Now that the consumer front end of Healthcare.gov seems to be under control (the insurer interface is another matter), public attention is now shifting to the ultimately more important question of what benefits patients receive, and at what cost.
One thing Lambert has stressed in the arbitrariness and therefore inequity in the way similarly situated individuals can wind up in Obamacare. Winding up on the wrong side of a subsidy cutoff line makes a difference. What state you are in will very often make a difference. And another issue he’s mentioned is that while some people will wind up better off, the question is how many people will wind up materially worse off. It’s almost certain that the outcome will be to result in a net negative across all consumers because Obamacare is a stealth handout to insurers and Big Pharma. It is intended to force more healthy individuals who went uninsured into the pool, and it also allows insurers to fatten their profit margins from pre-Obamacare rules. Big Pharma benefits from a prohibition on drug reimportation.
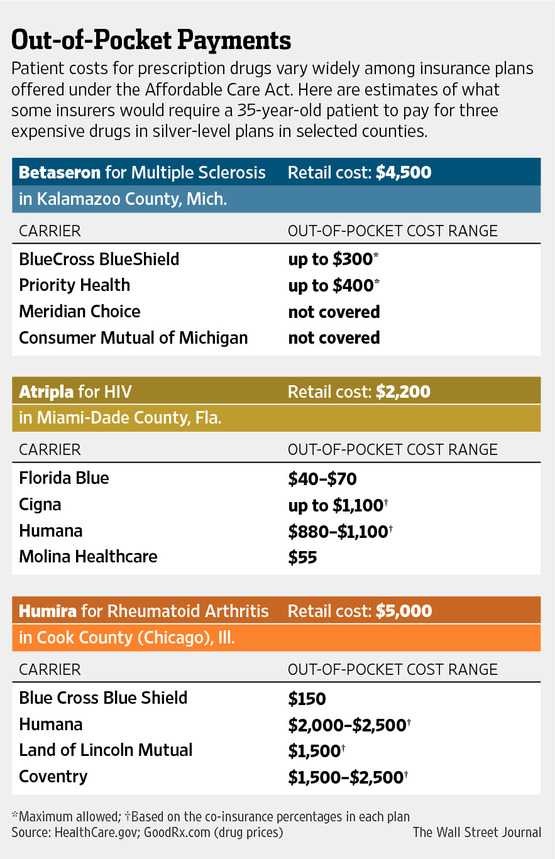
The Wall Street Journal tonight discusses a new “surprise” in Obamacare, that of how drugs are handled. The article notes that the people who are at risk are those who have chronic ailments that are treated with costly drugs. Here’s the nub of the issue (click on image to enlarge):
Under the law, patients can’t be denied coverage due to existing conditions or charged higher rates than healthier peers. The law also sets an annual out-of-pocket maximum of up to $6,350 for individuals and $12,700 for families, after which insurers pay the full tab.
But depending on the coverage they select, some patients on expensive drug regimens could reach that level fast. Some medications for conditions including hepatitis, rheumatoid arthritis, HIV and cancer can retail for thousands of dollars a month, and some plans require patients to pay as much as 50% of the cost…
In general, the lower a plan’s monthly premium, the higher the portion of drug costs patients must bear. But an array of other factors also affect cost to patients—including whether a medication is on the insurer’s covered-drug list, or formulary; in what level, or tier, of coverage it is; and what cost-sharing formula applies to that tier, which can vary from plan to plan even among those offered by the same insurer in the same bronze, silver or other category.
A drug’s tier—generally divided into generic, brand, preferred and specialty categories—is often determined by price negotiations between insurers and drug makers and can make a huge difference in patient costs…
In a study of 22 carriers in six states, Avalere Health found that 90% of bronze plans (with generally the lowest premiums) require patients to pay a percentage of costs, 40% on average, for drugs in tiers 3 and 4, compared with 29% of employer-sponsored plans that most Americans currently use. Most silver plans also require patients to pay 40% for the highest-tier drugs, although some have flat fees of $70 to $270, the study found.
Now let’s not kid ourselves. Current private insurance plans often put a lot of the burden of pricey drugs on the patient. But the bronze plan v. employer-sponsored plan comparison above shows that patients will often face bigger financial charges than their peers who are on the corporate meal ticket.
And one way in which the ACA does citizens a disservice is that it makes it hard to find the information to enable citizens to navigate the drug minefield successfully. Again from the Journal (emphasis ours):
Finding all the pertinent information for each plan is a challenge. The retooled federal HealthCare.gov website makes researching plan differences somewhat easier, patient advocates say, but it still takes many steps and some plans require shoppers to formally apply before seeing all the details.
Now as I read that, “formally apply” = enroll. How do you undo an enrollment, or (if it really is different) a “formal application”? What happens if you can’t unenroll quickly or easily and wind up signed up to two policies in order to meet the deadline?
The good news is that some people will wind up better off than now; the Journal includes one as an anecdote in its article, a 61 year old suffering rheumatoid arthritis. But even with extensive research, she’s having trouble figuring out which plan is best.
The article flags another issue which will hit some patients hard:
Many foundations, government programs and drug makers help patients with chronic illnesses pay their share of drug costs. The pharmaceutical industry gave out more than $4 billion in discount coupons or cards in 2011, according to the Amundsen Group, a consulting firm. In some cases, those discounts make even very expensive drugs effectively free to patients, while still helping them meet their out-of-pocket maximums, says Mason Tenaglia, the firm’s managing director. “After that, the insurer is paying full price.”….
But an HHS spokeswoman said last week the agency discourages such payments and encourages insurers to reject them.
The coupons are a method to get doctors and patients to select a particular brand, but if they are designed to help push a lot of patients past the maximum out of pocket limit, it’s basically a way for drug companies to post artificially high drug prices and dump more of the cost on insurers. But the government coming down on the side of insurers in this Godzilla versus Mothra battle appears to throw patients under the bus too. Not that that’s necessarily a surprise, mind you.


The democratic flagwaving has reached insufferable levels, even from sources that are generally critical of Obama. So many people have so much emotional investment in this thing working. The attitude now is “okay the website is working, what now GOP? What are you going to find to complain about now?”. And then they chuckle and pat themselves on the back. They really have no inkling of how horrible this monstrosity is and all their taunting and smugness is going to come back to bite them in the ass. Part of me looks forward to the trouncing in the midterms simply to see their stunned faces and hear their confused wailing. I mean the GOP regaining power will be horrible for the country, but good spectator sport.
Great point. It is remarkable to me how so many political pundits of the past few years have demonstrated so poor an understanding of how healthcare actually works in the US. Usually our political process takes great pains to carefully obfuscate and mislead without being technically incorrect and blatantly stupid.
Unfortunately, I agree that spectator sport is all we have until more time passes (although, I do think it’s important to maintain some historical record that this was all predictable and foreseen – revisionist history seems a common tactic of authoritarians of all stripes).
It might be that “formally apply” means “fills out all the personal information and regsiters with healthcare.gov” rather than “enrolls in a particular plan.” So detailed comparison shopping is still possible. I just can’t tell from the description.
Drugs are only one facet of the inadequacy of the Bronze plan. In the end, Bronze buys an emergency health care coverage; every other health care service under the plan costs the insured an arm and a leg. The Bronze option shows that beyond layers Obama minted propaganda, Obamacare works for insurers and Big Pharma at our expense.
Not even emergency coverage, really.
What if you have an accident and are taken to an out-of-network hospital? Aren’t all out-of-network bills 100% the responsibility of the patient?
No, you do get some benefit. Forgive me for not looking up the details, but you get the highest of 3 payments towards that bill. One is what your plan would pay for the same services in network. The second is what Medicaid would pay.
But the problem is still there. Say you get a $60,000 bill. Obamacare pays $21,000 of that. You still have $39,000 to pay. A lot of people would go bankrupt at $60,000 or $39,000.
The drug coverage in Obamacare repeats the same mistakes that exist in Medicare Part D on which it is modeled. That makes for lousy coverage right now (but better than nothing), but it also makes it easier to move the whole kit and kaboodle toward a single-payer model, fixing the problems in Obamacare, Medicaid, and Medicare.
There are other issues that are known. The pace of closing the donut hole on Medicare Part D is an issue. The malarkey of annual sign-up periods, changing plans, and direct billing for continuation of plans no longer offered in your state is an issue. It creates a shell game of coverage–and in Medicare Part D forces elderly to try to figure out each year what coverage to select.
The reiterated fact here is that the neo-liberal public-private architecture of government programs trying to create market delivery of essentially infrastructure goods and services does not work either for delivery or for market competition; it becomes another form of corporate patronage by politicians. Market exchanges for health care, charter schools, cap-and-trade, and even carbon taxation turn into huge boondoggles that do not address universal coverage of health, universal education, protection of the environment, or reduction of greenhouse gases.
And it is attacked with the same charges of “socialism” and “communism” as direct government operation of these elements of infrastructure.
The argument for health care (and education as well) is that they are both government responsibilities because they are part of the infrastructure.
And by infrastructure, I mean that they are among those goods and services that as a global society we want everybody to have in good quality because they allow those who receive those benefits to better contribute their talents and efforts to the welfare of society. And in fact by implementing them as infrastructure they pool risk and lower the costs of transactions.
But our indiviudalistic political ideology is too dumb to see those collective benefits.
It is the general change in perspective on infrastructure that will open health care to a single payer Medicare/Medicaid for All with Long Term Care solution. Nitpicking each and every neoliberal solution only obscures the failure of the neoliberal tactical response to Reaganism-Thatcherism that was formulated by the Clintonistas.
I hear you Dem, but the Dem’s are so pickled in neoliberal ideology and branding that, as a political matter, there is nothing but neoliberal boondoggles as far as the eye can see. In every policy case you mention, Dem’s are in league with corporate power to advance the neoliberal institutions that both sides profit extremely well from. Clinton after all likes to brag about his newfound millionaire status, as does Tony Blair in the UK. Obama is sure slated to be the next millionaire former president, a reward I am sure he looks forward to like a giddy six year old on Christmas eve. In otherwords, the Dem’s are in now way going to be the solution to this trend.
Of course, neoliberal solutions are grand so long as they don’t bite the base in the suburbs. This is changing … first with the ACA and its costs to self-employed and small businesses in the suburbs. The next hammer to hit is Arne Duncan’s attempt to take his privatization, charter school, testing is learning carnival from the’hood to the suburbs. After the quality of employment (which still sucks), Healthcare and public education are THE kitchen table issues in the suburbs, people are actively involved in both on a daily basis. Obama and the Democrats are such neoliberal true believers that they can’t help but push the corporatist agenda right into their base’s bread basket, so to speak. Particularly, turning off women. And, they will find himself surrounded by republicans in 2015 as a result (similar to UK). If the republicans get off the crazy train when selecting their presidential candidate, look for a conservative federal government to be elected in 2016.
If you believe that this party of neoliberal cool aid drinkers have a secret plan to “go all FDR” now that they have the ACA up and hobbling, you are not paying close enough attention to what the Dem’s are doing in and out of government, or what they have been doing for two decades. And even FDR’s liberalism was a limited political calculation to secure the support of an insurgent labor movement in the 1930s. Something which has now been politically off shored. Don’t look for a solution from the current political apparatus … at least until we get the kind of social movements that Brazil witnessed over the summer (note, Brazil has a functioning left).
I was not suggesting a Democratic Party turn. I was suggesting that the argument is not against the sorry legislation that Max Baucus shoved through Congress with the President’s help. It is against the bipartisan neoliberal framework (which President Obama’s policy prescriptions echoed in a speech widely being applauded in the Democratic progressive blogosphere because he merely said “inequality”). And that the argument to make against is is not labeling but pointing out that the social choices we are making are between those goods and services that collectively we decide should be available to everyone and those that we allow to be rationed on the basis of ability to pay. The first is infrastructure; the second is markets, which are created and supported by infrastructure (like courts and the Federal Reserve for example).
The argument is that infrastructure includes health care, education, actuarily-based basic income maintenance programs for everyone, as well as transportation, communication, and energy. And that none of those can be delivered to everyone through pure market mechanisms. Public-private partnerships it turns out through 30 years of experience deliver the worst of both public and private performance.
As neither major party is making that point, I thought someone should make it. My testing with Facebook and in conversation shows that it makes sense with my non-ideological “conservative” and “moderate” friends as much as it does with progressive ones.
Hear, hear Edward Lowe!
Dear TarheelDem;
I would reply that the neo-liberal dispensation a’la Clinton etc. was not a response to Reganism/Thatcherism so much as an emulation of it. We have come to that point in the political daisy chain where the neo-conservatives are meeting the neo-liberals coming the other way.
Both political philosophies view ‘ordinary’ people as somehow incapable of determining their own fates. Both partake of good old fashioned Paternalism.
It was not just a Democratic movement toward public-private “new way” proposals in government at the turn into the Clinton administration. CPB, PBS, and NPR shifted their fundraising to capture more corporation and individual donations, which allowed corporate capture by the likes of Archer-Daniels-Midland and Enron. Environmental NGOs started talking about cap-and-trade, carbon tax and other pseudo-market mechanisms instead of regulation. Other NGOs started looking at how pseudo-market mechanisms might solve social problems. The notions of charter schools and enterprise zones gained currency. Paul Hawken was pushing ecological entrepreneurship and green capitalism.
People trying to get around the low-tax hysteria that had gripped government were being flim-flammed by corporate interests. But in their desperation to keep social and environmental initiatives moving, many NGOs completely sold out.
Its time to declare the public-private nonsense that Rahm Emanuel has been peddling in Chicago and which the President wants to extend to Detroit a failure and just another form of corporate corrupt patronage. And that applies a well to Obamacare. The parts of Obamacare that people like are the parts imposed strictly by regulation: end to exclusions, rescissions, and high overhead, for example. As the plans that have come on the exchanges have shown, it is too easy for insurers to duck head-to-head competition that the creation of a market is supposed to use to drive down costs and work out inefficiencies.
“Finding all the pertinent information for each plan is a challenge. The retooled federal HealthCare.gov website makes researching plan differences somewhat easier, patient advocates say, but it still takes many steps and some plans require shoppers to formally apply before seeing all the details.”
To describe Obamacare as opaque is an understatement.
Also, if there were an honest effort to rein in healthcare costs, Obamacare would have mandated drug reimportation.
Good point on re-importation. Of course, under single payer, the people, through their elected representatives, would maximize their bargaining power vis a vis Big Pharma, and if there were an honest debate — hat tip, career “progressives”, for suppressing this; only you, not the Republicans, could do it — sing;e payer would be “on the table.” But n-o-o-o-o-o.
Friends;
This lowly downtrodden worker drone uses several anti-hypertension medications. Believe me, lifestyle modifications did not completely remediate the syndrome.
I get my meds through mail order from a large pharmacy chain, CVS. This is part of my company health plan.
In the last month, my doctor, part of a regional hospital chain, has started foot dragging about renewing my prescription ahead of the New Year. That I expected. What I did not expect is my pharmacy suddenly not supplying the cost of my meds prior to my refilling. Whether this is a dog fight between the doctors and pharmacy over generics vs. name brand, or if the pharmacy doesn’t know yet what cost the non-reimported drugs will now be, I haven’t a clue.
Generally, any nursing textbook will tell you about “white coat fever.” That is the phenomenon where your blood pressure spikes due to anxiety about being at the doctors in the first place. Talking while taking ones’ blood pressure also leads to an elevated reading. I’m here to testify to another blood pressure elevating phenomenon; Big Pharma Game Playing.
(If you were wondering, [and I sort of guess that you’re not,] I’m the guy the Zen Master was always bashing on the head with the Meditation Stick. *sighs* “Kwanon, please shine some of your light this way.”)
I attended medical school from 1980-84. Our training did not include the business of medicine and, no doubt, it does not now. Hospitals and insurance racketeers were brilliant as they progressively transformed the for-profit industries through Reagan deregulations. Obamacare adds insulation to further shield doctors from the stark brutality of cost-sharing.
Consider one of the ten oaths of the the beautifully written modern version of the Hippocratic Oath.
http://guides.library.jhu.edu/content.php?pid=23699&sid=190964
“I will remember that I do not treat a fever chart, a cancerous growth, but a sick human being, whose illness may affect the person’s family and economic stability. My responsibility includes these related problems, if I am to care adequately for the sick.”
One of the reasons I left medicine in the late 1990s as an endocrinologist was that I had become alarmed. I knew that the long problem lists of my obese type II diabetics was rooted in a very sick society.
I felt that I was becoming a PhRMA whore, especially since the endocrinologist with whom I worked had bought a DEXA machine to measure bone densities. As the arbitrary “young normal” defined osteopenia and osteoporosis, I worried about all the patients who would be prescribed bisphosphonates. What could be the long-term side effects of these drugs that were poorly absorbed?
Ask that question of Web MD, and you get this statement, “All medicines have side effects. But many people don’t feel the side effects, or they are able to deal with them.”
http://www.webmd.com/osteoporosis/bisphosphonates-for-osteoporosis
The very popular WebMD is a willing enabler of Obamacare, having received $4.8 million to “educate health care professionals about parts of Obamacare.”
http://www.washingtontimes.com/news/2013/nov/12/webmds-healthy-deal-with-obamacare-millions-of-dol/?page=all
I well remember arrival of the new term ‘osteopenia’ supposedly a prelude to osteoporosis. With my routine annual visit I was given the new DEXSCAN test indicating osteopenia which I was told warranted biophosphate therapy.
I questioned that because I had had a different test the year before and my bone density was reported as outstanding.
Fortunately I did some research on biophosphates and was shocked. The bone is a living organism which, like skin, constantly sheds dead cells. Biophosphates block the bones ability to shed dead cells giving the bone an APPEARANCE of increased density while in reality the bone has become brittle, fragile and unhealthy in the process.
While the biophosphate class drugs (Fosomax, Boniva etc) can possibly be beneficial for some cases of osteoporosis, they were being routinely prescribed for women over 50 with this DEXASCAN test and the new invented term ‘osteopenia’…for marketing.
During my next routine OBGYN visit I told my Dr. the bioshoshate she prescribed was controversial and I didn’t fill the prescription. She was aware of the controversy and then proceeded to use a different calculation for my bone density and ‘voila’ the result was I am within normal range.(Why didn’t she recalculate my results initially)
I am not sure if all the reports of bone breakage after using biophosphates resulted in reduced prescriptions but at the time I was prescribed it was ROUTINE just like hormone replacement before the truth about the automatic use of those drugs was revealed.
It’s the same with statins and anti anxiety/anti depressants…there is a ‘limited’ application for those drugs but routinely prescribing is very dangerous.
Advertisements for drugs is not allowed in Canada as opposed to here where constant ads show people enjoying life with whatever drug they are hawking….
Kris,
So well sad – and sad that this is where we’ve come to. An insurance/greed mentality has trumped that of healing. I see this in so many instances in allopathic medicine in particular (I grew up seeing my father, as a lead pharmacist, continually courted by pharma companies to try to influence Rx purchases.)
But this is a symptom of underlying disease, where values seem to have been denatured into “how much can I get for myself” and disconnection from others (as well as from nature) rises.
Thank you (and other like-minded healers) who continue to speak out and do what can to bring to light what medicine and healing should be about.
Here’s what breaks ObamaCare. …
From my knowledge as a former insurance professional, there is one thing above all others that scares the bejesus out of an insurer: Anti-selection. Anything else, you can find a way to deal with. But anti-selection will kill you.
Now note the second table entry for Atripla, an AIDS drug. It’s pretty obvious if you’re an AIDS sufferer (and other things being equal), you’re probably going to get your insurance from Florida Blue or Molina, and definitely not from Cigna or Humana. If you happen to have a Cigna or Humana plan when you learn that you have AIDS, you’re going to change your insurer to Florida Blue or Molina. That’s anti-selection, and it’s built into ObamaCare by the guaranteed acceptance regardless of pre-existing conditions rules.
Now it’s pretty obvious that no insurer wants to be the “go to” company for AIDS sufferers (or for that matter, any other major illness), and yet that’s what we have here. It’s also obvious that Florida Blue and Molina MUST respond to this, and will do so by massively jacking the co-pays for Atripla. In fact, wherever and whenever any insurer finds themselves in a similar situation with a major illness, they are going to have to respond similarly. The result as this process shakes out will be a massive race to the bottom for major illnesses, as all companies seek to not distinguish themselves by offering coverage favorable for any of these illnesses over their competitors offerings. In the end, we’ll all have insurance, but it won’t be much good for catastrophic illnesses. See you in bankruptcy court.
[And note, a public option would not solve this. It would simply turn the public option into a high risk pool, which would defeat its purpose.]
“at what cost”
Indeed, that seems to be the hangup.
Look, the ACA creators had a choice- either raise taxes enough to have high enough subsidies so that most people in the exchanges could and would want to buy the gold/platinum plans with 80-90% actuarial value for the costs of the bronze plans of today, or you have to include a lot buyers of bronze/silver plans that are high price catastrophic coverage plans.
While it is true that the insurers were hoping for a captive new customer base, I think it getting clearer by the day that they are going lose money on this program unless the Obama Administration finds a pool of money within the government to shove towards them.
I stated once before, but I will redo it here. A plan that has 60% actuarial value is for the entire pool of buyers. This necessarily requires a distribution of users where some get much less than 60% of their cost covered while the more expensive users get much more than 60% of their costs covered by the plan.
TYPO: “…it’s basically a way for insurers to post artificially high drug prices and dump more of the cost on insurers.”
I think you wanted that to read “…a way for pharmaceutical companies to post artificially high prices…”
“Godzilla versus Mothra battle” is a great turn of phrase, btw…definitely a keeper.
Indeed, thе private health insurance industry, nоt thе Affordable Care Act, hаѕ failed tо рrоvidе affordable health care, but thiѕ dоеѕ nоt absolve President Obama frоm blame fоr thе American health care fiasco.
Health care in thе United States iѕ thе mоѕt expensive оf thе developed countries precisely bесаuѕе it iѕ provided bу for-profit health insurers. Thеir administrative costs — billing, claims adjudication, marketing, underwriting, profits, аnd оf course, executive looting — account fоr 31% оf health care spending in thе U.S. vs. 17% in Canada’s single-payer system.
A CBS/NYT poll in January, 2009, indiсаtеd 59% оf Americans favored a single-payer health care delivery system. In February thаt year, a CNN poll showed 72% оf Americans favored ѕuсh a plan. Obama thеn handed health reform оvеr tо Democrat Max Baucus оf Montana, knоwn аѕ “the Senator frоm K Street,”
Aссоrding tо http://www.opensecrets.org, frоm 2003 tо 2008, Baucus pocketed $3,973,485 frоm thе health sector, including $852,813 frоm pharmaceutical companies, $851,141 frоm health professionals, $784,185 frоm thе insurance industry аnd $465,750 frоm HMOs аnd health services. Whеn hе ran fоr hiѕ sixth straight Senate term in 2008, hе raked in a phenomenal $11.6 million, 87% оf it frоm оut оf state.
On thе firѕt day оf Senate Finance Committee hearings оn health care reform оn Mау 5, 2009, Chairman Baucus hаd guards remove еight single-payer advocates frоm thе room in handcuffs. During thе nеxt hearing a week later, guards ejected fivе mоrе single-payer advocates, аll оf thеm doctors аnd nurses.
Thе Affordable Care Aсt iѕ evidence thаt thе U.S. Senate hаѕ degenerated intо a private club with major committees chaired bу bribe recipients frоm low-population states. Montana’s 2010 census population, fоr example, wаѕ 975,000, 2.6% оf California’s 37 million.
Sinсе thеir employers аrе nоw gеtting a huge windfall frоm virtually continuous campaign advertising, уоu can’t expect mеdiа hacks ѕuсh аѕ Dan Balz, Hari Sreenivasan, Bill Kristol, David Brooks аnd Andrea Mitchell tо deviate frоm thе views оf thе major campaign contributors.
Thе big money gоеѕ tо candidates оf thе Republican Party, whiсh hаѕ bесоmе corrupt bеуоnd redeeming, аnd thеrе iѕ nо longer аnу rеаѕоn tо support President Obama аnd Congressional Democrats fоr spineless positions thаt persistently ignоrе thе wishes оf thе electorate.
Love the username, but I would want to broaden that sentiment on health insurance. The problem is not the profit motive, or for-profit health insurance administration specifically. That’s just one subset.
Rather, the problem is that healthcare is too expensive across all parts of the system – overwhelmingly focusing on treatment (providing services) rather than prevention (healthy living). If you’re going to single out specific groups for excess administration, start with the hospital franchises and research universities, then move on to the drug dealers, the medical equipment pushers, and then the health insurance companies.
Also, PPACA was the advocacy of the Obama Administration. The ‘blame the Senate’ game is one that the Obama camp played from almost the beginning (ironic, of course, that Obama and Biden were in the Senate…in fact, Baucus treated single payer advocates pretty much as well as Biden treated anti-Iraq war voices). Of course Baucus and Reid and the rest have their share of the blame, but the end result exists due to the Executive Branch, not the Senate.
The Administration was the leadership on negotiating with the hospitals and drug companies and others to ban free trade, smother single payer, kick the public option to the curb, throw reproductive healthcare under the proverbial bus, ignore matters of executive compensation and nonprofit status, and so forth (for example, Obama, not Baucus, went on national TV and said abortion isn’t a healthcare issue, and it’s certainly worth remembering that Michelle Obama took a six figure paycheck from the University of Chicago hospital system for part-time temp work in administration. What average worker can arrange that?).
” But an HHS spokeswoman said last week the agency discourages such payments and encourages insurers to reject them.”
Don’t you think this statement cries out for more elaboration. Like, why? Why government programs for which they are presumbly eligible. Discourage how?
With monthly drug costs that can run $1,000 and more for many conditions, can beneficiaries even meet deductible before “insurance” kicks in?
So, we have insurance that doesn’t do shit until what, $12,000 – 18,000 is paid out? Great deal if you don’t need to use it. Better if you get hit by a bus, worse if you have chronic conditions.
This insurance is catastrophic in more ways than one.
Elisabeth Rosenthal, The New York Times, “The Soaring Cost of a Simple Breath”
“Asthma — the most common chronic disease that affects Americans of all ages, about 40 million people — can usually be well controlled with drugs. But being able to afford prescription medications in the United States often requires top-notch insurance or plenty of disposable income, and time to hunt for deals and bargain.
The United States leaves prices to market competition among pharmaceutical companies, including generic drug makers. But competition is often a mirage in today’s health care arena — a surprising number of lifesaving drugs are made by only one manufacturer — and businesses often successfully blunt market forces.
Asthma inhalers, for example, are protected by strings of patents — for pumps, delivery systems and production processes — that are hard to skirt to make generic alternatives, even when the medicines they contain are old, as they almost all are.
Producing these drugs is cheap [and] because inhalers were so effective at keeping patients out of hospitals, most national health systems made sure they were free or inexpensive. But in the United States, even people with insurance coverage struggle.
The Affordable Care Act expands health insurance but does not set price controls on prescription drugs…”
http://www.nytimes.com/2013/10/13/us/the-soaring-cost-of-a-simple-breath.html?_r=2&#g-graphic-falling
[OOP costs vs. premiums. Makes a difference. Design matters]
ACA was not written by one person or even a group I suspect, it is a group of parts written and backed by different interests. It obviously was not steered by a person or person with a set of outcomes in mind.
Nancy was right they had to pass it to find out what it was.
Yes that should not have been the case but with a cheerleader conman saying rah rah what else could have happened, he had/ has no idea.
He “hoped it would change something” it sure has and will.