Yves here. One of the things I can’t prove but know to be true is the great expansion in the number of MBA programs seen as having significant credentialing value has been to the great detriment of the US. When I was a kid, MBAs for the most part sought jobs in Wall Street, consulting, and big business. Over time, as more and more graduated, they increasingly colonized higher education, the health care industry, and not-for-profits. Roy Poses has been writing for years about their malign influence on health care.
Mind you, it isn’t merely that they have too little understanding of or interest in the business of the business. It’s that they also add a hugely costly administrative layer that focuses above all on increasing tis power and pay.
By Roy Poses, MD, Clinical Associate Professor of Medicine at Brown University, and the President of FIRM – the Foundation for Integrity and Responsibility in Medicine. Originally published at Health Care Renewal
Introduction: the Managers’ Coup d’Etat
As we wrote in 2006… in 1988, Alain Enthoven, an original member and driving force of the Jackson Hole group, published a short manifesto about “managed competition.” (Entoven AC. Theory and Practice of Managed Competition in Health Care Finance. Amsterdam: North Holland, 1988.) This is now not easy to find (but see Amazon here).
In this volume, Enthoven expounded on his scheme to wrest power over health care from physicians and give it to managers and bureaucrats. Enthoven thought of physicians as part of a tightly organized “guild,” that is, an economic alliance. His model for this was a pre-World War II document from a French medical society. Basically, he thought such guilds, which he believed to be in place in all Western democracies except in the UK and Scandinavia, were based on principles that were “not the natural expression of a free market in health care,” (p.33) and furthermore, that the guild model associated with health insurance “makes it very difficult for government or private payors to control cost growth,” (p.41) while they paradoxically “can also produce poor service (p. 42). To combat physicians’ overwhelming economic power, Enthoven called for managers to use “tools they have found to counteract market failure.” (p. 98) Finally, he suggested using a coordinated strategy to “break up the guild,” noting that “overcoming the guild has not been easy in the United States…. However, the guild has broken down.” (P. 122)
How much the guild has broken down, leaving health care leadership in the hands of managers, was illustrated by a recent research letter in the Mayo Clinic Proceedings (Logeman AL et al. Who Influences Health Care in the United States? A Study of Trends From 2002 to 2018. Mayo Clin Proc 2019; 94: 2360-1. Link here.)
Managers are Now the Most Influential People in Health Care
The authors studied the list of the 100 Most Influential People in Healthcare published by Modern Healthcare yearly since 2003. (The 2018 version is here.) They stated that:
Because it receives wide reporting and limited critique, this list stands as a useful longitudinal account of who others perceive to be in a position to influence health care.
Then,
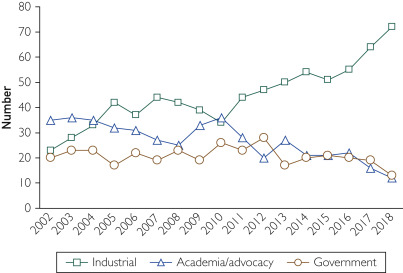
Using the published yearly list and the reported characteristics of the persons listed, we sought to determine the relative ranking over time, covering the period 2002 to 2018, of executives and administrators, academics and frontline advocates, and government officials. To achieve this, we determined the influencer’s sex and role (executive, member, independent, or other) as well as the sector from which each individual exerted their influence grouped into industry (nonprofit, for profit, payers, products, and providers), academia/advocacy, and government.
The results showed a striking trend over time.
There were 1700 persons named from 2002 to 2018, a minority of them women (range over the period, 17% to 28%). Most influencers are top executives from nonprofit health care provider organizations; their proportion has increased from 23% in 2002 to 72% in 2018, with an apparent substantial upward inflection in this trend since 2009 (Figure). This predominance appears to be at the expense of academics, advocates, and government officials.
A news article that featured an interview with Dr Victor Montori, the senior author of the article, noted in fact that the most recent (2018) list included quite a few CEOs of large for-profit health care corporations.
Among those topping the latest installment of the influential Modern Healthcare power index are the corporate heads of Amazon, Apple, Aetna, Humana, CVS and Minnetonka, Minn.-based United Health/Optum.
The authors concluded that
perceived influence over US health care of chief executives of health systems is increasing. To the extent that the ranking validly reflects influence, the sharp rise in the influence of chief executive officers at the expense of representatives of patients or health professionals may underscore the increasing industrialization of health care. It is not possible to find patients, patient advocates, clinicians, or clinician advocates at the top of this list. This trend placing health care influencers within C-suites, accountable to boards mostly comprising other corporate leaders, may explain the rise of business language and thinking
They suggested that it is possible that there is a
causal association between the concentration of executive influence and problems of patient care derived from efforts to optimize operational efficiency and financial performance, for example, clinician burnout, the heavy burden of treatment afflicting patients with chronic conditions, and the erection of barriers to care to optimize ‘payer mix.’
Dr Montori also said in the interview
Americans increasingly find themselves in a corporate-centric healthcare echo-chamber, one in which the public will increasingly approach tough policy decisions having heard only the viewpoint from the top.
‘The primary goals of CEOs are to advance the mission of their organization,’ Montori says. ‘If all that influences healthcare are the ideas of people who advocate for the success of their organizations, people who are not served by them will not have their voices heard.’
Furthermore, he suggested that the public may be befuddled by the current health policy debates, including those about universal health care and the possibility of reducing the power of commercial health insurance companies because
in the rest of the narrative all that they hear is about are the successes of biotech, the successes of tech companies, and the successes of healthcare corporations who achieve high levels of innovation thanks to the bold leadership of their executives. It’s why we have been calling for greater awareness of the industrialization of healthcare for some time now
Summary
The new study by Longman, Ponce, Alvarez-Villalobos and Montori adds to the evidence that health care has been taken over by business-trained managers, and in the US, especially by large commercial health care organizations run by such managers.
Since we started Health Care Renewal, we have frequently discussed the rise of generic managers, which later we realized has been called managerialism. Managerialism is the belief that trained managers are better leaders of health care, and every other sort of organization, than are than people familiar with the particulars of the organizations’ work. Managerialism has become an ascendant value in health care over the last 30 years. The majority of hospital CEOs are now management trained, but lacking in experience and training in medicine, direct health care, biomedical science, or public health. And managerialism is now ascendant in the US government. Our president, and many of his top-level appointees, are former business managers without political experience or government experience.
We noted an important article in the June, 2015 issue of the Medical Journal of Australia(1) that made these points:
– businesses of all types are now largely run by generic managers, trained in management but not necessarily knowledgeable about the details of the particular firm’s business
– this change was motivated by neoliberalism (also known as economism or market fundamentalism)
– managerialism now affects all kinds of organizations, including health care, educational and scientific organizations
– managerialism makes short-term revenue the first priority of all organizations
– managerialism undermines the health care mission and the values of health care professionals
Generic or managerialist managers by definition do not know much about health care, or about biomedical science, medicine, or public health. They are prototypical ill-informed leadership, and hence may blunder into actual incompetence. They are trained that they have a right to lead any sort of organization, which breeds arrogance. These managers are not taught about the values of health care professionals. Worse, they are taught in their business style training about the shareholder value dogma, which states that the main objective of any organization is to increase revenue. Thus, they often end up hostile to the fundamental mission of health care, to put care of the patient and the health of the population ahead of all other concerns, which we have called mission-hostile management. (Furthermore, it appears that the shareholder value dogma is just smokescreen to cover the real goal of managers, increasing their own wealth, e.g., look here.) Finally, arrogance and worship of revenue allows self-interested and conflicted, and even sometimes corrupt leadership.
Managerialists may be convinced that they are working for the greater good. However, I am convinced that our health care system would be a lot less dysfunctional if it were led by people who actually know something about biomedical science, health care, and public health, and who understand and uphold the values of health care and public health professionals – even if that would cost a lot of very well paid managerialists their jobs.
Maybe someday the top “influencers” in health care will actually be people who know something about health care and actually care about patients’ and the public’s health.


‘We’ve got to protect our phoney-baloney jobs, gentlemen.’ William J. Le Petomane
John Raulston Saul, in “Voltaire’s Bastards”, has produced an intellectual fireworks display that deals directly with the problem Dr.Poses sees pretty clearly. Endhoven proposes an attack on what he sees as a regressive medieval remnant, a Guild, an attack that has been pretty successful in a broad swath of our neoliberal world. Saul would recognize that attack immediately, and despise it. It’s what he wrote about with such fiery contempt.. And in my opinion, he’s right.
Managerialists, purveyors of “reason”, are leaving a trail of disaster in pretty much every area where their influence is powerful. Their ivy league, MBA-dominated education seemingly has failed to provide any sense of the human feelings and needs that must be an essential part of successful planning or policy. The bottom line trumps all else, and generates disaster as well as shareholder value. Treat yourself, as well as tantalize your wits. Read it.
In other words, the so-called physicians’ guild was replaced by an MBA guild. I’ve never seen an MBA contribute anything useful to an organization – their main skill seems to be driving companies into bankruptcy.
One wonders how many MBAs were involved in PG&E’s decisions to shift money from the maintenance budget to the executive compensation budget.
Thanks for the recommendation! – added to my list.
I would want a hardcopy but at $66 and up, it’s going to be a while for me. Of course, I could buy a Kindle copy for only $28.
Have you tried http://used.addall.com/
Lots of inexpensive HC copies there, it looks like.
Thanks for the suggestion. It looks like I can get inexpensive copies of all his books except for the one mentioned at the top of the post.
I do have a large, actually a gigantic of books in my to-read pile. I will just have to read all the other dozens of books while watching for a lower price. Or maybe I can get my financial aid in order so I will be able to buy it in two months times.
Health insirance CEO’s have bought up all the outstanding copies, which drives up the price.
They’re also probably paying Google to suppress search results for the online article.
Thanks for this post.
Two quotes that sum up much of the overpriced disfunction, imo.
Managerialism is the belief that trained managers are better leaders of health care, and every other sort of organization, than are than people familiar with the particulars of the organizations’ work.
Better leaders toward what goal?
– managerialism makes short-term revenue the first priority of all organizations
managerialism makes short-term revenue the first priority of all organizations
Except when it comes to manufacturing ideologies. There, they are quite capable of taking the long view with think tanks, generational influence (stacking) of the judical system, education, politics and policy and so on.* It’s not as if they are unaware of the concept of laying foundations. But short term revenue seems to be tightly coupled in their view to what they get to put in their pockets which in turn (perhaps ironically by the foundation builders: self worth by comparative metrics) has been tightly coupled to their perceived worth as human beings. (Ultimately, I believe, the phenomenon of comparative metrics literally projects the homeless -or in this case the paucity of care for whole segments of society- into existence and maintains their numbers in relation to those of the “managers.”) Interestingly, the mix of origins, whether such seminal ideas (“eat your vegetables, think of the starving Chineese”) are vernacular and borrowed and repurposed or canonical and disseminated helps in no small part to obscure the process.
*Even if the managers are not always the drivers, they are aware of the value.
Managerialism reworks old lessons. A person was once admonished to avoid doing to others what was objectionable to himself. That morphed into rationalizing the notion of objection in two ways.
First, sociopathic or psychopathic understanding or, if you will, misapprehension, widened the notional application.
Second, elision of messy details allowed rewording so that a person acted before being acted upon.
When doctors graduate from medical school with $500,000 in debt, what is the primary lesson they have learned?
In response to US economic sanctions, Cuba has adopted a state policy of training doctors in order to use those human skills as an export resource. By most accounts, that policy has been very successful on multiple levels.
Fighting corruption is the main problem, whether that corruption is public or private- both are unacceptable as we are painfully seeing today.
Citizens need to demand that their government works directly for them, not thru some obscure intermediary.
whenever i run across an article about a doctor shortage, i immediately think of the obvious solution: make more doctors.
it’s not like there’s no money for it…it’s about priorities and choices.
somebody chooses to make more MBA’s and grand larcenists and warmongers.
and, Norb…in addition to the Cuban Organic/Sustainable Ag revolution, the Doctors for Export thing is my favorite thing about Cuba.
The number of doctors, or residency spots, is controlled by Congress. The number could be increased if Congress wanted it to increase.
I read KevinMD now and then (website for docs).
Yes-indeed. That such a poor, oppressed country like Cuba can achieve those results puts to shame the argument that the US cannot achieve similar results. Such arguments are just flat out lies or distortions at best.
As for agriculture, I can see a massive jobs program that puts willing people back onto to land in order to build a more sustainable system.- and restore the environment at the same time. There needs to be a healthy connection between rural and urban environments that works. Government jobs at environmental restoration- like firemen, police, or military. Unless you have a citizenry dispersed on the land-enabled to make a living, how else is that ever going to happen?- it won’t. Ecological destruction follows. Farmers know this better than anyone. The Get Big or Get Out farm policy can be said to be a long term disaster. We need to support a Get Small policy. Forget wanting to be a millionaire, and just focus on living a healthy productive life. What’s wrong with that?
I think another shock is on the way regarding the US military which follows along these same lines. The resources wasted on our military jobs program, and its lack of effectiveness, will put the US in dire straits when it finally dawns on those in power that they have lost influence in the world and cannot force their will on others without dire consequences. More massive waste, to no positive, long lasting results.
Then again, other countries are forging ahead and provide plenty of examples and food for thought. Russia’s S-400? What sane person can argue that bombing people you don’t like or disagree with is a good idea. It only makes sense when it costs you next to nothing, or you have never been on the receiving end of such treatment. Its taken time, but this warmongering is another failed policy if anyone cares to look.
Only the well healed can afford to keep their eyes and minds closed.
When in history has so little gained seemed like so much? We really do live in a land of illusion, where most people are pulling in different directions.
I’m ready for a politics that gets people moving in a common direction that doesn’t require killing someone- whether quickly with a 500lb bomb, or slowly with economic starvation.
The thing that really irks me about our so-called health care system is how clueless and ineffective it is. Story from this past summer:
I was called back east to tend to my 93-year-old mother. Six weeks after I arrived, she was dead.
Before she died, there were two trips to the hospital. Between those two trips, there was a nursing home stay for rehabilitation.
Puh-leeze.
It was obvious, especially to me, that my mother was dying. She only weighed 77 pounds and wasn’t eating or drinking very much. The nursing home’s proposed solution? “We’ll try tube feeding.”
That one sent me through the roof.
Another thing that I found infuriating: Mom was sent to nursing home rehab because insurance would pay for it. Forget the fact that she was dying. Which meant that rehab was pointless.
During the second trip to the hospital, I was finally able to convince enough people that, yes, my mother was dying. It was hospice time.
I can’t say enough good things about that hospice. In addition to taking great care of my mother, they also looked after grumpy and worn-out Arizona Slim. They also provided pastoral care to my mother’s caregiver, who was distraught over the fact that, no matter how hard she tried, she couldn’t get Mom to eat or drink.
If I had the power to make the American health care system over again, I’d design something that looks a lot like that hospice. The people who tended to my mother were caring and attentive, but they weren’t pushy.
Sorry to hear about your mom. Peace and grace to all who surrounded her.
While I think she came at it from the Most Wrong-Headed Direction, Sarah Palin, bless her eagle-eyed clarity, was on to something when she mentioned death panels.
Obviously, the Death Panel needs to be the presumably compassionate immediate family and caregivers, not an ‘industry’ that seems to be driven by stripping familial resources.
Many States are enacting laws that make a pain-managed passage from life on earth illegal.
Obfuscated Life Panels.
Peace to you, AS, and all who are going through the familial upheaval of mortality.
I am sorry about your experience.
These types of situations are where it is very important to know what kind of intervention the person will want. All family members should discuss this amongst themselves so that, at a minimum, they will at least be cognizant of the person’s wishes in various medical scenarios. This is where advance directives can help.
Additionally, you never know when physical therapies will be effective or not.
I write from the opposite side from you. My Dad has Parkinsons and dementia. He almost died in the summer of 2016. He had a bad reaction from Bactrim – remember that name because it should not be used to treat elderly patients. He was in the hospital, written off by the staff. One of his doctors decided to try an appetite stimulus, and lo and behold, he recovered.
My sister was determined to keep him in nursing homes over his objections; these places basically immobilize patients (causing more and more weakness). So I brought him to live with me, where he got appropriate therapies and strengthened a great deal.
Over the years, he deteriorated such that he needed almost full time care (at night, he would get up frequently to pee). After two hospital stays in 2018, he went into re-hab and regained his strength. My brother and I bought him a recumbent bike, which he used daily (sometimes twice a day), and that kept his strength up. Over that time, I had also placed him into two different care centers (he didn’t want to go but was always mad over the expense of home care). The care was ridiculous; one was downright neglectful (I still have to file a complaint against them) – and both were supposedly upper end care places. At the more expensive place, he deteriorated to the point that he couldn’t even hold his head up to eat and leaned way over in the wheelchair – all in 30 days time. I took him back home; he improved immediately and received therapies and regained his strength.
The difference is that he wanted to do the therapies and worked hard to regain his strenght – despite his dementia. He is now in a memory care center (a small one – only 16 residents) because of his objections to the cost of home care. His bike is there, but the seat adjustment broke somehow (he probably broke it); now he has a small blood clot in his lower leg – likely because he can’t exercise. And his strength is declining again. Institutions simply will not provide the exercise needed for elderly patients.
Your mother sounds like she was ready, but IMO, people should be careful in drawing that conclusion without at least trying a few therapies first and seeing how that goes and how the patient responds.
My mother was indeed ready. To the point where she had this to say during her second trip to the hospital:
“I want to die.”
A few days later, she did.
My father died in the Canadian healthcare system in the spring. He was in pain due to neuropathy from diabetes and failing due to congestive heart failure. He ended up on palliative care and would have been transferred to hospice if he had survived long enough for a bed to open up. The “Death Panel” was a very caring doctor and excellent, experienced nurses. They were very focused on keeping him alive and trying to get him home while there was still hope but also clearly laid out the options to my father and family regarding palliative care and hospice when we asked about it. It was our family’s decision in the end, driven by my father’s wishes. The hospital had standard protocols in place for when the decision was made, so the transition to palliative care occurred over a period of hours with little fuss.
BTW – the bill for the ambulance trips and hospital stays in the last month or so was $0. They have no concept of balance billing is.
One of the key lessons in the Canadian healthcare system is that politicians are much more responsive to the public than healthcare corporations. It was clear that there were funding issues creating shortages of nurses on the floor at times, but they are looking into that and solutions may require small increases in funding (and taxes). Since the provincial system only spends at a rate of about 50% per capita compared to the US system, small amounts in that funding would not get them anywhere close to US costs.
Healthcare is not like other “industries”. When someone gets ill, he just wants to get better. No matter what it takes or how much it costs. Unlike when shopping for a car or widescreen or whatever, when people get sick they generally are not going out to do a multicriterion analysis to determine what doctor, hospital, treatment or therapy is the most economical or cost-effective. They just want to get cured and stay alive.
This simple fact of life seems to be lost on these bloviating MBA’s who feel they are uniquely qualified to run a public works department today, a hospital tomorrow and a steel mill the day after. To them it’s all about “the art of management” and they “don’t need to bother with the details”.
I wonder when it will dawn on organisations that lots of MBA’s are more economic and organizational deadweights than valuable contributors to their products or services.
It can’t be soon enough.
> This simple fact of life seems to be lost on these bloviating MBA’s . . .
On the contrary, this simple fact is so well known, it is the point of medical price gouging, whether by MBAs, doctors, big and little pharma or Pirate Equity buying up medical services like ambulances and charging $5,000 for a five minute ambulance ride.
The alarm bells should be clanging loud and hard when the first two medical influencers as listed in the post are Amazon and Apple, before any of the rest of the parasites within health care.
I ask, when has Bezos ever dealt in honest faith with anyone? The whip hand has an ever growing list of backs to whip.
My dad used to say whoever controls space will control the weather and whoever controls the weather controls the world. He was wrong. If the t.v. doesn’t tell us what to do it doesn’t get done. Sad.
In *healthcare*, it seems the lower you go on the ladder; the more genuine the care about patient’s welfare…
above the RN, CNA, technician, and housekeeping levels: its the benjamins.
…There’s no money in caring; only in billing.
I had to laugh when I saw Modern Healthcare referenced here. They need money to keep their site and articles going,even publishing quite a few “sponsored content” items from United Healthcare/Optum. I like the way they still confuse so many in the fact that they don’t realize United owns Optum. Mayo Clinic and Optum could not be any tighter, look at the retired Noseworthy CEO of Mayo, sits on the board of United Healthcare. This has gone on for a long time. You know of course this CEO and the last CEO of United Healthcare came from Arthur Andersen, famous from the old Enron days, so don’t expect much better over here.
I did a talk at a doctor’s convention a couple years ago and explained a lot of this since I have been writing about the healthcare algo cartel for years and how the software and algorithms developed early on by United allowed them to move into the driver seat years ago, everywhere. CMS is running so many of their quant business models, it’s not funny. United Healthcare made former CMS head, Andy Slavitt from UNH old Ingenix days and Senator Warren’s daughter very wealthy in 1999 when United bought this discount RX company.
I’m sorry I just laugh at half the stuff at Modern Healthcare anymore as they just want clicks like everyone else and you can easily see that when there site is now loaded with “sponsored content”.
“Algorithms, Scoring Metrics, Privacy and more in today’s Healthcare business world–The Healthcare Algo Cartel” if you want to watch it, about the 4th post down on front page. Stop kidding yourself and see the reality of who’s in control of all of this with powerful algos containing chocolate covered dopamine (makes the clicks taste better:) and computer code with the perceptions created that are not real but do disrupt the real world. They both retired by I had a couple of insiders at CMS both validating and confirming my content on all of this for 10 years. They found me at the Medical Quack blog and there’s no where else where you can find over 10 years of blow by blow acquisitions and explanations of how United used code and algos to profit and grow and it all came off our backs and out of our pocketbooks.
Who’s influential? United Healthcare is the largest insurer in the US, Anthem Blue Cross is number two and they are somewhere between 1/3 and 1/2 the size of United. There’s history on all of there if you want to research and see how United built themselves off the ignorance of the American Public for a lack of a better way of putting it. The virtual perceptions they sell don’t do a lot for you but they sure increase their profit and dividends keeping folks in the world of Operation Perception Deception.
From a post on your blog:
This should not really come as a big surprise as what hasn’t the pharmacy benefit managment business touched? So what is OptimizeRX? Most have probably not heard of this software but it is a connect to EMRs that will send your prescription right to the pharmacy. Oh, now you say, well the PBMs do that and they do but what they have been missing is a way to collect data on patients who are not using their PBM prescription card or those who do not have one. It’s all about getting more data about you to “score” and of course sell those scores to insurers and other interested parties. Once the pharmacy has the transaction, it does not fall under HIPAA rules as it’s a prescription, linked to an EMR to provide a transaction. As we all know, your medications in an EHR are protected but again, I’ll repeat this for those who still think HIPAA is covered at the pharmacy, it is not. It’s been a sore spot for years with privacy.
Yikes and thank you, bookmarked.
I don’t disagree that healthcare CEO’s tend to be MBA’s who are focused on the bottom line but I would just say that this problem is systemic …these manager types are struggling for survival…their businesses are capital intensive with extremely long cash cycles and they are in constant negotiation with insurance companies and government payors who tend to have even greater financial leverage; in addition most mid-sized hospital systems are outsized by larger health systems and have to manage with extreme vigilance in order to have any hope of independence. It’s a tough nut to solve…if any of these CEO’s were to take a different tack…ie address some of the problems raised in this study…they would immediately be sacked or merged or would introduce financial distress to their organizations…which would be bad for employees and patient care. I don’t have the answer…just sayin’
At the risk of seeming simplistic, –medicine as an artifact of late-stage capitalism seems to look a lot like the tragic rat race you describe. And there’s a couple dozen national systems that have fairly good, workable answers chugging along over here. At the age of 78, I abjectly thank anyone who might be listening up there that I’m working with the very imperfect but still wonderful French medical care system.
as i’ve related before, i rode the elevator, alone, with a few suits when wife was in the hospital…and i didn’t hesitate to engage them>
all of them obviously meant well, in their hearts(methodist hospital, “serving humanity to honor god”), but when pressed about the total disconnect between healthcare as a market, and the vast majority of folks i had talked to around that place who had no money or insurance…shrugged and blamed it on “The System”….which is apparently, some supernatural being that we mere humans have no control over.
to their credit…and thankfully!…they “forgave” our enormous hospital bill…just wrote it off…
but that just adds another layer of incomprehensibility…how many such write offs are there in a given month—keeping in mind the prolly 80% of people i randomly engaged with who couldn’t even begin to pay for their or their loved one’s care? how does that fit into the “business model”?
the one suit who shared the elevator with me the longest(i had rode to the top floor to see what was there(suits in suites!)), i actually put the question to him:” if this is a market, where’s the price discovery?”
jaw literally on his chest, gobsmacked, and taken totally off guard that a shaggy, rumpled hippie guy should use such terms.
he conceded, smiling weakly: “well, hell…that’s a pretty good question.”
i doubt that any of these 5-6 guys were the Top Dogs….but there was humanity behind their eyes, which is at the very least cause for hope.
the question is how to overcome the paradigm enforcement they swim in, and support them if/when they do decide that enough is enough(petit bourgeoisie is where the more successful revolutions come from, after all)
Yes the poor CEOs, making high 6 or 7 figure salaries. Even if you are correct about what they need to do to keep their fiefdoms solvent, couldn’t they simply do it for less money, thereby increasing the chances of solvency? But somehow these MBA types always consider themselves the top talent who simply can’t be paid a penny less than what they’re worth. And when asked impertinent questions about it, as Amfortas mentions above, they blame it on the system without having the self awareness to realize that they are what constitutes the system.
+1
The system is trending toward monopoly in pharma, insurance, etc. Break up the monopolies (does United Healthcare really need to control 60% of the market?) and re-introduce some competition, more options, etc. I don’t disagree with the comment “it’s the system”; the system is monopoly, break that up. Couldn’t hurt. Might help. And that’s before getting to M4A.
That’s why the breakup has to be done comprehensively, from the outside.
And yet that was true, was it not? The physicians in the US went out of their way–using the AMA–to fight socialized health care and defend their economic interests and succeeded all too well–opening the door for more enthusiastic capitalists to take over the “industry” (now the correct term). From that point of view the health care mess is merely another manifestation of the neoliberal destruction of the social contract.
What social contract in healthcare was destroyed? The physicians guild is ancient. The oath of Hippocrates reads more like a fraternal agreement than a social contract. Many pre-med students I knew felt a definite calling to help and serve — I don’t remember any of them getting into medical school. Did Neoliberalism destroy a social contract or take over an existing center for rent collection. Even a guild and ancient and powerful as the AMA can co-opted and taken over — ‘managed’ — by Neoliberalism.
Supposedly the AMA blocked govt healthcare plan during Truman administration–long before current neolib version. Their licensing restrictions play a big role in high healthcare costs (according to Dean Baker, not mere me).
Of course most doctors have altruistic motives, but the money issue intrudes and can also lead to bad medicine.
I am not sure most doctors have altruistic motives — or let’s say they have some altruistic motives. The pre-med programs where I attended college were known for the degree of cut-throat competition that went on. One common way to eliminate a competitor for the limited number of ‘A’s handed out was to sabotage their genetics lab experiments — genetics lab was a requirement for most students on a pre-med curriculum. I worked at a hospital as a graveyards switchboard-operator/”guard’ to save money for college when I take a little time off. The station nurses told some interesting tales about the altruism of the doctors at the hospital where I worked. One doctor figured he could pay-off his Winnebago by removing a hypochondriac patient’s gall bladder — and did. I think the system for selecting candidates for medical school does a very nice job of eliminating all by a small number of those who want to enter medicine for purely altruistic motives.
Of course the AMA blocked a govt healthcare plan during Truman administration. That is no evidence to suggest the powerful AMA was not co-opted and taken over — ‘managed’ — by Neoliberalism … after Truman. As far as I know. until Neoliberalism possessed our government, the AMA has never favored any policies that might undermine the power of physicians to exact rent for their services.
Of course the AMA blocked govt healthcare plan during Truman administration. That is no evidence to suggest the powerful AMA was not co-opted and taken over — ‘managed’ — by Neoliberalism … after Truman. As far as I know. until Neoliberalism possessed our government, the AMA has never favored any policies that might undermine the power of physicians to
Funny that. It was not all that long ago that there was a movement to make organizations much more flatter and to cut out all the middle, unproductive ranks. This is going the other way to insert in another layer of management, along with all their ancillary staff, to impose their own philosophies onto health care. What I resent so much about modern management is this idea that you can take an MBA and plug them into any industry to get them going. And they convince other leaders to think the same way. It does not matter what industry they are in, it is all about “products”. You talk to wine-growers and they talk about their “product”. You talk to Boeing and they talk about their “product”. It can lead to all sorts of blind spots in their industries as Boeing alone has proven.
Of course there is another aspect to this problem and that is the education industry that turns them out. Higher education has been very successful over the past few decades in inserting higher educational requirements into professions that did not require them. As an example, nursing was required in recent times to have a university degree to become nurses. Now that has happened, nurses refuse to empty bed-pans as they are university graduates so other staff has to be hired to do those former duties. Upgrading educational requirements always sounds like a great idea unless this ends up warping a whole economy with a parasitic class of managers that are not as educated and qualified as they think that they are. And now we are seeing the result.
It isn’t recent that nurses were required to have a unversity degree; I know nurses who got their degrees decades ago.
Also, I don’t know that the bedpan thing was created by nursing refusal or by people deciding that well-paid nurses’ skills were not being used well with less skilled tasks. Some stratification seems to make some sense.
Karma. I’m reading this while attending the annual meeting of the Association of American Medical Colleges, where managerialism is decried. Sometimes. But do they really mean it?
I believe they do mean it. Speaking to doctors, the managers have made their lives miserable (although still well compensated). The doctors couldn’t imagine the increased technology in medicine decades ago with the increased dependence on expensive pharmaceuticals and diagnostic equipment when they successfully held off socialized medicine decades ago. At that time, they were still largely a manual profession with stethoscopes, X-rays, and the first generation of antibiotics. Since that time, they have just become another cog in a very complex and expensive machine as they have become a much smaller percentage of the healthcare cost. That is why the manager have been able to take over to ensure “optimal allocation of resources” and “profit maximization”. Basically, the doctors won the battle and lost the war.
My top, middle, and bottom line has always been that my and my family’s healthcare should NOT be someone’s profit center…period. One of the goals established in the very first paragraph in the US Constitution is to “promote the general welfare”. If health care isn’t promoting the general welfare of our fellow citizens, then I guess its Neoliberalism Rule #2…..
In my head, when I read MBA, I hear a worker character from a B&W movie sneering “college boys.”
Of course, there must be a gratuitous dig at Trump:
Managerialism has become an ascendant value in health care over the last 30 years. The majority of hospital CEOs are now management trained, but lacking in experience and training in medicine, direct health care, biomedical science, or public health. And managerialism is now ascendant in the US government. Our president, and many of his top-level appointees, are former business managers without political experience or government experience.
Managerialism has been rampant everywhere – and we’ve seen the result with huge increases in prices, crapification of products, and contempt for the consumer. It’s everywhere, from the boeing manufacturing to medicine to grocery stores to software to government.
To attempt to dump this decades long trend on a president of 3 years is ridiculous. Government crapification started years ago (lead in water, anyone?). A handful of non-politicians appointed here and there is very unlikely to stop the trends; there is too much money to suck out of the system, and the crapifiers know it.
For those not in the know, residency slots are paid for by MediCare. Teaching hospitals are allowed to charge more to pay for the education, care, and feeding of residents.
If we’re all someones “asset” are we not then simply “slaves” for sale to the highest bidder?
Forward!
Into the past!
In related news, Kaiser Health News reports that the CEO of the Kaiser Foundation Hospital/Health Plan makes $16 million… A good gig for a non-profit.
Kaiser has also commmitted $295 million for “naming rights” to a sport stadium as well as $900 million for a new Oakland office building…
Say it’s not so! So?
So! One year’s compensation $16 million (I hate the word ‘compensation’ what is the $16 million compensating for?)
Rules for the designation non-profit – What might they be? Seems like bullshit. Kaiser put it’s name on a small stadium in Santa Cruz too.
Yet another example of neoliberal ego insecurity discourse embedding itself to seem relevant/productive while denying what they are actually doing is rent-seeking via public asset tripping. If one does an internet search for ‘the fourth factor of production’ numerous entries say ‘entrepreneurship’ (managerialism). This is the inverse of what the classic liberal conclusion came to, embodied by Simon Patten, the chair of the Wharton School of Business at the University of Pennsylvania, the first one in the country at the time. He pointed to the fourth factor of production was government infrastructure (transportation, utilities, education, banking, health care, fire and police, housing, insurance). These ‘natural monopolies’ could be run at cost, thus reducing overhead costs to the public and private business.
But, of course, Patten was eventually forced out by ‘business managers’ seeking to profit from the utility sector…
Neoliberalism: A method of re-establishing a landed gentry in an industrialized democracy.
Ok:
This: “The new study by Longman, Ponce, Alvarez-Villalobos and Montori adds to the evidence that health care has been taken over by business-trained managers, and in the US, especially by large commercial health care organizations run by such managers.” is actually a letter to the editor of “Mayo Clin Proc. n November 2019;94(11):2360-2365 letter 2019 Mayo Foundation for Medical Education and Research.” It may be a page and a half and not much of a study. It was written by “Adam L. Logeman, MS, Oscar Ponce, MD, Neri Álvarez-Villalobos, MD, Victor M. Montori, MD, MSc of the Knowledge and Evaluation Research Unit, Mayo Clinic, Rochester, MN.
There is “no” Longman. I first thought it was Phillip Longman of the “Best Care Anywhere” (referencing the VA) and it took me a while to find this letter to the editor as Dr. Roy Poses does not reference it anywhere that I can find. It may be there and I have just missed it. However, the letter to the editor can be found here: Who Influences Health Care in the United States? A Study of Trends From 2002 to 2018
Since I write on pharma and healthcare supplies having been in the manufacturing side of it, I do have an interest in how healthcare is managed. If we can recall, Dr. Donald Berwick upon departure as the director of Medicare and Medicaid said:
Most recently and in conjunction with Kocher, Berwick co-authored a brief While Considering Medicare For All: Policies For Making Health Care In The United States Better It is a transition to single payer or Medicare for All. It is worthy of consideration.
Doctors play an important part in the care and the inefficiency of it. There is a constant battle occurring with my PCP as he refers me to a specialist and I say “why?” Doctors, hospitals, and ACOs are a part of the inefficiencies and waste. Phillip Longman and Timothy Noah might tell you with concern to the care their hospitalized wives received and Phillip documented in his book
The WHO has a technical paper out which basically said R&D costs are recouped in a median period of 2 to 5 years due to the magnitude of sales revenue. The ICER issued a paper also and you were kind enough to carry it, The paper identified 100 drugs for which the pricing increases exceeded twice medical CPI. Of those, it pulled the top 9 drugs and examined them as to why. The ICER dropped two of them as their was new evidence which “could” justify the increases. The other 7 drugs had no justification for their increases.
I am in a battle with my Congressional person and staff to get them to recognize the issue of costs and pricing, Without the recognition of the former, you are tossing a dart at the latter.
My apology for dragging this out. I do not see a study or a paper. I see a letter to the editor which identifies an issue I would acknowledge. My keyboard giving me issues and I am going back to a hard wire.
And this is what happens when you put an expert in a room with modern managers-
https://www.youtube.com/watch?v=BKorP55Aqvg
Managerial Philosophy
I know an awful person from the Williams College/Mckinsey/BOA track who calls himself a “banker” but seems to specialize in creating Gantt charts for coders to finish website projects that he takes credit for…
Speaks in batches of manager-techy cache-phrase gibberish without any meaning or original thought, At all.
Couldn’t wrap his head around the fact that banks create money from thin air per bank of England report and blames voters for bad policy despite the fact their votes have exactly zero effect on policies the people they voted for actually enact….
Told me he can “manage” any enterprise better than the people who have years of expertise in a field because he knows how to “manage people” and doesn’t need subject matter competence…
Loudly trumpeted his allegiance for obama to anyone who would listen on the sole basis that the First Black™ president has, per se, brought more justice around the world, then quietly voted for trump because it would improve his bottom line…
This. Is. The. Liberal. Mentality.
It never ceases to amaze me that writers of otherwise excellent articles like this fail to fully research key figures in their story. Alain Enthoven was a premier RAND Corp. nuclear war strategist who was Deputy Assistant Secretary of Defense from 1961 to 1965, and Assistant Secretary of Defense for Systems Analysis, from 1965 to 1969. Body counts in Vietnam? Yeah, that’s Enthoven. I remember about two decades ago reading that Enthoven was changing his focus from the military to health care, and physically shuddered in revulsion at the likely consequences.
..and led by officers sworn to a hippocractic oath…
This is blatantly obvious in the mid michigan area. Doctors are part of companies where they all share offices, staff, etc. Doctors are nothing more than employees, serving the needs of their bosses who run and own the doctor company. If the bosses say “cut costs by cutting prescriptions & care”, then they follow orders or else they don’t get bonuses or risk being fired from the company. The opioid epidemic is an example. Insurance companies (not just medical but malpractice etc) are raising rates and cutting reimbursements to doctors who prescribe these meds, even if they are medically justified. These items affect the bottom line of the company. So doctors are managed to cut prescribing so that the bottom line stays high. (We won’t get into the profits they made while freely prescribing).
All the while ppl cry that the ACA or universal health care were going to get between the doctor/patient relationship. When in reality, this relationship has been destroyed by other means.