Further down, we have hoisted a long comment from Lambert eviscerating the new CDC guidance for Covid, treating it as just another respiratory virus, which as he points out, will also wind up being applied to measles, which like Covid can also inflict permanent damage. Lambert insinuates that this policy train wreck is intended to shield hospitals and doctors’ offices from liability and from spending money to upgrade ventilation.
Since we still have Covid minimizers who show up with their tired tropes, we thought we would also hoist the latest report from IM Doc, who has kept meticulous records about his patients from early in his career. He is practicing in an area with high average incomes (and a big fat tail of extremely wealthy) and an unusually healthy population, since it attracts sports and fitness buffs. It is also a very blue community, so vax levels are high.
Please be sure to read Lambert’s thorough CDC shellacking too. One has to wonder how people who has some sort of medical and/or science education can devise such a travesty. Even though “Great Reset”/cull the population theories do have the advantage of being tidy, it’s not as if the public health elite is dispensing this destructive advice to the masses while observing strict precautions themselves. They appear to be happily subjecting themselves to getting Covid and with it, all the long term health costs.
The result of this will be that introverts and the constitutionally contrary will in not that long a time have a longevity and relative IQ advantage. But people like that usually hate meetings. Will they be willing to step up and run things?
First from IM Doc:
I now have my numbers for the month of FEB.
This is now obviously completely unique in the past 4 years. By now, in each year, we would have been slowing down to almost zero as March approaches. That is not happening at all. We seem to have bottomed out at a baseline of 20-30 cases daily. It is not budging down at all.
And again – although not nearly sick enough to be in the hospital – we seem to be in a pattern where people are more and more sick at home.
Another interesting pattern is developing – the patients who never seem to get better – and are having positive COVID tests for weeks. I now have 4 of these people – the longest one has been sick and coughing for 6 weeks now. All 4 are basically healthy – not really all that chronically ill – and all 4 have been vaccinated between 5-9 times.
The breakdown for the month of February –
This week brought the CDC recommending the 9th dose – and like clockwork – I had an acute DVT on FRI Mar 1 – that had been vaxxed with their 9th shot on Wed. We will see what the next week brings.
298 total calls and cases – of these 298 – only 2 were truly unvaccinated [the first since last autumn] – the two I told you about around Valentine’s Day. All others were vaccinated as follows –
J&J – 0 cases
Unvaccinated – 2 cases
2 vaccines – 14 cases
3 vaccines 24 cases
4 vaccines 76 cases
5 vaccines 32 cases
6 vaccines – 101 cases
7 or more vaccines – 49 cases
It must also be noted that of these 298 cases – 227 were on their 3rd course of COVID or more.
The EMR has registered that 125 of these people are “unvaccinated” – and that is apparently what the tracking number is reported as – our last community report was 39% unvaccinated – and as you can see above – that is just not the case. I have looked over many of these – how this mistake is being made in the algorithm in the EMR is not remotely clear for the majority of these patients. And again – if medical studies are not clearly discussing that the charts are being abstracted at this time – they are worthless with regard to vaccination status of these patients. I have now talked to too many people in multiple places to realize the problem here.
FEB brought in 12 patients with Long COVID. Again – I am not including the pulmonary issues from post intubation – but there were 2 of those.
4 were mainly having headaches, severe vertigo, tinnitus, or actual chronic hearing loss.
9 of the patients have some form of new severe depression or brain fog.
1 has profound hives/urticaria that will not go away no matter what is done. This is becoming an interesting pattern.
11 of the 12 report complete and total change from previous functional capacity – decreased exercise capacity etc. I have now put three of these people on the treadmill – they have clear lungs on Xray – and their hearts seem to be stable during stress – but what is immediately apparent is a sudden dive of pulse ox on usually stage 3-4 and above. Their baseline PFTs are normal – I have no idea what is going on — and working with pulm and cardiologists in multiple centers.
All 12 of these people were vaccinated and boosted – at least 6 times – there are no unvaccinated – although the system reports that 4 of them are unvaccinated.
8 of them have had COVID at least 4 times – 2 have had COVID three times and two twice. There continues to be 2 different patterns – either being vaxxed before ever having had COVID that we know of – or having the Wuhan or alpha strain and then being vaxxed.
I am struggling. I am doing my very best to help these people – we are trying all kinds of things. Again – metformin and fluvoxamine seem to help more than anything else. Baseline pristine healthy status also. We have two of them in a cardiac rehab program – and unlike true cardiopulmonary patients they seem to be getting minimal benefits.
As I have stated before – our federal officials and universities barely deign to acknowledge this problem – there are no diagnostic criteria – and there are certainly is no treatment discussion. We are all alone out here trying to help. What a complete and total joke this all has become. This did not even happen in the worst of the AIDS years.
And we go from IM Doc in despair over the lack of any official interest, let alone guidance, for dealing with rising levels of sickness and disability, to Lambert’s dissecting of CDC democide dressed up as its latest “guidance”. Hoisted from comments:
Hygiene and Respiratory Viruses Prevention CDC. This is the new guidance.
First, note the scope:
This guidance provides practical recommendations and information to help people lower risk from a range of common respiratory viral illnesses, including COVID-19, flu, and RSV.
Measles is an airborne virus. So even though all this guidance doesn’t apply to measles, you know that’s how people will interpret it. Entertainingly, measles destroys immune memory from previous infections, so another scientific communication blunder from CDC will make the flu, RSV, and Covid all worse. (The Flu and RSV are also airborne, although other forms of transmission may occur.)
Hygiene and Respiratory Viruses Prevention
The key move here is to separate clean air from hygiene (at the very least, an institutional imperative for both CDC and hospitals, who are still fighting #CovidIsAirborne tooth and nail, preserving desks jobs at CDC, avoiding liability for hospitals). The guidance:
Covering your coughs and sneezes limits the spread of germs to protect others[1]. Handwashing with soap removes germs from your hands[2], making them less likely to infect your respiratory system when you touch your eyes, nose, or mouth. If soap and water are not available, using a hand sanitizer with at least 60 percent alcohol can kill these germs[3]. To remove germs and dirt on surfaces, use household cleaners that contain soap or detergent.
Notes:
[1] Coughing into your elbow does not limit Covid spread. And think of your hand as a very gappy mask. It won’t work either,
[2] Not Covid.
[3] Not Covid. Fomite transmission is not a thing with Covid, so hand sanitizers and surface cleaners are at best theatre.
Taking Steps for Cleaner Air for Respiratory Virus Prevention
The key move here is to separate “clean air” from masking. Obviously, since #CovidIsAirborne, airborne protection is a continuum (“Swiss Cheese Strategy”) that CDC chops up, making a coherent understanding of transmission impossible. The guidance:
Some germs spread in the air between people. This happens more easily in indoor, crowded spaces with poor airflow[1],[2]. To reduce the risk of exposure, it helps to improve air quality by increasing airflow, cleaning the air[3], or opting to gather outdoors[4].
Notes:
[1] Japan’s 3Cs formula — Closed, Crowded, Close Contact — is more memorable (and also known to work; 2020).
[2] CDC carefully omits the fact that one can measure the uncleanness (risk) of the air with a CO2 monitor like the Aranet4 or similar. It’s almost as if they want you to remain ignorant.
[3] Below, CDC mentions HEPA filters, but carefully omits Corsi-Rosenthal boxes, which are both cheaper and more effective.
[4] CDC also carefully omits UV. While Far-UV remains controversial, I believe that upper room UV is proven.
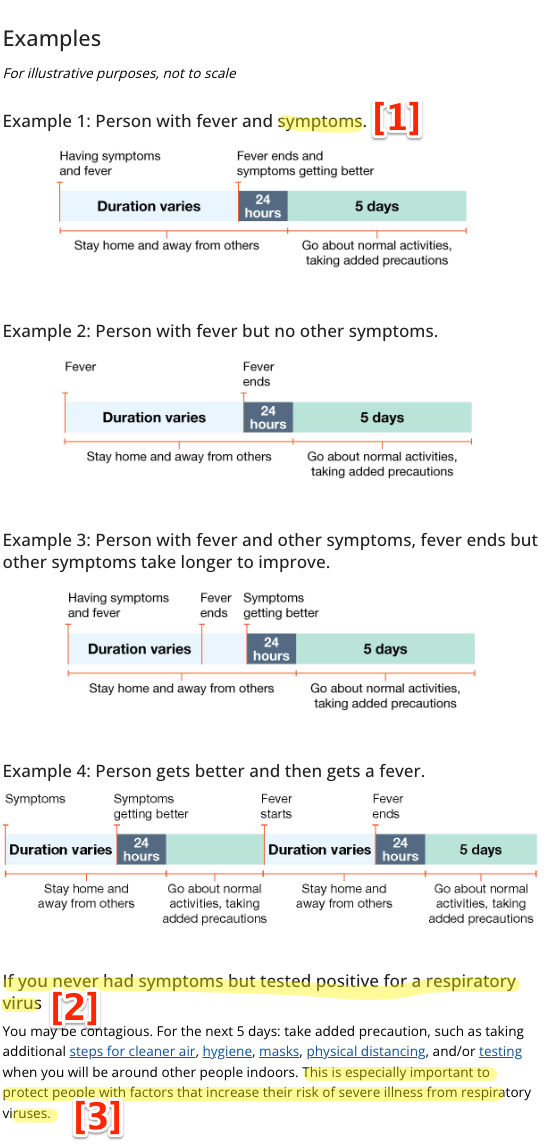
Preventing Spread of Respiratory Viruses When You’re Sick
Here too CDC carefully separates the concept of “preventing spread” from masks, even though masks help prevent spread.
Here is a diagram the “simple” and “streamlined” process that CDC recommends. I have helpfully annotated it:
Notes:
[1] Covid spreads asymptomatically (among superspreaders (Senegal): “Deepest transmission clusters are those with the highest percentage of asymptomatic members”).
[2] First, “nobody tests any more” (as the absolute numbers at Walgreens show). One reason for that is that the public health establishment systematically dismantled testing. Second, in a fine example of the principle Edward Tufte devised after analyzing NASA’s PowerPoints preceding the Challenger disaster, that which is institutionally least important will be buried, even if central-to-mission. Hence, explicit precautions like masks are placed in small type at the bottom of the diagram.
[3] Extending Tufte’s principle, protecting others is at the very bottom, in the last sentence.
Masks and Respiratory Viruses Prevention
The “what to know” section:
Wearing a mask is an additional prevention strategy[1] that you can choose to further protect yourself[2] and others[3].
Notes:
[1] “Additional” to what? Handwashing? The equally effective herbal remedies? Crystals? And heaven forfend we should connect masking to either hygiene to either hygiene or cleaner air; those are separate sections, even though masks — follow me closely, here — clean the air.
[2] Yourself first, naturally.
[3] Others last. There is no sense whatever that shared air is a public good that should be pathogen free.
Here is the simple and streamlined advice on masking:
Generally[1], masks can help act[2] as a filter to reduce the number of germs[3] you breathe in or out. Their effectiveness can vary against different viruses, for example, based on the size of the virus. When worn by a person who has a virus, masks can reduce the chances they spread it to others. Masks can also protect wearers from inhaling germs; this type of protection typically comes from better fitting masks (for example, N95 or KN95 respirators[4], [5]).
There are many different types of masks[6] that have varying abilities to block viruses depending on their design and how well they fit against your face. Cloth masks generally offer lower levels of protection to wearers, surgical/disposable masks usually offer more protection, international filtering facepiece respirators (like KN95 respirators) offer even more, and the most protective respirators are NIOSH Approved® filtering facepiece respirators (like N95® respirators).
When choosing to wear a mask, choose the most protective type you can. Determine how well it fits[7]. Gaps can let air leak in and out. Check for gaps by cupping your hands around the outside edges of the mask. If the mask has a good fit, you will feel warm air come through the front of the mask and may be able to see the mask material move in and out with each breath.
Learn about proper technique for wearing an N95 respirator.[8]
Notes:
[1] The “generally” qualifier is an open invitation to skip the entire section. Who among us, after all, is not “exceptional”?
[2] “Help” act? More faux qualification and precisions. What else is doing the filtration? My nose hairs?
[3] We started with viruses, now we have germs. Yet another scientific communication fail.
[4] Assumes the average reader knows what an N95 or KN95 is (and KN94 should be mentioned as well, but of course is not). Yet another scientific communication fail. The test: Could the average reader go on Amazon and even guess the right type of mask to buy? I say no.
[5] Now we have “respirators” as a subtype of mask, without explanation. Yet another scientific communication fail.
[6] “Many types” is confusing. Why not just say “blue surgical mask” (inferior) and respirator (superior), with an external link for Darth Vader masks? Note CDC carefully omits elastomeric masks with replaceable filters like Flo Mask. Yet another scientific communication fail.
[7] CDC carefully omits any mention (or external link to) “mask hacks” like Badger frames, twisting straps to tighten the seal, tips on re-usability, etc.
[8] This entire section reads like it was written by a hospital administrator who wants to keep buying baggy blues, and is making everything as complex as possible so obvious decisions that would benefit patients will never be made.
* * * It doesn’t get better, but that is all I have time for now. CDC’s guidance is a crime against humanity.


There was a mention the other day that there hadn’t been a sociopath of the day recently. I get it. They are all sociopaths. There is no picking. The sheer scope of their evil has become overwhelming.
I must applaud IM Doc again, and send both my thanks and my deepest admiration.
Pat, though likely frowned upon by the moderators I feel compelled to echo your sentiments.
And dear IM DOC, I hope that in what little free time you have you are able to recharge and rebalance yourself.
Thanks again to the NC crew and commentators, a beacon of reason and sanity in an unreasonable and insane world.
Thanks, very interesting and worrisome.
What would be the advise on vaccination now? Should we still get booster shots? Every time or once a year or? Which booster?
Confused about what to do, except masking.
I am not a vaccine maven nor does NC practice medicine. Personally, I would look into Novavax:
Peronally, I would avoid the mRNA vaccines based on Taleb’s “Lindy Effect” heuristic alone:
So I’d prefer a vaccine technology that’s been around for thirty years to one invented three or four years ago.
Taleb endorsed getting the vaccines as taking a bit of personal risk in order to protect others during roll out.
But I suppose the fact that no one is talking about protecting others or vaccines preventing transmission anymore also proves the rule.
Thanks Lambert!
One case with positive test in June 2022. Light!
I received Aztrozenica in US trial, a more old school vax.
I also took 2 Moderna spring 2021 to get card.
My choice no mRNA.
With more data I reject safety and effect “inferences”.
No faith in CDC.
Just got my first Novavaxx a month ago. Went 9 mo w/o an mRNA before doing so.
To my knowledge, I’m a “Novid.” I’ve not contracted it to my knowledge. Been sick, but never tested (+).
I’m O neg blood type.
Did an interesting anecdotal study on Mastodon the other day too. Asked for info about blood type and covid. The O’s reported significantly higher rates of Novid and/or common cold type symptoms. A/B groups were plagued with horrible stories of suffering and long covid.
I am a Novid also. 4 mRNA vaccines and for my fifth I switched to Novavax. Will stay with Novavax if I get future Covid vaccines. Still wear masks routinely with some lapses. I am an introvert. I am type O positive.
My mom is 0- and she caught covid last year. She took Paxlovid so it’s unclear why her symptoms were mild. She did seem to end up with a medical problem as a result (pancreatic insufficiency). To add to your anecdote survey.
Maybe still a Novid afaik. I had 2 X Astrazenica to start off in 2021, then 2 boosters with Novavax in 2022, 3 months apart (dictated by important family events). Had to wait ages for Novavax to be approved.
So far so good. Also mask with N95 everywhere in public, and am usually the only one, in stores with dozens of people. So no eating at cafes or restaurants which I miss a lot.
Partner, otoh, had 2 X Astrazenica to start off in 2021, then 2 x Moderna boosters in 2022. Since 2023 has been diagnosed with a life-threatening, very rare neurological disease of autoimmune encephalitis, and is on an IV drip once a month plus 6 monthly chemo drip. I think, looking back, it probably was starting in 2022 due to some small behaviour changes.
Partner believed the PR for the mRNAs over what I said. Of course I can’t prove that the two events are related, but I sure am wondering.
O+,
AZN and 2 Moderna.
One very little covid, 101 temp couple of days, no significant symptom beyond temp.
No boosters!
My dad’s blood type is O (not sure if it’s + or -), he caught a pretty bad case of Covid, with the attendant white lungs and was in the hospital for a significant period of time. The good news however is that he survived the ordeal, and he does not seem to be suffering from Long Covid. The sad thing is nowadays he pretty much refuses to wear a mask whenever he goes out.
I seem to recall a study from before covid vaccines that O blood types were about 20 percent less likely to get severe covid than À or B blood types, but I don’t have a link handy.
I’m O-, don’t mask, don’t take any particular precautions other than living healthily in general. I’ve had covid once, a year ago, while in a highly vaccinated country.
As a healthy, unvaccinated 60 year old, covid was 24 hours of a very sore throat, extreme tiredness, and brain fog. The brain fog was weird, more intense than the only time brain fog ever happened to me before (some bug many years ago).
On the whole, covid was 24 hours of fairly minor illness, after which I was tired for a few days.
I’ve had worse colds than covid.
You are ignoring the almost certain loss of 3 IQ points, which is enough to show up on tests but not enough for you to notice, and earlier onset of dementia.
Novid (4 Pfizer vaxxes with no particular reaction). O+.
OTOH, my AB+ brother is also a novid.
The problem is that our betters have so completely dropped the ball on this I think it is genuinely impossible unless you spend all your time and energy deep diving into the primary research to even come to preliminary conclusions on this. Nobody except scientists at the fringes are doing the sort of big data analyses that could allow non-specialists to come to anything like a fact based decision.
Take Novavax for example – all the data I’ve seen (disclaimer: I’m not an expert on any aspect of vaccines) suggests that its the best option for most people. The problem is that it seems that to get the most of Novavax you have to take it as a primary course and in a sequence of boosters. And even the Novavax stans don’t seem to agree on the details – mostly because of a lack of studies of sufficient sample size and length. And of course nobody can say what the 10-20 year outlook might be.
In my country, Ireland, its possible to get Novavax, but as a booster only, and now just as a single winter booster (i.e. once a year at most). I’ve asked multiple times if I could take it as a primary course, but they refuse to even consider it on the basis that I’ve already had my primary (RNA) series. All the evidence suggests that this is sub-optimal, but still probably better and (arguably) safer than the RNA vaccines.
Based on what I’ve read, if I was in a position to access any vaccine whenever I wanted, I would do a double course of Novavax with about 2 months separation, taking every possible effort to avoid infection before and during the period between vaccinations. I’d then (probably) take an annual booster using the most up to date formulation. But even this is, for me, based on more an educated series of guesses rather than any firm set of analytical findings that I’ve seen.
Thanks PlutoniumKun!
I’d also prefer the “normal” vaccine, as Lambert too suggested.
I haven’t even checked yet how easy or hard they are to get in my neighborhood (North Carolina).
I got Novavax shot on Friday in central NC at local CVS. Each package delivers 5 doses and the unused must be tossed at end of day. The store had 2 packages stocked so pharmacist had wanted to batch injection appointments to 1 day/wk. However, takeup has been so rare that after a wk she finally said just get shot, and tossed the rest. As I was waiting, 2 people came for mRNA. Only a slightly tender injection site over weekend now gone.
3 Moderna shots prior, to deal with critical care visits to family in their 90s while I was exposed to students. I’ve dodged Covid despite quarterly cross-country flights. I use Aura N95’s everywhere except when on weight machines in a low occupancy gym during weekly HIT.
Yes, you typically have to schedule ahead, usually by phone, so they can thaw out the vaccine, or even guarantee a supply. In Oregon, few pharmacies even offer Novavax, and the only ones that do are in the Portland/Vancouver area — a two hundred mile roundtrip for me. My vaccination came with zero side-effects.
P-Kim can you clarify your understanding of Novavax for me?
I had a double dose of Pfizer in early 2021, then a booster in 9/21, then caught covid twice in 3 month period, then got a Pfizer dose in 11/22. I got a Novavax shot in 11/23. Is my Novavax shot not providing much protection bc I never got a double dose of it?
I would repeat what I’ve said – I’m no expert, I’ve simply followed a few novavax stans online to try to cobble together some knowledge – and over time I’ve become more, not less confused. A problem issue is that its very hard to disentangle over time data from people with a multiplicity of different shots with differing exposure to covid. The latter of course is a major confounder on so many studies.
My understanding as of last year (I haven’t been following up much) is that having a Novavax shot as a booster does provide reasonable protection with fewer risks, certainly compared to RNA. However, to get the ‘full’ effect you need at least two shots, with a relatively short (2-3 months) spacing between them, and its very important not to be exposed to covid during that period.
Also, if you got a shot in November, its likely you had the most up to date version of novavax, which is a significant benefit.
So, my short answer would be ‘you are better off than most people’, but you still haven’t had the optimal course. Happy to be contradicted here by people with deeper and wider knowledge than me.
And where is my nasal/inhaled vaccine?
Exactly.
Why hasn’t there been an “operation warp speed” to test and potentially mass produce vaccines that would be as readily available to the general public as the steroid inhaler that I often use during the pollen allergy season. I haven’t kept up-to-date on whether or not there are already such products available in other countries. Any comments from NC readers?
Nasal drops vaccine, iNCOVACC, is generally available in India.
IIRC, first approved as a booster in late 2022, it is now also used as primary vaccine.
Sorry, don’t have time to look up link right now.
Well, I would offer an answer based upon the neat and tidy ” Long Stealth-Cull” theory but maybe that’s just me.
Maybe Occam’s Rusty Razor would suggest that Pfizer and Moderna want to keep selling their endless boosters for life, and a nasal vaccine would spoil the market for the mRNA para-vaccinoids.
I got my novavaxx at Costco.
Same, I’m not a member but they’ll let you in for the pharmacy vaccinations
Seems to me what IM Doc is saying is that the vaccine is a bad thing. Having no medical knowledge I have nothing to contribute here except to say I still refuse to get the vaccine and still have not had Covid.
I would say a more accurate way for me to describe what I feel right now is that we need to pause. We need to re-assess with completely accurate information what is going on with these boosters and we need a full accounting with accurate information of side effects. Complete and open raw data. For everyone to look over. No dumb questions. It is the only way. The fact that this has not been done since the beginning has unnerved me and many other providers.
We need to be doing complete and total risk stratification – which age groups benefit? how much? is it worth the risks? so on and so on. If this is found out to be having negative efficacy or an imbalanced risk/benefit ratio we need to pull them off the market right away. Half-baked studies are just no longer going to be sufficient. Raw data, please.
Your data clearly suggests the argument you are trying to make.
Is Lambert’s comment added to your post to dilute your key point? I do not understand the rationale.
Finally, someone came to the same conclusion I did! The VACCINE!
Ditto. No vaccine, no covid yet. Always an N95, Xlear and claritin, however. I don’t have any happy illusions about being somehow naturally safe.
I have only used mRNA so far, 3 times, but will be re-upping with traditional vaxxes in the future. If nothing else, the mRNA vaxxes have made me ill for 1-3 days, and my wife has gotten it worse.
The results of that doctor’s study above doesn’t necessarily mean mRNAs dont work or make things worse. In particular, the dip at 5 vaxxes that spikes back up at 7 makes me wonder if one of the two scenarios doesnt apply:
1. Perhaps people with many vaxxes have a false sense of security and take fewer precautions as a result.
2. Given that many places refuse to even give shots very frequently, this group could be the immunocompromised group that CAN be vaxxed more but being immunocompromised, also means they still get more infections.
In any case, Novavax is what I plan to do
I plan to take a covid vaccine when there has been one that has had at least 8 years of proper testing, with data carefully collected, and then at least 8 years on the market with follow up safety testing. Assuming the results are good, of course. And assuming that there are not perverse financial incentives for faking data. Given my age and even an optimistic life expectancy I guess I won’t be taking a covid vaccine. Not medical advice, but then I’m not sure where you’d get good medical advice on this topic. N95 masks are very good.
In the case of my husband, who has had three shots, and my father in law, who has had four, they are not taking more. However we are doing our utmost to keep them from catching anything (so far so good, knock on wood), since there really often appears to be a spiral down after a first infection.
Since we’re sharing our experiences in lieu of any significant research being available – I grabbed J&J/Janssen two dose initially. Had two mRNA/Moderna boosters because that was all that was available and finally a Novavax. I’m with Lambert on mRNA, it’s too new and agree with IM Doc in being suspicious of the spin on any adverse events in the current climate. If possible, I will get another Novavax for the next one or maybe forego since its protection is so limited.
Have thankfully not had a SARS-2 infection to my knowledge though it is getting harder to avoid as the social climate of denial continues to deepen.
Vaccines and the human immune system are by no means an easy problem and there can be subtle and not so subtle issues. Promoting vaccination as a silver bullet and the only intervention needed has been a big mistake in my opinion.
I can easily imagine a meeting at CDC headquarters. So, how do we “boost” vaccine efficacy numbers? Well, let’s remove from the list of vaccinated those that haven’t been boosted, let’s say, during the last 6 months. If this was a true conversation at a high level meeting it would be a reminder on how confident the wealth authorities are on vaccine efficacy. With luck, it might work for a few months. Yet this isn’t even the case. Please, go on with the silliness ad infinitum and keep boosting like crazy for no good reason and instate or re-instate google/microsoft controlled vaccine certificates so we, the PMC can easily detect any deplorable with a single click.
Then, as Lambert signals, there is the idiocy about masking/unmasking, and the false polemic about airborne/fomites transmission of respiratory viruses. Masking as an additional indicator of deplorable status? Now, the authorities want us to have the mandatory right to spread disease freely in as long as we wash our hands frequently. Because… we need to get used to live with disease?
Yet, we shouldn’t forget about the silliness of the lab-made conspiracy theory, the opportunity some saw to spread sinophobia.
This all looks pathetic in my opinion. Problem is that the silliness goes well beyond COVID as we see.
Any thoughts on why the j&j vaccine seems to be an outlier? Is it because, as Lambert notes above, existing tech & processes were used in creating it?
As I understand it, IM Doc’s list giving vaccinations – if any – and cases is reporting the vaccination data of his patients with COVID. It is not reporting on the illness status of his vaccinated patients. In other words, it is NOT an indication that J&J vaccinations were especially protective – rather, it is an indication that few of his patients who became ill had received the J&J vaccine. The J&J vaccine was problematic soon after its introduction, recommended against, and eventually withdrawn – for part of the history see
https://www.cdc.gov/mmwr/volumes/71/wr/mm7103a4.htm
An acquaintance used to work for J&J, and told me that the great majority of the doses manufactured were never used.
The issue with J&J was stroke risk…which in absolute risk terms was trivial, one in millions. But it was splashed all over newspaper front pages and was more than enough to tarnish J&J.
Call me cynical, but I suspect it had more to do with JNJ being a competitor with the mRNA vaccines which the NIH was a large intellectual property rights holder of.. not that those reasons are mutually exclusive. In retrospect it is strange how such a trivial issue became so newsworthy
The J&J vaccine uses an adenovirus envelope to carry the vaccine payload. I am not an expert but my understanding is that the virus needs to infect you in order to work so if your body has been exposed to the obscure virus and developed immunity to that, it doesn’t work. I think they used something they found in desert Africa. (Ad26.)
It uses a human cell line they developed which, in part, is designed to side step adverse reactions such as incurred from vaccines developed in chicken eggs, hamster ovaries, etc, which had been common before. So the tech is not as old-fashioned as the Novavax and roughly occupies a middle place between Novavax and the MRNA vaccines.
Backstory:
J&J bought the Dutch company Crucell in 2011. “The purchase equipped Johnson & Johnson with the tools to produce vaccines for the first time.”
Crucell was clearly not neoliberal enough for MBM. (Money Based Medicine.) At the time of purchase they were working with gold miners in South Africa who were co-infected with TB and HIV to develop a TB/HIV vaccine. (Not a Lloyd Blankfein approved business model.)
They had created a cell line PERC.6, (fetal retinal cells), and strikingly, had created a shared database so that Pharmas could all benefit from their individual findings using the cell line. (Aghastitude! WE don’t share!)
When the tsunami hit Acceh in 2004 they donated their pentavalent vaccine, (five childhood vaccines in one shot) to survivors. Perhaps someone else has info on the efficacy of this campaign.
After the purchase all of these efforts sank like a stone as far as I can find, and nothing was heard about the technology until 2021 with the emergence of their Ebola vaccine.
Then their SARS-Cov-2 vaccine came out in 2021. IMDoc’s February report is interesting re: J&J’s Covid cases, “J&J – 0 cases”, and I would appreciate hearing from him any trend over the months regarding the J&J vaccine. My intuition is that the fix was in when it was withdrawn.
I have no doubt that Coronavirus is endemic, continues to mutate, and has long-term adverse effects. It is not the Spanish flu that infected, killed and then went away. This treatment data is concerning. Boston COVID wastewater data indicates that the pandemic is seasonal — waning in February/March but not as quickly this, the fourth year. The conclusion becomes that this is intentional to make more money for the connected; not happenstance. Rather than spending tax money on public health to provide clean air in workplaces and schools or to fund quarantines and contact tracing; the decision across the world is to let the virus rip.
Professionals/managers will ignore this if their salary depends on it. But, when illness, disabilities and death affect family, caregivers, friends and colleagues, the dots will start to connect. When it becomes clear that eugenics/genocide on the quiet is underway, the current, end-stage, new world order will fall.
The proxy world war underway in Ukraine, genocide in Gaza, and this ongoing pandemic are all interrelated. Unrest is already here. This cannot be hidden much longer. When watching VP Kamala Harris call for an immediate ceasefire, listen to the tone of the cheers in the background.
Erm, Biobot is producing different results by region. Wastewater data shows higher Covid level in Feb v. Jan in the Midwest, and flattish in the West. So the seasonal decline notion is indeed falling apart, as IM Doc indicates. Perhaps March will show a decline across all regions, but that has yet to happen.
https://biobot.io/data/
> this, the fourth year.
I think we’re in the fifth year, but in a sense the count no longer matters. The public health authorities seem to have capitulated. It’s permanent pandemic from here on out.
Perhaps in future, the calendar will be adjusted to reflect the world-historical level of the changes in the approach to “public health” policy — we’ll count years as “Before COVID” and “In the year of our Distress.”
The conclusion becomes that this is intentional to make more money for the connected; not happenstance.
It could also simply be political pressure on the cdc to deliver the current administration a win. You note that the wars, the economy, CRE, homelessness, open borders, etc… are all abject failures, and at a family gathering of the PMC yesterday, trump is still the ONLY problem. I even had one imply that I wasn’t smart enough to know how wrong I am (I try to keep my mouth shut, but sometimes it’s impossible, and yeah, I let that one ride with just a bit of side eye. Family…they’ve all been sick in the recent past and none tested for covid.). The pressure to deliver a win can explain why the PMC who should know better, don’t.
From the article:
“J&J – 0 cases
Unvaccinated – 2 cases
2 vaccines – 14 cases
3 vaccines 24 cases
4 vaccines 76 cases
5 vaccines 32 cases
6 vaccines – 101 cases
7 or more vaccines – 49 cases”
But is that a higher, comparable, or lower vaccination rate than among the people not getting infected, or among the general community that IMDoc serves at large?
I work in a highly vaxxed area. However, there are a significant number of my patients that are from areas around us that are not so vaxxed.
I guess I should say initially vaxxed. With each new round of boosters, the numbers of people doing it have steadily fallen off.
What happens is that when we are in taking patients, the EMR tells us this person needs to be reminded of boosters, or this person is up to date. Unfortunately, the algorithms are not clearly keeping up with the level of confusion about boosters. For example, a young healthy patient who received the first two in 2021, but did not get a booster again until fall of 2022 is considered vaxxed. An older diabetic with the same pattern is unvaxxed and there are prompts to remind them about boosters. I can go on. It is a real mess. There are times when the recs do not make sense at all, and often the actual dosing is not even in the system. You can put the data in, but it takes days to update the system and that person will not be counted correctly. I do not think this is done intentionally at all, it is just the chaos of all the recommendations and poorly developed algorithms or algorithms not updated. I will say again, the EMRs are absolutely notorious for this in almost everything. I have, for example, all kinds of young athletic males who are “morbidly obese” in their charts. This is being reported to their insurance companies. I try repeatedly to get this off and corrected only to have it come back on future visits.
So, we really need to pay attention to the methods section in any of these studies. If the study is simply parroting the EMR reports, there are problems…..I am even OK with the verbiage “unvaccinated” “vaccinated” AND “under vaccinated”. That would clear this up instantly. But it would also take actual human beings ( abstractors) to go through the charts.
Since the advent of the EMR, I have noticed this same issue in so many things -not just Covid and obesity. The Med lists are wrong about half the time. Abstractors or chart readers are very expensive. This was one of the touted benefits of the EMR systems. Push a button and have instant comprehensive data. The truth is much different. It is easy to be oblivious to this when you are a researcher in an office in a medical school. When you are taking care of patients every day and see the constant problems, the GIGO becomes real plain real quick.
The pattern seems to provide some support for IGG4 class switching, I think linked to on NC a while ago, where the more vaccinated the more your body tolerates the invader. Yet in this case the invader is not an allergen that one would want to tolerate, but something that destroys your immune system.
Here is an article exploring the observed IgG4 class switching with repeated mRNA vaxes (which does not seem to occur with adenovirus vector shots). The possible repercussions of elevated IgG4 levels are also discussed. I thought it very interesting, but feel I need to read it again. I would love to hear the reactions of those more knowledgeable about immunology than I am.
https://www.ncbi.nlm.nih.gov/pmc/articles/PMC10222767/
To echo IM’s comment on EMR and prescriptions. I’ve been fighting this battle for years. Every visit, I’m asked to verify/correct my prescriptions (and I only have 2 active, but had a few more for a few months after a major surgery). Inevitably, there are old ones which I dutifully correct. The tech verifies my corrections and updates my records. Next visit some are gone, some are not, some previously fixed reappear. Some system they have there.
I’ve questioned the tech and doctor about this – why bother with these prescription updates when they don’t seem to “take”, and I get a shrug or eyeroll.
Here in the buboed groin of America, the North American Deep South (NADS), I have become used to being one of the very few masking in public any more. I have tried to try and elicit some sort of solidarity with other maskers met while out and about, but with almost no success. At present, masking in public seems to be treated as a moral failing, like wanking. Strangers studiously avoid eye contact with ‘maskers’ in my environs.
As a side note; I have encountered no, as in zero, proper respirators in public. N95 masks have been the most ‘sophisticated’ types of masks encountered.
So far, few examples of ‘robust’ pushback against my masking.
Stay safe all.
Thanks for the insights. Here in UK Midlands I’ve seen change over the past 3 years from one bad state of affairs to another. Early on, I frequently had quite middle-class appearing people (in one of the more “posher” supermarkets) “accidentally on purpose” push their trolley into me as I helped my elderly mother do shopping. I also experienced loud threatening verbal abuse in the street of the main shopping area of our suburb from groups of angry-looking men.
Now I am treated as if *I* must have the lurgy and miraculously often see a 1 metre space appear around me in shops and no smiles to me. Yet I constantly overhear people in the queue talk to others that “all the family is sick” and “I told everyone in our house that they weren’t going out for 3 days over a weekend so as to stop bringing bugs into this household”. Sheesh.
So far, nothing that bad over here.
I am a bit worried that, as the Pandemic gets rolling, “Maskers” will become convenient scapegoats for the inevitable public anger at the even now visible deterioration of the general quality of life as seen “on the Street.”
“She’s a witch!”
“How can you tell?”
“Er, she has a pointy nose!”
“Fair cop.”
“Burn her! Burn her!”
Do the continued alarums and apparitions blow away with the ashes of the witch? A question for Philosophers and Theologians, (both classes of Thought Leader being properly Credentialed, and Naturally Legal.)
I have several neighbors who haven’t spoken to me for 2+ years because I still wear a mask when I go out. Strangers are even more rude. They call me a variety of names and try to run me over in store parking lots with their cars. I have also experienced being hit with grocery carts while shopping. I try not to let it bother me too much. I have a chronic illness and so must continue to protect myself.
I was at a party and someone was proudly telling of shaming an old woman in a Costco for wearing a mask. If someone did that to me I would pull down my mask and say “Sufferin’ sucatash! YouTH are soooo righfhst, you have thft nothing to fear fthsrom me wiFthout my mask on (cough cough).” directly to their face in maximum spittle mode.
> at a party
The thought occurs that this might not be the best ideological crowd with which to share air, or whatever it is that partiers do at parties.
In the NYC metropolitan area,
there is slightly more masking going on than before.
Older people, especially women are more likely to mask.
Asian people are more likely to mask (young and old).
I’d say there was increased masking during the Jan/Feb period. I’m usually one of the few people masking and everyone avoids me when they see me with a mask. On the trains, people will avoid sitting next to me (great, keep your germs away).
Of those masking:
95% of the people are using masks with ear loops.
75% are surgical masks.
20% are N95 with ear loops or black face masks that look like N95.
5% of the people are using proper N95.
Not seen anyone with one of those Darth Vader N95 elastomeric respirators, yet!
I need to get me one for myself and then go around saying – “Luke I am your father.” LOL
One of the many horrifying side-effects of this debacle — which I know our moderators know about, but hasn’t been mentioned in this thread yet — is the total loss of respect for all institutions that has resulted.
Twitter this week is absolutely full of people saying that because the CDC has now said to treat COVID precautions the same as the flu, they were right all along, COVID is just the flu, the whole thing was a hoax, and they’ve been proven right. I’m not sure how they explain why all of those people died from the flu in 2020 and 2021.
And if COVID is not a thing, then long COVID can’t be a thing, either, so why worry?
We are living in the Alfred E. Neuman timeline.
One thing I’ll give CDC credit for is timing.
Vaccine/booster roll outs, adding protective measures to guidance, removing protective measures from guidance – all done just after the peak of the wave.
This way no matter what they do seems to be working.
Reading IM doc I think it is pretty clear that it is the vaxxed who get Covid over and over again. I quote: “298 total calls and cases – of these 298 – only 2 were truly unvaccinated [the first since last autumn] – the two I told you about around Valentine’s Day.” Further on he mentions that in his community 39% aren´t vaxxed. Actually it would be pretty easy to determine whether the vaxx makes any sense. Just choose two cohorts and follow them. They could have done that from the very start but didn´t. Pfizer “unblinded” the study after a few month. I think this is a sure one.
About Long Covid and the vaxx: here in Germany a leading goverment connected physician gave patients suffering from long covid the advice never to blame the vaxx if they wanted to get treatment.
It is all willfull obfuscation. They will never admit the desaster and that is why no real help is coming.
There are studies that show for mRNA boosters that while the patient does get a period of increase in protection, it’s only 2-3 months, and after that, the vaccines have negative efficacy.
I am not sure if this showed up on the first boosters, though (third shot). I believe it was for later boosters.
The Cleveland study is pretty clear. I quote: “The risk of COVID-19 also varied by the number of COVID-19 vaccine doses previously received. The higher the number of vaccines previously received, the higher the risk of contracting COVID.” Here the link: https://www.medrxiv.org/content/10.1101/2022.12.17.22283625v1.full
A friend of mine here in Germany and his wife have been (he) and his wife (still is) working for a big pharma company. They don´t believe in “conventional” medicine anymore at all. According to them the whole practise of medicine has been totally corrupted by money interests. Nothing new you might say. But it astonishes me to what length they go to avoid “normal” doctors and instead rely on “alternative” medicine. Not sure how much I would like to follow them. Both also didn´t get the VAXX. She was on maternity leave when this came up and he rather left and became self employed.
In regards to the “length they go to avoid “normal” doctors and instead rely on “alternative” medicine” I thought I’d throw this in. FWIW I recently was told by a nurse who was taking my blood for an annual exam that in general a DO (Doctor of Osteopathic Medicine) is more liable to encourage their patients to modify lifestyle/diet to reverse health problems. An MD will immediately grab the prescription pad for any ailments.
It did show up with the 3rd dose, too.
It’s impossible to say if it’s a real biological effect of waning immunity causing more infections, or if it’s just an artifact of delayed infections creating the illusion. (Since you really are immune to even mild infection for a couple of months after a vax dose, and since immunity from infection lasts longer, the unboostered could or will have longer periods of time where they’re immune as a result of infection.)
The latter may well be true but the vax side effects are on average way less bad than getting Covid. Losing 3 IQ point or more is a terrible outcome.
So IMHO the problem with multiple boostings is the probably net increase in odds of getting Covid (although you’d probably need to run a proper Monte Carlo simulation to be sure).
Thanks Yves. I remembered something to this effect but alas hadn’t bookmarked the articles on this subject, which explains why I’ve reached a point where I don’t regard mRNA boosters as worthwhile anymore.
I *think* it was the 2nd mRNA (thus 4th shot overall) that was followed by a COVID infection or reaction, though as I am careful to note elsewhere, I cannot and should not pin the blame on the shot. There are coincidences, after all. However, around here we have no power to choose which type of booster we get.
I don’t disagree with your overall point that IM Doc’s data seems to be raising the question of whether repeated vaccinations increase the risk of repeated covid infections or long covid or whatnot in the long run.
However my reading was that IM Doc was suggesting that the 39% unvaxxed rate in his county was probably because the county gets vaccination stats from EMRs, and the EMRs have a faulty and misleading way of determining how many patients are unvaccinated. So I don’t think that was meant to be an accurate estimate of how many people in his area or practice are totally unvaccinated.
I do very much agree with you that we never should have allowed Pfizer to vaccinate the controls. But you know, warp speed and all that.
There’s probably selection bias going on* — those who are unvaxxed are less likely to get tested and/or see a doctor. Personally, my son was never vaxxed and he still managed to get covid 3 times. I’m positive no one else at school tests as rigorously as we do and would never have known. The 3rd time he didnt even have a cold (mother was sick though)
*This isnt to say selection bias is enough to offset just how onesided IMDoc’s data is.. just that it may be somewhat misleading
I will never ever forget they mandated getting the “Jab” on pain of losing my job and how blithely my colleagues complied and saw me as “eccentric” for refusing, adding it up to my proclivity to question certain historical events that I need not mention.
Agree, and I won’t forget the people who wished me dead for refusing the shots.
Those would be the same people we see on FB and Twitter saying the CDC is great for what they just did and thank god for being vaccinated – because they are standing tall as one said.
Bite me!
Curiously, the situation which birthed the shameful and just-plain-wrong “pandemic of the vaccinated” mantra has, 4 years and 9 jabs later, developed into what can only be named a “pandemic of the vaccinated” though no one is calling it that, huh?
oops… original mantra should be pandemic of the unvaccinated… doh!
Several are calling it that. ‘pandemic of the vaccinated’ an aggressively deployed political trope, doubtless used as a divide and conquer tactic. It’s also specious. Covid is a pandemic of all of humanity and always will be, until we decide to put a stop to it and work together to do what is necessary to attain that outcome (which is technically fairly straightforward, but requires temporary sacrifice, and that window closed politically by the end of 2020, and was probably never open in the first place in the United States which, as the global hegemon, set the course for the world’s failure to solve this problem when instead it should have been ostracised by the rest of the world). Much easier to divert people from that fundamental and unglamorous reality when you dazzle them with inane ‘pandemic of the un/vaccinated’ clichés.
For Covid and related info someone I follow on X is Raina MacIntyre in Sydney. She works in disease surveillance and bio security.
Thanks for this post. To this day I wonder what the Department of Defense (DOD) is doing in this mess, why is the DOD involved?
Statement From HHS and DOD on FDA Emergency Use Authorization of a COVID-19 Vaccine Candidate
https://www.defense.gov/News/Releases/Release/Article/2445116/statement-from-hhs-and-dod-on-fda-emergency-use-authorization-of-a-covid-19-vac/
What is the DOD doing? It’s what they did. They birthed and started Moderna. Too late in the day to pass links but the DOD provided the start up funds and essentially created Moderna. Moderna had never produced any medical product until Covid.
“4 were mainly having headaches, severe vertigo, tinnitus, or actual chronic hearing loss.”
Thank you for your work Dr.
I highlight the above statistic because it immediately grabbed my attention when I read it. About two months I rushed home from work to take my wife to the ER. She thought she was having a stroke as the entire left side of her face had gone flaccid. She’s 45 years old.
An extremely perceptive ER doc (compared to my normal rural hospital experience) immediately diagnosed her with Ramsay Hunt syndrome (yeah, like Justin Bieber). It is brought on by an attack of shingles in the ear, which subsequently damages the facial nerve. Prognosis is 75% recover full facial movement over 6mo. She’s in month two w/o regaining movement.
All that to say, the foregoing were the precise constellation of symptoms she experienced. The actual shingles lesions are only sometimes visible. I say all this as cautionary to other readers. This is an extremely difficult illness to diagnose and time is critical as admin of steroids is critical within the first 3 days of symptoms appearing.
Stay safe out there people and please, maybe put in some positive thoughts for my wife.
Thank you.
All the best to your wife, Eric! Hope she’ll soon see improvement.
Best wishes for a speedy and complete recovery to her!
Sending positive healing thoughts to your wife! Thank goodness she had a skilled ER doctor who was able to correctly diagnose her.
Where are the whistle blowers who have copies of the almost-sure-to-exist “explosive” documentation of this intentional democide?
Hell, the IDF/Israeli actions at least have leaks of intent that make it into the record if ICJ filings, and how about those Wehrmacht generals chatting how to plausibly deny NATO’s war against Russia by using SUVs to deliver long-range Heinie cruise missiles to country 404?
There have to be leakable troves of inculpatory stuff, no? Or has the PMC Blue Wall closed completely off?
I don’t think the pharma-financed MSM would report on their information if they did come forward. How many reputable doctors have been struck off or silenced for bringing forward treatments the CDC and FDA do not endorse?
I think you are spot on. We can’t count on our “news” for truth or news, even if lives are at stake. 1984 was a manual not a novel as someone here so rightfully coined.
Senator Marshall:
Could long COVID be the bipartisan cause that brings the Senate together?
‘Sen. Roger Marshall’s voice was shaking with emotion as he made the case for speedy and focused research into long COVID. Marshall, the junior senator from Kansas, is a Republican and a medical doctor. But addressing the first-ever Senate hearing on long COVID last month, he wanted the audience to know that his interest wasn’t just professional and it definitely wasn’t just political. It was also personal.
‘One of his loved ones, he explained, suffered from severe long COVID. “We’ve taken my loved one to dozens of doctors,” he said. “I’ve talked to 40, 50, 60, 80. I’ve read everything there is to read about long COVID, talked to other members of the Senate that have had long COVID. What are they doing? So I share your frustration.”
…
‘Later in the hearing, Marshall blasted the National Institutes of Health, which at the end of 2020 received $1.15 billion to study long COVID, for “forming committees and praying about it” rather than working toward diagnostics and biomedical treatments.’
https://lasvegassun.com/news/2024/feb/24/could-long-covid-be-the-bipartisan-cause-that-brin/
I want to go into the question of the Why this is all happening so I will have to put on my Mark 2 Tinfoil Cap here so please bear with me. In short, it is all about November 2024. I suspect that last year the White House realized that the Pandemic was not going away but it was here to stay. But that created a problem. If there was one thing that the Biden White House did not need was the Pandemic as a campaign issue in the 2024 Presidential elections. So, what to do. They are trying to normalize it. So here are some ways that they are doing this. Having doctors say that herd immunity is a thing. Cutting back on the number of days that people should isolate to one and then eventually zero. Having businesses tell infected people to still come to work. Keep those schools going as everyday spreader events. Make it difficult for doctors to report field data to higher ups and make it clunky. Scale back on reporting mechanisms so that it is more difficult to determine the extent of the Pandemic at any one time. Discourage air filters in the work and study place. Tell people that vaccines are the solution to everything. When you normalize something then you are no longer afraid of it and I think that this is the aim here. I am not saying that there is a master plan or anything. But in the same way a flock of birds will all change direction at the same time, those of the professional managerial class can tell which way the winds blow and will follow that narrative in a flash and they have done so here.
Thank you. I don’t think it possible to be too cynical on this topic, and you may well be correct.
I would add (re: IM Doc’s data) that the choice not to distinguish “under-vaccinated” from “unvaccinated” strikes me as a rather transparent effort to degrade the data associated with the unvaxxed category. In other words, it would be a nightmare for those in charge if the true unvaxxed were to show distinctly better outcomes.
” In short, it is all about November 2024. ”
Remember the paper by Impact Research (iirc)? I’m trying to find a link to it, but I’m not having any success. It talked about the election and how to deal with the pandemic.
https://impactresearch.com/
“Proud pollsters for President Joe Biden”
I think that’s part of it, but encouraging vaxxing would put the disease on peoples’ minds (considering how unpleasant the process is) while filtratration can much more easily be hidden or ignored. Filtration in many workplaces would happen somewhere on a rooftop HVAC system, or be centered around a relatively innocuous floor or mounted unit.
Money is the other half of this. Filtration would require either subsidy or unfunded mandate, and the ruling class is loathe to spend anything on public welfare
Who would the Bidencrats be afraid would turn the Permademic into a campaign issue? The Trump campaign certainly would not/ will not. Maybe some Third, Fourth, Fifth parties would try to do so.
To echo IM’s comment on EMR and prescriptions. I’ve been fighting this battle for years. Every visit, I’m asked to verify/correct my prescriptions (and I only have 2 active, but had a few more for a few months after a major surgery). Inevitably, there are old ones which I dutifully correct. The tech verifies my corrections and updates my records. Next visit some are gone, some are not, some previously fixed reappear. Some system they have there.
I’ve questioned the tech and doctor about this – why bother with these prescription updates when they don’t seem to “take”, and I get a shrug or eyeroll.
For what it’s worth, this kind of persistent, permanent ringing sound, really a constellation of sounds, tones, bells, and so forth, can and does make people suicidal. If you don’t have it, trust me, you don’t want it.
I have had it mildly. The real problems start, I am told, when you cannot sleep. Happily I have never been that bad.
I’ve actually learned to live with it, but if you can’t “see” past it while trying to fall asleep, you’d definitely lose your mind. Full stop.
My mother had tinnitus. It was so bad, she made several suicide attempts. This was when I was in college. I lived at home, mostly because I was afraid to leave her alone, knowing what she might do. Her tinnitus did lessen somewhat (with no help from her doctor) after about 3 years. Why, I do not know.
As with so many things, there are a multitude of causes of tinnitus. I got it from listening to music too loudly both in my car and through headphones when I was younger. That eventually subsided for the most part, but later in life it began again – this time related to emotional issues of loneliness and lack of intimacy. Not much has been written on these last two points, but I have spoken to a few people who confirm this same “anecdotal” trend.
A few months before my mother developed tinnitus, she had been fired from her job after reporting that asbestos was falling from the office ceiling onto her desk. Losing her job was a very painful experience. I always thought the stress of that played a role in her getting tinnitus.
It has degrees. I’ve had it “mildly” for ages from going to too many gigs unprotected (subsequently went with well designed earplugs which helped greatly). Not a big deal.
But I once a more acute form on top of that as the side effect of a drug, and that was frightening. Thankfully it stopped when I discontinued the drug but I can absolutely see how that could make people suicidal.
Just fyi. From the White House website:
https://www.whitehouse.gov/visit/
To add another anecdotal data point:
I received two Pfizer mRNA vaccines early on, March 2021, three weeks apart. I dragged my feet on getting another “booster” but my mother (93 y.o. and suffering from cancer at the time) pressured me into getting another. I got the third Pfizer in late November 2021. After that third shot, I developed a strange case of urticaria, small extremely itchy fluid filled bumps mostly on my lower legs though it would pop up on my arms, too, on occasion. This lasted for about six weeks and slowly, very slowly tapered off so that I was back to normal by mid January. At that point I vowed no more mRNA.
Unless I have had an asymptomatic case, I remain “Novid” still. I mask in the grocery store, not at the gym or in dog training classes. I’m definitely an introvert, don’t get out much, not a fan of restaurants. My blood type is O+.
I have considered the Novavax but can’t seem to get myself to the CVS to request one. I’m holding out hope for a nasal vaccine…
I take a multitude of supplements including vitamin D and quercetin, also Turkey Tail sporadically. Plus, I have several herb blends for immune boosting that I do not take regularly, only when I intuit that it might be a good idea.
I have become increasingly cynical and wary of the medical industrial complex despite, or maybe partly because of, the fact that I worked as a provider for 30 plus years. I lean into “alternative” medicine, studied herbalism after I retired and grow much of my own medicines. I am grateful to all of you in the Naked Cap community. The discussions make me feel less like a crazy person. I don’t feel so alone.
Thanks for sharing your anecdote, CCinco. Very similar story here, except I had the Moderna jabs. Within a few weeks after getting a booster in Dec 2021 I developed hives that were fortunately well-controlled by cetirizine, but it was almost a year and a half before I could stop taking it without the urticaria returning. I’m also O+. Impossible to know for certain if the booster caused the hives but it seems to be a known potential side effect.
I’ve not had any additional boosters since the one. I recently read that CDC now recommends getting re-boosted every 4 months if age 65 or older but I’ve been reluctant. I may get the Novavax.
I still mask when going to the supermarket etc. but very few others do. If I’ve had COVID it was asymptomatic.
02 desaturation in stage III is consistent with loss of pulmonary capillary bed from 100’s of small unresolved emboli. I would bet if you measured Right Ventricular end diastolic pressures they would be elevated in these patients.
Ayone interested in the history of NIH bungling research into post viral illness should read up on ME/CFS. Osler’s Web is a good book, though old news now. More recently the ineptitude seems to be mixed with actual progress, search for opinions on the NIH intramural study of ME/CFS.
But gosh, wouldn’t it be nice to have 40 years of good research into post viral fatigue right about now?
Thank you IM Doc for your stats.
The way in which this whole COVID debacle has unfolded is quite extraordinary. Normally, one would assume the task of the CDC and most of the medical profession is to cure people, and one would conclude that they have entirely discredited themselves. However, when one sees that no lessons are being learned, one starts to realize that they’re in an entirely different business: that of manufacturing “reality”. China suffered a similar failure when young eager red guards replaced the “corrupt old surgeons” and performed surgeries with great fervor inspired by Mao’s little red book, but at least it was rather obvious. For the West, we’re following the path Aldous Huxley predicted:
democracies will change their nature; the quaint old forms—elections, parliaments, Supreme Courts and all the rest—will remain. The underlying substance will be a new kind of non-violent totalitarianism. All the traditional names, all the hallowed slogans will remain exactly what they were in the good old days. Democracy and freedom will be the theme of every broadcast and editorial—but democracy and freedom in a strictly Pickwickian sense. Meanwhile the ruling oligarchy and its highly trained elite of soldiers, policemen, thought-manufacturers and mind-manipulators will quietly run the show as they see fit.
As time goes on, I realize more and more that George Bush wasn’t an idiot missing from some village in Texas, as the bumper sticker went, but was that he telling us exactly how it is. When he said to journalists “We decide what reality is and you write it down”, he was simply describing how much of the West now works.
The fact that my local CVS in a heavily populated urban environment phased out covid testing is a damnable failure. Less than a mile from downtown in a major city.
I did three at home covid tests but still unsure if January was flu or something else. I need to check if blood donations still come with free covid antibody tests…
I am also interested in the IGG4 class switching Outside Observer mentioned.
More broadly, IM Doc’s report makes me curious whether unvaccinated and undervaccinated people have the same kind of long covid risk with repeated infections as the fully vaccinated. I could easily see how having, say, 10% of patients who were at increased risk of long covid with repeat infections would skew the overall result, potentially suggesting that everyone was at increased risk when actually only one group was. Or at least that, like with lung cancer and asbestos, everyone is at some risk but people with certain exposures are at much greater risk.
(The last I saw, vaccination neither protected from nor increased the risk of long covid–but this was nearly two years ago and so most people in the study were probably catching it for the first time.)
One statistic I would be interested in seeing is the proportion of IM Doc’s patients who are completely unvaccinated. Without that number, it is harder to parse what it means that 12/12 of new long covid patients were vaccinated at least somewhat. Also I would be quite curious to hear about the vaccination status of his long covid patients in months past.
Just watched an interesting and easily understandable video by a Doctor on the Cureus report that just came out regarding the vaccine trials (or lack thereof). The Doctor made the point that the mRna “vaccines” were not really vaccines. The lengths the powers that be are going to cover up this whole Covid debacle are amazing. Here’s a link to the video; https://youtu.be/p3F38nsP5Rw?si=J02iXKfR9xTLyoJ9
If you are a “novid”, there is a study by a group of immunologists, that’s apparently been going on for a couple years.
Covid Human Genetic Effort Study
>>>You or your loved one may be eligible if you/they:
Were admitted to or repeatedly seen at a hospital because of COVID-19
Did not get infected despite intense and repeated exposed to COVID-19
Of any age, from neonates to the elderly.
We particularly call for families in which multiple relatives have fallen ill from COVID-19.
I have a zoom church friend who is 65 who is in exceptional shape. Well, he was. He just retired from a government job and this past summer he bicycled across the U.S. with a group. He has had every single covid vaccine and has worn an N95 entirely faithfully. But now he has a very, very bad respiratory illness. A terrible cough, chest congestion and infection, pink eyes. First of all I don’t now how he caught this, wearing a mask. Second of all I wonder if it is the much feared (by a few) result of the IgG3 to IgG4 shift in the vaccinated. The worry is that the immune system’s learned disregard of the covid virus, would extend to other respiratory viruses since they bind to receptors that are similar to the ones the covid virus binds to. So learned antibodies that are lousy for covid will be lousy for those respiratory viruses, too. He is testing negative for everything they test him for (including covid).
I have a friend who has lived in his van for at least the 25+ years I have known him. He was an electrical engineer (no degree, but in Silicon Valley at the right time and smart) and is a veteran. So he has access to the VA hospital. He had covid last month and was hospitalized and it went very well considering that he is 81 years old. But now he is having spells of faintness. He asked me if I thought it was long covid, and if a test would show if it was. I told him there was no established test yet and that he should get himself in and get tested for stroke and heart and lung things; I think he will. He did not have the vaccine, so it’s not as if skipping the vaccine is some great panacea!! If he dies in his van no-one will know for a while since we have a rule that he has to contact me first, and he is estranged from all his relatives.
Wondering if we olds (60 plus) should get another MMR vax?
If protection wears off, sure don’t want to pick up measles in the current stew of viruses and so on.
Are new immigrants to the US vaccinated to US standards?
Regarding people who seem fine as far as heart and lungs but have trouble with exercise, I just saw this today: Low iron may play key role in long COVID. But I expect iron is on a standard blood panel and would have been noticed.
Vaccination started with a terrific record. Smallpox vaccine arrived in the 18th century. Today smallpox only exists as samples in labs. (Cue the suspenseful Covid music.) When I was a child in the 50s there was another child on my block with a withered arm, and another nearby in an iron lung. Then, like a gift from the gods, the polio vaccine arrived. Today polio only exists in a few isolated, wartorn corners of the world. Tetanus, diphtheria, and whooping cough all got vaccinated together. I became a parent and discovered vaccines for measles, mumps, and chickenpox. As an adult I reached the age where flu shots were offered, and discovered I did not need to expect to spend a week sick with the flu every year. Of course, that vaccine was not as effective, but it was still good. Then I reached the age for shingles and pneumonia shots.
Against all that success, HIV was stubbornly refusing to allow a vaccine. To this day, RSV is the only flavor of the common cold with a vaccine. Nothing for the more common rhinoviruses and coronaviruses. Then one day we discovered that the common cold coronaviruses had a cousin named Covid. President Trump could magically stare into the corona of the sun, and summoned the new-fangled Covid vaccines. What could go wrong?
As someone who has had seven Moderna shots, no known Covid infections, and no known side-effects, I cannot say what to think about the discussions above. My decades-old tinnitus recently developed a new trick, for which my doctor is sending me to a hearing specialist. Was that a side-effect? I miss the good old days when polio was bad and vaccine was good. Today we all have CDC whiplash. I just pray we do not get another big pandemic soon. We are not ready!
I have moderate tinnitus due to working around jet engines even with the best hearing protection available and yearly hearing tests. A side effect of the J&J vaccination was bouts of high tinnitus that came back after my first and second Covid infections.
Sasha Latypova writing about a new long covid study published in the Lancet 3 months ago on Dec 7, 2023.
Study in Lancet shows relationship between gut biome and “long-covid”
https://sashalatypova.substack.com/p/new-study-published-in-lancet-showing
She editorializes a bit in the first para and title; the rest of the article is about the study with a link to the study. It’s over my head. Maybe some readers will find it useful or interesting.
It has gotten to the point where it is very difficult to think that the Pfizer/ Moderna vaccines do a very good job of preventing people from getting sick. Sure, a lot of people say these vaccines reduce the severity of illness, but considering the very wide range of intensity of illness that characterizes Covid cases overall, that sounds like a highly subjective judgement.