An Academy Health Blog post last week set both Lambert’s and my “something is wrong with this picture” alarm bells ringing. The article, How coverage and technology interact, cites mainstream, widely-cited studies on what allegedly drives health care cost increases. Here are the opening paragraphs:
As I posted previously, many studies have pointed to technology as a principal driver of health care spending growth. Those studies also credit third party payment (i.e., insurance) and income for some of the blame too. More interesting, coverage, income, and technology interact; their intersection is explored in a few papers summarized below.
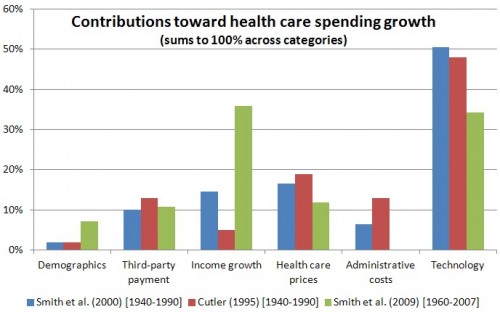
The 2009 paper in Health Affairs by Shelia Smith, Joseph Newhouse, and Mark Freeland is one of the sources for the chart above. (See this post for additional detail.) In it, the authors note that “interrelationships among technology, income, and insurance are strong,” which makes “it difficult to assign specific quantitative magnitudes to each factor.”…
Burton Weisbrod’s fascinating 1991 paper, “The Health Care Quadrilemma,” may have been the first to deeply contemplate the insurance-technology nexus. In it, he explained “how the expansion of health insurance has paid for the development of cost-increasing technologies, and how the new technologies have expanded demand for insurance.” Weisbrod recognized that the key linkage is the research and development (R&D) process…
This sort of thing drives me to despair. Go look at that chart. How can you begin to pretend that those categories are mutually exclusive? They aren’t even remotely, as even the snippet of the post I’ve provided demonstrates, and you’ll see even more proof if you read it in its entirety. So what is the point of engaging in the pretense of quantification when the explanatory variables are not at all discrete drivers?
And what should really get you skeptical is the vague term “technology”. What does that mean? Is a new drug “technology”? Even if so, what about all the new drugs (via FDA classification as “new drug applications”) that are merely exercises in intellectual property rent seeking? The overwhelming majority of NDAs (I’ve seen estimates of 88%) are not new drugs at all but merely minor reformulations, like an extended release version, that allow patent life to be extended and for price increases (the “new” version is pushed hard to doctors and always priced higher than the existing version).
But we don’t even have to get that granular. It turns out that “technology” is the error bar, all of the “not explained otherwise” factors. No, I am not making that up. From the 2009 Health Affairs paper cited above:
The conclusion that technological change explains much of the growth rests on a macroeconomic approach that seeks to estimate the contribution of known factors to health spending growth and assumes that most of the unexplained residual growth is attributable to technology.
Go look back and look at the chart again. How much faith can you put in an analysis where far and away the biggest single factor, in most cases accounting for roughly 50% of the total, is what you can’t otherwise explain? And worse, the researchers call it “technology” which makes it sound virtuous!
Let me give you a different picture of “technology” in medicine. I get annual physicals and an annual eye exam. Annual physicals are actually considered to be a waste of money but it is a tolling device for my doctor. I have one prescription (trivial and and old, cheap, medication) and prescriptions in pretty much all states are only valid for a year. So even though my dosage has been stable for years, and I could just get a simple blood test and maybe have a routine doctor visit associated with renewing the prescription, I have to go through the annual exam routine. By contrast, in Australia in the early 2000s, you could call your doctor for a prescription. Most of the time, if you were an established patient, they’d talk to you on the phone and issue it. They’d send you to a lab if they thought they needed to see bloodwork. The charge then was $A15. Cheaper and much less of a hassle for the patient (and also note Australian doctors are not as med happy as Americans; their response with a lot of conditions was “let’s wait and see” rather than running in to intervene).
While that sort of thing is sadly routine, it’s minor compared to my eye exam drill. All I really need annually is a glaucoma test (since my grandfather went blind from it, getting a test annually is warranted in my case) and a refraction test to see if I need my prescription changed (Getting an eye dilation test for them to look at the back of the eyeball is not a bad idea but I skip it as many years as possible since I can’t afford to not be able to read for four plus hours afterward). But I am put through a monster raft of tests, all with super fancy and I am sure super pricey equipment.
So as much as the MD annual exam drill bothers me, the upcharge from a regular office visit is only $75, and the rack rate is $250, since I refuse to get an EKG (not warranted in my case). So that is really not that bad. By contrast, the rack rate for my annual eye exam is $950, and that is with my skipping the dilation test. I can’t believe all these tests are necessary, but unlike my MD visit, where I know an EKG is not warranted and I can refuse it (and I don’t get any grief), I have no idea what all of these crazy eye tests are for and therefore am in no position to object to some of them.
Now is my eye doctor exploiting me? Exploiting my insurer? My insurer clearly does not think so; they always pay for all the tests (including the refraction, which is unusual). But this anecdote demonstrates that what is called “technology” looks to be in very large measure a US bias towards overtreatment. For instance, hardly any US doctors act the way one of my orthopedists did. I called his office to schedule an appointment because I thought I had broken my little toe. The doctor got on the phone and said: “Don’t bother coming in. Tape your little toe to the next toe and wear flats.”
The real issue is that health care in general, and US health care in particular, is a classic example of market failure. As we wrote in 2007, using a then-new book by Maggie Mahar, Money-Driven Medicine, as a point of departure:
The reason that [Tyler] Cowen supports Mahar’s assessment is that she explains why health care has failed in terms an economist can appreciate: she shows why the market has failed. One big culprit is information asymmetry. One of the conditions for a market to function well is that buyers and sellers have perfect information. In the medical arena, there is often a lack of good data as to what constitutes optimal practice. Among the many examples are the backing and forthing on hormone replacement therapy and mammograms. Now condiser: these treatments have been the subject of multiple large scale studies. Most protocols haven’t been investigated this intensely. And even when there is good information, the patient is at the mercy of his medical providers, the drug companies, and device makers. He can’t challenge their views; his best hope is to shop for a better practitioner, which is a costly, time consuming, and deeply flawed process (how can he judge whether a doctor is making sound recommendations?).
The other major element of market failure is the considerable disparity in buyer and seller power. If you are very sick, you will do anything to get better, which includes spending a lot of money. And our can-do, technology-loving culture favors doing more, whether beneficial or not.
From Cowen:
The book has the most coherent, supportable, and fleshed out anti-market story I’ve seen. It both tries to explain why the current system works as it does, and historically how it evolved from more modest and less expensive ways of doing business. It’s not just a rehash of the usual stories about the VA system or France. The discussions of the growth of for-profit hospitals, the increasing specialization of medicine, the problems with pay for performance, and markets for medical devices are all full of interesting tales.
I interpret the basic story as this: the American health care cost spiral comes from suppliers and their entrepreneurial abilities to market expensive and highly specialized services of dubious medical efficacy. Medical care starts off as ambiguous in value and hard to measure in quality. Customers are cowed by doctors and other family members into accepting or even demanding what is offered to them. Third-party payments make the problem worse, and government intervention has stoked rather than checked the basic dynamic. You end up with massive expenses, lots of stupidity, and – because of its expense — radically incomplete coverage. Every now and then the extra services do pay off, but not frequently enough to boost American stats on health care quality.
In other words, when you hear “technology” invoked as the reason for health care cost increases, recognize that in large measure this is really code for “bad incentives plus new and improved snake oil salesmanship.” While some medical treatments are powerful and beneficial, too many are low efficacy, or cutting-edge whiz-bang with only marginal at best improvements over older, cheaper methods. It’s hard for doctors to opt out of this Gresham’s dynamic; patients are conditioned to expect too much, and to see more treatment as better treatment. But the biggest crime is that Obama had a once in a generation opportunity to remedy these problems. Instead, he doubled down on the failed, high cost, market driven model.


I am going through something like this “groping in the dark” concerning my essential hypertension. Since I left my Boxx Store job, and now have no medical insurance in a no Big Medicaid state, I find myself experimenting with the drugs I previously took to try and discover which ones do me any good at all. Real money is involved, at least from my low income perspective. I have also refused to take the “new and improved” versions of some older drugs. One has to learn how to gently “reeducate” ones’ physician. (The older ones are, paradoxically, easier to reason with. Is it cultural bias, or finance anxiety? I don’t know.)
What I am observing is that this push to increase the rent extracted from medicine is harming the older members of our society, and the poor young, disproportionately. As the proportion of older, more civically engaged population increasingly perceives themselves as being victims of the extant system, they become a fertile breeding ground for “movements.” The old, and young are slowly becoming politicized. A United front will soon be possible between these two demographics. Ambitious politicians take note.
(The older ones are, paradoxically, easier to reason with. Is it cultural bias, or finance anxiety? I don’t know.)
———
We might get more set in our ways as we age, but the school of hard knocks seems to make us more empathetic over time and less idealistic.
The solidarity of the screwed-over…perhaps there is hope after all…
In large part I think it’s because older physicians have had more time personally to see the harms from therapeutic enthusiasm in their patients and get cautious and more judicious. Both harms and success are low rate events, so without long personal experience, it’s hard to accumulate enough data to see beyond preconceptions and various cognitive biases, such as “more is better”, and shiny gadgets are magical. Older docs estimate a lot more care is unnecessary than younger ones. I agree that a united front is possible, and we’re starting to see evidence for that.
When the economy crashed and Obama pushed the stimulus package, both MD practices and hospitals were “encouraged” to use computer charting-part of the purchase price would be reimbursed if certain criteria were met. Presently there are two companies that dominate, Epic and Cerner, whose CEOs have ties to Obama (bundling or worked on election campaign). Well to make a long story short, just about every hospital that bought these overpriced programs are having serious financial difficulty.
EMR, EMR, glaucoma, myopic retinae, technology costs, yoga
I recently escaped part-time locum tenens* piecework at a hospital system that was using Epic. I had wrongly expected it to be easy to learn since I had used a different version of Epic in another hospital 15 months earlier. But these vendors make more money selling the wonders of customization with subsequent consulting fees to fix the SNAFU of admin-academe-clinician(maybe) committee designs on top of the original EMR. They also charge to make EMR’s interoperable – even though the federal CCHIT certification is supposed to certify interoperability. In the Twin Cities, the Epic of Allina and the Epic of Health Partners cannot directly talk to one another. (Database fields must be a little different; I may also have misrecalled which two giant fascist health systems speak these dialects) The cost of technology indeed; knowing the price of everything, and the value of …
A little more rant on EMR’s. They are nearly all built upon the 25 year-old MicroSoft-SQL, so have the same sort of back end, yet they all have lousy front end interface, and they refuse to speak to one another without a consultant bribe. They cost doctors about 4 hours per week – and that is direct measurable time-cost, not including having to scan past the screens of crap collected for some billing-coder person, checkboxes for some other admin, and the seven mandated fields on smoking cessation, etc etc etc for future big data. (Personalized medicine, with actual DNA analysis really will improve health care and costs some day, IFF that is the intent, through the magical data-crunchers in the Cloud.) The only benefit I have truly seen so far is that prescriptions are becoming easier to write and track. In 1998, I was a beta-tester for an EMR already in use in Greensboro NC, by a large specialty group. Nothing I have seen since has worked so well.
I have a Family History of glaucoma and blindness, and of retinal detachment.
I used to have moderate essential hypertension (1997-2001). Then I took up Yoga (again) and got ejected, pre-whistle blow, by a large medical system in Wisconsin, The Gulag. BP now is great. Yoga cure, or exit the corporate monster,? – no telling. Diabetes positively correlates with bath towel absorbency ya know! Anyone can StartPage look up LifeForce Yoga, which is directed at depression and anxiety, but is generally safe for anyone, and ANYthing that increases parasympathetic tone will help with BP. I also don’t mind direct email if the site managers allow/facilitate. It’s just what I do, to keep my new practice insolvent!* Otherwise, propranolol, atenolol, lisinopril, diltiazem and HCTZ are pretty cheap.
I ought to have a yearly dilated retinal exam, but cannot currently afford it. Agree the yearly physical is unnecessary, and I refuse the decadal roto-rooter for now. My last glaucoma screening produced an impressive sonogram of my retina, yet I know that all I really need for glaucoma screening is the little air-puff measurement which could be done by a technician on 20 year-old equipment. As I tell my patients on some of the labs: “This might only cost $25 if I could send you to my vet.” Maybe Wal-Mart is kinda like a legal vet (health care innovation there? – how depressing; but Prozac is only $4, and the eyeglass frames are cheap).
*Locum tenens is temporary doctor placement, and how I help pay the salaries of some college MBA’s for another 3 1/2 years, as well as rent for the the private practice, which is integrative medicine/psychiatry and not yet making rent mainly due to to my new learning of another EMR, and all the et ceteras. What I really need is a part-time virtual assistant/ remote office receptionist-scheduler with a charming Greek accent. I am afraid to go online where I might end up with a boiler room op in Lower Dakotia. Anyone here know how to hire a real Greek person whose spending would happen in Greece itself?
I seriously doubt I am at actual risk for glaucoma. It is strongly correlated with hypertension and I don’t have that. But it’s easily treatable and I have to get an annual exam anyhow to check my prescription, so I don’t mind getting that test.
An optometrist can check for prescription changes, glaucoma, along with some other common eye problems, and where I live charges under $100. Almost $1000 annually for an eye exam in the absence of known disease is obscene, especially when compared to $75 for an annual physical. An EKG is not routinely performed during annual physicals. The pricing differential reflects the disparate compensation between generalists and specialists, along with the need to pass on the costs of the additional expensive technology typically found in opthalmologists’ practices.
Even with the stupid rack rate cost, after my insurance kicks in, what I pay after they apply their discount and at my co-pay percentage, it comes out cheaper than seeing an optometrist, which is not covered by my insurance. But this is a ridiculous set of incentives.
EMR tech costs
I recently escaped part-time locum tenens piecework at a hospital system that was using Epic. I had wrongly expected it to be easy to learn since I had used a different version of Epic in another hospital 15 months earlier. But these vendors make more money selling the wonders of customization with subsequent consulting fees to fix the SNAFU of admin-academe-clinician(maybe) committee designs on top of the original EMR. They also charge to make EMR’s interoperable – even though the federal CCHIT certification is supposed to certify interoperability. In the Twin Cities, the Epic of the Allina system and the Epic of Health Partners cannot directly talk to one another. The cost of technology indeed; knowing the price of everything, and the value of nothing (Oscar Wilde) …
A little more rant on EMR’s. They are nearly all built upon the 25 year-old MicroSoft-SQL, so have the same sort of back end, yet they all have bad to horrible lousy front end interface. They cost doctors about 4 hours per week per the AMA – and that is direct measurable time-cost, not including having to scan past the screens of crap collected for some billing-coder person, checkboxes for some other admin, and the seven mandated fields on smoking cessation, etc etc etc for future big data. (Personalized medicine, with actual DNA analysis really will improve health care and costs some day, IFF that is the intent, through the magical data-crunchers in the Cloud.) The only benefit I have truly seen so far is that prescriptions are becoming easier to write and track. In 1998, I was a beta-tester for an EMR already in use in Greensboro NC, by a large specialty group. Nothing I have seen since has worked so well.
. In it, he explained “how the expansion of health insurance has paid for the development of cost-increasing technologies, and how the new technologies have expanded demand for insurance.”
———–
Our monetary system is primarily based on creating money based on hard assets and collateral. Services are funded through the trickle down…. the lower these services are from the hard asset money printing and those who receive this new money, the less they will get funded.
Government is the best tool to get these services funded but over the last few decades, governments have been asked to mimic the private sector and itself also focuses on hard assets.
Here in Canada we keep on hearing about hospitals getting new MRI machines or other but having no budget to use them… so they stay unused somewhere in a dark closet.
Over the last few decades, universities have built a huge number of new pavilions everywhere but they now have no budget to pay for their maintenance or the profs.
There is always money for hard assets but never enough to maintain them or for services.
The problems of health care can’t be traced to market failure because there is no market to fail. Are firms without pricing power? No. Are prices set for firms by supply/demand equilibration? No. Do consumers have equivalent alternative choices? No. Do all participants have access to identical information? No. Are prices transparent? No.
Without all of these no market can exist.
Um but the policy assumption is that healthcare IS a market. People are now expected to shop for insurance, and worse, to enjoy it. They are expected to shop for doctors. It is also anticipated, in policy, that consumers (not patients!) will discipline doctors regarding pricing, that cost constraints will lead them to spend their medical dollars widely, as in frugally. What do you think all that coded talk of “bending the cost curve” was meant to signify? See this:
Better technology integration, greater collaboration among providers and higher co-pays for patients are among the ways to address the high cost of U.S. health care, according to leading policymakers and practitioners speaking at the School of Business Administration’s January 17 conference, “The Business of Health Care: Bending the Cost Curve.”
http://bus.miami.edu/faculty-and-research/conferences-and-seminars/healthcare2014/index.html
We’ve discussed elsewhere in numerous post that healthcare IT is a disaster and is now listed as a top risk hospital settings (too late for me to go through my archives but I am not making this up, I’ve had multiple posts on this issue). And the “higher co-pays” is classic supply-demand curve thinking. If you lower demand, of course prices will drop…
It’s kind of funny in a sick way because if “technology” is driving cost then it seems that perhaps technology is scarce and unable to keep up with demand.
It would seem to me that for improvement to occur you’d want “technology” to be a more common practice so that isn’t scarce.
Although in reality we’re not talking about a real market. In this pretend market they’ve created when I’m going to a doctor I know what’s wrong with me so I can price things. In most cases when you go to a doctor you have a list of complaints and the doctor works from there. Most people aren’t going to go to one doctor to test(providing his price menu is good), another for a diagnoses and then shop for another for a plan. That would be stupid. They usually go to a doctor who listens, sometimes tests, comes up with a diagnosis and then a treatment plan. It’s often done all at once, not broken up. Although thanks to meddling I have noticed that the doctor’s now charge me to read the tests they order . *shakes head* I actually think next time I head to the minute clinic I’ll ask them if they can just have the lab send ME the results and skip the charge(figure the odds that would be allowed to happen or should be allowed to happen.)
I think the continuing problem is attempting to impose market solutions where a market (in economic terms) does not exist. Do policies assume the existence of one? Sure, which indicates (to me) the term “market” is being used incorrectly to mean “non-government”. This demonstrates the thinking is ideological rather than technical and precise.
Fabulous post – many thanks Yves. Privatized medicine, the “market” solution, as public policy is necessarily extractive and predatory. Health care is not a service that we obtain from competing providers. If it were then we shouldn’t have any complaints about the less-than-rigorous disposal of human corpses. Somehow Americans do. Furthermore when we suffer or get sick we want help, and sometimes that help requires expenditures that no one individual can be expected to pay for alone. Especially under first world conditions, universal public health insurance, i.e. mandated participation and coverage for all citizens/residents is not just the morally correct solution – it is the economically correct solution, the one that produces the optimal price and distribution with desired levels of quality of a limited public good: qualified health care.
Adopting the “market” deceit precipitates “market” analyses when outcomes contradict ideology. The outcome in the US is glaringly at odds with ideology. Studies of costs in health systems must begin with explanatory variables that are discrete drivers. The discrete drivers in the US system are measures of extraction and predation: compensation levels among top predators.
Do all participants have access to identical information? No.
There is no market where participants have access to identical information. Participants have different information from each other and varied views from that different information is what makes a market.
The medical businesses in th US have gotten exemptions from what would be illegal conduct were you or I to try it.
What kind of market does the Mafia provide?
Of course there’s a Mafia Market – everyone gets to choose between a variety of providers – just like health care. The difference is that now the government is the “enforcer” and “collector” to make sure everybody pays one of the “providers”. In San Mateo County Ca, a lot of people (47 have plead guilty to bid rigging in Northern Ca) have been indicted for agreeing not to “bid” against each other – I see no reason that there has to be a formal agreement for this to work – Did anyone ever see a price war in the Drug Industry? or in Medical Care? How about any significant change that would affect pricing?
Got a link on that bid rigging?
Correct.
Healthcare is not the exception here. “Markets” don’t work in any sector. So to say that this is “not an example of a market failure” is simply in ignorance of what the Orthodoxy claim that markets are capable of.
Take a look at the oil sector and its collapsing bubble. Is that an example of a successful market? How about news media, education, telecommunications such as cell phones, cable TV, houses or automobiles?
Markets do not self regulate. They crapify and self-destruct, EVERY TIME!
It’s also worth noting that technologies, be they drugs or medical devices, are almost always built upon older technologies. Which is why the price of most drugs and medical devices should be trending down. You see this happening in other industries like telecommunications and computer software and hardware, but you won’t see this happening in healthcare. But why is this so, you ask? I’d say it’s mostly because, unlike telecommunications industry and the computer industry, the healthcare industry receives lots of federal subsidies. Then you may be tempted to argue that healthcare costs would drop to more affordable levels if we simply remove the subsidies. Well, that’s true, but it doesn’t make it right. Even if removing the subsidies were to make healthcare more affordable, you’d still have the problem of a large number of people unable to afford healthcare. It’s just morally wrong, cruel and inhumane to let people become handicapped or disabled or even die just because they can’t afford to pay their hospital bills or their prescription medicines.
The point that I’m trying to make here is that you can’t have affordable healthcare that’s both for-profit and heavily subsidized by the taxpayer. In fact, I will argue that the main reason why healthcare in the US is so outrageously unaffordable is because the healthcare industry has maintained its for-profit status while still receiving a growing number of subsidies from Uncle Sam. To make healthcare affordable, either you have to drop its for-profit status or get rid of the government subsidies. And because free-market, for-profit medicine is inherently inhumane, as I previously made the case, then we have no other choice but to have a healthcare system that’s fully and completely subsidized by the taxpayer. This means single payer is the only way to go if we want to rein in healthcare costs and achieve affordable healthcare for everyone.
And just because you have single payer healthcare don’t mean you also have to have a single healthcare provider — something which many on the Right can’t seem to get their head around. You can still have only one single payer and have multiple healthcare providers all competing with one another for a finite number of federal healthcare dollars.
Interesting read. I think the answer to not despairing about this kind of silly is to realize that they are simply part of the obfuscation (willing or not doesn’t really matter at this point).
The game is to keep discussion in the weeds rather than remarking upon the landscape as a whole, which is pretty obvious by now. For decades, the US has been spending too much on healthcare. The USFG spends more money per capita on healthcare to cover some citizens than other western nations spend to cover all their citizens.
No one inside the system can even acknowledge it because the soft corruption of careerism infects everything, from med schools to hospital franchises to drug dealers to equipment makers.
I have the opposite problem here. Getting doctors to test is like pulling teeth. For example, I recently was injured and have been diagnosed with cellulitis. However, there is a chance that it is osteomyelitis(the joint is inflamed and painful but the wound does not show as having penetrated there. They haven’t done a single test on me. No CBC to check my WBC. No labwork to check and make sure my Zen rock garden kidneys are doing okay. And definitely no x rays that might actually tell us if the area in question indeed needs to be treated. Nope. I’m doing 10 days of a second antibiotic after one day on an antibiotic that did not work and if after 10 days I’m still having problems I’ll get to make my third trip in to play “guess what’s wrong with me?”
You are part of the problem. Watchful waiting is cheaper and better than running a bunch of tests. If it is a superficial wound it will get better. The chances of an injury such as you describe leading to osteomyelitis are miniscule and there is no virtue in figuring it out early. If it is not getting better it might be because it was sutured so the bad stuff can’t get out or it might be because the wrong antibiotic was used or you might have diabetes or it might be a fungus. Interestingly the majority of soft tissue injuries do not need stitches and get better on their own if they are allowed to heal from below. Try telling that to a patient in an ER with a laceration. Patients expect and demand unnecessary care as well.
It isn’t a superficial wound. I was on antibiotics (Augmentin 875 mg x 2 doses) when my finger swelled up to the size of a sausage thus the diagnosis of cellulitis. When I made it to the doctor the second time ON ANTIBIOTICS it had already started to travel down my hand. Septra seems to have stemmed the redness but the joint is still stiff and swollen after 4 days on Septra.
I didn’t have any sutures. I don’t have diabetes that I’m aware of(might be able to know if I’m one of the millions running around with it undiagnosed had they actually done some TESTING…..but hey what do I know maybe doctors have special ways of sussing that out by looking at people. )
Watchful waiting may be cheaper short term but I question your opinion on it being better and cheaper long term. According to everything I’ve read if I indeed have osteomyelitis delaying treatment can impact the area that is infected. While my chances of having it are indeed fairly small(one of the reasons I grudgingly am waiting on demanding that they do further testing) if I have it my joint will likely become a CHRONIC problem. I fail to see how if it does become cheaper if I actually end up having a chronic problem in my affected joint.
Disclosure: I was a Navy corpsman (with a specialty in pharmacology)and an EMT. I actually tend to treat medicine as common sense. I know there is no cure for the cold or flu so I don’t bother to visit for those things(my exception is a kid with a 103 fever that isn’t being controlled well by motrin and tylenol. In that case I want you to pump some fluid in him and pretend that you can sympathize with a little body being exhausted.) I know how to treat sprains and strains.(ice, heat, motrin etc etc) I don’t smoke. I walk almost daily. Have a B/P cuff because of my migraines being accompanied by spikes in B/P and my family history of strokes.Despite that I have crappy genes. It irks me to no end that Doctors blame people for not being “proactive” about their health and then proceed to complain when they actually go to the doctor’s when something IS wrong. I’m not there because I have nothing better to do with the $20.(family day at the indoor pool, starbucks frapp and a book, redbox movie and a pizza all are preferences to sitting in a waiting room filled with germs) I’m there because something is wrong and I need help and I’d prefer not to have to make several trips(and co pays) to get it.
You are not alone and I did not mean my comment ad hominem……but the laymen who did not go to med school……..the lawyers…….the hospital executives…….the ER managers…….and the politicians are making the medical decisions nowadays. As long as the govt is paying for most of medical care one way or the other and as long as medical care is thought to be a public good like public school doctors should be on government salary just like teachers. Of course, the big fear is that then doctors would not work so hard…….so we have all sorts of artificial mechanisms to make them “productive.” I wonder why we don’t worry about firemen that way. Do we burn buildings down to get firemen out of the firehouse watching their big screen TV’s. One should be happy one does not need medical care. As you know half of the operations in the US are unnecessary in terms of health outcomes. On the other hand I cannot tell you how many times attorneys have begged me to put screws and stuff in people’s backs so they can get a big settlement and disability….convert a 30000 soft tissue case to a 500000 dollar case with the medical expenses on the governments dime………another unpublicized outcome of “healthcare” as well……..asset transfer from the government or employer or payer to the legal profession since they get 40% and don’t have to go under the knife.
My finger was the size of a sausage. Had I actually not gotten medical care the infection would have spread.
Yves, I disagree. I think this technology and the use of it in medicine would make the health of ppl better. How many times do ppl put off going to the doctor when they find a strange lump? What if doctors had the financial authority to really inspect all aspects of peoples health? Wouldn’t doctors catch changes sooner? Where they could begin treatment sooner and head off more costly treatment down the road?
I just think this is another “cut the benefits from the poor so that they don’t take from the rich”. Don’t tell me congressmen do not receive tremendous amounts of tests frequently so that any problems are solved early.
Careful what you wish for.
We already have an example with breast cancer. It turns out our use of Mammograms to find cancer catches far more early stages and are able to get women into chemo therapy sooner, and has a greater recovery percentage than in other countries with “socialized” medicine.
It sounds like a triumph of technology, right?
That is until you consider a counter study that didn’t find any difference in the breast cancer mortality rate. If the US system was truly better at finding and curing cancer, we should have a lower mortality rate.
The truth is that in the US, we have gotten good at detecting and treating false positives. And scientists are even suspecting that we may already have a natural immune response to some forms of cancer. We are likely finding and treating lumps that aren’t cancer or would go away on their own without intervention. So that isn’t really much of an achievement to run a woman through chemo and have her survive – when she never really had cancer to begin with. Of course she would come out of it as a cancer survivor.
But when it comes to real cancer, our technology and chemotherapy is no more effective than those used else where.
Worse yet, there are some concerns that regular mammograms may cause more cancer than it detects. This was real enough that the FDA felt it necessary to change the screening schedule.
One has to be carful that technology don’t give you false promises.
Here’s the first kicker: How many people actually shop around first and foremost for price ? Turns out they do if they have no to crappy insurance-especially when it comes to big-ticket items like surgery, where the overseas costs vs. domestic cost for the same procedure and care can vary up to 90%.
Just try to get up-front pricing – even form a vet for something simple like getting your cat’s teeth cleaned. Good luck….
You might be able to get upfront pricing. However, that assumes that the person walking into a doctor’s office knows what’s wrong with themselves to begin with and what kind of testing they’ll need. Many people go to a doctor to find out what’s wrong to begin with. How in the world are you supposed to price something without knowing what it is, how it’s tested and what treatment is used? If we all knew those things we wouldn’t need doctors to begin with.
I knew exactly what test I wanted. My doc didn’t know what the lab charged but she did know which were expensive–all of them. She is owned by a hospital, and has no say in anything. Ordinary plain Vanilla office visit went from $65 to $128!!! You should be able to have your test results sent via the ‘Health Portal’ if they have one set up. However, my ACA policy could never be bothered to tell me what, if anything, was covered so we did no tests. I have had none in over 10 years. Previously I had them several times a year. Oh well. Actually, it’s sort of been a relief not to have to sit and look at all those desperately sick patients in the specialist’s office. Kind of a preview of my likely future, you know? Now, I am about to get Medicare, but I still don’t know if I can afford the deductibles, co-pays, etc. If Medicare goes to some sort of HMO, I STILL won’t be able to see the specialists I was hoping to see, and my trusty old GP is on the verge of retirement. She is ill herself, and working so many extra hours just to fill in EMR crap–I think she is not getting paid for those hours, either–she ended up working full-time again. To escape EMR Hell, she changed her contract from 3 hrs twice a week to 1 hr, hoping to work only 5 hrs. As for your cellulitis, what tx would they use if you did have bone involvement? Would it be any different? If you’re really worried go to a specialist if you can. Ask your doc if soaking your hand in epsom salts would help/hurt. As for eye docs–yeah, what a rip-off! I finally went to the local glasses place, ordered cheap frames off the internet, and had him do the lens. Cost $100 instead of $600. Ugly frames, though!
I am shocked, SHOCKED, to find that artificial quantification of unquantified and effectively undefined variables is going on the The Dismal Pseudoscience. Now try getting someone to care that the economist has no clothes. All you’ll get as a response is, “It’s Economicstown, Jake.”
I wonder what you think of Obama’s latest announcement about our genetics see title of article below? I think large corporations will use the information to either suppress science if it benefits them or treat the symptoms if it benefits them. It will not be used for patient welfare and we won’t be able to have the information in our possession so that we can personally look at the data.
I took the 23andMe genetic testing before the FDA stepped in and told us we can’t have our health information (but Pfizer can) about ourselves because we can’t handle the truth. But I’m glad I have my information because I found out two specific health issues that could save my life. I was never going to get the information from maimstream medicine even though they should have picked up on it. He likely means precision-medicine a/k/a precision-pick-pocketing of patients.
Obama Announces $215 Million Precision-Medicine Genetic Plan
Effort Seeks to Take Advantage of Technological Advances to Analyze People’s Full Genetic Makeups
Naturally, the powers that be will take all necessary steps to make sure that the effects of this genetic lottery are fairly distributed.
Yes among the to big to fail pharmaceutical companies. The rest of us will not benefit.