The Wall Street Journal has broken an important story on Google’s foray into the medical arena. Without notifying patients or doctors, much the less obtaining their consent, the search giant has obtained the medical records of “tens of millions of people” in 21 states, all patients of Ascension, a St. Louis-based chain of 2600 hospitals.
Moreover, you can see that the effort is aggressive, with the aim of generating patient medical histories, linking individuals to family members, and making staffing and treatment suggestions….as well as identifying opportunities for upcoding and other ways to milk patients.
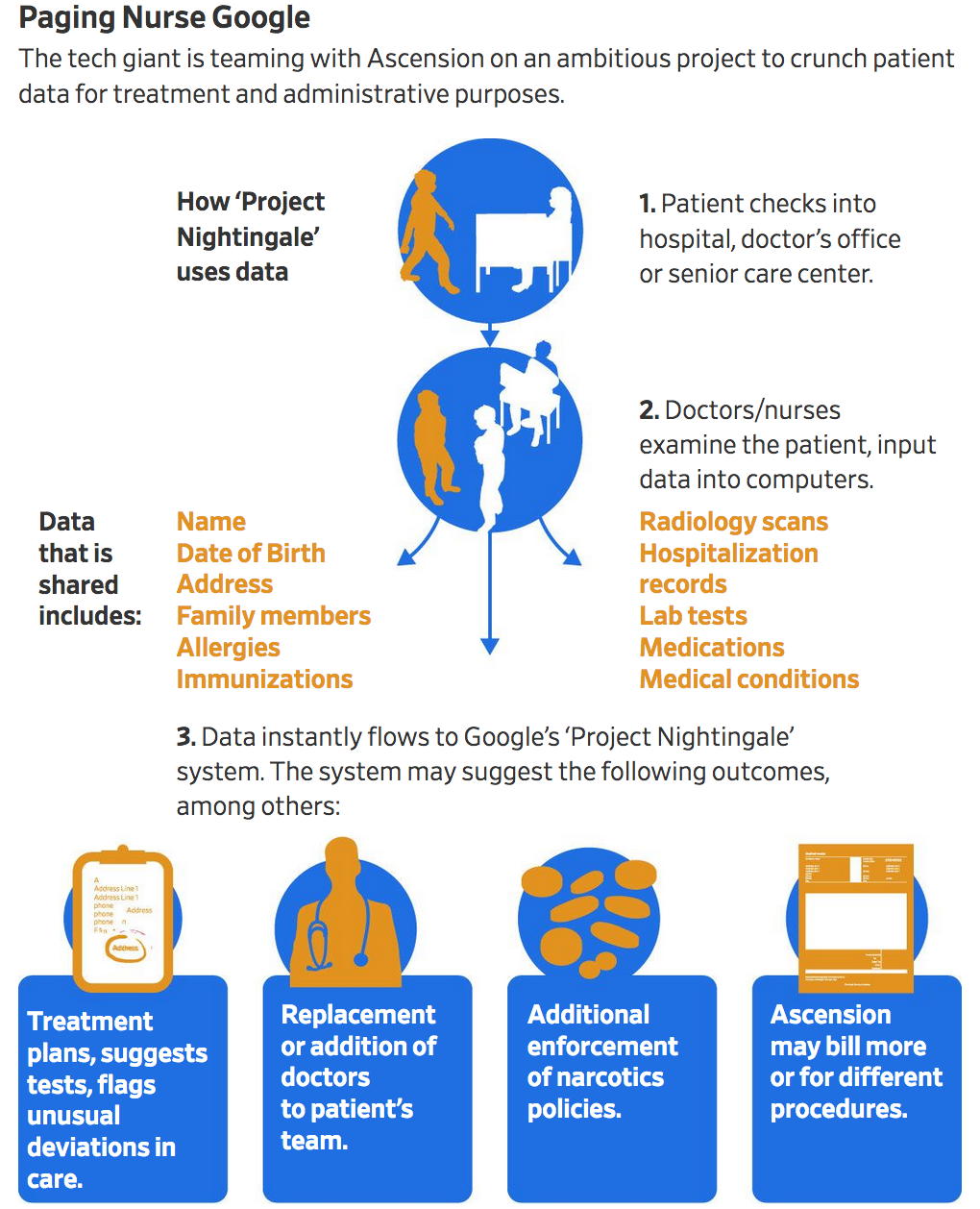
Google began Project Nightingale in secret last year with St. Louis-based Ascension, a Catholic chain of 2,600 hospitals, doctors’ offices and other facilities, with the data sharing accelerating since summer, according to internal documents.
The data involved in the initiative encompasses lab results, doctor diagnoses and hospitalization records, among other categories, and amounts to a complete health history, including patient names and dates of birth.
Neither patients nor doctors have been notified. At least 150 Google employees already have access to much of the data on tens of millions of patients, according to a person familiar with the matter and the documents.
And I wasn’t kidding about Ascension wanting to wring more out of patients:
Ascension, the second-largest health system in the U.S., aims in part to improve patient care. It also hopes to mine data to identify additional tests that could be necessary or other ways in which the system could generate more revenue from patients, documents show.
Yours truly regularly nixes doctor-suggested tests. It’s a no-brainer that it will become harder to just say no if you are in an HMO or PPO and Dr. Google disagrees with you.
Note that the project was secret until the Journal started digging. Ascension put out a joint press release with Google on Monday, which may have forced the Journal to publish the story before it had nailed down some final loose ends.
Specifically, the Journal repeats the claim from the joint press release that this data harvesting is permitted under HIPAA. The story not have any independent views, as in the expected expert quotes, but a bland, unsourced “privacy experts seem to think this is OK”. Huh?.
Google and Ascension are relying on the notion that Ascension can share data with a “business associate” under HIPAA, the misleadingly named Health Insurance Portability and Accountability Act, which is more a data sharing law than a privacy law. But notice the caveats on the HHS website:
The Privacy Rule allows covered providers and health plans to disclose protected health information to these “business associates” if the providers or plans obtain satisfactory assurances that the business associate will use the information only for the purposes for which it was engaged by the covered entity, will safeguard the information from misuse, and will help the covered entity comply with some of the covered entity’s duties under the Privacy Rule. Covered entities may disclose protected health information to an entity in its role as a business associate only to help the covered entity carry out its health care functions – not for the business associate’s independent use or purposes, except as needed for the proper management and administration of the business associate.
The Wall Street Journal article is explicit that Google is not doing this major project for Ascension for free out of the goodness of its heart, but to develop a marketable product:
Google has assigned dozens of engineers to Project Nightingale so far without charging for the work because it hopes to use the framework to sell similar products to other health systems. Its end goal is to create an omnibus search tool to aggregate disparate patient data and host it all in one place, documents show.
That runs afoul of the HIPAA requirements. The fact that Google is not getting paid does not give it the right to use its work for Ascension for any purpose other than to help Ascension.
Even though HIPAA does not conceptualize the relationship quite this way, it seems analogous to “work for hire” under intellectual property laws. If you are engaged by someone to produce a particular product, say an article, some code, a musical score, under a “work for hire” agreement, the company or person who engaged you owns the work product, except to the degree that you carved out specific rights (such as a right to reproduce for personal promotion).
It also appears that Google is sharing patient data more broadly within Google than is kosher under HIPAA. Again from the Journal:
Google in this case is using the data in part to design new software, underpinned by advanced artificial intelligence and machine learning, that zeroes in on individual patients to suggest changes to their care. Staffers across Alphabet Inc., Google’s parent, have access to the patient information, internal documents show, including some employees of Google Brain, a research science division credited with some of the company’s biggest breakthroughs.
The Journal points out that other health organizations that have been giving data for Google to chew on have, unlike Ascension, protected patient privacy:
Google appears to be sharing information within Project Nightingale more broadly than in its other forays into health-care data. In September, Google announced a 10-year deal with the Mayo Clinic to store the hospital system’s genetic, medical and financial records. Mayo officials said at the time that any data used to develop new software would be stripped of any information that could identify individual patients before it is shared with the tech giant.
One Wall Street Journal reader asserted that Google and Ascension are violating HIPAA:
John Travelstead
This is a direct violation of HIPAA laws. Google has no legal right to obtain personal health information.
The Federal government requires Business Associates Agreements for information sharing of personal health information and data between a vendor and covered entity to occur. GOOGLE QUALIFIES FOR NEITHER AND SHOULD BE REPORTED TO FEDERAL AUTHORITIES AT U.S. DEPARTMENT OF HEALTH AND HUMAN SERVICES. PERIOD.
The wee problem is that even if Mr. Travelstead is correct, HIPAA enforcement appears to be non-existant. The Wall Street Journal reported in 2007 that in a bit over three years, Department of Health and Human Services Office for Civil Rights had received over 23,000 complaints of privacy abuses, yet had taken no action. The only enforcement example listed in Wikipedia is an $885,000 settlement by UCLA over investigation findings that unauthorized employees repeatedly read protected electronic patient health care records.
However, Journal readers (at least as far as I read, and I got pretty far into the hundreds of comments) were without exception very upset about the prospect of Google having access to their medical data. Given that Big Tech is in the crosshairs of more than a few Congresscritters, one can hope that Google and Ascension officials will soon have to ‘splain themselves.
A few examples:
stuart jenner
NO. I use Google AdWords…They provide the data that they need in order to sell us….
No, I don’t trust Google with my information. They will set their systems to disadvantage patients, they will jerk partners around & and they will take away info people rely on in order to raise their prices — examples galore.
David Kessinger
Who will Google sell this information to? If they can’t sell it in some form they wouldn’t bother with it. Google at it’s core has no ethics beyond how to get money – to heck with who gets hurts.
STEVEN FRANKEL
This is not comforting. Rest assured this most personal information will be accessed by people you do not want anywhere near your personal information at some time. What would it take for Google or any other company or government employee to allow unauthorized people to your information? Probably not very much. And even a subpoena, how tough is that to obtain with the flimsiest of pretexts, especially with government employees not accountable for perjury, even to a FISA court? I would not give my doctor any information if it goes into a computer; I would rather pay cash and have no records other than the ones I would keep on flash drive.
It’s not hard to understand some of the motives for an initiative like this. As we’ve repeatedly posted, relying on the considerable work of the Health Care Renewal blog, electronic health records are a train wreck. They are designed around billing, not around doctor needs. Health Care Renewal has stressed that they if anything have made matters worse for doctors by diverting attention from patients and making it harder to find relevant information to the degree that they undermine care. They have been cited as a contributor to doctor burnout and even the reason some doctors stop practicing. An authoritative body, the ECRI Institute, even listed health care information technology as its number one patient risk in large health care organizations.
They are also often designed by relatively small players, so not only are they kludgy, but they are seldom compatible across health care organizations.
So you can see why there would be demand for a health care information system that is actually about health care. But given that Ascension has explicit upcoding and upselling motives, will that really result, or will this just be a less terrible, more portable version of the current EHRs?
Oh, and if you believe Google, this won’t just be about EHRs and helping organizations like
Ascension pull in more revenues (which translates into making health care an even bigger percentage of GDP), but bring techno hocus pocus to medicine. We quoted this section earlier:
Google in this case is using the data in part to design new software, underpinned by advanced artificial intelligence and machine learning, that zeroes in on individual patients to suggest changes to their care.
Notice that this is vaporware: Google hopes to do all of this but it remains to be seen what it can do. And it’s not clear that even with data on so many patients that it could develop decent AI for medical purposes. Bias in studies is already a big problem with medical research. One problem is that some populations are very much under-represented. Women are under-treated for heart disease in part because doctors see men as being at more risk, which is reinforced by studied being done mainly on men. Similarly, women have more trouble with hip replacements than men do because the studies were done on men…but women are not small men. They load their hips differently.
In other words, training set bias is a huge issue with AI, so even if Google has enough data to have a go at some conditions, there are still big risks with generalizing from the sample. And pray tell, who is liable when Dr. Google gets it wrong?
I happen to have the luxury of not being exposed to this sort of data sharing by virtue of not being in an HMO or PPO and always paying for my medical services (particularly tests!) and then submitting for reimbursement so my insurer does not have access to test results or MD notes. Nevertheless, I’m approaching Medicare age and soon won’t be able to escape this regime unless I leave the US and/or get a lot of my care abroad.
One practical suggestion, although it will be of use only when seeing a new doctor or joining a new health care organization: when presented with HIPAA forms, strike out the sections where you consent to sharing data with undisclosed partners and initial the strikeout. And do not ever provide your SSN on a medical intake form.
Regardless, this is a very troubling but not exactly surprising development. The fact that Google had a big security breach in 2018 involving over 50 million Google+ users will give opponents grounds for raising objections. But making a stink with your Senators and Representative is the best near-term move for keeping Google well away from your medical history.


Interesting selling point for M4A in this article – the software is written for the customer, the Insurance Industry. Patients and Doctors are just the product. A clean sheet medical care software that prioritizes patient care would save so much money while improving the quality of patient care.
Actually it’s worse than you would think. I got an earful regarding medical privacy from my sister, who works in billing at a major regional hospital. She told me last year, they no longer have an office full of women calling the insurance companies. Instead, both the hospital and the insurance companies have outsourced the entire thing to…. India. Natch, US data privacy laws don’t apply there. Instead of an office full of “her girls” she is managing a group halfway around the world. It boggles the mind, as if both the hospitals and the insurers weren’t getting enough money already– I have never witnessed such greed in all my days.
What kind of insurance do you have? Or, more specifically, how does a reader go about acquiring this sort of insurance?
Unfortunately, you can’t. I have a policy from 1987. It’s a legacy policy. My insurer keeps sending me letters trying to get me to drop it as arguably non-Obamacare compliant. My accountant begs to differ.
“always paying for my medical services (particularly tests!) and then submitting for reimbursement so my insurer does not have access to test results or MD notes.”
But the lab has your data in their computer system. And the actual lab work may very well be offshore.
Very unlikely. There’s a time limit for many samples before they become useless. Very few samples will last the days it would take to go offshore. At most in the context of the US it could go to Mexico but that would really only be viable for places near the border. That’s before we get to import laws related to human tissue and liquid samples.
Very few blood samples are actually looked at by a human in the case of routine cases. Only for more involved cases is there a human looking at anything. Some histology work may become offshored but the bandwidth and storage is massive so I don’t see it happening in addition to which that work is examined by Pathologists i.e. medical doctors and they will oppose it .
The issue is relating information across databases. You appear to have missed what torture that has been for the financial services industry despite having the identifier of a SSN to identify a unique person across vendors. No joke, it took a decade and a half for big banks and retailers to get any good at it.
I’m a cash customer. Labs are not set up to relate cash customer payments/tests to each other over time. I can tell that from what I have to go through the few times I have needed to get a duplicate receipt (the records do not have a patient ID and I have not set myself up with a “patient portal”).
They have astonishing difficulty in finding specific records of cash customers. And they don’t have incentives with cash customers to retain test results over time. Do you seriously think a third party lab would keep actual test results for one off test results for more than a year or two?
On top of that, Quest has many complaints about losing test results….on fresh tests! These tests are presumably almost entirely from patients where Quest bills the insurer and therefore has a patient account set up (as well as ones for the ordering MD):
https://www.consumeraffairs.com/health/quest_diagnostics.html
For the lab I use most often, they do not have the name of my insurer, much the less the ID with my insurer, which is what parties like Google will likely use to try to identify patients (I have had to get the procedure codes from the lab for each test and I submit those with my claim; the procedure codes are not on the cash receipt because the assumption is an insurer is not going to be part of the equation). And they don’t have my SSN. I don’t ever give it out in a medical context.
And I have used different labs (as in companies) as well as test centers.
How does the insurance verify the treatment or test is justifiable if they never see anything?
On a positive note, I think there could be great potential health benefits from AI. Though we will likely be faced with some interesting tradeoffs between privacy and health.
Or is it ‘privacy and death’?..
Maybe a motto for the Constitutional Convention circa 2030 ish?
I think as it stands, the trade offs will be between health and profit, or more accurately, between profit and more profit.
Health, like privacy, has taken on the same fictional or double speak status as words like liberty, democracy, and freedom.
If you think Google gives a rip about improving health outcomes (or Ascension, for that matter) I have a couple of bridges I’ll sell ya, real cheap. Any benefits to patients will be purely coincidental.
Modern “AI” is just pattern matching. All it does is fit data to an existing pattern.
Our medical system is rife with errors, bias, and intentional fleecing.
Given the inputs, what exactly do you think the AI is going to generate more of?
Being a geek, I’m willing to guess the AI part will be when to decide to taper or terminate certain options. There’s a datum that the last 6 mos of someone’s life is where the big expenses get racked up. Doubtless Google (or whoever) will be looking for the leading indicators that show you’re heading into your last 6 mos.
Patient health/quality really isn’t a piece of the puzzle. We have insurance companies and hospitals working towards lower costs. Doctors and pharma companies are trying to figure out how to push more services and drugs, regardless of how that actually works for the patient. This is the battle. Along with lawyers and politicians buzzing around like wasps to sting those who haven’t been vigilant enough to provide a “honey pot” or mount a vigorous defense against them.
Help me. I gather you are young and have not had much interaction with doctors.
I have the good fortune to have generally excellent health save orthopedic issues. Orthopedic issues ought to be the very simplest problems in medicine. Simple mechanical systems, hinges, levers, ball in socket joints. Good (X-rays) to what ought to be very good (MRI) imaging, so not a lot of mystery.
You cannot imagine what nonsense I have experienced with orthopedists. Just about none of them are capable of analysis. They tend to look at problems in an isolated manner when they aren’t.
Two examples:
1. I had plantar fasciitis, which is med-speak for “the bottom of my foot hurts”.
I was severely limited in how much I could walk for a year. I had to go to six orthopedists before I found one who looked at my gait and said, “Get in a low heel and wear orthodics.
This is a trivial medical issue that afflicts TONS of people. Six orthopedists in NYC, an area lousy with doctors, to get a productive treatment?
2. I had a knee debility which resulted in my not being able to stand for any length of time. No pain (I have a very high pain threshold) but I would favor the leg and my knee would get swollen, so this was not in my head.
The problem was to a significant degree the result of serious instability of my feet and ankles.
I spent ten years seeing everyone from MDs to witch doctors (the witch doctors on the whole were more productive). It was only when I got to a trainer who rehabs pro and Olympic level athletes (calling him a trainer understates his expertise; he has a masters in physical therapy and a huge network in the medical sports Mafia) that I got anywhere.
If you were able to get to MD notes on this stuff, which should not be medically hard, it would be useless. Contradictory and I can virtually guarantee stupid.
Quite honestly, my “miracle” cures have been thru chiropractic. Not all of them are great either, but I think there’s at least a tendency to look at the bigger picture, and to see what mechanically can be worked out. And he’s not afraid to say if I need to change or knock off some activity or food (I’m talking about you McD’s…). It is sad to think that an MD, with all that training, can still be rather ineffective. Or that you got 6 of them like that. Best to see some results of anyone’s profession before going there. Ironically Yelp might be doing more than any AI software can.
No, there will not be great benefits. why? Because big data loves looking at the average person to see how it can help the avergae person. But the average person does not get sick at an early age. The average person does not have Bipolar Disorder. There is no average person at all.
Garbage in, garbage out, that was the first lesson I learned way back in 1988 in Computer Science 101. AI is garbage becasue not only are the programmers garbage but so is the data.
And it is a false argument to say privacy and health are a trade off. We can have both but there is no profit in it.
Just a nitpick: it is HIPAA (Health Insurance Portability and Accountability Act), not HIPPA.
You’re correct. Post fixed. Thanks!
A policy Conceived, and deployed by those corpse-like Hipaacrites who reside on K st., at the aquiescence of that group of mortis CONgre$$ !
One wonders what tender bits of ‘privyness’ lay under Their golden threaded gowns.
Never ask for permission, always ask for forgiveness. The Silicon Valley-Wall Street motto.
eg, Uber-Lyft and jitney laws, AirBnB/local zoning.
PS, yes. HIPAA enforcement is non-existent (which is kinda funny given the massive amounts of money/resources devoted to compliance), thanks Bush-Obama.
They will change that idea when they are not forgiven.
No, they will just stop asking for forgiveness. “You’ve got no place else to go” is a unifying ethos of Silicon Valley and the liberal class.
Great! This information will end up on insurance company databases. You can just see the life insurance application denials and the claims of fraud when Auntie dies. And all the pre-existing conditions will be outed. Already, Long -Term Care is unaffordable. Watch existing LTC policy holders quit their plans when crooks like Genworth raise rates as they see all the new info on existing health problems.
My mother and father had LTC policies with a company that is now being liquidated. This company, like many other in the LTC insurance industry, is in trouble. Big trouble.
Why so much trouble? Because of the incompatibility of long-term care with insurance. The policies are sold to people who will eventually need to use them.
And that’s not the business model of insurance. It works best when it’s applied to infrequent events. For example, a tree falling on your house.
This is our future. Our personal “small data” being subsumed into cloud Big Data. Look at Epic Systems. They claim they hold over 56% of US patient medical records. A privately held company working under the cover of HIPPA. One could see our Epic cloud-based data being fodder for AI churning for their exploitation.
HIPPA provides a semi-permeable information membrane: all our data goes in via EHR and we the patient/data source, only gets to see a small, highly edited sample either via a doctor/care-giver or a sanitized “gateway”. Thanks to EHR and HIPPA we, the patients, have no control of what happens to our once-personal data.
Don’t even think elected officials can do anything about fixing this malignancy. Too much power and monies are with Hospitals/Providers, Healthcare Insurance, and EHR back-end systems. Look at MGH-BWH/Partners Healthcare/Allways/Epic for how these deeply incestuous relationships legally develop. Throw in Big Pharma too and the trap is complete.
Of course some will get served good medicine and get good results. Others not. We the non-HIPPA enabled don’t have a hope in hell to figure out why the difference.
Welcome to 21st century black-box medicine.
Google Delenda Est
dyslexia strikes again “HIPAA” not HIPPA
I’ve seen this movie before. After a lot of legal wrangling, Google will admit they they might have bent the rules a bit and will have to pay a few billion in fines which they will proceed to claim back on their next tax form. They will ensure, however, that they do not admit doing something illegal in court and so no executives will go to the slammer to stop this happening again. Google will also promise to delete that data.
Meanwhile, a copy of all these files will have gone to a set of their servers in a country that the US legal system cannot access where it will be analyzed further. Perhaps Google techs will be able to access it in California on a secured line. Non Disclosure Agreements will ensure that nobody talks about this work.
You know what will be the next big headline with Google and health services? It will be the discovery that Google has secretly purchased access to people’s DNA from Ancestry or 23andMe and now they will link your DNA with all those health records. Can’t tell me that they are not negotiating for it.
Google is a minority investor in 23andMe. I don’t have time to go digging about data sharing/purchasing, though. Maybe someone else can?
Thanks for that petal. Looks like it is going to be 23andMe and not Ancestry. Want a fun fact that I have just discovered? And I quote-
Sergey Brin, president of technology and a co-founder of Google is the husband of 23andMe Co-founder Anne Wojcicki. He previously invested around $10 million of his own money in 23andMe’s convertible debt financing, which was converted into Series B preferred stock as part of 23andMe’s Series B round.
How about that! Article at-
https://www.genomeweb.com/dxpgx/google-invests-another-26m-23andme
Oh yes, was aware of that for quite a while now. The companies have been attached at the hip from the beginning. Pillow talk? They are no longer together(Brin and Wojcicki). She was linked with ARod for awhile haha. Interesting group of characters involved.
My one regret was using 23andme, but I have to say it helped me so much it tempers the fact that I know parts of my “unidentifiable” genome is flying around out there somewhere. I think using gmail is more of a risk in reality. There is a lot more regulation risk pertaining to DNA data already on the books. Not saying it would stop them.
I was already degoogled before this Ascension news, but I just told my friends that I will not email them if they have a gmail address. A total boycott of google from me.
I work in healthcare IT, and I can certainly attest to the fact that insurance companies are keenly interested in acquiring clinical data. The term of art for this is “chart chasing”, and right now it is pretty much a manual process wherein the patient data is gathered by insurance company workers or their subcontractors reaching out to medical facilities for the patient data residing in file cabinets or computers.
It should come as no surprise that healthcare IT companies see a business opportunity in making this work more efficiently for payers – to suck in data at a rate that is orders of magnitude faster than currently possible. And you can be certain they are working on this right now.
What Google may or may be up to with patient data is another issue entirely.
Under HIPAA, a covered entity may acquire access to patient data under a so-called “purpose of use” that include Treatment, Payment or Operations.
Full article here: https://www.hipaajournal.com/purpose-of-hipaa/
If Google is developing software to analyze data on behalf of Ascension, that’s one thing. They should not have access to the data itself. It’s an important distinction. And I don’t trust Google to do the right thing.
As a patient, I would advise anyone who is worried about their data being shared with third parties to contact their doctor and ask them about their policy with respect to release of their data. You may find that the facility is releasing your information as they have an “opt-out” policy. If so, demand that your data not be shared without your explicit consent.
Google tried their hand at healthcare about 10 years ago with their failed Google Health project. They staffed the team with people who had no background in healthcare, but were otherwise the best and the brightest.
See https://www.mobihealthnews.com/11480/10-reasons-why-google-health-failed/
Incidentally, Microsoft’s Healthvault project only faired somewhat better. MS shutdown the project this month.
Finally, as someone who has worked in healthcare interoperability I disagree strongly that digitizing health data has been a one-sided disaster. On the contrary, giving clinicians access to health information about patients across different settings of care has in fact improved the quality of care and saved lives. I’m proud of my work in helping make this happen.
I should also note that making de-identified healtchare data available for population-based analytics is also a good thing. It’s not always about squeezing more $$$ out of patients.
“De-identified”, yeah right. I’ve seen study after study say you only need 3 data points to uniquely identify a person.
God bless the USA cause no one else will. We’ve all been thrown to the wolves.
See my comment above about my considerable experience with orthopedists.
There is way more garbage in, garbage out than you seem to appreciate.
Or as a biomedical engineer friend whose first job was with the NIH and the second, with Big Pharma, said, “Medicine is a medieval art.”
I don’t dispute that, Yves. One of the biggest problems with healthcare data is the quality of that data. However, I still maintain that facilitating exchange of data is still beneficial. You can contact me privately if you want more information.
Thanks for the post. The Affordable Care Act was an IT mess too. Perhaps Obama should have paid more attention during those meetings with what he called his “propeller heads” instead of playing with his Blackberry. But Al “streamlining government” Gore comes in for some blame too. These days we seem to barely regulate anything (except consumers trying to bring in drugs from overseas).
Some of us used to defend Google around here but that’s long gone. Bezos has talked about trying to get involved in health care as well. Perhaps Google felt they had to beat him to the punch.
Google also bought Fitbit giving them access to our exercise records
From my time in Stone Age big data, just because you’ve purchased a company doesn’t mean that its data will be compatible with the data you already own. Quite the contrary. And I shudder to think of the consequences of a cut-rate data conversion effort on medical data.
I whole-heartedly agree with you in a general sense here Lambert, but Google’s ability to convert and correlate that data is miles beyond what almost anyone else in the industry is capable. It’s not just a technological edge, they can pour as much money as they want into manual efforts and in this area they would spare no expense. And even if they are “wrong” who has the ability to call them out? It’s just a big black box.
All of these Internet Giants should be crushed until dead ! .. Until their collective multi-spectrum red terminator eyes cease to illuminate .. every damn one of em !!
I think we’re gonna need a much bigger pneumatic press ….
Unfortunately I think a different heroine provides the only real solution…”Nuke the entire site from orbit…it’s the only way to be sure”
https://www.youtube.com/watch?v=aCbfMkh940Q
What’s to prevent companies looking to hire people or credit agencies from obtaining this information? The credit reporting agencies have huge amounts of data on people – so why not add health histories? If you’re up for a job – the company wants to check out your health before it considers hiring you. One thing I don’t understand is if Ascension is not being paid for its patient information (unless I misread the post) what is it getting out of it? Not only do we have a “rip off” health care nightmare, Google will destroy the last vestiges of dr/patient care – and there’s not much left..
Cough cough, Fair Isaac sells consumer data, like Experian and Equifax.
There will be a lot of abuse before we see something good come out of the merger of big tech and health. A symptom checker at 96% accuracy rate will be good someday. So will transference of consciousness.
It reminds me of airplanes. Bombers and fighters came before truly functional commercial air travel.
Maybe that assumes that there is some kind of healthy progression from Very Bad to Less Bad — commercial air travel, as with ships and the sea where war and piracy paralleled “commerce” — and of course all that “commerce” comes at an externalized cost of billions of tons of CO2 and other problematic chemicals being injected into our bodies and our environment. I’d add that development of commercial aircraft like the DC-2 and DC-3 and Fokker Trimotor and the rest, and the rickety biplanes that preceded these, developed also on a parallel track.
My girlfriend works for a rather large health care system here in the Midwest. They rolled out a new check-in system where patients check in using an electronic device, pretty much bypassing the people at the window. A question pops up during the process asking the patient how they want to pay their copay or any outstanding balance. The patient can skip the question, but they have to jump through hoops to get around it.
So, not only are patients checking in on an electronic device on WiFi, they now have to pay before they see the doctor.
BTW, I have a service-connected disability so I use the VA for my primary care. I’m satisfied with my care at the VA.
Millennial Health bought out my PCP and uses that same system. It has leading questions just after check in and then displays a pharma ad. It is really crappy. Plus, do they disinfect those check in iPads every time?
Help me. This is not hard. Leave your mobile at home or profess only to have a dumb phone and make them check you in. Might take an extra 5 mins but I can assure you that the staff is better at circumventing the fields you want not to answer (so it might not take longer) plus you preserve employment.
The systems I have seen do not rely on the presence of a phone. You have a touch-screen terminal, and have to input your data (pay with your time to let the corporation offload data entry labor costs to the patient) and complete your insurance information and medical history and other stuff. Labcorp has put A version of these in, and cut their facility staffing “because of the savings” from the kiosks. Last time I went to the large Labcorp near me, there were two lonely, harried staffers who had to answer phones, do the blood draws, arrange the samples for delivery to the centralized actual lab locations, and also come out to help the infirm or unsavvy negotiate the login and data entry. And deal with “system crashes,” and all the rest. You cold tell that the workload was creating a lot of tension between the two staff — about who would have to carry the heavy end of the log… This is just like the “Self-checkout” terminals at Walmart and Home Depot. And one can bet that resistance may not be absolutely futile, but pretty much so.
Recall that those staffers are subject to the regimen of the New Business Model — more and more work from fewer and fewer employees under micromanagement to “metrics” for less and less pay. Making the receptionist-officemanager-med tech, etc, get up from a plethora of other tasks to ease some recalcitrant or reluctant or feeble “patient” (“health care partner”) into the condition (prepayment and personal data entry into Google-bound data systems) of a non-price-transparent “Medical consumption” system does not seem exactly fair. “Tax on time” applies many ways.
By the way, the VA has its own kiosk-check in system. They want to you present your VA authorization card to their laser scanner and then confirm that you are you —(must confirm birthdate, address, name, etc) if you want to get into the queue to be seen. At least the kiosks at Bay Pines give you a printout of upcoming appointments, a receipt for your claim for travel expenses (whose UNsurance covers THAT?) and a coupon for reduced price on coffee at the (privatized) Canteen over in the old main building. The VA still has sufficient staff, at least at Bay Pines facilities, to deal with those infirm and unsavvy old farts like myself.
Of course, the push is on to move ever more of the pretty good VA care into the “Community Care Program,” aka privatizing. A principal if weak benefit of the VA system is “continuity of care” via a cobbled-together (privatized installation) electronic medical record system, where nominally you can go to any VA facility for needed care and the docs and staff will have access to your likely lengthy and complex medical history. All this “Community Care Program” crapification and corruption is happening “transparently,” and despite pushback from veterans’ organizations. https://prospect.org/health/va-privatizing-veterans-health-care-launching-campaign-deny/
Oh, and the Dems supposedly are “fighting” for the veterans on this front: https://www.washingtonpost.com/politics/va-is-gearing-up-for-a-massive-reroute-of-health-care-to-the-private-sector-but-democrats-are-fighting-back/2019/03/21/637f732a-467b-11e9-90f0-0ccfeec87a61_story.html More sorry BS about how the Dems are “fighting for us.”
“Thank you for your service…”
Yes, I have seen those systems. Horrible. But the don’t ask for data you weren’t already providing.
No no no. Just because something is automated in medical care does not recuse doctors from upholding their Hippocratic Oath. First do no harm. Unnecessary tests are a harm. They are usually expensive, sometimes invasive, and occasionally very invasive.
It is also worth noting that Google recently purchased FitBit, released a new version of Google Assistant for your Android devices, and has ongoing work not only in genetic data analysis with Google Brain’s gene variant calling research, but also pharmaceutical work ongoing with Calico and Verily. Transparency regarding how data is operationalized between these units is absolutely lacking.
Can I ask why so many of us talk about “transparency,” as if that is some remedy for corruption and crapification? Do we really believe that if only we could see the interlocking mechanisms by which we and the planet are looted and our “rights” eradicated, that Something Would Be Done About It? There’s a fair amount of transparency in who is who in business boards and for those who can read between the lines of financial reports, and in other areas — you can follow the “trade press’ and see a lot of where trillions in stupid war toy expenditures end up. We got transparency around here and every other place I have lived where it comes to “legal announcements” and Requests for Procurement for public works and such — if you happen to subscribe to or have a service that is paid to track the content of those obscure local “newspapers of general circulation” that have become the only peephole into public business on a lot of fronts.
“Transparency,“ so easily gamed, ain’t going to stamp out corruption and Bad Acts.
Also I don’t think, as much as we would like to believe it, that the Hippocratic Oath actually has that “First, do no harm” in it. Here’s a link to both the classical and the modern version of the text: https://owlspace-ccm.rice.edu/access/content/user/ecy1/Nazi%20Human%20Experimentation/Pages/Hippocratic%20Oath-classic.html You have to tick the “modern” box to see the more recent version. Note that the classic version binds the new physician to take care of his teacher as in support him financially, and to give the teacher’s offspring free tuition and full revelation of all the newbie has learned. I see that notion is missing from the modern version, all you have to do is look at the tuition and fees charged by medical schools to see how far the departure has been…
What is even going on? Maybe we can contact Google support to find out.
.
.
.
.
.
[hollow laughter]
Please look into Ascention healthcare if you want to know how completely effed up this whole situation is!
https://www.stltoday.com/business/local/how-a-st-louis-based-health-care-system-became-one/article_c07ada87-ab74-5175-a0b0-5219dd7b95f1.html