After India finally gets somewhat of a grip on its deadly second wave, one of its health regulators just took away one of its main lines of defense.
India’s Directorate General of Health Services (DGHS) has executed a policy reversal that could have massive implications for the battle against covid-19, not only in India but around the world. Hundreds of thousands, if not millions of lives, could be at stake. The health regulator has overhauled its COVID-19 treatment guidelines and removed almost all of the repurposed medicines it had previously recommended for treating asymptomatic and mild cases. They include the antibiotic doxycycline, hydroxychloroquine, zinc, ivermectin and even multivitamins. The only medicines that are still recommended for early treatment are cold medicines, antipyretics such as paracetamol and inhaled budesonide.
“No other covid-specific medication [is] required,” say the new guidelines, which also discourage practitioners from prescribing unnecessary tests such as CT scans.
“Patients are advised to seek tele consultation; and Covid-19 appropriate behaviour must be observed such as mask, strict hand hygiene and physical distancing… [Patients are also advised to maintain] a healthy diet with proper hydration… [and] to stay connected [with family] and engage in positive talks through phone, video-calls, etc.”
The decision to remove ivermectin, multivitamins and zinc from the treatment guidelines is hard to comprehend given the current state of play in India — unless one assumes foul play. After suffering one of the worst covid-19 outbreaks since the pandemic began, resulting in the loss of hundreds of thousands of lives, India is not just flattening the curve, it is crushing it. And the widespread use of ivermectin, a potent anti-viral and anti-inflammatory with an excellent safety profile, appears to have played an instrumental role.
WHO’s Happy
Other countries in the region have already taken notice. Indonesia just approved the use of ivermectin in Kudus, a local contagion hotspot.
This is the last thing the World Health Organization (WHO) and the pharmaceutical companies whose interests it broadly represents want. As such, it was no surprise that WHO was delighted with the DGHS’ policy reversal. “Evidence based guidelines from @mohfw DGHS – simple, rational and clear guidance for physicians,” tweeted WHO’s chief scientist Soumya Swaminathan, of Indian descent. “Should be translated and disseminated in all Indian languages.”
As I posited in my recent article “I Don’t Know of a Bigger Story in the World” Right Now Than Ivermectin: NY Times Best-Selling Author, there are three possible explanations for global health regulators’ opposition to the use of a highly promising, well-tolerated off-label medicine such as ivermectin:
- As a generic, ivermectin is cheap and widely available, which means there would be a lot less money to be made by Big Pharma if it became the go-to early-stage treatment against covid.
- Other pharmaceutical companies are developing their own novel treatments for Covid-19 which would have to compete directly with ivermectin.
- If approved as a covid-19 treatment, ivermectin could even threaten the emergency use authorisation granted to covid-19 vaccines.
It’s worth noting that while India’s DGHS has dumped most cheap off-patent treatment options against Covid, including even multivitamins, more expensive patented medicines continue to get the green light. They include Gilead’s prohibitively expensive antiviral Remdesivir, which DGHS continues to recommend for “select moderate/ severe hospitalised COVID-19 patients”, even though “it is only an experimental drug with potential to harm.” It has also authorised the use of the anti-inflammatory medicine tocilizumab, which costs hundreds of dollars a dose.
Crushing the Curve
The DGHS began recommending the widespread use of ivermectin as early as April, in direct contradiction of the recommendations of the World Health Organization. Treatment packs were assembled in many states and distributed to patients testing positive for Covid. In at least two states — Goa and Uttarakhand — the medicine was distributed as a preventive. As has already happened in over 20 countries where ivermectin has been used — from Mexico, the Dominican Republic and Peru to Slovakia, the Czech Republic and Bangladesh — case numbers, hospitalizations and fatalities have fallen in almost vertical fashion. On Monday the country recorded its lowest number of new cases in 61 days. 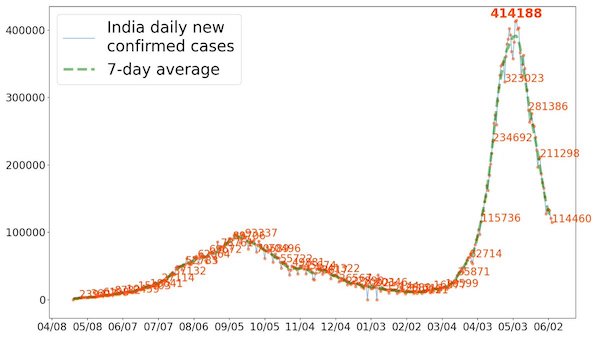
“When we started seeing more cases, we decided to take up a door-to-door survey,” Bagalkot District Health Officer Dr Ananth Desai told New India Express. “When the health officials noticed people with symptoms during the survey, they tested them immediately and provided them with home isolation kits, which had medicines like Ivermectin, calcium and zinc tablets along with paracetamol. We advised the patients to start with the medication even before their Covid-19 test results came out. With these measures, we noticed that many patients recovered faster. This helped in increasing the recovery rate”.
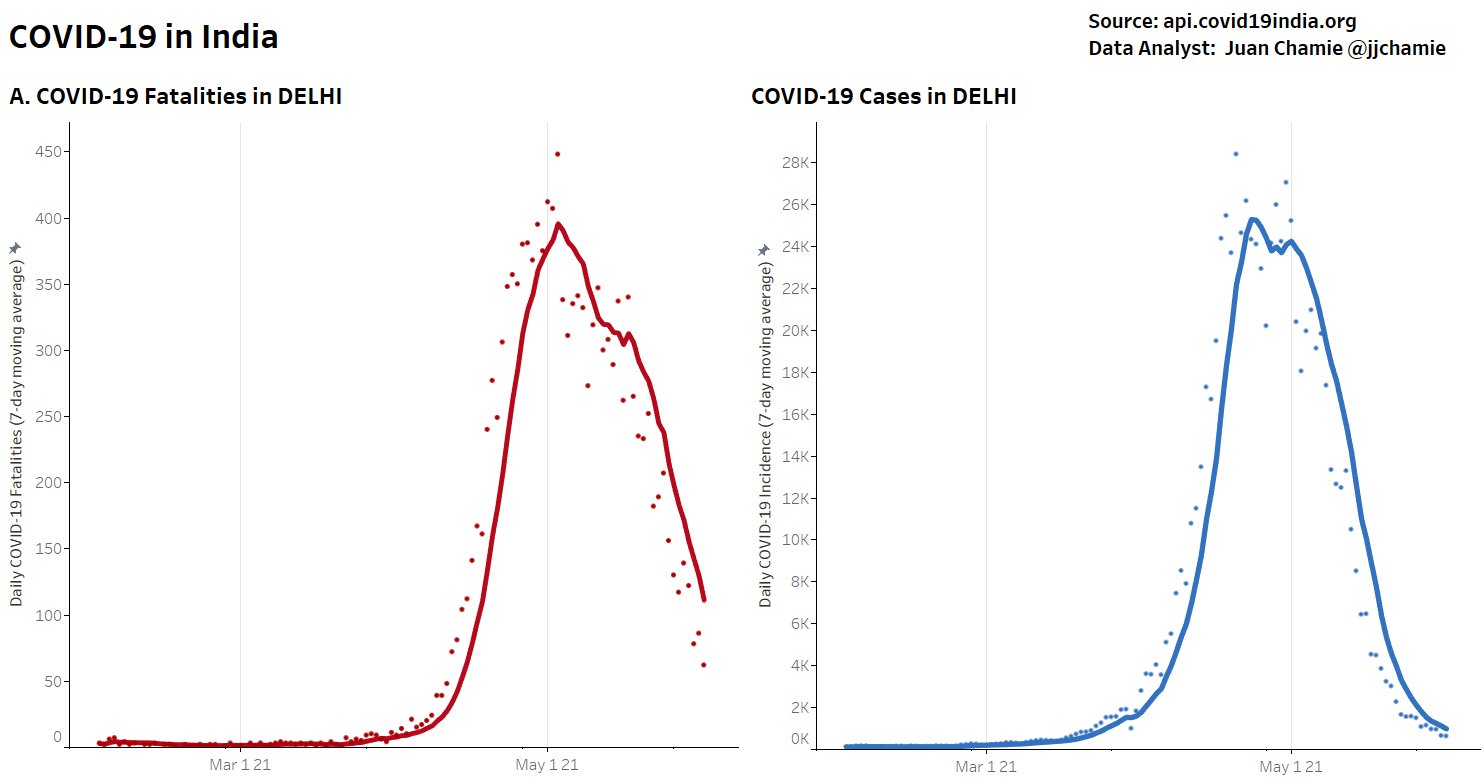
In India’s capital, Delhi, the number of people testing positive for Covid-19 daily has fallen 97% from a peak of 24,000 on April 24. The number of deaths is down by around 85%. Only 17% of the total beds earmarked for Covid-19 treatment in Delhi and around 40% of the ICU beds were occupied late last week, according to the government’s Delhi Corona app. At the peak, there were days when no ICU beds were available in the city.
Out of the Darkness, But For How Long?
Just over four weeks ago India was in a very dark place. At one point it was accounting for almost half of all global cases and one in every four covid-19 deaths. The government had lost complete control. Four weeks later, the country, while not out of the woods, is in a much better place. While the official numbers of cases and deaths are probably still a fraction of the real numbers, the trend is clearly moving in the right direction.
An important reason for that is that doctors in India have been treating covid patients as early as possible — something that isn’t happening in most countries, particularly rich ones that play an outsized role in setting global health policy. In India early treatment has helped to reduce the number of cases becoming acute. And that has helped to reduce the pressure on hospitals and vital resources such as oxygen. Ivermectin also appears to have helped reduce the spread of the virus, thanks to its potent anti-viral properties.
Just about everywhere ivermectin is used, the number of cases, hospitalizations and deaths fall precipitously. Of course, this is only a temporal correlation. But nonetheless a clear pattern across nations and territories has formed that strongly supports ivermectin’s purported efficacy. And that efficacy has been amply demonstrated in dozens of clinical studies and multiple meta-analyses. But it’s not proof enough for global health authorities, which have set the bar for ivermectin so high that it’s almost impossible to straddle.
Of course, other factors such as lockdowns, travel restrictions and increased herd immunity have also played a part in India’s rapid turnaround. But vaccines’ role has been minimal given that just 16 doses have been administered per hundred people. It’s going to take many more months, if not longer, to vaccinate a majority of the population. In the meantime, hundreds of millions of people will remain unprotected from the virus. Many will end up catching and transmitting it. Yet the Directorate General of Health Services has taken away one of the country’s only lines of defense.
It remains to be seen whether state governors and health bureaucrats will comply with the recommendations. For the moment the separate treatment protocols recommended by India’s Ministry of Health and Family Welfare (MOHFW) and the Indian Council of Medical Research (ICMR) continue to include ivermectin. As such, many doctors are likely to continue prescribing the medicine. But what happens if MOHFW and ICMR follow the DGHS’ lead and also drop ivermectin. Will doctors stop using a medicine they know to work against a virus that has already caused so much devastation?
India’s most populous state, Uttar Pradesh, has been using ivermectin since last summer. In this second wave the turnaround was so dramatic that even the World Health Organization (WHO) showcased its achievements. In a May 7 article titled “Going the Last Mile to Stop Covid-19” the WHO noted that aggressive population-wide health schemes, including home testing and “medicine kits”, had helped regain control of the virus. But what the WHO failed to mention is what was in those medicine kits.
Instead, three days later WHO’s chief scientist Soumya Swaminathan, of Indian descent, tweeted out a reminder that ivermectin is not recommended to treat covid-19 patients. The tweet included a press release issued by the company that manufactures the drug, Merck, saying it had found no evidence to support the use of ivermectin in the treatment of COVID-19. Merck, it’s worth recalling, is developing an antiviral compound, molnupiravir, that will have to compete directly with ivermectin, one of the cheapest, safest drugs on the planet — unless, of course, ivermectin is taken out of the picture.
A Cautionary Tale
But if that happens, the result is likely to be a lot more deaths. Peru, the first country to use ivermectin against Covid, is living proof of that. The medicine was first used in eight states during the very early stages of the pandemic (May-July). After showing promise, it was extended to the whole country. Excess deaths dropped 59% (25%) at +30 days and 75% (25%) at +45 days after day of peak deaths. But in October, after the first wave had been brought under control, a newly elected government in Lima took the inexplicable step of withdrawing a number of medicines, including ivermectin, from its treatment guide for the disease.
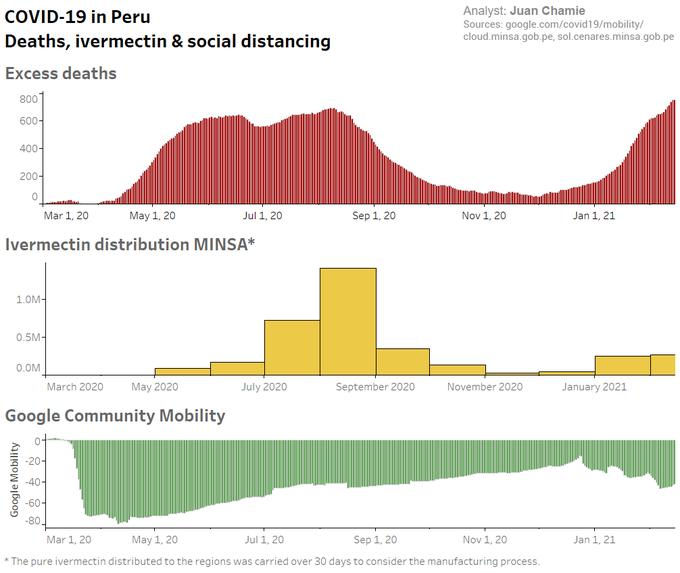
Within weeks hospitalizations and deaths were soaring once again. The graph above, taken from a study by Juan Chamie, Jennifer Hibberd of the University of Toronto and David Scheim of the US Public Health Service, shows the sharp rise, fall and resurgence in excess deaths (among the over 60 year-old cohort) in Peru as the virus waxed, waned and waxed again. Since Peru dropped ivermectin the virus has raged through the population. Peru now has the highest per-capita death rate from covid on the planet. It’s a cautionary tale that India, with a population more than 30 times that of Peru, would do well to heed.


This is so overtly sociopathic that it takes my breath away.
I suspect that swapping a velvet glove for a calving glove will have consequences.
Yes, it is overtly sociopathic. And there will be more. I fear one day it will be most of us on the short end.
Somehow, health care capitalism needs firm guidance, and control, which is gone for now.
A very strange decision IMO.
Consider the public-private, supra-national entity GAVI which is focused only on vaccines and is not accountable to any governmental or regulatory agency.
And has complete immunity. Look it up.
“Assimilation is complete. The Borg thanks you.”
Yes. Their funding is interesting, too.
https://www.kff.org/global-health-policy/fact-sheet/the-u-s-and-gavi-the-vaccine-alliance/
Complete with “innovative” financing including the IFFIm:
https://www.gov.uk/guidance/international-finance-facility-for-immunisation-iffim
adding: we know about big pharma’s interests.
The IFFIm sells vaccine bonds on the market. / ;)
https://iffim.org/press-releases/iffim-returns-market-us-750-million-5-year-oversubscribed-vaccine-bonds
It’s not sociopathic, it’s psychopathic.
“The decision to remove ivermectin, multivitamins and zinc from the treatment guidelines is hard to comprehend given the current state of play in India — unless one assumes foul play.”
Does any other assumption make sense?
This is astonishing and horrifying, and we must hope individual states’ health services ignore the DGHS.
Its getting to the point where this no longer looks like a classic case of scientific failure, it is increasingly looking like a situation whereby outright corruption is driving terrible public health decision making. It is very hard to see any other explanation for the aggressiveness of the anti-ivermectin campaign.
Or maybe it’s a case of “just hurry up and die already…”
Public Service Announcement, a list of doctors in the USA who will prescribe Ivermectin, some across state borders:
https://www.aestheticsadvisor.com/2021/02/find-doctor-prescribe-hydroxychloroquine-ivermectin.html
Chatting with my Dr, who I converted to a very silent IVM supporter, I said “It’s hard for me to believe that the health care establishment is actually killing people, until I realized it’s actually very common.
Tobacco Industry “We know we are killing people. We are making money. We don’t care”
Asbestos Industry “We know we are killing people. We are making money. We don’t care”
Lead Industry “We know we are killing people. We are making money. We don’t care”
Oxycontin Industry “We know we are killing people. We are making money. We don’t care”
Just add vaccine manufacturers to the list.
Like Bret Weinstein says, “Crime of the Century”
It’s the patents.
“If approved as a covid-19 treatment, ivermectin could even threaten the emergency use authorisation granted to covid-19 vaccines…”
And exactly when is there going to be official approval? What part of the experiment needs to be finished?
Is it the consistent production and effectiveness?
It’s like this is also some kind of operation to test how far they can go with a drug that is not officially approved.
And the final veil falls off the ugly face of late stage capitalism. I spoke last night to a friend who, along with his wife, recently recovered from Covid. His physician prescribed for them ivermectin, zinc, paracetamol and multivitamins, the very combination that’s meeting so much organized opposition led by the WHO. Global public health policy is a plaything for the rich, leveraged during this pandemic to extract a once-in-a-lifetime payday for the world’s most corrupt pharmaceutical companies. No facts on the ground wrt to effectiveness of cheap, readily available treatment modalities will stand in the way of the ravenous big pharma hordes.
Three words: Follow The Money.
I don’t know if this “press release” is legit. I can not find it on the indicated link for the Indian bar association, but if it is: “INDIAN BAR ASSOCIATION SERVES LEGAL NOTICE UPON DR. SOUMYA SWAMINATHAN, THE CHIEF SCIENTIST,
WORLD HEALTH ORGANISATION”
https://indianbarassociation.in/wp-content/uploads/2021/05/IBA-PRESS-RELEASE-MAY-26-2021.pdf
I very much hope the press release is legit. What jumped out at me was the involvement of the FLCCC, which I first learned about on the Darkhorse podcast. IMO, the world would be better off if the every decision maker in the WHO was replaced by someone from FLCCC.
Dr. Pierre Kory is one of my heroes. I’d like to meet him and personally thank him for being a doctor in the finest sense of the word.
Yes it’s legit
Use translator to translate article if you dont speak French. Scroll to the end of the article and play the Version Originale video for English version of the interview
https://www.francesoir.fr/politique-monde/livermectine-utilisee-en-inde-avec-succes-confirmee-comme-traitement-contre-la-covid
Link to the legal notice
https://indianbarassociation.in/wp-content/uploads/2021/05/Legal-Notice-to-Dr.-Soumya-Swaminathan_Chief-Scientist-WHO-1.pdf
I pointed this out when it came up the other day, so forgive me for repeating myself. It’s legit in the sense that the Indian Bar Association is a thing that exists and as such has the ability to issue press releases. But:
1. The Indian Bar Association is a marginal organisation which isn’t analogous to what might be commonly expected in the rest of the anglophone world from an organisation representing itself as a bar association. In India, that organisation would be the Bar Council of India.
2. The press release is conspicuously short on fairly important detail such as on what grounds/by which legislation is the Indian Bar Association bringing suit. It might be frivolous, it might not, but from the press release I lean toward the former.
Leaving aside the ivermectin question, could it be the cost of daily vitamins and zinc that they don’t want to pay? This reminds me of the project to develop rice with vitamin A, so that wages need not cover the cost of decent food or even vitamin pills.
That makes little sense to me — supplements like zinc, vitamin C etc and Ivermectin are cheap, far cheaper than a vaccine.
It looks like Modi will join an exclusive club along with people like Brazil’s Bolsanaro. To join it, you have to be recognized as one of that country’s largest mass murderers of your own people.
Widely available and inexpensive treatment options would be a plus given:
“As of June 1, 2021, more than 135 million people in the United States had been fully vaccinated against COVID-19.
During the same time, CDC received reports from 47 U.S. states and territories of 3,016 patients with COVID-19 vaccine breakthrough infection who were hospitalized or died.” CDC
And that:
“The number of COVID-19 vaccine breakthrough infections reported to CDC likely are an undercount of all SARS-CoV-2 infections among fully vaccinated persons. National surveillance relies on passive and voluntary reporting, and data might not be complete or representative. These surveillance data are a snapshot and help identify patterns and look for signals among vaccine breakthrough cases.”
And that there are these little buggers popping up:
“Possible attributes of a variant of concern:
In addition to the possible attributes of a variant of interest
Evidence of impact on diagnostics, treatments, or vaccines
Widespread interference with diagnostic test targets
Evidence of substantially decreased susceptibility to one or more class of therapies
Evidence of significant decreased neutralization by antibodies generated during previous infection or vaccination
Evidence of reduced vaccine-induced protection from severe disease
Evidence of increased transmissibility
Evidence of increased disease severity”
recent article here:
https://jamanetwork.com/journals/jama/fullarticle/2777389
Here’s a key part of that article based on a study of mild COVID patients with n=200 in both treatment and placebo arms: “Time to resolution of symptoms in patients assigned to ivermectin vs placebo was not significantly different (median, 10 days vs 12 days; difference, −2 days [IQR, −4 to 2]; HR for resolution of symptoms, 1.07 [95% CI, 0.87 to 1.32]; P = .53) (Figure 2 and Table 2). In the ivermectin and placebo groups, symptoms resolved in 82% and 79% of patients, respectively, by day 21 (Table 2).”
the confidence interval for time to resolution was -4 to +2 days.
I keep seeing pulling ivermectin for “mild cases”, but what about non-mild cases? What about giving to non-family members as a prophylactic?
also, this study had a few quirks that occurred during the test. The authors have explanations, but it seems like a lot happened in a small amount of time.
1. “On October 20, 2020, the lead pharmacist observed that a labeling error had occurred between September 29 and October 15, 2020, resulting in all patients receiving ivermectin and none receiving placebo during this time frame. The study blind was not unmasked due to this error. The data and safety monitoring board recommended excluding these patients from the primary analysis but retaining them for sensitivity analysis. The protocol was amended to replace these patients to retain the originally calculated study power. The primary analysis population included patients who were analyzed according to their randomization group, but excluded patients recruited between September 29 and October 15, 2020, as well as patients who were randomized but later found to be in violation of selection criteria.”
2. “Up to August 26, 2020, the placebo was a mixture of 5% dextrose in saline and 5% dextrose in distilled water, after which placebo was a solution with similar organoleptic properties to ivermectin provided by the manufacturer. Because blinding could be jeopardized due to the different taste and smell of ivermectin and the saline/dextrose placebo, only 1 patient per household was included in the study until the manufacturer’s placebo was available.”
3. “The primary outcome was originally defined as the time from randomization until worsening by 2 points on the 8-category ordinal scale. According to the literature, approximately 18% of patients were expected to have such an outcome.23 However, before the interim analysis, it became apparent that the pooled event rate of worsening by 2 points was substantially lower than the initial 18% expectation, requiring an unattainable sample size. Therefore, on August 31, 2020, the principal investigator proposed to the data and safety monitoring board to modify the primary end point to time from randomization to complete resolution of symptoms within the 21-day follow-up period. This was approved on September 2, 2020.”
Lastly, there are other RCTs on Ivermectin that showed a positive result. I hear there may be a large ivermectin RCT in the pipeline, but I have yet to see any RCT with test samples above 500. I could be wrong and/or ignorant though.
I recently described this study as embarrassing for anything other than a Junior High School Science Fair. I could be wrong, since Dr. Marik of the FLCCC recently described its quality as at the third grade level. I have never seen a paper as poor as this published in any major journal—and yes, I have the credentials to say this. Of course the ‘credentialism’ of public science has been a poor guide to the truth. One should ask why JAMA published this and not the multiple, well conducted, RCTs showing the benefits of IVM.
Meta-analysis of multiple quality RCTs is a better guide than fixating on sample size—especially this study of Lopez-Medina et al. which has too few events to make any conclusion. The appropriate sample size is chosen based on the number of events you expect and the rough degree of accuracy you wish to observe. The overwhelming evidence from meta-analysis is that IVM has major positive impacts on virus loads, progression, and death rates. Compare the IVM data to that of remdesivir which had minor -if any effects- in a small trial which led to its approval,and completely failed efficacy in a larger one. Still recommended here and in India at $3000 per treatment. For the remdesivir trial Fauci changed the end points after the study was completed and called the drug a ‘game changer’. It was to Gilead who made 3.5 billion dollars from a worthless drug.
Do you see a pattern here?
And why is it not widely known and discussed that Fauci’s favorite standard of care, remdesivir, was co-invented by Fauci’s long time pal Ralph Baric? https://www.unc.edu/posts/2020/04/30/remdesivir-proves-effective-against-covid-19-in-niaid-human-clinical-trials/
Believe it or not, Baric is also the guy who taught Batlady gain of function at Wuhan. https://www.the-scientist.com/news-opinion/lab-made-coronavirus-triggers-debate-34502 https://www.wral.com/coronavirus/controversial-virus-research-seen-both-as-groundbreaking-reckless/19098107/
Topping it off, in 2010, Baric co authored NIH paper stating that ZINC + Zinc Ionophores was effective against corona viruses including SARS-1.
Zn2+ Inhibits Coronavirus and Arterivirus RNA Polymerase Activity In Vitro and Zinc Ionophores Block the Replication of These Viruses in Cell Culture Author Summary Positive-stranded RNA (+RNA) viruses include many important pathogens. They have evolved a variety of replication strategies, but are unified in the fact that an RNA-dependent RNA poly…
https://journals.plos.org/plospathogens/article?id=10.1371/journal.ppat.1001176
Fauci and Baric knew this, but kept mum about it when covid appeared, never informing the public, or following up on the research. Both are 1st class devils.
Pfizer and Moderna did not publish clinical trial data on mild cases.
…read the comments from credentialed sources with serious doubts about the conclusion. Do you have any expertise that will tell me which professionals to believe? These days expertise is extremely fungible, seems to me… as are the conflicting reports on this controversial subject.
Where have you been blintz?
Watch June 1 conversation between Dr. Pierre Kory and evolutionary biologist Bret Weinstein Ph.D. titled “Covid, Ivermectin, and the Crime of the Century.
https://www.youtube.com/watch?v=Tn_b4NRTB6k&t=3557s
The full podcast runs 2hrs:32mins— and best to watch from the very beginning all the way through.
But you can also get the critical gist, watching from minute 59 to 1hr:30.
Dr. Peter McCullough, spent 1.5 hours answering a comprehensive array of very direct questions which will also help clarify for you the reality of the situation. The full podcast is here: https://rumble.com/vhp7y5-full-interview-world-renowned-doctor-blows-lid-off-of-covid-vaccine.html?mref=6gby3&mc=98uay
There is also a 17 minute version: https://rumble.com/vhp8e1-massive-world-renowned-doctor-blows-lid-off-of-covid-vaccine.html
Dr. Pierre Kory M.D., M.P.A Founding member of the FLCCC Alliance and co-author of the MATH+ and I-MASK+ Prophylaxis and Treatment Protocols for COVID-19
Contributions to the Field of Medicine: https://covid19criticalcare.com/wp-content/uploads/2021/01/FLCCC-Alliance-member-CV-Kory.pdf
Dr. Peter McCullough MD: https://www.cardiometabolichealth.org/peter-mccullough.html
Professor of Medicine
Vice Chief of Internal Medicine
Baylor University Medical Center
Dallas, TX
Yes, I’ve been following the dispute and am convinced that ivermectin should be front-line intervention. My response to Kelpworth was as polite as I could muster, assuming he posted it here as an attempt to further shut down the conversation. Pro-big pharma types do that a lot.
Thank you for links. Very informative.
I am open minded that ivermectin could have a mechanism of action that works in Covid. It appears to influence translocation to the nucleus of viral particles in some studies.
However, all I see in the Indian and Peruvian case charts is an exponential (strictly, logistic) curve of increase and decay in cases. It does not require ivermectin for an outbreak to subside as fast as it began. I don’t think these data carry the weight some place on them. And I don’t think a rambling podcast is the best way to sell the science.
I will check out the website for FLCC but I would like a more solid edifice of evidence built on my hope.
In the pipeline has a good recent post on ivermectin, noting what a mysterious drug it still is.
https://blogs.sciencemag.org/pipeline/archives/2021/06/07/ivermectin-as-a-covid-19-therapy
Dr. John Campbell with Dr. Tess Lawrie: https://www.youtube.com/watch?v=vYF8bnmdQfY
…and I challenge your definition of “rambling.”
Your comment chimes with my nagging observation about India and IVM, which seems so obvious that I wonder if I’m missing something or just an idiot: If IVM was being recommended by the authorities in India as early as April (after presumably a lot more time being used on the ground) and the drug is so effective as prophylactic and early treatment, then why did India have such a bad time of it in May? Supply problems? Slow uptake? Jurisdictional variances?
I share your open-mindedness (and indeed harbour optimism!) about Ivermectin, and would probably feel more comfortable taking it over one of the mRNA vaccines as it stands. I say this because some might think from my above comments that I’m anti-IVM; I’m not, just trying to be socratic. The whole thing is a bit of an epistemic headache for a layman like myself.
Basil, yes when you ask “Jurisdictional variances? “. The one (of maybe a couple) states refusing IVM, Goa, cases off the chain and continued massive increase. States using IVM: Uttar Pradesh; Delhi; Haryana; etc., cases plummeting.
The “Supply problems” are with the vaccine. Miniscule percent of population is getting vaccine. Low vaccine combined with low IVM = many cases. Low vaccine, high IVM = low cases. Hmm, an observable pattern without a randomized control trial. On your deathbed, what would you do??
This is criminal. Those graphs show that even if you can’t prove ivermectin is solely responsible for the downward trajectory, at a minimum it does not make things worse! I hope the doctors ignore the DGHS and WHO and continue to practice medicine based on their own good judgement. Otherwise, if those graphs switch direction we will know exactly who has blood on their hands.
I have upcoming appointment with Integrative Medicine doctor who is working with patients with significant post-vax symptoms and prescribing Ivermectin. At the end of Dr. Korys Dark Horse Interview he said Ivermectin also shows results in post-covid vax symptoms and his description of immune response overload to vax for some after having recovered from mild covid is my (suspected) profile too and so testing for antibodies before vax should be protocol. Yes, he is doing a tremendous service and no doubt taking alot of heat.
If this doesn’t clear moderation, I’d be glad to report my experience directly to host emails if interested.
I should also note that specialists like dermatologists and ENTs seeing significant post-vax symptoms do not have solutions at present. Steroids for tinnitus, hearing loss, head pressure (diagnosed as ototoxicity- toxic exposure damage of inner ear, cerebral nerves), persistent rash etc have not had good results. They don’t know how to address new phenomenon.
So if Ivermectin can produce relief for post-vax symptoms, it would be life changing for many.
Doctors are also sèeing results on long covid with Ivermectin. Here 2 vids of Dr Been interviewing fellow doctors:
With Dr Tina Peers (UK) https://m.youtube.com/watch?v=NOkUDh3vHVU
With Dr Syed Haider (US) https://m.youtube.com/watch?v=v8-J1ES86os
This is maddening, just like the toxic clique on Twitter, that, in The Netherlands, comes out, to repeat the hollow and stale arguments against Ivermectin all the time. One of our politicians has been bringing up Ivermectin for quite some time, and all the trolls just come out in droves, every time he posts something about this. It will be really hard to do something about the indoctrinated masses, who just repeat the main stream media talking points.
I took a rather unpleasant bruising on Twitter the other day for posting links to meta-analysis studies and other peer-reviewed studies on Ivermectin and trying to start a discussion. The sneering condescension, outright rejection and insulting comments of the scientists and doctors critising Ivermectin really took me aback. I was called a cultist, a joke, a moron, naive, accused of being ant-vax and a troll. These were doctors and scientists!? The arguments were rarely on the actaual data and, if so, only to rubbish the methodology and reluability. I was left incredulous, a bit shaken and really questioning my conclusions.
I kept seeing the discussion break down along tribal/political battlelines:
Advocates:
1. Frontline practising physicians
2. Enquiring minds (incl. scientists)
3. Vax-hesitant
4. Anti-vaxxers
Critics (to put it mildly)
1. Physicians (mostly non-frontline)
2. Scientists & Academics
3. Anti-Tump/Bolsanaro/Modi
Critics seem to think they are defending “good science” from the barbaric hoards promoting “bad science” aka unproven quack remedies.
For me is the repeated testimony of practising doctors (and the available data from multiple studies albeit of admittedly varying quality) that convinces me Ivermectin is effective. That it is quite apparently being surpressed by WHO is deeply unsettling.
Bret Weinstein made a very good point that the original official narrative push was about protecting the hospitals and ICUs from collapse and pursuing herd immunity thru vaccination. Well, Ivermectin helps keep people out hospital! And it should be seen as an integral 3rd prong alongside vaccination and infection-conferred immunity towards achieving herd immunity.
I share Dr Kory’s incredulity that doctors and scientists are seemingly content to recommend infected patients cannot be treated until they deteriorate to the point they need hospitalisation. WTF?