Yves here. I am featuring this post on Mauritius in part due to Colonel Smithers, but also because the way Mauritius responded to Covid-19 really puts the US to shame. On the one hand, they did have the ability to cordon themselves, even though that came at the high cost to their substantial tourist industry. On the other hand, they also quickly organized a number of relief programs, including food distribution to the poor and housebound.
By Jaime de Melo, Senior Fellow, FERDI; Emeritus professor, University of Geneva; Verena Tandrayen-Ragoobur, Associate Professor in Economics, University of Mauritius; and Boopen Seetanah, Professor, University of Mauritius. Originally published at VoxEU
When they are strict and prolonged, the public health and social measures to contain Covid-19 have proven difficult to respect. This column gives evidence of the different outcomes, as of 23 May, across a sample of 20 tourist-dependent island states with populations of between 100,000 and 10 million. If tourist-dependent islands have been hit hard by the shock, most have fared well, particularly those – like Mauritius – that acted early and imposed a strict lockdown.
The pandemic brings new information every day. Factors contributing to the large differences in trajectories are the subject of intense investigation (e.g. Helsinki Graduate School of Economics Situation Room 2020). This column summarises findings from our study of island states that have received relatively little attention (Melo et al. 2020). We cover the Mauritian case is covered in some detail, and compare it with 19 other island states from Our World in Data (OWD) with populations in the range of 100,000 to 10 million. The sharing of common characteristics across islands, limiting the sample to islands not exceeding 10 million people, is a first-pass crude attempt at ‘apples versus apples’ comparisons. Since some islands still have active cases, this is a progress report. We start with Mauritius, which closed all cases within 40 days (but see concluding paragraph), and then show that other islands that acted early, taking tough lockdowns with relatively long containment periods, have exited recently.
The Mauritian Case
Mauritius followed the ‘Act fast. Act now. Keep the lights on’ approach rather than the act slow, immunisation strategy followed by Sweden and, to a lesser extent, the UK. The health authorities followed the contact-tracing route. Figure 1 shows no active cases as of 17 May, with the last reported case on 25 April. Tests have been carried out on approximately 8% of the population, placing Mauritius in the top 7% in the OWD database and first in Africa with respect to COVID testing. With 10 deaths, the country’s naïve case fatality rate (CFR), a standard estimate of the lethality of a pandemic, is 3%. Notably, the low death rate during the first quarter was helped by the lower death toll from road accidents.1
Figure 1 Timeline of confinement measures
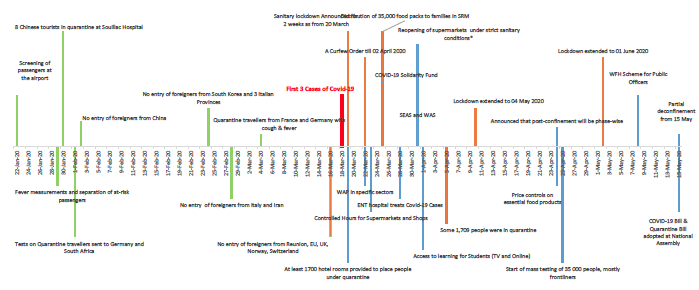
Source: Authors’ compilation from BeSafeMoris and press announcements, 2020
Notes: (1) WAP: Work Access Permit; (2) WFH: Work From Home; (3) WAS: Wage Assistance Scheme. The scheme targets businesses in the private sector and their employees drawing a monthly basic wage of up to Rs 50,000; (4) SEAS: Self Employed Assistance Scheme. The aim of the scheme is to assist self-employed persons who have suffered a loss in revenue as a consequence of the lockdown.; (5) *Customers are allowed to enter supermarkets as per alphabetical order on specific days. They must have their national identity cards and wear masks. Basic essential products are also limited to three units per person.
Baldwin (2020) views containment policies as balancing infections and tolerability. Public health and social measures must stay in a ‘corridor’ where they are stringent enough to avoid overwhelming hospitals, but lax enough to avoid exceeding citizens’ tolerance levels.
Health-Related Measures
Figure 1 shows the timeline of the containment measures in Mauritius. The combination of preventing foreign travellers early on and the stay-at-home measures have prevented overload of the healthcare system – by reducing what Pueyo (2020) calls ‘seeding’ and ‘spreading’. Screening started on 22 January, with suspected tourists quarantined. These precautionary measures must have contributed to a relatively small pool of ‘suspected’ when the first three cases were announced on 18 March. Two days later, a strict lockdown (only health and essential workers could leave their residences) was put in place for seven days.2 A reopening of supermarkets was allowed under strict conditions from 30 March. The lockdown was extended twice until 1 June, with the re-opening of the economy taking place in phases, starting with government services and other essential services on 15 May. Cabinet and health officials aired daily progress reports every evening in the three languages (creole, French and Hindi). People were warned of severe penalties for breaking the confinement measures and for issuing false news.
Wealth-Related Measures
Daily press communiques by the COVID National Communication Committee helped calm the population. At the start of the lockdown, the government announced the immediate distribution of 35,000 food packs to families in poverty (as per the Social Register of Mauritius), to the disabled and to at-home residents. All labour contracts set to expire this year were extended through to December 2020. Wage and income support measures to employers were introduced, ranging from US$125 to $315 for workers with salaries below $625 (15 days’ salary basis) per month to $315 for those in the $625-1,300 range (through the Government Wage Assistance Scheme). Workers earning over $1,300 received no support. Self-employed individuals as well as trade persons in both the formal and the informal sector received financial support of U$130 (equivalent to half of the monthly national minimum wage) through the Self-Employed Assistance Scheme (SEAC). These measures were extended until 31 May. The government also announced about 1.6% of GDP increase in spending along with extra tax deductions for SMEs.
Mauritius does not have unemployment insurance, but free health coverage is universal and all citizens over 60 receive a pension of around $300 per month. These social support measures compare favourably with those provided in higher-income countries.
Hit hard by the fall in tourism receipts, estimated to result in a reduction in GDP above 10% for 2020, Mauritius was successful in eliminating the spread of Covid-19 in 40 days. The government acted early and decisively at the outset. Stringent policies aided by geographical factors contributed to meeting the health constraint. Substantial income support contributed to meeting the wealth constraint, keeping the country in the narrow ‘stringency corridor’.
How Unique Is Mauritius? Comparisons With Other Islands
Figures 2-5 compare episodes across 20 islands, from the start of the first declared case in each country up until 23 May. Data are spotty. Figure 2 reports data on country characteristics (population and per capita GDP), estimates of total tests per 10,000 where available, total cases per 10,000, and the value of the composite ordinal Stringency Index (SI) on containment and closure measures (the Oxford COVID-19 Government Response Tracker, OXCGRT) at the end of the first week of reported cases. Figure 3 compares the SI index against the measure of mobility reported in the Google mobility tracker at the end of week 1 and week 4. Figure 4 reports a crude estimate of lethality – namely, the case fatality rate (CFR). Figure 5 reports the evolution of closed cases (recovered plus deaths over total cases) on a weekly basis. At best, available data allow for caveat-ridden comparisons.
As an example of diversity across islands, Ireland and New Zealand, with similar populations, had their first cases one day apart. Neither tested extensively, but New Zealand started with more restrictive policies, ramping up with yet more restrictive policies as reflected in a greater reduction in mobility (Figure 3). Figure 4 shows that Ireland has the highest number of cases and is among those with a high CFR. By contrast, New Zealand has both few cases and a low CFR. Contrast also Puerto Rico (2.8 million) with Bahrain (1.7 million). Puerto Rico has fewer cases but a higher CFR than Bahrain, the lowest in the sample.
Next, compare ‘successful’ countries. Fiji reported 18 cases, no fatalities and has only 3 active cases (Figure 5). With a CFR of 0.5% (Figure 3), Iceland, an early reporter, is among the most successful. It succeeded with the combination of the highest testing rate and relatively loose containment measures (the lowest SI score after 2 months, possible because randomised testing allowed the infected to be isolated).
In sum, no patterns appear across the islands beyond the observation that low testing rates are generally associated with a low case rate. With the exception of Mauritius, containment measures tightened over the weeks. Figure 2 reveals no correlation between current case rates and population. Neither is there a correlation between case rates and per capita GDP, or between the case rate and the number of days date since the date of the first reported case. However, the correlation between the case rate and population density (not reported here) is 0.6.
Figure 2 Anatomy of Covid-19 in island nations (populations between 10,000 and 10 million)
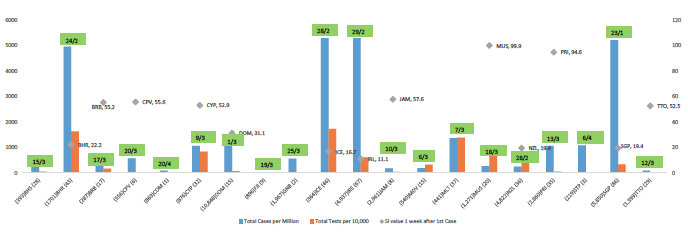
Source: Authors’ Compilation of data for 21 Islands from Our Word in Data (OWD), Worldometer and Oxford COVID-19 Government Response Tracker, 2020.
Notes: (1) Left-hand axis: Number of confirmed Covid-19 cases per million as of 23 May. (2) Left-hand axis: Total Cumulative tests per 10,000 as of latest date available. The data is not strictly comparable because of different reporting and multiple tests per person. Different data sources- Wikipedia, Our Word in Data (OWD) and Worldometer, 2020. Data on the number of Covid-19 tests effected is not available for Comoros. The cumulative Covid-19 tests per 10,000 are on the very low side for Suriname, Sao Tome and Principe, Guinea Bissau and Haiti. (3) Right-hand axis: Stringency Index (range: 0-100: higher values indicate stricter confinement measures). Data taken one week after first reported Covid-19 case in OWD. (4) Data on Stringency Index (SI) is not available for Bahamas, Fiji, Guinea Bissau, Haiti, Maldives, Malta and Sao Tome and Principe. (5) First Covid-19 Case for each country is included at the top of each bar chart. (6) Horizontal axis: Population in thousand, Country Code, GDP per capita in thousand USD. Figures rounded to nearest thousand for population and GDP per capita. (7) Country Codes and Names: BHS- Bahamas; BHR- Bahrain; BRB – Barbados; CPV- Cape Verde; COM- Comoros; CYP- Cyprus (excluding North); DOM- Dominican Republic; FJI – Fiji; GNB- Guinea Bissau; HTI- Haiti; ICE- Iceland; IRE- Ireland; JAM- Jamaica; MDV- Maldives; MLT – Malta; MUS- Mauritius; NZL- New Zealand; PRI- Puerto Rico; STP- Sao Tome and Principe; SGP- Singapore; SUR- Suriname; TTO- Trinidad and Tobago.
Figure 3 plots the value of the SI index against the average reduction in weekly mobility relative to the average during the month of January for two dates: week 1 and week 4. This is a first check of the effectiveness of measures to prevent ‘spreading’. The association is strong for both periods (0.91 and 0.93), confirming that the SI value is a useful proxy of the strictness of containment measures as captured by aggregate mobility.
Figure 3 Stringency Index and average mobility reduction one week and one month after first reported Covid case
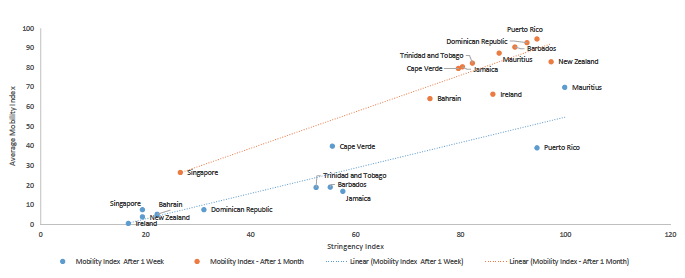
Source: Authors’ Calculation from Oxford COVID-19 Government Response Tracker, 2020 and Google Mobility Report 2020.
Notes: (1) Data on mobility is the average reduction in mobility relative to the reference period (average over Jan 3 to Feb 3). SI index ranges from 0 and 100. Higher values indicate stronger confinement measures. (2) Data on Mobility for Singapore is taken for the 6 weeks after the first Covid case. (3) No SI data for Bahamas, Guinea Bissau, Fiji, Haiti, Maldives, Malta, and Sao Tome and Principe. (4) No data on Mobility for Bahamas, Iceland, Maldives, Cuba, Cyprus and Suriname
The SI was low for all countries in week 1 except for Puerto Rico and Mauritius. However, for Puerto Rico, a pronounced reduction in mobility was only registered in week 4.3 Second, except for Mauritius, all countries ramped up restrictions between week 1 and week 4. This was accompanied by a decrease in mobility from 10-20% to 70-90%. ‘Stay-at-home’ was greater than in the US, which registered a 30% decline in mobility over the same period. Third, Mauritius is the only country that put the brakes on immediately, relaxing restrictions marginally by week 4.
Figure 4 gives an estimate of the lethality by reporting the CFR based on total confirmed deaths. This is a crude estimate of deaths because cases will have gone undetected (not tested or tested but returning a false negative) and deaths are recorded differently across countries. Still, the cluster of countries with 10-20 reported deaths suggests that these late comers in the pandemic have managed to contain the spread relatively well. The figure also shows a large range in CFR estimates. Assuming that Iceland, Cyprus, Malta, New Zealand, Mauritius and Singapore have the more reliable estimates cases because of more extensive testing, even if was not random (except for Iceland), still leaves a very wide range (0.25% to 3%) of CFR estimates.
Figure 4 Total confirmed Covid-19 deaths versus cases, 23 May 2020
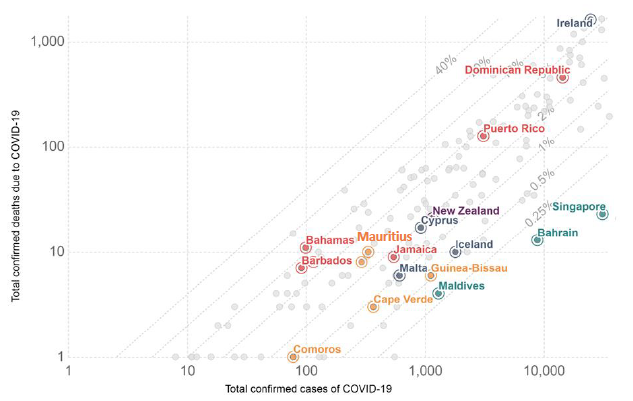
Source: Our World in Data, 2020
Note: Due to no reported deaths, Fiji is not in the figure.
Figure 5 shows the evolution of closed cases (recovered plus deaths over total cases) on a weekly basis. On the top, starting from the left, a group with a smooth weekly progression path features Iceland, Mauritius, Trinidad and Tobago and New Zealand and Fiji. Indicators suggest these countries have controlled the spread and exited. Ireland and Malta still have many cases but appear to be on the path of closing cases, though with a high CFR for Ireland. Malta (CFR of 1%) and Cyprus (CFR of 2%) have managed relatively well. Maldives shows new cases, probably a result of increased testing. Singapore, well-covered in the press, is an example of spreading through close group contacts in a high-density environment. The others are still active.
Figure 5 Share of closed cases (weekly averages since first reported case)
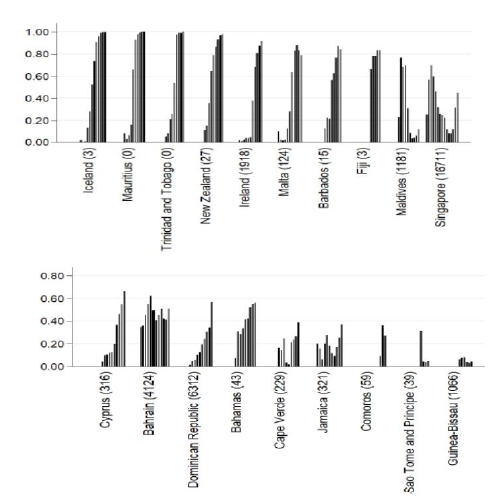
Source: Authors’ calculations from Worldometer
Notes: Weekly averages since week of first reported case. Number of active cases as of 23 May in parenthesis
In sum, in spite of common characteristics, the group of islands covered here followed different containment strategies and mostly avoided a run on their healthcare systems. Among the more successful, Fiji, Mauritius, and New Zealand followed a strict path of contact tracing. Mauritius also followed a strict 40-day long confinement strategy early on, accompanied by substantial income support. This combination kept the country in the ‘stringency corridor’. New Zealand achieved the same. Fiji, Iceland, New Zealand and Trinidad and Tobago have also succeeded following a more progressive containment path. Others tended to follow less-aggressive containment strategies.
As a reminder that this is a ‘work in progress’, as we were finalising this column on the evening of 24 May we learnt that two passengers on a return flight from India to Mauritius on 10 May tested positive in quarantine on 23 May. These passengers had tested negative before leaving on 9 May and again during quarantine. It was only on the second and last test before exiting quarantine that they tested positive. This news has not been well received by Mauritians, who were already pleading with the government that, with no new cases since 25 April, the containment measures should not be continued until 1 June. Navigating the health and wealth constraints is also proving difficult on islands!
Editors’ note: This version of the column, written on 24 May, replaces the original version written on 17 May. A shorter, wider-audience version appeared in Le Defi Media Group on 20 May.
See original post for references


Many thanks, Yves.
I am glad that you found something in English. Much of the coverage has hitherto been in French, hence my reluctance to share.
Unfortunately, the island is not out of the woods. In addition to tourism, or lack thereof, climate change, a possible, if not probable, EU blacklisting later this year for not taking money laundering seriously, and the demise of the sugar and textile industries mean that the island has some tough years ahead.
One hopes that readers will be able to visit this beautiful and friendly country.
When you think about it, the Coronavirus pandemic has really become a ‘touchstone’ of good governance in countries across the planet. If asked a few months ago, I would have said that small countries like Mauritius would be primed for failure but I would have been (happily) wrong. A lot of small countries have had outstanding success in tackling the pandemic while larger, more wealthy countries have made a proper dog’s breakfast of their response. I do wonder if this will effect the standing of different countries going forward as investors, for example, will see that such countries are good places to invest in.
“I do wonder if this will effect the standing of different countries going forward as investors, for example, will see that such countries are good places to invest in.”
Considering what “investors” do to countries, I kinda hope NOT.
It seems to me that “what the world needs now” (to quote a song) is a steady-state economy, not an investors’ economy.
Some new news is that there may be a useful link between covid 19 and the old MMR vaccine. Many countries with up to date MMR vaccinations programs seem to be faring much better with recent serious cases and deaths. Use or lack of the MMR explains a lot of things in a lot of places. Like Madagascar and American Samoa for example. Brazil and the Teddy Roosevelt.
https://www.researchgate.net/publication/341354165_MMR_Vaccine_Appears_to_Confer_Strong_Protection_from_COVID-19_Few_Deaths_from_SARS-CoV-2_in_Highly_Vaccinated_Populations
https://www.medrxiv.org/content/10.1101/2020.04.10.20053207v1.full.pdf
Perhaps worth mentioning in this context, the situation regarding Covid-19 in Cuba, another small country depending heavily on tourism (the first three detected Covid-19 cases were Italian tourists).
Total population: 11.3 million.
Total cases: 2005.
Total death: 82.
Let’s not forget, the current US administration reinforced the embargo against Cuba last April.
Cuban doctors have been helping in the fight against Covid-19 in China, Italy, Andorra, and several Caribbean and African countries.
You wouldn’t know any of this by reading the US or Western mainstream media.
Correction about “last April”, in my above comment. I meant April, 2019. See link for announcement by then U.S. national security adviser John Bolton:
https://www.reuters.com/article/us-venezuela-politics-bolton/trump-security-adviser-unveils-new-u-s-sanctions-to-pressure-cuba-venezuela-idUSKCN1RT29X
Apologies for the mistake.
It’s not so funny in nearby Mayotte (part of France, legally). https://www.francetvinfo.fr/sante/maladie/coronavirus/coronavirus-pourquoi-la-situation-a-mayotte-est-inquietante_3962453.html
I think one of the lessons from the New Zealand response (note the move from top right to far lower left in the graph) is that restricting mobility is extremely effective, if costly. At the risk of stating the obvious, the virus cannot move on its own – it must hitchhike. By locking people down to their immediate neighborhoods and restricting all travel, NZ placed a hard limit on the potential maximum rate of geographical spread. This meant that while we had some quite large clusters from the pre-lockdown period, they stayed local and didn’t trigger further clusters or exponential growth.
The main exception permitted, and the reason for most movement during the lockdown, was grocery shopping. But because it was only an hour a week, and everybody concerned knew that it was by far the riskiest thing they would do that week, compliance with public safety measures was very good. I’ve read no reports of transmission in supermarkets from that period, which is quite remarkable given that it was our main contact with other humans in that critical first 1-2 weeks when growth was still rapid and just starting to flatten to linear from exponential. We all knew that that was the one transmission vector we couldn’t eliminate, and behaved accordingly. There was nothing quite like a trip to the supermarket during lockdown to remind you how serious it all was – I still have vivid memories of mine.
The one thing NZ never did was encourage mask wearing. I’m still unsure why this was. I think it might have been because there is a high inconvenience factor associated with them, and because they were already asking a lot of us with the lockdown they may have decided it wasn’t the best use of their political capital. People were also starved of social connection during that time, which masks further inhibit (you’d see people having long conversations from opposite sides of the road, for example). In general the theme during the lockdown was to avoid all contact (so if you were close enough that a mask might be needed, you were too close) but they never required them of supermarket shoppers, for example, although staff did get PPE.
Unfortunately, this good news is negated somewhat by the death of Romeo “Romy” Castillo Jr, (34) earlier this week.
https://www.standard.co.uk/news/health/romeo-castillo-travel-agent-dies-coronavirus-trip-mauritius-a4452906.html
At what point Castillo caught the virus will probably never be determined, but in any case, it does no favours to Mauritius as a vacation destination.