This is Naked Capitalism fundraising week. 752 donors have already invested in our efforts to shed light on the dark and seamy corners of finance. Join us and participate via our Tip Jar or another credit card portal, WePay in the right column, or read about why we’re doing this fundraiser and other ways to donate, such as by check, as well as our current goal, on our kickoff post. And read about our current target here
Lambert here: As some commenters have noted recently, “tempting” not least if one feels that cannabis is an effective and safe alternative to Big Pharma’s formulations.
By Jan van Ours, Professor in Labour Economics, Tilburg University;Professorial Fellow at the Department of Economics, University of Melbourne; CEPR Research Fellow, and Ali Palali, PhD candidate at the Department of Economics, Tilburg University. Originally published at VoxEU.
Although worries about cannabis are usually based on prevalence rates of cannabis use in the population, age of the first use of cannabis is important as well. Early onset age of cannabis may have serious short-term and long-term negative effects on individuals. Previous studies find that early cannabis use increases the intensity of use and the probability of subsequent drug use (Yamaguchi and Kandel 1984). Van Ours and Williams (2007) find using Australian data that individuals who start using cannabis early in life are less likely to quit at later ages. Van Ours (2007) finds for cannabis users in Amsterdam that quitting rates increase with the age of onset. Van Ours et al. (2013) find using data from New Zealand that early onset of cannabis use may lead to mental-health problems i.e. to suicidal thoughts.
Current Cannabis Policies
Cannabis policies across the world differ – cannabis use can be:
- Legal
- Illegal but decriminalised
- Illegal but unenforced, or
- Illegal
The slight difference between decriminalisation and non-enforcement is that under decriminalisation there is no legal punishment, whereas under non-enforcement there is a punishment, but this is rarely enforced. Only four states in the world have legal or quasi-legal cannabis use: the Netherlands, the states of Washington and Colorado in the US, and North Korea.1 Several European and South American countries and states in North America have decriminalised cannabis use. However, countries which forbid cannabis use still outnumber the others (Figure 1).
Figure 1. Cannabis policies across the world
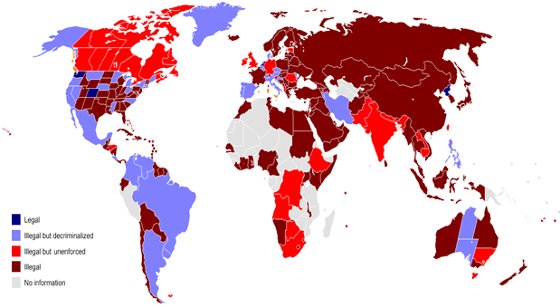
Source: Wikipedia.
Contrary to the general expectation that easier access will induce more use, existing empirical studies – largely focusing on medical-marijuana dispensaries in the US – fail to provide a unique conclusion on the issue. In the US, several states have medical-marijuana dispensaries which make access to cannabis easy. Cerda et al. (2012) and Wall et al. (2011) find that allowing for medical-marijuana dispensaries might have increased cannabis use. However Harper et al. (2012) and Anderson et al. (2012) show that there is no such effect. Therefore, there is not yet a consensus about the possible effects of easy access to cannabis on cannabis use.
A Short History of Coffeeshops in the Netherlands
Cannabis use is quasi-legalised in the Netherlands. Selling or buying small quantities of cannabis through so-called coffeeshops is not prosecuted. Drug policy in the Netherlands mainly focuses on the protection of public health (van Laar 2010) and can be summarised as ‘tolerant’ (van Solinge 1999). The basic aim of these tolerant policies is to reduce the harm done to users and their immediate environment in order to protect public health. The main drugs law of the Netherlands is the Opium Law of 1976, which introduced a distinction between soft drugs and hard drugs. The production and trade of soft drugs were considered to be much more severe offences than personal use. Possession of a small amount of cannabis was considered not as an offence but as a misdemeanour, and therefore not prosecuted. This flexibility paved the way for house dealers, which after a while turned into coffeeshops. Later on in the 1980s, the policy of tolerance of coffeeshops was publicly announced, and this announcement was followed by a sharp increase in the number of coffeeshops (Jansen 1991). In the mid-1990s, there were around 1,500 coffeeshops.
However, the 1990s also saw increased criticism of the Netherlands’ tolerant cannabis policy, both from inside the country and from other countries. The rules under which coffeeshops could operate were changed by the Dutch government in 1995. From 1996 onwards, the limit for personal possession of cannabis was decreased from 30 grams to five grams. Moreover, the monitoring and punishment of production and trade of cannabis were increased, and local governments were given the opportunity to decide whether or not they wanted to have a coffeeshop in their municipality. These more restrictive policies caused a substantial decrease in the number of coffeeshops in the country to an estimated 1,200 in the late 1990s (Bieleman et al. 2007). In 1999, the so-called ‘Damocles’ law gave more flexibility to local governments for closure of coffeeshops in their municipalities. The law resulted in a further decline in the total number of cannabis shops. In 1999 there were 846 cannabis shops across the Netherlands – a number that went down to 651 in 2011. Figure 2 shows the number of coffeeshops in each municipality in 2007.
Figure 2. Coffeeshops in the Netherlands, 2007
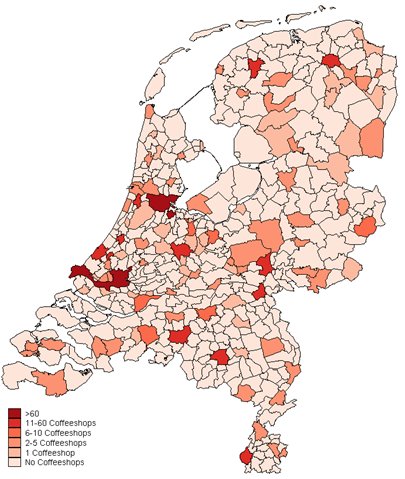
Source: Bieleman (2007).
Are Coffeeshops Tempting?
Our recent paper investigates if cannabis shops in the Netherlands have had negative spillover effects on youngsters by analysing to what extent living near a coffeeshop affects the age of onset of cannabis use (Palali and Van Ours 2013). If there was a negative spillover effect, then we would expect those who are living close to coffeeshops to have a lower age of onset of cannabis use. Table 1 below shows that the distance to a municipality with a coffeeshop seems to matter. More than half of the individuals in our sample live in, or within 5km of, a municipality that has a coffeeshop. In the young cohort, given on the left-hand side of Table 1, the individuals in this short distance range had a 40% lifetime probability of cannabis use, whereas individuals living more than 20km away from a coffeeshop had a lifetime prevalence of 16.9%.
In order to investigate whether there is indeed a causal effect from distance to cannabis use, we perform a counterfactual analysis in two parts by analysing starting ages of cannabis use of an older cohort, and starting ages of tobacco use of both cohorts. Table 1 below shows that for the uptake of tobacco, the distance to a cannabis shop does not matter. This suggests that people who live close to a cannabis shop do not have a different attitude toward use of other drugs, i.e. towards smoking. Since unobserved factors related to attitudes toward drug use would be correlated with unobserved factors behind attitudes toward smoking, this result shows that cannabis shops do not open up in neighbourhoods where people are systematically different in terms of risky health behaviours. Second, we show that the effect of distance on cannabis uptake is only present for the younger birth cohort. Individuals from an older birth cohort, given on the right-hand side of Table 1 – who grew up before the era of coffeeshops – are not affected by present-day distance to a cannabis shop.
Table 1. Distribution of distance to cannabis variable, lifetime cannabis use and lifetime tobacco use based on distance categories for young and old cohorts
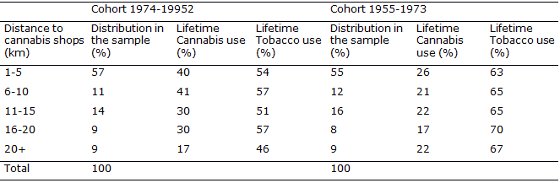
This is additional evidence that coffeeshops are not located in environments where people are more likely to start using cannabis anyway. The reason is that these individuals in the old cohort were already in their mid-20s when the first coffeeshops were opened (the mid-1980s), indicating that they had already by and large made their decisions about cannabis use before the first coffeeshop was established. If there was a correlation between location of coffeeshops and general attitude of residents toward cannabis use, this would be shown in the distribution of lifetime cannabis use of the old cohort in Table 1. However, as indicated above, lifetime cannabis use percentages for the old cohort do not seem to differ across distance ranges.
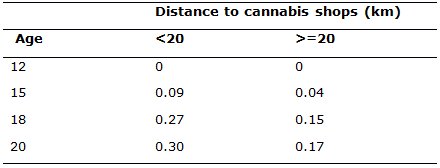
In order to provide further evidence for our preliminary findings, we analyse the starting age of cannabis use and tobacco use for young and old cohorts by using duration models. In these models we control both observable and unobservable characteristics that would affect uptake of cannabis. After an extensive examination of the results, we conclude that those who live within 20 km of a coffeeshop start using cannabis at earlier ages. We find that the starting age of cannabis use in the old cohort and the starting age of tobacco use in both cohorts are unaffected by the distance to cannabis shops. Based on our baseline parameter estimates, Table 2 below presents the results of a simulation exercise showing the effect of the distance variable on the probability of using cannabis at a specified age. We find that those who live far away from coffeeshops have a lower probability at any age.
Table 2. Simulation results showing the effect of distance to coffeeshops
The results above confirm the fear that availability of cannabis at Dutch coffeeshops has an adverse spillover effect on youngsters. Does such a finding immediately suggest that it is better to close coffeeshops? Not necessarily so. Even though we find that youngsters who live closer to coffeeshops display a lower uptake age, we cannot conclude that there is a welfare loss induced by the coffeeshops. There are numerous other factors that need to be taken into consideration, such as the intensity of use, the uptake of hard drugs and the effects of an uncontrolled environment. Our study does not provide evidence on how the intensity of cannabis use might be affected by the existence of cannabis shops. Furthermore, we would expect the closure of all cannabis shops to lead some potential users to go on the black market in search of cannabis, where they will be more likely to come across dealers of hard drugs. All in all, although existence of coffeeshops seems to have an adverse effect on the uptake of cannabis among youngsters, this is insufficient reason to advocate closure of coffeeshops.
Please see original post for references
1 Recently, the parliament in Uruguay approved a law that will legalise cannabis.


“Furthermore, we would expect the closure of all cannabis shops to lead some potential users to go on the black market in search of cannabis, where they will be more likely to come across dealers of hard drugs.”
Like ethanol
Let’s talk about alcohol…
The big problem I have with normalising cannabis (or any other drug) use is that, for people with mental health issues, you tacitly make it easier for people with those conditions to self-medicate.
Prompt and effective (and yes, thereby hangs a huge tail I know, but not one I’ll go into here) interventions are key to improving outcomes for people with mental illness. But making drugs available — such as cannabis — means that ill people are less likely to seek treatment. Incorrectly administered drugs — or even drugs which are contraindicated — will make matters worse.
It was tragic to observe patients who attended the mental health charity I was involved with a decade or so ago rendered psychotic and pretty much unreachable because they had self medicated using cannabis, opioids or even prescription drugs.
On most other things, I’m as liberal as the day is long. But not on this issue, for that reason.
While I understand your concerns, would you rather that we return to prohibition, with all its problems?
Hi diptherio, apologies, I should have explained myself better — I think you’re right and prohibition doesn’t work. I’m more in favour of the lines that upstater made — a controlled substance, available through a highly regulated distribution channel, quality controlled and priced to deter use. Any revenues to be diverted to providing health support for users, mandatory counselling and screening for mental health problems.
I was more reacting to the “coffee shop” approach in the original feature — unregulated, freely available and at, presumably, a market clearing price (i.e. lower than a regulated price could be set at as a deterrence).
‘available through a highly regulated distribution channel, quality controlled and priced to deter use. ‘
It is a weed that is easily grown. Such regulation is impossible(note vast quantities currently dope grown indoors and outdoors in US). Perhaps offer up something possible?
I notice that calls for practical alternatives seem to go unanswered. Surely there is some actual evidence that the drug warriors can present that marijuana should be regulated more heavily than alcohol?
Or maybe the MJ experts really don’t know that aspirin kills more Americans than marijuana? Or maybe they don’t know that you can brew beer in your basement without a doctor’s prescription? Or that alcohol kills more Americans than all illegal recreational drugs combined?
@Clive
I agree entirely. We have a family member that used semi-legal, high-test cannibis in Canada while at university. Daily use preceded the first of several psychotic episodes.
The link between cannabis and psychosis is a topic that has not received adequate funding. But there are studies that find strong relationships see (also read Patrick & Henry Cockburn “Henry’s Demons”):
http://www.bmj.com/content/342/bmj.d738.full
The problem is that cannabis is unregulated. Consumers REALLY do not know what they are getting. Potency has been increased through selective breeding and it is sometimes intentionally adulterated with chemicals. The so-called “medical marijuana” approaches 20% TCH. This is NOT the same product as the 1970s.
Cannabindiol (CBD) is a component of cannabis that has shown some promise in treating mental illness, but again, funding is inadequate to develop a legitimate medication.
The present state of cannabis is a wild-west unsupervised, unregulated public health nightmare. Deal with a pot-smoking psychotic person and you will agree.
I’m sorry about your family member, but do remember that correlation is not causations. I don’t agree that current cannabis policy is a public health nightmare. I think that phrase better describes the over prescription of anti-depressants, anti-anxiety meds, opiate painkillers, stimulants for behavior modification of children, as well as the overuse of Tylenol, which causes large numbers of tragic overdoses.
Self medication is not necessarily bad medication. I know several people who self medicate with cannabis for anxiety and chronic pain, and function quite well. My opinion is that they would be better off learning meditation and yoga, and that they could control or learn to live with their conditions in that way. I think at some point they will, most people get tired of being stoned, but if they were using the official medications for their conditions they would be physically addicted and would have a far harder time making a transition to truly healthy choices if they wanted to.
“Consumers REALLY do not know what they are getting. Potency has been increased through selective breeding and it is sometimes intentionally adulterated with chemicals. The so-called “medical marijuana” approaches 20% TCH. This is NOT the same product as the 1970s.”
Everything you say above is reefer madness. I obtain samples of Marijuana that contain over 25% THC *frequently*, not just “approaching 20%” – more THC is not dangerous than less THC, it simply means I use less than I otherwise would, which seems like a good thing when you’re inhaling smoke.
The idea that marijuana is more potent nowadays than it was in the 70s is a myth. The quality is more consistent, but ask any old pothead about the glory days of sativa strains and look at the twinkle they get in their eyes. The strains they remember had more psychoactive properties but for various reasons those strains are more difficult / less profitable to grow so you don’t see them around very much.
In the old days the weak weed you would get, the only kind you seem to think existed, was often dipped in byproducts from the manufacture of heroin – strong marijuana is quality marijuana, it is not something to be feared.
As for being “intentionally adulterated with chemicals” – see my reference to the bad stuff from the 70s, the kind you would claim is less dangerous because of lower THC levels. I know of *zero* dispensaries that are “intentionally adulterating” their product with chemicals (Portland Oregon here) and the lab testing that shows levels of THC sometimes over 25% would flag any garbage in my pot.
Your ignorance is pretty amazing on this subject and I could say the same for just about everyone else who’s chiming in. Quit spreading FUD on pot. It’s not just less harmful than alcohol, it’s arguably safer than aspirin or caffeine too.
I should also add…
Cannabis should not be criminalized. It should be safe and regulated (i.e., known composition and unadulterated).
And taxed VERY highly, to pay for the inevitable mental health mess it creates.
” Cannabis should not be criminalized”
Interesting, what other social behavior should be criminalized? I don’t like people smoking ciggs outside; or using cellphones anywhere I can hear them. These behaviors should be criminalized AND TAXED very highly.
“…It should be safe and regulated (i.e., known composition and unadulterated)…
Like tobacco! .. oh wait… :o/
“..And taxed VERY highly, to pay for the inevitable mental health mess it creates…”
Do you have any evidence it “creates a mental health mess” or do we just run w/ the assumption? Ok, How much of a mental health mess? Can you swag an estimated cost to remediate the “mess” sowe can codify another Tax program and engage a retooled Law Enforcement Bureaucracy? Lordy knows that will be a fantastic number of DEA, ATF, FBI and CIA that will have to seek gainful employment.
@optimader
Did you even READ my posting? Did you follow any of the links? Do you assume every peer-reviewed journal is a schill for big Pharma?
Obviously the “war on drugs” is a stunning failure but is a self-perpetuating entity like the military-industrial complex, the national security state, etc, etc.
Do you think having legal, safe and heavily taxed pot is a problem? Tax the hell out of it to pay for mental health and rehab, instead of this nonsense we now have.
“Did you even READ my posting?”
Yes I read your very interesting posts.
Can you explain how you would propose “regulating” a plant that’s cultivation, distribution and consumption are all presently codified as criminal behavior and subject to Federal prosecution?
(I feel) your thoughts on the matter are not, well, very well thought out.
Or do I misunderstand your logical thread?
Are you suggesting reversing all presently enacted criminal statutes regarding cultivation, distribution and consumption?
If that is the case, how do you propose enforcement of these new (civil?)Regulations you propose?
Good luck enforcing them applied to a weed that will happily grow on a railroad right-of away.
The big problem I have with normalising cannabis … you tacitly make it easier for …to self-medicate
Like with ethanol!
We should try making alcohol illegal at the Federal level, (I feel) that it will reduce psychotic behavior and addiction!…oh wait :o/
“…It was tragic to observe patients who attended the mental health charity I was involved with a decade or so ago rendered psychotic and pretty much unreachable because they had self medicated using cannabis, opioids or even prescription drugs…”
Clive, no doubt you are well intentioned but all the unsubstantiated claims you state should include the preamble “I feel”. How exactly do you know any patient(?) of the charity was rendered unreachable by self medication with ***? Did you know them before they “self medicated”?
Your statement implies equivalency between cannabis and opioids and prescription drugs. Is that your intent? Really?
BTW, take a crack at clarifying what is a liberal?
(Do you feel) this is a liberal vs (not)liberal issue?
Sorry but all the evidence I’ve seen concludes that cannabis carries a significant risk of being damaging to mental health. E.g.
http://www.thelancet.com/journals/lancet/article/PIIS0140673607611623/fulltext
(“Other Articles of Interest” linked to from the same page; this journal is well regarded for its independence and quality of published research, although drug companies do play with the results of trials. This is not about drug trials, however)
As for “this is a liberal issue”, generally one talks of “liberalising” drug laws and that was the context in which I used the word. What I was trying to convey was that I am not some rabit right-winger intent on criminalising everything in sight.
Well we know the Lancet would never shill for the pharma/medical industrial complex , but did you actually read the link you posted?
You have a “liberal?” interpretation of what the word evidence means.
“The uncertainty about whether cannabis causes psychosis is unlikely to be resolved by further longitudinal studies such as those reviewed here”
This has to be one of the most mealy mouthed examples of “evidence” I’ve read in a while.
Your comment really requires policy analysis at the country level. In the US context, it is our present system that is disgusting in its negligence of addressing mental health needs. Lack of national health insurance that covers emergency hospitalization, regular therapy, and prescription drugs is why people self medicate. It’s a money thing, not a marijuana thing. Just checking into the psychiatric ward of a hospital for a few days can incur tens of thousands of dollars in costs, never mind lifelong therapy and medication for chronic but otherwise stable conditions.
Self-medicating via marijuana is so low on the list of problems that raising it in a US context suggests either ignorance of the totality of the issues or purposeful misdirection away from the heart of the matter.
Also, your premise is flawed. You seem to think that prohibition renders marijuana difficult to obtain.
Also, in order to do a cost-benefit analysis, all costs and benefits should be considered. Even if one just restricts this to medical concerns, the benefits of marijuana for patients suffering pain and nauseousness, for example, outweigh the harms to the small subset of the population that may overdo self-medication.
Also, your lumping together of marijuana, opiods, and prescription drugs demonstrates a carelessness of unrelated issues that undermines the credibility you are trying to develop by talking about working in a mental health organization.
Finally, your argument only makes sense if you advocate the criminalization of all recreational drugs and the prescription model for all medical drugs, from alcohol to aspirin to Ritalin. That’s certainly a legitimate belief, but one which is an extremely tiny minority opinion. The vast majority of Americans are willing to accept that aspirin and alcohol kill people because their ‘over the counter’ availability is worth the public health costs.
P.S., if you know of mental health charities that provide affordable (ie, free) long-term therapy and prescription drugs for mental health illnesses, please post a comprehensive list. This would be an invaluable resource to millions of Americans, particularly one organized by geographic location (ie, if you are in Louisville, KY, go to organization X to get a Lamictal prescription written and the money to purchase it).
Exactly! We need to treat marijuana just like prescription drugs, and then there won’t be any problems with abuse or effective self-medicating.
Rasta Man Vibrashaaans
the prevalence of financial services firms in the U.S. has an adverse effect on youngsters, offering a “gateway drug” into more pernicious pathological states of materialism, obsessive greed, financial status anxiety and moral degeneration, which in turn can lead to criminal behavior and outright pathological pyschosis.
This is a public health threat as yet unrecognized by the National Institute of Health and other govermint organizations.
Pehaps cannabis coffee shops could be offered to the population as a form of therapy.
And in “circular reference watch”, the treatment centre I used to volunteer at was way, way, over over-represented in patients from the financial services industry. Most were poly-addicted (substance e.g. cocaine, behavioural e.g. gambling and compulsivity e.g. binge spending simultaneously).
Their lives were completely unmanageable by any sort of functional measure, most required 3 months of intensive professional help just to regain a semblance of being able to cope without their “supports” to get them over the “humps” of day-to-day living. Yet they were entrusted with the running of £1bn+ portfolios in some cases.
In a (very !) roundabout way, they depended on their addictions which depended on the pushing of debt addiction to newbie addicts as you describe above.
Cannabis fried me that’s for sure. Sometimes I got ahold of weird sh*t that made me paranoid as hell. Once I thought my left arm was on the right side of my body and my right arm was on the left side. After a while, I was afraid to smoke it.
Some dudes I knew just cruised on it, night and day, in a mellow fog. They seemed to function effortlessly. Me, I was a piece of toast after about 4 bong hits or a joint.
But alcohol always wasted my brain more than cannibis. I still remember sitting in the university library on a Sunday night, my brain blank as a test pattern from 4 or 5 nights of heavy partying. then I’d go back to the frat house and maybe have a few bong hits and watch TV.
I didn’t learn much in college. That’s why I had to go to Univeristy of Magonia when things got serious.
I am waiting for the Lancet study on the prevalence of individuals that brcome members of College Fraternities having psychotic episodes later in life.
Interpretation
The evidence is consistent with the view that College Fraternities increase risk of psychotic outcomes independently of confounding and transient intoxication effects, although evidence for affective outcomes is less strong. The uncertainty about whether College Fraternities causes psychosis is unlikely to be resolved by further longitudinal studies such as those reviewed here. However, we conclude that there is now sufficient evidence to warn young people that College Fraternities could increase their risk of developing a psychotic illness later in life.
You may replace College Fraternities with anything you don’t understand or are afraid of.
Interpretation:
Certainly the human populations reaction to most anything will be normally distributed from adverse to beneficial.
I’ve seen people freak out over what they read on the internet — but I’m not saying where! hahahaha. I wonder if there’s a double-blind test for that. If somebody throws money at it, I’m sure there will be.
Try the banana peels, they are potent this time of year.
whoa. pretty weird about your arms changing sides like that. made me remember tales of “dusted” pot in college. it had PCB, or maybe acid, or who knows what mixed in.
but even with normal pot paranoia can be a problem. like fear of a jail sentence, the fbi, cia or whoever is monitoring you, and the general feeling that authority is a danger to oneself.
but it wears off. doesn’t it?
Actually, it was probably PCP, aka Phencyclidine, a very potent warper of reality, whether snorted or smoked (usually w/MJ in a joint). In the day, it added “spice” to many a party. Almost as much fun as “unusual attitudes” training for a private pilot’s license. BTW, ingestion of any PCB, aka Polychlorinated biphenyl, via any method would probably prove fatal.
Been a long time. I did mean PCP (also called horse tranquilizer, I think – we had an ag school too).
Ya, PCB very bad. We used it for large transformer coolant in the very olden days. Then throw them away in the water supply.
The last couple of years I’ve had to deal with intense home care (by me) and numerous hospitalizations of a couple of close family members, including one death. If it weren’t for cannabis, I’d probably have had a stroke or a nervous breakdown from the stress. It may have saved my life. (It also cured my hives, without the side effects of prednisone.)
I’ve used it off and on since I was a teenager, now I’m middle aged. Why would I even want to quit? It’s waaaay safer than self medicating with alcohol.
Clearly you are mentally ill and have an addictive personality..
Haha. Clearly.
My stars; this is like an academic version of ‘Reefer Madness’. Even the conservative Rand Drug Policy Research Center found that the gatewway drug for teens and hard drugs was alcohol. Their initial findings were even less damning of cannabis, so they…tweaked them a bit.
Those of you so high on BigPharma for mental illness must not be very aware of the difficulites finding and regulating the dosages for *what works*, nor the agonies of the downsides of the ‘medications’.
Totalitarianism lurks under a thin veneer of misguided good intentions.
Speaking only for myself, my scorn for BigPharma is pretty much unmatched in its vociferousness. Being anti-cannabis general availability does, however, not make you pro BigPharma.
I must be overlooking the third alternative?
BTW
“…Being anti-cannabis general availability…”
Clive, if (the consequences of) general availability is your angst about cannabis, I have some distressing Breaking News for you.
In a history do over, I wish GWB had a steady supply when he was POTUS, (I feel) that may have been preferable to the decisions of an agitated alcohol addict.
All this talk of gateway drugs and no one mentions tobacco.
>
this leads back to that age old question : will it be modern madness or reefer madness?
http://acmeartscollective.com/mlaw/2013/09/23/will-it-be-modern-madness-or-reffer-madness/
That article is simply brilliant! Thank you very much for providing that link!
Ahhhhhh, marijuana is a gateway drug!
Quick, lock up all the poors and coloreds!
All of the studies start from the idea that cannabis is bad. But so far, almost all scientific and anecdotal evidence points to an incredible amount of positive benefits and very few if any real negative side effects. Considering the damage that tobacco and alcohol have done to human society, it is laughable how we keep seeing studies talking about the dangers of marijuana.
And did anyone else notice on those charts, how the closer you lived to a coffee shop, the less likely you were to smoke cigarettes?
So let’s reframe the study: Easy access to cannabis helps cut down on tobacco usage.
The argument is being won by the masses, and the least likely to change their opinions are elderly. The issue is marijuana is relatively easy to grow, and here is the key point, the supply necessary to placate the demand is small.
What this means is without prescription pricing, I don’t think dispensaries can stay in business in much of the country. Pot will just be grown in yards or available at community markets because one doesn’t need to much of it.
The primary cost of pot is the police can arrest you for having it. Marijuana prohibition pays for the drug war, the prison industry, much of local police forces, and the politicians who benefit.
The issue is what politicians collect funds by tossing people in jail. Obama and Clinton have launched massive crackdowns on drugs which routinely sweep up marijuana users. Diane Feinstein is a major recipient of donations from the private prison industry despite representing that “liberal haven” of California. I bet she gets a host of celebrities who support marijuana legalization and use pot in the open to give her money.