Needless to say, Boris Johnson having become an unintended participant in his Government’s earlier “herd immunity” strategy might seem to constitute sufficient evidence that this wasn’t a great idea. Admittedly, the UK switched course rapidly, but the damage of the initial barmy idea was done. As summarized in Fortune:
His government was pursuing a strategy that rested, at least in part, on the idea of shielding the most vulnerable members of the British public from infection while allowing a large percentage of others to catch the virus. The hope was that most of these people would experience relatively mild symptoms, recover, and wind up immune, stopping the virus’s further transmission.
But this kind of herd immunity, experts said, could require upwards of 60% of the population becoming infected. Herd immunity as a deliberate policy, epidemiologists said, is usually achieved through a vaccination program. It was untested as a tool for responding to a pandemic.
Epidemiologists and medical experts immediately assailed the plan as a dangerous gamble. And, when epidemiologists at Imperial College London, who had been advising the government on the likely spread of the virus, updated their models to take into account information on the number of hospital patients requiring intensive care in Italy, it became apparent that the minimal, voluntary restrictions Johnson had suggested were unlikely to save the NHS from being overwhelmed.
And the cost will be high. From the Guardian:
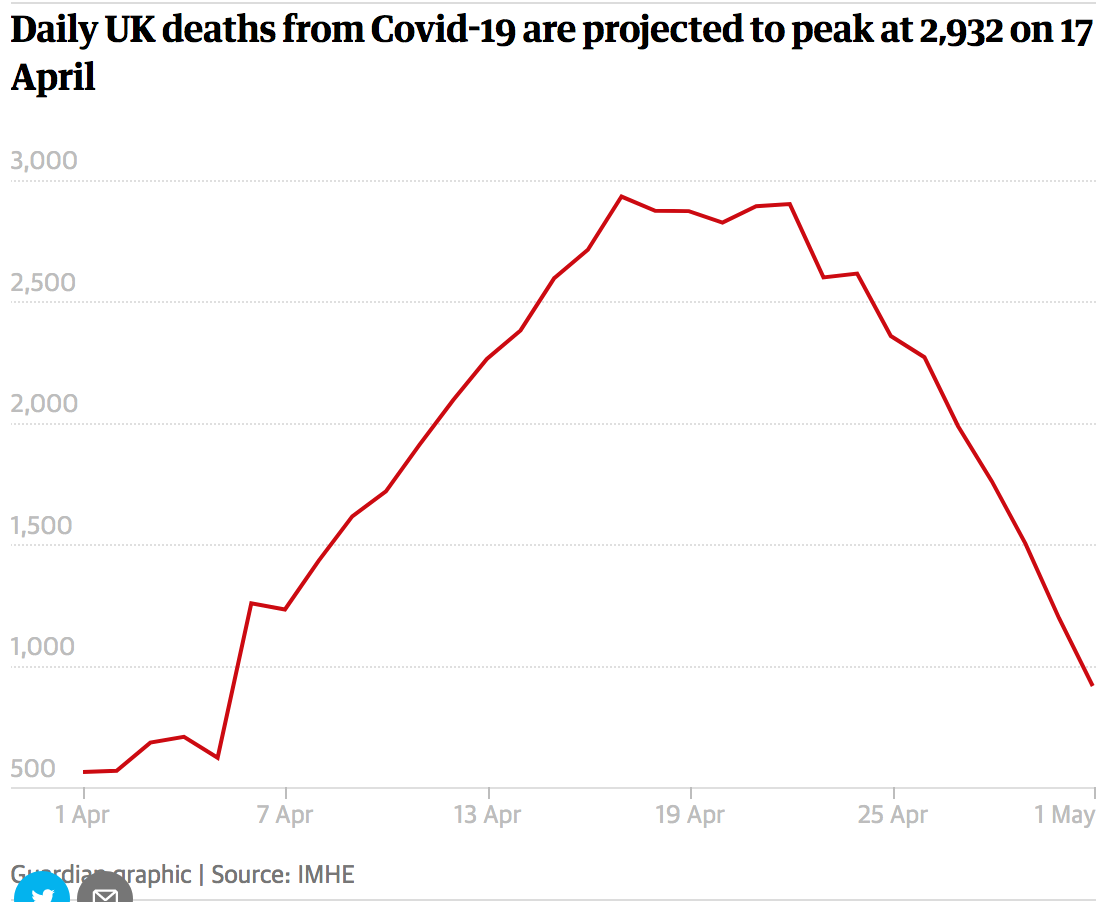
World-leading disease data analysts have projected that the UK will become the country worst hit by the coronavirus pandemic in Europe, accounting for more than 40% of total deaths across the continent.
The Institute for Health Metrics and Evaluation (IHME) in Seattle predicts 66,000 UK deaths from Covid-19 by August, with a peak of nearly 3,000 a day, based on a steep climb in daily deaths early in the outbreak.
The analysts also claim discussions over “herd immunity” led to a delay in the UK introducing physical distancing measures, which were brought in from 23 March in England when the coronavirus daily death toll was 54. Portugal, by comparison, had just one confirmed death when distancing measures were imposed.
Readers also felt compelled to weigh in on the barminess of this approach. From Dr. Larry B via e-mail:
The notion of herd immunity in the present context seems to have been advocated by Dominic Cummings, which after serious criticism he appears to have abandoned. Well, it shouldn’t have been advocated, in the given context, in the first place, as it was inapplicable.
If you wish to observe a herd’s immunity to a given pathogen, you allow it to be infected and then observe the course of the disease. Those left are either immune to the disease or robust enough to fight off the infection. This immunity of course applies only to the given pathogen and can’t be easily generalized. This is not usually a strategy adopted for human beings.
The term is usually used in the context of the introduction of a vaccine where you are creating, to the extent you can, herd immunity. You then observe how well the vaccine works. If the vaccine works, you have created herd immunity for a certain period of time, a period associated with the pathogen and the immune system’s response to it. It will be different for each pathogen. For standard flu, it appears to be about a year. For covid-19, no one seems to know.
To have a scientific government spokesman like Vallance support this dangerously absurd conception was a travesty. Cummings’ suggestions, and the basis of possible bullying of scientific advisors, stem, perhaps for the most part, from readings he has summarized in his blog, which shows ill-digested and sometimes incoherent summaries of things he has read. He is widely read, but it is unclear whether he understands what he has read. From the evidence of his blog and the things he has said in the period he has been Johnson’s advisor, it does not seem as if he understand much, if anything, that he has read.
As for herd immunity in the absence of a vaccine, what effectively you are doing is allowing a pathogen to cull the herd. This sort of thing has been advocated by eugenicists. I am not certain but it may be that Cummings is a believer in eugenics, a discredited theory of genetic purity of a population. There is a long and well developed literature discrediting eugenics theorizing. That Johnson and some of those around him listen to this kind of bullshit is disturbing, to say the least. Some are still working to this proposition, preposterous as that may seem.
Cummings’ understanding and apparent infatuation with complex systems and complexity, applied, say, to epidemics, does not seem to translate into coherent applications, simply because he doesn’t seem to understand them. The rest of the cabinet appear to be similarly ignorant and incompetent. And with Johnson out of the way, they also appear rudderless.
Another concept Cummings doesn’t understand, which he has used, is Schumpeter’s notion of creative destruction. I will leave that, though he contends that this concept is central to his approach to his ‘job’.
Cummings has also contracted coronavirus. Per the Daily Mail, he is still missing in action:
Dominic Cummings is yet to return to Downing Street after developing coronavirus symptoms and entering self-isolation more than a week ago.
Boris Johnson’s top aide has not been seen in public since before Monday March 30 when he put himself into isolation after getting symptoms over the weekend.
Number 10 has been insistent that Mr Cummings is working remotely but his continued absence is likely to spark further scrutiny of the health of key government players, especially after Mr Johnson was hospitalised with the disease.
There are growing concerns about the state of the Downing Street operation after numerous staff were laid low by the killer bug.
he PM’s other top adviser, Sir Eddie Lister, 70, has not been seen in public since the start of lockdown with his age putting him in an at-risk group. A number of other aides have also been off with symptoms.
Readers in comments yesterday also pointed out, as Dr. Larry did in passing, that it isn’t even clear how much immunity contracting coronavirus might confer. From Phacops:
You cannot make that presumption of immunity until there is clinical testing for immunoglobulin (G) serum titre and followup for reinfection. We are not anywhere capable of that in our for-profit medical system as is clearly evident by the fact that we are in our current situation by putting profit ahead of resilience of care for all our communities.
Even with the 4 most common coronaviruses that cause respiratory infections (the common cold) immunity is frequently weak and not long lasting. Magical thinking will not promote immunity. Rather, what this pandemic is demonstrating is that class/social inequalities in the lack of adequate provision of healthcare to all Americans creates the underlying health issues that make class and race factors in COVID comorbidity and risk of death. Want to recover from this and prepare for other zoonotic diseases in the future? Then, we need universal healthcare that is free at point of use to encourage use and prevention.
Note that findings are decidedly mixed. One study of SARS suggested that survivors had antibodies, and hence immunity, for three years, while those who had MERS appeared to have immunity for only a year.
And then there’s the question of mild or asymptomatic infections. There is evidence that at least some of those individuals may not have developed immunity. From Time:
A study on recovered COVID-19 patients in the southern Chinese city of Shenzhen found that 38 out of 262, or almost 15% of the patients, tested positive after they were discharged. They were confirmed via PCR (polymerase chain reaction) tests, currently the gold standard for coronavirus testing. The study has yet to be peer reviewed, but offers some early insight into the potential for re-infection. The 38 patients were mostly young (below the age of 14) and displayed mild symptoms during their period of infection. The patients generally were not symptomatic at the time of their second positive test.
In Wuhan, China, where the pandemic began, researchers looked at a case study of four medical workers who had three consecutive positive PCR tests after having seemingly recovered. Similar to the study in Shenzhen, the patients were asymptomatic and their family members were not infected.
Outside of China, at least two such cases have also been reported in Japan (including one Diamond Princess cruise passenger) and one case was reported in South Korea. All three of them reportedly showed symptoms of infection after an initial recovery, and then re-tested as positive.
In other words, these cases do not appear to be a combo of false and real positives.
Finally consider this observation from ZacP about the limits of antibody testing, now touted as the way to be sure of that someone contracted coronavirus:
It is important to note that an antibody test can mean different things depending on the specific infection. For example, a person who tests positive for the HIV antibody still also is a carrier of the virus and can infect other people. It can also take months, as many as six, for antibodies to become detectable via the standard labwork.
Combine that with false +/- results, length of time to ramp up production of testing kits, and we still need evidence to be able to interpret what a +antibody result would even mean in the case of COVID19…….serum testing still seems to be a long, long way out from actually being able to guide decision making.
A new article by Fierce Biotech confirmed these concerns:
With over two dozen different molecular diagnostics now authorized by the FDA for COVID-19, the field is beginning to see the first of a new group of tests aimed at screening for people’s immune responses to the disease and cataloguing past infections instead of active ones.
While overall testing capacity of any kind remains far short of meeting demand, antibody blood tests would provide additional data on the spread of the novel coronavirus, and results showing immunity could be used to give people an all-clear to leave quarantine and return to work.
Their accuracy would, of course, have to be paramount—any false positives could send unprotected people back into harm’s way. But researchers at the University of Oxford tasked with evaluating these serological tests say they’re still weeks away from solid validation and that no versions to date have performed well.
We see many false negatives (tests where no antibody is detected despite the fact we know it is there) and we also see false positives,” wrote Sir John Bell, the Regius Professor of Medicine at the University of Oxford and a government adviser on life sciences, in a university blog post.
“None of the tests we have validated would meet the criteria for a good test” described by the U.K.’s Medicines and Healthcare products Regulatory Agency, Bell added. “This is not a good result for test suppliers or for us.”
Bell stated a month is the bare minimum time before a test would be sufficiently improved and validated to be authorized for mass rollout.
And yet another bottleneck: a lack of staff to run tests on who is infected now. How many more would be needed to check for having had the coronavirus? From CIDRAP earlier this month:
Health experts from the Mayo Clinic to King County, Washington caution, that although testing is critical, it might not be possible at the levels needed to facilitate proposed plans. Even now, testing in most states is reserved for healthcare workers, or patients so sick they require hospitalization…
To confront testing material shortages, Pritt said Mayo has at least three different testing platforms to use, so if one runs out of a necessary reagent, another test can be used. Still, even with back-up plans, she said labs have to get creative….
For Jeff Duchin, MD, the limits of testing are only worsened by the limits of a stripped down public health workforce. Duchin is the health officer for Public Health Seattle–King County….
“A lot of plans proposed imagine unlimited testing capacity and instantaneous results, which would necessitate a public health army that doesn’t exist,” said Duchin. He said that in absence of a total Wuhan, China-style lockdown, containment of the virus would require a robust, boots-on-the-ground contact tracing effort that would require public health employees that no state or county currently has.
“Is the bang worth the buck in respect of the tremendous investment of time and energy needed to perform those tasks?” Duchin said. “If people are willing to fund and staff [them], it might be feasible if transmission dynamics of the disease make it a rational option. But in absence of a total lockdown, it’s too much work.”
Duchin said he sees serologic testing, which would detect COVID-19 antibodies in the blood, as potentially informing public health strategy. “With serology we would know what proportion of the population remains vulnerable, and which remain susceptible.”…
At the Minnesota Department of Health (MDH), health workers have dealt with a shortage of testing for weeks. Stephanie Yendell, DVM, MPH, senior epidemiology supervisor at the MDH, said the agency has started using other avenues to gain information about how the disease is spreading within state communities, and for that she’s using syndromic surveillance.
“We can’t be relying on testing moving forward to be the only indicator,” Wendell said. “We needed to have eyes on other indicators for illness, in order to put down on paper how all these pieces fit together.”
Yendell said most people with COVID-19 won’t seek medical care, because they experience only mild to moderate symptoms. For those people, self-reporting to existing surveillance websites is a way for public health departments to track community spread of the virus. Other patients will likely report only to outpatient clinics, where COVID tests are unlikely to be available.
“The power and drawback of syndromic surveillance is you can capture people who didn’t get a COVID test, or maybe, if they did see a doctor, their healthcare provider was suspicious of COVID but the visit was not coded as such,” said Yendell.
Now, she said MDH scientists are working on establishing which symptoms they want to track via electronic medical health records and user-interface websites.
Notice the considerable gap between the mainstream coverage of the idea that testing, particularly for immunity, would relatively soon become widely available, versus experts anticipating that it would be able to be done only at most to ascertain levels of infection and recovery in communities, and not to identify that individuals can work or travel safely. Look at how much the front-line public health officials discount the idea that testing will be the main source of information. Bear in mind that South Korea, held as the gold standard for testing, had actually performed as of mid March only 338,000 tests on a population of 51 million.
That does not mean that better tests won’t give very valuable insight. But there’s been way too much hope invested in science as a magic bullet. As Lambert pointed out early on, we’re still having to rely on 19th century methods more than 21st century ones.
But having said that, we may have a lucky break on the vaccine front. More and more evidence suggests an old vaccine used against tuberculosis confers considerable protection against Covid-19. It could be deployed straight up for now if the results continue to hold up, and tweaked to improve efficacy against Covid-19. From Irish Times (hat tip PlutoniumKun):
More “striking” evidence has emerged that the BCG vaccine given to counter TB may provide protection against Covid-19 and significantly reduce death rates in countries with high levels of vaccination.
A study of 178 countries by an Irish medical consultant working with epidemiologists at the University of Texas in Houston shows countries with vaccination programmes – including Ireland – have far fewer coronavirus cases by a factor 10, compared to where BCG programmes are no longer deployed.
This translates into a death rate up to 20-times less, according to urologist Paul Hegarty of the Mater Hospital, Dublin.
Their “correlation” study, expected to be published shortly by PLOS journal, is largely a statistical one and comes with caveats because of possibility of confounding factors. But it is more comprehensive than an initial one conducted in New York, which prompted a scaling up of clinical trials on people with Covid-19.
Vlade provided a link to a 2018 paper on the BCG vaccine. In lay terms,it appears to be a general immune system booster:
Epidemiological studies regarding many successful vaccines suggest that vaccination may lead to a reduction in child mortality and morbidity worldwide, on a grander scale than is attributable to protection against the specific target diseases of these vaccines. These non-specific effects (NSEs) of the Bacille Calmette-Guérin (BCG) vaccine, for instance, implicate adaptive and innate immune mechanisms, with recent evidence suggesting that trained immunity might be a key instrument at play.
While this is encouraging news, the effectiveness of BCG against coronavirus still needs to be firmed up. But at least we have a promising candidate, and one already known to be generally safe.


There is increasing evidence of persistent lung, heart, and even neurological damage in many COVID-19 survivors. This damage typically varies based on the primary site of inflection.
This means that the herd immunity approach will result in a large number of people with chronic health issues, placing a further drain on limited health care resources, as well as reduced productivity and economic activity. Not to mention the human toll in terms of suffer and premature death.
At least Britian eventually reversed course on herd immunity. But what about Sweden and Belarus?
Good question. What about them? How come we don’t get any comparative studies of, say, Sweden and Denmark in order to find out the relative merits of herd immunity vs. lockdown?
Sweden is doing worse than Norway, and this was despite Norway have the second highest infection rate in Europe early on due to a lot of people from Italy having visited. From the Washington Post yesterday, in Is Sweden’s lax approach to the coronavirus backfiring?
https://www.washingtonpost.com/opinions/2020/04/08/is-swedens-lax-approach-coronavirus-backfiring/
In the early stages of the infection when they were trying to do contact tracing here in Sweden for the first few-hundred reported cases the vast majority could be tied to people returning from holidays skiing in Northern Italy during the one-week winter “sportlov” vacation.
Ironically one of the long-standing reasons for this school break in February/March was to slow down the spread of infectious diseases like the flu by closing schools, but that doesn’t work so well in 2020 when it means that every upper-middle class or upper-class Swede jets off to the Alps or to the beach in Florida.
Also worse than Finland.
I find another interesting aspect of the swedish approach is the absence of politicians in most (the heathcare side) of this. Few to no policitians are advocating “tougher” measures (aka Norway, Denmark)… At least at the moment.
No presence in the daily update (all are employees/tjänsteman in a relevant agency): https://www.youtube.com/watch?v=jCD_daF8oaE
I think when this is over (whenever that is) the comparison with Norway & Denmark certainly will be made.
Based on the IHME estimate for Sweden, 4K, but then it assumes 97(?) ICU beds available ( its about 950 still expanding from around 470 or so). So there is that for trust in the model.
If this goes the wrong (already has ?) another major casualty will be the general trust people have (had?) in swedish government (at all levels). It will go down… I suspect, drastically, which will rewrite the politic landscape dramatically, I assume.
Also, its not that people are living their live like normal. Working from home since 4 weeks (mandated by my employer). Been to the shop 3 times since then. People seem to be analysing anyone who approach, and determine the risk level and take evasive action.
But then you have people sitting on a terrace, in the sun, having a drink. As they says “That is great TV”.
Official information:
https://www.folkhalsomyndigheten.se/smittskydd-beredskap/utbrott/aktuella-utbrott/covid-19/bekraftade-fall-i-sverige
https://experience.arcgis.com/experience/09f821667ce64bf7be6f9f87457ed9aa
At a guess then I’d say that the model being used in Sweden has a couple of faulty assumptions:
1. That all working people have sick-pay. Which is not true, a significant minority only get paid for hours spent at work.
2. That all people with barely noticeable symptoms used ‘common sense’ and stayed at home. Might have happened if they had sick-pay but….
3. That the warnings and recommendations of Swedish public tv reached all. Not true, people are getting their news from multiple sources and some might not watch public tv
4. That people were able to self-isolate. Not true, many of the lower-income simply did not have access to low-cost accomodation so were/are forced to share accomodation.
The single-household might be common in Sweden but the shared accomodation is getting more and more common and the ones sharing might often be people in ‘low’-skill jobs involving plenty of interaction with the general public. Accomodation great for picking up, mixing and spreading germs.
It is safe to say that for better or worse, Sweden is no longer what it was when the current Swedish leaders were growing up. I’d not be surprised if their experience of being new entrant to the workforce and how it was for them to get their first home away from parents from 30 years ago has created a strong bias and from that bias a bad model has been created.
There is a balance to be struck between risking causing panic and not imparting the seriousness of the situation. One might induce panic-related deaths, the other might reduce the number of people saved as they did not understand the seriousness of the situation. I am not sure if the communication in Sweden had the right balance. Time will tell.
I would not be surprised by such biases and in Stockholm some of the immigration-heavy, low-income areas (“invandrartäta förorter”) are more stricken than other area(2x to 3x times more infections). Which can probably explained by many of the causes you describe.
Indeed the communication leaves a lot to be desired, because I found this
2meter rule. But this seems only to apply in health settings.
The state epidemiologist was yesterday talking about armlenghts distance, and was questioned by a journalists without answering with a specific distance. As a restaurant owner there is no official distance between guests being communicated. But it seems to going to do some enforcement starting today…
I think strategicaly, by not closing anything at all they missed an opportunity to communicate the severity of the disease. This is not business as usual (with few nudges).
I’m not sure how many death per day the swedish society can stomach. Because based on the numbers it seems the ride will be rough.
Here is a graph of Covid-19 infections that occurred in ski resort in the US: Sun Valley:
https://www.mtexpress.com/news/blaine_county/infographic-track-the-outbreak-in-blaine-county/article_fe42b282-743d-11ea-b4ef-0b819c36a5b0.html
Infections went from 40 to over 400 in nine days. Strict “social distancing” is now enforced and the rate of infection is slowing (dramatically).
Sweden’s state epidemiologist is in for some severe chagrin.
I’ve just read that the Somali community counts for 40% of the deaths in the Stockholm area. And also that 40% of the deaths over 70 were from people living in homes. Something went wrong, definitely.
If the theory is true, that blood disorders (clotting and haemoglobin) are risk factors for fatal COVID infection, the size of immigrant populations with known risks higher prevalence will correlate with deaths. I don’t have breakdown by ethnicity and blood risk but the following figures may explain the divergence between Scandinavians.
Finland – no immigrants 6/mil dead
Denmark – 14% immigrants 35/mil dead
Sweden – 24% immigrants 59/mil dead
I should add Norway but I suspect it is close to Finland,
Timed out editing.
You would expect 9/mil based on adjusting for minorities’ risk for Sweden, 1.5x higher. Remaining 6x difference has to come from more aggressive outbreak and perhaps being later in the curve (better travel connections).
The Scandinavian immigrants are significantly Syrians (they took a ton and it has proven to be destabilizing), who are genetically the aboriginals of that area with Arab and Armenian intermarriage. See here for more: https://www.ncbi.nlm.nih.gov/pmc/articles/PMC3249957/
At first glance, those figures do look rather alarming — Why, Sweden now has 3.5 times as many COVID-19 deaths as Denmark and 7.4 times as many as Norway!
But if divide those deaths by the total population of each country (using Wikipedia as a source), then the situation starts to look a little different:
Sweden: 10,333,456 inhabitants; per-capita Corona deaths: 0.0000664
Denmark: 5,822,763 inhabitants; per-capita Corona deaths: 0.0000374
Norway: 5,367,580 inhabitants; per-capita Corona deaths: 0.0000173
The first thing to point out is that a comparison of the death rates is, of course, lower than a comparison of the absolute number of deaths. Per capita, Sweden now has only 1.8 times as many deaths as Denmark, and 3.8 as many as Norway.
The other point that needs to be made is these death rates are, one and all, incredibly low. This is not the New Black Death we were promised. In fact–and I know some people get tired of hearing this, but it remains true nonetheless–these figures are definitely comparable to your annual influenza death rates. So why don’t we shut down Western Civilization for a few months every winter during flu season?
To my way of thinking then, the much-derided economic factor is worth considering.
Lambert’s Water Cooler features this site, http://91-divoc.com/pages/covid-visualization/ which allows you to track several measures by country in a most useful interactive graphic.
The Swedish state epidemiologist Tegnell said in an interview yesterday that (translation mine) “the goal is to get the spread to go as slowly as possible, but we know, like most people who study this type of illness, that the virus isn’t going to stop spreading until something like flock immunity is reached.”
Maybe this is strictly true, but after reading Dr. Larry’s comments in the post it doesn’t inspire a lot of confidence when I consider that as recently as mid-March Tegnell said that Sweden and the UK both have a more “scientific” approach to handling the virus. Seems like the public health authority might ought to be more concerned about buying time to collect data and less concerned with minimizing disruption to GDP.
This type of modelling is reminiscent of economists saying ‘first, imagine a can opener’. You can only come up with a strategy like the UK and Sweden (and possibly the Netherlands too) if you simply ignore unknowns and other forms of risk. It looks scientific, but it’s the opposite of real science, as real science always acknowledges unknowns and tail risks and never falls into the trap of false certitude. It’s using science as a cover for a politically convenient policy.
In this case it’s “Assume immunity”.
In the UK government’s case, (when they thought it was just going to polish off a few O.A.P. and weaklings), “Assume we give a shlt”.
Not quite sure what is meant in any of this by “boosting the immune system,” as in connection with BCG. This enters into the realm of complexity, I’m no immunologist,, so maybe there is partial truth to the notion, but the “immune system” is a system of systems with a lot of moving parts. And “boosting the immune system” can in many cases lead to some bad outcomes. Here’s from WaPo:
Since news about the coronavirus broke, there is a good chance you have read or seen advice about how to “boost” your immune system — whether it is loading up on citrus fruit, sipping herbal or green tea, eating yogurt for the probiotics, or taking vitamin or zinc supplements. Unfortunately, there is no evidence any of these strategies will supercharge immunity. To understand why, let’s consider how the immune system works.
The immune system’s role is to defend your body against disease by fighting infection. It is “system” in the truest sense — it has many interconnected working parts: white blood cells, antibodies, bone marrow, the spleen, the thymus and lymphatic system. These cells and organs operate in concert to hunt down and destroy dangerous pathogens, such as viruses, that enter your body.
A “boost” in that process would not be a good thing. Scientifically, it would mean your immune system was overactive, and overactive immune systems lead to autoimmune disorders. You just want the immune system to function normally, so it helps prevent infection. … https://www.washingtonpost.com/lifestyle/wellness/immune-boost-coronavirus/2020/03/05/e111554a-5e73-11ea-b014-4fafa866bb81_story.html
Maybe BCG improves the functioning of elements of the pathogen recognition and antigen activation mechanisms, and adds to the body’s ability to generate antibodies for pathogens not previously encountered, yet without initiating that cytokines storm which is on all our radars as “bad” (and it is: https://en.wikipedia.org/wiki/Cytokine_storm .) Maybe chloroquine and/or hydroxychloroquie is beneficial, when administered at particular stages of the disease, and in particular doses and routes of administration, to a set of people whose unique physiologists can benefit from those meds. Same questions for all the other therapies that physicians are trying, in frustration and desperation, to mitigate the death and dysfunction. Lots of “maybes.”
Seems pretty clear to me that there is a lot of fumbling around in the science realm, lots of false leads and backtracking as the “novelty” of this pathogen is slowly worked out (maybe, too, this bit of “code” is a moving target, like the worst kind of ‘computer viruses’ that can “learn” as they propagate.) there have been lots of bits of information that people seize on, in our very human desire to assess our own risks of death and debility and inform thinking about response policies and, of course, “Getting the world economy back on the rails of Groaf!”
Do people “get over” infection?” How many will become carriers? Is there a “rate” of mutation of the virus code, a “direction” of mutation toward greater or lesser lethality? Does surviving the infection confer immunity, and if so, for how long? Can people who have survived one infection get reinfected? What percent of the population will be permanently damaged by the virus, at what cost in providing care (if the neoliberals even allow such care to be provided? When will there be a vaccine? Is a vaccine even possible, looking now at the so far fruitless efforts to develop a vaccine to HIV, another pandemic that kills millions, where the search for a vaccine has been going on for 0ver 30 years? There is a vaccine for HPV, but that’s a different beast. Lots more unanswered questions, but of course actions and policies “are taken” because individuals and important powers demand that “something must be done NOW.”
This should lead to a lot of questioning about what is important, and even possible, “going forward.” Seems to me like Gaia is forcing us to stop and take a deep breath (those if us whose lungs and other organs are not currently devastated by the pathogen) and maybe think a bit about possibly going down some different paths from here.
Early in my medical training (the 1980s), BCG was being used as immunotherapy for malignant melanoma with some promising studies.
I have wondered about the claims of “life time” vaccines since I got my series of Hepatitis B vaccines. I was subsequently found to be antibody negative. No seroconversion. And no consensus on what that meant.
There are so many factors that go into the efficacy of a vaccine.
Effect of Vaccine Administration Modality on Immunogenicity and Efficacy
https://www.ncbi.nlm.nih.gov/pmc/articles/PMC4915566/
(1) features of the vaccine itself, including immunogen design, vaccine type, formulation, adjuvant, and dosing; (2) individual variations among vaccine recipients; and (3) vaccine administration-related parameters.
The CDC points out that in general, current flu vaccines tend to work better against influenza B and influenza A(H1N1) viruses and offer lower protection against influenza A(H3N2) viruses.
Indeed, this comes from the CDC:
The more I learn, the less I “know” about vaccines.
I had never heard this important info before. Thanks Kris.
Hi JTMP
Wonderful insight! I had never made the now, (thanks!) obvious connection between, “Boosting the immune system” and “autoimmune disease”.
The terrible truth is that this corona virus is still, largely, a mystery to us.
About immune system boosts. I have come across only two, Vitamin D for Northern hemisphere folk and sleep.
Two studies done in the USA, showed fairly comprehensively that ‘good & efficient’ sleep does boost the immune system against viruses.
By ‘good & efficient’ sleep the researches talk about getting to bed by 11pm and having the first few hours of sleep uninterrupted. TV and computer screens will alter the circadian rhythms.
Anecdotally, medical staff treating CV19 patients are not getting enough sleep and therefore their immune systems can be compromised
Whenever Tegnell is mentioned, I think of George W. Bush’s “Heck of of a job Brownie.”
There’s no mention of disability, so adding this to the mix.
A former colleague, mid-30s physically active, was diagnosed with COVID-19 before tests were readily available. All of the classic symptoms, dry cough, high temperature, etc yet avoided hospitalization. One of the lingering remnants of the disease is weak lung capacity, raising the question of whether or not there’s permanent damage. (For obvious reasons, it will probably be a while before follow up medical appointments are available)
If the disease leaves physical damage behind, how is herd immunity useful if people who survive COVID-19 develop permanent disabilities?
Everyone is getting antsy…A quote from the Guardian live blog from the Irish Heath Minister, Simon Harris:
Unpacking that quote a bit…there’s no discussion of how you have a “sustainable” rate of death in this scenario. And that is presuming that people are marked with some sort of a scarlet letter which is – You will die of Covid-19, it is written in the stars. It seems they will just end the lockdown without a notion of what to do (or use tests that don’t work all that well).
Adding to all that, the R0 with no social distancing or extreme lockdown is now estimated at 5.7 (according to new numbers out of the CDC). Like that is superamazing infectous. So, letting it loose, you’ll just have to lock down over and over. I mean if that’s the strategy, it smells like an adjusted version of herd immunity.
There is no give in Western economies. And the powers-that-be will just lift everything come May. And then what? I’ve seen video (can’t confirm if they are real, to be honest) of people falling over dying in Wuhan and in Indonesia before the governments took it seriously. Is that what we’re going to have to deal with?
Holy shit. Can you provide a link to an article or the CDC page with that 5.7 number? That is horror movie scary bad. It does make me feel less nutty about having become Miss Alcohol Spray bottle and handwashing nut even before there were any official cases here. But it also means continuing to be loony level vigilant is important. Masks, gloves, and maybe even goggles all the time!
This is also a death sentence for most restaurants. And I don’t know how nursing homes (and agencies like the one we use that sends aides to the elderly that stay in their homes) keep from killing all their charges.
I found this link from Forbes, The COVID-19 Coronavirus Disease May Be Twice As
Thanks!
To back up the worry around how to deal with this, there is a great thread by Dr Eric Feigl-Ding from yesterday:
So it is not 60% as was assumed (ugh), but around 82% of the population would need to be immune to have herd immunity.
Just to add to this, but its reported that soon to be published research indicates that the BCG (TB) vaccine may provide very significant protection from the SARS2 virus. If that’s the situation, then I would guess that the R0 value in countries with vaccination may be significantly less. It’s certainly one explanation for why Covid seems to be spreading more slowly in eastern Europe.
That’s in the post when it went up with an attribution to you.
So sorry, I don’t know how I missed that!
It may also be why Islington, which is the most densely populated council in the UK (and Europe) isn’t an epicenter (it’s not the worst in London by far). They’ve had a problem with TB for some time and require children to get a BCG shot – ergo children won’t be carriers. I don’t know how long they have done that, but I think it has been for some time, so there maybe something to it.
This might contribute to CV’s virulence in the US, which never adopted a universal immunization approach for TB.
My small town Doc in the 50s – 60s – 70s paid less attention to the official, universal, or govt guidelines and paid more attention to the science literature and to what he knew was was important. He was a Doc in WWI , old enough to know the ravages of TB first hand. And so I and my sibs did get the TB vaccs, even if it wasn’t in the guidelines. Thanks, Doc. Thanks, Mom. (Mom had no use for anti-vaxxers.)
Expect many kids in the US got TB vaccs in the 50s and 60s no matter the official position, thanks to small town and large town Docs who knew what was what. Hope so.
Just bear in my how very much we all want to see a magic bullet. BCG has more hope than hydrochloraquine (sic) because it is not such a obvious panacea, but the human impulse to grasp is the same. BCG is really just one more lead to be chased down. Many successful treatments for cancer in recent years, along with those for HIV, have usually been combinations of things cooked-up and refined over time, with patience. People need to maintain that perspective
In the U.K. virtually every adult over 30 has had the BCG. So I don’t hold up much hope for it.
Yes, I got it (late, late, late clinging on by my fingertips forties) as a child. As I think did most certainly up ’til the 60-ish bracket. Older than that is doubtful. It doesn’t seem to be helping that much.
Background to the UK’s history of the vaccination programme here https://view.officeapps.live.com/op/view.aspx?src=http%3A%2F%2Fwww.wales.nhs.uk%2Fsitesplus%2Fdocuments%2F888%2FBCG.doc.doc
(started in 1953, ended in 2005 routinely, although as Redlife2017 says correctly, it is still administered in some higher risk districts; limited efficacy when given in adulthood).
erm… not to be, you know, one of those people… but does that include the ‘over thirty’ group of recent arrivals (within the past 20 years) ? ( Yes, this sounds totally like one of those people, I know, but it is not. ) Data disaggregation is important in science for correct data assignments. Sorry for the pedantry.
Good question, Flora. The U.K. has had a growing problem with TB since the 80’s in the Daily Mail’s chosen people, immigrants and HIV carriers. The current policy of vaccinating only these groups, their families and people who work with them was adopted in 2005, replacing universal BCG at 13.
This was done because BCG was too successful. I kid you not – the cost of treatment was cheaper than the cost of prevention for the marginal extra case in a low incidence country.
I cannot find the paper I read the details in but this paper for Ireland gives you the flavour of the mentality.
https://archpublichealth.biomedcentral.com/articles/10.1186/s13690-016-0141-0
The observant will note that at the end, the authors recommend somebody actually studies what it would cost to move to selective vaccination plus an active screening and treatment programme, because their whole quality adjusted life year house of cards considers the reduction in costs of moving from universal to selective vaccination but not upgrading treatment to cope! Treatment which is profoundly unpleasant, has high non compliance and is increasingly difficult because multi-drug resistant TB is spreading. The shortsightedness is unbelievable.
I have read it suggested that the protection provided by BGG weakens with time so those who received it prior to 2005 may only benefit in small degree.
BCG immunity typically lasts only 15 years.
https://www.healthed.govt.nz/resource/bcg-vaccine-information-parents-%E2%80%93-english-version
Dunno about the UK, but in the US, most doctors are terrible about giving vaccinations periodically for tetanus, where the immunity lasts only 10 years. I hadn’t had a shot since my childhood and had to ask my NYC MD for one. She should have volunteered, but all of my past MDs were similarly lax. I suspect most UK readers would recall if they got any BCG shots in their adulthood….
Countries with BCG programmes already in place may indeed fare better, but what does that imply for future policy? Would BCG vaccinations now affect people’s susceptibility, and if so, in what ways?
Then there’s the question of viral load to consider regarding the uninfected person. Is the initial level of virus at infection related to disease severity?
Viral dynamics in mild and severe cases of COVID-19
https://www.thelancet.com/journals/laninf/article/PIIS1473-3099(20)30232-2/fulltext
The mean viral load of severe cases was around 60 times higher than that of mild cases, suggesting that higher viral loads might be associated with severe clinical outcomes.
Redlife2017: completion of the link you only copied part of:
https://wwwnc.cdc.gov/eid/article/26/7/20-0282_article
That 5.7 number also appearing today’s Links in an article called “Virus May Spread Twice as Fast as Earlier Thought, Study Says”-
https://www.bloomberg.com/news/articles/2020-04-08/virus-may-spread-twice-as-fast-as-earlier-thought-study-says
This thing is just a beast.
Yes, I’m trying to contemplate how to deal with this when the lockdown is removed in the UK at some point in May. My partner has severe asthma and, you know, killing your significant other by accident does happen (I know someone who did that, it was awful), but I’d rather not do that if I can. But of course, the government might view it as ‘the price is worth it‘.
Also to note, a really good source of info is from one of the first to sound the alarm in the US: Dr Eric Feigl-Ding He had a link to the 5.7 number yesterday as he’s always looking at what the latest medical news is on this.
Existing respiratory conditions do not appear rot increase odds of death in ICU patients (ICNARC paper). Even slight decrease o the data!
If micro thrombosis and/or haemoglobin insult hypotheses are true, this would be predicted as the problem is oxygen transfer, not ventilation (may even be protective because of long term lung adaptation to mild hypoxia, as is probably the reason for low prevalence of COVID in smokers).
NB: Odds increase with respiratory condition of ending up in ICU unknown so far. Data only covers ICU outcome, not admission.
Here’s the paper: https://wwwnc.cdc.gov/eid/article/26/7/20-0282_article
So the method used for R0 was based on population-level data. You can also estimate with individual data. I think we don’t need an exact R0 to know that this is quite an infectious beast. Bear in mind that this R0 was calculated with data on an emerging outbreak as it was the case in Wuhan. We don’t have population-level data to calculate the steady R0 level it reaches in more advanced epidemics. I guess it would be somehow lower but any case it should be clear this is a very difficult guy to control!
I believe Redlife is probably talking about https://wwwnc.cdc.gov/eid/article/26/7/20-0282_article
“High Contagiousness and Rapid Spread of Severe Acute Respiratory Syndrome Coronavirus” off of the CDC’s Emerging Infectious Diseases journal.
I am not planning on going to a sit-down restaurant or bar until the end of 2021 unless a successful vaccine is introduced before then or if I have serological testing indicating adequate antibodies. So restaurants need to be prepared for 18 months of takeout.
My version of herd immunity is this:
1. Social distancing to prevent infection
2. Wear mask when in public around people
3. Work from home and go to workplace as little as possible over the next 18 months
4. Avoid public places like sit-down restaurants, bars, concerts etc. where you will be around people for extended time
There seems to be evidence out there that severity of disease for most people is likely to be a function of the viral load you are exposed. With the measures above, hopefully my viral exposure load would be small even if exposed. That may be enough down the road to give me immunity without undergoing a severe case.
My risk group based on age, gender, etc. would be right at the inflection point where it goes from something a little bit worse than regular flu to the much greater than 1% range. So I shouldn’t be greater than 1%, but that is still worse odds than I am looking for.
Delaying getting sick gives them time clear out the hospitals and figure out successful treatments. I suspect outcomes will be better by early 2021 because they will have a lot more experience and calibrated data.
The “send everybody back to work and see who dies” approach is bonkers.
Simon Harris isn’t known for his way with words (in Ireland, the tradition is that the Health portfolio is given to whoever the Prime Minister wants to destroy politically), but it’s pretty clear I think what he means. The idea is to accept that the virus can’t be eliminated until a vaccine is developed, but that the rate can be reduced to a level that the health system can deal with. This is behind the strategy (in Ireland anyway) of trying to keep Covid treatment centres separate from the main hospital system. Its pretty clear that they see this as like TB – a disease which was managed as far as possible until it was possible to largely eliminate.
While I don’t have a lot of faith in him (or the Irish health system for that matter), it is good to see that at least they are looking at a longer term exit strategy that isn’t dependent on an assumption of a magic bullet.
I feel like the whole scapegoating of the UK for aiming for herd immunity is a bit too easy. As what I’m missing in most articles is an alternative. Keeping countries in lock down for one to two years while waiting for a vaccination is not that good an alternative.
Also, I’m not too familiar with the exact details of the UK position, but they were certainly not the only ones aiming for herd immunity as an exit strategy. I know the Netherlands was on the same page and still is. Only, herd immunity is not a goal on itself. The goal is to ride this pandemic with as little damage to the economy as possible while keeping the curve flat enough so the hospitals can cope (and while keeping the trust of the public, also very important). At least the experts here are honest enough to acknowledge there are a lot of unknowns, so they are researching the validity of their assumptions and adapt accordingly. I assume (and hope) the same is happening in the UK.
Two generations ago, British soldiers went into battle “For King and Country!”. Are we civilians in this era supposed to go into battle against Coronavirus shouting “For Dow and Jones?” Going for herd immunity is the solution of a technocrat who is willing to sacrifice apart of the population for the good of the economy. Boris thought it a good idea – until he discovered that that meant himself as well. And he may escape with is life but what sort of damage will it leave on his system for the rest of his life?
And if you want to save the economy, this is how you do it. Everybody wears masks – everybody. You do aggressive testing and tracing. You quarantine those that might be affected and take care of their basic needs like food, medical gear, etc. You make testing free and you make any treatment free as well so that people are encouraged to go for treatment. You do social distancing and anything else to flatten the curve so that the hospitals are not over-run. You quarantine all people from overseas come into the country. There are other methods but they are not rocket science and are time-tested.
And people will cooperate because they know that their government is on their side and is not using them like rats in a lab experiment.
I can see a poster not unlike the WWI poster “your country needs you” instead it reads “your country needs you, grandma”
The problem with this is that we know that you can’t manage both – the notion that you can somehow gently flatten out the curve while maintaining the economy is similar to economists once thinking that all you had to do was gently adjust a few economic levers, and slow and steady economic growth could be achieved whatever.
The problem is that there is so much we don’t know about this virus that the possibility of getting it horribly wrong are just too dangerous to contemplate. South Korea and Taiwan acted fast, they acted aggressively, and now they still have intact economies and systems in place to tamp down future infections. They are reaping the benefit of ‘over reacting’. This isn’t by chance, they recognised (from previous experience) that the worst case scenario of the disease was just too high a risk to accept – Nicholas Nassim Taleb has written extensively on this (I keep referring to him BTL primarily because he is one of the few academic writers who has been proven consistently right on this from the beginning).
The notion that you can somehow manage this disease as if it was a leaking water pipe is simple nonsense – and yet that is precisely what the UK, the Netherlands and Sweden are doing. It sounds very rational and clever, but then again, so did most economists up to 2007. It’s intellectual arrogance dressed up as science and rationality.
Please include the US in your list of “leaking water pipe management” failures… We are lucky to have a “federal” system where individual state political rulers can screw up in a whole wide set of different ways.
IMO, one of the most difficult decisions is about schools. Should these be opened next September as usual or not?
Heck no! Keep your nasty little infectious varmints at home! Disclaimer: I live with 2 of them. Yeah, it’s one of those wholly unprecedented questions that will have to be sorted out. School systems around the world are on the list of institutions we’ve been able to take for granted for generations that are now quite upside down.
Once you get the new cases to low single or double digit level, you can then do aggressive containment strategy — testing, tracing, isolation, masks and so on. Then you can start reopening the economy gradually. As you say, Taiwan and Korea is still quite open, including their schools. China, even considering their trustworthiness, is slowly recovering. So there is a way forward, but not pretty. Restaurants, clubs, bars and travels will be the problems — people unmasking, talking, drinking, and eating. So life not as usual and and subdued economy until we have vaccines and treatments.
Um, did you read the post? US public health officials said no way does the US have the capacity to do enough testing, let alone tracing. UK is in a similar position. The US isn’t willing to hire enough people to do it correctly.
And everyone would need to carry a smart phone in theory, but in fact, they can geolocate only to +/- 5 five meters for consumer grade equipment.
Yves, once you get New cases down to “low single or double digit level”, then you can do containment tracing. Right now no. Hong Kong does not do as much smartphone tracing but still does ok. I think the problem is the willingness to do it. By the way, thanks for your great work. The NC readers are among the most considerate and knowledgeable group anywhere. Very enlightening.
This can’t do attitude since a Reagan years is how wars are lost. Not enough capacity? Make more! There are tens of millions of people sitting on the sidelines with nothing to do all day. I’m pretty sure you can find a good fraction willing to solve this problem for you in exchange for a paycheck and government health plan.
If you can get everyone else back to work this totally pays for itself. Of course, we might have to admit we are pinning our hopes on government being good for something after all.
I’m not sure why you keep referring to the Netherlands along with Sweden and the UK. My best friend (Dutch by birth) just spoke with a friend of his two days ago who lives in a Rotterdam suburb. According to the woman in Rotterdam, they are under the same lockdown restrictions that we are here in Illinois. It’s more difficult for them in some respects, because they still have a lot of small, individual purveyors–separate greengrocers, butchers, etc. Everyone is wearing masks, keeping a 2 meter distance and limiting the number of patrons in the store at any time. Hospitalization may occur in either Holland or Germany, depending on the availability of beds. Sounds pretty sane to me.
Agreed Rev,
It boggles the mind that so many people are having a hard time with this . As you said this isnt rocket science folks. A robust regime for testing , contact tracing, quarantine/treatment, until there is a vaccine is the only viable rational path forward.
Last night i was subjected to a youtube video of radio personality kim iverson interview with a fellow living and doing business out of china. In so far as he paints a very rosy picture of the Chinese response, the gentleman is clearly propagandizing for the Chinese state. Nevertheless it was interesting to hear a different perspective. But the thing that drove me nuts was at the end of interview the host, kim iverson, proposed with unbelievable certainty that the only way out is herd immunity! This was on march 27. Lordy, with progressives like this who needs enemies.
See the above comment. It would take a vast investment in resources, hiring, and oversight. Na ga happen.
That is frankly what I’m afraid of.
I would expect my state and city authorities to begin hiring and training THOUSANDS of workers immediately for the contact tracing program to begin once we get the number of new cases low enough. But i have not heard a single thing about organizing this effort from the mayor or governor (chicago, IL).
Terrified for my mom and other family elders.
This is the plan our Director of Health for Ohio has been talking about. These are the steps and resources she keeps repeating we need and are in the process of establishing to even begin to let up even slightly on the “social distancing”, and the Gov. seems to be in agreement. However, at the very same daily press conferences the Gov. also speaks of forthcoming state budget cuts and resource cutbacks. The Director of Health, Dr. Amy Acton, is telling us early next week we will hear and see in depth the long term plan. How it all will be funded and how willing the Gov will be to fully fund and staff what is needed remains very much in question.
The problem is, it is not known whether herd immunity is achievable. We have nil herd immunity against common cold – most people catch it once a year if not more.
That is why you need the slowdown – so that you can find more about the virus w/o it turning into Spanish Flu Mk2.
It’s possible that we end up with some sort of herd-immunity (incidentally, herd immunity more or less implies vaccine _is_ possible, as fundamentally both deliver antibodies). If people are squeamish about shortcutting vaccination tests, why should we not be even more squeamish about being unwilling participants in mass-testing?
Vlade, from an evolutionary perspective, it is more than likely that humans and the various cold viruses have been accomodating themselves to each other for hundreds of thousands of years if not longer. Those that did not die and were able to reproduce passed on, in a statistical way, their resistance. So, at present, we are not completely resistant, but, it seems, highly reisistant as hardly anyone dies from the common cold. 50% of colds are apparently due to the rhinovirus. Since that seems to be the case, there is a case to be made for a vaccine against the rhinovirus, but Big Pharma finds it more lucrative to sell us nostrums for dealing with the symptoms.
Should humans last long enough, the same accomodation should emerge with covid-19 should it stay around consistently enough long enough.The time scale is too long to wait, however, for this to occur. And Big Pharma has no nosturms that work for this pathogen and are unlikely to develop any.
Oh, I don’t doubt that we can very well come to an accomodation with CV over time, as it’s not pox or similar. But we can’t right now – and that’s my point, that we have no idea whether any accomodation (and herd immunity is accomodation too) is achievable in near term.
“Herd immunity” is an attempt at vaccination w/o testing the vaccine for safety and efectivnes.
Understood. I agree; I don’t think so either. But in terms of herd immunity, I would, I think, prefer to say that such immunity may, perhaps inadvertently, be functioning as a (cheap) substitute for vaccination, thus obviating the need for any real testing, which might be costly (at least in time and other resources). I don’t think we are in disagreement here. A reason I wish to put it the way I did is that I don’t want to conflate vaccination, which is a particular type of procedure, with what is actually taking place.
Some of us appear to be immune in varying degrees to this particular infection. Not herd immunity, then, but that old chestnut about ‘survival of the fittest.”
Also, in the realm of Gramsci’s famous observation about “morbid symptoms,” there’s this:
“ Fake cops are stopping drivers for violating coronavirus stay-at-home orders,”
https://www.usatoday.com/story/news/nation/2020/04/08/coronavirus-stay-home-orders-see-fake-cops-go-after-motorists/5099762002/
Maybe something complex like symbiosis and herd immunity. Herbalists say that the antidote always grows next to the poison. And in the garden of our lungs both coronaviruses and TB bacilli were harbored together since forever. Kinda makes sense that BCG works; that we owe coronavirus immunity to the enemy of our enemy. Like some people are immune today to HIV because their ancient ancestors had or developed an immunity to the black plague. And other aspects of symbiosis like Rtah100’s comment on the hemoglobin connection between coronavirus “pneumonia” and malaria. So that dugs for other ailments mysteriously work on new infections. Let’s hope we are lucky enough to stay ahead of a virus that exponentiates at an R value of 5.7.
This
is perhaps the one of the most accurate comments provided so far on try to decide what to do in response to the pandemic. While Rev Kev’s solution above might be the most humane solution I think one could say that if one is trying to recover the economy we remember from before this storm it would not work. But then again nothing is going to do that. We have passed an inflection point and we will eventually, sometime down the road, reach a new normal. A normal significantly different then the one so many fondly remember. A likely harsher new reality but still one better than the mess we have today. I have some issues with Geer, but his description of the long descent from step down to step down applies well here.
While Sweden is an interesting example of pursuing some kind of herd immunity I am pretty sure the US is going to be the poster boy for an example of just using a bull rush to try and slam through the problem with brute force. The US still has not performed a country wide lockdown and almost surely never will. Those still resisting are not likely to go on with one due to the disintegrating economy. The business community is already exerting tremendous pressure on politicians to unchain the economy before it is too late. All the talk on the news is already focused on the ‘we are seeing the signs of the curve flattening finally’ meme. Trump is bound and determined to return with a roar. Does anyone doubt that he will unleash the restrictions soon? Will he even last to the end of the month? I am convinced that the US is quickly approaching the limits of what the business community and the public will put up with. In the face of all the science and showing a complete lack of common sense we are going to try and return to standard behavior – I think.
So the goal that Maurice mentioned of just getting the economy going and ‘trying’ to keep the flow of sick into the medical system somewhere below the threshold of overwhelming the healthcare system is exactly what we are going to try and do. If we don’t do this the reasoning goes is that there will not be an economy left to go back to. So we have no choice in the matter. We charge ahead and take our losses. In the meantime we jump on every sparkly miracle suggestion like chloroquine, remdesivir, bcg, dozens of attempts at vaccines, zinc this or that, yadda yadda in order to placate those of the public paying any attention to the news that we are working hard to solve this. But bottom line is we try hard to restart the economy. The herd immunity is a byproduct.
We find ourselves in a situation similar to that faced by our grandparents (mine at least) during the 1918 flu epidemic. All the sparkly talk about vaccines and drugs did not exist back then. It was just another epidemic in a long human history of epidemics and all society could do was try and live through it and keep things running. Sometimes this worked better than others but it was the only choice you had. To those who think that one cannot place a value on human life history has demonstrated on innumerable occasions that this idea is simply not true. We have always done so and we do so every day – we just try hard never to talk about it. The science indicates there is a significant possibility that for a coronavirus developing a strong long lasting vaccine may not be possible or may take many years. This leaves herd immunity in some form as the default solution. We are damned if we do and damned if we don’t and this is the idea behind the cure being worse than the disease mind set. Ahh well I better go it is time to walk the dog.
The problem for .gov is that sensible people and organizations already locked themselves down, long before they were told to by the state. The state was reacting to the reality on the ground, so they didn’t look like chumps.
I think the Mises.org enthusiasts will find that, when they do the grand re-opening, sales will be extremely meager for some time. Reasonable people don’t put their nearest and dearest into an early grave “for the sake of the economy”.
It’s probably better for everyone to just sweep it under the ‘lockdown’ rug until it really is all clear, and demand returns. In the meantime, give a UBI so people can meet their financial obligations without endangering everyone else. However, that is ideologically impossible with the Randians running the USA.
ps I hope you are your wife are back to 100% health!
I didn’t realize Mises.org was a thing.
I went there and am now horrified.
Our society practices human sacrifice on a scale even the Mayans would blanch at–the priests once sacrificed to please the gods, now the economists sacrifice to please the “economy.”
I can hear the economist-priests chanting now, it’s getting louder: “Economy want blood! Economy want blood! Blood must flow!”
CV19 poster “your country needs YOU, Grandma”
Greer, John Michael, not Geer. For those who don’t know him already.
I see what they are saying and understand it. There’s always a risk-reward assessment, whether subjective or calculated in play. Right now, for all this talk that the “let it flow/ herd immunity” strategy was abandoned we don’t have a “full-stop/ lock down ” strategy, just a partial one with its corollary – a partial, very weak perhaps “let it flow ” strategy. For example:
All people in the food distribution chain are interacting with the attendant risks of transmission. Yes, even ourselves when we go and get the food. The subjective risk reward assessment is that without food we all die x the cost of the deaths versus the assessed probability of getting CV by taking part in the distribution x the assessed probability of dying x cost of a death.
A similar calculation exists for partially keeping the medical system flowing.
Now this is of course obvious but I think it needs stating explicitly so the “somewhat opening up some of the lockdowns at some time ” argument isn’t responded with “you are trying to kill us”.
The devil is of course in the details. So people should be researching, simulating, modeling, and discussing it openly so that the assessments of the risks / rewards associated with various possibilities are out in the open.
Immunoglobulin testing is tricky as you not only have to determine whether a person has the coronavirus-specific antidody, but also that the antibody is produced in sufficient quantity. This not something that can be widely deployed quickly as the testing is labour intensive and need trained personnel.
My lab at Northwestern is in the process of submitting a proposal to NIH to adapt our testing system for coronavirus immunoglobulin. Other universities are doing the same. But the fastest we could deploy these systems would be 3 – 6 months and the capacity would be pretty low. We can currently process 500 patients per day and there is no ability to quickly scale this up, we could go to 1500 a day by the end of the year, but that’s about it.
So you might be able to poll the population with 10,000 random samples to determine the rate of immunity, but we are not capable of testing the whole population.
Very helpful, thanks!
Exactly.I think this would be the correct use of antiserum testing: just have an idea of how many have developed immune response. Enough. So it is not that useful to control the epidemics but as a registry tool.
OK, we are now about 5% immune.
Now we are 12% immune.
etc.
So we might find a working vaccine that, to be effective, would then be massively administered. Then the antivaxxers promptly go nuts and oppose it.
If it wasn’t for their kids, I’d say “let them eat virus”.
The kids seems to get off very easy. So I’d say let them have it, it’s a unique disease in the way that the retribution for any adult stupidity on behalf of their children ends up on them!
My daughter was quite ill for 3 weeks, her son (5), had fever, bad stomach, headache and pains in his arms and legs for two days.
Two other people in the household (smaller child and older adults) had nothing.
Odds are it was flu then. adults have been exposed to many types with a fair amount of immunity, either partial or full. Kids have less exposure and less likely to have wide-range of immunity.
I had a nasty short bug in late February after travelling from Upstate NY to the Midwest and back. One day fever but explosive cough for 2-3 weeks. Someone else in the family had that same type of thing about 3 weeks later, but they had a co-worker who had a positive flu test a week earlier.
There is a reason that most test results come back negative for Covid. Influenza A and B have been making the rounds and B was not a good match for this year’s vaccine.
Making this clear now because I see how this could spin out of control. I do not believe that there are “superior genes” so I am in no way a eugenicist. My senior thesis paper was on John Collier who was the head of the Indian Affairs bureau in the U.S in the early 1900’s and was a eugenicist later in his life. I know what eugenics is and I do not like it at all. So if you come out of this thinking I favor eugenics you have to assume that you do not understand what I am proposing.
I have a genetic trait, I am what is called a FUT2 non-secretor. This provides me more protection from the norovirus and several other viruses as well, most likely SARS-CoV-2. I was part of a past population that was naturally selected for that trait after some virus probably wrecked a population somewhere in Europe.
So I had a thought Experiment regarding Eugenics; Is the opposite of eugenics any better? Is inhibiting natural selection via a vaccine necessarily going to lead to an overall positive outcome?
While eugenics is searching for the perfect genetics, vaccines, which make any genetic robustness to a virus irrelevant, erases the influence of our genetics making the resulting larger population even more dependent on vaccines.
So is it possible to have a neutral view on life and death? Can we see that they are two sides of the same coin and that by weighting down a side of that coin the randomness that is built into our very genetics throws the whole system out of balance? Is it possible that we do not have to live like the eugenicists, thinking some particular set of genes are more superior, but not use vaccines thinking that genes are insignificant and irrelevant? Can we just devote our time to caring for people and the environment so the need for vaccines becomes insignificant?
It would be fair to say that before the invention of modern medicine the ecosystem has practiced “eugenics” and it has helped humanity survive for 200,000 years. Look at sickle cell and malaria. Evolution had to make a bargain, many people would be protected from malaria but that meant that some would have to die young. No vaccines needed and humanity in Africa survived for hundreds and thousands of years.
Maybe being a financial blog you can all imagine vaccines as a form of debt?
And if we think vaccines are good enough for humans, why not all the animals of the world? By excluding humanity from the viral roulette we are just creating a huge imbalance in the ecosystem of the planet.
So like all forms of debt, suffer now or suffer more later. It might be that vaccines are pushing the suffering onto future generations.
“the ecosystem has practiced “eugenics” “, yes it could said and has been and that is natural selection, which is difficult to you really understand without really studying it. It does not at all work in the manner one might think. There isn’t any grand plan to theory, different life forms in different environments basically place bets on how to live. Many try few are chosen. Then within a given ecological niche organisms, cooperate to support that niche. There is more cooperation than competition. Lastly, life itself alters the ecological niche it is in, thus creating a positive feedback loop, were over time certain random genetic mutations give certain species the ability to better adapt to any given niche. It can be argued the genes that built our brains allow us to create vaccines thus protect our specious from the harm they might do. Else why do we have the ability? Virus aren’t alive, they are simply random bits of rna or dna code that can cause a great deal of mischief. Our species is one that uses tools to adapt, as do birds, as do a thousand other species. Seems to have worked out evolutionarily wise.
…Being the Superior Species; we have attempted to override the process of Natural Selection…
Payback is a…….!
Yes, thanks. Either way, vaccine or enforced herd immunity, they both are an attempt to control natural selection.
You are making too many assumption about what I am trying to get across.
I am not saying there is a “grand plan” but rather, a law, that is that nature seeks balance, an increase in entropy with an end result of entropy=0. Gravity is a law, not a grand plan. We can push that law, by flying, but that takes energy and creates new risks. The energy we add into the environment decreases entropy.
And your understanding of evolutionary genetics is poor TBH. “Many try and few are chosen” is invalidated now that epigenetics has been understood. Epigenetics communicates what is going on in the environment to our genes and influences future genetics.
And my point is that vaccines make those mutation irrelevant and therefore humanity is now dependent on that vaccine. How long can that last? Is that as stable as having no vaccine? Imagine if we use vaccines for 1000 years and as a result any genetic immunity is bred out of the population. Then suddenly we cannot produce that vaccine. That would leave humanity with zero protection.
As far as viruses not being alive, that is a bold statement and not even have the majority of scientists have made that conclusion. We in fact are merely just larger clumps or random DNA and RNA. I would say that the fact they reproduce means there is some energetic drive to survival. And why would something not survive want to survive?
I will not debate that the last 1000 years has lead to the overpopulation of humanity. But saying that it is an evolutionary “worked out” cannot yet be determined.
And don’t you see you are in fact being a eugenicist by saying that? That the genes that created human intelligence are the “best genes” because they have “worked out evolutionarily wise” in that “there are more of us” and we “dominate the planet”?
Epigenetics no doubt plays a role!
Chronic stress is associated with autonomic dysregulation. The sympathetic nervous system is jacked up. And Angiotensin Converting Enzyme (ACE)–Covid’s portal to human infection–is a major player.
Now throw severe acute stress from this virus onto the immune system.
https://www.ncbi.nlm.nih.gov/pmc/articles/PMC4465119/
Thank you very much. I have been reading/lurking here at NC for perhaps 10 years and this is a very thought provoking and insightful contribution – especially the conceptual link between vaccines and debt.
They are nuanced points that you raise and it’s a real credit to this site and community that it is not immediately torn down simply on a keyword basis.
Now I, too, need my own disclaimers: I have completely mainstream views on vaccines, am a typical[1] consumer of vaccines and do not typically take part in what I consider to be a foolish “debate”.
Your post reminds me of a thought experiment I have done, privately, in recent years and the experiment goes like this: Imagine you wake up with a superpower – a visual superpower – that allows you to now *see* cold and flu germ particles. Now let’s further stipulate that you are able to successfully use this new superpower to avoid the cold and flu for the rest of your life.
We all know what the upside of that would be: you would no longer experience colds or the flu. Which is fantastic. But my question is: would there be any downsides to that ?
Let’s say you’re 40 years old at the time of (gaining visual superpower) and you live the next 30 years exploiting the (visual superpower) … what does your immune system look like at age 70 ? What ramifications are there to not working up the response to the common cold every 1-2 years or the response to the flu every few years ?
This thought has germinated in response to a fairly rapid societal shift from “Influenza vaccine should be saved for elderly/compromised” to “failure to influenza vaccinate is identical to failure to rubella vaccinate” which I am conflicted about.
Perhaps the best response would be to just relax and purchase shares of GSK[2].
[1] Actually, not so typical – as a fire/medic in CA I am required to consume the influenza vaccine annually, and in my younger days as a naval reservist I was given a very, very comprehensive diet of vaccines.
[2] https://en.wikipedia.org/wiki/Pandemrix
Amen to nuance! I like your thought experiment. I would assume it would be a strain to be constantly avoiding viruses all day as well.
It comes down to short term benefit, right? We constantly point our technology to solving short term problems. Like the atomic bomb. We trade the current known outcome for the future unknown outcome,. I only see that as a problem when we use advanced technologies like agriculture and vaccines. Or maybe it is the advertising; always focus on the positives, never the negative, like a Trump Coronavirus update.
” It might be that vaccines are pushing the suffering onto future generations.”
Or it might be that vaccines are a major part of eliminating the suffering altogether, as it has with smallpox and rinderpest, and is in the process of doing with polio, malaria, syphilis, rubella, rabies et al.
Just because humans eradicated smallpox does not mean the world is a better place. I will agree it is better for human population growth, but that was not my point.
It seems that smallpox started with trade as well. Maybe that was the first lesson we should have learned.
Are vaccines making us less ‘fit’ in an evolutionary sense? That depends on the ecological niche we occupy.
We could abandon vaccines and our remaining children will be fitter for a virus laden niche.
Should we give up spectacles to improve our remaining childrens’ chances against rampaging tigers?
We made our choice a long time ago. We will make our own niche, one in which all our children can remain, because we do not measure their value by how resistant they are to viruses or tigers.
That choice has pros and cons but no-one’s going back deliberately.
Nature is the only one who will determine how well we fit in any niche. You say we made a choice like helpd long deliberations about it, but we didn’t.
We will go back, kicking and screaming like children. We are not the gods you think we are.
Not gods, just not dumb animals who have to put up with whatever nature does to us. Every time we do something to protect our (immediate) children we are choosing to give nature the finger.
Not many parents would sacrifice some of their childrens’ lives now in the hope that the descendants of the rest may gain some advantage in one small area of their evolutionary struggle. So we are going to remain dependent on vaccines until there are no more viruses.
Or you can look at it as a massive human population will help generate the diversity needed to survive the next challenge we can’t simply vaccinate away.
Yes, this was something I thought of, because by having more children people there will be more genetic diversity. But I was told that was an assumption by an evolutionary biologist. We do not need a large population for genetic diversity, we can have genetic diversity, like we have had for 100,000 years, by species separation in smaller groups.
This solves the problems that are caused by overpopulation as well.
Being dependent on a vaccines, we have artificially created a niche, and we could never survive the challenge of not having science or a vaccine. It might be overpopulation that kills us us all from war and aggression. Then do we vaccinate that away?
What are we seeing right now? The best protection is separation. Low tech!
On the topic of Dominic Cummings and Eugenics. Yes, it is true as can be seen from the following article which appeared in late February which was probably the time when the idea of herd immunity was being floated-
https://www.theguardian.com/politics/2020/feb/19/sabisky-row-dominic-cummings-criticised-over-designer-babies-post
The article has all sorts of quotes and thoughts by Cummings on this idea but I will quote one section-
In a blogpost published in 2014 after he had attended a Silicon Valley science conference at Google’s HQ, Cummings proposed allowing people to select eggs for their babies that appeared to have the best chance of having a high IQ, if genes for high intelligence could be identified in the future.
This was the plot for “Gattaca” – and he wanted it done through the NHS.
The irony is that IQ can really only be reliably used to detect subnormal intelligence. High IQ scores just show an aptitude for IQ tests.
https://supermemo.guru/wiki/IQ_is_a_dismal_measure_of_intelligence
Sorry I may have posted a comment regarding the availability of antibody tests in France in the wrong thread. It is here . Feel free to move it to this thread if you want.
Summary : 10-15€, self administered, no false positive, very few false negative 2 weeks after recovery, 1 million production capacity per month from July.
Exceptional post, great scientific information all in one place and unlike most peer reviewed written papers, is very well written and easy to understand. Someone else who has been hammering away at Covid-19 and Specifically why the U.K. is so [family blog]ed up is Dr.Richard North. His PhD deals specifically with the science of the spread of infectious diseases. He is as cranky as ever but when he sticks to the hard stuff it makes for very informed reading. He doesn’t have a very high regard for any “herd” theory. It all comes done to keeping well people well and sick people away until there is a vaccine. The rest could be a Netflix soap of stupid people doing stupid things.
you don’t need Netflix for that, all you have to do is watch the news
Re ‘herd immunity’. Immunity to something due to a genetic factor such as Krystyn’s would be transmissible to offspring in some cases. If the gene is dominant, the entire surviving herd would be permanently immune, if it is recessive only about 25% would be permanently immune. I wouldn’t consider that a success, unless your goal is a much smaller herd.
Acquired immunity, whether by vaccination or successfully creating antibodies on being infected, is not generally transmissible to offspring, and in many case, doesn’t even last in the individual — we are hearing 1 to 2 years for SARS and MERS infected, many vaccines require periodic boosters. So in a couple of years we’ll have to do it all again?
Yes, It is just like the financial system. QE is a flu vaccine for the economy. We need to get a shot of it every year now.
LOL! Because those durn unconventional financial instruments just keep on a-mutatin’.
Slightly off topic perhaps, but I wonder if part of the explanation for the “herd immunity” nonsense is our culture’s increasing tendency to substitute theoretical interpretations for practical knowledge. Just as we don’t export any more but we have highly complex models of International trade, just as we no longer have functioning organizations but we have management consultants to tell us how to ruin what’s left, so we have shattered and demoralized health services but we have mathematical models of how to manage epidemics. Indeed, if you look at the implications of the “herd immunity” policy, then the medical services, as such, are not central to it. It becomes a management issue, susceptible to output measurement and smart management for optimal use of resources (with bonuses). I wonder if a young twit with a degree in Really Theoretical Mathematics didn’t accost Cummings, saying “with my model we can defeat this epidemic without needing doctors.” Why, after all, labour to defeat problems in real life, when you can defeat them in a computer simulation?
The well known, gold standard in pandemic simulations is widespread testing and contact tracing with enforced quarantine for the sick.
If as you suggest, we are data driven to a fault, the people in charge might have used the last 30 years this was a known threat, to come up with a department capable of rolling something like that out.
Now, since our protectors in the government didn’t prepare to do any of that, they have given us the unofficial “Herd immunity debate” as a deflection and distraction from their failure. Now we can form our own worthless opinions, based on how little compassion we have vs. self interest, and bicker about them online (changing nothing).
It’s like Brexit all over again. This time the “Millwall fan” types are being agitated into being very vocal advocates for how expendable the lives of their fellows are.
It would be more acceptable if the “data” was accurate and useful. It isn’t. Numbers are not the same as data.
This reminds me of a quote I heard a while back : In theory, theory and practice are the same, in practice they are not.
I’ve observed the narrative shift in the weeks since lockdowns were instituted around the world. At first saving lives and flattening the curve were the key, if not the only considerations, with the economy only mentioned in passing, then a gradual shift to achieving a balance between curve flattening and managing the impact on the economy emerged. I expect the prominence to invert in favour of the economy in the coming weeks, relegating saving lives to a secondary concern, although the narrative will continue the appearance of a balance between the two. Talk about herd immunity and “risk adapted strategies” to reopening economies imho point to a level of resignation, if not soft capitulation, by our ruling classes that we are in virgin territory, that nobody knows with any certainty where things are going to end up and everyone is swinging wild punches in the dark and hoping to hit something.
As regards talk about mitigating irrepairable economic ruin, it sounds like a pragmatic approach to not make the cure worse than the disease of course, to say nothing of it being emotionally reassuring to the masses of people worldwide plagued by the incessant contemplation of uncertain economic futures. That said, the objective of protecting the economy (by restarting it) is at present wildly incompatible with the one of flattening the curve and saving lives. I have a sense that many of the strategies that will be devised to achieve a balance between these two objectives will end up on the cutting room floor and not see the light of day, or will be quickly knocked back after a short but unpleasant collision with reality. A lot of trial baloons will be popped before a credible path forward emerges. With the data that’s available at present, I see only two viable paths in front of us: develop and test a vaccine in record time, or cryogenically freeze the global economy until the last patient is cured of covid 19 (possible chronic debilitating disabilities aside), both admittedly outlandish and perhaps in the realm of wishful thinking. I will update my thinking as more data becomes available, but that’s what I see now. If covid 19 turns the whole world into a mortuary with corpses lining the streets, there will be no economy to save in any event.
The virus moves much faster than a restarted economy could be expected to reach even a sliver of its normal operating temperature, and a resurgence of infections will necessitate another lockdown. Added to this, real life isn’t like the internet where web crawlers could be sent out into the environment to scrape for actionable, near-real time data that could be used to make constant tactical adjustments to maintain a balance between these two currently incompatible objectives. Our governments have demonstrated incompetence at the best of times, now that invisible barbarians are storming the gates it’s difficult to see how the bubble wrap of ineptitude our leaders are ensconced in will suddenly give way to allow clarity, insight and purpose to come through. One thing is for sure, nature is providing us with an opportunity to beta test mega crisis response strategies because i’m almost certain this won’t be the last one.
only two viable paths in front of us: develop and test a vaccine in record time, or cryogenically freeze the global economy
Freezing the global economy presumably means no production, no distribution, and no consumption. No economic activity. No hospitals. Nobody searching for vaccines or treatments.
Is that really the only viable alternative to a vaccine?
BbcBy “freeze” I mean the only economic activity allowed is one generated by essential services, including the ones you mention. Relief packages by governments see to the survival needs of citizens during this time. As stated, I don’t see any viable path based on current data. Any attempts to prematurely restart the economy will falter very fast and these lockups we are all enduring right now will prove to have been in vain.
I don’t have the solutions, and I don’t believe those in charge of taking the decisions do, there’s a lot of spaghetti being thrown on a lot of walls around the world, and all the throwers are hoping something sticks.
Not expecting insight from idiots, I haven’t explored Johnson’s and Cummings’ version of herd immunity. “If everyone gets it some will die and the rest will be immune so the best policy is carry on as usual” seemed to be the essence of it, crap for several reasons.
However, it remains the case that many people will get it, and it’s still an open question whether survivors will have immunity or for how long. Medical Xpress has this take on the idea (not sure if their definition of H.E. is exactly the same as above):
Herd immunity
The fourth option may include carefully controlled transmission of the SARS-CoV-2 virus in select low-risk groups, which is an extremely dangerous path.
However, the almost complete absence of mortality in children and young adults may allow us to consider ways by which we can increase population-wide immunity, while protecting the vulnerable to avoid the huge rates of death seen in the elderly.
The term “herd immunity” has generated considerable controversy since the start of this pandemic. But ensuring a significant proportion of the population develop natural immunity to the virus—in a controlled manner—could be the only way to slow its spread while returning to our previous lifestyles, in the absence of an effective vaccine.
We still need to understand better the risks posed to young people from natural infection, as well as the strength and duration of natural immunity. But current indications are the disease is relatively benign in healthy, young people and that they do acquire immunity. This very distinctive pattern may provide a key to coming out of lockdown while minimizing risks—if an effective vaccine fails to materialize in the near future.
This option would need to be carefully controlled to ensure the virus cannot spread to the elderly and the vulnerable. How this could be achieved remains to be considered, but could involve the creation of environments in which transmission can be carefully facilitated among healthy young volunteers, without any risk of spread to the general community.
Natural immunity in a substantial proportion of the younger generation would allow those individuals to get on with their lives without putting others at risk. It would also slow any recurrent outbreaks that may occur once lockdown restrictions are relaxed.
Although there are no easy answers, we need to actively debate our exit strategy now, and collect the necessary information to guide our decision making. We may have to consider different solutions in different environments, but with an overarching strategy that is nationally coordinated.
“Now we’re in lockdown, how can we get out? 4 scenarios to prevent a second wave”
https://medicalxpress.com/news/2020-04-lockdown-scenarios.html
Can you say with confidence that children and young people who don’t die from COVID will also avoid diminished organ function? If a vaccine doesn’t manifest, will successive COVID infections further diminish those that didn’t escape the first round unscathed?
Yes, I know asking any to prognosticate about future cycles of COVID given all the unknowns is unfair, but we should keep the youth in mind along with worst case scenario when we start sketching life after quarantine. Or at least I would if anyone asked me…
I don’t think anyone can answer those questions with any confidence, and I’d be highly sceptical and suspicious of anyone claiming they can at this stage. That doesn’t mean we shouldn’t be asking. The young are getting infected, and apparently often recovering when they do get sick, which may have implications for where we go from here.
I’m beginning to think “herd immunity” is a way to sound smart while being dumb. The goal of these discussions is to reopen an economy that benefits the ruling class at the expense of everyone else, in this case with added panache so since lower income people have a much higher death rate. Essential services have continued and the government has full powers to continue writing checks to anyone who’s struggling — they merely choose not to do so. So the rush is motivated by people who are sad their asset prices have declined.
As Yves’ post examines in detail, there are too many unknowns to even begin to theorize how we’d achieve “herd immunity” safely. Repeat infections, curtailed immunity, permanent organ damage, R0 of 5.7 or higher, etc. At this point “herd immunity” doesn’t rise above the level of nonsense — it’s “not even wrong” to borrow a phrase.
There have been multiple deaths outside China of young people including infants.
In case it escaped notice, younger generations can’t afford to live on their own and don’t. They’re not going to keep their infections to themselves, but spread them to everyone they live with including Mom, Dad, and Grandpa, or all 4 of their roommates who also lack health insurance.
Anyway, we’re going to need a lot more treatment options to even consider resuming a bunch of critical big dollar industries like tourism and restaurants. At least we can look forward to a booming business in convalescent blood plasma (for however long their antibodies last).
Just wanted to add this link to the conversation. This is an interview with Michael Osterholm published on FXstreet on April 6th. He is basically saying what he has been saying all along. We are barely getting started with this virus.
https://www.fxstreet.com/analysis/covid-19-weekly-excerpts-from-a-covid-19-expert-conversation-202004060730
Interesting article with the usual bluntness of Osterholm. Thank you Steve.
If our military cargo planes really are ferrying PPE to Israel for the use of the IDF, this article will infuriate you.
No, it appears that this was a mis-translation. U.S. based representatives of the 51st State were simply using the blank checks provided to them by the U.S. DoD to purchase PPE from China. Not that the 51st State’s ability to fill-in blank checks drawn on the U.S. DoD account doesn’t drive-up prices for the other 50 States…
https://electronicintifada.net/blogs/ali-abunimah/did-us-just-supply-million-face-masks-israeli-army
Meanwhile, Santa Cruz has banned all surfing for the next week due to concerns about local hospitals lacking adequate supplies of PPE. I’m not making this up:
https://www.santacruzsentinel.com/2020/04/08/coronavirus-santa-cruz-county-temporarily-closes-parks-and-beaches-bans-surfing/
I was told in So Cal (San Diego environs) that beaches and parks were closed prior to March 25. I had mistakenly assumed that was state-wide.
State Parks here had closed their parking lots, but you could walk or bike in. Now they say they’ll write a ticket if you’re in the water.
Surfing has cult/religious status for Santa Cruz locals. Would have been better to put road blocks at the county line as this was really about stopping kooks from out of town from crowding the beaches. People are going to lose their minds…
One thing I noted in your link, the Israeli office in New York is supposed to use our aid to buy from US vendors. Is China now a US vendor?
“However, the mission of this office is specifically to purchase supplies for the Israeli military from US vendors, using US military aid”
Thanks Steve, that was a great share. And thanks Yves for a great article. And as usual I learned just as much from reading the comments as the article itself. SO many knowledgeable people here on NC. My takeaway from all this, and please someone correct me if I am wrong, is 1, our government has bungled the handling this pandemic, is still bungling it, and has no plan or leadership in place to handle the worse yet to come. 2, it seems like all we are really doing now is flattening the curve in the short term, but is a stopgap measure that will not work for very long. 3, we need to expect that the pandemic will reoccur in “waves” until a vaccine is developed and close to 100% of the world population is inoculated. To prepare for the long term and handle these “waves” we need to greatly strengthen our health care system, put identification, tracking, and tracing programs in place, and limit close proximity and touching of other individuals as much as possible. Sadly, I see none of this type of thinking or forethought occurring in our government. Fiscal band aids are the current cause celebre.
Another “elephant in the room” is the general health of population. Incentivized by a perverse economic system, we now have one or two generations raised on fast food & sugary drinks with predictable results of obesity related HPB, diabetes and other degenerative disease that cannot withstand a viral assault.
An economic system that advocates for unlimited environmental destruction and barbaric practices in creating factory livestock raising that flaunts natural law and severally damages immunity for animal and human existence on the premise that human beings need to glut themselves on vast quantities of animal protein. And ravages wildlife, all life forms and the environment for the most perverse and frivolous profiteering incentives.
As a society, how do we turn this battleship around? It would require an educational and economic system that purges the old incentives and produces major mindset and lifestyle changes, a generational project. I don’t see it happening.
Well, speaking of “herd immunity” I actually think we can change. It takes a percentage of the total population to bring change, sometimes (Rupert Sheldrake’s monkeys) only about 13% to bring about a change in the rest of the population. It’s like a very low infection rate. Already we see enough panic and dismay to know we have changed individually. And we are definitely confused socially; our reactions have been inept. So that can’t be tolerated again.
BTW, is there any example of “herd immunity” achieved through letting the disease run its course, i.e. not with vaccination? It all seems like nonsense to me for the simple reason that if it was so easy, then why were vaccines invented in the first place?
1918-19. It worked well then. Only 675,000 dead in the US and 50 million world-wide.
Smallpox, measles, and polio were others. Many of the Europeans developed immunities to them from surviving exposure but it wiped out the Native Americans in the 1600s-1800s.
Smallpox, measles, and polio were eradicated by the use of vaccines. There may have been some immunity but not enough to stop the diseases. People were still dying of these diseases in Europe, Asia, and the Americas before vaccines became commonplace. I think people who knew about these diseases were just more wary about interacting with the sick than Native Americans were.
Or maybe the Native Americans had not been exposed to similar diseases that activated their immune systems such as cowpox.
Read Charles C. Mann’s “1491”.
The Europeans died from these or recovered. That was a primary reason for fairly low lifespans. However, once they got sick and recovered they were generally immune. So it was a natural herd immunity effect where these diseases and bubonic plague would go in periodic waves.
Since these diseases were unknown to Native Americans, their genetics had very little self-selection over many generations for surviving these diseases and the impacts were an order of magnitude worse than for Europeans which effectively wiped out entire communities.
> Since these diseases were unknown to Native Americans, their genetics had very little self-selection over many generations for surviving these diseases and the impacts were an order of magnitude worse than for Europeans which effectively wiped out entire communities.
See Charles Mann’s 1491 and 1492, if you have not (apologies if already mentioned upthread).
There was no herd immunity with things like polio which was a constant nightmare for both parents and kids until what, the 1960s? Kids would disappear for months or even years and the next time you saw them they were in metal braces. It took a vaccine to take this monster down.
Well, the problem I have with that is these examples look more like “herd culling” than “herd immunity”. Just let the evolution do its thing and remove “weak” from the pool. Also smallpox, measles, etc. were finally wiped out by vaccination, so in a sense even herd culling didn’t actually work.
Hoof and Mouth disease might be a good model for testing the sanity of the ‘herd immunity’idea for dealing with COVID-19. Hoof and Mouth disease is caused by virus. Any rancher who decided to strengthen his future cattle stock by herd immunity could end up without much of a herd.
“Two important aspects of the pathogenesis of Hoof and Mouth disease lead to control problems. One is the ability of the virus to multiply in the pharyngeal region of vaccinated or even recovered cattle. Another is the ability of the virus to persist in cattle, sheep, and goats, but not in swine, for weeks or even months after all lesions have healed. Much circumstantial evidence shows that the persistently infected animals, referred to as carriers, can transmit virus to other animals and thereby cause new outbreaks of disease, but such transmission has not been shown under controlled laboratory conditions.”
“Hoof and Mouth Disease” [http://livestocktrail.illinois.edu/dairynet/paperDisplay.cfm?ContentID=603] This paper is from 2001 … but I don’t think much has changed.
I read your comment yesterday about how ranchers don’t practice herd immunity and I appreciated it very much as it put so much of the argument into context about economic interests. You are right. Ask people spruiking herd immunity why farmers and ranchers don’t practice herd immunity and watch for their answers.
I have not had the time to scour all of the above, but I have noticed in general that there is no reporting on two points. First, are any post mortems being done to attempt to determince the number of cases of death being caused (apparently) solely to Covid-19 as opposed to Covid-19 exacerbating pre-existing conditions?
Second, can pre-existing conditions be linked to social issues such as inadequate health systems as is the case in the US and other undeveloped nations?
Then, is there any indication that environmental conditions (e.g., gross air pollution) that cause damage to lungs and which are generally linked to economic ideologies provide pre-existing conditions leading to severe reactions to Covid-19 and deaths?
60% exposure is a number generally linked to network analyses that predict network robustness.
Finally, vaccinations are effective only when 60% or more receive vaccinations, i.e., join the herd in being immune. Herd immunity is another name for this 60% number. We will be safe from a reoccurrence of a pandemic only when we, the human population, acquires a cure or achieves 60% or greater immunity. We can only KNOW when this occurs via wholesale testing.
One reason that simply letting a disease run rampant through a population has not been attempted (but has occurrd inadvertently) is that letting people die is seen as immoral in most societies. A second reason is that this must be done worldwide and roughly at the same time..
And even if a vaccine exists and is administeredd on a worldwide basis, there is no guarantee that local outbreaks won’t occur. Herd immunity means that the outbreak is highly unlikely to become a pandemic.
There seems to be a reluctance to recognize that nothing will stop the spread of Covid-19. Deaths will occur. Many of these deaths will be linkd to our social reluctance to have a broadly available medical care system available to all. Many will be linke to ignorance. Many will never beunderstood.
“Misguided discussion of Herd Immunity?”
As someone currently abiding by all social distancing protocol, I am somewhat disappointed to read that those of us keeping an open mind to the ‘herd immunity’ concept should not do so. Especially when the sources for such an edict are the Guardian Newspaper and the plethora of model-making experts–warning of mass death yet changing their models on a daily basis–all over the mainstream media.
Part of the problem here may be a matter of language. Unfortunately demagogues like Trump and Johnson co-opted the term “herd immunity” early on in this crisis, and used it for their own ideological purposes. But the concept as outlined by the many medical experts that are speaking out against the isolate for “18 months and wait for a vaccine school of thought” are saying something quite different .
Perhaps a better way of putting it is that allowing mass exposure to the virus– in a approach that still protects the very elderly and those at risk –is mother nature’s vaccine.
To refute this hypothesis out of hand, or because we politicize the discussion unnecessarily seems unwise.
Here in British Columbia , with a population of over 5M people, we have had 1266 confirmed cases. As of April 7th 783, or 70% ,have already recovered. We have sadly lost 48 people.All very elderly or very sick. Which is a 3.1% mortality rate. But this fatality rate is very dubious because no one knows how many people have actually been infected. The trend rates around the world seem to indicate the same pattern–especially in countries with reasonably decent health care systems.
Naturally we are all entitled to our own opinions about what is going on here. And hopefully we will all continue to carefully evaluate the data as it unfolds. But woe betide us if we revert into hostile camps and denounce each other if someone dares raise a question based on information from a website we don’t particularly like, or a bungling politician we despise.
Certainly I am willing to abide by a total shut down–and possible collapse of the global economy– if actual peer reviewed science says it is necessary. I will also await a so-called vaccine solution , assuming one can actually be found, if the scientific evidence says the same thing.
But so far that does not appear to be the case. There is much dispute among very credible scientific authorities on this issue at the moment. It does not help that they are being excoriated and their arguments suppressed by some authoritarian minded officials.
Can we not at least facilitate a rational and respectful discussion about this subject without labeling anyone who questions the narrative of the dominant elites as “misguided?”
With R0 of 6 +/- 3 (the los alamos paper has spurious precision!), you need 85% immunity for herd immunity. Are your vulnerable <15% of population?
If the blood pathomechanisms are right, we may need to worry less about age and more about genetic traits like blood disorders like thalassaemia and, the biggie, being a man! Perhaps the second wave will be feminism? :-)
On the other hand if the blood disorders theory is right, we may have viable treatments and end up with a new TB, with coronavirus hospitals for mild and serious patients and everybody wearing masks outside….
Anybody referring to the R0 number is already on shaky ground. This from a comprehensive Atlantic article on R0:
“R0 is not easy to calculate. That’s especially true in the early days of an epidemic, when it’s not even clear how many cases there have been. Some people might have been infected without showing symptoms. Others might not have reported their symptoms to health authorities. Absent clear data on who has the disease, let alone how they’re moving around and interacting with other people, scientists have to calculate R0 by doing complicated simulations using a variety of possible methods. That’s why early estimates can vary so wildly, and why they should be taken with a grain of salt.
Read the rest of the article for FIVE other reasons why this number should be basically ignored by laymen!
https://www.theatlantic.com/science/archive/2020/01/how-fast-and-far-will-new-coronavirus-spread/605632/
Are you there, Yves?
There is a nightmare scenario which makes this idea sound like utter folly:
1) immunity to this corona virus is like other corona viruses and only lasts a few months.
2) many survivors of the infection emerge with long term or permanent lung, neural and heart damage.
#2 is bad enough, but if it comes back to hit you again and again every year? Egad!
You are going to have to work harder to convince me that getting sick is a good idea.
Who here is trying to convince you that getting sick is a good idea?
Dennis Brown seems to be saying an open mind is a good idea. Do you think a closed mind is better?
Some kind of herd immunity may already be occurring. Should we refuse to think about it just because idiots like Trump and Johnson use or misuse the term? Many appear to be infected without symptoms, and many with symptoms recover. Do we ignore these facts, or investigate further?
I’m concerned that we may not have any options besides “herd immunity”. Long term lockdowns only make sense if slowing the spread buys time to develop a vaccine or effective treatment.
I have a number of friends in academic biology/biochemistry departments who feel like a vaccine may not be possible (as mentioned in the article, it may not be possible to make an effective coronavirus vaccine). Effective therapeutics could take years to develop. If this is the case, what is the alternative to herd immunity? Indefinite lockdowns? Nobody is allowed to meet with friends, visit family, go to work (if “nonessential”), travel, date in person?
I can tell you that I’m in a moderate risk category (I’m in my early 30s but do have asthma and high blood pressure) but if my choices are live in lockdown for 2-3 years or take my chances on even a 3% risk of death, I will absolutely take my chances. I find being trapped in my small apartment in Chicago to be extremely depressing and I have never enjoyed “social media”. I live alone, having recently gotten out of a relationship. Not being able to socialize in person, travel (one of the things I enjoy most in life and I live over 1,000 miles from my family), go on dates, and go to work (I love my job and work long hours but it is very much worth it) would be intolerable for me.
Living in long term lockdown without being able to work, visit other people, or travel frankly isn’t a life I’d consider particularly worth living (and I’m betting their are a large number of people who feel the same way). If we really have to maintain this for 1-2 years or more, expect a huge jump in depression/suicides/domestic violence/etc. Humans are social creatures and eliminating the social aspect of our lives will have enormous negative consequences for mental health. I frankly don’t care about “the economy” but I still consider long term lockdowns (meaning 1+ years) a bad policy. I am fine with lockdowns even until the fall but only if we have a clear plan with concrete, achievable goals.
This is a comment to an article in Information.dk made by a person who has worked with virus called Henrik Leffers. https://www.information.dk/indland/2020/04/oeger-smitterisikoen-slippe-boernene-derfor-deler-vandene-eksperterne#kommentarer
“The corona virus is just one of many RNA viruses and all of us here have been infected with them many times, because they are the ones who give you the colds and various stomach problems. They all have virtually the same biology and the same life cycle, and they give different diseases because they affect different cell types and thereby different organs. But they have two things in common: none of them can be treated and there is no vaccines against any of them!
That they cannot be treated is not surprising, the only viral disease we can deal with is HIV (which provides AIDS), but we all know that the treatment requires that you take large doses of medicine every day for the rest of your life. All the treatments we have against other viruses are in effect just trying to alleviate the symptoms and do nothing to virus!
It means that we never get rid of this version of the corona virus! The only way to get around it is to “survive” an infection with it. For although it is mutating again ( all RNA viruses do!), it means that having had it, new mutants will “only” provide something that looks like a normal cold.
So it is unfortunately better to be infected by it, for then it gets easier next time. And I would like to add that we should perhaps consider to get those closest to us infected while the whole of society is geared to provide optimum treatment to make it easier next time! There is no escaping the virus! “
“There is already characterized almost a hundred mutants of covid-19, so it behaves like other common colds viruses and those you can very well be sick of several times. -And no RNA viruses of this type can “be in cells” because the DNA does not exist in their life cycle and RNA will not survive long in cells. The viruses which can cross into our genome is all DNA viruses (as herpes), or they have a gene which codes for a reverse transcriptase that makes a DNA COPY OF THEIR RNA genome (HIV).”
“For all RNA viruses the problem is that they mutate very quickly, so you must have a new vaccination each year to be updated to protect against the latest version of the flu virus.
So there will presumably come a vaccine against the corona virus we just now are exposed to, but it will only protect against the version of the virus we are affected by now!
There is already over 100 different mutants described, and that is precisely the ability to mutate that the common cold viruses can continue to infect us. But it is a new version of the virus each time as we can not be infected by any of them we have had because our immune system will catch them before they make us ill.”
This is a bit like the media complaining about lack of a control study on hydroxychloroquine. Who’s going to volunteer for the placebo fed control group?
From today’s Guardian:
US institute revises down forecast for UK coronavirus deaths