Yves here. Universal testing and isolation were the South Korea approach, except they geared up so quickly, their testing only had to be aggressive and extensive.
By Reda Cherif and Fuad Hasanov, Senior Economists at the IMF. Originally published at VoxEU
Lockdown measures, contact tracing, and widespread testing have dominated the policy responses of many countries to the Covid-19 crisis. This column argues that a universal testing and isolation policy is the most viable way to vanquish the pandemic. Its implementation requires an epidemiological, rather than clinical, approach to testing, and requires the ramping up of testing kit production in order to achieve a scale and speed that the market alone would fail to provide. The estimated cost of universal testing is dwarfed by its return, mitigating the economic fallout of the pandemic.
The world is racing against time to vanquish Covid-19, the disease resulting from the novel coronavirus that spread rapidly across the world in early 2020. After millions of cases and hundreds of thousands of deaths (Johns Hopkins University 2020), extraordinary strains on healthcare and medical personnel, national lockdowns, and economic fallouts unseen since the Great Depression of the 1930s, the world has yet to see the emergence of a viable global strategy (Baldwin and Weder di Mauro 2020a, 2020b).
A Return to Normalcy
As lockdowns were implemented to ‘flatten the curve’, the debate about saving lives or saving jobs ensued (Chang and Velasco 2020). However, the policy debate should be about expanding the frontier of how much economic activity could be pursued while keeping the epidemic in check (Budish 2020). What is needed is an assessment of the viability of policies in terms of the speed of reopening the economy with minimal restrictions, the efficiency in keeping the epidemic in check in different contexts (advanced versus emerging and low-income countries), as well as policy cost. Keeping minimal restrictions on the majority of economic activities is key to ensuring policy viability. Policies based solely on strict non-pharmaceutical interventions (e.g. full or age- and geography-dependent lockdowns) would not be viable as they would slow down the epidemic, while not helping reopen economies fully and safely. Many of these measures, such as lockdowns or contact tracing, would also be difficult to implement in developing countries, or past a certain epidemic stage.
We argue that the most viable way to vanquish the pandemic is a universal testing and isolation policy (Cherif and Hasanov, 2020). Using a modified Susceptible, Infected, and Recovered (SIR) model with R0 of 3 and a 25 percent leakage of the quarantined, we argue that a continuous universal testing and isolation of the infected would keep the epidemic in check. Combined with “smart” testing strategies such as group (pooling individual samples for testing) and periodic testing as opposed to random testing (e.g., using blocks of population by a geographic grid) the testing rate required would be about 5 percent of the population per day instead of 20–30 percent of the population with random and individual tests.
An epidemiological Approach to Testing
To succeed, policymakers should adopt an epidemiological, rather than clinical, approach to testing, sacrificing accuracy (sensitivity and specificity) for scalability, convenience, and speed. The aim of this approach is to identify (and isolate) ‘enough’ infected individuals, rather than to provide a precise clinical diagnosis. Rapid serological tests for antibodies (IgM) or antigens, which are similar to pregnancy tests, and Point-of-Care (POC) rapid molecular tests could be good candidates to reach a large share of the population. Including ‘symptom-based’ tests to identify infected patients could further reduce the number of required tests to below 5%. This type of ‘test’ (including fever measurement) could be implemented immediately, albeit at the cost of isolating many false positives, but still at a fraction of the cost of a lockdown.
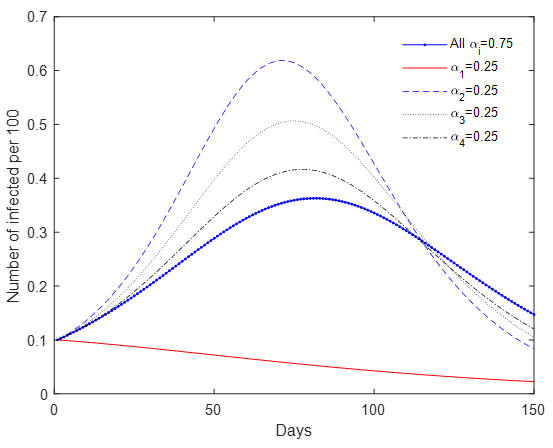
Universal testing could be further complemented with other ‘smart strategies’. Mobility restrictions in and out of urban centres could help reduce contagion across cities and regions, and minimise the number of tests needed overall. In an SIR model with mobility and universal testing, we show that with the same testing rates, restricting movement to ‘the hub’ by 75% reduces infections from day 1. In contrast, reducing movements to any grid by 75%, or to all grids by 25%, results in a resurgence of infections, or ‘second wave’ (Figure 1). This approach promotes the idea of ‘urban villages’, and minimises restrictions on economic activities. In the same vein, prioritising potential infection clusters (e.g. hospitals, care homes, prisons, schools, and public gatherings) could reduce the spread of the virus spread substantially, since approximately 20% of infected cases generate around 80% of subsequent transmissions due to ‘super-spreader events’ (Adam and Cowling 2020). Light non-pharmaceutical intervention measures such as maintaining distance in public and mask wearing could further reduce transmission rates.
Figure 1 An SIR model with mobility across four grids: Travel restrictions by (1-a) percent (grid 1 is a hub)
To ‘squash the curve’, universal periodic testing needs to be continuous, until a safe vaccine or a cure is developed. An early warning system could help monitor and control the spread of the infection. Alternative methods could be used to detect infection clusters, such as testing for the virus in sewage systems, a method used to assess the vaccination campaign against polio (Mallapaty 2020).
Countries or regions that have used large-scale testing have slowed the epidemic substantially. At the onset, South Korea conducted widespread testing that helped it keep the epidemic spread in check (Cheong 2020). In Italy, the region of Veneto achieved a much slower progression of the epidemic, mostly due to its large-scale testing and isolation (which included asymptomatic people), in comparison to Lombardy. The small town of Vò (in Veneto) conducted universal testing of its population and isolated the infected before and after the two-week lockdown; the virus was wiped out as a result (Zingales 2020).
Although there is a growing chorus of voices arguing that testing is key, there is no consensus on how much testing is needed (Romer 2020a, 2020b, Siddarth and Weyl 2020, Baldwin 2020, Berger et al. 2020, Brotherhood et al. 2020, Eichenbaum et al. 2020, Bethune and Korinek 2020, Acemoglu et al. 2020, and Piguillem and Shi 2020). Our own simulation results – about 5% of the population per day – call for a smaller number of periodic tests than Romer (2020b), and a broadly similar number of tests as proposed by Siddarth and Weyl (2020), in order to keep the epidemic in check. Testing rates in many countries (including smaller economies) fall far below these rates. By late June 2020, the maximum daily (on a 7-day rolling average) population testing rates have been achieved by Luxembourg (0.9 percent), Bahrain and Iceland (0.5%), and Denmark and Lithuania (0.25%) (Roser et al. 2020).
Universal Testing Is Feasible
Although experts agree on its ability to ‘squash the curve’, universal testing has not gained much traction because it has been considered ‘infeasible’. Indeed, the sheer number of tests needed compared to current production in each country, and the difficulty of scaling up collecting and processing samples, could suggest that this task is impossible (e.g. Kofler and Baylis 2020, Rose 2020). Huge shortages of ventilators and personal protective equipment across the world, including in many advanced economies, seem to confirm this view (e.g. Azmeh 2020, Bradley 2020).
The perception of the infeasibility of universal testing stems from the adoption of a clinical approach to testing, as well as a laissez faire approach to production. Even the rate of approximately 5% of population a day (with a smart epidemiological approach and cheaper tests) would still be far beyond the existing production capacity of most countries and could seem infeasible if one ignores market failures.
Indeed, the market for tests in the context of a raging pandemic is laden with market failures stemming from uncertainty, capacity constraints, coordination failures, externalities, and market power. Industrial policy is needed to correct these failures (Cherif and Hasanov 2019) and ramp up the production of tests. We sketch such a strategy to define clear objectives in terms of testing rates. Policymakers should: set up an appropriate institutional apparatus to coordinate government agencies and the private sector along the whole value chain, align incentives (e.g. financing and intellectual property), and enforce accountability when support is provided (Cherif and Hasanov 2020).
The feasibility of a rapid scale-up in the production of tests is akin to war mobilisation efforts during WWII, when the US and the Soviet Union drastically increased their production of military equipment at an unprecedented scale and in a record amount of time. For example, ammunition factories were built from scratch in as little as three months. The existential threat of war motivated policymakers to spring into action. Although not trivial, the current task is minuscule in comparison, yet the danger of an endemic pandemic is real and entails enormous costs. The global cost of testing is only a small fraction (about 1-2 months) of the 2020 global economic losses and fiscal stimulus (about $20 trillion). To put this into perspective, the number of testing kits needed is only a fraction of the number of soft drink cans consumed globally (about a trillion per year), as Romer (2020b) has also pointed out for the US.
Global support and coordination could make universal testing possible. Similar to the huge government resources invested in vaccine development, the same strategy is needed to develop rapid and convenient tests. If enough firms pool their resources (and there is substantial public funding, support, and coordination), most countries could meet the demand for tests relatively fast. Recent developments give hope that a vaccine, or a cure, could be found within a year, but there is no guarantee. Betting only on a safe vaccine or a cure to vanquish the pandemic illustrates the ‘incredible certitude’ of policymakers (Manski 2019). With the enormous costs and risks of a protracted crisis (especially in developing countries), universal testing, which could be implemented in a matter of months, would be a viable alternative strategy.
Authors’ note: The views expressed in this column are those of the authors and do not necessarily represent the views of the IMF, its Executive Board, or IMF management.
See original post for references


Makes sense. A. Can it be implemented? B. Would the tracking methods and enforcement of consequences for breaking quarantines be taken?
A. The epidemic has been relatively good for the elite in the US. Thanks in part to trillions in bailouts to wall street stock indices are near record highs. Will it be possible to get agreement to put resources into this testing plan, as opposed to other perhaps more lucrative choices?
B. Anecdotally, at the local costco here in central VA, yesterday I noted more customers with either joke masks (bandanas below the nose etc) or even saw an elderly couple wearing sheilds with no masks at all. For the quarantine portion of the plan to work there has to be real support (apartments or hotel room’s, food delivery, etc) plus real enforcement – checking on compliance, probably some tracking app as the Koreans use, and consequences for failure to comply.
The plan could work in may countries but I doubt the US or say Brazil under the current leadership has the capacity.
I’m surprised that your local Costco does not do more to enforce the mask mandate. Around here they are pretty militant about it.
why economists think they understand epidemiology?????
This was published last May: “The surprisingly simple way to open America in 14 days and avoid a depression”
Makes quarantine unnecessary.
Hmm. Cost of testing, X% of the population daily, vs the cost of 25% unemployment for 6+ months, going on however long? Should be a no-brainer.
Repost of some numbers, more on-topic here. My point will be that testing 5% of the population is a pretty tall order (but not because of the $$ cost). There will likely be a vaccine by the time it is available.
Start with China. As of late July, they’re claiming (pooled?) test capacity of 4.8 million/day, or 0.34% of the population. [National Health Commission of China]. The press release touches on some limiting factors: Technicians (38000, or one for every 128 test capacity), Reagents (capacity equiv 6.5 million tests/day), ‘analysis units’ (analyzer machines??) (adding 170/day).
US is doing 0.75 million tests/day [Johns Hopkins], recently dialed back a bit to relieve the backlog / delays. Anyway, that is 0.22% of population per day. A first generation of lower quality but faster point of care devices is in the pipeline, due to emerge in 6-8 weeks if optimistic. A second generation is entering the pipeline, due by end of year. Each of those generations supposedly corresponding to capacity on the order of 1% of population/day, but good luck getting a clear answer on any of this from HHS’s inconsistent statements.
Also, China fought and won their first round battle with the epidemic before they had any of this. What they had was masks, temperature checks, mandatory big-brother level contact tracing, cordon sanitaire, and strict enforcement of quarantines.
Testing is an invaluable guidance tool, which should make similar results possible with less draconian measures. But what actually stops the epidemic is still isolation and contact tracing. As we can see in the US, contact tracing is not effective due to overwhelming case load, isolation is implemented haphazardly, and the epidemic remains out of control.
“These are not the externalities you are looking for”
– Toby Wan Kenobi, Ben’s Economist brother.
Short video interview with Michael Mina on Cheap Rapid Daily Testing
https://www.medcram.com/courses/antigen-highlights?wvideo=k6ki6losyk
https://www.harvardmagazine.com/2020/08/covid-19-test-for-public-health this is a link to a helpful article basded on an interview with Mina.
This idea is really based on detecting infectious individuals cheaply and quickly – and therefore almost universally. Mina points out that the antigen test, from an infection control point of view is in fact more sensitive than a PCR where the Ct number is not routinely revealed (ie you are +ve or -ve for viral RNA). The PCR, even if people got the tested when needed and the results returned within a day (not happening or ever likely to happen), keeps returning a positive result during the long tail of days (after the c1 week of infectivity) when the person is no longer infectious. This drastically reduces the sensitivity of the test in determining if a person is infectious and hence its usefulness in controlling the epidemic. Cheap, rapid, even possibly do-it-yourself antigen tests register reliably positive almost (might miss a few hours as replication takes off) as soon as the viral load passes a now known threshold needed for transmission and, more importantly, ceases to do so as viral load falls off below that threshold. The fact that such tests can be done frequently means (explained in the article) contact tracing would no longer be necessary. Schools could open safely as could work places….. and on and on…
the problem in getting this generally accepted and then approved seems to be the confusion with use as a diagnostic tool and the need for FDA approval – then how to ramp up production capacity to produce hundreds of millions of doses….
just now it seems there isn`t the will on high to get this thing under control….. but the fight seems to be on with this proposal gaining traction!!
Dr. Mina’s approach seems ideal. Low cost ($1-$2), self-administered, self-evaluated, immediate results, renders contact tracing unnecessary, results only positive if you are INFECTIOUS, which is exactly what you need from a public health point of view. It’s irrelevant if you had it 3 weeks ago. Just take the test every day, and quarantine yourself if positive. I fail to understand why this is not universally adopted NOW. He says the major hurdle in U.S. is FDA approval, which so far has not been given. Everyone should write to Congress people, Governors, and Mayors to lobby for adoption and for FDA approval. The reduced sensitivity of this test is actually a good thing, not a bad thing.
Could one of the states that was told it was on its own do this on its own and set an example? (If they could find the money, that is. I’m presuming someone in the state could round up the know-how. How long ago was it that nc had a link to a brewery that figured out it could do basic screening tests with its own in-house equipment.)
Makes sense right? Works like a home pregnancy test (those are down to $4 ea at wal mart online) but with oral sample.
However, for a lateral-flow type antigen test, it looks like the federal govt is going with a Quidel product, at least according to this summary [NIH] of the manufacturing-ramp-up grants, via the $500 million RADx program. Quidel got $71mm according to this. There were some earlier phase grants in the million $ ballpark for antigen tests on saliva, awarded in the spring, but I don’t know what became of those.
An even bigger pile of development money, from what I can tell, was spent for some of the first generation of ramp-ups for the various genetic tests.
Also, I think $4.5B was given in the HEROES Act to the office of the secretary of HHS. The part relevant to this discussion is the Biomedical Advanced Research and Development Authority, which covers r&d, manufacturing ramp-ups, and purchase/construction of facilities to be owned by the grant recipients.
TWiV640 podcast has lengthy discussion with Mina.
https://www.microbe.tv/twiv/twiv-640/
“To put this into perspective, the number of testing kits needed is only a fraction of the number of soft drink cans consumed globally (about a trillion per year), as Romer (2020b) has also pointed out for the US.”
It’s a point to consider: a company like Coca-Cola would have more than a few pointers on massive global distribution. Say what you will about the company’s product or history, but Coke has been EVERYWHERE for a looonnnggg time.
The kind of quarantine policy you all are talking about would ot get the economy gping for long.
I would think of a quarantine as being a big death sentence for people that may have otherwise survived the disease.
And people getting tested then being sent off somewhere in THIS non-healthcare, but for-profit- care would be an a #1 hell for anyone not rich (and don’t think these won’t be class segragated facilities.)
It would only take a few times of this snatching of people before people locked themselves down as much as possible not to risk what would be a for sure death sentence.
Death Houses like in documentaries about the plague.
The effor would have to be a Public Health initiate.
Gasp!
A not for profit program? How Un-American.
I did read here yesterday that there is no US large scale testing because the test makers could not be ensured a 3 year profitable program.
We could try this, sure, but we’ve already tried doing nothing and we’re going to stick with that while hoping for different results
Another indicator, in my view, that economists should never be allowed to talk about anything of any real importance.
This is not primarily a production issue: no doubt enough testing kits could be produced, given sufficient investment. But if you’re going to use WW2 mobilisation as an example, it helps to know that the main constraint was not productive capacity as such, but raw materials and most of all labour, especially skilled labour. This was why the Germans (who lost the production war) wound up using prisoners of war and even concentration camp inmates as labour in war production. Here, the constraint is going to be skilled personnel able to administer the tests and interpret the results, as well as contact those with positive tests.
As an illustration, testing 5% of the population of a major European nation would indicate around 3M tests per day. Since you wouldn’t be testing the same 5% each day, you would need a series of travelling test facilities, moving around the country. I went for a test last week, and the appointments were at five minute intervals, which is probably the minimum administratively possible. Each technician (wearing full hazmat protection and googles in a sterile environment) could therefore handle a dozen subjects per hour. Because the environment must be sterile, and kept so, there’s a limit to how many testing points you can have at a time. Let’s say fifty. If you run the testing sixteen hours a day, in two eight hour shifts with breaks (wearing this gear is hot and exhausting) you would still manage no more than 10,000 tests per site. So you’d need 300 sites, every day, Now these figures are only an illustration, but they give some indication of the problems of just carrying out the tests, near mind interpreting them, contacting those who test positive etc. I really wonder whether any country actually has the resources to do testing at this scale.
Another economist “assume a tin-opener” argument?
Theoretically, at some point 100% will have been tested.
Then what?
There’s no cure. How can a vaccine work if those who have already had the virus, have no immunity?
I think the whole testing thing is an example of “We have to do SOMETHING”, Keep busy
rather than face the reality that there is nothing we can do.
I don’t get it.
Also, if I get tested & it’s negative, what if I catch C-19 on the way home? Should I get tested again tomorrow? Absurd.
There is a two week period when the infected shred the virus. If the infected person does not contact an uninfected person, there is no viral transmission. If every infected person can be detected and isolated, the pandemic is halted. Universal testing at home before going to work and school and isolating at home if test positive and informing your work/school group will end the pandemic. The problems are 1) making the hundreds of millions of tests and distributing them (the post office is being hobbled to assure the election of Republicans), 2) getting public buy in for the program, and 3) catching and securing the scofflaws in safe isolation centers. Only a functional government like South Korea can do this.
The whole of intent of the plutocratic 1980s counter revolt, the rise multinational monopoly corporations, and globalism is to destroy democracy. End taxes and regulation. Oligarchs succeeded. As long as neoliberals rule the West, the Pandemic will remain endemic, never going away. The service/travel industry, 80% of the US economy will never recover.
The last Great Depression ended in a World War.
Medcram is a good source for COVID information. The interview with Dr Michael Mina is great. https://www.youtube.com/watch?v=i536vS3z3e8
@ Vet:
Those are some big IFs. If immunity is not acquired from infection, what keeps the pandemic from cycling
endlessly until it mutates benignly or we’re all dead. 1 case starts the whole thing again. A needle in a field
of haystacks & you have to test the whole field each round. But we’re leaving the needles in place.
I don’t see anybody being rounded up so I’ll go back to my point: What is the point (of all this testing)?
I am jousting with alternate realities where there is democracy and the will to control the pandemic. Universal testing could do this. Antigen tests can detect new mutated strains. Instead the ruling class is using the pandemic to get richer. 300,000 Americans are projected to die this year. If no vaccine, a similar number of deaths each following year unless the virus mutates to less deadly strain or a treatment is found.
Another virus, HIV killed 1.5 million persons globally last year. There is no vaccine four decades after Dr. Anthony Fauci’s first failure. 13,000 died of AIDS in the USA last year where a cocktail antiviral treatment is available for the approximately one and half million Americans infected with the virus.
American life expectancy will continue its decline. The economy will never recover for the 80% who worked in the service and travel industries unless it is safe to go out in public.
IFs are speculative. we could develop theraputic cures, we could develop vaccines, and immunity could be partially effective reducing the severity to mild symptoms or making a portion of the population immune — all with good chances of happening. In the meantime the more testing which is done the more data we get, which is crucial to making policies, and to give us the time to find solutions. we don’t have final cures for colds, which may include those from corona viruses, but colds can usually be managed so they are not deadly or permanently debilitating.
If they were quarantining all the positives it might work. But they’re not. If they tried it nobody
would get tested. Catch-22
So to get to my point, which is What is the point? (of all the testing)
PLEASE don’t obfuscate it with long winded banter.
WHAT IS THE POINT?
Laissez Faire does not win wars. How come public health isn’t exposed to Sun Tzu?
Given the trillions spent, why not pay COVID positives living expenses plus during the quarantine period. I don’t think you get much complaints from people being asked to take a 2-3 week paid vacation; for those that are asymptomatic. Universal care for all others stricken.
Please see https://www.rapidtests.org/
“Why rapid tests?
Existing technology using paper strips allows for contagious-COVID testing that is rapid and inexpensive. Research shows that if done properly, these testing protocols could drive down infections close to zero.
Millions of these tests can easily be manufactured and distributed.
At as low as $1 per test, you can take a test every day. Tests could be administered at the entrance to schools and offices, and some could be taken at home.
Rapid tests for contagiousness are currently not approved for this type of use, since they do not meet overly strict sensitivity requirements.”
@ Pilgrim:
Where do the positive kids go? Positive school?
How do you run a business with workers turned away at the door?
Test customers too?
The whole thing is seeming cultish to me ala Jim Jones. Remember Rajneesh? LOL
Lots of ideas about what “everybody” should do.
The testing being done has nothing to do with clinical study of any cure or vaccine.
I’ll stick to my theory it is busywork to justify the existence of legions of busybodies.
Epidemiologists say they need follow up antibody tests of fully recovered “specimens” to determine the percentages of likely survivors with/without a vaccine, & to see if such antibodies even exist.
This is not being done.
The neg/pos test is “nice to know” but has no practical use.
As I said before, at some theoretical point 100% will have been tested. Then what?
With the tests all performed at different times & test types, with
a moving, evolving target, any conclusions will be “open to interpretation”.
So they test. Then count, add, subtract, multiply, divide, seasonally adjust, normalize, revise.
In ten years, if we’re alive, we’ll still be arguing about the “Covid numbers”, just like we still haggle about the 2008 crash. Where zero bankers went to jail. As time goes by the murkier it gets. Samol samol.
For wannabe investigators, (& bloggers), Average Joe will doze off long before you prove anything.
With the rapid testing you know if one is shedding the virus, during which time one should not be going around spreading it. That’s VERY practical knowledge. Cheap rapid, at home or needing no special equipment, tests, now under development, could be done daily, and one is positive then one can avoid contact with other people while looking for medical care if needed. Spit on the paper strip, and if you test positive it means you are shedding, and you stay home. This is not rocket science.
Good read. Thank you for sharing.