Yves here. It seems quite remarkable that none of these economists seem able to acknowledge that the rise in the pain medication prescriptions for people at the lower end of the educational spectrum might be due in part, and perhaps in large measure, to workplace-related factors, as in limits on hours and stipulations on work conditions. For instance, even though one of my brothers is still in a union shop and does desk work, the mill’s regular schedule is now 12 hour shifts. That would have been inconceivable in the days of greater labor bargaining power. It is hard enough to do a job that requires you to be on your feet for eight hours. Imagine the greater stress and risk at 12 hours. And then imagine how that interacts with the fact that overweight and obesity are far more common than they were 30 years ago.
By Silvia Merler, an Affiliate Fellow at Bruegel and previously an Economic Analyst in DG Economic and Financial Affairs of the European Commission. Originally published at Bruegel
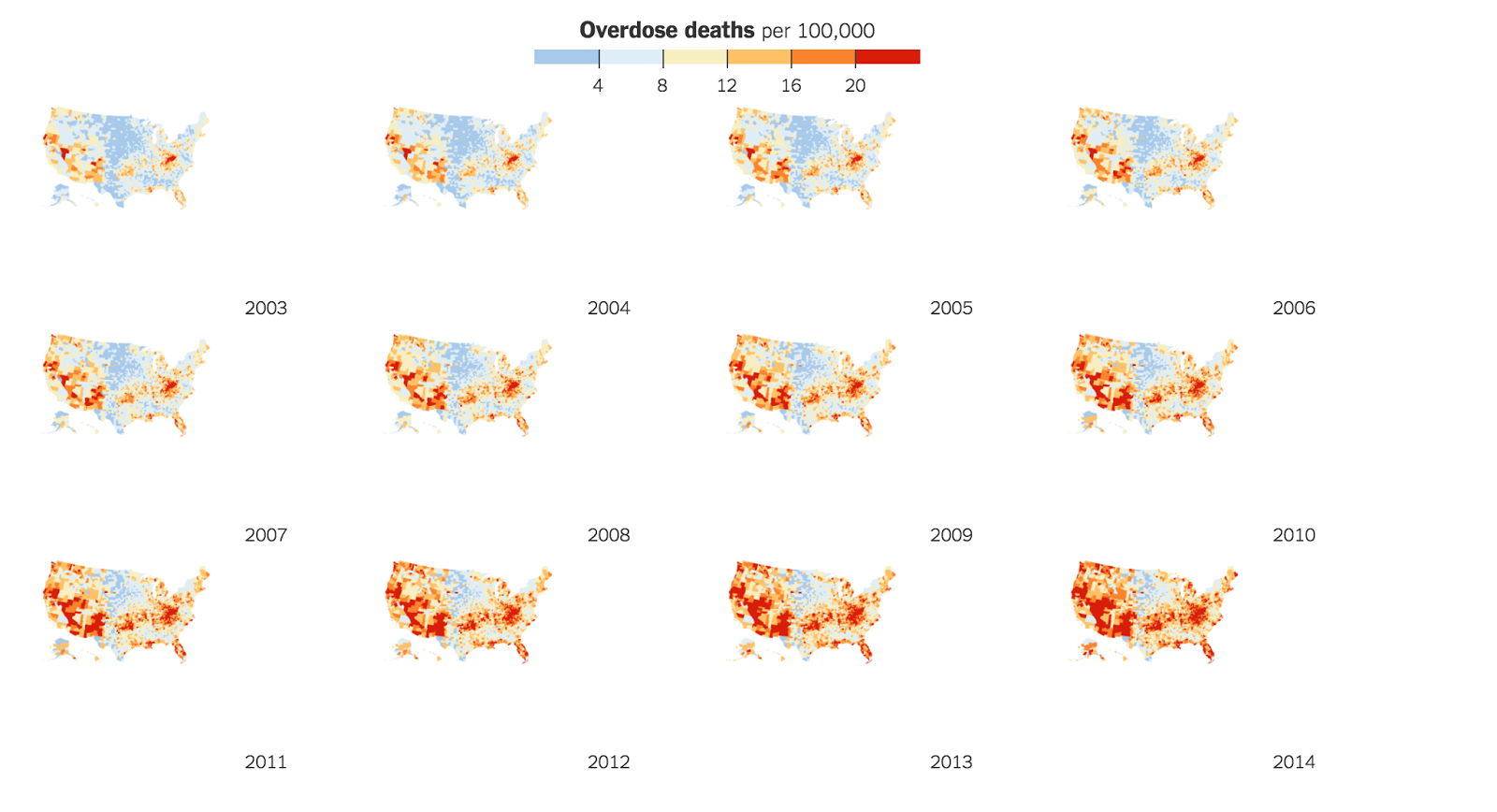
According to the Centers for Disease Control and Prevention, 91 Americans die every day from an opioid overdose. From 2000 to 2015, more than half a million people died from drug overdoses. Overdoses from prescription opioids are a driving force: since 1999, the amount of prescription opioids sold in the U.S. nearly quadrupled, and deaths from prescription opioids – drugs like oxycodone, hydrocodone, and methadone – have more than quadrupled. Some of the largest concentrations of overdose deaths were in Appalachia and the Southwest (Figure 1), with West Virginia, New Mexico, New Hampshire, Kentucky and Ohio being top-5 States. CNN has a historical overview of how opioids turned from “wonder drug” to abuse epidemics.
Source: The New York Times
This trend may be connected to another disquieting statistics. In 2015 Princeton’s Anne Case and Angus Deaton documented a 21st century rise in the proportion of white non-Hispanic Americans dying in middle age. While midlife increases in suicides and drug poisonings had been previously noted – they argue – the fact that these upward trends were persistent and large enough to drive up all-cause midlife mortality was overlooked. Case and Deaton argue that concurrent declines in self-reported health, mental health, and ability to work, increased reports of pain, and deteriorating measures of liver function all pointed to increasing midlife distress.
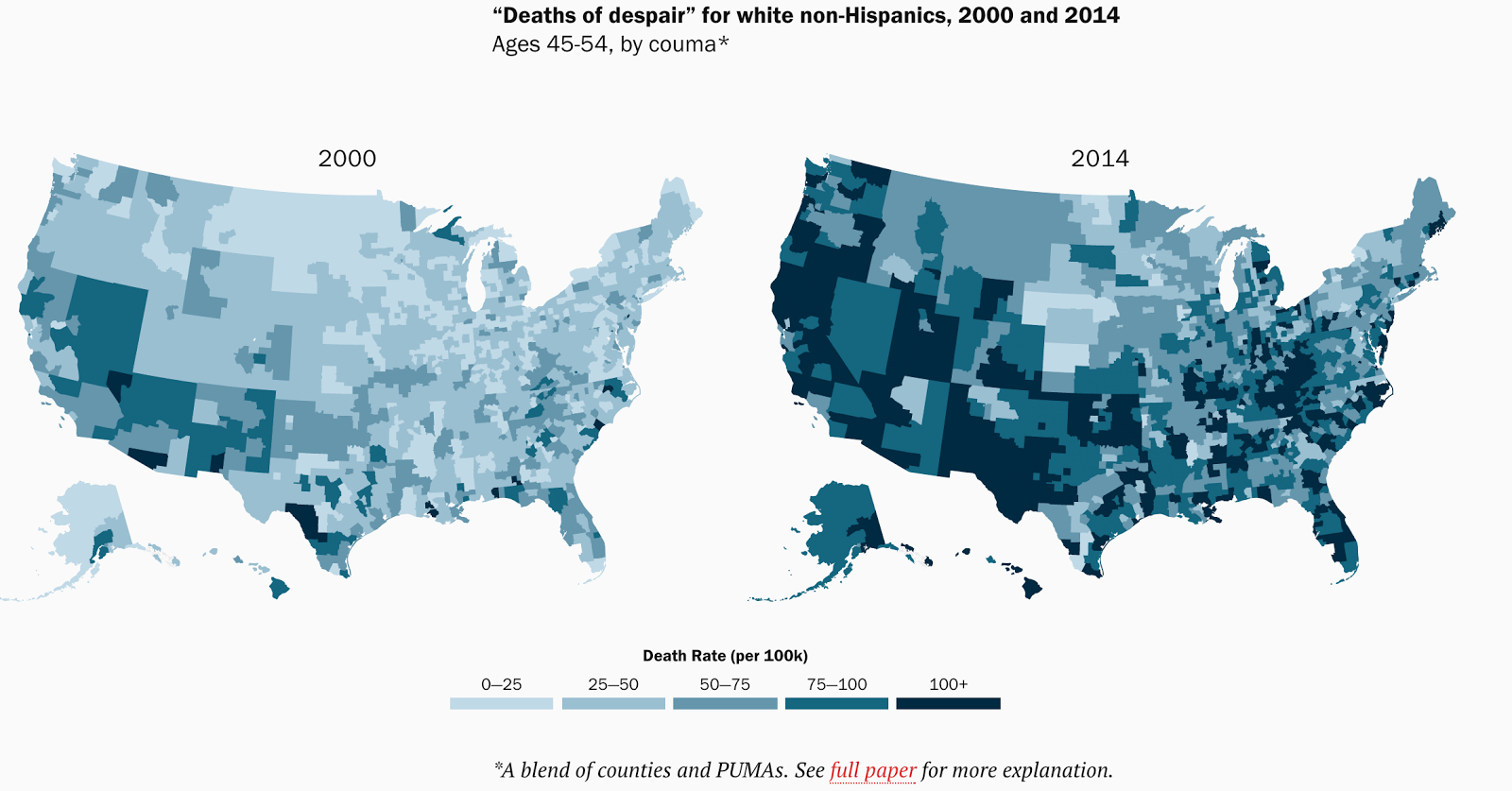
In 2017, Case and Deaton are following up on the same topic, in a Brookings Paper on Economic Activity. Dividing the country into 1,000-plus regions, they find that the rate of “deaths of despair” (deaths by drugs, alcohol, and suicide) in midlife for white non-Hispanics rose in nearly every part of the country and at every level of urbanisation – from deep rural areas to large central cities – hitting men and women similarly. In 2000, the epidemic was centered in the southwest, today it’s country-wide (Figure 2). The increases in “deaths of despair” are accompanied by a measurable deterioration in economic and social well being, which has become more pronounced for each successive birth cohort.
The opioid epidemic is also central to recent political events. Shannon Monnat at Penn State University examines the relationship between county-level rates of mortality from drugs, alcohol and suicide (2006-2014) and voting patterns in the 2016 Presidential election. She finds that Trump over-performed the most in counties with the highest drug, alcohol and suicide mortality rates, and that much of this relationship is accounted for by economic distress and the proportion of working-class residents. Many of the counties with high mortality rates where Trump did the best have also experienced significant employment losses in manufacturing over the past several decades.
Possible economic drivers of the opioid epidemics
Hollingsworth, Ruhm and Simon have a NBER paper on macroeconomic conditions and opioid abuse. They examine how deaths and emergency department (ED) visits related to use of opioids and other drugs vary with macroeconomic conditions. They find that as the county unemployment rate increases by one percentage point, the opioid death rate per 100,000 rises by 0.19 (3.6%) and the opioid overdose ED visit rate per 100,000 increases by 0.95 (7.0%). Macroeconomic shocks also increase the overall drug death rate, but this increase is driven by rising opioid deaths. The findings are primarily driven by adverse events among whites.
A previous study by Carpenter, McClellan and Rees found strong evidence that economic downturns lead to increases in substance use disorders involving hallucinogens and prescription pain relievers. These effects are robust to a variety of specification choices and are concentrated among prime-age white males with low educational attainment. Based on these findings, they conclude that the returns to spending on the treatment of substance use disorders are particularly high during economic downturns.
Charles and DeCicca examine the relationship between local labour market conditions and several measures of health and health behaviors for a sample of working-aged men living in the 58 largest metropolitan areas in the US. They find evidence of procyclical relationships for weight-related health and mental health for men with low ex ante employment probabilities. Separate estimates suggest worsening labour market conditions lead to weight gains and reduced mental health among African-American men and lower mental health among less-educated males. The findings related to mental health are most pronounced, which is significant given the connection of mental health to other phenomena including drug abuse.
Pierce and Schott investigate the impact of a large economic shock on mortality. They find that counties more exposed to a plausibly exogenous trade liberalisation exhibit higher rates of suicide and related causes of death, concentrated among whites, especially white males. These trends are consistent with the finding that more-exposed counties experience relative declines in manufacturing employment, a sector in which whites and males are disproportionately employed.
The economic and social costs
This 2013 NYT article has a brief overview of the soaring costs of the opioids epidemic, including for screening tests, hospitalisation, legal expenses and workplace costs.
Birnbaum et al. (2011) attempted to estimate the societal costs of prescription opioid abuse, dependence, and misuse in the United States. Costs were grouped into three categories (health care, workplace, and criminal justice) and estimated by quantity method and apportionment method. They estimate the total US societal costs of prescription opioid abuse at $55.7 billion in 2007, of which workplace costs (including both lost earnings from premature death and reduced compensation/lost employment) accounted for 46%, health care costs accounted for 45%, and criminal justice costs accounted for 9%.
Noah Smith argues that “one of the worst US social problems [the opioid epidemic] might also be one of its chief economic woes”. Registered unemployment is low in the US, but labour-force participation is also low. Many reasons have been suggested for this, but Smith argues that one simple factor often overlooked is health: a less healthy population works less. Besides obesity, the biggest health problem afflicting the US in recent years has indeed been opioid and opiate abuse. Drug abuse is bound to have a deleterious impact on Americans’ ability to work.
Smith refers to a recent paper by economist Alan Krueger, who looks at the decline in the labour force participation rate, and finds that about half of prime-age men who are not in the labour force (NLF) take pain medication on a daily basis, and in nearly two-thirds of cases they take prescription pain medication. For some, Smith argues, it’s probably because injuries or illnesses make them unable to work. But there’s no obvious reason why so many more prime-age men should have become injured and sick in recent years. It seems likely that abuse of painkillers – and, later, addiction to heroin – makes many people not want to work.


“Some medical examiner and coroner offices, including Connecticut’s, are so overworked that they risk losing accreditation, because their pathologists are on track to perform more than 325 autopsies a year — the limit in standards set by the National Association of Medical Examiners’ accrediting program.
At the Hamilton County Coroner’s Office in Cincinnati, the four forensic pathologists are on pace to do many more autopsies than the 325 limit, and the agency faces the loss of its accreditation, said the coroner, Dr. Lakshmi Sammarco.
In Los Angeles County, which has also seen a surge in fatal overdoses linked to fentanyl, medical examiner-coroner Mark Fajardo announced in March that he was resigning, saying understaffing left him unable to do the job amid complaints of stacked bodies and testing backlogs.”
Overdose deaths stressing limits of medical examiner, coroner offices
Isn’t it ironic that these deaths are coming from medical doctors, and that medical examiners are at risk of losing their accreditation because of it?
Maybe they could Automated it or hire more Coroner’s
Obviously, we’ll have to start billing survivors, privatize harvesting & marketing organs, in- denturing offspring to fill-in at the deceased’s workplace until “final expenses” are paid off?
Are we above thinking that the whole organ harvesting scenario is not being played out as we speak?
Actually, the increase in OD deaths has improved availability of transplant organs:
https://www.google.ca/webhp?sourceid=chrome-instant&ion=1&espv=2&ie=UTF-8#q=overdose+deaths+transplant+organs&*
Thanks, needs me some cheery life affirmation just ’bout now! Wonder if WalMart has organ-recycling kiosks yet? https://www.ncbi.nlm.nih.gov/pmc/articles/PMC3027447/
UberTaker
And nobody will ever know, when their autonomous organ harvesting droids fuck up? http://www.truth-out.org/news/item/40024-trump-nominates-alligator-clayton-to-run-sec http://www.commondreams.org/news/2017/03/29/nuclear-power-suffers-major-blow-westinghouse-bankruptcy
Maybe cut out the middleman, and ship the corpses directly to the prescribing doctors?
The Republicans want to reintroduce legislation to drug test citizens attempting to get unemployment benefits. I wonder if the drug tests will including testing for opiods, fentanyl, etc.? If not, why not? Is it ok for people to be addicted prescription meds, but not ok to be addicted to street drugs? Why? What’s the difference? Oh yeah, right: rich fat cat BigPharma CEOs are the pushers who make money from prescription meds, while mostly poor people who push street drugs must be punished.
I am opposed to drug testing for unemployment benefits. It’s a costly waste of time meant mainly to humiliate citizens who are down on their luck and does absolutely nothing in terms of abating the drug scourge in our nation.
It’s meant to cow us from applying; force us to beg them, tattered sweat-stained hat in hand, for whatever shitty job they can’t connive to force onto the aching shoulders of our undocumented sisters and brothers (or indenture, incarcerate or otherwise enslave our co-workers into to doing here & overseas).That’s what America’s always been about: government of, by and for the plantation owners, gangsters and oligarchs.
https://youtu.be/7nyH_7afSM8
Liked this better (though, I know Dave’s basically lying): https://youtu.be/ofnSojq-vqI?t=159 Meanwhile… it’s all kinda academic: https://theintercept.com/2017/03/28/donald-trump-rewards-fossil-fuel-industry-by-signing-climate-denial-executive-order/ https://www.desmogblog.com/2017/03/27/trump-kingmakers-rebekah-and-robert-mercer-heartland-institute-s-climate-science-denial-conference http://www.truth-out.org/news/item/40026-as-trump-complains-about-alleged-surveillance-republicans-gut-internet-privacy-rules http://www.counterpunch.org/2017/03/29/bloodbath-in-west-mosul-civilians-being-shot-by-both-isis-and-iraqi-troops/
and even though I don’t think it’s necessary to argue we earned benefits for all benefits WE ACTUALLY DID earn our unemployment benefits. It was part of what employers paid to have an employee. So it was part of the compensation from working. So it’s absolutely obscene to make people then take drug tests to claim them.
Notice the Vonnegutesque joke about the meaning of the word “entitlements” By the dictionary, entitlements are things you absolutely deserve, things that, if you don’t get them, can only have been stolen from you. That isn’t how The Powers want to use the word.
Excellent points.
Entitlement. n. Something you aren’t entitled to.
Never, ever.
What is humiliation is the idea of a reserve pool of unemployed as a hedge against inflation.
The poor, or in this case, the unemployed will be with you always.
In that case, per the quote, opioid death will be with you always.
That, not drug testing, is something more fundamental for us to oppose. If they really cared, they’d test and get the patients treated. “Go ahead, test.”
Asking for unemployment benefits is already humiliating, and worse, demeaning and demoralizing. Being part of a cyclical profession, there is a substantial difference between being laid off in 2001 and being laid off today.
In 2001, a laid off person could make a call and in a week start receiving benefits. This was my case in California, 2001. When Obama took office, unemployment benefits were extended but there was a stricter set of instructions that needed to be followed; but it was not onerous.
Today, it appears that every claim filed is scrutinized by “employment” officer. Congresscritters thought using the term “unemployed” was too derogatory. Unfortunately, they changed the name for the better but change the process for the worst. And I was required to come in for two office visits, complete some online courses, redo my resume to the liking of a government employee who had no understanding of my profession and was offered NO job opportunities to apply for. My claim was bumped for further review and my benefits denied until the review took place. Fortunately, I took whatever job I could and gave up on relying on benefits; now and in the future.
I can’t imagine how much worse it could be if I was addicted to opiates. More than likely; depressing and hopeless. I have mentioned this to elected officials and their representatives and my take away is that there is NO compassion or concern. Political indifference; the TRUE Epidemic
What about testing for alcohol use?
If some heinous regulations aren’t added to each and every government benefit that helps people, they can’t then point and say “See how intrusive the government is?”
Meanwhile, remember the bailout ransom note? It was a 3 page piece of paper with a lot of requirements for the bankstas to self-police…hahahaha….
It also focuses public money into private hands, i.e., the companies doing the drug testing. Florida may have been the first and the Governor’s wife owned many of the laboratories.
Thank you! https://www.forbes.com/sites/judystone/2015/02/17/the-sham-of-drug-testing-walker-scott-and-political-pandering/#59be2eca59be http://postonpolitics.blog.palmbeachpost.com/2015/08/05/corruption-in-the-drug-rehab-industry-how-peeing-in-a-cup-can-make-millions/ https://www.thefix.com/content/drug-testing-industry-corruption9952 http://www.csmonitor.com/USA/USA-Update/2013/1122/Chemist-who-falsified-drug-tests-in-criminal-cases-goes-to-jail-herself-video http://www.tampabay.com/news/business/gov-rick-scott-solantic-and-conflict-of-interest-whats-the-deal/1161158 soon, they’ll be using bogus testing to blackmail us forEVER.
In all honesty, I would much rather the political parties pass a law that they themselves should be held liable for decisions made while being intoxicated in one way or another. POTUS, members of Congress, judges, police officers doctors and nurses. These are the people who need to be monitored.
For every drug test given to an incoming or an outgoing employee, the senior management of that company should have to undergo the same series of tests.
I’ve always felt legislators should be drug tested before every vote.
” Drug abuse is bound to have a deleterious impact on Americans’ ability to work.”
Isn’t it usually the other way around?
Americans inability to find gainful employment leads to use of drugs abs alcohol abuse
I think you’ve got it right. There was no “opiod problem” among workers until they started losing their jobs…..they didn’t lose all those jobs because of opiods.
Read the Rat Park study.
https://en.m.wikipedia.org/wiki/Rat_Park
People keep trying to blame the drug and not the environment of the user. If opioids were the problem then everyone who’s ever had a root canal would be an addict.
There’s an enormously reactionary trend among otherwise good leftists that basically takes the worst most right wing positions on anything drug related and it’s really sad
People CAN survive on opiates, it’s not an automatic death sentence (and not just the suboxines or methadones either). I don’t recommend it mind you, I’m not recommending one go through their life as a drug addict afterall. But it seems it all depends on the opiate. The mild ones are pretty safe to take for life.
Roughly 70% of OD’s involve the use of other drugs such as alcohol &/or benzo’s (ie xanax, Valium etc)
Opoid medication will come with a prescribed dosage which, if adhered to, should not endanger the user
“should not” in a description of potential output (e.g. opiate use) or result should be banned.
When I read of the more than 50,000 people who die of hospital-induced problems each year, I wonder how many are the result of an incorrect assumption. I have personally witnessed incorrect administration of opiates based on the assumption that all humans are basically the same, so even if the dosage being administered might cause serious harm (or death), It “should not”. Frankly, that is WRONG. It is interesting that no one seems very interested in investigating and reviewing why this is going on. Take a look at “The Flight of the Phoenix”.
People keep trying to blame the drug and not the environment of the user.
Seriously????? That study was from the 70’s, by the way, and it sounds like something purdue pharma relied on when claiming that its blockbuster, oxycontin, was not at all addictive, and all the doctors who thought / think so are just clinging to their prehistoric notions, so prescribe away.
From your link:
Further studies failed to reproduce the original experiment’s results.[5][6] One of those studies[5] found that both caged and “park” rats showed a decreased preference for morphine, suggesting a genetic difference.
Translation: it’s not defective drugs, it’s defective people. Jeez.
As an aside, root canals are not the main problem. It is the use of opioids for chronic not episodic conditions, because they’re quick and dirty and get the patients out the door faster.
I searched on this page for the word “Purdue” Katniss, and you are the only person who even mentioned the name of the criminal racket behind the entire opioid crisis.
Every single discussion of this subject should call out the role of Purdue Pharmaceuticals and their owners, the Sackler family, as operating one of the biggest criminal drug cartels on the planet. The Sacklers, who revel in donating big bucks to cultural institutions, should be in prison for life, and all of their assets, including Purdue, should be liquidated with all proceeds devoted to treating the victims of opioid abuse. Hospitals, doctors and pharmacies that engaged in the criminal conspiracy should be indicted and duly penalized — at the very least, society must be protected from them. That’s what a functioning justice system would do, but of course, had we a functioning justice system we would not have come to this pass.
Are you aware there is an actual thing called the “Medical Advertising Hall of Fame” and Arthur Sackler is an inductee for his efforts making Valium the world’s first hundred million dollar drug? After Arthur’s death in 1987 Sackler brothers and Purdue co-founders Mortimer and Raymond went on to make billions with the aggressive marketing and subsequent popularity of the highly addictive drug Oxycontin.
What kind of a country has a thing called the “Medical Advertising Hall” of fame where scheming billionaire drug pushers are glorified as heroes while poor kids caught with a little bit of weed are locked up and stigmatized for life? Narcos like Escobar and Guzman look wholesome next to the Purdue family. Wacky values here in the US of A.
Link to the Medical Advertising Hall of Fame.
Thanks, Jerry. Now I have to go claw out my eyeballs.
Yes, thank you! NO WHERE in the mainstream media is it discussed these swamp creatures that falsely marketed and profiteered off of so much human and societal destruction leaving tax payers to pick up the bill.
“who knew” these drugs were so addictive ………….puleasee…..are you kidding me???
I myself experienced the cavalier prescribing of this stuff 5 years ago when a broken ankle was misdiagnosed as a sprain. After several weeks I inquired with the orthopedist why the pain had not subsided and the response was “just take more Vicodin and let me know if you need more”. I was already prescribed 30 and easily could have gotten considerably more and succumbed to addiction. I heard that some doctors were rewarded for quantity of prescriptions.
I knew using that much opioid was a slippery slope and yet the medical profession did not???
I then went to a recommended orthopedist who discovered the joint had not been x-rayed from the correct angle and 2 surgeries later I was mended with a very sparing use of Vicodin which is also very hard of GI track.
Purdue should be criminally prosecuted and their billions of profit confiscated for rehab programs.
Lots of people who’ve had root canals have become addicts.
People tend to trust their physicians even when it’s unwarranted because they’re supposed to be the experts. I can say from firsthand experience that the largest hospital in my state had been handing these things out like candy. If we hadn’t known enough to tell the hospital orderly who tried to push these pills on my wife when she complained of a very minor temporary pain that we didn’t want them, my wife could be addicted now too.
The state legislature recently passed regs to limit the amount of opioids that hospitals could hand out since they can’t seem to limit themselves due to all the kickbacks they get from drug companies.
And since no good deed goes unpunished, I see this morning on the front page of the newspaper that there may be a lawsuit against the state by some chronic pain sufferers who don’t want their prescriptions to be limited at all.
Want to really solve the problem? – throw some pharmaceutical and hospital execs in the slammer for the same amount of time that repeat street heroin dealers get.
Lots of people who’ve had root canals have become addicts.
Got a link?
I meant that figuratively as a substitute for minor procedures since it’s what the original commenter used.
But besides my personal anecdote, I had in mind an article I read a few years ago in the Portland Press Herald describing otherwise well adjusted middle class people who’d become addicted after receiving prescriptions for opioids and following doctors’ orders. I can’t put my finger on the specific article right now due since I can no longer find anything through a search engine that wasn’t recently published. You may have better luck than me but as I’m sure you;re aware ‘type in opioid addiction’ and pretty much any location or major newspaper and you’ll find all kinds of info.
And there’s this which speaks to another point I made about kickbacks –
http://www.pressherald.com/2016/12/25/even-amid-crisis-opioid-makers-plied-doctors-with-perks/
Got it. There was an article here on NC recently that stated that addiction could occur with as short as a 5 day course. But it’s my understanding that most occur with chronic use. Kind of hard to believe that your wife was offered an Rx, what with all the brouhaha going on.
But I couldn’t stop thinking about your “no good deed goes unpunished” lawsuit story. While it may seem counterproductive, i believe I’d argue that they should continue to get their prescriptions, at least until an effective, non-judgmental, non-exploitative alternative therapy was widely and readily available which, today, it is not.
Just yanking access by denying further prescriptions is what drives people, many of whom have become addicted due to medical establishment malfeasance, into the streets, and puts them at the mercy of illegal drug dealers, which is what turns a serious situation into a tragic death.
It seems to me that suddenly denying access demonstrates a fundamental lack of understanding by big pharma, the rest of the medical establishment and federal regulators of the dire predicament they have caused through their grossly inappropriate overprescribing and underregulating of a dangerously addictive, dishonestly marketed and inadequately evaluated drug.
I further feel that unceremoniously cutting people off represents an abrogation of the responsibility the medical establishment must assume for the havoc it has wreaked and has the responsibility to rectify. Simply expecting people to deal with an iatrogenic addiction on their own is victim blaming of the highest order, and tends to reinforce the antiquated idea that all drug addiction is a demonstration of personal moral inadequacy. Or “mental illness.”
In addition to your recommendation for jail time, I’d also require the medical establishment, including big pharma, to stand the cost of all treatment.
It seems to me there are two immediate concerns here–those patients who are already addicted and those not yet addicted. For those already addicted, they should be maintained with safe, legal prescriptions until they can be treated. For those not yet addicted, strict prevention should be the rule. Use of these opioids should be restricted to hospitals ONLY, under strict supervision in limited doses for limited time. Safer, albeit more familiar, drugs should be used to manage chronic pain along with more “mundane” prescriptions such as diet, exercise, physical therapy and possibly even alternative therapies such as acupuncture.
Finally, I would end direct-to-consumer drug advertising once and for all. Americans must be disabused of the notion that there is a pill for every ailment, and that every pill results in a romp through a bucolic field as the picture of health, merely as the result of your swallowing it.
Whew. Glad I got that off my chest.
You are correct of course regarding prescription cut offs and I didn’t mean to suggest that those who really needed then should just go without.
Here’s the article I referenced from today – http://www.pressherald.com/2017/03/28/two-mainers-threaten-to-sue-state-over-opioid-taper-rule/
The law doesn’t just cut people off but aims to limit dosage and taper down prescriptions. So this threatened suit is an attempt to carve out an exception for people who may really need to receive a higher dose in order to function. Never used opioids myself but having been in the company of people who’ve abused them, I do have to wonder whether after a certain threshold, people are still really functioning. No idea if the limits proposed in the article are reasonable or not.
That being said, I also have to wonder if all those mentioned as currently being prescribed higher doses than the new legal limit would be in that situation had they been prescribed correctly in the first place. Also, Maine has had legal medical marijuana for years and just legalized it for recreational use too. Opioids simply can’t be the only pain remedy out there and I’ve read anecdotal evidence of many people who do use MJ for valid pain relief purposes and they won’t be hooked for life for doing so.
My fear about this potential lawsuit is that pharmaceutical companies will get behind it and wind up completely watering down the law meant to rein them in and we’ll never be rid of this scourge, while big pharma execs, lobbyists and the other usual suspects continue to get rich of the misery of others.
In 2005 I suffered an accident at work. The first major injury that I had ever received while working, required surgery to fix what was broke.
Fortunately, the attending physician was a well known orthopod who can still be seen walking the sidelines of our home town professional football team. The repair order went well and as a send off, prescribed synthetic heroin as a pain killer to take the edge off.
I took on dose. That was it, and threw the rest out, which in retrospect, was probably not the best thing to do with unused meds.
At my first follow up with Pro Doc, his first question to me wasn’t related to my rehab, nor even about the weather, but rather, how I liked the drugs he gave me. I have to think that they have a paid relationship with their providers. As a surgeon the guy is great. As a person, I’ll have to get back with you on that one.
chronic pain is a real problem though and chronic pain suffers deserve relief (assuming there is no other relief). Of course if OTC stuff doesn’t work (and it won’t for severe pain), marijuana and kratum (opiate-like but less addictive) are safer things to try first. It depends on the pain.
I took two Aleve (naproxen) for the root canal I had today. The endodontist didn’t prescribe any narcotics. The pendulum has now swung in the direction of no narcotics for procedures. I’m doing well without narcotics, thank you.
I have never heard of anyone getting addicted to narcotics after a root canal. Katniss is correct; it’s the use of narcotics for chronic illness that’s most likely to result in addiction.
Unless the doctor made a total hash of the procedure, there is no reason to need painkillers after a root canal. Even 25 years ago, when the way they packed the root might do result in a bit of bruising, the most you would need is aspirin for 8 hours or equivalent. It’s basically a placebo for people who get freaked out.
The dental procedure where you might need an opioid is an extraction, and then only if you lose the clot, which I can tell you from personal experience is horrific, and I have a very high pain threshold. I don’t like using prescription painkillers, but I ran out and got my Vicodin, which not only did very little for the pain, but made me feel God awful. I did better alternating every hour doses for four hours of aspirin and then naxprofen.
I’ve been fortunate, so far, not to need any serious pain relief, or almost any prescription drugs at all, in my 54 years (thanks for the genes, Mom and Dad!). So it’s kind of jarring when a practitioner taking my medical history asks “which prescription drugs are you taking?”, and finds it surprising when I answer “none.” Or when I had a couple of wisdom teeth out, and beforehand I was asked “what’s your favorite pain prescription?” in the same manner I might be asked my favorite football team. Well, that’s a bad example because I don’t know squat about sports, either. Anyway, they gave me a prescription for one of the opioids, but I didn’t end up needing it. I guess I should add I didn’t end up using it either. Not even selling it.
From the Wikipedia article on the Rat Park study:
“There were 16–20 rats of both sexes in residence, food, balls and wheels for play, and enough space for mating.”
If I was in a place with 16-20 other humans of both sexes, food, balls and wheels for play, and enough space for mating, I[m pretty certain I wouldn’t have a problem with drug abuse.
yea I know, we all want to be Rat Park rats, it sure beats the rat race. Actually for some people college came close to that I guess. But never after. Pretty pathetic but life in this system does leave one envying a well treated rat.
…and having a bunch of doctors watching you…..
chicken, egg?
I got lucky, I guess. I became addicted to hiking. Oh,and yoga!!!
Not everyone can do that.
Not to disagree, but a contributing factor could also be that, with the collapse of unionization and labor protections in general, workers are being compelled to work longer shifts (as per Yves observation) under more dangerous/stressful conditions.
I know that if I was working in an Amazon warehouse, I’d need something to get me through the shift or to recover from it.
“It’s a virtuous circle, quit arguing about which came first.”
Signed your Big Pharma Overlord
After 20 years behind the desk I like many others are dealing with spinal problems and horrendous pain. I can understand why its easy to get addicted for those who are legitimately injured. The pain is very intense and there is no escape from it. I’m still working though opioids cause their own set of problems. I think I might be better off if I had a more physical job in some ways. I’ve been surprised by the rate at which the effectiveness of the drugs have decreased. I can’t imagine taking them for recreational use, or to escape from life. I expected there to be a eurphoria effect most of the time, but there’s been almost none and that was only for a few days when starting. Its more like Sudafed the rest of the time where time passes by sluggishly. The experience greatly increased my empathy for someone who uses it as a crutch as things must be very bad. I’ve never been one to drink, but if I were I would much rather go that route for escape.
My younger brothers generation use it as a counter balance to uppers (meth) from what I hear. Mixed with alcohol it helps them sleep. I can see it wouldn’t be hard to misjudge a “dosage”. The worst part will be their children who will grow up seeing this sorry state as normal, living with their grandparents in some cases because of dead or missing parents. It sucks being deplorable.
So sorry to hear this. I could chirpily tell you to “eat better (which would be a mindless assumption on my part that you don’t), or “start moving more” (which does seem to help even badly arthritic people, but is not necessarily even your problem)…” yet I find beyond already being in pain people in your situation are:
1) stuck behind the desk for >40hrs a week
2) have a minimim 45 minute (x2 = 1.5 hr) commute
3) even if a healthy lunch is available it’s hard when you are miserable to avoid the “comfort food” right up in your face and cheaper than the healthy stuff too!
4) when you do get home you just collapse no matter what promises you have made to yourself
Moving to Europe would work great, and it’s just about as likely a possibility as addressing 1->4, huh?
I am wonder if when I started wearing suspenders and stopped wearing a belt then my stomach muscles had to become stronger. That is when I stopped having back trouble.
“… plausibly exogenous trade liberalisation”
Give me a break.
“Objective consideration of contemporary phenomena compels the conclusion that success or failure in competitive activities exhibits no tendency to be commensurate with innate capacity, but that a considerable element of the unpredictable must inevitably be taken into account.”
“I returned, and saw under the sun, that the race is not to the swift, nor the battle to the strong, neither yet bread to the wise, nor yet riches to men of understanding, nor yet favor to men of skill; but time and chance happeneth to them all.”
Thanks to George Orwell quoted by Oliver Strunk.
I’d like to remind everyone that we’ve seen this before. This is not new and probably was predictable if we’d have been paying attention.
I refer you to what happened to Native Americans. There is a lot to be learned from their example, primarily that you cannot destroy a way of life without repercussions. It is amazing what a review of our own history can teach us.
So what is society’s plan to deal with this new addiction? The same method we used for Native Americans? Call them lazy and deplorable and isolate them further from society? Perhaps prison? Or maybe, like we do with other social problems, get really excited about it for a while and then let it drift off……
Society has no plan. Capitalism has declared those people to be of no value to corporate profits. They will be left to rot like all poor people and told to pull themselves together. The day they stop being reliable Republican voters will be the day the GOP introduces some kind of system to keep them from voting.
Just the GOP? Income inequality has increased pretty monotonically and at much the same rate from Reagan through Obama.
The problem isn’t just reactionaries. Liberals need to take their share of responsibility for this, too. This endgame was foreseen generations in advance and the liberal response has been largely to turn a blind eye to the reproletarianization of the sub-10% and to hold out their rice bowls for some donor class cheddar.
Thank you Cheese for that sane comment.
We can always make, “chewing coca leaves” legal……..
It’s the same with Native Australians / Aborigenes and New Zealanders / Maori and the Khoi and San peoples of the Cape.
Exactly! Thank you! Makes me wonder why we study history when we seem incapable of learning anything from it.
At least the Maori got a somewhat better deal then their contemporaries …
Heck I was brainwashed into believing for quite a while that Native Americans had a “genetic propensity” to be alcoholics. Jesus help me.
https://www.nfb.ca/film/cottonland/ “lots of reporters came around. Said it reminded them of an indian reservation: no work, no money”
The new reservation: the fly-over states. Send the addicts to treatment. Give them job training programs. Anything to help them cope with the new normal, lol.
The native americans knew the answer before they ended up on the reservations: defeat the aliens or be defeated. It’s the same for the inhabitants of the fly-over states.
We have essentially colonized Middle America, using drugs and economic hitmen. I want to see who is next.
The plan is to continue monetizing human suffering, as the Sacklers have so ably done
Frontline: How Bad is the Opioid Epidemic:
Whites and Native Americans have experienced the largest rise in death rates, particularly when it comes to opioid-related fatalities. By 2014, whites and Native Americans were dying at double or triple the rates of African-Americans and Latinos, according to the CDC.
According to CDC data, the highest fatal opioid overdoses are more likely in the middle-age 45-54 range, 11.7 per 100,000ppl. Next is the 35-44 range with 10.3 per 100,000ppl.
The top 12 states for opioid prescriptions than people 2012:
Alabama: 142.9 per 100 people
Tennessee: 142.8
West Virginia: 137.6
Kentucky: 128.4
Oklahoma: 127.8
Mississippi: 120.3
Louisiana: 118
Arkansas: 115.8
Indiana: 109.1
Michigan: 107
South Carolina: 101.8
Ohio: 100.1
What factors significantly increase opioid addictive populations in these 12 states?
It’s also interesting that these states overlap with the largest meth producing states.
As mentioned upthread, it’s possible the pills are being used in conjunction with meth as a counterbalance. Meth is largely a rural drug, so it wouldn’t be that surprising that relatively easy access to opioids would find greater demand in rural areas.
Grits, incest, NASCAR & Baby Jesus; just perhaps, brominated vegetable oil, Skoal, Guaraná & HFCS are gateway drugs we could incarcerate & asset forfeiture uppity peckerwoods over? I just donated to ProPublica who really broke this all? https://www.propublica.org/donate/
Does the substance abuse researcher even know the total USE percentage when it includes hospice care, Use as a pain reducer or a “deadening agent” for serious operations? [Always ask where the “CRASH CART” IS GOING TO BE WHEN YOU ARE OPERATED UPON AND WHERE WILL THE PEOPLE WHO KNOW HOW TO USE IT BE. . . . . .Life’s lessons are hard…..
Prescription drug overdose.
Is it all on Big Pharma or also on doctors?
Yes. (both)
How about all those poor people forced to work two or three jobs to make ends meet? Most jobs seem to require standing and lifting. I used to do hospital work–not uncommon to have 24 hours shifts, go home a couple hours and do another 24. Plus, constantly lifting 300lb patients with insufficient staff. The mechanical lifts–won’t pick a patient off the floor or one heavier than 300lbs, and there are quite a few. I once caught a 500 pounder as she fell off a gurney. Enough years of that and you’re a wreck. The one unionized job I had actually limited the hours, and provided the opportunity to take a nap as long as other staff covered. Those days are long gone….
I also worked in a hospital. I retired at 55 after numerous back injuries. The one thing that protected me was a strong union to back me up when I refused to lift heavy patients without adequate staff.
I had a patients family tell me I shouldn’t be working in the there ( hospital) if I couldn’t lift patients, after I told her her dad had to wait until I could find help.
The RN’s in Ontario have a good strong union and they are well paid ( I retired in 2004 making $32/hr) but it is very hard work.
I am suffering now with joint issues and I know opiods are not the answer to chronic pain…but some relief would be really nice
> I once caught a 500 pounder as she fell off a gurney.
I know it’s not supposed to be funny, but that made me laugh out loud.
We all laughed when it happened, too! I am not all that strong, so I guess it was a sight to behold. My back, knees, etc. never stop hurting. Yeah, some relief would be nice.
Have you tried tumeric tablets? You have to take 2-3 per day and it takes about 2 months to build up in your system to work….but it did wonders for me. I didn’t want to take aleve constantly so took the tumeric 6 months prior to surgery (joint). Once I stopped it (10 days prior to hospitalization) I realized just how much it was helping me. Might be worth looking into.
On Feb 25, 2017, Zerohedge had a discussion thread entitled “America’s Fentanyl Crisis” is Surging, with No End in Sight.
Apparently, the synthetic opioids are much stronger and much easier to manufacture synthetically than growing poppies.
I won’t link the thread, but here are a few comments:
DocMims: [an anesthesiologist]
This is totally a Fentanyl epidemic. Chinese Fentanyl is cheaper than opium. The drug cartels are counterfeiting heroin and prescription drugs using Fentanyl as the narcotic. The users get the narcotic effect, but far greater respiratory depression than the drug they think they are taking. There is unsafe quality control when you are taking street drugs. I believe there would be fewer deaths if the stuff was legalized with high standards of quality control.
YHC-FTSE: It’s interesting that the “Chinese Fentanyl” is being pushed by the MSM. Fentanyl is manufactured by various big pharma brands which are subsidiaries of Johnson & Johnson like Alza Corp and Janssen Pharma. Besides Acetyl Fentanyl was banned for export by China. They do sell a lot of pill pressing machines to the distributors but I’d like to know exactly where all the illicit drugs are actually coming from.
This convoluted drug supply war in America – with competing big pharma, CIA heroin, DEA coke and weed – is exemplified by the fact that last year, Arizona based Insys Therapeutics (NASDAQ:INSYS) which manufactures fentanyl donated $500,000 to the campaign to keep marijuana illegal in Arizona. Now why would they do that if they were not pushing their own drugs in competition to the same customer base?
Slammofandango: Heroin sold on the street is almost always branded with a dealer’s mark for reputation purposes yet it is almost never close to being pure. But when junkies hear news of someone overdosing, they all think it’s a good idea to buy their next fix of heroin from the same dealer that sold to the person that ODed on the assumption that a particular batch of street Heroin is close to pure.
Part of this new epidemic involving Fentanyl is that dealers will purposely lace a single packet of normally unpure Heroin with a dangerous level of Fentanyl. The dealers are actually intentionally poisoning low potency Heoin purchased by random users so as to gain their brand the reputation of being pure Heroin which they otherwise aren’t doing at all.
SixisNine:
look – here’s the problem – according to the DEA new variations of fentanyl have been found and are active @ a few micrograms.
edit: and if the “elephant” versions are thousands of times more potent – then what? 1/8 microgram is a potentialy lethal dose? Get outta here !
That’s 1,000 micrograms in a milligram. There’s 1,000mg in a gram. Do you get the problem now? 1 Million mcg in a gram. 100 to 300 thousand doses in a gram?
seriously – think about that. $1 buck a dose. wholesale. $200,000 profit for one gram? this is a problem folks.
now what if it’s the elephant version and you get 2 or 3 million doses in a gram? $2million a gram? you can bet that incentivies a lot of young chinese chemists.
Someone who has the intention of spiking some product, in say, Mexico – and puts an order in to china – which is the wild west of chemicals apparently – can put 10 grams or 100 grams in an envelope or whatever. sends it up the channels to USA.
lethal dose potential astronomical.
this is a PROBLEM.
Montana Cowboy: If anyone thinks the war on drugs is effective, fentanyl will reveal what a joke the DEA really is. This stuff cannot be stopped because it is so concentrated. It can be packaged like blotter LSD. The back page of a Happy Birthday card can be impregnated with 1000 doses or more because fentanyl is 50X stronger than heroin. But there is also carfentanyl which is 10,000X the strength of heroin and still legal to manufacture in China. There is simply no way to interdict anything this concentrated and concealable.
The DEA clampdown on doctor-prescribed pain killers has sent many patients to the street – and that is no accident. There is a bumper crop since the US (and daddy Bush/CIA) have taken over the business in Afghanistan. In some countries, a hit of heroin on the street has reached as low as $1 USD. Too much product. They need to steal the medical customers.
—————————————————————————————————————————-end
My own mother, now age 88, was a pharmacist for over 50 years and she saw very little problem with Oxycontin. In a farming town with a lumbermill, many of her chronic pain customers were back leading very productive lives. If they were addicted, it was to being pain free.
Didn’t the Brits once upon a time keep the Chinese addicted? Turnabout, fair play?
My vote, legalize drugs. And for goddess sake, at the very least don’t limit those in chronic, pain management situations.
That was my first thought. Karmic payback. I took some upper level science courses in the early eighties. The Asian exchange students were without peer in the Chemistry Department.
Ding ding ding. The problem isn’t even that the dealers do a bad job cutting it, it’s that carfentanil is so concentrated that you end up getting clumping no matter what you do. If oxy was free and OTC I guarantee the OD rate would fall. It’s the fact that they start you on Oxy and it is the one thing that makes your shit life suck less then they try and cut you off so you turn to the street where you can get the cheep stuff but it is impossible to dose correctly,
I was on Fentanyl for a pretty good time. I became allergic to the adhesive for the time release patch. I can understand why some people just stop breathing.
I’ve had 4 big operations along with stuff that hasn’t, and never will be possible to repair.
I did not ever mess around with pills or morphine or heroin, but loved pot and hashish. As a pilot it was important not to use drugs that diminished my ability to safely fly a plane.
or even drive since I had a professional license for a good deal of my movie technician career.
All the opiates & the mother of all drugs, alcohol, must be used correctly, or you can’t fly.
Pot as a joint and you are definitely safe after 24 hours, commercial or private.
Hashish eaten I say you aren’t really safe for 3 days. You get pretty high off hash if you chew it up.
I was an aviation ground services manager or lineman, or a movie and television grip, gaffer, or DP. In both careers you had better be right on with safety or people either die or get really hurt.
I am proud of my safety record.
US law aimed at labor, especially educated experienced labor means fear & poverty & disrespect at every turn.
For most of us who live lives of labor there is little to zero respect if we know anything or don’t, and death or prison is always close around the corner.
When Rome made serfs of citizens with taxes for Emperor shows to holiday holiday 121 holidays a year Rome they became willing to welcome the barbarians.
In the recent days of the US they just elected another barbarian and all his barbarian & financial terrorist friends.
They were the same friends of the Clintons.
No chance in hell for USPO Service Industrial banking is there. Best Practices would mean make another nation.
A nation of airports is an affordable labor revolution to make work out.
From the Charles and DiCicca study summarized above:
Separate estimates suggest worsening labour market conditions lead to weight gains and reduced mental health among African-American men and lower mental health among less-educated males. The findings related to mental health are most pronounced, which is significant given the connection of mental health to other phenomena including drug abuse.
Trying to figure out what it is about this mess that pisses me off so much.
As I read it, with “worsening ‘labour’ market conditions,” black men get fat and become mentally ill, “less-educated men” (in general?) become mentally ill, and mental illness is “connected” to drug abuse.
It sounds like a case of statistical “analysis” gone horribly wrong to me. I’d imagine a creative interpretation of the words “lower mental health” is involved.
Constantly tying work into self-worth drives me crazy. Especially how we in the US so often define work. Puritanical to neoliberal… same as it ever was.
I take issue with the media’s distinction of pain killers as opioids and Heroin as a drug. They are the same dang thing. Saw an article that 25% of heroin overdoses are for athletes, from which it can be inferred their addiction started with pain killers. so 50-75% of the remaining ODs are resulting from painkiller addiction.
But big pharma is looking out for us. They just released a new drug to fix the constipation you get from the opioids…
I’m writing a new song. The chorus goes like this:
Heroin legalized by the FDA,
A white trash genocide, so its okay?
Let’s not forget to blame drug advertising and doctors who would rather push drugs than appropriate treatment for some of this. As a long time chronic pain patient, I would not be disabled today had my doctor twenty years ago honored my request for a chiropractic referral.
One thing that tends to be swept under the rug is that there is very little correlation in the amount of relief found in opiods for pain – chronic or otherwise. Unless healthcare professionals spend the time to determine why someone has pain, they cannot treat the problem…just the symptoms!
You don’t need a referral to see a chiropractic. They are not doctors. Twenty years ago you merely had to look in a phone book and call….
Twenty years ago was the age of HMOs and introduction to PPOs, so if you wanted insurance to pay for a chiropractor, you had to get a referral from your primary physician. And chiropractors may not be doctors in the M.D. sense of the word, but they study the same things and are not quacks or charlatans. Dated someone in his final year at Chiro school and got creeped out by the dead bodies they used for study when we had to stop in for some reason one day.
Doctors and chiropractors do not study the same things. And most doctors wouldn’t refer patients to chiropractors. According to this study from 2006, “only 24% of DO’s and 29% of MD’s had themselves formally referred a patient to a chiropractor. The common reasons for referring a patient to a chiropractor were back or neck pains, unresponsive chronic pain, fibromyalgias, and musculoskeletal conditions. A vast majority of both DO’s and MD’s preferred that their patients contact chiropractors on their own rather than the physicians initiating a formal referral themselves.” https://www.ncbi.nlm.nih.gov/pmc/articles/PMC1456998/
Yes and no. In the U.S., mainstream medicine absorbed mainstream chiropractors 50+ years ago. That’s what DOs are, and it’s why most other countries don’t have them.
Now, here’s the question that may be a little off-topic, but has been bothering me for ages. Does it seem like the DOs who practice family and internal medicine in the NYC-DC corridor almost never do “chiropractic adjustments” these days, but they frequently have a Rikki (traditional Japanese energy) healer on site? Meanwhile, the ultra-orthodox chiropractors who actually do traditional chiropractic adjustments usually work with other ultra-orthodox chiropractors? Or am I imagining it? And if it is real, do the rich people in the tri-state area really get that much more of a benefit from it?
This is just so sad and depressing. I’m going to roll a joint
I can see no other explanation than the rich and powerful wanting you all to just die.
And, make it soon you know, they’ve got lives to live and they don’t want to see you.
In fact they don’t
Some of the people, possibly mentally ill but certainly in serious emotional pain, are making sure that everyone sees how they feel. Two very public suicides by middle aged men in the past month in Boulder County. Also, in 2015 “67 suicides were reported in Boulder County, the majority of which were middle-aged males.”
http://www.dailycamera.com/lafayette-news/ci_30884723/lafayette-suicides-spotlight-increased-mental-health-concerns?source=mostpopular
The relevant natural experiment is opiate use by US soldiers in Viet Nam. AFAIK it was morphine, grown in the Golden Triangle in SE Asia and transported by the CIA front airline Air America. The figure I heard was 20%. It was expected that there would be a massive problem when the addicted GIs returned, but it never happened. Apparently they had no problem giving it up with they re-established family, social and job relationships. This tends to support the Rat Park theory.
OTOH a big motivation for the formation of the FDA was the large number of respectable women who were quietly addicted to patent medicines containing opiates. But we don’t have studies on how many had other problems that contributed to the situation.
Either way, the facts don’t determine whether criminizing a category of drugs is the best policy. If the opioid problem is entirely due to economic and social breakdown, repairing the damage appears to be enormously expensive and slow. (The mistaken policy on cannabis has made the situation worse.)
Fentanyl has been around for a while. I recall hearing about a local anesthesiologist who gave it as a treat to his golf foursome back in the 1980s.
The definitive text of pharmacology is Goodman & Gilman. My copy is old, but the chapter on drugs of abuse is excellent. It will be interesting to see what they have to say about this. The book is available for free on the internet, but it looks like the only way to download it is as one big file. It’s 1000-2000 pages and I keep putting it off.
But how many opiate addicts actually voted?
A friend of mine has relatives in W Virginia. This relative told him about a couple of times he’s come home with thieve who have nodded off from drugs, sitting there with the potentially stolen goods in a bag at their side. One time he was on the phone with his relative and his kin had to stop the conversation to run off some junkies trying to sneak in through the back door.
It’s hard for me to believe that these are the people to “blame” for Trump’s victory.
No, the Trump voters are your garden variety wanting-tax-breaks upper and middle income people or frustrated entrepreneurs – of various ethnicities qnd backgrounds.
You’re right–the addicted and other members of the ever-increasing “lumpen proletariat” that is over the last ten years absorbing more and more formerly working families as communities disintegrate from the effect of more and more people’s inability to earn a living and as more and more of people in those disintegrating communities fall into various pathologies-they have never thought of voting. That’s not part of their world.
But there are also lots of other people in those communities still above water who could see that the world was going to hell and that only one candidate had noticed or at least claimed to have noticed.
I can add a little first-hand experience to the “workplace-related factors.” Working as a public defender in upstate New York, I represented a few former employees of Kodak. They were all white men, had been injured in some way while working and were prescribed some kind of opioid for the pain. Each one told me that after Kodak’s bankruptcy and restructuring they lost whatever part of their health plan covered the opioids. After that, they turned to heroin. It was easy to find and they could afford it. Nothing they told me surprised me or seemed untrue. This was especially the case since I could drive by Kodak and see buildings that looked they had just been reduced to rubble with a wrecking ball. Destroy a company, destroy a building, destroy a life.
I would just like to note a factoid I heard recently on NPR radio. This should be called the poly-substance overdose epidemic, since the majority of overdoses include alcohol and other pharmaceutical drugs such as tranquilizers and barbiturates.
This does not of course undermine the premise that this is a consequence of social and economic conditions.
It does agree with my own understanding of the phenomena and what I think is probably a common sense approach.
Opiates and heroin of course are another boogie man propaganda weapon that has long been used to fuel the drug war against the poor.
http://www.counterpunch.org/2017/03/17/manufactured-opioid-crisis-a-ploy-to-salvage-war-on-drugs/
This article addresses the issue of multiple drug use and implications for criminalization of drugs.
And a follow-up today: http://www.counterpunch.org/2017/03/31/opioids-arent-the-problem-and-chris-christie-isnt-the-solution/
Working as a social worker in rural Michigan I see a lot of addiction of all kinds. Many of my recovering addicts have told me that the most addictive part of drug use was dealing drugs. Generally speaking when people use drugs they deal, sometimes a little, sometimes a lot.
Dealing drugs or winning the lottery are the only two ways poor people see to escape a minimum wage job. These MCjobs have no benefits, no set work schedule, no guaranteed 40 hours, no pension, and no chance of much advancement. You can work a 40+ hour a week job and take home $300. You have to have reliable transportation (no mass transit of any sort in rural America) and if you are a woman , childcare.
If you deal drugs you can work from home and make $300 in a few days. That is until you get busted, or start using yourself and “eat” all the profits.
This is a pet peeve-
“my recovering addicts ”
“Your” addicts? I heard a parole officer refer to his charges as “his clients” and thought he was joking. Nope, that’s the preferred nomenclature.
Two weeks ago I got a total knee replacement. Due to the politics of opioids and the primary directive in for-profit medicine to CYA (and likely the culture of the Carolinas vs Chicago) I have had to endlessly advocate for myself to get enough meds to keep my pain managed so I can progress at my desired pace – quickly! I graduated from the walker to the cane this week and can bend my knee to 100° – woo-hoo!
After the first 5 days at 15 mg Oxycodone every 3 hours I scaled myself back to half that (10 mg every 4 hours). But despite my documented progress and lack of any complications with side effects, the doc is doling out 3 and 4 days’ worth at a time as if I am exhibiting drug-seeking behavior. Numerous calls to request a better regimen just result in another dribble of Oxy. I was taken off NSAIDs prior to the surgery and apparently they are not an option since I am taking aspirin as a blood thinner.
Generally my experience has been good but I am FURIOUS that at a time like this without any assessment of me as an individual, some generic notion of pain management has resulted in me having to short myself, sometimes on days when I have a grueling PT session. From my work in hospice I am familiar with the combo of a long-acting and a short-acting opioid for breakthrough pain. Apparently my doc doesn’t do this, no idea why cuz I can’t get hold of him.
Narcotics are actually less addictive than nicotine, and pretty harmless on the organs as compared to nicotine, alcohol, or cocaine.
The problem really is that they are seen as a criminal and not a public health issue: harm reduction practices NIDA has been advocating for since before Just Say No if adopted would have prevented untold overdose deaths.
Ultimately the problem is lack of care: individualized and designed to benefit the patient, not maximize efficiency or minimize risk.
Ugh!
Yup. People get addicted because their life sucks not because opioids are magic. They overdose because illegal supplies are impossible to dose correctly. I had to fight like crazy when I broke my elbow 5 years ago it was so insane I just gave up and bought some street stuff to get me through the recovery. Didn’t get magically addicted.
A friend of mine is a primary care physician in student health services. They deal with a lot of sports related injuries. The kids get referred to the orthopaedic practice at the local hospital, where it has been standard practice to prescribe something like 100 pills of whatever opioid after surgery. The doctors in the student health services clinic started a represcribing campaign. They took the original prescription from the ortho docs, and gave their patients a prescription for 10 pills, telling them they could get a refill if necessary. Almost never happened.
Meanwhile one of our local surgeons started looking into how much pain meds patients actually used, vs how much they prescribed, and is working to change prescribing patterns accordingly.
https://www.washingtonpost.com/news/to-your-health/wp/2017/03/07/surgeons-were-told-to-stop-prescribing-so-many-painkillers-the-results-were-remarkable/
…Credentialed drugs Good…all else: Bad!
Oaf get it now…
Just to bring up another possible factor….Hopelessness. I recall a college professor I had from Lithuania saying that citizens were so depressed and hopeless under the Russian regimes that large numbers of the population would drink themselves to death. Alcoholism was rampant.
I think a general statement can be made that human beings bereft of hope will numb themselves with any kind of substance to quell the sadness and depression that accompanies hopelessness.
It will be a growing feature of living in the US.
Same as cougars in a cage…
Hope matters.
This has been studied. One term for it is “learned helplessness”.
https://en.wikipedia.org/wiki/Learned_helplessness
https://youarenotsosmart.com/2009/11/11/learned-helplessness/
Lost my nephew to downers. We avoided them when I was young. Drugs are a folkways and the market is dominated by downers from all I hear.
I am disabled by pain without timed release morphine, and I am always in pain. For trying some Colorado cookies, which helped, my morphine of 6 years was withdrawn & I could not rest. Unbearable to even be around was what it became.
Forced morphine withdraw is something worse than anything I’ve gone through for reasons I ought even keep to myself sometimes.
Some of my pain was caused by economics besides the incompetence. Incompetence on the doctors part affecting the financial ability of the drug that was supposed to counter withdrawal torture.
Where I am malpractice is capped. Malpractice attorneys in general don’t want to work where even the awards are capped.
Overall in the world of disabling pain dumbasses killing themselves has hurt us more than regular sufferances and insults like pot piss testing which the doctors know has no harm, and is potentially very helpful.
I felt some well being with all working & the cookies. I’m chronically sick.
So when you hear the NRA say they will come looking for those with legal registered guns before they will find the ones with the ones used to rob you or murder you, be for sure they are right.
The system is pathological & bad laws make a bad society and like they say, if they ain’t got you yet, they are coming for you next.
Things have been bad and they just keep getting worse. Most of us are trapped. Even if you aren’t lost you are trapped.
The Feds got the Left for smaller government with bad drug laws, the DEA, & Hoover policing aimed at young people.
They got the Right for small government with lies about how the economy really works & what the Central bank is for, and then Privatization and fees & fines for breathing.
I was telling youth to move to Montevideo in groups of friends to defend Uruguay from the US. I may still sing that song. It is far from lots of tanks.