the cases in Massachusetts from June 5-Jun 16. This is total reported Covid Cases. I got 1302. (Someone needs to double check this, I can add but did this very much on the fly)
You are saying that there were 3,641 breakthrough cases in Massachusetts as of June 5. But yesterday they reported 4000 covid cases. So that’s 4000-3,641, or 358 breakthrough covid cases covid cases since June 5th. That means that =359/1302 or, eeeeh, about 28% of covid cases are reported during that period are breakthrough cases. Which…if you are to assume that these numbers are correct and all people in these groups have an equal likelihood of getting covid (which are bad assumptions, but they ones that the vaccine companies used, so) then, you have about 61% efficacy just based off all these numbers.
So….what I am doing wrong here? Someone else have a look, please?
Thanks.
I think I follow but aren’t we talking about two different questions:
1. How many people who are vaccinated get covid?
2. How many new covid cases are people that are fully vaccinated?
If I understand what you are saying, 28% of all new covid cases in Mass. in the last two weeks are people that are fully vaccinated.
If true that is shocking. Am I missing something?
Yes, they are different questions. But the point is that without talking about the background rate, it doesn’t matter how many vaccinated people are getting COVID. It needs to be compared to unvaccinated people, otherwise it isn’t meaningful. You could just be describing a situation where…there is a very low rate of covid in the population. Which is why you need to compare attack rate in vaccinated and unvaccinated populations.
Umm….yes, if that number is right…I wouldn’t call it shocking the 95% number was designed to be an overestimate. But I think it is shocking given that all of our policy and press is using the 95% number as if it is real and telling people to behave accordingly. In that context yes.
My question is is it right? I mean, what I did was simple enough but is it right? I don’t know. It doesn’t look good. It would be good to compare it to other data, but….as you and NC are pointing out, that’s hard to come by.
The category “VOC” is misleading in this context — variants get declared VOCs for reasons other than their immune evasiveness;
B.1.1.7 is a VOC but it is not immune evasive — there is a minor drop in neutralization with it, but for all practical purposes it is antigenically the same thing.
And in that preprint you sent it is 40% of infections.
There is the inverse effect too — for something to be a VOC, it has to have been declared a VOC.
But there are a long list of variants out there that have strongly immune evasive mutations but nobody has declared them as VOCs.
They just get dumped in the “others/non-VOC” category even though they are hugely relevant to immune escape.
The “Lambda” that was declared a VOC yesterday by the WHO (and please, please, don’t use that stupid notation — the proper name for that is C.37) was very obviously such a case for a couple months since it started showing up in the databases, but until the formal declaration, it was not counted as a VOC.
The more I hear about the lack of monitoring of those with vaccinations of an experimental kind (not used in this mass way before) the less inclined I am to be convinced to stick the crap in my body.
My gut feeling is “the elites” (politicians, big business, the very wealthy, etc) have come to the conclusion (herd mentality) that covi19 should now be treated just like we do the flu.
Those who die from covid19 going forward, can go die and dissappear as usual. This plan is how essential workers have been treated, and not the estimated 50% excess deaths in the US (we are closercto 1 million not 600,000.
Now that they and friends and family are protected from hosp and death (for the most part transmission doesn’t matter), we can get back to normal!
bingo
For a long time I have operated under the assumption that Flat Earthers find me and my beliefs (in the twisted way they see them) just as weird as I find them and their beliefs (in the twisted way I see them). Sort of a draw. But the results I see after Biden’s, Mission Accomplished swan dive (or what I thought would surely be his swan dive) is suggestive that the Dems have a slight edge on the credulity level they can squeeze out of those who gravitate to their particular Suckers-Sphere.
Specifically, I thought most people would continue wearing masks and take Biden’s Peak-a-boo I can’t see any virus…It’s gone! message for what it was worth; a total disregard of more death for more profit. But no, over the last couple of weeks more and more people have removed the mask completely regardless of the venue until now it’s the odd one who is still wearing one. Here in taxachusetts no less where people pride themselves on the amount of ivy the bricks of our education buildings can boast of as well as how they look down the snout of their nose at others. Our form of rifles. The thinking state. Mr. Rational. Trump in tweed.
After all, Biden’s message was basically the mirror image (a fun house mirror) of Trump’s drink bleach message. Crazy! Bat effluent insane in light of the variants and the nothing-burger we are doing to deal with them and this whole horrid mess globally. And finally people would see the CDC, or at least it’s upper mgmt. for what it is: Rachael Maddow dressed up in a white lab coat pimping one of those old chemistry sets for kids and saying the Dems knocked it out of the park.
To be fair, Massachusetts is first and foremost reactionary. When they aren’t worried about something, they might reset to being slightly more liberal than the status quo, but Boston hasn’t earned it’s reputation by accident either. It’s not so much a case of “even Taxachussetts” but yeah, it’s Massachusetts. Matt Groening might be from Oregon (Springfield is Eugene), but the original group of writers and Conan O’Brian are Massholes. The Simpsons, the extended cast, and town are effectively a satire of Massachusetts. The kids seem to be alright, but it is what it is.
It’s not so much a case of “even Taxachussetts” but yeah, it’s Massachusetts.
Agree. But I have a tendency towards a subtle bias and it is particularly frustrating to see it consistently fail when ever put to the test.
This policy also ensures we won’t know if vaccinated people, once infected, might suffer from long COVID; I linked a Times story a few weeks ago where this seemed to be what happened to one vaccinated person, but without data collection on this, who knows? Perhaps useful information might emerge from other countries that are taking this seriously?
Indeed. This is the same argument I have been making and what Robert H. Shmerling, MD, Senior Faculty Editor of Harvard Health Publishing thinks as one of numerous reasons why this CDC decision is bonkers public health policy.
https://www.health.harvard.edu/blog/should-we-track-all-breakthrough-cases-of-covid-19-202106032471
> This policy also ensures we won’t know if vaccinated people, once infected, might suffer from long COVID
Excellent point. I should have worked that in.
Outside groups are collecting this data. From first look seems to point to being able to get long covid just fine with breakthrough.
https://twitter.com/dianaberrent/status/1402996441312677900
I find in my conversations with them that this quote sums up the consensus of the liberal mind.
But, looking closely at the data – both nationally and locally – shows positivity rates that largely mirror rates from this time last year. Basically, in answer to the question of “is it the vaccines or is it a seasonal artifact,” and given my locality has a 39% vaccination rate, it appears the decline (which strangely and exactly matches, day-by-day, the numbers of 2020) is largely seasonal.
I’m beginning to suspect from mid-October on is going to prove difficult for some people to square with their faith in the CDC under Biden.
This is something I have not seen discussed much at all.
The COVID rates we are seeing now are not wildly different from what we saw 12 months ago, another time when the Mission Accomplished people were all out in force. Now, the triumphalism is justified by the fact that about half the US population has been vaccinated, presumably important but of unknown efficacy and nowhere near the level presumed to be needed for “herd immunity” even for existing COVID variants.
I obviously hope the rates stay low going forward, but IMO at least some skepticism and caution is justified considering that everyone who up to now thought the epidemic was over has been spectacularly wrong.
Precisely – and precisely my fear.
Good post. We need real studies, and not just of the limited populations the CDC has selected.
In my flyover city, the CMO of one of the hospitals looked at Covid admissions from March 1 through June 1, and all patients except one, who was immunocompromised, were unvaccinated. (I heard of one fully vaccinated Covid case, working age with no underlying conditions, with a brief hospital admission prior to March, but I have no real data prior to March 1.) Neither of these breakthroughs was with a variant.
That 3-month data from the local hospital is useful because it looks at ALL patients admitted for Covid over a defined period of time. Real world data, or reports from the field, on asymptomatic and mildly symptomatic cases are much less useful, because of the possibility of unrepresentative sampling. Who gets tested and who doesn’t? Remember when so many were saying that kids don’t tend to get infected when, really, they were just being tested much less than adults? (There was a good presentation on kids at the last VRBPAC meeting June 10 – slides here: https://www.fda.gov/media/150050/download, and video on the FDA website and YouTube.) Grayslady mentioned a group of 8 vaccinated friends who went to lunch, then tested positive. Why did they get tested? Did they all get the virus from the same source, or did they pass it to each other? (Remember, the wide incubation period range allows for the possibility of the same date of symptom onset or peak virus with different inoculation paths.) How many vaccinated people just like that group of friends didn’t get tested?
We need good longitudinal studies of vaccinated and unvaccinated groups with frequent, routine testing, enough information about the enrollees to be able to account for behavior (e.g., masks) and prior infection, and detailed enough testing (PCR and sequencing) to be able to draw conclusions about the amount and length of viral carriage in the upper airways and to make correlations with infectiousness as shown by contact tracing. The studies should be ongoing, so we can see what happens over time to those with mild illness and determine whether the vaccines prevent long Covid, and we can see whether there are any long term side effects of the vaccine. The number of asymptomatic cases, the nonspecific nature of so many of the signs and symptoms, and the wide range of the incubation period (extremes of 2 to 14 days) make gathering meaningful data challenging; rigorous studies are needed. I think the FDA should require the pharmaceutical companies to provide such information as part of their applications for biologics licenses.
About vaccines and sterilizing immunity or elimination of a disease, I heard Paul Offit a few weeks ago say that with diseases with a longer incubation period, such as measles, German measles or chicken pox, with an incubation period of 10-14 days, there is enough time for memory cells to activate and differentiate, which takes 3-5 days. With typical mucosal infections with a short incubation period, such as the flu at 1-2 days or rotavirus at 2-4 days, there is not enough time for the memory cells to come into play to do anything other than modify the disease. Sars-CoV-2 is intermediate, with a common incubation period of 6 days, so he said that we would not expect a vaccine to completely prevent disease. Only with a virus with a longer incubation period can a vaccine induce sterilizing immunity and completely eliminate the virus and disease. (Section starts here: https://youtu.be/da2AuPN1ehI?t=1552. ) He did not specifically comment on why we have breakthrough cases now, when antibodies from the vaccines should be high, except to say that virus in the bloodstream is not an important part of pathogenesis of Sars-CoV-2, and, from other sources, I know that the antibodies are not sufficiently represented in the upper airways. During the December VRBPAC meeting about the EUA for Pfizer, the Janssen representative said that blood had been collected for nucleocapsid and spike antibodies to give an indication of whether there was asymptomatic infection after vaccination, and that data would be released at the beginning of the new year. I have yet to be able to find it, and have done a few Google searches over time. Those of a suspicious nature might think that Janssen didn’t like the result.
One last comment: we do not know as much as we would like about the vaccines, but they do seem to be effective in reducing severe disease and fatalities. In areas with the number of cases falling, an unvaccinated individual is less likely to encounter the virus and therefore is less at risk than during the peaks, but, still, emergency situations make it impossible to completely prevent exposure. You can be extremely careful, but then have a car accident on the way to your contactless grocery pick-up, or have a car swerve and hit you while walking or biking, and then all bets are off. A friend’s husband, who rarely went out, but when he did, wore goggles and double masked, with one mask being an N95-type, was taken to a busy ER late December for severe back pain, complained to his wife that he was near a Covid patient in the ER, several days later went back to the hospital short of breath, and died of Covid on a ventilator a few weeks later. I hope those here who are hesitating about being vaccinated realize that we can’t completely control our exposures, and take that into account in their risk/benefit assessments.
End of second to last paragraph about antibody testing should be Pfizer, not Janssen. Someone was talking to me about Janssen while I was typing about Pfizer, and the name made its way from my ears to my fingers. Sorry.
“Many public-health laboratories at the state and local level have been diligently tracking breakthroughs of all kinds for months, and are unsure of whether to mirror the CDC’s shifting priorities. “
Is this is infor from various places being aggregated in one place? I also fear they would be pressured to stop with an increas in the number of breakthroughs.
“…Saskia Popescu, an infection-prevention expert at George Mason University, told me. “If we’re telling people they can be unmasked and we’re still [frequently] testing them, what’s the signal we’re sending?”
AYFKM??? Hey, Mr. Alleged Infection-Prevention expert…you tell people testing during this this time is part of infection-prevention with a continually mutating virus.
The extroverts and pharma shills are going to kill us all.
Meanwhile, somewhere in the Atlantic Ocean,
The good news is that with Ron DeSantis banning cruise lines from demanding proof of vaccination,
we’ll never know whether the inevitable mass outbreak came from someone who had been vaxxed.
I am baffled by the CDC’s downplaying of aerosolization as the means this virus is transmitted.
As this article points out, “many respiratory viruses are believed to transmit over multiple routes, of which droplet and aerosol transmission paths become paramount, but their significance in transmitting the disease remains unclear.”
https://www.ncbi.nlm.nih.gov/pmc/articles/PMC7293495/
Could it be that because aerosolized biological agents have been weaponized and this association would add more sinister conspiratorial aspects to the Wuhan lab leak theory?
Or is this recognition creating too many hurdles for hospitals, schools and businesses that need a lower threshold to remain safely open without addressing indoor air quality?
The conclusion of the aforementioned article, “Transmission of COVID-19 virus by droplets and aerosols: A critical review on the unresolved dichotomy,”
It would cost money to fix the problem so we’ll just ignore it