Yves here. It’s good to see Tom Neuburger discussing a possible misperception by some of what the “95% effective” Covid mRNA vaccine results touted by Pfizer and Moderna mean, when they are on the verge of receiving an FDA Emergency Use Authorization to allow their release.
While we have your attention, we’ll point out another misperception, which the press is amplifying, that having been vaccinated would prevent the recipient from transmitting Covid. For instance, some business owners are saying they will require employees to be vaccinated, not because they are concerned about worker safety, but because they intend to market their venue as safe for customers by virtue of having vaccinated staff.
At this point, the effect of any of the Covid vaccines on disease transmission is a known unknown. From Wired in late November:
The problem is, a Covid-19 vaccine that only prevents illness—which is to say, symptoms—might not prevent infection with the virus or transmission of it to other people. Worst case, a vaccinated person could still be an asymptomatic carrier. That could be bad.
The article further points out that so far, only the Oxford/AstraZeneca vaccine has evidence that it reduces transmission, as opposed to protecting recipients of the disease.
A more technical explanation from The Lancet, in September:
Multiple COVID-19 vaccines are currently in phase 3 trials with efficacy assessed as prevention of virologically confirmed disease. WHO recommends that successful vaccines should show disease risk reduction of at least 50%, with 95% CI that true vaccine efficacy exceeds 30%. However, the impact of these COVID-19 vaccines on infection and thus transmission is not being assessed. Even if vaccines were able to confer protection from disease, they might not reduce transmission similarly.
Challenge studies in vaccinated primates showed reductions in pathology, symptoms, and viral load in the lower respiratory tract, but failed to elicit sterilising immunity in the upper airways. Sterilising immunity in the upper airways has been claimed for one vaccine, but peer-reviewed publication of these data are awaited.
The sterlizing immunity claim came from Phase 1 trials of the Novavax vaccine.
By Thomas Neuburger. Originally published at Substack
Excessive haste could have fatal consequences, since public trust and wide vaccination are the only ways any vaccine, even the best ones, can work.
A note before I begin: This is not a recommendation not to be vaccinated against Coronavirus. It’s an encouragement to decide for yourself and your family when to be vaccinated and which vaccine to choose based on the most accurate information available. That said, let’s proceed.
“Done right, vaccines end pandemics. Done wrong, pandemics end vaccines.”
—Andy Slavitt here
People in the United States, along with people in all of the rest of the world, are eager for a vaccine that provides immunity to the Covid-19 virus. Drug manufacturers, with a market of tens of billions of injections to sell into, are eager to roll one off the production line. Both groups are highly incentivized to get a vaccine into distribution quickly.
Hundreds of Billions in Potential Revenue
Let’s look at the revenue side first. Here, for example, is what the three leading vaccine candidates are projected to cost in the UK according to a recent Sky News piece:
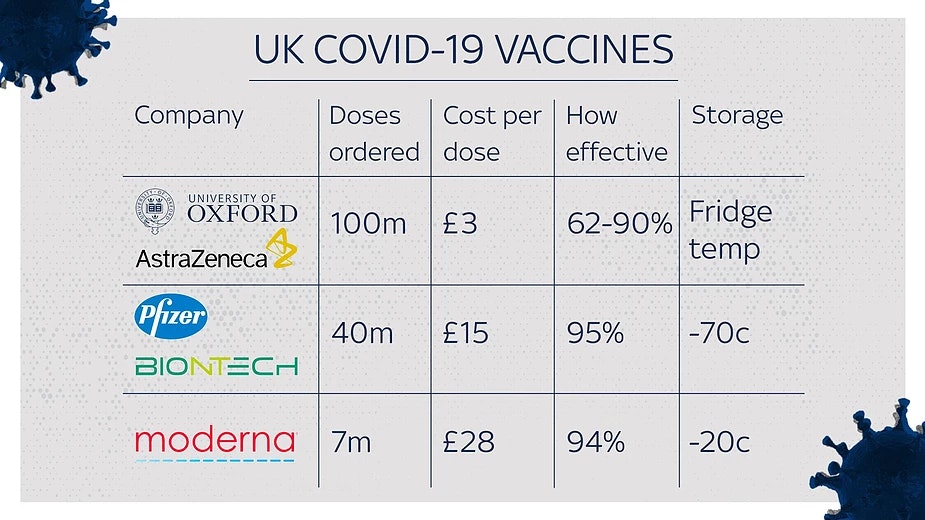
In two years the earth is projected to hold 8 billion people, and most leading vaccine candidates require at least two doses. Let’s be conservative: If Moderna, say, sold its Covid vaccine to 1 billion people at ₤28 (about $37) per dose, the revenue stream from those sales would turn into real money fast — $74 billion in revenue at retail prices in less than two years.And that’s for capturing less than a sixth of the global market. A vaccine manufacturer that captures a third of that market would swim in wealth till the climate crisis took us all.
For comparison, consider Moderna’s recent revenue profile. For the last few years, Moderna income has run between $60 and $200 million per year. Revenue for just the last quarter, however, jumped to $158 million. Moderna is clearly set for a windfall.
Needless to say, something like $100 billion or more in revenue would more than cover the cost of Covid vaccine development, so why the high price retail prices? One can only guess.
How Effective Is “Effective”?
About effectiveness, much is claimed. From the same Sky News article:
The UK has become the first country in the world to approve the Pfizer/BioNTech COVID-19 vaccine for use.
The government says the jab [vaccine], which has been given the green light by independent health regulator MHRA, will be rolled out across the UK from early next week.
Studies have shown the jab is 95% effective and works in all age groups. [emphasis added]
Moderna claims similar effectiveness — 94% — for its own vaccine candidate. But what does effectiveness mean?
To a lay person, a phrase like “95% effective” means one of two things: either that she or he, upon exposure to the virus, is protected 95% of the time, or that 95% of the people who take the vaccine are protected 100% of the time.
And this is where the mutual eagerness of the two highly motivated groups — the public; the profiteers — intersect. The public wants to hear “95% effectiveness” and think it knows what those words means. The drug companies want the same thing as the public; it wants the public to think it knows what those words mean.
But in the world of drug advertising, the word “effective” does not mean what you think it means. The other way to look at effectiveness is this: Based on the numbers released from phase 3 trials, the Pfizer vaccine is 95% effective, but 1% of the time. In the same way, the Moderna vaccine is 94% effective, but 2% of the time.
Relative Effectiveness
To sort this out, let’s look at real numbers, thanks to Twitter friend David Windt.
For the Moderna product, the phase 3 trial contained 30,000 individuals divided between those given the vaccine and those given a placebo. Let’s assume that individuals in each group were allowed to roam freely “in the wild” — that is, told to live their regular lives among the general population, including going out infrequently, staying masked, and practicing social distance — as opposed being proactively and aggressively exposed to the virus by the researchers, which would be highly immoral, to say the least.
In the Moderna vaccinated group, 11 people out of 15,000 got the virus (by Moderna’s definition of what “got the virus means”) for an overall infection rate of 0.07%. (There’s disagreement about whether the drug company’s “got the virus” measurements are well chosen; see the Forbes article “Covid-19 Vaccine Protocols Reveal That Trials Are Designed To Succeed.” But we’ll ignore that point for now.)
In the Moderna placebo group, 185 people of 15,000 got the virus, for an overall infection rate of 1.23%.
Do you see where this is headed? If you divide 0.07% by 1.23%, you get a 5.7% infection rate — or inversely, a 94% protection rate, which is what’s claimed. But that’s a percentage of a percentage, a ratio of a ratio, something called the “relative rate” in the medical profession. What this really means is that, of the 1.23% of people who would have gotten the virus in the vaccinated group, 94% of them didn’t.
But Moderna isn’t testing 30,000 people who are infected with the virus, or even 15,000 people. Only 185 people “got the virus” (by their definition) in the placebo group. That population was reduced to 11 people with vaccination. These are very small numbers.As stated above, the Moderna vaccine is 94% effective — but only 1.23% of the time.
(For another way to see that using a percentage of a percentage, or a ratio of a ratio, is confusing, consider an advertisement that claims a company’s new product is “twice as effective” as its old one. If the old product was effective only 2% of the time, and you knew this, would you buy the new one?)
Infection rates in those clinical trials seem low, by the way, which could be just an accident of statistics, or something off in their way of measuring who is counted as infected. From the start of the pandemic until now, the overall disease rate for Maricopa County, a high-infection zone, is 5034 per 100,000 people, or 5%. At the lower end, the overall disease rate for Multnomah County, a less-infected but still urban county, is 2363 per 100,000 people, or 2.4%.
Both rates are higher than the infection rates of the Moderna and Pfizer placebo groups. As stated, Moderna’s placebo group experienced a 1.23% infection rate, and Pfizer’s placebo group was infected just 0.75% of the time. Does this indicate a difference in how “infection” is determined, or just something else about these studies? Hard to tell at this point.
None of this is to imply dishonesty on the part of the drug companies. Measuring “effectiveness” using the relative rate of infection is common in that world. It’s just more meaningful when the overall infection rate of a pathogen is, say, 70% or higher, instead of 5% or less.
Absolute Effectiveness
For comparison, let’s look at the absolute numbers from the Moderna test. In the unprotected population, 1.23% of the people who could have been exposed to the virus, got it. In the vaccinated population exposed to the same conditions, a little less than 0.07% got the virus. Subtracting the two, the absolute gain in protection was 1.16% — that is, taking the vaccine bought you a little over 1% in absolute protection.
The numbers for the Pfizer vaccine are similar. According to Windt, “the infection rate was reduced slightly, from 0.75% to 0.04% – that’s “95% efficacy” [but] these results do NOT mean that 95% of those vaccinated are protected.” In absolute terms, taking the Pfizer vaccine reduced the risk of getting the virus by just 0.71%.
So far, the Moderna vaccine works 94% of the time, 1.23% of the time! https://t.co/uixesVMW2O pic.twitter.com/AteRlyfcwo
— David Windt (@DavidLWindt) December 6, 2020
Do you trust any of these drug manufacturers and their massively under-tested vaccines enough that you would take whatever risk is associated with their product to gain that amount of protection? I know good doctors who won’t, and others who will.
Testing and Public Trust
I want to point to two articles about testing and public trust. First from MIT in November, consider this caution about public trust:
Covid-19 vaccines shouldn’t get emergency-use authorization
Public trust in vaccines is already in decline. The FDA should proceed with caution.
…The pace of covid-19 vaccine research has been astonishing: there are more than 200 vaccine candidates in some stage of development, including several that are already in phase 3 clinical trials, mere months after covid-19 became a global public health emergency. In order for the FDA to approve a vaccine, however, not only do these clinical trials need to be completed—a process that typically involves following tens of thousands of participants for at least six months—but the agency also needs to inspect production facilities, review detailed manufacturing plans and data about the product’s stability, and pore over reams of trial data. This review can easily take a year or more.
Excessive haste could have fatal consequences, since public confidence and wide vaccination are the only ways any vaccine, even the best ones, can work: “Public health experts caution that vaccines don’t protect people; only vaccinations do. A vaccine that hasn’t gained enough public trust will therefore have a limited ability to control the pandemic even if it’s highly effective.” [emphasis mine]
This Forbes article from September, titled “Covid-19 Vaccine Protocols Reveal That Trials Are Designed To Succeed,” argues that the vaccine trials it examined measure efficacy by testing for the wrong things — the absence or presence of symptoms, especially mild ones:
One of the more immediate questions a trial needs to answer is whether a vaccine prevents infection. If someone takes this vaccine, are they far less likely to become infected with the virus? These trials all clearly focus on eliminating symptoms of Covid-19, and not infections themselves. Asymptomatic infection is listed as a secondary objective in these trials when they should be of critical importance.
It appears that all the pharmaceutical companies assume that the vaccine will never prevent infection. Their criteria for approval is the difference in symptoms between an infected control group and an infected vaccine group. They do not measure the difference between infection and noninfection as a primary motivation. [emphasis added]
Is this true of the latest trials? Last September is forever in Covid years. I’ll look at this side of the issue in a follow-up piece, but my early research says that the Forbes point is still valid. If this turns out to be the flaw Forbes thinks it is, public trust could be even more greatly eroded as these vaccines fail to deliver what’s we’re led to expect of them.
To Vaccinate or Not To Vaccinate?
As I said before, this is an not an encouragement reject the vaccines. It’s an encouragement to decide about them wisely by considering a number of factors — your need to feel “safe,” your need to end this constant quarantine, and society’s need to inoculate nearly everyone, versus your trust in the approval process, your personal level of caution, and the benefit of taking a relatively untested product to reduce your Covid risk by maybe 2% in absolute terms.
There are Covid hot-spots after all, areas of the country and the world where infections are soaring, and even low infection rates come at a heavy price. Covid has changed for the worse both the way we live and our economy. And people do die from it.
Maybe the first vaccines out of the gate, perhaps these three, will be everything a mother could want for her family and nation. But even if these products are are very very good, they have to be trusted to be effective.
If that trust is given blindly, and then betrayed, the consequences will be severe.


any studies or testing on fertility? what about breast feeding? what about long term symtpoms? [ hint ; the manufacturers have nothing] what does that tell you?
Pharma/FDA: “We can’t worry about that right now. We have a pandemic to fight. And investors to consider. And year-end bonuses are coming up. And a political class looking for a quick fix.”
Indeed we can’t worry about that now say Pharma, that’s why you absolutely must completely indemnify us from any financial repercussions too.
And since media depend on our ad dollars, we can control the PR repercussions.
The Wodarg/Yeadon petition to the EMA (which, contrary to some reports, does not say “it causes sterilisation”) is worth reading
https://2020news.de/en/dr-wodarg-and-dr-yeadon-request-a-stop-of-all-corona-vaccination-studies-and-call-for-co-signing-the-petition/
Yeadon appears to be being branded as a nut in the mainstream British media (and, indeed, Associated Press have published an article refuting the allegation that the vaccine causes sterility, by disproving assertions that Wodarg & Yeadon did not make.) In my book, that probably means he is not 180 degrees wrong…
Put “sterilization” in the press release and Karen is going deep undercover to sniff it out. She knows what’s up. She found documents on the website
It’s all for the children!…..
I don’t know the answer to this, but just yesterday the Oxford Zeneca vaccine reported a number of issues with allergic reactions. It raised the question on whether they deliberately excluded people with known allergies from their test subjects (this is not uncommon in early drug testing as a safety precaution). If even 1% have a serious allergic reaction, this would throw the benefit/risk balance out.
The potential harm of getting his roll out badly wrong could be catastrophic for public health policy for decades to come. I’ve a very bad feeling that there have been too many incentives built in to cut corners and fudge data. Who wants to be the mid level scientist in one of those companies with an awkward question to raise during a weekly meeting? We may well be throwing a dice and hoping for the best, rather than focusing on getting the right answer.
Is it O/Z, or the Pfizer one? NHS yesterday issued a guideline to stop vaccinating anyone with “history of allergic reactions”, which was for Pfizer vaccine.
If it’s just one vaccine, it could be an oversight. If both/all, it could be a real problem – as you say, a potential catastrophe for decades.
It was the Pfizer one, I don’t think AZ had been released for general use anywhere yet.
Sorry, yes, I meant to Pfizer one.
Is the sample skewed?
If I had severe or eve moderate allergies, I wouldn’t volunteer for a drug test, especially given the current state of US health scare.
With all due respect, the author and his Twitter friend seem very confused about how to interpret the efficacy numbers. The quantitative reasoning is fundamentally erroneous.
> The other way to look at effectiveness is this: Based on the numbers released from phase 3 trials, the Pfizer vaccine is 95% effective, but 1% of the time. In the same way, the Moderna vaccine is 94% effective, but 2% of the time.
That “1% of the time” and “2% of the time” reflects the approximate likelihood that a subject from among the test groups was exposed to a high enough dose of SARS2-CoV to cause symptoms and a positive PCR test over the course of the trial. It has absolutely zero to do with the efficacy or lack thereof of the vaccines. Let me repeat that. The overall proportion of infection among all trial participants has no bearing, in and of itself, on the actual efficacy.
Note that these percentages are smaller than the overall “rate” of infection (proper term would be “proportion”) in e.g. Maricopa Cty, AZ because the latter proportions are with regard to the entire pandemic whereas the proportions observed in the vaccine studies reflect the limited duration of the study. Also keep in mind that a fair amount of data collection likely happened over the summer before the cases started skyrocketing again.
With that said, the problem, such as it is, with the low percentage of people who got infected is that it reduces the effective sample size, relative to the number of people who actually enrolled in the study. However, the sample sizes are not so small as to be inadequate to demonstrate high efficacy for the purposes of these trials.
Now, there are plenty of caveats here if you really want to pick these thing apart. The author correctly notes that these studies demonstrate efficacy in terms of getting full-blown symptomatic COVID-19, not in terms of preventing transmission or avoiding the disease entirely.
Also, the results only apply to the *sampled population*, which are the people among the test subjects who became positive. Is that population *representative* of the whole population? Does it include children? The elderly? People of different social class and/or living situations? People of different “colors”? People with history of severe allergies? And are the proportions of each of these (and any others I *can’t* think of) similar within the sampled population as in the whole population?
Second, the result assumes that the study is blinded. Blinded means that subjects don’t know whether they have been given a real vaccine or a placebo. If subjects are not blinded, they may alter their own behavior accordingly. For example, a test subject who knows (s)he is vaccined might be more nonchalant about social interactions, which could increase their frequency of exposure to COVID vs. subjects who knew they got placebo.
While the studies themselves have surely taken precautions to avoid accidentally un-blinding the subjects (unless an adverse reaction occurs, which is handled separately in the data), the media has reported repeatedly and extensively, while these trails are on-going, that side-effects are common. This is very bad because this information gives test subjects knowledge they can use to judge whether they are actually vaccinated or not. Even if said subjects are wrong in their assessment, simply believing they have extra knowledge can change their behavior, and if this phenomenon is not identical between the placebo and experimental groups, it will throw off the results. An analogy in the legal world is how jurors are advised not to watch or listen to news reports about the trial they are serving in. Whether they choose to believe or disbelieve the reported information, it has the potential to harm their impartiality.
By the way, I’m not trying to defend these vaccines or their manufacturers for their own sake. The author is correct that these vaccines are “under-tested”, and I believe pushing them onto the market so quickly comes with substantial risks, both directly to public health and indirectly via potential severe damage to trust and credibility. I adhere to the maxim that Murphy was an optimist, and Murphy would say that there’s a lot that can go wrong in this scenario.
Thanks. I was concerned that the emphasis trying to undercut the 95% claim was overegged, but I had separately been bothered by how small the effective sample was. It appears the Pfizer sample was skewed by excluding people who were allergic and not having read their data release, it isn’t clear how up front they were about that (you’d think the NHS wouldn’t have gone about injecting their staff willy nilly and getting two severe bad reactions the first day if they had had a clue).
You’re welcome, but I’m not sure I explained as well as I could have.
The reports of serious allergic reactions from the Pfizer vaccine on its debut day surprised me. I imagined lots of things that could go wrong, but two bad reactions on the first day? Perhaps these incidents will be limited to people with “a history of serious allergic reactions”, but I also know that anaphylaxis is unpredictable and I know many people anecdotally who only had such a reaction later in life.
As such, this Pfizer vaccine and possibly the Moderna one too if it has the same problem, will require that patients be monitored for anaphylactic symptoms for some significant duration of time (an hour?) after the injection. Now consider this potential possibility in light of the other logistical difficulties surrounding the vaccine distribution and administration to huge numbers. It probably won’t be via drive-thru service.
As I understand it the 2 people in the UK who suffered the reaction were aware of their allergy issues and carried epi-pens, but the allergic effects just weren’t flagged in any of the resources accompanying the rolled-out vaccine or asked of them when they got the jab. Which rather speaks of a rushed and botched process to me.
Well, the anaphylaxis, regardless of state of health, indicates that there are antigens present in the formulation which are unrelated to the protein the vaccine will manufacture in cells. While it can even be a mucopolysaccharide rather than a protein, the fact remains that the carrier is not benign and we are not being provided with all the information.
In the Adenovirus carrier vaccines the virus shell is in itself immunogenic, which makes a booster problematic unless, as with Sputnik 5, different adenoviruses are used for the primary and booster.
I intend to be vaccinated, but I’m witholding judgement until more data is presented about the currently highlighted vaccines until I see data on either attenuated virus or adjuvated purified protein vaccines.
Coming from a time before polio vaccination, what I have not lost sight of is the fact that vaccination in general has been breathtakingly successful in improving and maintaining our health at low cost.
AZ say that Phase III of their trials was double blind with 40k subjects. The official title of the study is A Phase III Randomized, Double-blind, Placebo-controlled Multicenter Study in Adults to Determine the Safety, Efficacy, and Immunogenicity of AZD1222, a Non-replicating ChAdOx1 Vector Vaccine, for the Prevention of COVID-19 whose start date was August 2020, Primary completion date as March 2021, and Estimated study completion date as February 2023. A lttle more data can be found at https://clinicaltrials.gov/ct2/show/NCT04516746 (ClinicalTrials.gov of the NIH).
One could be forgiven for thinking that the trials are currently not finished. If so, does that mean the vaccine was rushed out with all the consequences resulting from that?
Yep, I am wondering of the consequences of rushing out the vaccines and I am convinced the pressure is 99% political. There are governments too eager to announce mass vaccination and putting too much confidence in early reports so worried they are with the socioeconomic impact of the pandemic. And this can show (will show) problematic if mass vaccination is started before a thorough examination of further trial results and problems like allergic reaction and others that might surge in the course of the trials.
It is absolutely unwise to throw ourselves into a rush based on early reports that account for very little exposure time and which are biased by the nature of the vaccine. One cannot even suppose that the placebo group and the vaccinated group behaved similarly given the high reactogenicity reported by the vaccines (particularly the RNA vaccines). This reports were obtained with data gathered about 12 weeks after the trial start. Imagine, given that two shoots were provided and each shoot produces quite a nasty reaction that can last nearly a week, nearly 20% of the time the subjects that were vaccinated were suffering symptoms related with the vaccination and this would alter their behaviour significantly compared with the placebo subjects.
Given the time course of antibody production after vaccination, with a peak shortly after the second shoot, the results are biased by the peak and the real protective rate will be different when specific immunoglobulin levels decline. One can consider this 95% efficacy as transient efficacy and we will almost certainly see that further data reveals a sharp reduction. Repeating 95%! 95! all the time will probably result in a sense of deception later that could be counterproductive.
I don’t think data is fudge, that would be really, really stupid, but it is being badly misinterpreted and can conduct to cutting corners to mass deployment with unintended consequences.
Yes, but as the post does explain, that 40K participants translates into a very small number that contracted the disease (and in the injection group, were assumed to have gotten it but beat it back). So the effective sample was way way smaller.
Exactly. The number of infections are so small that while one may estimate efficacy, the power of the estimate (beta error; calling something true when it is in fact, false) is high. The best I could really see statistically given the data is the ability to reject the null hypothesis in a F-test (no difference between the groups) with reasonable confidence (1 – alpha; the chance of rejecting something as false when it is in fact true).
As with any sample from a larger population, it is important to understand the uncertainty of the estimate, which at least Oxford/AZ is providing.
They published the CI, and if I recall correctly it was 95% of something like 92%-98.5% effective. The sample size was just big enough to calculate it, but just so. But what’s more important, in my opinion, is that the method they used to calculate the effectiveness of the vaccine are the same they use for every other vaccine. I.e.: they’re not doing exception for this one, which is important. We know it’s a Phase III study with the limitations of all Phase III studies.
Ah, thanks. I was puzzled by the argument, because it seemed a bit like saying that routinely carrying umbrellas did not provide 95% protection against rain because it only rained some of the time. More relevantly, though, consider vaccinations against tropical diseases. I’ve had many and need to check on them before I go to certain countries. They are generally considered highly effective – it’s assumed, 100% or nearly so in some cases. But if, say, 10000 vaccinated people visit a country in the course of a year, but only 500 come into contact with a contagious source (which would not be surprising) and none get ill, then the efficacy of the vaccine would presumably only be 0.05% according to the logic of the article. So what, as a layman, am I missing, (apart from the issue of sample size)?
> Ah, thanks. I was puzzled by the argument, because it seemed a bit like saying that routinely carrying umbrellas did not provide 95% protection against rain because it only rained some of the time.
Exactly, and thanks for your concise example.
isn’t this precisely why the burden of interpreting the efficacy claims shouldn’t be offloaded to the general public? If the numbers require a level of maths proficiency not many can lay claim to to interpret then therein lie opportunities for misrepresentation via numerical sleight of hand, which if history is anything to go by, will be exploited to hoodwink an unsuspecting public, especially with a pot of gold filled to the brim with billions of dollars lying in wait. Most laymen don’t have the maths chops to pick apart the claims and will most likely throw their hands in the air and walk away with “it’s 95% effective” as the takeaway, caveats of data interpretation be damned. The efficacy should be communicated to the public in as simple and absolute terms as possible, in a language that is a sharp departure from that usually employed in the fine print of legal documents to make things unintelligible while embedding opportunities for plausible deniability should things go belly up.
I think what was said here is important. We provide people very little education and most others end up specialists. Yet at the same time everyone knows everything and needs to know everything because everyone is trying to screw you over. And worse yet, most people do not know that they are stupid or can speak about a topic knowing they are probably wrong.
It’s all so damn stressful I will just take my chances without the vaccine and be as careful as I can not to infect others. I know a lot about human biology, but not enough about vaccines and the companies and the people who own them. I do not trust the government because it is controlled by corporations and not the people.
A nice visual would answer this question but I can’t find one with DuckDuckGo.
There are two separate groups of people (each 15,000 in the Moderna case), placebo and vaccine. We’ll measure the (small) subset of each group that gets infected and compare the numbers.
If 100 in the placebo group get infected and 100 in the vaccine group get infected, that vaccine was 0% effective. No apparent benefit from the vaccine, outcomes look identical.
If 100 in the placebo group and 50 in the vaccine group get infected, that vaccine was about 50% effective. Not great. Maybe the severity of disease was less in the vaccine group, but that’s a secondary goal and not what we’re measuring primarily.
100 in the placebo group and 5 in the vaccine group get infected. That’s called 95% effective.
The size of our trial dictates our level of confidence in these numbers. If our original groups of people were tiny and/or we have barely any infections in either group, we can’t say much anything with confidence because small numbers of infections in either group can swing the numbers in either direction.
I was an engineering major so I have no issues with interpreting the data, however it’s laid out. The same can’t be said for some members of the general public, hence my assertion that the claims on efficacy should leave very little room for “depends on how you look at it, absolute vs relative” interpretations that will serve only to confuse. Can the pharma companies stand behind the claim that it’s 95% effective without resorting to numerical semantics or lobbying for liability shields? If so then by all means tell the public that the vaccines are 95% effective. If they say “well we did say it’s 95% but what we meant was…” then we are in the territory of bait and switch.
There’s too much at stake to leave even little room for exaggerated claims from profiteers because the anti-vaxxers will have a field day exploiting any discrepancy between claimed and actual performance for these vaccines and guess what, with that will go public trust.
I can get behind what you’re saying, but how might you suggest this be communicated? It seems like a failure of the press if they can’t convey the essential fact that there were two groups of people and it looks like there were significantly fewer (but not zero) infections among the 15,000 that got the vaccine.
People (especially managers) usually want one single metric to compare even if it’s woefully inadequate. Quantifying reductions in infection or maybe severe disease seem like reasonable single-metric comparisons to me.
The 95% efficacy claim shouldn’t depend on the lens you wear to interpret the data, that’s my point. As Stephen the tech critic mentions, people are going to alter their behaviour based on these claims once vaccinated, so 95% should mean 95% in absolute terms and contra-indications should also be clearly communicated to at-risk populations. Auditable transparency should be the name of the game, if we’ve learnt anything from the 737max debacle it’s that companies, when left to their own devices, place profit ahead of human lives.
I guess “absolute effectiveness” as a metric like the author defines it is might be a reasonable for people assessing their individual risk or as a public health metric but it’s a moving target and totally specific to a certain population over a certain span of time, so it’s not especially useful for comparing vaccines. I don’t think explaining it sounds any easier than the other numbers.
Why should Vietnam show a terrible “absolute effectiveness” compared to France if the goal is to analyze the same vaccine? As the number of people exposed to the virus approaches the entirety of the population (if half were vaccinated and all members are susceptible to infection) the number would approach the vaccine efficacy as the companies define it.
Our back-and-forth is proving my point, you and I are somewhat equipped with the intellectual/statistical/mathematical wherewithal to do an analytical deep dive and look at the data from different angles, some (most?) people aren’t. It’s this knowledgeable that the general population lack the mathematical grasp to make sense of marketing claims, especially those presented as numbers, that companies exploit to mislead the public. That’s why I contend that the claims should be presented as simply as possible, stripped of opportunities for profiteers to obsfuscate anything. Freebird has a suggestion below, which I’m 100% on board with
Exactly. I would even ditch the ‘95% effective’ language. They need to say ‘if 10,000 people were exposed to the virus, ordinarily about n would get infected. With this vaccine, the number infected was n’. This is language people can grasp.
Exactly
Except that even the above language can still be interpreted through different “lenses”. Certainly with the relatively sample size, it should be clarified that there’s a pretty big “bubble” of uncertainty around the ‘n’, just considering the basic statistics.
But suppose that for the 75 years and older population the vaccine only works at 50% efficacy, so if I’m 81.5 years old and the TV tells me that the vaccine prevents “9500 out of 10000 infections”, I might take myself out of isolation when that may be otherwise ill-advised. Likewise, if I’m an allergy sufferer, I might want to know if said suffers have a 1 in 100 chance of a severe allergic reaction vs. say 1 in 10000 for the general populace. So how do we communicate all these nuances in a way that makes them understandable to the wider public? I don’t really see an easy way.
In a sense, this is what doctors and regulatory authorities are supposed to do for people, but much of that is broken right now. Western societies have utterly failed to contain the virus when it doing so would have been much easier, and they refuse to take the steps required to contain it now. They have forced themselves into a situation with no alternatives. They are grasping for a “Hollywood solution” in the form of a high-tech vaccine “developed in a single weekend”.
Where n/10000 is so small, if I wanted to be a Covid-denier I would point to that tiny number and argue that not getting vaccinated is already 100%-1.23% = 98.77% effective.
To get it right, I have to think about the period of the trial. In X week trial period, my chance of infection might be 1.23%.
At 4X weeks it approaches 5%.
16X weeks (caeteris paribus) we’re talking about serious risk.
But 16X might be a year, and we need test results sooner than that.
That’s similar to a (fallacious) argument people use all the time, which is that there’s a 99.whatever% chance of survival if you get Covid-19.
I hate that fallacy, the binary of 0.X% COVID death vs 99.Y% full recovery. It ignores Long COVID risk, potentially affecting 20% of symptomatic patients per a UK study. It ignores the pain, medical cost (especially in no-Medicare4All Murica), & lost-wages opportunity cost of a non-death hospitalized case.
It is shameful that Long COVID is barely discussed by public health experts, politicians, or CorpMedia.
I don’t think anyone can possibly put a number on this. It seems like the answer is likely to be 10,000 unless some people have some innate immunity for reasons we don’t understand. Exposure isn’t really binary, someone singing in a phone booth choir with a sick person is much more likely to get infected than if they were just passing by a sick person in the grocery store.
It’s a very different statement than what the post author tries to capture with “absolute accuracy” which scales from zero (no cases) to the vaccine efficacy for a whole population.
Surely the only way to achieve “absolute accuracy” would be to ensure that both groups are a) identical in age ranges from 0 – 100, sex and biology/medical history, b) subject 100% of both groups to identical exposure to the virus, and c) isolate both groups from each other and the general population for a fortnight to prevent additional exposure from outside. In the absence of the above there is too much scope for a) deliberate and nefarious manipulation, and b) uncontrollable input influencing the numbers. IMHO.
I was born three years before doctors began giving a new drug on the market declared safe in pregnancy to mothers for morning sickness. It was called Thalidomide.
I won’t be taking this one.
Exactly! We can never know what ‘n’ is unless we purposely expose a population to Covid and then measure how many of them come down with the disease – and to me, that would be a highly unethical test to employ. So that ‘n’ as described is meaningless at best.
All we can know is how many people given the placebo come down with the disease v. how many of the group that get the vaccine come down with the disease and go from there. We know that not all of the people in either group will be exposed since most of them probably are taking precaution they can to avoid the disease like most of us – which means that the numbers of people who do get Covid will be small – and that is where ‘statistically significant’ comes into play. If there is any criticism it would be there – did they test enough people and long enough to get statistically significant numbers?
If you want ‘absolute accuracy’, then you have to be willing to throw ethics out the window and purposely give people Covid. Then you can study the effects and get ‘real numbers’ if that is what is necessary to convince the critics.
But they don’t know how many were infected. This is a leap of logic in your example. They had a number of infections identified in each group and INFERRED an infection rate, as in assumed that the rate of contracting the disease was the same in the injected group as in the control.
There’s more cause for pause given that a top HIV expert pointed out that the bar for designating an infection is too low:
https://www.forbes.com/sites/williamhaseltine/2020/09/23/covid-19-vaccine-protocols-reveal-that-trials-are-designed-to-succeed/
Where is the leap in my logic? A lower threshold for diagnosing disease (risking more false or dubious positives) is bad for the pharma companies.
False positives in the vaccine group are disproportionally worse for efficacy when the manufacturers want to be able to claim an order of magnitude fewer infections for that group.
I’m glad it wasn’t only me, although I was thinking along the lines that parachutes are highly effective in only the 1–2% of the population that goes skydiving. (But, to analogize to COVID-19 somewhat, you’d end up in a plane about to be pushed out without expecting it or wanting to.) It struck me as a way not to interpret the statistics.
Actually, it would about 0% plus whatever smoothing coefficient you choose to apply for your prior (Jeffreys would give 0.5 / 500.5 = ~0.1%). The number of vaccinated people here is has an indirect impact, via Bayesian chaining – it will give you a confidence interval for the number of exposed people (via a binomial with the maximum at about 500/10000 = 5%), which is then propagated into the confidence interval of the number of infected ones.
What was the testing protocol for people who were asymptomatic? That is, we’re the 95% of people all tested, or just assumed free of disease?
Apparently I can’t form a sentence this early in the morning.
My concern is that the vaccine creates a class of people who are asymptomatic carriers that 1) continue to spread the disease and 2) may still have damage from the disease, because we have seen that asymptomatic carriers can still get lung and heart damage .
How would you know someone is an asymptomatic carrier unless you tested them?
Probably. No. Yes. Yes. Yes. Unlikely. Close. Also, no pregnant people. But the vaccine has not been approved for children nor pregnant people.
It was randomized and double-blinded.
The common side effect was redness, swelling, and pain in the injection area. Mild side effects in less than 10% (otherwise, it would have not been approved by the NHS). I don’t think that’s enough to “unblind” participants, at least in significant numbers.
Do we know if they’ve weakened the criteria in the approval process? Because I might be wrong/misinformed, but from what I’ve read, any other vaccine at any other time would get a Phase IV approval with the data provided.
I do agree with the part that we shouldn’t lift all the restrictions just because we have the vaccine. Only when and if infection rates drop down to anecdotal, we can slowly and carefully begin to get back to normal (whatever that may be).
You are understating the side effects. Many people feel like crap for a day:
https://www.cnbc.com/2020/10/01/coronavirus-vaccine-trial-participants-exhaustion-fever-headaches.html
Is feeling crap for a day a mild symptom ¿ i dont know either way in terms or what is considered mild, but it doesn’t sound too severe.
The article appears to over egg the efficacy concerns. Did they want people 30, 000 to be deliberately infected to test the exact number. I think a large number of human challenge trials are ongoing. I think its reasonable to except the efficacy to be over 80% but the exact number is to be determined with further studies.
If you can’t take a day off from work, and many can’t, it’s not trivial. And Pfizer appears to have underplayed the fever issue. Some experts took note of the fact that everyone who took the Pfizer vaccine in the trials was encouraged to take acetaminophen afterwards. That’s not normal. IM Doc wrote this in today’s Links:
And if you read the comments above from those who are statistically well versed, the issue is that the effective sample is so small that there is a high degree of statistical uncertainty around the efficacy numbers. And that’s before getting to the fact that messenger RNA technology (the one used in the Pfizer and Moderna vaccines) have never before been used (except in a Zika trial of ~100, too small to be reliable) and the long term effects are unknown.
There are plenty of MDs who never prescribe a new med that has been out less than a year to patients. I won’t take the Pfizer or Moderna vaccine. I’ll wait for a conventional vaccine (there are plenty in trials, so several are likely to win approval).
It was not my intention at all. What “mild” means is pre-defined, and one day of flu-like symptoms is considered mild. Likewise, the cut-off to go to Phase IV from Phase III is predefined, and that means <10% of mild symptoms. I'm not trying to minimize the severity of the side effects, I'm trying to put in context that "many". "Many" means <10% or it wouldn't be approved (or so is my understanding), and this is, as far as I understand, the norm.
You’ve just made clear you are out over your skis. The Pfizer data contradicts your assertions. This is from IM Doc who unlike you has read the Pfizer data:
But as I understand it, the point is precisely that the sample is unrepresentative. What the trials did is ethical equivalent of randomly choosing 185 people, vaccinating them, then infecting then with the virus and then observing that only 11 got sick.
Just 185 seems really low.
I really appreciate the explanation. There is another element that has bothered me from the beginning of the phase 2/3 trial: that any and all symptoms are self reported. I’m in the Pfizer trial and received the doses in August and I asked repeatadly what level of pain/discomfort/deviation from the norm would warrant reporting and was told ANY change. But I am curious how many asked that and actually did it. Meaning, my guess is that the level of infections in the placebo group is actually higher when combined with the truly asymptomatic. But the same may be true in the vaccine group as well. They are trying to root out the asymptomatic spread with challenge trials, if they get approved.
You are right about his weird choice of language but his point is accurate
in ANY medical intervention one wants to know BOTH Relative efficacy and Absolute.
this vaccine reduced the RELATIVE rate of infections dramatically.. But since the overall incidence of infections was low, the ABSOLUTe reduction was very small.
this is also true of say STATINs in low risk patients.
The Vaccine Drumbeat in my jurisdiction is increasing and I’m sure will become deafening. Talk show radio hosts actually giving medical advice. No recommendations to consult with a doctor regarding your personal health circumstances and risks or those of your loved ones.
This is all orchestrated by Public Health officials who apparently have never heard of personal health care. We are all just one big Herd. To me this is a desecration of the doctor patient relationship by so-called health professionals. All of which is extremely dangerous and bad medical advice.
They’re trying to prevent people who *cannot* take the vaccine for whatever reason from dying, by encouraging people who are merely worried but have no actual reason not to take the vaccine other than paranoia and ungrounded conspiracy-mongering to take the bloody thing. This seems like, y’know, their job, and entirely praiseworthy.
The disease *does* see us as one big herd, or rather as a pile of individual infectable cells. It seems right to deal with the response to it on the same level.
Re: companies mandating staff to be vaccinated to market their establishments as “safe”. The tone and substance of the post is clearly meant to be a “proceed with caution” advisory on taking the vaccine, despite the author being at pains to emphasize that it’s not an “encouragement to reject vaccines”. Some quarters of the labour market are clearly going to render this moot for the serfs who’ll be required to either sign up to be guinea pigs or lose their jobs, wow. Swallow the tail risk of unknown medium to long-term health effects of these rapidly developed vaccines for the short term gain of a (most likely crap) salary? So agency over one’s health is now signed over to employers as a means to eke out a meagre existence, double wow.
Don’t forget they are using flawed PCR tests and except for Moderna in the US all other countries and companies where studies have been conducted are using another vaccine instead of a true saline or inert placebo.
Not to mention most of these Pharmaceutical Companies have been sued for tens of billions of dollars for harmful drugs , buried information, fraud ect. We’re supposed to trust them with safety studies for medical products they have indemnity for. Thank you for pointing out how deceptive these numbers can be for the average person.
Can you elaborate on why PCR testing is flawed? What better alternative is there for determining an infection with high specificity?
My understanding (and my understanding of all this is not perfect!) is that PCR tests are flawed (a) because they iterate an amplification process until they find something, and that something could be the remnants of another CV caused by a cold you had 3 months previously and (b) at least in the UK, the testing labs are not necessarily as well-versed in the hygene procedures you need to avoid cross-contamination. So there is a high risk of false positives.
Moreover, if I am reading the background to the clinical trials correctly, they count as “success” situations where someone who has one positive PCR test plus some fairly common cold symptoms does not then go on to develop full-blown CV19 symptoms. The problem is, given the PCR is acknowledged to generate a lot of false positives, then the success rate will be overstated, because the denominator in the success rate calculations will be swollen with subjects who didn’t actually have the CV19 virus to start with…
(I can’t quite believe that the test can be that dumb, so perhaps I am totally wrong about that? But I fear I am not.)
The Cycle Threshold of a sample (for PCR tests that provide it) gives some indication of the quantity of virus in the sample. I think that for only viral fragments a very high CT value (low amount of virus) will be an indicator that repeat testing may be necessary. I haven’t read the actual protocols to learn how they handle this.
I don’t follow your thinking here, if false positives are equally distributed across the placebo and vaccine groups then it will make the vaccine look less effective.
Let’s say 100 people really get infected in the placebo group and 10 in the vaccine group (90% efficacy). If you add an equal number of false positives to both groups, it can only push efficacy number down. If we add 10 to each group, efficacy is down to ~80%. If we add 20 to each group, efficacy is down to 75%.
Treating symptoms and not the underlying disease appears very profitable to me. How can that possibly create herd immunity?
Does that mean herd immunity is achieved when a significant number are asymptomatic, infected and capable of infecting the uninoculated?
I am assuming that infected asymptomatic individuals are capable of infecting others.
A question that this raises for me is whether sterilising immunity is conferred by the innate immune response to infection with live virus.
If not, then “herd immunity” would not be achieved by letting the virus “run” through the population, as has been advocated by some. The commentary I have seen on this generally assumes that people who have recovered from infection are not only protected from disease symptoms, but cannot for some length of time become reinfected and asymptomatic spreaders. Perhaps they can.
This is a very bad prospect for vulnerable populations.
If a vaccinated individual can still transmit COVID, then herd immunity may not be practical.
“Herd immunity is a form of indirect protection from infectious disease…..Immune individuals are unlikely to contribute to disease transmission, disrupting chains of infection, which stops or slows the spread of disease. The greater the proportion of immune individuals in a community, the smaller the probability that non-immune individuals will come into contact with an infectious individual.”
There is a comic meme going around at the moment:
1st mouse says: Are you going to get vaccinated?
2nd mouse replies: Are you mad? They haven’t completed the human trials!
I’m still having a hard time wrapping my head around this. What do the ‘numbers’ look like for a proven vaccine that’s been around for several decades or more (e.g. smallpox, polio, etc)?
Are these vaccines truly “95% effective”: illness prevented and infection eliminated in 95% of everyone vaccinated. Period?
Am I thinking about this the right way?
Thank you.
Let’s just make this simple.
Not everyone is going to be exposed to Covid-19 just like not everyone is going to be exposed to the flu. So why do you take the flu vaccine? Isn’t it because if you are unlucky and DO get exposed, you have some protection from getting sick?
Not everyone was going to be exposed to small pox or polio, but for those that were unlucky enough to get exposed, those vaccines protected MOST of them from getting the diseases, I’m not sure what the ‘effectiveness’ of those vaccines were, but you don’t hear of small pox or polio pandemics any more. Isn’t that what a vaccine is supposed to do?
The reason for getting a Covid-19 vaccine is just the same. You may never be exposed to Covid-19 so the vaccine will have nothing to protect you from – so, according to this article, it’s effectiveness for you will be zero. Remember only 185 of 15,000 people who were taking the placebo got exposed. So, if you are unlucky and do get exposed, wouldn’t you like to have some protection from what Covid-19 can do? And what the numbers are saying is that IF you do get exposed to Covid-19 that you have a 95% chance of being protected and NOT getting that disease. To me that sounds a whole lot better than nothing!
I call articles like the above “fun with math”. They send you down the wrong path when it comes to what you can rationally expect from vaccines and they provide fodder for the anti-vaxxers.
That said, I wish we had more time to see what the possible side effects are, but sadly Covid is killing people at a too rapid pace for us to wait for the perfect vaccine.
Exactly. I’d like to write a long form rebuttal to this article, but I have to go to work in 30 minutes.
“It sucks, and is bordering on intentionally misleading” is my short form response.
My thinking is like I’m being given a choice between two syringes: one has an unknown dose of Covid-19. The other is the vaccine.
I’ll be getting the vaccine as soon as I can.
“…bordering on intentionally misleading”
I thought so, too.
I have a growing problem with the claims without any proof of efficacy. One of the vaccine makers bragged about creating the vaccine “one weekend” Vaccines take years to develop. That these are miraculously appearing within months by companies with a financial interest in being first. In a word, bushwa.
So far many claims have been made that have passed no test to justify. Only immunity from prosecution and personal responsibility are important to the vaccine makers at this point. The populous waits on bated breath for every word they spew.
Dr. Chris Martenson has a few things to say about it from his perspective as an expert in pathology. We, the people, desparately need rational voices that know statistics to begin with. Numbers are always mistaken for facts when presented by those alleged to be in authority. It doesn’t mean they understand them, or are working hard to be certain that the statistics are accurate, not just supportive of their claims.
I would make this silly prediction based on what I know now;
Prophylaxis with Ivermectin and vitamin supplements has already shown much higher efficacy in preventing infection, transmission, length of symptoms and outcome. But it doesn’t make huge profits. There are no horrible side effects.
When was the last time we were asked to accept a drug that was supported by the pharma companies? Statins? The benefits only seem to appear if one is hospitalized in critical care. The side effects may have injured more than the drug helped. But this sacred cow too is making companies lots of money.
Stop the viral functions vs. alter the body chemistry. When did our science think this was acceptable to alter our functioning immune systems and then say it was AOK? Was it just the lucre? We can’t imagine that our science has become snake oil from where it began.
I am not an expert or have medical training. I do read a lot. Re “Vaccines take years to develop”, you are correct. From my reading, the basic science for mRNA started in 1983. What happened afterwards has irony. The principle scientist/investigator repeatedly had difficulty in getting grant money to do her study because granting agencies did not think that the mRNA would be accepted by the human body. It was thought that the auto immune system would automatically reject it. The principle scientist/investigator failed to get tenure at her university because she was not able to bring much grant money to the university. Nonetheless, she persevered and finally together with a collaborator, they found a way of introducing mRNA without alerting the immune system. Their work was published in 2005. Their work was largely unnoticed except for two people who saw the medical opportunity provided by mRNA. Further study was done and eventually medical science and entrepreneurship merged together which led to the formation of BioNtech (based on the words, “biopharmaceuticals”, “New”, “Technologies”) and Moderna (based on the words “Modified”, “RNA”). Neither BioNtech nor Moderna had a vaccine a year ago. Instead, they had the technology. When the genetic code for the virus was released to the world by Chinese scientists, BioNtech and Moderna could then program their mRNA technology for the Sars-Cov-2 virus. With their technology, it could be said that they already had a head start in making the vaccine. The principle scientist and her collaborator work separately. One is now employed with Moderna and the other is with BioNtech.
None of the “Western” developers would of course now give any credit to their Chinese helpers!!! We only hear of “China steals our intellectual property.”
Remember the days when Jonas Salk refused to patent and make money from his polio vaccine?
They had a head start in making this vaccine *and possibly all future ones too*. This is a game-changer: it’s quite possible that future diseases may routinely have a vaccine entering clinical trials *days* after its genome is known, rather than having to work on it for months to decades first.
(Now all we have to do is convince people that it’s not a dark plot and that actually these things do save lives.)
I too am getting dizzy with all these statistics and caveats. I have had a flu jab every year for the last 12. I have had bugs of one kind or another over the years but I only had some kind of flu once — this February as it happens. There is no way that anybody can estimate how many flu bugs I was exposed to and what their impact would be on a healthy man in his 60s in the last decade. Anyway, I don’t worry about the statistics but make a simple risk assessment. Is the risk of a flu vaccine less than the risk of getting flu? The answer has to be yes.
With covid19 vaccinations I don’t much care whether it’s efficacy can be measured as 95% or 70% or 60%. Anything is better than nothing. Anyway, it’s like wearing masks. Its efficacy depends upon large numbers of people being vaccinated. I help protect you as well as myself and you protect me as well as yourself. I worry that large numbers of people will decide not to have any vaccine, ensuring that covid19 will continue to kill unprotected people.
Only one thing concerns me at present. Safety. Sadly, enough doubts have been raised about the two new experimental vaccines to make me think the risk is not worth it. I will wait for the Oxford vaccine to become available I think — while trying to keep a sensible open-minded watching brief.
There is no reason that you should go right out and get poked with these barely-tested, and IMHO experimental vaccines.
Salk and Sabin were hailed as heroes – which they were – for giving humanity polio vaccines. What has gone down the memory hole though, is how Pharma family blogged up the production of the vaccines. You should really check these links to see how bad this was/is.
https://en.wikipedia.org/wiki/Cutter_Laboratories (children vaccinated with live polio virus that survived the production process)
https://en.wikipedia.org/wiki/SV40 (90% of US children and 60% of adults inoculated with polio vaccine contaminated with a monkey virus that turns out be carcinogenic – it’s also passed down in-utero, so we all have increased likelihood of certain cancers, thanks pharma)
Public health is standing between greedy sociopaths and a big pile of cash, and it’ll probably get run over. I fail to see why we should expect a sound vaccine in this environment.
I haven’t seen my parents in a year. My parents haven’t seen anyone in a year. There’s a bloody good reason to go out and get vaccinated for us!
There’s a reason for everyone else too: some old and vulnerable people won’t be able to get vaccinated, which means they’ll be stuck in isolation until enough people have been vaccinated that they don’t need to worry about dying of this thing every time they go out in public or meet anyone ever.
Whether or not the vaccine is capable of interrupting transmission absolutely should have been front and centre in these studies especially when it’s presented to people with an extremely low chance of being harmed by the virus (ie. the fit & young who might be the ones likely to be affected by any fertility issues).
It could be assumed that less severe symptoms means less chance for spread which may be the case, but then I can’t see how logically that fits with the mainstream view that of the virus as something that is transmitted asymptomatically so readily anyway? (Although I think this asymptomatic spread idea is probably wildly overblown).
Asymptomatic and presymptomatic are not the same. Studies show that most of the asymptomatic people who transmit the disease end up developing symptoms (I’ve seen systematic reviews that show anything between 83% to 94%). I.e.: asymptomatic transmission is possible, but mostly by presymptomatic people.
The early bird gets the worm, but the second mouse gets the cheese!
As a practical matter, I expect that these vaccines will reduce the incidence and severity of both disease and transmission in the treated populations, and do so with little risk to the treated indivduals, so that there is very likely to be a net benefit to a treated individual, to the population of treated individuals, and [to a lesser exent] to the non-treated individuals in the general population.
I am confident that more information will emerge to support and refine the above hypotheses. It will only be a matter of degree. Speaking as a 69 year-old physician, I would take any of the three leading vaccines at the first opportunity. I expect that when we look back in a few years we will see that the immunized population did better than the age-sex-etc matched non-immunized population. To some extent, my wife and I are relying on unbalanced articles like this to at least temporarily deter some people from having the vaccine, so that we can get to the front of the line more quickly.
Out of curiosity, what informs your confidence in these vaccines apart from the press releases and efficacy claims from the pharma companies developing them? Is it something we the general public aren’t privy to that physicians have given the heads up on? I’m in now way being flippant, it’s just that a good number of doctors I know personally wouldn’t go near any of these vaccines, at least not until there’s enough data backing up their efficacy in the real world.
That’s a pretty contradictory position. You don’t get real world data unless real world people take the vaccine. Very telling of those -probably wealthy- doctors to let others assume that risk. Let’s not forget that tens of thousands of people already took the vaccine with significantly fewer assurances. I guess it’s alright to go to poor and desperate people first? That’s what I call solidarity and prosocial behavior.
No, the doctors aren’t convinced by the studies and the claims emerging from that, at least not yet. If signing up to be a guinea pig for something you’re not entirely convinced of is your idea of solidarity and pro-social behaviour then by all means, go right ahead, they’re not stopping you. By the way, more data can be the result of more extensive clinical trials with better designed studies that aren’t “designed to succeed”, and is not limited to being obtained from poor people being lined up to volunteer as guinea pigs, as you imply.
In any event all of this “being at the head of the queue” talk is academic for us in Africa, the big wealthy nations have resolved to hoard the supplies of whatever credible vaccine becomes available. Maybe you could lobby them to share in the name of solidarity.
If you put it like that, and people interpret it like that, no clinical trials ever would happen, except in Nazi Germany, where they forced people to submit to medical experiments (see, we can all be overly dramatic). If the vaccine is not good enough for you, it shouldn’t be good enough for anybody, and we never get a vaccine for anything, ever.
Therefore, yes, I will gladly accept the vaccine once it’s my turn, because at this point is civic duty and safety is as guaranteed as any other Phase IV drug. Again, the two alternatives are being a hypocrite or not having a vaccine.
Even better, I advocate to allow the vaccine to be produced in developing countries freely, without IP concerns. I doubt the wealthy countries will accept the proposal, but I also hope those countries will ignore international law and manufacture it for local consumption anyway.
I don’t know if it’s selfishness on the doctors’ part, or just so much familiarity with the avarice of the pharmaceutical industry that they don’t trust the data that has been molded into a neat report, likely as not full of hidden flaws or deliberately misleading conclusions. Unfortunately the truth will not come out til a lot of people have taken the vaccines, and I can’t blame a front line worker for not wanting to be at the front of the line.
I don’t doubt the avarice of Big Pharma. I count on it. But the people who actually developed the vaccine and actually run the experiments won’t see a penny of the billions Pfizer is going to make with this vaccine. At that point, I would expect at least a couple of trustworthy sources, with a conscience and without billions to blind it, would blow the whistle on any data manipulation. Like all conspiracies, the more people are involved, the shorter they live. Thousands have participated in the Phase III. So far, all the complains come from people who don’t trust Pfizer because Pfizer is not trustworthy, and people who are concerned for political reasons. And don’t get me wrong, you can’t trust Pfizer and there are clear political concerns, but as long as it’s just that, keeping an eye open and taking the vaccine is the right thing to do. Again, because otherwise we probably won’t get a vaccine in decades, if ever.
Don’t be in such a rush to get to the head of the que-
https://www.youtube.com/watch?v=arwZcw0Ejcc
I 2nd Thuto here.
I have a good friend who is a practicing MD dealing with Covid patients who I talk to regularly about the vaccines and the epidemic. He has a low opinion of how the trials have been conducted and thinks that there is a high chance of several surprising issues popping up (like the adverse reactions mentioned above). He, contrary to you, intends to let the early vaccine recipient’s finish the more comprehensive testing which should have occurred as part of the stage 3 trials.
Dr. Smith
You are no doubt aware that mRNA “vaccines” are not really vaccines at all in the conventional sense, but rather might more accurately be termed “genetic immune response modifiers.’ This approach to disease control has been speculated about for some time and subject to investigation, but has never been administered at scale in a human population. “Testing” to observe whether recipients immediately fall ill after the first or second shot is essentially meaningless except to the extent that it may retard or stop entirely the use of the drug. There are enough theoretical pitfalls with this radical methodology that no one can predict their long term impact. Perhaps after three years, but certainly not after 90 days.
Conventional vaccines like those for Polio and Smallpox utilize modified or disabled forms of the disease pathogens to stimulate antibodies to provide resistance when they encounter the disease “in the wild.” We have decades of experience and millions of cases using this type of vaccine which lends a high level of confidence that a new conventional vaccine can be used safely on a new pathogen.
MD’s like yourself have years of experience and training in identifying and treating disease — certainly far beyond that of the the average layman. But you are also the product of a culture that determines how you think about your practice. For example, “Only medicines that have gone through the approval and patent process are suitable for human use.” Or, “All medicines obtained from foreign countries are suspect or dangerous.” Or: “Authorities like the AMA, NIH or WHO are the only reliable sources of information” Or: “Deviating from approved practice can/will result in lawsuits and being barred from practicing medicine.”
By all means dash to the head of the Pfizer/Moderna Corvid vaccine line. We need more willing volunteers like yourself so authorities like Bill Gates won’t have to test new vaccines on poor children in Africa and India to determine whether the side effects include sterility or the re-emergence of Polio.
This.
Considering the questions that people have been asking on this website on how the mRNA vaccine works, I doubt that most people understand that this is not like the other vaccines that people have taken, and uses a completely different mechanism for eliciting an immune response than traditional vaccines.
It uses exactly the same mechanism: presentation of an antigen on cell surfaces. It even uses the same antigen as some of the more conventional SARS-CoV-2 vaccines. The antigen is even produced in the same place: the inside of the recipients’ cells. The only unusual thing is where the RNA comes from that is used to do this: is it on its own, or does it come packaged with other viral RNA implementing a complete working virus not common in human populations which has been modified to produce this antigen?
(I don’t know why anyone would consider it safer to take a traditional vaccine which has an actual working virus in it, even if said virus only causes a mild cold, than it would be to take these new ones which have no viral replication machinery whatsoever. The Moderna/biontech stuff is new, but not because it was previously believed unsafe, merely because eukaryotes are vicious to naked RNA outside their cells and destroy it on sight with some of the most efficient enzymes known because, well, it’s a sign of viral infection. So RNA-based vaccines never got close to getting inside enough cells to be useful, so you needed a whole viral capsid to do the job, like the more traditional Astra-Zeneca vaccine. That’s the problem that’s been solved.)
There will be some who make the specious argument that only ~2% of the subjects in the study got symptomatic Covid, so “big deal”. That sort of argument would carry more weight if it had been expressed in terms of “cases per unit time”. In this case, it looks as though the median time was about 2 months.
I expect that as time goes on we would find that a very large proportion of the control group [maybe 10%] would develop clinical symptoms, and a much larger proportion would develop asymptomatic disease [which carries a poorly defined risk of serious but silent damage to the heart, brain, etc].
As good studies emerge, like BioNTech, we can read the original peer reviewed literature and the commentaries on it, and draw our own conclusions:
SARS-CoV-2 Vaccination — An Ounce (Actually, Much Less) of Prevention
https://www.nejm.org/doi/full/10.1056/NEJMe2034717?query=RP
Safety and Efficacy of the BNT162b2 mRNA Covid-19 Vaccine
https://www.nejm.org/doi/full/10.1056/NEJMoa2034577?query=RP
To some extent, my wife and I are relying on unbalanced articles like this to at least temporarily deter some people from having the vaccine, so that we can get to the front of the line more quickly.
Fine by me. The more human guinea-pigs that stand between me and this stuff – and remain standing – the more likely I’ll be to take it. Eventually. Tho’ if your confidence is justified and you help take Runder1 perhaps I won’t even have to risk it.
While there are some clear misunderstandings about these numbers from both sides, several pointed out that we have zero knowledge about other aspects of the vaccine, such as:
1) Can people still transmit the virus after “successful” immunization from the vaccine?
2) How long will the immunity from vaccination last?
3) How long before a vaccine-resistant mutation emerges?
We should be focused on better testing (both developing and administering), pervasive contact tracing, and innovative technologies such as air filtering with vertical flow, better masks, better public support for masks, better strategies for isolating sick individuals in crowded situations, better treatments. What terrifies me about the vaccine craze is that it is distracting everyone from doing the right things not just to stem the death toll from this pandemic, but also from using this as a learning experience to be better prepared for the next one.
There is the expression “closing the barn doors after the cows have gone.” A more complete analogy in this case would be “a fire started in the barn, luckily the cows were able to run out the open door. We went into the barn and closed the door from the inside without a fire extinguisher.”
The COVID coverage by Michael Haseltine on Forbes is well worth reading. His Sep. 23 piece titled Covid-19 Vaccine Protocols Reveal That Trials Are Designed To Succeed is especially relevant.
William A. Haseltine, who was a pioneer during the early HIV/AIDS epidemic.
This part is damning:
https://www.forbes.com/sites/williamhaseltine/2020/09/23/covid-19-vaccine-protocols-reveal-that-trials-are-designed-to-succeed/
Why is that damning? The lower their threshold for a positive, the more likely they are to have false positives. False positives in the vaccine group make the efficacy values plunge.
It is totally counterproductive if the intention is to game the results. Then the smart play would be to only count serious disease.
By tomorrow, according to Worldmeters, 5% of the population in the US will have tested positive for c-19-studies have put the actual penetration of those infected at anywhere from 2X to 10X the counted numbers (16 million, or so). Are persons that have been tested positive, or carry antibodies, exempt from any mass vaccination program? It seems to me the enormous rush to get vaccines to market is the fear that, lockdowns notwithstanding, we are heading towards that time when a majority of the US population will have already become infected. I can envision the panic in big phamas boardrooms as the see that every week another million potential customers are removed from their expected profit sheets.
It’s worse than that. Not long ago some were saying how the number of American dead in this pandemic was approaching the number killed in Vietnam. Now the daily total exceeds that lost on 9/11 and is accelerating.
Not to worry. Simply denying the ability to fly, work, drive a car, or go to the supermarket to everyone without a digital vaccine certification card will ensure a high level of compliance with the Universal Mandate and continued joy in the boardrooms of Pfizer. The goal is to monetize Pharma Power, not to control Corid19. So bringing all those who have self-vaccinated by contacting a mild case of the disease or have a strong T-cell immunity response into the Fold is just good business.
Speaking of business opportunities, printing black market certification cards @ $100 each promises to put BitCoin to shame.
About that 5% of the US population that have tested positive:
At the conventional PCR Cr of 40 about 5% will have a viral loading such that they are actively spreading infection to others. The other 95% could be more accurately termed as false positives.
I assume it’s probably some degree of both. I mean just cause something might be true doesn’t mean it is true.
I also question these numbers and/or reasoning. Do you have a link supporting this statement?
I too have a problem with the way my source arrived at their 97% false positive claim. The internal logic is indeed correct, but it feels like using statistics in a less than transparent manner.
https://www.rt.com/op-ed/507937-covid-pcr-test-fail/
https://www.zerohedge.com/medical/covid-19-rt-pcr-test-how-mislead-all-humanity-accepting-societal-lock-downs
I had read that a cycle rep of about 25 was more commonly used. 40 would pick up a lot false positives.
Regarding monetizing Pharma Power: The Norwegian institute CEPI – Coalition for Epidemic Preparedness Innovations was founded in 2017 with the goal (amongst others) of being in the forefront in the development of vaccines for new infectious diseases and their distribution at an affordable price (or no price if countries can’t afford it) throughout the world. Funding for CEPI has come from the governments, trusts and foundations. Read all about it here.
https://cepi.net
What happened with CEPI and the development of Covid vaccines? The pharma companies would not give up their right to determine prices, for “competitive business reasons”.
Goggle Translate of an NRK article: https://www.nrk.no/dokumentar/ble-makteslost-vitne-til-dod-_-selv-om-vaksinen-fantes-1.15060685
——-
The pharmaceutical industry, on the other hand, did not like the rules, according to Richard Hatchett. He has been the director of CEPI since April 2017, when he left his job as deputy commander of BARDA. It is the agency of the US Department of Health that buys and develops vaccines.
In a sensational article, Hatchett explains what happened to CEPI’s policy:
CEPI’s rules are based on the idealism on which the coalition was founded. However, several multinational vaccine companies said they did not “reflect the business reality of vaccine developers,” according to the CEPI director. They also disliked the fact that CEPI should be able to set the price.
For industry, the rules were simply not in line with a competitive business model, according to Richard Hatchett.
——
BTW, the sensational article referred to above, results in this:
https://www.sciencedirect.com/science/article/pii/S0264410X19317190#!
Gerald Posner discusses CEPI in a New York Times article (from March): https://www.nytimes.com/2020/03/02/opinion/contributors/pharma-vaccines.html
—-
Before Covid-19 was identified last December, CEPI had raised three-fourths of the $1 billion it determined was necessary to fund the innovative research for expedited development of vaccines to treat new epidemics. Japan, Germany, Canada, Australia and Norway, as well as the Wellcome Trust and the Bill & Melinda Gates Foundation, had given $460 million. In the last two years, CEPI has used that money to provide grants for some leading edge biotechnologies that could revolutionize vaccine research and production.
But what has played mostly out of public view over that same time was the organization’s failed effort to get large pharmaceutical firms to agree to be partners without insisting on substantial profits or proprietary rights to research that CEPI helped to finance and produce (my bolding). That did not surprise many industry observers who knew that since the 1930s, the National Institutes of Health had spent over $900 billion on grants that drug firms relied on to patent brand-name medications.
————
The band plays on: Tanz mit Laibach
https://www.youtube.com/watch?v=Glu9wA4HjE0
Several lines of evidence show that immunity after COVID-19 wanes quite rapidly, and that immunity after immuniztion with several of the vaccines persists quite nicely, both in animal and human models. The reason for this is that the vaccines are engineered to stimulate strong defensive responses which include both antibody-mediated immunity and T-cell mediated immunity. Many of the vaccine candidates include adjuvants, which are materials which facilitate and enhance the immune response to the antigens in the vaccine.
just a thought to all who venture here now and again,
this post represents the reason i make Naked Capitalism my first click of the day
the content and the comments are priceless
and the combination unique and invaluable
thanks Yves
thanks All
The big unknown is of course the number of people in the test population who were actually exposed to the infection. If everyone in the test population were exposed and only 11 of the 15000 vaccinated developed symptons then we have 11/15000 or 99.9% effectiveness. However, if only 5% (1500)were actually exposed to infection during the test period then we have 11/750 or 98.5%, which looks pretty good. Does this sound logical? Ok the other unknown is the number of people in the vaccinated population whose own immune systems would have defeated the virus without the vaccine. That’s where the ratio helps 1-11/185 or 94% effective. Looks good to me.
The assumption is that the exposure rate was the same in both groups, therefore the expected number of infections in both groups should be about the same. The inoculated group had 5% the number of cases of the placebo group, and that’s where the 95% effectiveness rate comes from. Whether you like how they calculated it or not, the important thing to understand is that there’s nothing special or ad-hoc about this method, this is how they calculate the effectiveness of all vaccines (and prophylactic treatments in general), and the effectiveness of a good flu vaccine is around 60%, and it’s frequently as low as 40%.
I thought this was a sober and sobering post from Peter Doshi the assoicate editor at the British Medical Journal.
https://blogs.bmj.com/bmj/2020/11/26/peter-doshi-pfizer-and-modernas-95-effective-vaccines-lets-be-cautious-and-first-see-the-full-data/
The author also fails to address one other important issue: the trials have so far not demonstrated that these vaccines prevent real morbiidity mortality.
to do so, the trials would have needed to be MUCH larger.
Still, preventing symptomatic infection looks good. Does that translate into preventing mortality? We dont yet know. The published data admits this . the differnce in severe cases HAD Extremely wide confidence intervals.
Stopping transmission would be nice. But instilling sufficient immunity to not become seriously ill, much less die, is REALLY nice. If we could cut our current 3,000 deaths a day by even 50%, wouldn’t that be great?
Note I am a month into recovery from COVID, caught from my son, who probably caught it from anti-maskers at the factory where he works. (He’s in a high-metal-dust environment, his clothes are a different color by the end of the day, so for someone to not wear a mask is political correctness taken way too far.) We were both fortunate – he was back to 12-hours days once his quarantine was done. I still have some head cold symptoms, but it is that time of year. However, I know multiple people who have been hospitalized, and one person who died. One 30-something RN whose avocation is boxing (eg, he was in extraordinary physical condition) ended up critical. And all this was before Thanksgiving, before the current explosion of cases and consequent deterioration of the care that those critically ill will receive.
As to the math, it’s unfortunate from a statistical sense that right now wasn’t the core of the testing period. The number of cases among the placebo group would be far higher, and it would be easier to explain to the vast majority of the population who are not trained in statistical thinking. Even there humility is needed: I have formal training, graduate school courses in math stats and econometrics, and decades of empirical work employing that training. Nevertheless my reflexes remain those of a normal human in terms of misperceiving the impact of long odds. I have to consciously apply my training.
Finally, the above paragraph reflects a mind game. It’s not unfortunate in a human sense that the vaccines are far enough along to grant provisional approval. If only they’d been available even earlier…
Am I being overly cynical, or does it occur to anyone else that making a vaccine that just prevents symptoms but doesn’t prevent infection and transmission will tend to make the virus endemic, rather than extinguishing it. This will gradually increase the dangers to the unvaccinated population, creating a class of sick whose ‘access’ to vaccination has not actually provided vaccine. Assuming the vaccination will need to be refreshed, it also creates a large group of
hostagesrepeat customers. — Nice lungs you got there, it’d be a shame if somethin’ were to happen to ’emAnd here we see the inevitable result of poor analysis: the author speculates the vaccine may not prevent transmission; of course, many readers interpret this as “the vaccine doesn’t stop transmission” and now will spread this speculation as rock hard fact.
I’m starting to think the best health measure we could take would be to dismantle the internet. Crowdsourced wisdom will be our end.
another option is ending public health as a path to riches, as this is the primary reason for most of the skepticism, who would you like to blame that on?
Seems to me it’s the inevitable result of a broken health care system
Your reading comprehension seems poor.
By requiring that the vaccine provides durable sterilizing immunity you’ve set the bar higher, maybe by orders of magnitude, I don’t think the science is there for anyone to know for this virus.
I think Mike Smitka makes a compelling case for setting a lower threshold in preventing serious disease is priority number one, and one can say that without being a shill for the pharma companies. If none of the vaccines provide durable immunity it is of course great for their collective bottom lines, but if you know of an immunologist who thinks that they’re doing so deliberately I would be very interested to see a link.
Errr… this disease is endemic. With approaching a billion likely cases at this point, extinguishing it is a pipe-dream. It’ll be almost as hard to exterminate as it is to exterminate the flu. That horse has left the barn. It probably left the barn before the end of last year…
Indeed. At least at present, however, there is one big difference with flu: low levels of mutation (perhaps zero = a single strain) for the surface proteins of SARS-CoV-2, so that the vaccines currently being approved will continue to be effective. So while we may need a booster every year or two, depending on how long the immunity from a given vaccine, it will “work.”
In contrast flu vaccines protect against only a few strains (the most common vaccine type in the US targets 3), but with many, many strains in circulation at any given time (and new ones arising on a regular basis), those may not be the right strains. Hence new vaccines are developed 2x a year to target the strains epidemiologists predict will be the most prevalent. They can for example look at the strains prevalent in the winter in the southern hemisphere, and use what they see to guide their choices. Ditto what’s going on in winter in the north to guide vaccines for administration in the south. Needless to say, those predictions are not always accurate, and even if they do target the 3 most prevalent strains, you may by chance be exposed to one of the strains not included. Adding more strains to the flu vaccine doesn’t work, as the body won’t react equally to all of them: put in 6 strains, and your body may generate weak immunity to 2, very weak to another 2, and none at all to the last 2. (My body might develop moderate immunity to 1 and none to 5.)
Over time we may see substantive mutations that affect vaccine efficacy. But with the current vaccines, it would in principle be possible to wipe out the virus that causes COVID, assuming that a very high proportion of the population gets vaccinated (and potentially revaccinated), and constant monitoring for new zoonotic outbreaks among humans catching it from animal populations in which it would remain endemic.
I don’t expect that to happen. That’s because, thankfully, average mortality rates for COVID are well under 1%, whereas for smallpox they were 20%-30%. Too many people will be lax about immunizations, while governments will not enact the draconian policies that would be needed to offset that – unlike if we saw a reemergence of smallpox.
I am frustrated but hopeful that viable treatments will be approved for use like CytoDyn’s Leronlimab. I personally would choose a proven safe and effective treatment vs any of the vaccines!
Antiviral treatments or monoclonal antibodies are only useful if you apply them very early in the course of disease. Most people, by the time they show up in the hospital, can not benefit from these treatments and can have worse outcomes. I suggest searching for Dr. Daniel Griffin’s material about the “phases of covid” to understand how clinical protocols are evolving.
The real questions is
I can 100% answer at least the last question: the vaccine has not been approved for children nor pregnant woman, and immunocompromised people never get vaccines. They are protected by herd immunity or not at all. Same for people with allergic reactions to any of the vaccine components.
As usual, we won’t have the answer to most of the other questions until we’re further into Phase IV, which just started.