By Lambert Strether of Corrente.
Previously in this series of round-ups, we looked at Covid and global GDP, as well as GDP in various counties; at the effects of interventions, pharmaceutical and not; and at “belief scarring,” a form of hysteresis. That was January; in February, we looked at labor force participation, as well as the quality of the labor force, positing that cognitive dysfunction from (often repeated) Covid infection degraded skills. This month we will repeat and expand on these themes, first looking at the so-called post-Covid economic recovery, then at Covid and the labor market and labor force participation, and finally at Covid and cognitive dysfunction in skilled workers, especially pilots.
The Economic Recovery from Covid
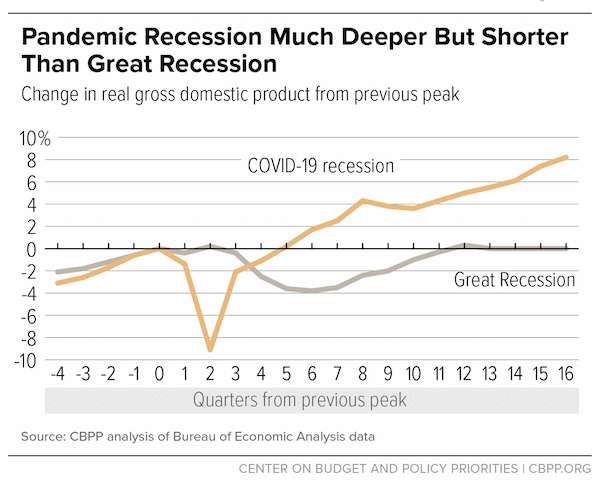
The Center on Budget and Policy Priorites has released (April 2024) “Chart Book: Tracking the Recovery From the Pandemic Recession.” For those who remember the brutal “recovery” frpm the Great Financial Crisis under Obama:
Real gross domestic product (GDP) early in the pandemic fell abruptly to 9 percent below its level at the start of the recession — a much steeper decline than the nearly 4 percent drop in the deepest part of the Great Recession. But the recovery and relief legislation enacted in March and April 2020, plus the relaxation in May of some restrictions on economic activity, led to a sharp (though partial) bounce-back in GDP in the third quarter of 2020. Subsequent relief and recovery legislation enacted in December 2020 and early 2021 gave the recovery an added boost.
As a result, real (inflation-adjusted) GDP surpassed its pre-recession peak in the first quarter of 2021, less than a year after the trough of the recession. GDP rose above the Congressional Budget Office’s (CBO) February 2024 estimate of potential GDP — the high-employment, maximum sustainable level of GDP — from the third quarter of 2021 through the first quarter of 2022 and then again in the third and fourth quarters of 2023. In the Great Recession, in contrast, GDP didn’t surpass its previous peak for two years and the actual-potential gap did not close until the third quarter of 2018, more than eight years after the recession ended.
Here is a handy chart:
And regarding the labor market (of which more shortly):
Like GDP and payroll employment, the official measures of household employment and unemployment… improved faster than initial projections. This is especially impressive because, as discussed below, some of these measures failed to fully capture the amount of labor market slack — that is, excess joblessness and underemployment — in the depths of the recession and early in the recovery.
Employment normally recovers more slowly than output after recessions, usually because employers are uncertain about how permanent an increase in demand for goods and services will be and they have an underutilized existing workforce they can use initially to meet an increase in demand. Until recently, however, labor markets in the current recovery were tight, with demand for workers growing faster than the supply.
This is what the economists are saying, of course. Your mileage may vary — and apparently that’s true for a lot of people. (For those of us who remember how Obama butchered his agonizingly slow recovery, today’s economy may seem preferable.)
Covid and the Labor Market
The Brookings Institution has published (March 2024) “The US labor market post-COVID: What’s changed, and what hasn’t?“, which is a report from a conference held in January with about 40 leading labor economists. There’s a lot here, and I picked out two nuggets. On wages:
After decades of growing wage inequality, the post-pandemic period has seen a substantial decrease in earnings dispersion between the 10th and 90th percentiles. However, participants noted that this reduced inequality is confined to those at the very bottom: Workers at the median of the earnings distribution, who have also been losing ground relative to the top decile for decades, have not seen gains post-pandemic.
Participants noted that, in typical business cycles, low-wage employees experience higher earnings when the economy is strong because they work more hours, not because their wages increase, making the wage compression during the COVID episode atypical….
Brad Hershbein of the Upjohn Institute noted that while wages have grown fastest for very low-wage workers, inflation has likely grown fastest for them as well, because they are more likely to spend a high proportion of their income on goods whose prices have risen the most since COVID-19. Steven Davis showed charts using data from the Atlanta Federal Reserve Wage Growth Tracker and the Employment Cost Index, published by the Bureau of Labor Statistics, in which inflation-adjusted compensation is, if anything, a little below its pre-pandemic level. Other economists took issue with the specific measures he chose and insisted the picture was less pessimistic. More generally, the participants agreed that using different measures of inflation and wages can significantly change one’s findings about the trends in real wages growth in recent years.
Weak wage growth across the board despite a tight post-pandemic job market puzzled many in the room. Ball hypothesized that goods whose prices increased due to supply shocks may have fed into inflation without putting upward pressure on wages. Some reiterated that the real wage declines could be partially explained by the non-pecuniary benefits offered to workers through remote work. Others pointed out that the labor market may not be as tight as suggested by recent increases in payroll growth because a surge in immigration has increased labor supply in the past two years.
And speaking of immigration, this chart from a presentation in the second session:
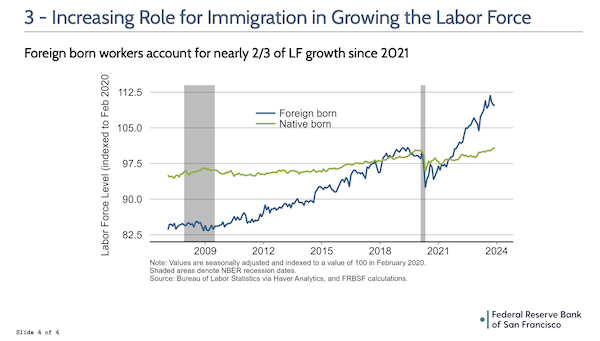
The economists don’t discuss the causes of the pre- and “post”-Covid discontinuity, but it’s hard to imagine that a million deaths and a mass disabling event didn’t create demand for foreign workers.
Fortune points out (April 2024) that “The number of job vacancies around the world is still unusually high–and there is no end in sight to the global labor shortage“, so it’s not just us:
In addition to an aging world, the Great Resignation was real, with many workers having left the workforce since the pandemic. In the U.S., an unprecedented 50 million workers stepped down in 2021 and 2022, reflecting a growing dissatisfaction with work following the COVID-19 pandemic. Although initially perceived as predominantly an American trend, the data suggest that this general dissatisfaction has spread to other parts of the world. France witnessed a record 2.7 million voluntary resignations in 2022, with similar trends observed across Europe, though Asia saw a decline in resignations. In Australia, there are growing signs of similar worker discontent. And even in the U.S. where quit rates have recently fallen, certain industries like personal care services continue to report higher-than-average resignation rates.
The labor shortages we observe can partly be traced back to the devastating impact of COVID-19, including the lingering effects of long COVID. In the U.S., the workforce has not only mourned the loss of over a quarter-million working-age individuals to the virus but has also seen a lasting reduction, with a figure more than twice as large across various age groups withdrawing from employment. Particularly affected were migrant communities, which suffered higher COVID-19 mortality rates, further exacerbating the decrease in available migrant labor.
Following the pandemic, a pronounced shift in work preferences has emerged, with a growing demand for reduced hours, enhanced flexibility, and better work-life balance. In the U.S., a substantial number of employees, for whom resignation isn’t a viable choice, have voiced a clear preference for more flexible working conditions, remote opportunities, and improved work-life balance–an enduring legacy of the pandemic’s impact on workplace norms.
The National Association of Manufacturers (NAM) also exhibits (March 2024) a welcome sense of realism, writing “Increase in Long COVID Cases Could Continue“:
A recent increase in cases of long COVID—the continuation or appearance of virus symptoms months after initial infection—could go well into this year, according to Medscape.
“About 17.6% of those surveyed by the Census Bureau in January said they have experienced long COVID. The number for February was 17.4[%]. Compare these new numbers to October 2023 and earlier, when long COVID numbers hovered between 14% and 15% of the US adult population as far back as June 2022.”
Researchers and clinicians say they are also seeing an increase in long COVID cases among patients who have had the virus two or three times.
The numbers could be even higher, however. In many cases, people either test positive at home or don’t know they have COVID-19.
NAM doesn’t explain why it’s concerned in this piece, but published “‘Long COVID’ Casts Long Shadow Over Workforce” in 2022.
Covid and Labor Force Participation
The Federal Reserve Bank of San Francisco published (March 2024) “To Retire or Keep Working after a Pandemic?” It includes this claim:
Before the pandemic, the rate of participation in the labor market for workers age 55 and older had remained fairly stable since 2012, at around 40%. At the onset of the pandemic, the rate abruptly stepped down to a new lower level, with no indication that workers would return to prior levels of active participation in the labor market. This description, however, masks a significant difference across this age group according to workers’ level of educational attainment.
The data in Figure 3 show that nearly all the surge in retirements around the arrival of COVID-19 is explained by the behavior of people age 55 and older without a college degree.
A further breakdown of the data (not shown) reveals that this rising share of retirements among workers without a college degree age 55 and older is similar across men and women and is concentrated among white individuals. The shares of retirements in 2023 among Hispanic and Black workers approximately align with their respective pre-pandemic trends. Other research suggests that this may be due to higher wealth saved for retirement among White workers compared with workers of other races and ethnicities, in combination with the safety and physical concerns associated with the occupations of workers without college degrees (Montes et al. 2022).
Meanwhile, the Federal Reserve Bank of St Louis had published (Q1, 2024) “Pandemic Labor Force Participation and Net Worth Fluctuation.” From the Abstract:
The US labor force participation rate (LFPR) experienced a record drop during the early pandemic. While it has since recovered to 62.2 percent as of December 2022, it was still 1.41 percentage points below its pre-pandemic peak. This gap is explained mostly by a permanent decline in the LFPR for workers older than 55. This article argues that wealth effects driven by the historically high returns in major asset classes such as stocks and housing may have influenced these trends. Combining an estimated model of wealth effects on labor supply with micro data on balance sheet composition, we show that changes in net worth caused by realized returns explain half of the drop in LFPR in the 2020-21 period and over 80 percent of “excess retirements” during the same period.
We have “nearly all” from the San Francisco Fed vs. “half” from the St Louis Fed, but from a narrative standpoint, the idea that older working class whites who had some money socked away in the house got out while they could seems to be consistent with both papers. Perhaps if we have some real economists in the readership they can comment!
Covid and Cognitive Dysfunction in Skilled Workers
The idea that our ongoing and unchecked Covid pandemic has created a mass disabling event seems to be slowly penetrating the public mind. Here for example is a Saturday Night Live sketch:
I don’t know if this was accidental or based of lived experience of some of the SNL writers, but an inconvenient truth was written into Ryan Goslings script for the show “my therapist got dementia during Covid”.
Covid raises your risk of dementia by 60% 1 year after “mild” if >60 pic.twitter.com/zajcknzliz— Prognostic Chats (@PrognosticChats) April 14, 2024
I can’t tell you how many stories like this I’ve read on the Twitter; and I’m sure if I followed Covid on Reddit, I would say the same. Meanwhile, the science on Covid (post- or Long) continues to pop. From Nature (February 2024) “Insights into attention and memory difficulties in post-COVID syndrome using standardized neuropsychological tests and experimental cognitive tasks“:
The COVID-19 pandemic has given rise to post-acute cognitive symptoms, often described as ‘brain fog’. To comprehensively grasp the extent of these issues, we conducted a study integrating traditional neuropsychological assessments with experimental cognitive tasks targeting attention control, working memory, and long-term memory, three cognitive domains most commonly associated with ‘brain fog’. We enrolled 33 post-COVID patients, all self-reporting cognitive difficulties, and a matched control group (N = 27) for cognitive and psychological assessments. Our findings revealed significant attention deficits in post-COVID patients across both neuropsychological measurements and experimental cognitive tasks, evidencing reduced performance in tasks involving interference resolution and selective and sustained attention. Mild executive function and naming impairments also emerged from the neuropsychological assessment. Notably, 61% of patients reported significant prospective memory failures in daily life, aligning with our recruitment focus. Furthermore, our patient group showed significant alterations in the psycho-affective domain, indicating a complex interplay between cognitive and psychological factors, which could point to a non-cognitive determinant of subjectively experienced cognitive changes following COVID-19.
No wonder people’s performance on the job is affected. From Nature (April 2024), “Long COVID still has no cure — so these patients are turning to research“:
In the weeks after her initial COVID-19 infection, Hannah Davis found herself struggling with severe brain fog, to the point at which she could barely string two sentences together. Davis, who at the time was working as a data analyst and artist, with a particular focus on addressing biases in machine learning, kept waiting for her cognitive function to go back to normal, only for it never to return. ‘I had, and continue to have, terrible, terrible cognitive impairment,’ says Davis, who is one of the co-founders of the [Patient-Led Research Collaborative (PLRC)]. Brain fog is having a significant impact on people’s livelihoods, says Wes Ely, a physician-scientist who works in intensive care at Vanderbilt University Medical Center in Nashville, Tennessee. People with long COVID have a form of cognitive impairment that is often ‘like mild and moderate dementia’, he says.
One industry where cognitive functioning is especially important is the airline industry; not only air traffic control (here; here), but on pilots. Alert reader JB threw the following over the transom. From the Public Health Communications Centre in Aotearoa, NZ (March 2024) “Long Covid in Aotearoa NZ: Risk assessment and preventive action urgently needed“:
The frequency of (often undiagnosed) cognitive impairment after a mild infection indicates a need for risk assessment of impacts on occupational safety and performance. Occupations of particular concern because of safety implications include healthcare workers, airline pilots, electricians, truck drivers, and first responders.
JB comments:
It’s clear to me this language is going to spread. And with good reason. Especially if the crash in NC where 8 souls were lost is affirmatively attributed to a pilot who had once contracted COVID19[1]. Meaning, he lost control and killed himself and 7 others due to suffering from the effects of PASC (long-COVID). If this is ever determined to be the proximate cause, all Hell is going to shake loose. And not just for pilots, but drivers, and anybody who’s hand-eye coordination is part of the deal – think crane operators, commercial divers, demolition experts, miners, etc.
Meanwhile, as you may know, I’m a pilot and job one before a flight is to self-certify that I’m good to go. Means if I don’t feel well, or am hung over, have taken some drug that may poses a risk of me falling asleep (antihistamines being an example), then *I* must decide if it’s better to postpone the trip. This is the meaning behind self-certify – there’s no *mother may I* – mechanism. It’s 100% on me as the pilot in command (and this is the language – PIC – pilot in command) to make the determination.
Really, this is no different, if you think about it, than what we as drivers decide before taking the wheel. Except unlike in pilot training, I don’t recall in Driver’s Ed. actually being taught this (beyond the obvious, don’t drive and drunk – and not even sure that was mentioned, e.g. it was implicit). Ditto regarding the wisdom of driving whilst feeling sleepy. However, with pilots, it’s specifically taught. It’s a responsibility that comes with the territory and which I, for one, take quite seriously (and this seriousness is shared, I’m pretty certain, by all pilots).
Yes, *all* is doing some heavy lifting in that last sentence. So do they all take it as seriously as me? Nope! No more so than all drivers will never take the wheel whilst drunk. But we are (we being collectively, the pilot population) taught to self-certify and I believe, we’re doing the best we can. Do some break the rules? Definitely, recall recent news of some airline pilot being dragged off a flight as unfit for duty due to being *very* hungover.
Problem (predictably) is going to arise in the adversarial relationship between FAA and pilots. Similar to the adversarial relationship between commercial pilots and their employers (reason an unfit pilot thought he could depend on his copilot to perform the duty whilst he slept it off). Had he raised his hand, e.g. called dispatch and said he was sick or otherwise unfit, he’d soon lose his job.
Added to which, there are economic consequences for losing a pilot’s license just as there would be for a commercial trucker losing his CDL (commercial driver’s license). Outsized consequences as in meaning they wouldn’t be able to earn a living so in addition to the rest of their bills, they may be on the hook for payments for the truck/airplane, etc. Since nobody will make them whole, they’re going to cheat the system. Human nature.
Also, people aren’t necessarily aware that they are cognitively impaired. That’s human nature too. I imagine when executive jets start colliding or falling out of the sky, some notice will be taken. So, optimism.
Conclusion
I keep toying with the slogan that “the only market is the labor market.” If you can’t get workers because of a labor shortage, or if the workers you can get are cognitively impaired, your business is at the least under stress, and might go under (think Boeing and MCAS, except with cognitive impairment). In other words, the labor market is — or at least can be — material. From ginormous accounting firm KPMG, “COVID-19 and income statement presentation and disclosure“:
Under IAS 11, when items of income or expense are material, a company discloses their nature and amount separately, either on the face of the income statement or in the notes. A company’s approach for COVID-19 will depend on its ability to determine the impacts on a non-arbitrary basis (i.e. quantify them reliably) and on the pervasiveness of those effects to the financial performance of the company.
Quantifying the impacts of COVID-19 on a non-arbitrary basis may require significant judgment – distinguishing between income and expenses that are part of normal operations versus those that specifically relate to COVID-19. As a company adjusts its operations to the new reality, making that cut is becoming more and more challenging. If the impacts cannot be determined on a non-arbitrary basis, we believe the company should not present them on the face of the income statement, but consider disclosure in the notes, providing quantitative (when possible) and qualitative information and stating whether only some, or all, of the effects have been identified.
In some cases, a company may be able to determine the impacts of COVID-19 but find that they are pervasive – e.g. affecting nearly all line items of the income statement. In that case, we believe it may be impracticable or less meaningful to present the impacts on the face of the income statement. Instead, the company should consider disclosing them in the notes.
From a purely business perspective, since the damage from repeated Covid infection is cumulative, it might make sense for companies to address (“quantify”) potential cognitive dysfunction in the workforce sooner rather than later (ditto, from the other side of the house, hedgies and shorts). Pilots, surgeons, nuclear power plant operators…
NOTES
[1] See here from AP: “The pilot of a small plane that crashed off North Carolina’s coast in 2022, killing the pilot, four teens and three other adults, was likely distracted while trying to program the aircraft’s flight management system.” Oh.


https://fred.stlouisfed.org/graph/?g=16Twa
January 4, 2020
Labor Force with a disability, * 2010-2024
* Age 16 and over
(Indexed to 2010)
https://fred.stlouisfed.org/graph/?g=17ENT
January 4, 2020
Labor Force men and women with a disability, * 2010-2024
* Age 16 to 64
(Indexed to 2010)
https://fred.stlouisfed.org/graph/?g=1eaS9
January 4, 2020
Labor Force and Population with a disability, * 2010-2024
* Age 16 and over
(Indexed to 2010)
Thanks. I couldnl’t get to disability. Maybe next time. (AFAIK, our disability system is horrid, so these figures are probably artificially low).
“Thanks. I couldn’t get to disability…”
( Almost certainly the Labor Department disability figures I set down, though alarming, understate the problem. )
( What Lambert Strether has been doing and has now done on Covid is superb. )
Pandemic of the vaccinated…
Exactly. The mRNA vaccines cause themselves “long Covid”:
https://www.ncbi.nlm.nih.gov/pmc/articles/PMC10849259/#:~:text=In%20the%20current%20study%20of,(long%20long%2DCOVID).
It’s not just the infection. Also, they cause a number of other issues that if people are curious enough they can go read the scientific papers. Such as this one:
https://www.journalofinfection.com/article/S0163-4453(24)00053-7/fulltext#:~:text=Rubio%2DCasillas%20A.-,IgG4%20antibodies%20induced%20by%20repeated%20vaccination%20may%20generate%20immune%20tolerance,%2DCoV%2D2%20spike%20protein.&text=Following%20repeated%20mRNA%20vaccination%2C%20IgG4,to%2019.27%25%20after%20three%20doses.
No matter how much that research piles up, some , probably most, people, just cant bring themselves to “go there”.
I have few regrets but getting two clotshots might be my biggest .
Nobody here is arguing that there aren’t harms to vaccines. But to make vaccines the primary driver of post-covid vascular problems is, well — today is my day to be kind, so I won’t say “dishonest” or “deranged” or “in utter bad faith” — wrong.
NOTE “Clotshot” is brilliant and totally non-organic; suddenly it was all over my timeline. Whoever coined it earned every penny.
Then how did all those people ended up totally f****d up back in 2020 before there were vaccines, and how did the same happen in much greater proportions with the much more severe SARS1 back in 2003?
Enlighten us.
A vitamin D deficiency? An Ivermectin deficiency? A natto deficiency? A low BMI deficiency? A black seed (aka kulangi) deficiency? A sauna deficiency? .
….
Now you know. Just follow the bread crumbs!
There is what seems to be a human tendency to look for simple, one-dimensional human agency when “bad things happen to good people.” Hence, “it’s the vax.” (Or, I suppose, in the Middle Ages, divine agency; “the Gods must be angry.”) Then we can cast the blame on a few individuals, and once that is done, normality returns. The political advantages of this style of thought are obvious.
Sadly, that’s not how pandemics work. Or complex systems, or the natural world.
The Black Swan> We have to accept the fuzziness of the familiar “because” no matter how queasy it makes us feel (and it does make us queasy to remove the analgesic illusion of causality). I repeat that we are explanation-seeking animals who tend to think that everything has an identifiable cause and grab the most apparent one as the explanation. Yet there may not be a visible because; to the contrary, frequently there is nothing, not even a spectrum of possible explanations. But silent evidence masks this fact… The Aristotelian “because” is not there to account for a solid link between two items, but rather… to cater to our hidden weakness for imparting explanations.
[One reason good science is so hard to do is eliminating confounders. Difficult to do when Cuomo took out thousands of the most vulnerable population before the vax was available. For example.]
One note on this, Taleb has emphatically stated that pandemics are not black swan events because they are one of the constants of built civilizations. their risk was known but ignored, or dealt with, to put it in a phrase he would jot off, in an imbecilic manner.
> Then how did all those people ended up totally f****d up back in 2020 before there were vaccines, and how did the same happen in much greater proportions with the much more severe SARS1 back in 2003?
*** Crickets ***
> The mRNA vaccines cause themselves “long Covid”:
Here at NC we insist on links, and for good reason.
From your first link from the NBCI, here is the Conclusion in the Abstract. I have helpfully added two notes:
So there are two problems with your claim. The first is that it is false, for two reasons. The second is that it’s context-free.
[1] When you say “The mRNA vaccines cause themselves [sic] ‘long Covid'” you omit (a) that the study did not distinguish between vaccine types, and (b) that the study urges this is true for “people who have already contracted COVID-19.” (In other words, there are enormous confounders.) So your claim is false. (You may have attempted to cover yourself with “it’s not just the infection,” whatever that means, but that’s straw manning. I haven’t made such a claim.)
Further, I don’t think much of the study; it’s based on phone interviews; there’s no proof that vaccination was actually performed, and no tests were performed for the actual presence of Long Covid.
Finally, a serious study would have addressed the additional confounders of vaccine type: mRNA, vector, protein (ideally killed virus too, but sadly the United States is not China). Do the effects differ between mRNA and the other two? I would bet yes, but the study doesn’t investigate.
[2] The implicit conclusion a layperson would draw from your claim is “Don’t get vaccinated.” The study, however, urges that the risk of death be factored in.
Here is the correct link to your second study, which does in proposes an interesting mechanism. I have also added two notes. From the Abstract:
[1] The text of the study is heavily qualified, as we see. So “they cause a number of other issues” overstates your case substantially.
[2] This study, as well, is context-free. I understand people don’t like Sophie’s (or Hobson’s) choices, but here we are. It is not up to the study to provide that context, of course, but to the person who cites to it.
First link is also limited by the study taking place in Iran, whose response to the pathogen was notably disastrous. Purported harms of vaccination are bound to be confounded with harms of infection (as they were in USA, where both the disease and the vaccine per se were politicised in the stupidest ways, which many people fell for – ie “just a cold”, and, on the flip side, the “clot shot” infantilism. This saw preliminary surveillance tools like VAERS flooded with a lot of not very useful data that was nevertheless taken far more seriously than it should have been by those who were keen from the beginning to paint the “cure” (never a cure, never any prospect of it being a cure by itself) as worse than the disease, for political reasons.
Oft ignored by the “everything bad is because of the vaccine” crowd are the erstwhile “Zero Covid” countries which for the most part had a discrete period of mass vaccination campaign followed by a period of mass infection. Recorded harms at an epidemiologically discernible and significant scale like excess death – remember, vaccine fearmongers were saying the vaccines killed en masse – always happened following mass infection, not vaccination (vaccine harms were reported mind you; Australia observed elevated clotting risk in AstraZeneca – not the mRNA products – and subsequently curtailed their rollout, not recommending them to the groups deemed to be at higher risk). See this thread re: New Zealand for the best example I’ve seen, with data, of what I’m describing.
Thanks for threadjacking, champ. See the headline? “More Economic Effects of Our Ongoing Covid Pandemic (with Cognitive Dysfunction and the Labor Market)”
When I want to post on vaccine harms — and take the time to disentangle all the anti-vax talking points, of which there are a plethora, many though not all untrue — I’ll do it. I had not planned to invest the time hosing out that particular Augean stable in a post mainly focused on the labor market which is why I didn’t cover that topic.
Lambert, you are doing God’s work with not only your covid coverage but also with your replies to commenters clearly operating in bad faith. Indefatigable!
. . . ” Also, people aren’t necessarily aware that they are cognitively impaired. That’s human nature too. I imagine when executive jets start colliding or falling out of the sky, some notice will be taken. So, optimism.” . .
If that would actually do it, then perhaps a way should be found to keep giving covid over and over and over again to executive jet pilots till enough of them collide or fall out of the sky that the upper classes decide this covid thing has gone too far and the time has come to reign it in.
It helps to accept the possibility of being impaired. It seems to be an article of faith of some, and I am deliberately using the word faith, that Covid must be mild or it is just propaganda, the vaccine protects, and that somehow the Good People will be okay.
Having gotten it at least twice despite masking, using items like that horse paste, and generally isolating myself, I have made an effort to note anything at all that might show impairment. So far, it has been mild and transitory, but I think that I might not have noticed it had I not made the effort. At least, I think so.
Among those people who downplay it, I think it likely that they would actively resist noticing any impairment. We all have days when the brain or the body just does not work right after all. People are very good at not noticing what they do not want to notice.
I did about a page or so of notes on this thing (anosognosia) and sent them through to Lambert maybe a day or two ago. I’m not going to burn-up this comments section by posting the whole damn piece, but you might find this interesting:
Functional connectivity underlying cognitive and psychiatric symptoms in post-COVID-19 syndrome: is anosognosia a key determinant?
Lack of awareness of cognitive impairment (i.e. anosognosia) could be a key factor for distinguishing between neuropsychological post-COVID-19 condition phenotypes.
https://pubmed.ncbi.nlm.nih.gov/35350554/
Bottom-line: covid can cause physical damage to the brain that could keep a person from realizing they’re ill, but I see no reason that psychological factors (denial) cannot have a similar effect.
> I did about a page or so of notes on this thing (anosognosia) and sent them through to Lambert maybe a day or two ago
I need to revise my contact info once more (I did, but removed it). I would have missed your work without your comment.
Of course, we’re assuming a distinction between physical and psychological (not to be reductionist, but).
I’m a layman who was trying to get a better grasp on Frontotemporal dementia (FTD). The info on covid/anosognosia was tangential to my research, but something that I found… interesting.
Anosognosia, this type of lack of insight, is because of physical damage to the brain: this is not an assumption.
My step-mother was afflicted by this disorder via Alzheimer’s, and my father has this condition likely as a result from FTD (in his case, we’ve had CT scans from 2014 and 2021 to work with, the latter suggesting “cerebral atrophy… frontal lobe atrophy”).
The link I provided can give you some numbers that are useful for back-of-the-envelope calculations that could give you a better idea of the magnitude that this disorder poses, especially given it’s relation to executive dysfunction in “people (who) aren’t necessarily aware that they are cognitively impaired.”
If you’ve got contacts in the world of neuropsychology, I’d love to see them lend their $.02 to the issue.
I should add that I installed UV air filtration systems at all employee stations that should create “virus-free bubbles” covering ~220 ft2, and our lab has free-flowing outside air (at least when it’s not too cold here in Southern California). It’s hard to understand why the CDC has chosen not to inform the public about the various non-Vax defenses, especially given the acknowledged non-100% effectivity of the vaccines!
I mean, layered defenses could have made a lot of money, but it would not have gone to big pharma.
> I have made an effort to note anything at all that might show impairment
My first thought was that there should be an app, but it would have to be carefully tuned to the individual. For example, I am — so far as I know — not cognitively impaired, but I am dyslexic, so any test would need to account for that. The same, I would imagine, for color-blindness, and I am sure many other exampled. I’m sure there’s plenty of science to be had here, but whether a classic Silicon Valley “Minimum Viable Product” would be a sound approach is an open question.
Loss of smell, in IMH (non-medical) opinion, signifies neurological damage caused by the virus.
One of my employees (20s, female) had this symptom, and she never recovered her writing and editing skills in the 18 months post-infection she remained with my company. There was brain fog for a couple of months. She did not recognize the deficiency but would not catch editorial items in my draft writing that she would have caught prior. I had to pick up some of the slack.
My point is neurological deficiencies can be subtle and undetectable by self-diagnosis!
Also, even now that everyone knows COVID is not a thing, I take Ivermectin and other key supplements whenever I find myself with an upcoming high-risk event (Mask up if I see on NC, COVID in my area is a thing), etc. I really do not want permanent neurological deficiencies.
I already had plenty of reasons for not travelling, and that was before the 737 MAX, but COVID-linked dementia in pilots is the cherry on top!
Thanks for this most useful compilation!
Quietly tending my garden, and hoping that the wildfire smoke isn’t too bad this summer …
> the wildfire smoke
Due diligence compels me to remark that N95s and Corsi-Rosenthal boxes both protect against wildfire smoke, which is nasty stuff.
My HEPA air cleaner was on 24/7 for some weeks during the last major fire season. It was the only reason that I was able to not cough continuously and sleep, but I was trapped in my bedroom. Or in the car with its own HEPA. We should reduce our use of electricity and tech, but seems that modern technology is needed just to breathe and stay alive some days in sunny California.
I have an uneasy feeling that in the LTC industry, COVID-induced cognitive impairment might be a profit center, inasmuch as it could warrant a higher level of care than for unimpaired residents.
Forget about the LTC industry, the whole COVID response ended up precisely as if it was driven by the objective of profit maximization through getting as much of the population to chronically wreck its health as possible.
For the record, I don’t think this was the primary motivation, as I have explained many times. It went like this is in order of priorities:
1) No more lockdowns after the first one, with the first one being as short as possible, and then no proper containment effort ever again.
The way you handle something like this is the way the Chinese did, and the way the West maybe would have too once upon a time back in the 1960s-1970s, when public health was still a thing. That means total quarantine, hyperaggressive test-and-trace, population-scale mass testing (we never had that tool previously in history, but now we do, and it makes the job so much easier), closed borders, etc. And you keep this going until local elimination in each country, and eventually worldwide.
The problem is that someone had to pay for it all. To pay people to stay home and not work, to pay for setting up the infrastructure to do all this, etc. etc. Who would have had to pay for it ultimately? Ordinary people have nothing, so it had to be the elites. Completely unacceptable in the modern world — there is no USSR as an alternative anymore, so we just don’t do the thing where the elites pay for anything contributing to the common good anymore. And a lot of the details of it were not just merely unacceptable, but outright mortal threats to the system. Paying people not to work? Complete anathema because what kind of precedent does that set? And they were saying so openly at the time — business media back in March-April-May 2020 featured one talking head after another bitterly complaining precisely about that issue. Then you had to freeze and cancel debts. Even more sacrilegious — the whole system of exploitation is founded on the right of some people to issue debt out of thin air and have the rest of us pay interest to them in real goods and services. If you freeze or cancel debts that undermines the sanctity of those obligations (BTW, Michael Hudson missed a huge opportunity to connect his work to the reality of the COVID response back in those days, and I still don’t understand why, but that’s a separate discussion). That’s the first win (for them).
2) From the very start it was known that the old and/or frail are most at risk of dying. This was very welcome news to the powers that be, who had been looking for ways to reduce pension and healthcare spending for decades prior to the pandemic. And what better way to do so but to decrease life expectancy dramatically and to also take out the immunocompromised, the cancer patients, etc. within the younger cohorts? Get rid of the human waste and transfer those resources to the elites, who need to buy themselves even bigger yachts. Win-win.
3) The issue of chronic disease only comes third. It was known from the start that this will be a mass disabling event, because that is precisely what happened with SARS1 back in the days in 2003, but at a much higher rate because it was a lot more severe in general. At least half of the 10,000 or so people who got it back then were left with some kind of serious permanent issues, many of them totally disabled (as in never being able to return to work, severely impaired in daily life, and never recovering even many years later). The only question was what the rate would be with SARS2, but then you add reinfections to the picture, and it’s an endless game of Russian roulette, which everyone loses eventually.
Again, this was known with reasonable certainty already in the first months of 2020. And we know what the business model of Big Pharma is — curing people is not profitable, treating them is, so it is preferable to never cure them. This too is not at all hidden — it has been openly discussed in the business press for many years. What could be better for business then than a mass disabling event that creates a tsunami of chronic health issues in the population?
The eventual “response” ended up precisely along these lines — a vaccine that doesn’t work but was pushed as the one and only and final solution to the problem, plus very expensive drugs like Molnupiravir (which doesn’t work at all), Paxlovid (which kind of does, but nowhere near sufficiently well to solve the problem, plus barely anyone has access to it anyway), and monoclonals (most of which were quickly made obsolete by antigenic drift and access to which is even more limited than it is for Paxlovid because of the even higher cost).
Win-win-win.
But still, that is only the third item on the list of priorities. Early on what they were mortally scared of was the socioeconomic ramifications of lockdown. They only went for it because they were even more scare of the ramifications of forcing people to go to work and school while they are dying on the streets (never happened in the West, but did happen in some Third world locations). Once they were sure they would be able to stretch out the deaths over time so that it never gets to that point, it was let it rip and forget about infection control.
Well said.
I remain shocked at three things (at least):
1) The complete moral and ethical degradation of the hegemonic PMC[1] who enabled our capitalist ruling class to execute this eugenic strategy (looking at you, Mandy, but you’re only an ideal type). Hippocratic oath, professional integrity, “Veritas” (Harvard), “Lux et veritas” (Yale), all down the crapper, with the worst of the worst[2] still making bank.
2) President Xi (a) throwing a million or so Chinese working class people under the bus because some financiers and Western reporters in Shanghai muscled him, and (b) failing, despite knowing that Covid is airborne in early 2020, to adopt a clean air strategy, despite having the manufacturing might to do it. (Of course, one might argue that China’s ruling class has the same motivations as our own, which would upset a lot of people).
3) The willingness of the ordinary population to accept nonsense like infecting their own children to prevent infection, and a million other “stupidest timeline” talking points. Oh, and the supreme importance of the “normal” (i.e., the convenient and the pleasurable, like brunch). I still don’t know how this trick was managed (“know” at a low, epidemiological level, as if with seating diagrams). This third point to me is the most discouraging, and demoralizing, of all. “In spite of everything I still believe that people are really good at heart.”
NOTE
[1] Not all, of course. The valiant aerosol scientists who managed to (one hopes) mortally wound droplet dogma are also PMC.
[1] Stanford, “Die Luft der Freiheit weht” (“the wind of freedom blows.” Indeed. Although it does sound better in the original German).
The third point is the most striking.
The trend for decades had been towards helicopter parenting and extreme concern about the slightest inconvenience that might befall one’s precious progeny, completely disproportional to the actual treats in existence.
Often combined with extreme hypochondria and germophobia,to the point where it was likely actually harming kids (exposure to regular bacteria seems to be needed for the proper development of the immune system; but note — normal everyday bacteria, not pathogenic viruses).
Then those very same populations who had descended down that rabbit hole were ready to physically fight for infecting their precious kids with a SARS virus.
It makes absolutely zero sense, doesn’t it?
I have thought a lot about this one and what it reveals about human psychology.
Human behavior is driven by the evolutionary mandate to maximize inclusive fitness. The catch is that no human until the mid-20th century knew what inclusive fitness is, and 99.99% still have no clue to this day. So behavior is not actually driven by inclusive fitness maximization, but by various other factors that historically have been proxies for inclusive fitness. They don’t need to be perfect proxies though, and that can create these perverse situations in which people will do actively harmful to their progeny things.
One of the main such proxies is social status, and in this case, in the name of preserving it, people were willing to force infect themselves and their kids with SARS instead of fighting the system that as forcing that choice on them.
That also revealed that to most parents kids don’t really have much of an intrinsic value; social status is more important. A simplistic reading of evolutionary theory would tell you that parents would never harm their own kids in such a way, and yet it happened on a global scale. Because, again, behavior is actually driven by proxies.
“…actual treats in existence.” is actually closer to what the boomer deferred childrearing and fundie cohorts I observed from the late Eighties forward were afraid their offspring would encounter.
Typo supremo!
My impression is that people have a biologically set amount of time that they feel they should spend with their kids. So helicopter parenting came to be because people don’t have their kids around much as they did in the old days (because in modern times kids are typically in school or at school type activities). So to make up for the lack of time with their kids, they hovered over them when they had them. Once the kids were not in school due to covid, parents discovered that they didn’t much want to be around them all the time. So it wasn’t social status; it is that there is a certain amount of time that people can stand being around their kids and having them at home exceeded that. Maybe the biological basis for this is the need to train small kids to exist in the outside world (and people are too stupid to override this during a pandemic). Of course individuals vary in their ability to tolerate kid company. Maybe the same biological qualities that make religion tolerable also make having kids around tolerable. The sickness risk is not relevant since mentally healthy people don’t in their hearts think they will get sick; only excessively rational people do.
That blather is my way of explaining this to myself; maybe there is even something to it.
GM: Many thanks for this post. You take a long view. You place things in their scientific context (what was known and and what could have been, and can still be, hypothesized). You examine the economic factors and the malignity of the current economic fantasies as they apply to us human beings.
My only quibble: I suspect that people in the West were dying on the streets. But the shambles of the health-care system in places like the U S of A and England mainly recorded the deaths as overuse of the Emergency Room. Extra charge required.
I think that the main cause wild push for AI despite its many flaws comes from gradual destruction of the people needed to keep a society running. It is just too bad that the technology seems to cause as much problems as it solves for the ruling class.
I retired in 2021. I’m turning 62 years old and I am NEVER going back to work, and especially not in any congregant settings.
Is the damage from COVID actionable – I a, thinking the good doctor Dr. Fauci o might look good in Court.
What I think will start weighting heavily are insurance rates and coverage exclusions.
This will possibly compell firms to start implementing effective Covid-19 preventing measures. The impact on their business statements will be very tangible when firms can no longer find qualified personnel medically certified to be fit for specific jobs, or get coverage for civil liability.
I’d love to see that GDP chart with the FIRE sector removed. I think increased predation of consumers and financialization may account for a GDP bounce back. PE roll-ups in numerous sectors have resulted in effective monopolies in many areas that were at least nominally competitive after the GFC.
Covid causes people to spend more and that’s all that matters, https://www.reuters.com/markets/us/us-retail-sales-beat-expectations-march-2024-04-15/
Cognitive skills are overrated when credit is still available.
Last July, a CDC report found that approximately 96% of Americans, age 16 and older, have some COVID-19 immunity. It must therefore be challenging to assemble an infection- and vaccine-naive control group for the study of cognitive dysfunction due to “long COVID.”
Dr. Coleman, epidemiologist: Please link to the report that shows 96 percent immunity to a disease that produces only a fleeting immunity.
Also, why would someone assemble an “infection- and vaccine-naive control group”? What would the hypothesis to test? At this point, the studies of long Covid, of which Lambert Strether, our Covid-reporter stalwart, has published many links. Most of these studies would be observational studies, wouldn’t they? We are talking about people reporting their own symptoms to medical doctors?
“Long COVID”? IN quotation marks? Are you one of those people who show up at web sites after mass killings with long guns to dispute the use of the term “semi-automatic rifle”? No, alas, it’s a bulleting-spewing blunderbuss!
Finally, I will assign you some homework: Read GM’s excellent comment just above.
> We are talking about people reporting their own symptoms to medical doctors?
There’s a lot of ways to do this: Self-reported surveys, medical examinations, biomarkers (the last not yet reliable).
In any case, this comment seems to be an example of (Brownnose Institute-induced) RCT fetishism (“control group”). I don’t see, for example, how we could have produced an RCT for the Black Death, even if we had the tools then. “Global” is, perhaps, a synomym for “heavily confounded.” RCTs are only one tool, and not necessarily the best one.
> Last July, a CDC report
I’m not seeing a link.
The link: https://www.cdc.gov/mmwr/volumes/72/wr/mm7222a3.htm
In the Summary, see What is added by this report?
“By the third quarter of 2022, an estimated 96.4% of persons aged ≥16 years in a longitudinal blood donor cohort had SARS-CoV-2 antibodies from previous infection or vaccination….”
How do you have a mythical efficient market economy when more and more people are being taken out of the work force due to Long Covid. And this is at all levels of the work force from people slinging burgers right up to high-powered executives. It’s like having an anchor chain attached the the economy that only gets heavier and heavier over time. In prioritizing “the economy” over worker’s health, they ended up sabotaging both. God forbid that we have another pandemic in our lifetime because you just know that our leaders will f*** up with that one as well, more so of it is spread by aerosol action.
> God forbid that we have another pandemic in our lifetime
10 major disease outbreaks in the 21st century so far CNBC (2022).
I would be very surprised if we didn’t have another SARS-CoV-2-level pandemic in the next twenty years. Maybe 10; all the systematic risks identified by Taleb et al. in January 2020 still exist, especially mobility/connectivity (mostly air travel, though Boeing has really stepped up to the plate here).
On top of all those factors not being addressed and only worsening, we now also have a thoroughly destroyed public health system that won’t play the game of pretending to try to contain that next pandemic, we will go straight to let-it-rip.
You are seeing it right at this moment on at least three fronts:
1) H5N1 in cattle in the US.
2) Monkeypox in the DRC (this is the serious strain with the 5% or so IFR, not the mild one from 2022).
3) The creeping measles outbreak in the UK.
And I’m watching all three very carefully.* IIRC, the closest CDC came to admitting mpox was airborne was agreeing that tiny little fomites appeared when bedding was shaken (maybe its not, but mo fair hearing was ever given). And we are, naturally, only worrying about symptomatic cases of H5N1 in cattle. Let the culling begun!
* Why my section heading is Pandemics, no longer #COVID19
I have to wonder if during BS sessions involving a bunch of actuaries on coffee break at life and disability insurance companies, they ponder the effects of possible future pandemics on current rates charged on policies. Term life and whole life policies. Disability insurance rates now that we are a few years in.
IIRC not too far into the C-19 pandemic there was a gentleman at an insurance company that had put out done numbers. Apologies for not tracking down having to head out the door.
Thanks Lambert for the article. The economic consequences are becoming difficult to ignore. Considering the current war environment, it will be interesting to see the effect of Covid and Long-Covid in the army. At least, the UK Army has added moderate and severe Covid as a medical condition for ineligibility.
https://jobs.army.mod.uk/how-to-join/can-i-apply/medical/
(Under other conditions)
Lambert, thanks for keeping the tracking going. A couple of things:
1) 1 million deaths after adjusting for age of the deceased translates into a drop in the labor force of about 300,000 workers, about 0.2 percent of the current 168,000,000 estimate. Long COVID is where the big impact is at.
2) The problem with the Fed studies is that they both use 55 and older data as a group. The reason they do this is that BLS seasonally-adjusts data for this age group, but not for the 55-59, 60-64 etc. groups, and seasonal adjustment allows for comparing one month (January 2020) with any other month (March 2024).
This problem came up in earlier studies that concluded there was a huge increase in early retirements (<65). Simply looking at the non-adjusted data and using the same month for comparison (e.g. January 2020 and January 2022) showed that it was older workers that had a decline in participation, which is still the case (see below). Just looking at the 55+ leads to a different conclusion because it misses the change in composition of that age group toward older workers who have a much lower participation rate.
Here are the comparisons for the age groups. A word of caution: there is noise, so it would be better to view several years of data. There are some differences male/female (BLS and Census are still binary)
55-59: Jan 2020, 72.7; Jan 2024, 73.7
60-64: Jan 2020, 57.2; Jan 2024, 58.1
65-69: Jan 2020, 33.4; Jan 2024, 32.6
70-74: Jan 2020, 20.6; Jan 2024, 19.5
75+: Jan 2020, 9.7; Jan 2024, 8.3 (Note: this rate was 8.3 in Jan 2018, so maybe 2018-21 was an aberration? Or sample error.)