Medical experts and some pundits are raising alarm about the spread of monkeypox, a far more containable disease than Covid. But apparently because the public has been told to get used to endemic Covid, it’s supposed to resign itself to endemic Covid. A fresh report from IM Doc illustrates how appalling state of public health in America.
A little background courtesy Twitter:
1470 cases of monkeypox. No longer any point in comparing to the outbreak 19 years ago when we were able to contain it after 47 cases.
Is it time to say the quiet part out loud? Our individualized perspective to public health ruined our ability to control diseases.— Dr. Theresa Chapple (@Theresa_Chapple) July 15, 2022
MONKEYPOX IS NOT AN STI. MONKEYPOX IS NOT AN STI. MONKEYPOX IS NOT AN STI.
modes of transmission:
skin contact
bodily fluids
large respiratory droplets
fomites (particularly clothes n bedding)
infected animals— ☼ (@livelaughlmao) July 19, 2022
From IM Doc at the start of the week:
Today a gay patient in his 30s showed up in the office. He is healthy and very athletic. He is a “boy” to another older gay man.
They travel the world and are into serious gay fetish play. Spanking, bondage, discipline etc.
Patient has had fever and chills and horrible headache for 3 days. A reticulonodular rash has developed but no vesicles yet. They have been playing in clubs, parties, and orgies in 4 major cities the past 2 weeks.
There are so many things in that diagnostic differential but of course monkeypox is right up there.
And of course NO TESTING IS AVAILABLE. I called all levels of health department and even CDC today. The CDC is voice mail hell. Never talked to a human. It took several hours for a health dept human but by then the patient was already gone potentially spreading the wealth everywhere. They are acting as if I was talking about the Martian Flu. Again, we have known about this two months now, and it was like I was asking for the Holy Grail. Testing? “I need to call so and so……not sure…..but I’ll get right back to you……..”. And don’t get me started about their handling of the quarantine.
I have no idea if he is really a case. Multiple tests are pending. But not monkeypox. There is apparently no blood test for that. You have to swab the vesicles. But what if we do not have vesicles yet? Or if a patient may be past the vesicular stage? Crickets.
I would like to think there is a baseline competence. But that is too much an ask right now.
Again two months all over the news and this is what we have.
We are a completely unserious nation.
Remember that IM Doc is in a wealthy destination in Flyover. Apparently the local public health officials not only think that monkeypox is exclusively a gay STD, but also that they can’t have it locally because there are no gay men in their part of the world. Did they miss Brokeback Mountain? Or the private jet landing schedule?
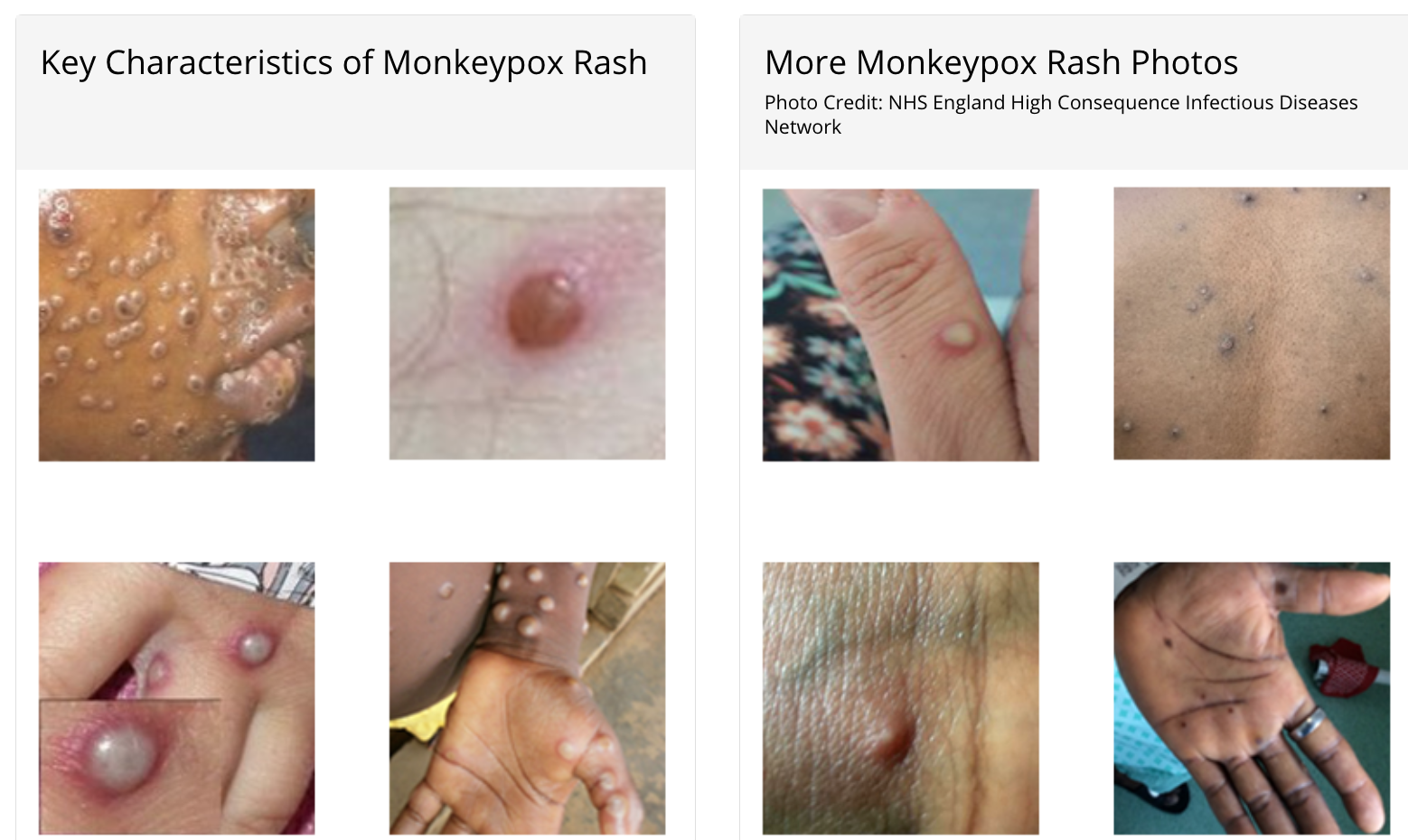
On top of that, the local public health officials appear unable to use a search engine. In fact, there are monkeypox tests, but as IM Doc did correctly infer, they can’t be used before the vesicles stage, which is 2-4+ days after lesions start forming. Oh, and monkeypox patients are contagious as soon as they start having lesions and potentially also during the prodome period, before rash starts.
Persons with monkeypox will develop an early set of symptoms (prodrome). A person may sometimes be contagious during this period.
- The first symptoms include fever, malaise, headache, sometimes sore throat and cough, and lymphadenopathy (swollen lymph nodes).
- Lymphadenopathy is a distinguishing feature of monkeypox from smallpox.
- This typically occurs with fever onset, 1–2 days before rash onset, or rarely with rash onset.
- Lymph nodes may swell in the neck (submandibular & cervical), armpits (axillary), or groin (inguinal) and occur on both sides of the body or just one.
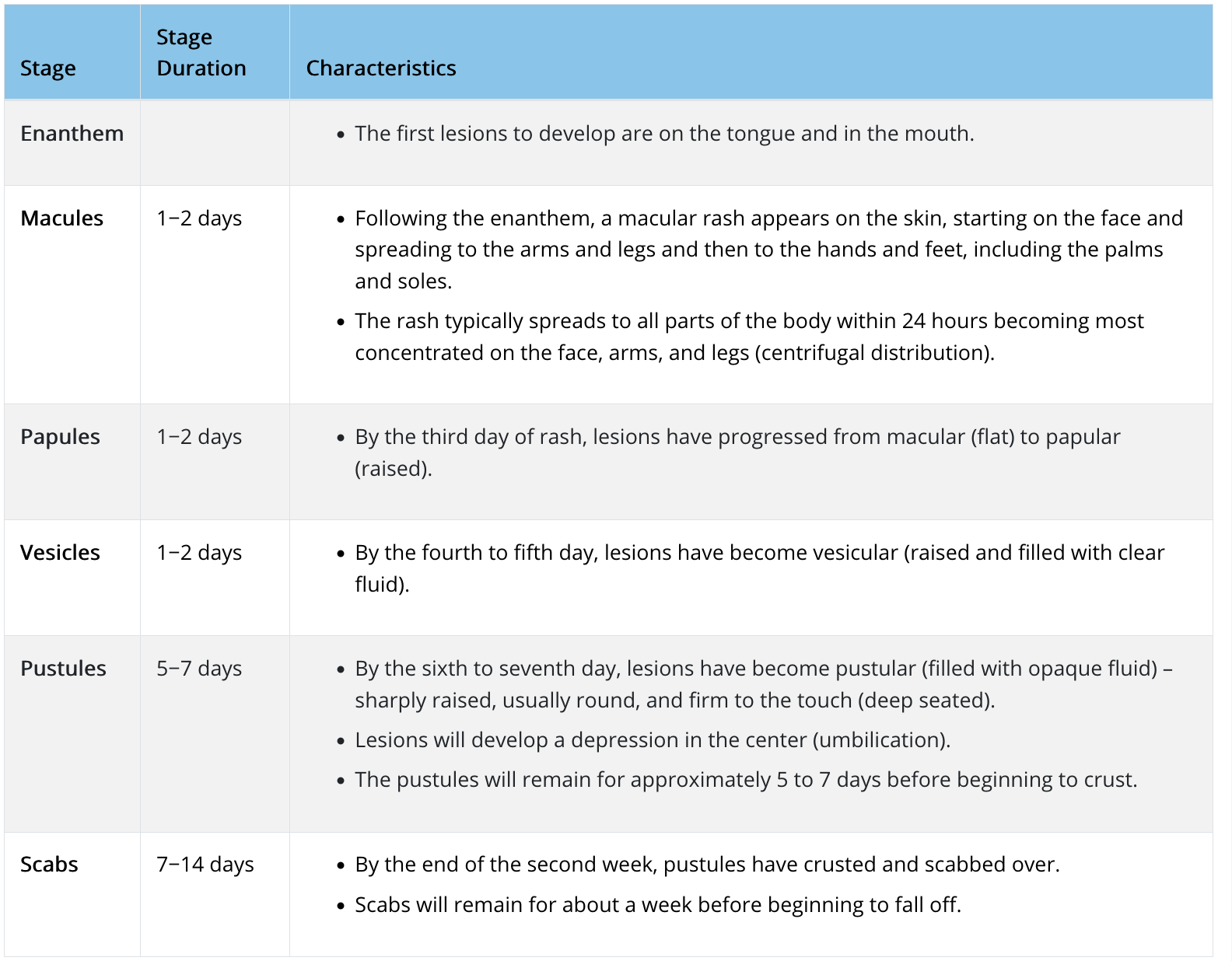
And the disease progression:
So let us return to IM Doc’s predicament. Yes, the CDC has been announcing that various labs are now testing for monkeypox. For instance, from a July 13 press release:
Starting today, Quest Diagnostics will begin testing for monkeypox. The company has developed a real-time polymerase chain reaction (PCR) test that uses patient swab specimens to qualitatively detect non-variola orthpoxviruses and monkeypox virus DNA. The test is now available to healthcare providers nationwide (except in New York)*….
Quest will offer monkeypox virus testing at the company’s advanced laboratory in San Juan Capistrano, Calif. and can accept specimens from anywhere in the country.* Quest’s testing will continue to increase the current capacity provided through CDC’s Laboratory Response Network (LRN), Labcorp, and Mayo Clinic Laboratories, providing testing capacity of up to 60,000 specimens per week by the end of July.
On June 22, HHS announced that five commercial laboratory companies would soon begin offering monkeypox testing. Since then, CDC has shipped the tests to the laboratories and their employees have been trained on their administration, among other steps.
Anyone with a rash that should talk to their healthcare provider about whether they need to get tested, even if they don’t think they had contact with someone who has monkeypox. Healthcare providers can order monkeypox virus testing from Quest as they normally would order other tests. People seeking testing for monkeypox must consult with their healthcare provider first; they cannot separately go to a Quest lab, submit a specimen, and request testing
This sounds easy-peasy, right? Except it isn’t. From the CDC Monkeypox: Preparation and Collection of Specimens (boldface ours):
Effective communication and precautionary measures between specimen collection teams and laboratory staff are essential to maximizing safety when manipulating specimens suspected to contain monkeypox virus….
Procedures and materials used for collecting specimens may vary depending on the phase of the rash (i.e., swab of lesion surface or crust from healing lesion).
For initial laboratory testing of monkeypox virus specimens at Laboratory Response Network (LRN) laboratories or authorized commercial laboratories, the recommended specimen type is skin lesion material. Specifics on the acceptable specimen type accepted within these laboratories may vary.Please contact the appropriate public health department or commercial laboratory to determine acceptable specimens.
For further characterization of the specimen at CDC, dry swabs of lesion material, swabs of lesion material in VTM, or crusts are acceptable. To ensure specimens are stored and shipped within the required timeframe, consultation with the CDC is suggested.
Personnel who collect specimens should use personal protective equipment (PPE) in accordance with recommendations for healthcare settings. Specimens should be collected in the manner outlined below. When possible, use a plastic, sterile, leak-proof container rather than glass materials for specimen collection.
Two swabs from each lesion should be collected for testing. Using two sterile synthetic swabs (including, but not limited to polyester, nylon, or Dacron) with a plastic, wood, or thin aluminum shaft, swab the lesion vigorously to collect adequate DNA. Do not use cotton swabs. It is not necessary to de-roof the lesion before swabbing. Break off the end of each swab’s applicator into a 1.5-or 2-mL screw-capped tube with O-ring or place the entire swab in a sterile container that has a gasket seal and is able to be shipped under the required conditions. Two swabs from each lesion should be collected, preferably from different locations on the body or from lesions which differ in appearance. Swabs and other specimens should each be placed in different containers. If using transport media, only VTM is accepted at CDC at this time; do not use universal or other transport media.
Specimen collection, storage, and shipping of human specimens is subject to CLIA restrictions. Specimens being sent to CDC for testing should be stored refrigerated (2-8°C) or frozen (-20°C or lower) within an hour of collection. CDC 50.34 form must be included for each specimen. When possible, ship specimens on dry ice. Specimens received outside of acceptable temperature ranges will be rejected.
Laboratory testing has indicated that the current monkeypox outbreak is associated with the West African clade of monkeypox virus. The U.S. government does not consider the West African clade of monkeypox virus as meeting the definition of Category A infectious substance under the Hazardous Materials Regulations (HMR). Therefore, specimens and material suspected or confirmed to contain the West African clade of monkeypox virus can be shipped as UN 3373 Biological Substance, Category B. See U.S. Department of Transportation’s (DOT) Transporting Infectious Substances Safely and Managing Solid Waste Contaminated with a Category A Infectious Substance (pg. 94) for further guidance.
Refer to the Poxvirus Serology test on the CDC Test Directory for further specimen storage, packaging, and shipping instructions.
For current information on the Molecular Detection test, please contact the CDC at poxvirus@cdc.gov for details on collection, storage, packaging, and shipping of specimens.
Now perhaps this sort of specimen collection and shipment is routine for many small hospitals like IM Doc’s. But the repeated “Call the CDC for instruction” suggests otherwise. So even if IM Doc’s patient had monkeypox-looking pustules that could have been sampled and tested, neither the CDC nor the local health department did a damned thing to help.
From a later message, after I had informed IM Doc that there were monkeypox tests, but only of vesicles (as he’d inferred):
Is it not a sad state of affairs that you are able to find this and the public health dept did not know the first thing about this?
I am thinking they are probably able to assist now after this incident yesterday, but it is the total lack of preparedness that is very disturbing. They did not know the first thing about testing.
And from what I am told this PCR testing is on the vesicle swabs only. My questions remain. What if the patient is in a prodrome of fever and rash but no vesicles? What if the patient has already convalesced through the vesicles? What do we swab in those instances? Are we certain that every single monkeypox patient will have vesicles? What do we do when this is highly suspected and the patient is already having a high fever and pain and rash but no vesicles? And most importantly, should any of the examples above be placed into quarantine until further notice? The fact that none of these questions could be answered and still are not today, especially the quarantine of highly suspected patients, is of the most concern to me. These are simple obvious issues that any clinician would raise and it is as if they have never been thought of before.
The patient from yesterday, for example, has been reported. Multiple blood tests for many other things done. Most of which are pending. I still do not know for sure his diagnosis, and he has no vesicles when I followed up with him today. And there is no quarantine at all.
This just does not jive well in my opinion with the level of fear they are exhibiting about this getting out of control.
This is what I have been talking about for the past two years. In the past, the CDC would have been all over making sure every primary care doctor in the USA knew exactly what the protocol was. I have heard or seen nothing. I go over my email daily. I have found nothing on their website that is more than simple platitudes. Certainly nothing that would guide me through the above questions. And to my disappointment, the health department personnel were in no better shape than I was. Just like Ebola, COVID, and West Nile virus, monkeypox is something no one of us has ever handled. I would have expected after two months for the entire system to be on the ball, and after our first scare in my area, it is clear we are nowhere near prepared. Acute public health issues like this are only as strong as the weakest link, and we failed yesterday.
This departure from past behavior from the CDC has been the most difficult for us old docs to stomach.
And to add an additional point: the fact that there is a monkeypox test of some sort suggests that the CDC is in mission accomplished mode and isn’t pushing for the development of a blood test, which would enable clinicians to find the infection earlier (and perhaps later) than the skin-sampling ones do, and would also be less nasty to administer from the patient and practitioner perspective.
So we are well on the way to having monkeypox be as bad as it could be. Scientist GM added:
We actually have no idea how bad monkeypox is right now.
Notice that there are no statistics released on how many of the cases are hospitalized, how many in ICU, etc. We had that reporting system fairly quickly with COVID back in 2020. And it is being rolled back now, with the move to weekly reporting in many places, likely to be followed by no reporting at all eventually (other than some quarterly or annual retrospective summaries)
So the lessons – that if you don’t control infections, you need to control information – have been learned.
And it is very much possible that people have died of monkeypox in the West but it is not reported yet.
So far 3 people have officially died of monkeypox in the last two months, all in Africa. And Africa has reported very few cases in that period, i.e. the CFR there is in line with what it has been historically.
Now it is certain that they have always missed cases there, but I also have doubts it is the same undercount ratio that it is for COVID, as monkeypox is a rather visible disease that drags for longer than COVID and the pain is serious.
Which means that we have the following possibilities:
1) Mortality is low in western hospitals but high in Africa where hospitals are less well equipped. That sounds attractive on the surface, but if you think about it, it doesn’t really make that much sense – it would if there were a lot of people in ICU on their death bed and we in the West are doing miracles to save them that they don’t have the resources for in Africa. But we are not hearing about that.
2) The people it is hitting right now are a lot less susceptible to dying. I doubt that though, as this isn’t a disease known to exhibit drastic differences in CFR across different populations….
3) The virus has mutated on its way to the growing pandemic outside Africa and is less pathogenic now. Meanwhile those 3 people who died in Africa got the ancestral Nigerian strain (with the 3-4% CFR, while the Congo strain with the 10% CFR hasn’t been exported at all) and this is why they died
4) We aren’t told the truth.
We will unfortunately know more in the coming months. Once schools reopen and community-wide transmission has ramped up even more, there should be massive outbreaks in children, from where it will infect parents, etc. And then there will be serious pressure on hospitals. This will likely coincide with yet another major COVID wave and your guess is as good as mine about what will happen then…
Remember that GM’s gloomy-seeming calls on Covid most of the time weren’t pessimistic enough. So take that as a warning.
And while we are at it, CDC delanda est.
–


If this continues to spread, I imagine fomite barriers that we originally got to protect against Covid may become more important, especially for health care workers (gloves and shields in particular). This virus can live on surfaces for days (up to 15 days on bedding per SF DOH). Thank you Yves and IM Doc and GM for raising awareness. There are public health experts who live and train to help out in these situations and it seems their hands are tied yet again. My heart hurts for those who are exposed and can’t get the proper help, and for the experts who have apparently been sidelined to serve other purposes.
Note that as far as mitigation of fomite spread goes, soap and water is apparently inadequate at killing the virus – 70% alcohol sanitiser the minimum needed to do the job. Gloves + long sleeved garms also advised. I’m not doing this yet bc Australia remains pretty low risk for transmission even though there are definitely cases here, but something to keep in mind for future
Yes, 70% EtOH or bleach.
Soap is not sufficient.
The reason is that apparently orthopoxvirus virions remain infectious even if stripped of their lipid envelope (which is what is destroyed by soap). In contrast, coronaviruses are dependent on it.
So you need to denature the proteins.
Oh, great, so if you go to a hotel, you need to bring your own sheets and towels?
How about my trusty povidone iodine? What if you use the OTC 10% solution and wipe yourself down with that and let it sit on your skin for maybe a minute or two before showering every day? Would that do?
The only advice I can give is to not go to hotels until you are vaccinated.
The good news here is that this a one-and-done disease and the vaccine will hold a long time too (though not as long as convalescence).
So it won’t be like COVID where whether you are vaccinated or not doesn’t change much in terms of the required behavior.
But, of course, COVID itself also means no going to hotels, and that will not change any time soon…
I’ve been going to hotels. With windows that open. After I do that, CO2 monitor = <600. I wear a N95 until I get that reading and wear it when I go out.
Monkeypox vaccine only available now to gays and trans. Not making that up. In NYC you need to meet three criteria and that's one of them. I can't imagine being able to get it here in the South.
FWIW in areas with anything approaching urban population density and the kind of wastewater levels we’re seeing here in CA, I don’t trust air coming in from the outdoors to be Covid-safe. I route air coming into our house through a room with a Corsi box next to the window, set up so that air exiting the room should have made at least a couple passes through the MERV-13’s. An unanticipated benefit is that it removes the scent of our neighbor’s dryer sheets. Helpful for my allergies too.
Please. On the >5th floor????
Please as in Oh Puhleez? Lol. Please, pretty please, and pretty please with sugar on top, don’t let your guard down too much. What would we do without you?
In built-up areas during calm weather air flow along streets and building surfaces may not involve the kind of mixing and dilution we intuitively expect from outdoor air. If smells like engine exhaust can reach your window, people’s exhalates can too.
And we’re stuck in a situation where there’s perpetually no basis yet for sound conventional wisdom about the risk of long-distance contagion from whatever our latest version of SARS-2 is.
I have never smelled any street smells in a hotel with the windows open. Evah. And I have a pretty good nose.
also re: vaccines, just for the sake of public info, my understanding is that the newer Monkeypox vaccine (Jynneos) is better than the older vaccines which have a higher incidence of adverse outcomes. I suspect availability will not be widely accessible for a while though. Please do correct me if I’m wrong.
I have read that the smallpox vaccine can help against monkeypox, is that true? Although from my understanding you would need a fresh booster as the smallpox vax I got as a child in the 50s would no longer protect against monkeypox.
Oh, and the vaccine that we have the most of, which itself sounds dangerous, is hilariously made by Emergent BioSolutions, the same shop that failed at making a SARS-COV-2 vaccine earlier in the pandemic, and has been basically defrauding the government for a decade besides. I certainly wouldn’t want to be taking any vaccines manufactured by them.
Monkeypox Case Reported in U.S. Emergent BioSolutions Makes a Vaccine.
Emergent Hid Evidence of Covid Vaccine Problems at Plant, Report Says
These people should all be in jail.
Ever since my mom got rashes after using a towel provided by a five star hotel, I always bring my own towel when traveling. Why risk it?
Also, I haven’t stayed in hotels for a long time, but whenever I stay at an AirBnb, the first thing I would do is throw all the provided bed sheet, pillow cover, etc into the washer. Again, why risk it? With this monkeypox thingy, though, the question is more, should I even bring my own pillow? If the answer is yes, the travel industry would soon be dead :(
When younger I spent quite a few nights in Youth Hostels overseas and one requirement was a sleeping sheet. It was typically a cotton sheet in the form of a sleeping bag and at the top, there was a sort of space to insert a pillow. You would sleep on a bed there and have their blankets on top and use their pillows. Maybe that might be an option for travelers – but probably larger and made of silk to save on weight.
Would you believe that one of the suggested items for young Gentlemen to take with them on their Grand Tour in the 18th century was their own sheets? Looks like we are going back to that practice.
“Oh, great, so if you go to a hotel, you need to bring your own sheets and towels?”
If you fly on an airplane, you need to bring your own seat covers?
Most people don’t have bare skin against the seat. I don’t see women wearing halters or passengers in short shorts.
Moreover the issue is getting monkeypox cooties on your skin. If you do not have bare skin on the seat, any monkeypox cooties would get on the outside of your clothes, not the part against your skin. This is not at all the same as sleeping on potentially contaminated sheets, which most do substantially or entirely undressed.
It seems to me that bare arms (short-sleeves or sleeveless) touching the backrest could be a real exposure. Granted, not the same as sleeping, but I think it could still be a problem.
Thanks for using the technical term ‘cooties’. For the non-Anglo-Americans, a cootie is the child’s version of germs, generalized to describe any invisible taintage that spreads via touch.
For example, veganism is all about the avoidance of animal death cooties. Keeping a kosher kitchen is about keeping milk cooties separate from animal death cooties.
Much of our culture war is built around cooties. Public cancellations occur when the target is tainted by unperson cooties.
Honestly, I can’t help but admire the damned things. Reading about Orthopoxvirus has been eye-opening. I find myself inclined to think that indeed, they are not alive. On the other hand, I wouldn’t call them less than alive. To the contrary, I find myself feeling rather less-than
Apparently alcohol won’t do it. Hypochloric acid is the thing. HOCl. It’s easy to make, safe, and essentially electrolysed salt water.
It also says in the same thread to use oxy clean.. which might be easier to find!
Thank you very much. Interesting products out there.
Would Clorox wipes still work?
Apparently Clorox disinfectant wipes can be used to disinfect EVPs like monkeypox according to the EPA. Here’s the list of disinfectants: https://www.epa.gov/pesticide-registration/disinfectants-emerging-viral-pathogens-evps-list-q
The best information I’ve found so far on surface disinfection pointed to using 4.8% chloroxylenol, commonly sold in the UK as Dettol: https://sfamjournals.onlinelibrary.wiley.com/doi/10.1111/j.1365-2672.2005.02601.x.
But this product seems nearly impossible to reliably obtain in the US (the sellers I found had indicators of fraud–reports of not-new and not-fully-filled bottles, product not smelling like the Dettol people had used in the UK, etc.).
As a mom, I would like to comment that there are a multitude of viral infections (Fifth’s, Cocksackie, Chicken pox, etc.) that kids are susceptible to. They all START with fever and malaise, and the skin outbreak is a LATER symptom. Terrible that testing waits for pustules and depends on them. Take care everybody!
An interesting source of info re: Monkeypox testing/testing generally is Alex Meshkin, who runs a private testing lab. His firm seems to use a saliva test for both MPX and Covid. They ran a public MPX testing clinic in LA (and testing wasn’t limited to gay men only, which it has been in some other places) and it had a 19% positivity rate, all men thus far.
And lets not forget to add in the flu during this coming wave. It’s my understanding that Australia is having a bad flu year (on trajectory to match 2019 a record year) and they typically precede the US & Europe as it’s winter there now.
You’re right, Adam. Australia’s latest weekly flu tracking report (pdf) is here:
https://www.flutracking.net/Info/Report/202230/AU
Does long ago small pox innoculation afford any protection or mitigation against monkey pox?
I don’t have sources to hand and I apologise but my understanding is: it depends. Theoretically it’s possible, but given that Smallpox vaccination campaigns were a long time ago, it’s possible that immunity will have waned for many vaccinees. Hard to predict whether it will on an individual basis or not
Apparently yes:
https://www.cbs8.com/article/news/verify/verify-yes-if-youre-vaccinated-against-smallpox-you-have-some-protection-against-monkeypox/509-1226c359-c43c-469e-9a1b-ec39cb54ec9d
Many may not remember this part about getting the smallpox vaccine.
Has me sweating a bit about masses of people now going to get the smallpox vaccine:
https://www.cdc.gov/vaccines/vpd/smallpox/public/who-gets-vaccination.html/
After you are vaccinated, you must:
Cover the vaccination site loosely with a piece of gauze held in place with first aid tape or a semi-permeable bandage (one that allows air to flow through, but not fluids).
Wear a shirt with sleeves that cover the bandage.
Keep the vaccination site dry.
If the gauze bandage gets wet, change it right away.
While bathing, cover your vaccination site with a waterproof bandage, and don’t share towels.
Change your bandage at least every 3 days. Change it sooner if it gets dirty or wet.
Wash your hands carefully every time after you touch the vaccination site or anything that might be contaminated with the virus from the vaccination site.
Try not to touch your vaccination site. Do not let others touch the site or items that have touched it such as bandages, clothes, sheets, or towels.
Do your own laundry. Use a separate laundry hamper for clothes, towels, sheets, and other items that may come into contact with your vaccination site or pus from the site. Machine wash items that have touched the vaccination site in hot water with detergent and/or bleach.
Put used bandages in plastic zip bags, then throw them away in the regular trash.
After the scab falls off, put it in a plastic zip bag and throw it away.
If you do not follow these instructions, you can spread the virus to other parts of your body or to other people.
Note: not sure but are these precautions only for the ACAM2000 vax?
Meanwhile, Jynneos has not been as broadly used so there could still be issues that weren’t revealed in clinical trials.
And the CDC site says smallpox vaccination is good for 3 -5 years….
“Smallpox vaccination can protect you from smallpox for about 3 to 5 years. After that time, its ability to protect you decreases. If you need long-term protection, you may need to get a booster vaccination. Find out who should get smallpox vaccine….”
I prefer to look at a source that might be trustworthy. I found a study dated 2008 which is titled
Immunity from Smallpox Vaccine Persists for Decades
Excerpt from abstract:
RESULTS
Vaccinated participants maintained antivaccinia IgG and neutralizing antibody titers above 3 natural logs essentially indefinitely. The absolute titer of antivaccinia antibody was only slightly higher after multiple vaccinations. In 97% of the participants, no decrease in vaccinia-specific antibody titers was noted with age over a follow-up period of up to 88 years. Moreover, Baltimore Longitudinal Study of Aging participants who survived active smallpox infections in their youth retained antivaccinia antibody titers that were similar to the levels detected in vaccinated subjects.
CONCLUSION
These data suggest that multiple or recent vaccinations are not essential to maintain vaccinia-specific antibody responses in human subjects.
…
ncbi.nlm.nih.gov/pmc/articles/PMC2610468/
https://www.cdc.gov/smallpox/vaccine-basics/index.html/
“Smallpox vaccination can protect you from smallpox for about 3 to 5 years. After that time, its ability to protect you decreases. If you need long-term protection, you may need to get a booster vaccination. Find out who should get smallpox vaccine….”
I don’t really see anything about how much it decreases. To 85% or to 10%…so there’s that.
https://www.cdc.gov/poxvirus/monkeypox/clinicians/smallpox-vaccine.html/
There is this to remember about the vaccines too:
ACAM2000 is administered as a live Vaccinia virus preparation that is inoculated into the skin by pricking the skin surface. Following a successful inoculation, a lesion will develop at the site of the vaccination (i.e., a “take”). The virus growing at the site of this inoculation lesion can be spread to other parts of the body or even to other people. Individuals who receive vaccination with ACAM2000 must take precautions to prevent the spread of the vaccine virus and are considered vaccinated within 28 days.
JYNNEOSTM is administered as a live virus that is non-replicating. It is administered as two subcutaneous injections four weeks apart. There is no visible “take” and as a result, no risk for spread to other parts of the body or other people. People who receive JYNNEOS TM are not considered vaccinated until 2 weeks after they receive the second dose of the vaccine.
Clinician told me a bad strain of Influenza type “A” (the one that quite often causes pandemics) is prevalent in Australia (I have dual citizenship with there). So Northern Hemisphere will no doubt put a broad strength version of a vaccine against A types in the triple/quadruple cocktail for the autumn vaccination schedule.
I’ll just enter the age range for automatic eligibility for RNA based 4th anti-covid “vaccine”. Not yet sure if I want it. I’m already back under cardiologist care to add to other specialists required since my first infection in Feb 2020.
Monkeypox? I’m still reading the literature….. But I won’t be getting it by getting jiggly with anyone! Meanwhile we remain in avian flu zone.
“Don’t worry, only Gay men get it” should set off alarm bells for anyone who remembers the AIDS epidemic.
I’m old enough to have seen how disfiguring smallpox scars can be, how soon will plastic surgeons start specializing in MPX scars?
And what’s going to happen when it hits Sidwell Friend’s school or the public schools in Atherton,Piedmont and Beverly Hills?
It’s seriously disfiguring (Unlike Covid) and that is going to cause panic and outrage amongst the PMC and their betters.
If it were a class marker (Only the poors look like that!) it would be OK, but how well will the Kardashians and their ilk deal with suddenly becoming as ugly on the outside as they are on the inside?
And a 3 week quarantine In the USA?
It’s going to be an interesting next six months.
“And a 3 week quarantine In the USA?”
3 – 4 weeks. And it’s going to be something that’s visible and undeniable. The USA will be lost without it’s default response of denial.
As I said, It’s going to get WEIRD.
Did IMDoc try contacting PrEP4All (btw excellent fact sheet there with graphic NSFW images)? They have been pushing this issue hard and are encouraging people to contact them.
They also have a petition to the federal government.
And any attempt to get the vaccine for the patient? Supposedly it can help with speeding recovery.
Monkeypox is airborne. Airborne. Not droplets. Airborne. Like Covid.
It was listed so until weeks ago by WHO and CDC. And then they put the information down.
The US is undercounting cases by the thousands. Spain has the highest official per capita rate. If you apply that rate to the US, there should have been 20 thousand diagnosed cases by now.
RUI,Smallpoxisn’t airborne either as of a few weeks ago.
Think of all the problems we could solve the same way!
Homelessness, poverty,corruption,the list is almost endless.
Every day will get better and better in this, the best possible possible Country in the World.
Don’t believe me?
Ask Dr Jill.
It is not airborne in the way Covid is airborne:
https://www.cdc.gov/poxvirus/monkeypox/transmission.html
And from Advisory:
https://www.advisory.com/daily-briefing/2022/06/09/monkeypox-transmission
“It is not airborne in the way Covid is airborne”
That doesn’t make any sense. It is either airborne or it isn’t and you quote info confirming it is. It is kind of ironic to quote the CDC as a reliable source of info on a post where you are disparaging the same CDC. As I said, the CDC took down their own info on monkeypox being airborne. How long did it take them to admit the airborne root for Covid?
If what you mean is that it is less infectious than Covid, that is a different issue.
“However, it is not clear how much airborne transmission contributes to the overall spread of the virus.” At the speed cases are growing, I would say airborne is an important root of transmission.
But that is not my point. Airborne transmission is a reality that is being severely hushed down for monkeypox. There will be a price tag for this denial.
I imagine you mean it doesn’t transmit in that fashion nearly so readily?
I mention this because people who really, really ought to know better have described it as a big fat heavy DNA virus with a whole bunch of genes that falls to the floor quickly. Personally I’m inclined to think that anything that can fit inside a single human cell can float in the air just fine.
I haven’t seen any real discussion of the matter, but I’ve been assuming that this is an issue of infectious dose.
As always I’m happy to be corrected if I’m off on the wrong foot, but my impression is that so long as the virus is moving in and out of its animal reservoir there may not be much selective pressure towards infecting humans at a lower dose: The virus pays a price in genetic diversity with each passage through one of us, and the more virions along for the ride the more potential there is to reclaim some of that later, once safely ensconced in a nice rodent population.
That changed with the variolas, they became commited to us.
I should have said aerosolized, which is the degree of alarm consistent with the opening comment. There is no evidence whatsoever that monkeypox is aerosolized. It appears to be droplets and even then to require a fairly high exposure to produce an infection.
Forgive me, I’m going to be pedantic, because it’s such an important subject. Transmission without physical contact is evidence for aerosol transmission, and transmission without physical contact with the persons or animals believed to the source of the infection has in fact been documented for monkeypox.
If transmission only occurs over relatively short distances, that is evidence for constraints on aerosol transmission, but the relative probability of such transmission occuring via particles which descend directly to the ground versus via those small and light enough to float about a bit is very low. The ones that float about, even briefly, are aerosols
Last time I checked, large droplets had only ever been demonstrated causing transmission via direct contact, or by fomite formation.
You are not using terminology correctly, so you are off base in your “pedantic” finger-wagging.
Aerosol is not the same as droplets. Aerosol and droplets are both subsets of airborne. You mean airborne. I SPECIFICALLY said aerosol.
In simplistic terms, aerosol = hangs in the air.
Droplets = goes thought the air but pretty quickly fall to the ground or on a surface.
Monkeypox is transmitted through close contact. That is not consistent with aerosol. The (very few) case of contracting monkeypox without close contact are among health care workers in the same facility as active monkeypox patients (and perhaps a prison too). These are institutional settings with inmates/patients sleeping (using sheets), bathing (using towels), and eating multiple meals. It has NOT been reported in other settings like schools or other workplaces where there were monkeypox cases. You’d see it in many many more settings if monkeypox were transmitted via aerosols.
Given that fabric used by the infected is a known infection vector, and ordinary laundry does not deactivate the virus, it is far more likely that these HCW contracted it via things like handling linens or contact with surfaces.
‘Close contact’ is a circumstance, not a mode of transmission. This is important because the CDC et al have often used the term for purposes of obfuscation.
Even inside two meters distance from an infected person, the liklihood of one’s inhaling ‘big’ 100 micron aerosol particles from their exhalates is much greater than the liklihood of inhaling larger droplets. Monkeypox virions run about one fourth that diameter.
Thus your assertion that observed spread is inconsistent with aerosol tranmission amounts to an assertion about monkeypox’s ability to infect the respiratory tract. If its efficacy at that is low then you’re describing spread that is quite consistent with aerosol transmission.
There are case accounts from Nigeria (a driver and a ferryman) and from the ‘pet prarie dog’ outbreak here in the US some years back, where direct physical contact, contact with body products, contact with fomites and inhalation of large droplets all seem to have been unlikely.
Household attack rates in Nigeria run around 50%. Sleeping outdoors is associated with lower risk. This is a pattern consistent with aerosols as one mode of transmission. I can’t comment on what sort of pattern would be consistent with large droplet transmission because, I say it once again, so far as I’m aware this has never been documented for any disease.
I have less respect for the CDC than I do the Uvalde PD.
The rank physical cowardice and incompetence at Uvalde pales to near invisibility compared to the Moral Cowardice and venality of the CDC which has resulted in hundreds of thousands of unnecessary deaths.
The actions of both are unforgivable but the damage done by the CDC is orders of magnitude worse.
Is anyone here foolish enough to think that Wolensky or Fauci will be held responsible for their depravity?
“Wolensky or Fauci […] held responsible for their depravity?”
In this life? Only if the torches and pitchforks arrive in time for them to be drug out of their holes and presented to a people’s tribunal. In the next? Should there be one, I hope, by the many and several deities I honor, that each enjoy an existence of pain and darkness, forever fully aware of their condition, until this universe in turn ends. As I speak it, so be it.
I am frustrated because those of us with serious chronic illnesses have been screaming this since Bush II was in office and they began seriously dismantling the healthcare system.
On the flip side of this coin, our hospital (large tertiary academic/trauma center in a major metro area) has a monkeypox testing and isolation protocol in place and our lab performs the test in house. We’ve picked up a few positives too. On this issue, we’ve had excellent communication between local public health agencies, hospitals, and infection control. That’s been my perception from the ER anyway.
I certainly do not mean this in any kind of negative way.
But I feel I need to reiterate my comment above about the fact that public health in a society is only as strong as its weakest link. I fear we have all kinds of weak links all over this country.
I too was in an academic big city environment for decades. And there was absolutely much more support there. I would say from talking to colleagues lately that what has changed in the past few years is that the center in which I worked has just taken it upon themselves to be prepared for things because the vacuum from public health and CDC was so intense.
I am also very concerned about what “public health” has become in our big cities. For the past 2 years, it has been forbidden to have simple human things like having patients surrounded by their family members upon death in nursing homes, to be present for births, and so many other things. All forbidden because of COVID.
And yet – for monkeypox – why we as public health dare not say anything about anonymous gay sex – because we would not want to offend any marginalized communities. It is as if the lessons of the 1980s and the gay bath house superspreader events in AIDS – were just thrown right out the window. At this point, this really does seem to be concentrated in that one community. How much of an ask would it be to have public health really work on the value of giving up that activity for just one month.
But public health in our big cities is just not going to do that – would not want to offend anyone. In fact, I have read reports where they are bending themselves into pretzels to allow anonymous gay sex to continue – and in so doing actually endangering the health of the public. Anyone saying anything like I am saying in this comment is immediately branded a bigoted homophobe. Interestingly, this exact tactic was used to horrible effect in the 1980s during the AIDS crisis.
So right now – monkeypox is largely confined to that one group – but that will not be the case for long. A golden opportunity to halt the spread – and again we are not going to offend anyone in a marginalized group.
For a vigorous discussion of this and many linked stories in multiple cities – I would point you to this substack article.
So it seems we have multiple problems with public health both in our rural areas and our big cities.
I would say to American citizens that at one point, these institutions – the FDA CDC and NIH were the crown jewels of your country. It is like we have thrown the pearls to the swine.
To be only a bit snarky, the only true crown jewels in this country are the DOD, CIA, and NSA. All other jewels are subordinate to these crown jewels.
Heh, I don’t know, NSA got pwnd pretty badly only a few years ago. So not crown jewels in the sense that IM Doc probably means, in that they’re highly competent institutions. But definitely darlings when it comes time for Congress to appropriate funds without limit.
While the public health establishment has anxiety about offending anyone, at least some gay activists – particularly those whose history includes the bad times of the AIDS pandemic – are loudly pointing out that while this isn’t a ‘gay’ disease, it predominantly affects men who have sex with men and that is the population that needs to be targeted with interventions of all types to contain the virus.
Not that the PH establishment is apt to listen to them.
As a side note, back in the day ACT UP advocated for healthcare for all, having come to the realization that diseases do not exist in isolation. Wish the US as a whole could understand this basic concept.
I think sent a comment on this into the ether. If I got modded then apologies for repeating myself, and making you guys repeat the modding.
IM Doc, I think you’re missing half the picture. You seem to see the failure to address the need for restraint on the part of the population currently most affected as an issue of wokeness. But is there anything remotely woke about the sotto voce peddling of this disease as a gay plague?
Having the disease blow up catastrophically among gay men first and only then become visible to ‘normal’ people will ensure an angry, bogus controversy, driven by homphobia and deranged id-pol. This will provide all the pr cover necessary for a policy of unmitigated spread.
You’re also mistaken about those agencies. Large-droplet transmission was a theory, abundantly falsified, and with literally zero supporting evidence, that was promulgated by our public health establishment for seventy years after it should have been trashcanned. Needless death and unecessary suffering was not only allowed, but excused, by lies, on a vast scale, long before Covid.
Everything from seasonal flu pandemics to rampant nosocomial infections and medication-resistant pathogens are afflictions we encounter as a matter of course in our lives, but ought to regard as outrages.
The jewels were paste, the pearls were plastic, and the swine were already running the joint. Per GM, our public health Prime Directive is “Never Again!” (to the New Deal.)
>>>But public health in our big cities is just not going to do that – would not want to offend anyone.
I would think death or disability would be much more offensive. This foolishness itself is so blastedly offensive.
“public health dare not say anything about anonymous gay sex – because we would not want to offend any marginalized communities”
Pardon the expression but this is indeed low hanging fruit. What happened to NC being a stan for all things personal responsibility and non-pharma intervention, a la covid? Odd that.
and who exactly comprises the “marginalized communities” in this instance?
those “marginalized communities” IM describes, gallivanting global hedonist vectors on private planes to attend creepy-fabulous anon orgies? that marginalized community? is it too early to blame climate change?
and if the pox vax is reserved only for the marginalized, why? and who then is marginalized?
As a hairstylist/barber I am concerned. Sometimes there are pustules on the head and neck.
We use disinfectant on our clippers and trimmers, and hand sanitizer, but not sure what else to do to help with prevention.
Some of my coworkers have apparently stopped believing in germs, and stopped cleaning surfaces between clients. I am the only employee that wears a mask everyday.
Yes, that was one of the predictable (and predicted) effects of not containing COVID – concern about all other infectious diseases would also go away. And it has.
Youtube is filled with memes etc. that hold that monkey pox is just another power play by elites. One image summed it all up succinctly: “Take off your mask and smell the bull$hit!” But as discussed above, monkey pox is going to be impossible to ignore or brush off as a bad cold.
and now Marburg in Ghana
https://www.vice.com/en/article/4axwyp/ghana-marburg-virus-west-africa
lets make certain that the airfare is at a discount, and pshaw on robust quarantine…
sigh.
i’ve been necessarily avoiding the news, here lately…but i did come across a tidbit somewhere that monkeypox is difficult to distinguish from smallpox in a clinical setting…especially with a healthcare system that hasn’t encountered either of them in decades, at best.
this has had me ruminating on Jackpot Potential: flood the zone with Monkeypox, make sure to hamhand the entire ordeal(as much anecdata seems to indicate)…then release the Real Thing.
Blame it on Russia…
and repair to one’s bunker to wait…and emerge to a world with a lot fewer humans.
numerous existential problems solved!
my conundrum: when to i shoot the tires on all our vehicles…perhaps fell a tree or two across the dirt road…to keep the boys on-site?
doesn’t look like vaccination is gonna be in the cards,lol.
for us, at least.
I’ll appeal to the Brain Trust to correct me if I’m wrong, but from what I’ve read the orthopoxvirsuses should all be considered smallpox-in-waiting.
I’m oversimplifying of course, but if an orthopoxvirus goes on a long enough sojourn in Homo Sapiens, without chilling in some rodents for a nice long while, then it’s going to either become smallpox, or die out. This is why letting monkeypox spread is so monstrously outrageous.
Monkeypox resembles smallpox enough that it wasn’t recognized as a human pathogen till smallpox had been all but eradicated, and outbreaks of what looked like smallpox continued in central Africa.
“I’ll appeal to the Brain Trust to correct me if I’m wrong, but from what I’ve read the orthopoxvirsuses should all be considered smallpox-in-waiting….”
Starting to suspect the same thing. A big ?
The JYNNEOSTM probably isn’t considered a monkeypox & smallpox vaccine for nothing.
That is correct. MPX is smallpox, it’s just that it is convenient to pretend it isn’t.
It’s also forgotten that smallpox itself existed in two varieties — variola major and variola minor, The former was really bad — up to 30% IFR, the latter was much milder — 1% IFR.
There was also a lot of variation between different strains of variola major, some were more pathogenic than others.
Monkeypox in Africa had two strains, one with 3-4% CFR, and one with 10% CFR. Cases were missed so we don’t know the true IFR, but still, MPX basically fell in between the two smallpox strains in terms of lethality, i.e. it was worse than the variola minor smallpox we still diligently eradicated in the late 1970s.
The curious thing is that all the pathogenic orthopoxviruses appear to derive from largely harmless strains. If I recall correctly, something resembling camelpox is the ancestor, though camelpox itself is smallpox-level bad for camels (but not for us).
Most importantly, pathogenicity here evolves by losing genes — these things have very large genomes with hundreds of genes, and a common trait between the pathogenic strains compared to the more benign ones is loss of some of those genes.
I am not sure if it’s known why exactly that results in increased pathogenicity. But the important thing is that this makes the “mild” strains a ticking time bomb, as losing genes is very easy in evolution. Gaining things is much harder.
In fact it increasingly looks like smallpox itself wasn’t as bad when it initially jumped onto humans as it was in the last few centuries — it mutated towards much worse somewhere around the end of the Middle Ages.
For these reasons the people who studied smallpox had been warning for decades to pay very serious attention to MPX — because we eliminated smallpox but if we allow MPX to establish itself, we are at the mercy of evolution and eventually we might allow it to evolve into something as bad as smallpox again.
But then COVID came and here we are. The WHO, the CDC, and every other public health institutions in the world are completely corrupted and degraded in competence and capabilities, and the very idea of infection control has been killed.
Your monkeypox … to smallpox scenario is reminiscent of the nanobot scourge in Hugh Howey’s “Silo Trilogy”.
Ghana…interesting. Also caught this on the CDC website:
https://www.cdc.gov/poxvirus/monkeypox/outbreak/us-outbreaks.html/
2003 Outbreak from Imported Mammals
In 2003, forty-seven confirmed and probable cases of monkeypox were reported from six states—Illinois, Indiana, Kansas, Missouri, Ohio, and Wisconsin. All people infected with monkeypox in this outbreak became ill after having contact with pet prairie dogs. The pets were infected after being housed near imported small mammals from Ghana. This was the first time that human monkeypox was reported outside of Africa.
What caused the 2003 U.S. outbreak?
Investigators determined that a shipment of animals from Ghana, imported to Texas in April 2003, introduced monkeypox virus into the United States. The shipment contained approximately 800 small mammals representing nine different species, including six types of rodents. These rodents included rope squirrels, tree squirrels, African giant pouched rats, brush-tailed porcupines, dormice, and striped mice. CDC laboratory testing showed that two African giant pouched rats, nine dormice, and three rope squirrels were infected with monkeypox virus. After importation into the United States, some of the infected animals were housed near prairie dogs at the facilities of an Illinois animal vendor. These prairie dogs were sold as pets before they developed signs of infection.
All people infected with monkeypox became ill after having contact with infected pet prairie dogs. A study conducted after the outbreak suggested that certain activities associated with animals were more likely to lead to monkeypox infection. These activities included touching a sick animal or receiving a bite or scratch that broke the skin. Another important factor was cleaning the cage or touching the bedding of a sick animal. No instances of monkeypox infection were attributed exclusively to person-to-person contact.
How was the outbreak contained?
CDC and the public health departments in the affected states, together with the U.S. Department of Agriculture, the Food and Drug Administration, and other agencies, participated in a variety of activities that prevented further spread of monkeypox. This included extensive laboratory testing; deployment of smallpox vaccine and treatments; development of guidance for patients, healthcare providers, veterinarians, and other animal handlers; tracking potentially infected animals; and investigation into possible human cases. Partners in the response issued an immediate embargo and prohibition on the importation, interstate transportation, sale, and release into the environment of certain species of rodents including prairie dogs. FDA later rescinded the part of the order that restricted the capture, sale, and interstate movement of prairie dogs or domestically-bred African rodents, but CDC’s restriction on the importation of African rodents remains in place.”
________________________________________________________________
That 2003 outbreak where no instances were attributed to person-to-person contact speaks to the mutations that have been incubating.
“flood the zone with Monkeypox, make sure to hamhand the entire ordeal(as much anecdata seems to indicate)…then release the Real Thing….”
We’re about to find out how well someone fares who comes down with Covid and then gets Monkeypox or vice versa.
That may be enough to do the trick.
I live in one of the Bluest parts of California in a town full of “Highly educated” people and mask wearing is almost nonexistent.
Since Sebastopol also has an older population ( Lots of well to do retirees) I suspect that we’ll be starting to see a lot of them become very ill or die starting real soon.
I have seen quite a few people I am acquainted with who are older than I (68) eating in packed restaurants or attending large social events unmasked.
Many of them have serious health issues.
It’s going to cause a large transfer of wealth to younger generations ( And the SPCA) and put Social Security on a sound financial basis…
Don’t forget all the summertime time visitors and vacationers to the area especially as the weather makes it just great for the drive.
So far I’ve only read about the acute phase — Can infection leave someone in a similar situation to long-COVID? If so, I’d expect that to be suppressed as well; You can’t trust any official communication any more.
Post-viral syndromes are far more common and serious than most people seem to realiize. SARS-CoV-2 is exceptionally bad in this regard, so if anyone wants to they can claim monkeypox isn’t that bad, but that’s like saying someone’s not as evil as Hitler.
Researchers in Africa have reported various apparent sequelae to monkeypox, including an elevated rate of suicide among survivors.
I’ve wondered about this much lately; Have I just been lucky and dodged long term repercussions (that I’m aware of) from various viral infections I’ve gotten throughout my life? If we did a random population sample, what would we actually find? Are all kinds of viral and bacterial infections more damaging than we’re aware of?
Disconcerting.
But I guess it was always silly that I assumed anytime I got sick with a ‘common cold’ I’d just recover; I guess not everyone always does.
It wasn’t until this Pandemic that I found I needed to become a virologist and public health expert; I thought we had, you know, experts for that, at the CDC, or something.
Of interest with regards to this theme: just this year, landmark research showing a strong plausible causative link between Epstein-Barr virus and Multiple Sclerosis was published
There won’t be LongCOVID, but there are still quite bad sequelae — some of the common complications of smallpox were blindness (pustules and then scars can form on the eyes), and osteomyelitis in children leading to deformities.
And, of course, the facial scarring.
Well I would say “Send him to Oregon”. But obviously not a solution.
I know the Oregon Health Authority here asked for some number of “thousands” of Monkey Pox tests a couple of weeks ago from the CDC. No idea if we actually received them. So here there is some planning, the OHA seems to actually care about the health of the state’s citizens. That doesn’t mean they are competent though.
Though the u.s. is the land of my birth and the place where I have spent my life, I feel as if I am become a stranger in a strange land.
I wonder whether video games like Metro 2033 might suffer a drop in popularity as day-to-day life grows ever more similar to the dystopian worlds of their game play right down to the necessary costumes of protective gear.
Just checked SCAN’s monkeypox page:
https://soe-wbe-pilot.wl.r.appspot.com/charts#page=overview_mpxv
So far they’ve had signal from Palo Alto, San Jose, Gilroy, Sacramento, both of the SF plants in the project, and CODIGA, which is at Stanford. Before July 1 it was only in SF.
Last week I saw an estimate from Europe of R0 ~ 1.5. Given that half the population is without immunity, and that this time around people really might catch the ‘gay’ disease from a toilet seat, or from sharing a taxi, we’re looking at a catastrophe that, for the US at least, will be worse than HIV. I don’t say that lightly. AIDS cut short the lives of two men I knew when we were kids. Given the current state of healthcare, if monkypox isn’t stopped we’ll be lucky if it’s only one child per classroom.
Once it gets into schools, we have a recipe for catastrophe.
Even if it’s indeed attenuated.
And if it’s not and it is as bad as it has been in Nigeria, all hell will break loose.
Because while grandma could be heartlessly triaged and people would very seriously talk about the need to sacrifice the elderly for the economy, this will hit very differently as now kids are highly vulnerable. If you have a lot of kids in serious condition with MPX, there will be nowhere to treat them — kids generally don’t get sick all that much and this is why pediatric hospital capacity is very limited. So you will have a lot of very angry entitled parents (who will likely be sick themselves too) with a lot of practice in wanting to speak to the manager and demanding explanations.
The reason smallpox could be “lived with” back in the days was that immunity is lifelong (unlike COVID, which cannot be lived with because immunity to it is very short lived, meaning endless waves every few months). So only young kids got it, roughly at the rate at which kids were born, everyone else had already either died or recovered.
And, of course, back then when someone got it, he lied in bed and, again, either died or recovered, there was no expectation of high-intensity hospital care.
This is a very different situation — it is being introduced into the population, so we can expect a huge wave of simultaneous infections, but in the same time the population still expects to be cared for, and this is happening after hospitals systems are now in permanent collapse mode as a result of the damage that COVID has done to them.
We will see what happens, but it doesn’t look like anyone has fully war gamed the possible outcomes here (or if they have, the plan is to somehow keep a tight lid on the information flow).
It’s hard to see evidence of foresight in our leaders’ handling of much of anything recently, except the usual political theater I guess. But I find myself lying awake at night wondering about it. The thought that they might have a plan is horrifying.
I see that vaccine-strain polio may be on the loose in NY. I had forgotten about polio eradication as an example of official risk-taking without a realistic endgame. Maybe I’ll sleep a little easier.
Another important issue to remember is that the previous largest outbreak of monkeypox in the U.S. was caused by imported Ghana mice.
We do not know how many other animals besides rodents and primates can get it and transmit it. This could have the potential for ample animal reservoirs across the world.
Edward Jenner used cowpox pus to immunize against its Big Brother smallpox, as cowpox was milder (rarely fatal) and did not leave scars (as much). And it immunized against smallpox. We now read that smallpox vaccination immunizes against monkeypox, at least until the immunity wanes (which it would do, seeing as how smallpox has been eradicated so there is no exposure to challenge/reactivate the antibodies. Oh, those orthopoxviruses! But at least they are consistent.
Btw, cowpox is also known nowadays as catpox since it is now transmitted to humans mainly from cats who get it from rodents, which are the current reservoir of the virus. I guess there are good reasons we use lab rats, mice, guinea pigs, and hamsters. Source in NZ. So, would a cowpox/catpox test show positive for monkeypox? On further reading, it seems the rare cases of cowpox/catpox were identified by isolating and culturing the virus. So, not a routine or quick test. Maybe we should be asking veterinary colleges?
I got a smallpox vaccination about 55 years or more ago. Would a smallpox vaccination that long ago protect against monkeypox today?
I think there are a lot of older people who are wondering about that. Contrary to what the CDC says, and based on the conclusion that the smallpox vaccine protects against monkeypox, the answer appears to be YES. (see my reply to a comment above for a 2008 study).
So that young woman’s TikTok was not just comedy or hyperbole … grrrrreeeaaaat.
Unsurprising TBH … but alarming to the nth degree. America’s rancid leadership does. not. give. a. family-blog. about. us.