Our mini-fundraiser for Water Cooler is on! As of this hour, 152CalPE donors — our goal is 275 –have already invested to support Water Cooler, which provides both economic and political coverage, to help us all keep our footing in today’s torrent of propaganda and sheer bullsh*t. Independent funding is key to having an independent editorial point of view. Please join us and participate via Lambert’s Water Cooler Tip Jar, which shows how to give via check, credit card, debit card, PayPal, or even the US mail. To give more, click on the arrow heads to the right of the amount. Thanks to all!
The IQVIA Institute published its 2017 recap, Medicine Use and Spending in the U.S. A key finding was the sharp fall in opioid prescriptions:
The report stated:
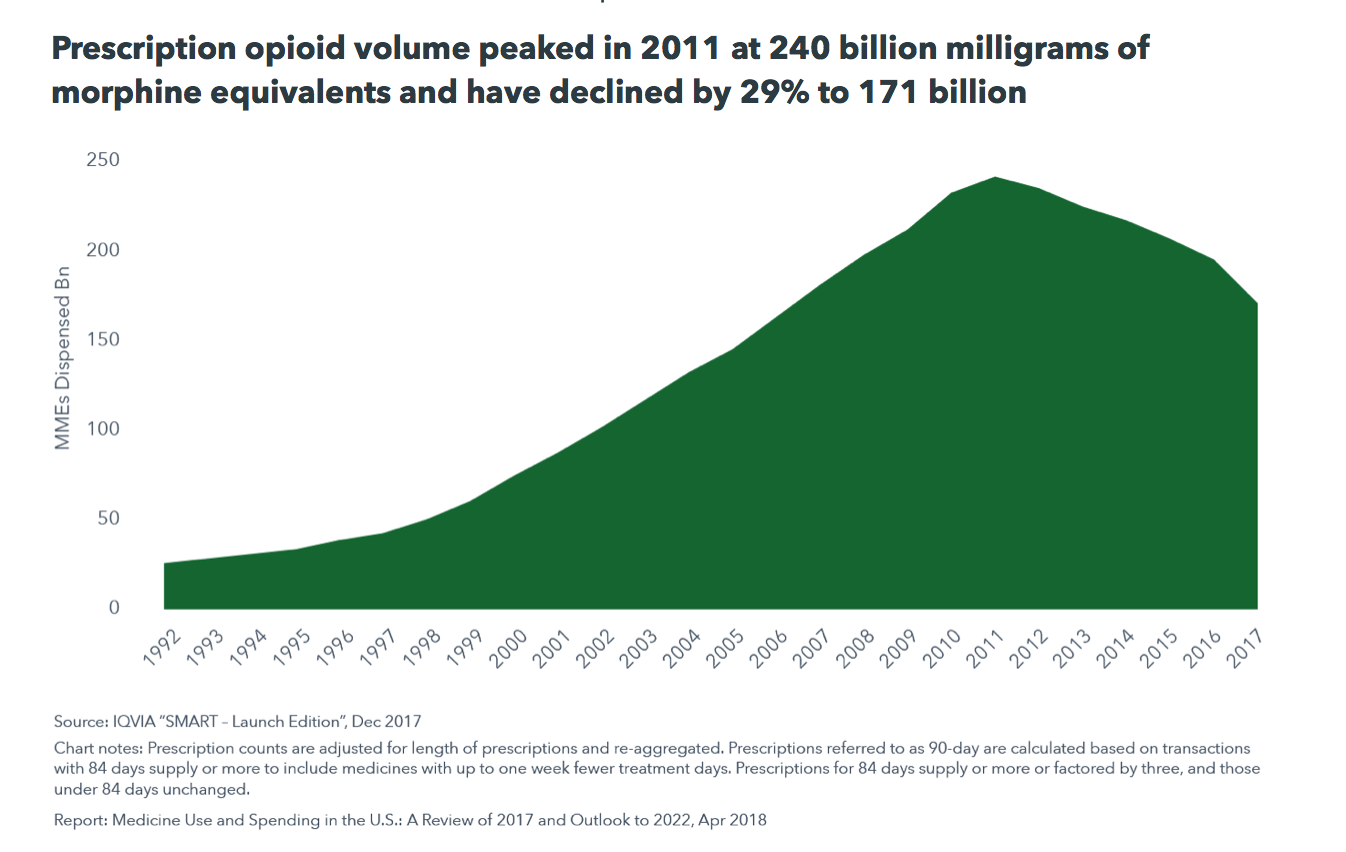
• Prescription opioid usage in the United States increased considerably from the mid 1990’s to its peak in 2011, at 240 billion morphine milligram equivalents (MMEs). It is now declining rapidly; the largest single year change in 2017 was a decline of 23.3 billion MMEs, or 12.0%.
• Prescription opioid usage was about 22 pills or 134 MMEs per adult in 1992 and rose to a peak of 72 pills or 1,011 MMEs in 2011. Usage has since declined to 52 pills or 676 MMEs per adult.
• Decreases in prescription opioid volume have been driven by changes in clinical usage, which have been influenced by regulatory and reimbursement policies and legislation that have been increasingly restricting prescription opioid use since 2012.
However, even with the marked decline from the 2011 peak, opioid prescriptions are only back to their level in, say, 2006 or 2007. The increase in dosage, from 134 MMEs in 1992 to 676 in 2017, is an over five-fold increase that cannot begin to be explained by aging Boomers with creaky joints and higher rates of overweight and obesity.
It is important to understand the degree to which drugs, like stocks, are sold. Pharmaceutical sales are widely recognized as the most sophisticated. For instance, ex military personnel are highly sought after as detailmen (the in-person sales force) because they are both willing to comply with the requirement to stick strictly to the scripts for marketing various drugs yet also be aggressive and persistent. Detailmen are given highly structured pitches, with an elevator spiel rolling into a one-minute version that can then go to three minutes if the doctor will give that much time. A typical detailman will sell at most three drugs, so an MD will often have more than one rep from the same company calling on him. The detailmen will also have that doctor’s prescription levels relative to that of his supposed peers, and the detailmen will try to depict him as remiss if his Rx level is lower than theirs.
Purdue Pharma, the maker of OxyContin, became the master of this game. From a must-read New Yorker story last year:
In the past, doctors had been reluctant to prescribe strong opioids—as synthetic drugs derived from opium are known—except for acute cancer pain and end-of-life palliative care, because of a long-standing, and well-founded, fear about the addictive properties of these drugs. “Few drugs are as dangerous as the opioids,” David Kessler, the former commissioner of the Food and Drug Administration, told me.
Purdue launched OxyContin with a marketing campaign that attempted to counter this attitude and change the prescribing habits of doctors. The company funded research and paid doctors to make the case that concerns about opioid addiction were overblown, and that OxyContin could safely treat an ever-wider range of maladies. Sales representatives marketed OxyContin as a product “to start with and to stay with.” Millions of patients found the drug to be a vital salve for excruciating pain. But many others grew so hooked on it that, between doses, they experienced debilitating withdrawal…
Andrew Kolodny, the co-director of the Opioid Policy Research Collaborative, at Brandeis University, has worked with hundreds of patients addicted to opioids. He told me that, though many fatal overdoses have resulted from opioids other than OxyContin, the crisis was initially precipitated by a shift in the culture of prescribing—a shift carefully engineered by Purdue. “If you look at the prescribing trends for all the different opioids, it’s in 1996 that prescribing really takes off,” Kolodny said. “It’s not a coincidence. That was the year Purdue launched a multifaceted campaign that misinformed the medical community about the risks.” When I asked Kolodny how much of the blame Purdue bears for the current public-health crisis, he responded, “The lion’s share.”
Perdue pitched OxyContin as a remedy for chronic but moderate pain, such as arthritis, when historically opiates were used for acute but short-term pain.
Purdue targeted less well educated doctors in areas where there were likely to be high levels of orthopedic injuries, such as factory towns. Purdue also presented the drug as providing 12 hour relief, when for many patients, pain returned after 8 hours. And Perdue knew that. What was their response? To tell doctors to prescribe higher doses. One doctor described this as a prescription for addiction.
Again from the New Yorker story:
Keith Humphreys, a professor of psychiatry at Stanford, who served as a drug-policy adviser to the Obama Administration, said, “That’s the real Greek tragedy of this—that so many well-meaning doctors got co-opted. The level of influence is just mind-boggling. Purdue gave money to continuing medical education, to state medical boards, to faux grassroots organizations.” According to training materials, Purdue instructed sales representatives to assure doctors—repeatedly and without evidence—that “fewer than one per cent” of patients who took OxyContin became addicted. (In 1999, a Purdue-funded study of patients who used OxyContin for headaches found that the addiction rate was thirteen per cent.)
Readers will no doubt point out that fentanyl and heroin are bigger causes of deaths than prescription opioids. But the prescription drugs are overwhelmingly the start of the path to addiction and abuse. From the Financial Times:
The decline suggests that policymakers are beginning to get to grips with a crisis that is killing more people each year than car accidents: 63,632 Americans died of a drug overdose in 2016, a 21.5 per cent increase on a year earlier, according to the Centers for Disease Control….
The number of overdose deaths caused by heroin has spiked because dealers are mixing the drug with fentanyl, a cheap and powerful synthetic opioid that is being smuggled from overseas.
Even though the majority of overdose fatalities are caused by heroin laced with fentanyl, most victims became addicted to prescription painkillers before progressing to the illegal drug. Reducing the number of opioid prescriptions is therefore seen as a major step in stemming the crisis….
Dr Andrew Kolodny, who studies addiction at Massachusetts-based Brandeis University, said: “We are still massively overprescribing, even if this trend is in the right direction. We have a long way to go before we are at rational levels.”
While this is a step in the right direction, reducing the level of opioid abuse will not remedy a big underlying cause, namely, that large swathes of rural America have become dead ends for many people as jobs disappear and desperation rises. But at the same time, other policies are helping reduce the demand for opioids for pain relief. A new study published in JAMA found a significant reduction in opioid prescriptions in states that allowed for any use of medical marijuana, with the biggest declines in ones that legalized dispensaries.
But this reduction in opioid prescription levels is still far short of where we should be. From the close of the Financial Times account:
Dr Kolodny pointed to figures in the Iqvia report showing that at the end of 2017, almost 3m new patients a month were being prescribed an opioid painkiller.
“If we are still prescribing at these levels, the opioid abuse crisis will never come to an end,” he added.


This is definitely a piece of good news, Next step should be a federal lawsuit against Purdue. The cause,more deaths than car accidents is strong enough i believe.
I disagree and the politicians need to stay out of my doctors office. I have used low level opiates for years without needing an increase. This is an individual person problem, there is no personal responsibility anymore and that needs to be restored. I also believe in natural selection, if you are stupid to wipe yourself out with them well its your fault not the doctors or drug manufacturers. Most of the problems today are from illegal street drugs not duly prescribed units.
With all due respect, you are a fool.
You clearly have no clue how much time and money Big Pharma spends in doctors’ offices pushing meds. There is no other industry which spends even remotely as much on in-person selling to small businesses. Drug companies spend more on marketing than they do on R&D.
And that marketing kills people. Bone up on Vioxx. It was an anti-inflammatory whose only natural market was for the small segment of the population for whom NSAIDs bothered their digestion. But the detailmen pushed it as better than other anti-inflammatories when that wasn’t true. Merck also cooked the data to hide that it increased the risk of heart attacks.
When Merck “voluntarily” withdrew Vioxx, the death rate fell that month. That’s how big the impact was.
See here for a long-form discussion:
https://mathbabe.org/2012/02/15/how-big-pharma-cooks-data-the-case-of-vioxx-and-heart-disease/
I also suggest you bone of up on Radithor, the drug that led to the FDA being given real power. This patent medicine, for which the doctor got a kickback, contained radium. Radium drink had been common but previously the doses had been so low that no one got hurt. Radithor was the real deal. Eben Byers, a rich sportsman, took 2-3 drinks a day after he had a shoulder injury. His teeth fell out and he developed holes in his jaw and skull and abscesses in his brain before he died.
This article says that 63,632 Americans died of a drug overdose in 2016. In the entire Vietnam war history, some 58,220 Americans died so overdose deaths are several thousand more annually than for the entire Vietnam war. That is not good. Even AIDS at its worst was able to kill only about 41,700 Americans in one year. At least with AIDS people were able to get together and force their government to take action. I have this horrible feeling that the reason that this is being allowed to continue is that it is being seen through the lens of a form of social darwinism. If true, then this might explain the disregard for so many tens of thousands of deaths each and every year.
It’s time to re-read the history of ACT UP, aka the AIDS Coalition to Unleash Power. Link:
https://endaids.actupny.com/
My condolences to all the people in pain who are now suffering because the DEA needed a domain expansion as marijuana wound down as a controlled substance.
Also to the Doctors who now have to avoid helping any patient who comes in with a back injury until months of tests because they could be DEA or State Police undercover agents.
Boo hoo nobody cares about this side of the story
Sorry, I don’t buy your story and you provide no links to support it. The fact is, and the chart and data show it as clear as a bell, that opioid prescriptions have gone up massively on a per capita basis. I know people with back and other chronic pain and they don’t have trouble getting medication.
Moreover, opioids are actually NOT well suited to treating chronic moderate pain. Frankly, I haven’t found them any better at treating acute pain (and I had two days of agonizing pain in at the end of February) than high doses of OTC meds (basically double the frequency of the recommended dosage, which can disagree up your stomach unless you have some food and/or rotate among meds and of course do not do that with acetaminophen, since high does will kill you).
And on top of that, the Sacklers funded tons of astroturf pain lobbying groups, and the fact that nothing like that existed organically prior to the throwing their money behind it says the idea that pain was undertreated is exaggerated (or perhaps more accurately, as my experience with pain meds shows, if you are in a lot of pain, there isn’t necessarily anything you can do about it if you aren’t willing to be medicated into unconsciousness).
You might be interested in this article form this month’s Harpers which discusses people with legitimate pain issues being denied medication: https://harpers.org/archive/2018/04/the-pain-refugees/
My initial reaction when I began reading it was “How much did the pharma companies pay you to publish this one?” because it does tend to gloss over the enormous opioid overprescription problem and ought-to-be criminal activity of the drug companies. But if you read the whole thing it does make the case that a pretty large group of chronic pain sufferers are now being denied the medication they need to function properly. Of course it does not mention any possible alternatives, and I’m not knowledgeable enough to know what those might be or their efficacy.
I do know that the overprescription has been a problem for years – over 10 years ago my wife went to the ER claiming pain of 2 on a scale of 1-10 and they handed her opioids to treat this very mild and temporary pain, despite our protests that they were addictive and unnecessary. We wound up disposing of them woithout taking any, but kaching for the drug companies anyway.
Kolodny and his crony will make a killing with the Warren 100 billion bill for suboxone clinic. Portraying intractable/chronic pain patients as addicts just enlarge the territory. Meanwhile the CDC guidelines are made into laws in different states and the DEA is so aggressive, doctors are giving up prescribing opioid. That’s the reality.
Addicts can have opioid and pain patients can’t. Patients are organizing now and putting pressure, just open your eyes and stop thinking it’s always big pharma behind. It’s not. The VA, Medicare, Medicaid are all pushing doctors to tapper off patients. And low dose opioid is actually safer for chronic pain than NSAID because of GI bleeding/liver/kidney toxicity.
I am putting the links in a separate comment because those that I posted previously were not published.
The Myth of What’s Driving the Opioid Crisis
https://www.politico.com/magazine/story/2018/02/21/the-myth-of-the-roots-of-the-opioid-crisis-217034
Persistence Pays Off For the Marine with Chronic Pain
http://nationalpainreport.com/persistence-pays-off-for-the-marine-with-chronic-pain-8835789.html
Unhelpful and Risky: Health Professionals’ Response to the 2019 CMS Plan
https://docs.google.com/document/d/11Tp7kAkMc9S2wVGklaSwVub5ABeJGl76M5bX8N4LBRM/edit
Are Prescription Opioids Driving the Opioid Crisis? Assumptions vs Facts
https://academic.oup.com/painmedicine/advance-article/doi/10.1093/pm/pnx048/3583229
Challenging the Chronic Pain Personality Profile
https://www.practicalpainmanagement.com/treatments/psychological/challenging-chronic-pain-personality-profile
Durations of Opioid, Nonopioid Drug, and Behavioral Clinical Trials for Chronic Pain: Adequate or Inadequate?
https://www.ncbi.nlm.nih.gov/pubmed/27880651
Can confirm, an elderly family member of mine with chronic debilitating back and ankle pain has been on opiods for years. That family member’s current (old) doctor understands that it’s either the pain meds or risky surgery or suffering. Now that doctor is retiring and has warned this family member that his/her new (young) doctor will almost certainly discontinue his meds simply because the doctor does not like prescribing them. I have seen what life is like for this family member without the meds, it is terrible. It’s a sad world when you have to suffer for no reason.
…
It’s a sad world when you have to suffer for no reason.
Yes! 0 strikes and you’re out. I suppose it’s not really for no reason, the crisis is a real one, but it sure feels like it when you suffer intense to excruciating pain because your dentist/doctor solves the over-prescribing stigma by simply eliminating synthetic opiates all together. In those bouts with pain, it’s bitter comfort that the doctor is so virtuous with your pain, but then the fact remains that his/her practice can and will suffer simply by prescribing opioids too frequently regardless of the merits. And yet, particularly when you’re not in pain, it’s not hard to sympathize with those who have become addicts due to indiscriminate or profit driven prescriptions (regardless of who’s at fault) and the suffering they go through.
My own complaint is simply that in this, like so many other things, we seem to do poorly at making adjustments. Instead, we reel from one (sometimes expedient) extreme to the other.
I injured my back at work in 2006. Three herniated discs and two of them were torn. The pain was unbelievable, to the point my daughters would leave the house to avoid hearing me writhing in pain. I would have to use a urinal as the pain of attempting to get out of my bed to go to the bathroom was atrocious.
I was out on workman’s comp for 2 years, permanent nerve damage. Eventually the company settled and I used the proceeds to go to college at 40 years old and get my degree.
When the company finally settled the MD who took care of me said that I will no longer prescribe you meds. I told him earnestly that I still had chronic pain 24hrs/7days/365…he said he would write me one last scrip.
I self tapered the pain meds, but was still having pain around every 4-6 hrs post med. Then I finally ran out and had my tylenol, motrin and heating pads at the ready.
After 7 days without the opiate medication my pain literally went away, much to my surprise. It was at this point that I realized my pain was a trigger for my craving of opiates. To this day I am able to work and function relatively normally. I do have bad days where my back goes out, but that is a distinct minority of the time. I do exercise with a focus on core strength and upper body strength to compensate for my bad back, but I never had surgery(and I would suggest to all not to have surgery as well).
I put myself through school and eventually became an ICU nurse in the Medical ICU of a level 1 trauma hospital.
I am by no means saying the pain is not real, because I myself felt that pain day in and day out…… I can assure you it is real. The question is what is triggering the pain? Is it really physiological, or perhaps psychological.
I see they have a new migraine drug, erenumab, that affects calcitonin. The cause of pain may be brain chemicals we are barely aware of at present. That would explain some chronic pain.
Yes, insurance companies and various other doctors associations have been holding doctor conferences preaching to doctors that they will lose their licenses if they do not cut their opioid prescribing by significant numbers. And then they are telling new doctors that they will go to prison if they get caught prescribing.
Second, as one of the points of the article state, most deaths are from heroin overdoses. So what happens. The doctor stops the prescription for Vicodin, then the person turns to heroin to stop the withdrawal symptoms. But the patient is not given options for treatment and they are left to deal with the addiction on the black market. And of course the doctors are not taking responsibility for what happens after.
Is there overprescribing going on? Yes. Are there issues with the use of the meds? Yes. But what is the problem with prescribing these meds? Are we saying there’s a problem giving a 80 year old pain meds? Are they the ones overdosing?
Or is all of this due to the fact that OxyContin went generic last year and so now the price of the med is falling, and so are the margins?
The hard answer here is that we need to admit that living with some pain will be the reality for a lot of people. Targeting a zero on the pain scale was never a successful strategy and it has done far more harm than good.
“Also to the Doctors who now have to avoid helping any patient who comes in with a back injury until months of tests because they could be DEA or State Police undercover agents.”
Not even close to the truth, but it sure does sound like the kind of redflag pill seeker talking points I watch out for when I see new patients.
Easy to say when you’re not the one in pain.
ain’t that the truth,lol.
I am fortunate to have the same doctor and pharmacist for 20+ years.
They know me, and know my situation.
went to see Doc the other day, for a spring sinus infection, and we agreed to up the dose of hydrocodone(to 7.5).
he said he worries about me when he retires, one day…that doctors are under such scrutiny and pressure that they often just won’t prescribe such medicine…even when they are effective…or, in my case, the only thing that has been found to be effective.
Last september, on my own initiative, I took a month long drug holiday…
doc had never heard of such a thing, but agreed that it was a good idea.
I went from 10mg, 2 times a day(with the occasional mid-day pill for hurricanes or ditch digging) to nothing but pot.
no withdrawal….except for the return of unmitigated pain(neck down,global arthritis). In october, i started on the lowest dose, again(5mg), and it turns out the holiday worked as expected.
it’s about managing my tolerance.
since I’ll likely hafta take this stuff for the rest of my life, I want it to continue to be effective….and I am averse to the “next step up the ladder” to oxycodone…which makes me itch and sleep too much.
I feel for the folks addicted to these medicines…and their street analogs… I know many of them, and have known many of the overdoses and suicides around here.
But their troubles are not my troubles, and I shouldn’t be made to suffer needlessly because somebody else had a bad time of it.
doc says that out of 400 some regular patients, he has 9 who are like me, on long term opiates. all are like me in that they are involved and aware of the problems…although I am the youngest(48).
I spent 20 years trying every alternative available to manage this pain….screwed up my gut in the process, with no relief, to boot. “Thinking happy thoughts” just ain’t gonna cut it.
This is what works for me…and I tremble at the thought of this new crusade….while it’s attempting to address a real problem, it is more likely to target me, than the folks it purports to be after.
I also think it is worth considering where the raw material is coming from. That chart shows that up to ten times the opioids were prescribed in 2011, and presumably the prescriptions were filled, than in 1992 — never mind the illegal stuff. The US is involved in a seemingly interminable war in Afghanistan. The connection betw the CIA and opium has long been alleged and some ‘conspiracy theorists’ even postulate FBI and DEA collusion. I will leave you to search out links. Some of the sources are pretty CT, and I don’t know who to trust on this, except probably not the CIA.
Point from the old cost accountant: that opium has got to be coming from somewhere, and somebody is profiting from it. If it is, say, a powerful nation’s clandestine service, in league with the worlds’ most powerful military ™, various government agencies and assorted ex-presidents, do we think there will be a solution to opioid deaths anytime soon?
it looks like the raw materials come from down under
I can’t seem to be able to copy an exact quote, so I will paraphrase. Tarmania produces 85% of the world’s thebaine, which is used in Oxycotin production.
Oxycodone wiki
Thank you, Kurtismayfield, I will look that up.
another interesting ‘what if’ for future historians to argue in addition to: what if in 2009 Obama got tough on the banks. what if in 2010 Obama got tough on opioid crisis?
Restoring a sense of optimism and genuine hope might have stopped some from pressing the nuclear button in the voting booth during 2016.
don’t forget regulators. *cough* cuz you know those dumb doctors—-they’re just so darn naive and gullible. how did they ever finish med school?
….served as a drug-policy adviser to the Obama Administration, ‘“That’s the real Greek tragedy of this—that so many well-meaning doctors got co-opted. The level of influence is just mind-boggling…..”
Big pharm = big money and influence.
Perhaps the biggest indicator of big pharm’s influence to me, is that no school, college, professors etc are issuing walkout threats, demanding enforcement or legislative action or threaten politicians with withholding votes on what is a national epidemic.
The movie, ‘Thank you for smoking’ was ahead of its time.
Hello, heroin!
The problem ain’t going to go away, it will just be channeled into new forms.
In January, the FDA Opioid Policy Steering Committee held a public hearing to
One of the speakers was Dr. Richard Lawhern from the Alliance for the Treatment of Intractable Pain. From the transcript,
Dr. Lawhern then goes on to discuss the questions in the REMS and how they impact pain patients. Bottom line from Dr. Lawhern,
Apologies for the length.
This is just my personal opinion re chronic pain & opiods. I decided last year to go on medical marijuana instead of slapping down nsaid’s like no one business. The marijuana allowed me to sleep almost through the night for the first time in many years. I had two major surgeries three years apart and with the second one this past January, I was very upfront with my surgeon, anesthesiologist, doctors, etc that I planned to continue with the medical marijuana rather than take opiods. I thought it really interesting that no one on my medical team even asked me any questions – i.e. how often do you take it, what are your pain levels at night (the most difficult time was for me to lie down), etc. I was not asked ONE question but…. I was given a prescription for oxycodone (90 tablets!) after my release from the hospital. I needed to use marijuana for the surgical pain for a couple of days at home and then went on to just Tylenol. I still have the oxycodone which I’ll save for when everything comes crashing down :) but for me marijuana was truly a life saver….
BTW – did you know that it is only the female marijuana plants that bud? Hmmmmm –
There will be dancing in the poppy fields around the world. All this cutting back done with out any support to addicts will drive them to other sources.
MME
The y-axis is MME (morphine milligram equivalents), not number of prescriptions. The MME reduction could reflect a trend toward prescribing lower-strength opioids to reduce the risk of overdose and death, as the CDC recommend. https://www.cdc.gov/drugoverdose/pdf/calculating_total_daily_dose-a.pdf
As David points out, the opioid crisis has a legal side and an illegal side. The drugs with the highest MMEs, from which most people are overdosing and dying, are illegal.
As HotFlash points out, the illegal side of the “opioid crisis” may have something to do with the US war in Afghanistan, where most of the world’s opium grows, and where heroin, a high-MME drug, is refined.
The “war on drugs” was a failure, but we learned something about “harm reduction” that we should apply to the “opioid crisis”.
One way to reduce harm on the legal side is to limit prescribed MMEs, as the CDC recommend. A good way to reduce harm on the illegal side is for the US military and their camp-followers to pull out of Afghanistan.
It should come as no surprise that the overdose death problem has followed the peak in opioid prescriptions. All those patients who used to get the legal stuff, especially those who were abusing the system at phony pain clinics, are still addicted.
Some years back, the government cracked down on the Hillbilly Heroin problem by shutting down the most egregious pain clinic operators. The addicted customers were not enrolled in detox clinics, so the street became the new pharmacy. The street stuff is much less reliable and is killing the addicts.
Yay! Prescriptions are down. However, the climb in overdose deaths was baked in the cake.
They are quite addictive, even if you’re strong willed it can take advantage of you. I thought I was immune to anything like this, but I got injured about a year ago and I was prescribed a moderate dose and that’s when I realized no one is immune to the effects of these drugs.
Once the pain started to subside I knew I had to stop because you can literally feel the pull. Good thing there are at least some checks and balances going on and there are plenty of lawyers https://www.kishishlaw.com/opioid-lawsuit looking to step up and and start some legal discussions on this.
I don’t know if there has been any headway, but it is a decent start.