If you were to read the popular press, you’d come away with the impression that a shortage of primary care physicians was a looming issue, as opposed to an emerging crisis. As this post will explain soon, relying on IM Doc’s assessment, primary care doctors are increasingly being replaced by nurse practitioners, who simply don’t have the training or experience to perform the key job of a front-line doctor, that of diagnosis. Whether this shift to the inappropriate use of nurse practitioners is a bad adaptation to fewer doctors entering and staying in primary patient care or a MBA scheme to lower the costs of initial patient care, IM Doc also explains how nurse practitioners wind up overloading the system, increasing costs and degrading patient care.
A gander on search does clearly portray that the primary care physician shortage is acute. And even then, most of the coverage is in medical industry publications, as opposed to the mainstream media. From STAT in September:
According to a 2021 report by the National Academy of Sciences, Engineering, and Medicine, an increased supply of PCPs is associated with better population health and more equitable outcomes. With our country’s fraying healthcare system, it is essential to have a PCP who knows you, because it is almost impossible to access any type of coherent medical care without the coordination of a PCP.
The U.S. is running low on primary care physicians, with an estimated shortage of between 17,800 and 48,000 predicted by 2034. The dearth of doctors in this area has broad ramifications, ranging from more patients seeking care from specialty and emergency medicine to increased costs to the health care system and poorer public health outcomes.
Harvard Health in September 2022 provided anecdata, admittedly in a non-alarmist way, that it’s hard to find a primary care physician, and not just in rural America:
According to a 2021 report by the National Academy of Sciences, Engineering, and Medicine, an increased supply of PCPs is associated with better population health and more equitable outcomes…
The most common question I get asked as a doctor — by friends, acquaintances, relatives, families of patients, colleagues — is “Can you help me find a PCP?” I can’t. None of us can. Why is it so difficult to find a PCP nowadays?
While the COVID pandemic certainly pushed a large subset of already burned-out PCPs over the brink into semi- or full retirement, or into less stressful jobs, the current primary care crisis has been brewing for much longer. The US is expected to face a shortage of primary care physicians ranging from 21,000 to 55,000 by the year 2033.
Both patients and doctors are getting older. As patients age, they tend to need more care from their PCPs to address the proliferation of medical problems and medications that inevitably comes with aging. At the same time, the Association of American Medical Colleges reports more than 40% of active physicians in the United States will be 65 or older within the next decade..
Further, one-fifth of doctors say they will likely leave their current practice within the next two years, and one-third of doctors are intending to reduce their work hours within the next 12 months….
Primary care is getting hit harder than most specialties, due to having lower salaries, higher ratings of burnout, and a growing feeling that their job is generally impossible and thankless on all fronts.
The Harvard story acknowledged that medical systems are keen to replace primary care doctors with nurse practitioners (NPs) or physician’s assistants (PAs), and depicts that os OK for routine care but not anything complicated. As you’ll see below, IM Doc explains why that is false for everyone but the beancounters.
This tweet triggered IM Doc’s reaction:
As of today the entire Brigham & Women’s system in Boston is not accepting any new patients for primary care.
This is US healthcare.@BrighamWomens
— David Mayhew, MD, PhD (@DavidLMayhew) November 10, 2023
For those not in the US, Brigham & Women’s is a top medical training institution. From Wikipedia:
Brigham and Women’s Hospital (BWH) is the second largest teaching hospital of Harvard Medical School and the largest hospital in the Longwood Medical Area in Boston, Massachusetts. Along with Massachusetts General Hospital, it is one of the two founding members of Mass General Brigham, the largest healthcare provider in Massachusetts. Robert Higgins, MD, MSHA serves as the hospital’s current president.[1]
Brigham and Women’s Hospital conducts the second largest (behind MGH) hospital-based research program in the world, with an annual research budget of more than $630 million.[2] Pioneering achievements at BWH have included the world’s first successful heart valve operation and the world’s first solid organ transplant.
Lambert snidely observed:
On the bright side, Brigham’s is one of the main driver’s in HICPAC’s drive to reduce PPE in hospitals and nursing homes to levels even lower than they were pre-pandemic. So some slots for new patients should open up soon….
Now to IM Doc:
I called the three largest groups of internists in the nearby mega city for an appt for [immediate family member]. An appt with a NP in September- that is the best they could do. The university there is accepting no new patients in their primary care right now. My PCP at that university resigned about two months ago. I have been unable to find anyone.
This is no longer just Medicare patients.
The crisis will soon be upon us.
Remember all the hoo-hoo in the past 15 years or so about our wonderful system?
About how the wait times in those “socialist” systems like Canada were just killing people right and left?
How is that working out for us now?
I have not heard that clap trap in some time. Wonder why?
We are grateful I guess for the appt next Sep. All of us maintain our health and have little need for the health care system. But I guarantee you there are many others who are not so fortunate. And mind you – her Sep visit is with an NP.
I played out in my mid all kinds of routes for the demise starting about 15 years ago when anyone with a brain back then could see what was coming. Never in a million years did I see the NP thing coming. I love RNs – but their training is not even close to what we do as physicians. I would never dream of usurping an RN on the wards – their entire world view and work is vastly different. But the NP thing is really quite frightening. They get their RN – and then the vast majority of them nowadays get into NP school usually within the first year. Virtually zero actual independent clinical experience. The vast majority of them then end up in a 16 month or so correspondence school and are then unleashed upon the world as “providers”.
The tragedies I have had to deal with from this arrangement are just too numerous to discuss here. But there are very simple and tangible ways this too is absolutely cratering the system. Because they are so poorly clinically trained in diagnosis – they make many mistakes. But they also send almost every patient to all kinds of consults with specialists that would be unneeded with a properly trained PCP. Therefore, the specialists offices are now drowning in way more consults than they can handle for the most ridiculous of things.
What does that mean for everyone else? – Well, I now have two very sick patients that need urgent subspecialty attention – one rheum and one endo. The nearest rheum visit is in APRIL of next year – the nearest ENDO is is July. I do my best to take care of people as a general internist – and have been trained to do so from an intense program and career in the inner city where there were no specialists – but even I need help with very complicated patients. I am holding them together with bailing wire right now and calling weekly to beg for help. Never in my wildest dreams. And this is now chronic and across many subspecialties.
Furthermore, there is a myth out there that the NPs will be doing primary care. What a laugh. The ones that do get involved in primary care get burned out within a year just like the rest of us from the overwork and miserable pay. They often leave primary care – and then end up as an NP in GI or cardiology or Pulmonary or ortho or what have you. Why not? If I just had a 16 month correspondence zero clinic training – why would I not go for a more cush life and higher pay. It really is an intelligence test. What would happen if I, as a general internist, tried to pass myself off as a GI “provider”. I would probably end up in jail.
The outpatient general internists and family practice docs are the lynchpin of our entire health care system. The emotional and spiritual duress is now becoming unmanageable. They are leaving in droves. I found out this past week, my very first intern as an attending was a very successful general internist in Florida. She is 53 years old. She left her practice of 2000 patients and is now teaching school at a local private high school. She reports to us all – “Life is so much better – I can breathe.”
IM Doc then pointed to a related, recent story from The Hill: 1 in 4 US medical students consider quitting, most don’t plan to treat patients: report. Key sections:
The report “Clinician of the Future: Education Edition,” which was released by the health science and journal publisher Elsevier, surveyed 2,212 students from 91 countries between April and May of this year…
Among the surveyed medical students, 60 percent said they were concerned about their mental health, 69 percent said they were concerned about their income, 63 percent expressed concerns about experiencing burnout and 60 percent were worried about how clinician shortages would affect them.
Overall, 12 percent of medical students around the world said they were considering quitting their studies. Among U.S. students, this percentage more than doubled to 25 percent.
More than half of medical and nursing students — 58 percent — said they viewed their current studies as a stepping stone to careers in health care that don’t involve treating patients.
IM Doc’s comments:
Ten or more years ago, I would have considered this type of report an LSD trip. 58% have no intention of ever seeing patients? 25% of medical students want out before graduating? Really?
Five years or more ago, I would have said that I could see it but they have really overestimated the numbers.
Now, today, I think this is right in line.
I have a parade of students every month from all over the country, but mostly from the elite medical schools of the coasts.
I have been told by more than half of them over the past year that they have absolutely no intention of ever laying hands on a patient in any way after they are done with their residency. Patient care is now considered “dirty work” by many of the students in our elite schools. The action is now in Big Pharma, Big Hospital, and Big Insurance. They will have huge incomes and never have to bother themselves caring for a soul.
I can scarcely believe it, but it is absolutely true. Our taxpayers are paying a fortune for the education of these people and they have zero intention of ever seeing a patient their entire careers. And this in the jaws of the worst physician shortage in our history.
This is especially true in the more elite schools. Therefore, it is unsurprising that a place like Boston would be the epicenter of having no PCP options.
When I discuss this with these students, it is very unfortunate but very clear that many of them have the unspoke attitude – “I am elite, I have worked hard for this career, why would I want to waste my precious brain on any kind of interaction with the hoi-polloi? These people refused to be vaccinated and have questions — why am I going to waste my time?” That kind of thinking was unknown in my youth, and if it had been exhibited would have been beaten out of that person with great fury.
And you just thought the Hillary Clinton “deplorable” schtick was just an offhand remark……
The humiliation of my entire profession, and indeed the country, is at hand.
I have said the US is on track to suffer the sort of social disintegration that Russia suffered in the 1990s. It probably won’t be as cataclysmic or complete, but we do seem to be setting up the level of lifespan reduction Russia suffered, with the slow-motion collapse of many components of health care, and started from a base line of life expectancy reduction out of line with advanced economy peers and even much poorer societies:
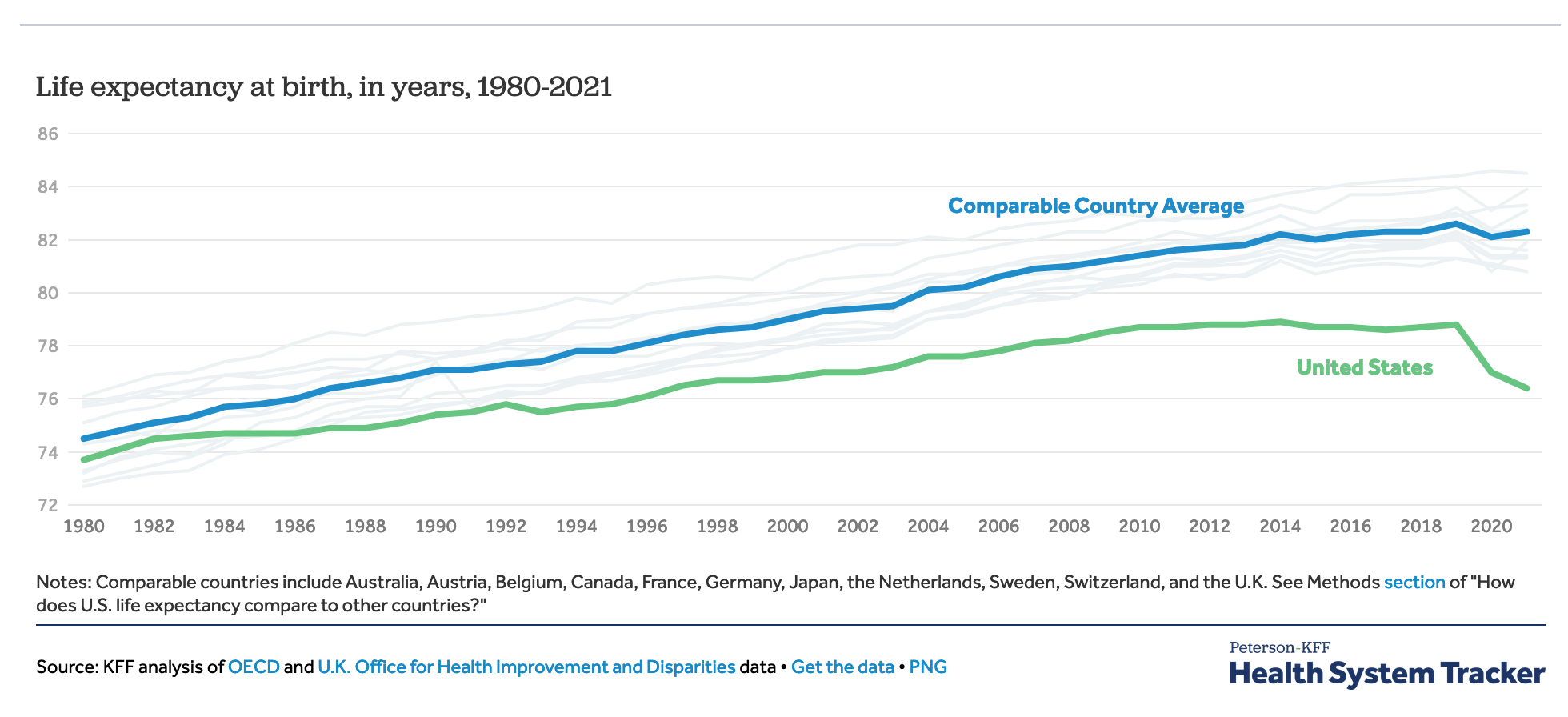
Thailand has higher life expectancy at birth than the US, despite a GDP per capita of $7,300 versus $64,200 for the US. Looting has even bigger costs than you might have thought.


I recall Peter Drucker predicting in passing to me that nurse practioners would increasingly be used on the front line to replace doctors when I interviewed him almost a quarter-century ago, when he was 92. But I’m sure Drucker didn’t have this in mind:-
‘More than half of medical and nursing students — 58 percent — said they viewed their current studies as a stepping stone to careers in health care that don’t involve treating patients.
‘I have been told by more than half of them over the past year that they have absolutely no intention of ever laying hands on a patient … after they are done with their residency … The action is now in Big Pharma, Big Hospital, and Big Insurance. They will have huge incomes and never have to bother themselves caring for a soul.’
These people may think that, but there are only so many of those jobs and it won’t work out that way for many of them. This will be more grist for intra-elite competition and late-stage imperial collapse a la Peter Turchin.
Well, it couldn’t happen to a nicer country than the US. I may visit to renew my green card next year; I may not.
Yves S: Looting has even bigger costs than you might have thought.
April 13, 2023 – U.S. life expectancy has declined to 76.4 years, the shortest it’s been in nearly two decades, according to December data from the CDC
https://www.hsph.harvard.edu/news/hsph-in-the-news/whats-behind-shocking-u-s-life-expectancy-decline-and-what-to-do-about-it/
Some comparisons —
The current average life expectancy for Monaco in 2023 is 87.0143 years of age. A 0.14% increase from 2022, when the average life expectancy was 86.8951 years, from birth to death.
https://database.earth/population/monaco/life-expectancy
The current life expectancy for U.K. in 2023 is 81.77 years, a 0.15% increase from 2022. The life expectancy for U.K. in 2022 was 81.65 years, a 0.15% increase from 2021. The life expectancy for U.K. in 2021 was 81.52 years, a 0.15% increase from 2020.
https://www.macrotrends.net/countries/GBR/united-kingdom/life-expectancy
The current life expectancy for Greece in 2023 is 82.80 years, a 0.2% increase from 2022. The life expectancy for Greece in 2022 was 82.64 years, a 0.2% increase from 2021.
https://www.macrotrends.net/countries/GRC/greece/life-expectancy
The current life expectancy for China in 2023 is 77.47 years, a 0.22% increase from 2022.
https://www.macrotrends.net/countries/CHN/china/life-expectancy
Drucker and his harmful ideas were all airbrushed out of the curriculum of Business Schools by Milton Friedman and Eugene Fama and other worthless eons ago. This happened after the Powell Memo I think? Wonder if any books were written on the impact of corporate cash on Academia. Would be an interesting read. Drucker introduced the concept of ‘Human Resource’ as in employees are assets IIRC.
Same situation in Canada – if you don’t already have a primary care physician, get on a waiting list. Not sure if the contributing factors are the same, suspect it is more demand-related rather than the weird elitism that IM DOc identifies, but it has a direct impact on my family – my PCP is 72 and if his wife has her way, he will be retiring soon.
Is this yet another example of the general crapification and corruption that afflicts us as a society?
I don’t understand the part about demand-related. If demand has increased, shouldn’t the powers that be work to get more PCPs in?
Ha, ha, ha … the Canadian government plan for the impacts of mass immigration (500,000 plus a year, that’s 1.25% plus of the population each year)! Employ more doctors and nurses, have the government build high quality housing as its done in Singapore, build new railways and subways to stop gridlock, facilitate the quick identification of immigrants academic and professional credentials, provide free and widely available English/French language classes for those not fully fluent …. Ha, ha, ha this is lackadaisical Canada mate and all that spending would need us to reinstate some of those higher taxes on the rich, eh!
This depends mainly on provincial funding and some provinces seem to hate putting government money into anything that has to do with public health. The Conservative Govts seem to be the worst but it applies to governments
of all stripes. Putting money into training is not all that flashy or vote-getting.
There seems to be some hint of expansion but we are looking at a long training process even after the money arrives.
The beacon of public health was Tommy Douglas who brought public healthcare to Saskatchewan 15 years before the rest of Canada. He also managed a balanced budget for his entire term without a single deficit. When my family moved to rural Ontario in 1974 we had the choice of 3 family doctor’s. Since the retirement of the one we chose non.
~ Our Urgent/Emergency centers here are overwhelmed with patients who do not have a PCP of any kind, including NP or PA. To get into Urgent Care at all, you have to have an appointment, and to make the appointment you have to have a portal and the ability to make that appointment online. If it is in fact ‘urgent’ but you’re odds of being seen exceeds 2 hours, you’re referred to Emergency. There’s a sign outside those doors explaining the difference between ‘urgent’ and ’emergency’, as though wagging a finger at the patient in crisis to pause for a moment and ask themselves, ‘Are these really the right services for you? Maybe you could be better served somewhere else?’ Like at Urgent Care that just passed the buck?
~ My NP refers me to specialists. ‘Referring’ seems to be her primary job. I can see the examine room while I wait and that it’s full of equipment and supplies, but it’s like they’re props on a movie set. Apart from using her stethoscope to check my heart and lungs, I’ve never seen those cabinet doors opened and the miracle of a ‘procedure’ performed for my benefit or anyone else’s… as in I glanced over on my way down the hall through an open door and observed that something of a medical nature had happened or was about to.
~ I’ve been having fun with surgical glue. Lately it’s been gluing back together my cracking heel, but also a finger that wasn’t healing (Husband, bless his heart, sharpened all my knives), and then yesterday my left thumb. I stood there watching the blood pool into my palm trying to decide if there was any chance that needed stitches and what my odds were of getting into Urgent Care in under two hours and if ‘no’, then could I just take care of this myself? What would be the best course of action? As I considered this, I realized we had amassed a lot of medical equipment and supplies over the last few years. We were becoming our own ‘Urgent Care’ department, for just two patients. (I see a future where we treat ourselves in clinics made up of lay people with some training, much like rural areas where you’re often far from help.) I let the blood flow since the shears I was using were grubby, then used compression till it stopped, cleaned it, glued, created a few butterfly bandages for tension and a bandaide.
Got through the night fine and this morning it looks pretty good.
If you don’t have, ahem, access to surgical glue, Gorilla Glue can work in a pinch. During the winter months, I use it to put cracked fingertips and thumb tips back together.
I don’t know why it didn’t occur to me sooner. I carry a pack of those single-use super glue tubes in our first aid kit. I whacked the back of my index finger once with a knife that cut it to the bone. Husband took me to Urgent Care back when you could just walk in and wait your turn. They hit it with some kind of antibiotic/anesthetizing shot (?) waited, then applied surgical glue and dressed it. Cleanest little scar I’d acquired in years and fairly painless healing. Much better than sutures!
The glue I ordered was veterinary. Goes on like ‘liquid bandage’ and works very well.
Another great idea! Thank you!
Super glue works, but it burns like all hell.
Good to know. John. I haven’t used super glue yet but think it might do in a pinch… meanwhile, now a big fan of surgical glue. Two days have passed and the end of my thumb isn’t pretty, but it is pain free and knitting back together nicely.
For future reference, ground black pepper stops bleeding. I have used it and it works. BTW, no stinging whatsoever.
https://www.peoplespharmacy.com/articles/pouring-ground-black-pepper-on-a-cut-stops-its-bleeding
As a sub specialist I can attest to the number of useless consultation requests I get from poorly trained HCP. They are our very own “barefoot doctors”!
I am in Boston and I found a PCP no problem and can get an appointment often the very next day. The PCP is in a hospital and has referred me to specialists at that hospital who have seen me in weeks rather than months.
The secret is it is in a community hospital not affiliated with a university.
I know this isn’t a systemic solution, just an observation.
Correlation is not cause. Certainly there are many instances wherein people die because of lack of access to primary care, but that does not make it the primary cause of lowered life expectancy stats.
The mix of possible causes is large, it includes poverty, stress, poor life style choices, bad medical advice dispensed both by “real” doctors and other providers, a lousy insurance system combined with ever-spiralling-upward costs of all aspects of care, etc. etc. In such a complex system of bad causes, there are available a plethora of studies that will assign to different factors the distinction of being the primary cause of shortened life expectancy. Such is the nature of chaos.
You forgot to put COVID on that list, and rural hospitals have been closing in many states.
“…an increased supply of PCPs is associated with better population health and more equitable outcomes.”
So, neo-liberal agenda is going according to plan I guess…
Beachwalker: Correlation is not cause. Certainly there are many instances wherein people die because of lack of access to primary care, but that does not make it the primary cause of lowered life expectancy stats. The mix of possible causes is large.
The U.S. has 4.23 percent of the world’s population yet 80 percent of the world’s opioid consumers, IIRC, with over a million drug overdose fatalities since 2000.*
So there might even be a significant argument to be made that in many instances it’s precisely the access to primary care Americans have — because it’s often bad primary care; e.g. fentanyl, Sacklers, etc. — that is the main factor in lowered US life expectancy stats..
(*Sorry, on the go w. just my phone and couldn’t find a link to back that figure up.)
I thought PCPs were used as gatekeepers by HMOs and similar, so they have to deal with a lot of requests for referrals by patients with chronic issues who know very well which specialist they need? That is not contributing to the shortage?
And why/how did it become standard to pay specialists vastly more than PCPs? Especially if their is a shortage? Has supply and demand been completely abolished?
Supply/demand only works when there’s 2 parties. Add a 3rd party — insurance companies — actually making the payments (who many times owns the very same providers they are making payments too) and you can see how supply/demand dynamics wont work
Perhaps someone can correct me if I’m wrong, but specialists generally earn more than PCPs do and I think it’s been that way for quite some time. I believe it’s common for lot of medical students to choose the more lucrative specialties.
True and dont forget skyrocketing student loan debt of graduating docs makes primary care a nonstarter financially for many.
What if the US were to train doctors at no cost to them, providing they stayed at least 5-7 years as primary care doctors? I would imagine there would be plenty of takers, especially if we had universal health care. Oh, I forgot, that’s socialism. And we really need that money to fund more slaughters around the globe.
As a subspecialist, I spend a lot of time training (referring, and the 3 days of formal training some get as an elective rotation) NP’s about my specialty. Many patients get an MRI before referral, instead of a diagnostic history and physical exam. Waiting for the scan (and the radiologists reading) before referral is routine. NP’s (at least in my community) often do not even look at the actual images and rely fully on the radiologist, accepting their interpretation. Understand that the radiologist has not seen the patient or know the history, beyond what is written on the script (like “pain”). Sometimes, NP’s call and read the MRI results to me, then ask about the problem, urgency, and how to treat the patient. When this happens, many are unable to answer basic questions about symptoms or MRI finding severity. These are the ones who care enough to call and ask questions. For many problems, delays mean worse outcomes.
NP’s face similar high-output/profit/insurer/employer pressures as most doctors. Many experienced NP’s develop substantial skills, but that takes time and attention, along with adequate feedback to learn from results/patient outcomes. Giant practices often mean no personal follow up, short or long term, beyond reading others interpretations on a chart. NP’s are not held to the same malpractice standards as physicians, reflecting training and practice differences.
“Many patients get an MRI before referral, instead of a diagnostic history and physical exam.”
I’m curious about the efficacy of MRIs. They seem to be becoming a regular thing. Certainly a large chunk of change goes to the medical cartel whenever they are used. Are they any good at uncovering medical issues? It would seem to be a must in lieu of a diagnostic history and physical exam. Are they any good at confirming known adverse physical conditions? Color me skeptical. I would appreciate it if you could deposit this bias into the large ash can of all my other biases.
MRI has been routine for decades and is one of humankinds last great diagnostic inventions. A miracle of engineering and clinical utility. Now our bright students fight over who will make the next tiktok
MRI is more sensitive and specific than CT in a majority of cases. It is slower and machines are very $$$. But there is no harmful ionizing radiation and for many organs and pathology there is no better option than MRI.
Now to the messy reality…Your doctor may order an incorrect MRI. If a tech makes me aware of an incorrect order i will fix it. I dont see all orders before they are done, its not possible. Of i read an MRI that was incorrectly ordered and needs additional imaging i make sure to include in report “at no additional charge to the patient” as i was trained.
Some docs are burned out/apathetic and let these incorrect orders through because to call and fight the ordering docs/np/pa several times a day takes energy and time and im reward for your efforts the hospital admin will call you obstructionist if you block too many. So they just approve all MRI orders anyway. Techs are not doctors and do the best they can to clarify glaringly obvious wrong orders. You can always ask the imaging center if the radiologist agrees with that particular MRI study as the best for your condition. It may delay your care but MRI is one of the best tools we have.
chuck roast: I’m curious about the efficacy of MRIs … Are they any good at uncovering medical issues? … Are they any good at confirming known adverse physical conditions?
What RPC says. Still, while he describes the realities of actual hospital use, MRI technology also has granular practical limitations.
So, for instance, if you’ve suffered a concussion and with it, maybe, memory loss, sensations of dizziness, ringing in your ears, and problems with your vision, MRI scans can establish whether you have subdural haematomas or haemorrhaging — bleeding on or in your brain.
MRIs will not capture interactions between the neurons and blood vessels in brain cells, which is generally what concussion affects. Nor, therefore, are they likely to detect post-concussion syndrome.
Thank you both.
MRI’s are good at seeing the physical structure. Accuracy is pretty good for most soft tissues, and not as good for bony tissue (as a CT). They do not visualize tiny structures well, without extra (costly) testing beyond the routine.
MRI’s do not see metabolic aspects, unless there physical change. They do not see motion-related, over-time related, or instability related things – only secondary physical changes. Studies can be repeated over time, or in different positions, to pick up more subtleties ($$) but the ordering physician generally has to evaluate the patient accurately and suspect the problem to know what to order.
For example, an MRI can show a pocket of fluid. It requires more understanding to figure out if that fluid is pus, blood or clear cystic kind of fluid. Ordering a study with and without contrast can help discriminate, but again the ordering physician has to know what they are looking for to order correctly.
In some cases, the group owns the scanner and profits from studies, and physicians may be paid more for ordering them. It’s no surprise this US medical system feature does not work well for patients or for physicians who take extra (uncompensated) time with patients to carefully diagnose and consider studies.
Another factor is “preauthorization” requirements, the mechanism used by insurance companies limit/approve which studies are covered under which circumstances. Some that should be approved right away are denied, while others are not. Insurers often use adult norms for children, one size fits all norms for adults (regardless of other health problems, age, sex), requirement to wait for other treatments to fail before proceeding, and so forth. It gets quite messy.
My experiences with nurse practitioners has been superior to that with physicians. NPs actually listen to what you say, are able to spend more time in-person, and waiting times to see them are a whole lot shorter than waiting for a primary care doc.
This certainly describes my situation. I had been seeing a real doctor and he was excellent. I now see a Physicians Assistant at the same office that is not very good. I don’t really want to see her again. I’ve searched for a real doctor as my PCP but have had little luck.
In my area many of the doctors are part of the University of Pittsburg Medical Center (UPMC), whose executives have salaries in the millions and are often not even doctors AFAICT.
In the town we’d been living for the last 10+ years a recent nurse-practitioner hire who was fresh out of school refused to refill a prescription that I had been taking for years, one that had always been routinely refilled. I was stunned and asked to be transferred to a new NP ASAP, which did happen. Now we’ve moved to a different county and I am able to see a real doc most of the time, thankfully.
Fun fact, UPMC has a big tech incubator.
(bold mine)
Gotta justify those big salaries somehow, I guess.
https://enterprises.upmc.com
I have a silver bullet solution to this problem. It was used to cure the great “Engineers shortage ” as was beoootifully explained by our Superiors such as Bill Gates and Larry Ellison and Steven Jobs (God bless his soul). America will fall behind in international competition if we do not pass H1-B visa legislation to import millions of Imdoan Engineers to fix the shortage. So it was said and so it was done. Do the same for Physicians. Import from India and other countries that have excellent Medical schools. Q.E.D ;–)
Local practice here, my G P is Lithuanian, 8 total docs, others are from Qatar, Vietnam, Greece and Philippines. My guy is great, I’m lucky to have him.
Last month I got a referral to physical therapy for a vertigo/ balance issue. They are not taking any new patients until next April…. I solved the issue myself with YouTube videos recommended by Dr Google.
My wife has had five GPs in eight years,
first one was great, she left to a weird private situation.
Next one was terrible and got fired.
Next guy was decent but quit medicine entirely
Fourth was the Qatari, he seemed ok but disengaged, lax follow-up after her “hostile and violent” ( per surgeon) ruptured appendix surgery. He moved to Texas(!) this summer.
She sees his replacement in a couple of weeks . Had been having some complaints but not sufficient to go to the ER…. Hope she checks out well
The practice just advertised hiring a married couple of internists so maybe there is a future…
As an RN for over forty years, and remaining in direct care, sadly I can nod yes to all of this. I have worked with very bright and capable NPs, but that was in the past, and have been shaking my head over the past few years about how little they know, how incapable of addressing simple situations. Forget about PAs. Likewise I see all too many aging friends with health concerns not being addressed, as they pour limited income into insurance plans which don’t deliver either.
I live in a rural community with a dearth of doctors. There is a community clinic staffed by NPs that are supervised by a physician via phone from a distant city.
I currently treat with an internist who is 70 miles away for chronic pain. I have been with her fror many years and it suits my needs.
When I inquired about seeing an NP in town for simple issues, I was told that I would have to give up my internist all together. Forever more. And I would have to go to a pain clinic for my chronic pain issues – also 70 miles away. I kid you not. Are they getting kickbacks on referrals or something???
Of course I determined it would be best to stick with my internist…a no brainer really. Luckily she agreed to treat me for simple issues via telemed should the need ever arise.
My internist is young enough that I hope I don’t have to worry about her retiring. I do worry she might move away though, especially since the practice was bought out by a hedge fund a couple of years ago and has changed quite a bit.
Paul Starr details the stranglehold of the American Medical Association clearly in “The Social Transformation of American Medicine”. Much of the dismal state of affairs can be laid at the feet of the Specialty Physicians lobby via the AMA. They wanted a Guild which will always have fewer Physicians always to keep pay high and they did this by many methods but mainly by making Medical school admission tough and Medical school curriculum highly demanding. IIRC it takes 10 years to train a Specialty Physician and 8 for a PCP? This is pretty ridiculous. In India one goes directly from High School into Medical School. There is none of this 4 year basic degree nonsense there. Result is we have plenty of well trained Physicians there. Also here in the US the other gauntlet is the number of needless Organic Chem classes that are mandated which makes Medical schools unpalatable for many. Canada seems a little easier I hear. Anyway, the AMA is getting a comeuppance from Wall Street. They grew their Golden Goose too big and fat and the temptation was just too great for the Money Changers who are now taking their slice of the.pie. Not surprising that Medical care went down the toilet. When you ignore PCP and the Specialty Physicians rule the roost then this is what you get. Our system is incontrovertible proof that for profit medicine will always fail especially if the for.profit angle is stressed so much over the social mandate that all Physicians implicitly sign up for when they enter the field.
Yes. And the tail end of the baby boom generation, who would have been their own solution to today’s shortages, were turned away from the profession in huge droves. Limited slots in medical schools, stringent competition, ‘gatekeeper’ courses to weed the crowd down. And funny thing, it turns out maybe calculus and organic chem courses aren’t the best preparation for being a good diagnostician. And funny thing, the AMA members so anxious to restrict their own numbers, are now burnout cases working for vicious corporate masters.
Starr’s book was required reading for a college course I was taking back in the early 90’s. If it’s the same book… what stuck in my mind all these years is what happened to midwives, as the AMA put all their considerable political weight behind booting them from delivering babies, by delegitimizing them for their lack of formal schooling and state licensing. I’m pretty certain it’s the purpose of such a long and expensive education.
“the number of needless Organic Chem classes”
Actually, no. Currently only two are required, while one that addresses fundamentals of structure and function may be sufficient. Organic chemistry is difficult, yes. And a useful pre-test of sorts. But if a physician cannot look at a molecule and immediately understand whether it is soluble in water or not, whether it is planar or “squiggly,” simple or complex, s/he is not so different from an architect without a fundamental understanding of structural engineering. As for calculus, that depends on which physics classes are taken. A BS degree may require a year of calculus, but calculus-based physics is not required for medical school. Physics is, however. Hard to understand the lung, the heart and cardiovascular system, and the musculoskeletal system without physics.
Having said that, yes, Medical Education is as target-rich as Big Pharma, Big Biomedicine, and Big Insurance.
To your point, I’ve had scientists say the reverse, too many doctors think they know way more about biochemistry than they do and it causes trouble.
Late to the party again.
Great point. Of this I have no doubt! This stuff gets complicated and a little knowledge can be a dangerous thing. When I was majoring in Biochemistry and later as a graduate student in Biochemistry & Molecular Biology, the old timers were unnaturally proud they didn’t care one way or another if premed students learned something that would be useful to them as medical students and later as physicians. Now they teach Human Biochemistry at a high level for those aspiring doctors who have guts to risk a “B-” on their transcript. I had absolutely no real understanding of diabetes until I taught medical students. This has changed, somewhat. But I have a medical school colleague who still thinks the amino acid on the other side of the oxygen binding site in hemoglobin is something a medical student should know. Actually there are only a few thousand biochemists and structural biologists who need to know that. The medical student only needs to understand how hemoglobin works as an oxygen carrier through both positive and negative cooperativity. Biochemistry alert: When the first (actually second most of the time) oxygen molecule binds in the lungs, the third and fourth are more likely to bind. When the first pops off in peripheral tissues where oxygen concentration is lower, the next two are more likely to do the same. If hemoglobin did not work this way we would not be the large multicellular organisms we are.
One biochemistry course is required by many medical schools, which is a change from years past. Some (ours) allow an introductory biochemistry course to take the place of the second organic chemistry course. This is a much more useful sequence for physicians-to-be. The second semester of organic chemistry is largely synthetic organic chemistry. I could not move the electrons around in the Grignard Reaction after so many years if my life depended on it, without reference to my organic chemistry textbook by the professor who taught my molecular mechanics class as a graduate student.
But knowledge of the fundamentals of organic chemistry is an absolute prerequisite for biochemistry. The point of basic biochemistry (and cell biology) is for medical students to develop some knowledge of metabolism and nutrition, protein structure and function, enzyme regulation, protein/RNA/DNA synthesis, signal transduction, basic immunology, and hormone action. These are the foundations of physiology (gastrointestinal system, cardiology, renal physiology, endocrinology) and pharmacology (diabetes, cancer chemotherapy and the cell cycle, arthritis, autoimmune disease). A medical student with some knowledge of genetics and microbiology is also ahead of the game. But the “top” student in a given class often majored in history or anthropology…as someone who spent a lot of time in both departments, this does not surprise me.
Either your physician knows these things in sufficient detail to take with a mountain of salt what Big Pharma sells or s/he does not. This is why your doctor needs a good working knowledge of the basic sciences of medicine. Then s/he can use her healing hands as they should be used but are so often not.
In the words of Sir William Osler (Oh-slur), a founder of the Johns Hopkins Hospital/School of Medicine and modern medical education, from a time when a physician and a surgeon could be separate things:
“You cannot become a competent surgeon without a full knowledge of human anatomy and physiology, and the physician without physiology and biochemistry flounders along in aimless fashion, never able to gain any accurate conception of disease (or health), practicing a sort of popgun pharmacy, hitting the malady and again the patient…usually not knowing which.”
Popgun Pharmacy and Big Pharma, has a definite ring to it.
OK, I’ll return to my corner now.
This has been the perfect NC thread!
I respectfully disagree with your assessment regarding keeping people out of medicine and gatekeeping course. Being a physician is a very hard job and requires a very strong grasping in science in order to do well in Medical School. People who want to become doctors have to learn how to study difficult concepts and that includes learning Calculus and Organic Chemistry I believe that the solution is to improve our k-12 education system so perspective college students have the tools to do well in college stem courses
Last time I went in for a routine checkup I was shunted off to a nurse practitioner instead of my actual doctor, and was wondering why. Now I know – so nice to be trendy.
A few years back I went to the emergency room after a bike accident and never saw a doctor although my impression was that the NPs are always supposed to have a doctor nearby for consultation. Perhaps things have gotten worse since then but in America we have always made medicine about money and that aspect of the problem has certainly gotten worse. And lest physicians want to put all the blame on Big Finance one might point out that their AMA was a major player in opposing socialized medicine. They kept government out of medicine and thereby opened the door for that competing power center to step in and take over.
Now there’s so much money sloshing around in the system that it has become the Medical Industrial Complex and if you visit towns like mine or the one next door you’d be under the impression that the major employers were the hospitals. Capitalism leverages the irrational to create rational outcomes until it doesn’t.
When I was in college I majored in Chemistry. needless to say, many of my classes were full of pre-med students. In conversations with these students I learned that the primary motivation for becoming a physician was the high incomes and social status that comes with the title “Dr. So and So”. Nobody should go into any health care profession with the expectation of becoming “filthy rich”. These students should instead work in venture capital and private equity. The AMA should not control medical school curricula and standards for admission. The conflicts are too wide and deep. It’s akin to the local Police Officer’s Association running the police academy. Bad outcomes in both instances.
Funny you should say that. My mom had a clerical job in a local college chemistry dept. and would ask the organic chemistry students why they wanted to be doctors. They all said the same thing.
But we should distinguish between the run of the mill aspirants and the really good doctors that we run of the mill patients might never see.
I think they all want to be dermatologists; I heard that was a particularly competitive specialty. The ones I’ve seen throughout the years were either dismissive, a**holes, or both. A couple at least seemed genuinely interested in my case, but that was the minority.
My late MD father was a career researcher on the faculty of a major US medical school. From time to time, he served on the school’s admissions committee, and he reached the same conclusion. He did his best to weed out the most detectably venal and narcissistic of the applicants, but he was in the minority and it was a losing battle.
As a radiologist we are literally drowning with the massive incease in volume of unindicated advanced imaging ordered by NP/PAs taking over ED and hospitalist physician roles. This imaging is expensive , time consuming to interpret even if negative, and delays reporting of indicated studies.
Hospitals see decreased labor costs from PA/NP midlevels and the increased # of ct/mri results in increased technical fees. Meanwhile physician professional fees are constantly being cut to the point that the excess volume now is unwelcome. We are working at unsustainable levels. The CMO of a major insurer admitted to me that this scenario isnt going to end well but they of course have to follow congress/cms lead and act innocent.
What was once an intellectually stimulating rewarding field has been reduced to a highly paid amazon factory worker type gig where speed trumps all. 50% of my partners looking to cut time. Problem is we cant hire anyone, and the younger grads we do find dont have the appetite for working a grinding job for 30years. I dont blame them. The labor shortage is unbelievable and they have the power. Thus the door is opening for even more midlevel creep. The future takeover of NPs and PAs is inevitable.
Im trying to go part time. I cant because community needs me and my subspecialty. There is noone else. I keep pushing my date back by 6mos despite declining personal health not because i need $ but because literally there will be a gap in care if i leave. Multiply my scenario by tens of thousands. The system is way more precarious than anyone admits.
Agree that physician training is overrestricted, focused on arcane knowledge and too expensive (not for government here in U.S., but to the students they foist the burden on).
Give me a colleague with real empathy and a desire to help people with even just a little knowledge over brilliant uncaring or self serving people.
On moving to a ranching, mining, and farming state a few years ago (howdy, Mildred!), I was referred to a PCP by my landlord, a RN. A few months later, he quit – he had mentioned a recently increased workload to me, but I don’t really know why. Since then, I’ve been cared for by two NPs.
The first, 90 minutes from any city over 30,000, had been doing it ten years after about fifteen as a ward RN. He kept a tight reign on testing, hada rep as an excellent diagnostician, and indeed started me down a path to dropping a med with powerful side effects that he suspected I no longer needed, and put me on a more common med for a diff issue.
I had to move. Now thirty mins outside the regional medical hub. Specialist appointments six to fourteen months out. My current NP was in her third year as RN when the monopoly hospital/HMO chain in town terminated her for declining the Moderna. She picked up the NP cert and now serves our very low pop area. Very open to give and take discussion, even patient research, certainly inclined to order tests but flexible when suggested we hold off on a particular one. Finished protocol to stop the heavy med I no longer needed.
So for an older, experienced via via family members at manipulating the system, not too dumb guy- NPs have been FAR from a disaster, superior to the (un)”coordinated care” I got from Kaiser. YMMV, and the lack of provisioning of medical care IS a crisis, but FWIW.
Hmmm, might be a keeper. My NP also took me off a med that clearly wasn’t doing anything but giving me a gut ache. ‘Flexibility’ may be something NP’s bring to the table. I’ve been concerned for a while with what I see as physician’s ‘dogma’.
I agree with the general observations of Paul Art. I enjoy IM Doc’s observations on the condition of public health.
I have spent a lot of time in EDs and hospitals over my life. There was a time when the professional in the wards were either doctors or nurses. There was a deep pool of knowledge. Today, I notice the healthcare is fragmented into every tiny function. There is person who puts the armband on, the one who takes BP, someone who gives pills, etc. and then a nurse on occasion and perhaps and an appearance by a doctor. There is not a wealth of knowledge around, but there are an incredible amount of billable events.
Doctors once were involved with there patients in the hospital. Once attending physicians followed patients. Now it is ‘hospitalists’. Another downgrade in knowledge.
I remember in the 1990’s NP were going to replace GPs. Not Internal Medicine, but GPs. The training was extensive and the NP’s, including my wife were very qualified. But over the last 20 years education has changed – PT, OT, NP, all are awarded doctorates after changes in the curriculum. More credentials, no increase in knowledge. And a lack of clinical experience. More billable opportunities.
We have to remember, doctors did everything possible to ensure NPs were subservient to Drs. PAs were invented by doctors because by definition they are subservient and PAs were hired before NPs to “keep them in their place.” BTW, some states allow NPs to operate independently – they are quite success when they are independent.
Doctors always need to be on the pedestal. Doctors, via the AMA, fought single payer medical care in the 1940’s until the present day. They did not want the government telling them what to do. They limited doctors to maintain high wages. They push to import nurses but block the arrival of doctors and dentists.
Unfortunately for doctors, they never realized that in order to stay on the pedestal they were empowering insurance companies and big money. Senator Rick Scott eviscerated hospitals and doctors in the 1980-90s. The doctors are now just another stop on the factory floor.
So true re AMA. But i dont thnk the results of their work are unintended. Most docs i work with hate the AMA. Never met a fan or advocate. Most of their decisions are so obviously anti-doctor in the long run. Makes me wonder who they really represent
I had a senior colleague when I was a postdoc who was an MD who became an expert in enzymes of bacterial DNA replication. On the day I attended his lecture on DNA replication, his class immediately followed an “informational” presentation to first-year students from the AMA. He began by saying to his captive and very attentive audience: “That was all well and good, but just remember that they need you a lot more than you need them.”
I was the academic department head for all of the nurse practitioner programs in the state before I moved home to Canada when I realized the U.S. was going to crash. That was 20 years ago. I am now retired from teaching nursing. In that rural state, we created and ran programs for family NPs, paediatric NPs, psychiatric NPs, geriatric NPs, and clinical nurse specialists. The programs were all 2-year masters degree programs, heavy on clinical practice and internship. When we created these programs, doctors were extremely reluctant to have an NP for their internship in their practice. I had to beg them to give it a try. They preferred PAs, who were poorly trained and cannot practice without direct physician supervision. Then, whenever I was successful at placing an NP in a group practice for their internship, every one of them was offered a job. “You mean you can do all of our nursing home visits? You mean you can see all of the babies with ear infections? You mean you can do all the menopause counselling? You can manage all of our diabetic patients? You’re hired.” Everything changed.
Physician groups would advertise for new hires and the candidates would come from other states and ask, “OK, so how many NPs do you have in this practice?” When the answer was “none” the candidate would walk away. Then a representative from the practice would call me and beg for applicants from our next graduating class.
We NEVER accepted applicants to the NP programs who had less than 2 years experience in med-surg nursing and the specialty they intended to pursue. Almost all of the applicants had more than 5 years experience. Our programs were accredited by the national body. I was a member of the national accreditation body who travelled to other states to accredit their NP programs. All of them were at least 2 year masters degree programs.
Where the hell are these “correspondence” courses? Who accredits them? How did this happen? Are hospitals running their own ersatz NP programs like they used to do for RNs way back in the day? Why are the state and national nursing associations not screaming bloody murder over this?
In Canada I cannot get a family doctor or a family nurse practitioner. There are not enough. I am paying through the nose for a naturopath who can write the prescriptions I need. I say it, she writes it. I have two uncommon auto-immune conditions and she says, “You’re the expert, just tell me what you want.” If I were indigenous I would be dead by now.
I think we’re about ten years behind you.
Wanted to share one more very personal story regarding the very long reach of the AMA. I moved from India to the USA for an M.S in Computer Technology in 1990. In the queue for my visa interview at the US Consulate there was a Doctor in front of me hoping to get a visa to travel to the USA. We got chatting and he told me that after his initial Medical training in India he had trained in Germany as an Andrologist. After returning to India he established a thriving practice in Hyderabad and he had tried unsuccessfully almost 4 times to get a visa to come to the US on a shopping trip for his clinic but was refused every time. He showed me press clippings about his pioneering practice in India which he was going to show as proof to the US Immigration Officer of his resolve not to stay back in the US. He went ahead of me and when he came out of the interview booth he gave me a thumbs down signaling he had failed yet again. The AMA uses its political clout to make sure that if you are a Doctor outside the US then you don’t get a visa very easily at the US Consulate to enter the US. This is in keeping with their efforts to minimize immigration of foreign Physicians that might unbalance the low supply of Doctors here in the US. They don’t want the same thing that happened to Engineers (H1-B visas etc) to happen to them. Electrical Engineers, Computer Engineers and Software Engineers saw their salaries dwindle rapidly in the 1990s when the H1-B visa took off. I don’t know about the situation now but in the 1990s if you mentioned anywhere in your visa application that you were a Physician then you were guaranteed to be rejected. After I came to the US, the next Spring semester I bumped into another fellow Indian in the Science department – he did his Medical degree after a 3 year B.S in India (this is not uncommon) and using that he applied for an M.S in the US completely hiding his Medical degree. He got his visa, came here, wrote his ECFMG (Educational Commission for Foreign Medical Graduates) exam, got a residency, tore off his whiskers revealing himself to be a Physician, quit school and is living the American dream. The other channel for Doctors from India to move here is via an opportunistic marriage. They marry someone here already, come here and then take the ECFMG and get a job. Many Hospitals process H1-B visas for candidates like this. I have two close family members who followed this path. The point though is – while we import Engineers en masse from India on H1-B visas, the same is not allowed (with some exceptions I think) for Physicians. That demonstrates the political power of the AME. They dictate immigration policy when it comes to Physicians. Once you are here though, the system takes you in if you pass the ECFMG exams which basically certifies that you are worthy of serving in the American medical system. The AMA has a choke hold on the supply of Physicians in this country. They make sure that Supply is ALWAYS way lesser than demand.
Great comment. Economist Dean Baker used to talk about how our policy was free trade regardless of consequences to working people combined with strict protectionism for professionals like doctors. In other words the theme throughout our US society and not just foreign policy is “it’s ok when we [the elites] do it.”
Of course not all physicians are even members of the AMA much less support its positions., Bravo for them.
I’ve spoken to many people who have been treated by doctors from India and all of them had nothing but praise for them.
None of these problems will be solved unless the profit motive is removed from health care. (as well as dental care). The profit motive won’t be removed unless and until capitalism is greatly reformed or scrapped entirely. Housing, education, and health care (including dental care) should all be public goods, not commodities to be bought and sold in the “marketplace”. It’s not a coincidence that crises exists in all three. It’s also no coincidence that huge profits are enjoyed by the connected players in all three.
AI is going to eliminate diagnostic work in the near future. What’s left is hands on care: taking blood and running tests to feed into the diagnostic AI, performing procedures guided by AI to treat the problems. Definitely no need for calculus and organic chemistry for taking blood out other procedural work. This will be true not just for medicine but also other diagnostic intensive fields like auto repair.
Diagnosing faulty AI systems, on the other hand, will remain the province of humans.
Good point but I wonder how much control the AMA has over medical data which they would need in tons for training the AI systems.
If AMA interferes, that’s another industry we turn over to China.
That will work great (from the corporate perspective), for those of us on Medicare, who are supposed to die early for fiscal reasons anyway. Our annual “wellness check” consists of having the doctor ask you about a questionnaire you have already filled out and not even examine your body. But aren’t most younger people’s doctors supposed to actually look at them and see if there are any obvious physical signs that something is wrong? I don’t see an AI replacing that, no matter how fancy they try to make it.
I’m old myself v but I come from a computer background so I understand AI (plus math background so I understand exponential growth). Impossible for most old people to appreciate how fast AI can improve. To answer your question, the AI system looks at you.
So this is going to impact us soon, I think. When we retired 2 years ago, we transitioned to Obamacare insurance. We were able to keep the PCP we had been with for 20 years by searching for a plan where he was included. This was an HMO plan so it was affordable, but had a deductible double what I was used to, but we are low users of the medical system currently so it was fine.
We were notified that the contract his group (part of Providence) had with our insurance HMO will not be renewed. To keep him as our doctor we would need to move to a PPO plan which isn’t affordable for us and without his group, the local HMO network is tiny.
So we are changing to Kaiser which is more expensive than our old plan, but much less than the PPO. I do understand the Kaiser system, but the key to using it is getting a decent PCP. It will be interesting to see how that works out.
I have Blue Shield of California health insurance and for the past 12 years I have had the same PCP operating out of Sharp rees-stealy in San Diego. Last year he quit and joined the circus or something and I was assigned a new PCP. At my first visit with him a few months ago he ended the exam by telling me that his PA would be taking over from there on out. When I asked why he said something like he gives his good patients to her and exited the room fairly quickly. Apparently he didn’t want to answer any more questions. Thanks for the post as I was wondering if I was being singled out by some nameless faceless entity who was out to get me.
The best thing for this country – and probably the world – would be for the value of its money to turn to crap. Maybe then ‘health care professionals’ could go back to practicing medicine – or find a less detrimental way to loot the public. Same thing for turning the world’s remaining natural resources into more US government debt, AKA money, ‘the dollar’.
I was wondering why the USA is reluctant to have “boots on the ground” military confrontations? Could one of the reasons be a lack of medical doctors (I know the government can “draft” doctors if needed)? Is anyone aware of the field doctor conditions now in the military?
This article and letters are so interesting. I can’t tell you the number of conversations I’ve had with people–unsolicited–over the last year where they are simply unable to find PCPs or unable to get appointments for months on out. Even an uncle who lives in New York who has enormous wealth and sophistication finds himself unable to navigate the (non)system of getting a new PCP. All the while Covid, amongst other things, continues to assure that people are plenty sick. So this conversation is happening everywhere, with great urgency and concern.
And yet, and yet, and yet….it’s under the surface. You will search with despair to find any affirmation or validation amidst our major media about this phenomenon, of something that the public is vividly experiencing as the evaporation of a system as essential to living as air. It’s just a non-issue.
But the thing that really inflames me is the clear sense that it’s yet another disaster that is unacknowledged–in this moment–precisely because it reflects terribly on the Biden administration. In the same way that any critical coverage of the adminstration’s derelict Covid policies simply cannot be spoken–as Covid continues to run wild through a population that is unwarned and unprotected. Let’s imagine for a moment what grisly pictures the MSM would paint for us were Trump still President.
It’s all terrifying. Nothing of consequence can lifted to public media discourse because it might contribute to the Democrats losing in 2024. So liberals are more and more petulant as they know less and less, but clamor with greater stridency on the virtues of a criminally negligent adminstration.
Many years ago I read Dawkin’s Selfish gene and there were some things that stuck with me. He and an associate computer specialist have conducted simulations with various populations (cooperative/selfish) and they established that climatic, stable states can be reached with majority cooperative populations as well as with selfish populations.
The future doesn’t look pretty at all. Reminds me of the artificial hell described in “The Surface Detail’ by the late Iain M. Banks, hell developed to scare and threaten a planet’s population to stay under the control of an oligarchy.
When we moved last year we had to find a new PCP. We chose a local clinic affiliated with a big state-wide hospital and some specialty hospitals. It was a shocker. We got assigned to a NP who was a master at deflecting your questions. Anything she couldn’t answer caused her to talk really fast about other things and then bring the consultation back to stuff she could handle, which wasn’t much. I was suspicious but I let it pass. Then our BXBS insurance refused to pay her bill because she was not qualified, they said. They could not find her credentials. When she couldn’t come up with them she got fired. She’d apparently been passing as a qualified NP for a year or so. She left, she said, because she had decided to run her own weight loss clinic. Fat chance. Fortunately she was professional enough to do no harm but it was a depressing eye opener about the entire system. We now have a qualified NP PCP who is very good. So far so good. She actually encourages me to “google it.”
Joe Well is right (above), If you want good medical care, go to a community hospital, not a hospital associated with a medical school. The reason is, the med school hospital’s prime goal is teaching students, not providing prompt, effective, humane care for the sick. If the intern screws up, it’s a “teachable moment”, not a disaster. (The exceptions are rare medical conditions, or major trauma.) Also, if a lot of med students want to quit, it’s partly because some med school attending are sociopaths. As for the concept of “elite medical schools”: phooey, their recruitment policies admit pampered princelings. “it’s not enough that I should succeed, others must fail!”, the Harvard ethic. The medical establishment fought off socialized medicine like a cornered weasels, only to roll right over for Wall Street. Thank you for this good thread.
My spouse is a doctor and based on conversations I’ll just chime in with something minor that I don’t see elsewhere here… Doctors need to be able to detect possible drug interactions for any drug they prescribe. Patients, especially older ones, often take boatloads of other drugs, and often have multiple underlying health conditions that further complicate things. So part of the skill of the physician is being able to foresee how the new drugs that might help them will interact with the drugs they’re already taking–and these interactions can be very, very severe if someone doesn’t know what they’re doing. PAs/NPs, from what I understand, often have a very simplistic approach to prescribing drugs, without a deep knowledge of possible interactions.
Fwiw, the doctors that I know all complain about admin and paperwork. My good friend is a GP and went over to a ‘concierge’ practice, where he has a fixed number of patients who pay a fixed price per year but can call him anytime for input… it has not worked out as well as he’d hoped.
When I was in Boston, Cambridge Health Alliance (CHA) was the provider I went to; During my 4 years there, I had 3 different PCPs, they kept rotating them through. The two I met were young, probably recently out of medical school. The third I don’t know, I was getting emails about getting the initial COVID shots, and I let her know that I’d moved out of state by then.
Societal collapse is difficult to fathom. I guess you just have to live it.
My PCP back in Orlando was great, but he was old enough to be at retirement age and probably did retire by now. Out here, when I called a year ago, my PCP couldn’t see me for an annual physical for like 4 months. I haven’t been or tried again since then, that was 12 months ago.
There are now two of those off-insurance general practitioner clinics in town that promise real appointments and the like. At $150/month, all you can eat, I’m reaching the conclusion that it’s the right decision.
My wife has a major autoimmune disease and has most of her life. It’s a wacky one with symptoms of most of the others. I’ve got deep experience with Mayo and the University of Michigan. Her best and most successful care was a time where the rheumatologist at UM was the platonic idea of a doctor and he led her care like an internist/GP. He was backed up by the doctor who left running an ER in a major Florida city to be nearer his kids and be the doctor at a university health center. The latter had the time to dedicate to patients and the former somehow made the time.
I still feel dirty and bougie about even contemplating the whole Private medicine thing. But these days between getting an appointment and the cost of a visit, the $150/month doesn’t seem so bad. We blow through her out of pocket maximum every year anyhow.
New solutions on the horizon. Will not “fix the system” but should improve the environment… https://www.tandfonline.com/doi/full/10.1080/0142159X.2023.2271153
Thank you for the great post.
I have been a ‘patient’ of an ever-larger doctor group in New Jersey for about 20 years now. When I started with them they were a partnership with doctors who would take time to talk. Several acquisitions later, it is now owned by a major pharmacy/insurance conglomerate, with long waits and rushed visits. I engage with them as little as possible but when I had covid, which triggered shingles, I asked them for help, and after waiting several hours in my car on a freezing morning, a physician at urgent care gave me the bum’s rush, as callously as any insurance apparatchik. I’m in my 60s, and I am not a fragile flower, but I remember thinking what a travesty of attitude and behavior it was for this young doctor to treat someone that way when they are suffering. (I ended up going to a Holy Cross hospital in Northern Jersey, where I received a monoclonal antibody infusion, was better within hours, and perhaps as importantly was treated with dignity. (Echoing in a small way one of the patterns that aided the rise of Christianity.)
More recently, I had lyme disease, and after a round of antibiotics, I still had significant joint pain. So the nurse practitioner ordered up a blood test. She and whatever chatbot they use concluded that there was the continued presence of lyme, so I made an appointment with infectious disease and rheumatology specialists, but the next day the infectious disease specialist’s assistant called to say the test was misinterpreted and the appointment cancelled. At the time I was pissed, thinking that even were I complete hypochondriac they could still see me and talk to me. Not long after it was clear that I did not in fact have Lyme any more, and I concluded the specialist was right. It is interesting now reading IMDoc’s account of so many mistaken referrals by NPs.
Pretty much the entire model, with their emphasis on vaccines and statins, stinks to me. I haven’t met any doctors with intuition. I try to have as little as possible to do with any of them. But what to do when something big comes along…
Thank IM Doc.