Some common cognitive biases impede effective responses to looming dangers like Covid. They are disconcertingly apparent as more and more evidence supports the notion that new strains of Covid, like the UK one spreading in the US, are markedly more infectious. That means (unless the UK strain is milder, which so far does not appear to be the case) we will shortly see a big increase the number of hospitalizations. This will take place when medical systems in many parts of the US are already at the breaking point, with even ambulance crews nearing their physical limits.
Yet rather than get in front of a near and present danger, the authorities and pundits are acting as if they can hold the present course, when that isn’t working very well in the US and UK. All bets are on Magic Covid Vaccines making the pandemic go away, when polls show only about 40% are willing to take them now (roughly 20% are anti-vaxxers and another 40% want to hold off to be assured of safety). Even if that cheery view might work out in the longer term, it ignores the cost of potentially catastrophic near-term damage.
Three fresh pieces look at the severity of the ossible downside. One, an interview with Phillip Alvelda originally published at the Institute for New Economic Thinking website, presented some critical facts relatively late in the article, which means they may have escaped the notice of some readers. Another is from MIT Technology Review yesterday, and the third is from Ben Hunt’s Epsilon Theory newsletter, which Hubert Horan kindly forwarded. Hunt’s take is the most comprehensive, so we’ll turn to that last.
The MIT Technology Review article underscores that the higher transmission rate of the UK variant is the real deal and the implications are dire:
If the variant strain, first spotted in the United Kingdom, is as infectious as some suspect, it could dominate US case numbers by March, send covid-19 deaths to unprecedented levels, and collide with the rollout of vaccines, research suggests.
British scientists fear that the new strain, which they say is 50% to 74% more transmissible (meaning the average case generates even more follow-on infections), has put wings on the feet of the pandemic in the UK, where covid-19 case numbers have risen swiftly….
“If the variant becomes common [in] the US,” Tom Frieden, former director of the CDC, said on Twitter, “it’s close to a worst-case scenario.” He says political turmoil, overtaxed hospitals, and an unrelenting new form of the virus could create a “perfect storm.”
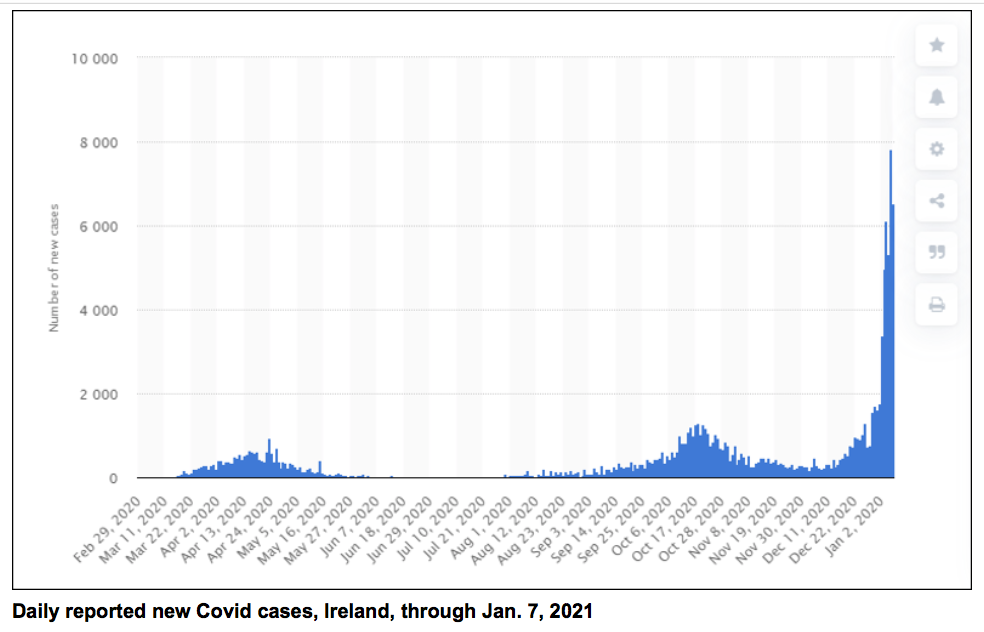
I've never seen an epi curve like this. The B.1.1.7 variant is spreading like wildfire in the UK and Ireland. If it spreads here, it will make an already-bad situation even worse. pic.twitter.com/VZB5BPm5om
— Dr. Tom Frieden (@DrTomFrieden) January 11, 2021
The article notes that Danish researchers peg the UK variant at 70% more contagious. And simple models show that the increased infection level will kill more people than a comparable percentage increase in mortality.
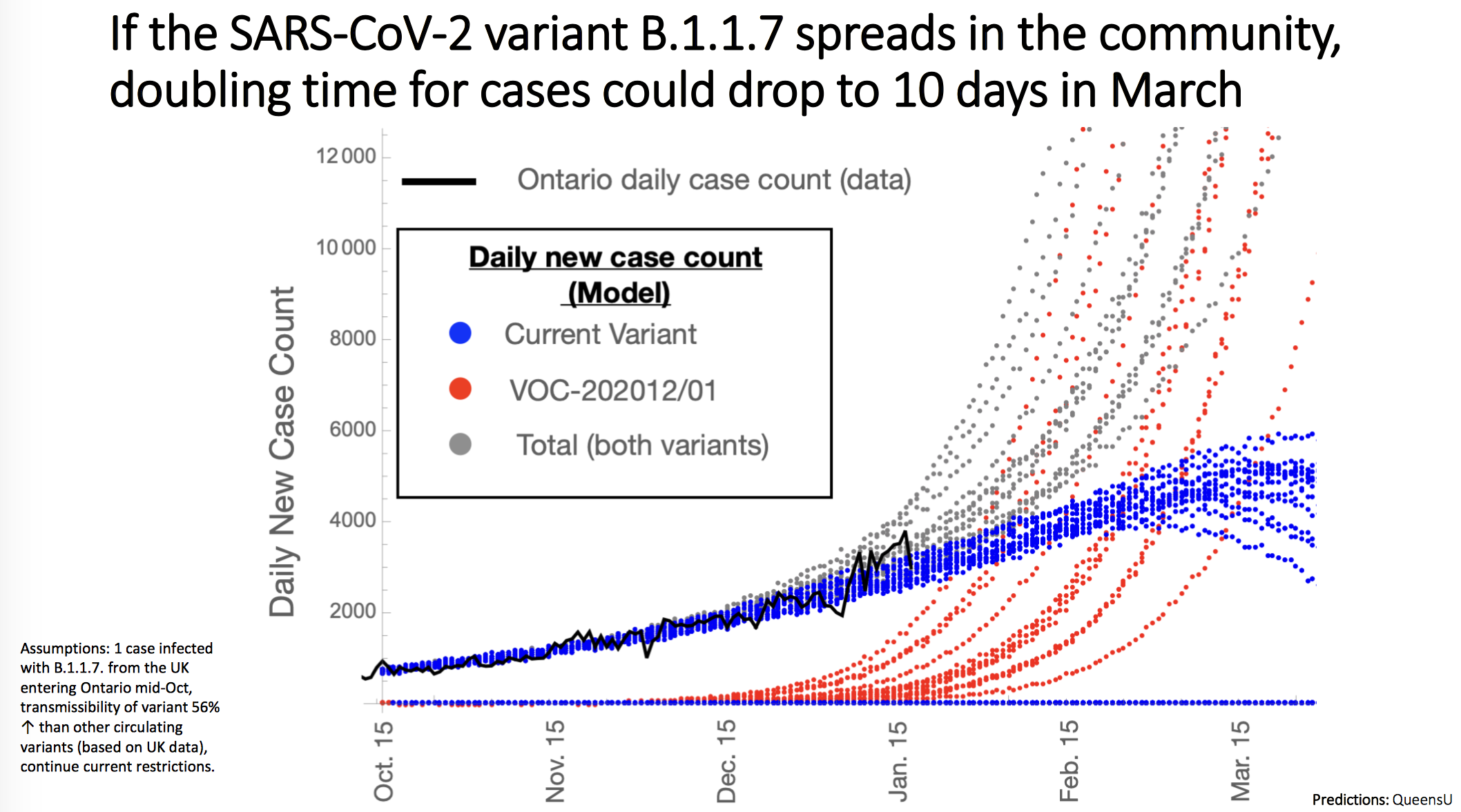
Reader CanChemist provided more detail in Links yesterday,: and referred to Slide 22 in new information published by the Government of Ontario as it issued “stay at home” order:
The new strains are terrifying, game-changing developments. That can’t be overstated. The one in particular focus right now is B117 which is actively circulating beyond the UK now into many countries including Denmark, USA, Canada. There has been serious discussion this past week now on Twitter under hashtag #B117 and the projections are extremely grim. The mainstream media has communicated that there is a new, more contagious strain, but not the true implications of that in practice….
The blue line is the projections of existing covid. The red line is B117 and the gray line is the total of existing + B117. The spread in lines is the probability spread based on different assumptions. This plot matches projections from other countries as well. In a nutshell, B117 is 50-70% more infectious and measures that control existing covid, like lockdowns, have been largely ineffectual so far against it. It means we seem to be on a pathway of “when, not if” to having the pandemic go so far out of control that I can’t even speculate what that looks like.
At INET, Alvelda argued that the UK variant appears to be better at binding to spike receptors, which means it can infect individuals at a lower viral load. He believes it will take only two months before the new variant becomes prevalent, which is consistent with the MIT Technology Review and Ontario estimates.
American failed state tendencies make it pretty much impossible to know where the new strain is spreading and implement aggressive contact tracing/isolation measures. Again from the MIT Technology Review:
Even as new variants threaten to emerge, the US still lacks the ability to adequately monitor changes to the virus, according to James Lu, cofounder and president of the Helix lab. He says the US as a whole has been sequencing about 300 to 400 virus samples a day but needs to sequence around 7,000 each day (or 5% of all tests) to get an accurate picture of what variations of the virus are spreading….
By comparison with other advanced countries, the US sequences a much smaller proportion of cases. According to the Washington Post, the country is sequencing one in every 300, compared with about 60% in Australia, 12% in Denmark, and 7.5% in the United Kingdom.
“We’re off by more than an order of magnitude from a proper level of surveillance,” says Lu. “The goal is to catch it before it before it becomes common.”
However, a second INET article provides correlations that strongly suggest the UK variant is responsible for sudden surges in cities with non-stop connections:
In states that have cities where direct U.K. flights terminate, such as Los Angeles, Houston, Seattle, New York City, Chicago, and Miami, Covid cases are picking up at an alarming rate.
And back to the Magic Covid Vaccine strategy. If you were paying attention and did a little math based on two doses, you could see that the current level of vaccinations is very far below the rate needed to achieve 70%+ vaccination levels in 2021. From the INET article:
We’ve administered something like 4.2 million doses– and that’s only the first dose. We haven’t fully immunized anyone. As with other Trump policies, he decided to work from the federal level in kind of a minimalist way and left the end point, the last mile of distribution, to the states, which didn’t have the foggiest clue how to manage distribution at that scale.
We’re seeing a supply chain that doesn’t have sufficient cold storage, that doesn’t have enough people, that isn’t organized, that doesn’t have tracking systems, that is just one tenth of the speed that you’d imagine. They didn’t do any testing or preparation for the last mile at all. I think the sad truth is that at the rate we’re going, it’s going to be mid to late 2022 before we start to see the effects of induced immunity from the vaccine.
But take some heart—-the 2022 estimate is if we keep going the way we’re going. I’m confident that the Biden administration will exercise more centralized control and we’ll have some real experts managing the distribution where it’s been largely a political exercise up until now….. My hope is that as more vaccines get approved and some have more relaxed handling requirements, you’ll start to see the rate of vaccination pick up. But I do think that best-case scenario, we’re going to be in this until the end of 2021 maybe slightly into 2022.
Note that the much less fussy Astra Zeneca isn’t expected to be approved until April.
And it isn’t at all clear that the Biden Administration will be able to do all that much better than the Trump Administration. The US is hampered by a fragmented health care system, including public health. States rather than the Feds regulate hospitals and pharmacies, the two main channels for drug distribution. There has yet to be even the teeniest signal that the Biden Administration is even thinking of trying to cut the Gordian knot and building independent channels or using the Defense Production Act to address supply shortages. They are real. Down in Alabama, I was shocked to go to the urgent care center last week to be told they were only doing so many Covid tests per day and I had come after they had hit their maximum. This restriction was clearly driven by test supplies; there was ample manpower in the facility. I went to a nearby merchant to run an errand and grumbled about my test fail. He said patients regularly lined up for hours before the center opened to be sure they’d get a test.
Instead, Politico reported earlier this week on infighting in the Biden Covid team, including Biden chewing out his no-prior-public-health experience Covid czar Jeff Zients over poor vaccination performance. And yesterday, Politico reported that most of Biden’s Covid advisory board has been frozen out on the development of the new Administration’s Covid response, set to be presented today.
The US has invested heavily in the Pfizer vaccine. It require tight coordination of deliveries and competent handling. It’s not as demanding as just in time, but a maximum 30 day hold in those Pfizer boxes and then only 5 days at refrigerator temps. And the high-by-vaccine-level of anaphylatic reactions is creating further distribution problems. And then there’s this, from USA Today:
People who receive a COVID-19 vaccine have to be watched for 15 minutes to ensure they don’t have an allergic reaction. This requires hospitals to set aside space and personnel – both of which are at a premium.
The observation period is 30 minutes for patients with a history of allergic reactions. This need slows down distribution in a hospital, since a nurse can’t trundle from room to room with a cart, delivering shots. It similarly reduces throughput in a pharmacy where another constraint is limited space for the vaccinated to hang out until they are deemed good to go.
In other words, some of the vaccination problems are due to having bet on the Pfizer version, which is difficult to deliver on multiple fronts, and a fragmented, very decentralized health care system is poorly suited to deal with “difficult”. An editorial in Newsday (yes, Dem hostile) describes the chaotic New York City vaccine rollout….and remember that New York, generally speaking, has more competent government and more resources than other jurisdictions (although Mayor De Blasio is widely recognized as performing poorly).
With all of these warning signs, the CDC has chosen to take a big dose of hopium. The CDC’s models show that the agency assumes that 77 million have already had symptomatic Covid. That’s a big multiple of 23 million confirmed cases. That means the CDC assumes over 20% of the population already has immunity…at least as long as immunity lasts.
Now to Ben Hunt (emphasis his):
I believe there is a non-trivial chance that the United States will experience a rolling series of “Ireland events” over the next 30-45 days, where the Covid effective reproductive number (Re not R0) reaches a value between 2.4 and 3.0 in states and regions where a) the more infectious UK-variant (or similar) Covid strain has been introduced, and b) Covid fatigue has led to deterioration in social distancing behaviors.
A single Ireland event is a disaster. A series of Ireland events on the scale of the United States is catastrophic. If this were to occur, I’d expect to see a doubling of new Covid cases/day from current levels in the aggregate (today’s 7-day average is 240k/day), peaking somewhere around 500,000 new daily cases before draconian economic shutdowns (more severe than anything we’ve seen to date) would occur in every impacted major metro area. Hospital systems across the country would be placed under enormous additional strain, leading to meaningfully higher case fatality ratios (CFRs) as medical care was rationed. Most critically, this new infection rate would far outpace our current vaccine distribution capacity and policy. Assuming that vaccines are preferentially administered to the elderly, aggregate infection fatality ratios (IFRs) should decrease, but the overall burden of severe outcomes (death, long-term health consequences) would shift to younger demographics.
Hunt argues that the CDC position that 77 million have already had symptomatic Covid cases is politically driven, since it’s not credible that so many would brush off Covid indicators as a mere seasonal bug. He continues:
A full-blown Ireland event is driven by both the more virulent UK-strain AND a deterioration in social distancing behaviors… Irish health authorities estimate that their starting point for Covid Re was something between 1.1 and 1.3 (meaning that, on average, one person infected with the SARS-CoV-2 virus would pass it along to 1.1 – 1.3 new people). They blame deteriorating masking/social distancing for the majority of their “event” (say, a 0.9 – 1.1 increase in the Re number), and the UK-variant for the balance (say, a 0.5 – 0.7 increase in Re)…Notably, the UK-variant is, relatively speaking, significantly more infectious than the baseline virus for “close contacts” (not face-to-face, up to 2 meters apart) rather than “direct contacts”, meaning that the UK-variant virus is particularly successful at bridging the air gap between strangers or short-duration contacts in an indoor space…. the UK-variant virus dramatically reduces the margin of error we have with mask wearing and social distancing outside of the home.
And to add to the cheery news, CNBC reports that reserachers have found two new strains, apparently-home-grown in the US, in Ohio. Oh, and they appear to be more infectious that the now-dominant strain in the US:
Researchers in Ohio said Wednesday that they’ve discovered two new variants of the coronavirus that likely originated in the U.S. — one of which quickly became the dominant strain in Columbus, Ohio, over a three-week period in late December and early January.
Like the strain first detected in the U.K., the U.S. mutations appear to make Covid-19 more contagious but do not seem like they will diminish the effectiveness of the vaccines, researchers said….
One of the new strains, found in just one patient in Ohio, contains a mutation identical to the now-dominant variant in the U.K., researchers said, noting that it “likely arose in a virus strain already present in the United States.” However, the “Columbus strain,” which the researchers said in a press release has become dominant in the city, includes “three other gene mutations not previously seen together in SARS-CoV2.”
“This new Columbus strain has the same genetic backbone as earlier cases we’ve studied, but these three mutations represent a significant evolution,” Dr. Dan Jones, vice chair of the division of molecular pathology at Ohio State and lead author of the study, said in a statement. “We know this shift didn’t come from the U.K. or South African branches of the virus.”
Now even if infections do spike, it’s possible that doctors outside hospitals will be forced to get more serious about treatments, a prong of attack that has oddly been downplayed in Covid combat strategies. But will behavior change soon enough in that scenario? Infection spikes worse than what we saw in New York and California last spring, with the medical system already looking like it’s relying on duct tape and baling wire means the remedy is even more stringent lockdowns than we’ve had….and for those to be bearable, that means another round of heavy-duty income support, an idea to which Washington is allergic.
And is the US even capable of serious enforcement? A friend’s significant other just went to Poland to see her family. The drill: 14 day mandatory quarantine. She can’t even go in the yard. Cameras trained on the house plus neighbors enlisted to monitor. First violation is a 5,000 euro fine. The second violation is a 15,000 euro fine and 6 to 12 months of incarceration. The fact that the US is incapable of cracking down on Covid scofflaws means we are setting up the worst outcomes.
Hubert Horan’s assessment via e-mail:
The new issue is the potential for a really massive spike in Covid cases, where medical systems break down completely. So much of the economic/political status quo seemed to depend on the (largely irrational) optimism that followed the initial vaccine approval. If this gets replaced by a universal “OMG we are so fucked” the damage could be catastrophic–stock market, many industries that have been hanging on the edge, rage at media, doctors, politicians–any “voice of authority”. Even if (rationally) it turns out to be a two-month issue that the vaccines could have reversed.
Obviously Biden won’t be up for this challenge but no other current or recent politician would have either. I don’t think events will fit any current narratives, and MSM attempts to spin them will fail. The general public won’t specifically blame either Biden or Trump. But if another 10 million people are suddenly out of work, no one will understand why it suddenly happened, and no one will trust anyone’s ideas about what to do next.
This scenario sounds all too plausible.
____
1 One bit of less downbeat news: the INET piece appears to have understated the potency of masks in reducing transmission, and understated the efficacy of surgical masks. Yes, K/N95s are better, but they have to be fitted, and every N95 I’ve gotten leaks on the side just like a surgical mask, albeit less so, so I have doubts that the increase in infection reduction in layperson use is as great at the author suggested. See this comprehensive review of the data on mask efficacy, which Lambert linked to yesterday. The issue seems to be increasing uptake, as well as getting users to wear them properly (none of this below the nose nonsense, or worse, pulling them down when speaking).


Just a comment on the Irish figures – the spike is somewhat exaggerated, as there was a slowdown in testing just before and after Christmas, meaning there was a ‘catch-up’ spike in the first week of January. But it was still staggeringly fast and steep and far beyond even the more pessimistic projections. At first, it didn’t seem to have been driven by the new variant, but this is now at around 45% of cases and rising. The past few days indicate that a peak may have been reached in cases, but we are now seeing a sudden increase in deaths, which seems to lag positive tests by about 3-4 weeks.
The data isn’t fully in, but what seems to have happened in Ireland is that the new variant established itself late November/early December, mostly among young people. It must be emphasised that mask and social distancing compliance has been generally very good in Ireland. But the likeliest scenario is that a bunch of super spreader events occurred among young people at school and partying in early December then spread through their elders at Christmas social events. In other words, a perfect storm in mid December caused this huge spike. The most likely scenario now is that actual cases will drop rapidly due to new restrictions, but death rates will rise very rapidly as the virus works its way up the age cohorts.
I think its hard to exaggerate just what bad news this variant could be. I suspect that it is now too late to stop its spread in North America and Europe, and even the Chinese may struggle to deal with it if it has established a foothold. It could lead to 2021 being as bad as 2020. Even worse, if hospital systems break down – the NHS is already at a genuine breaking point in parts of England.
And once again, it shows just how misguided and dangerous the whole herd immunity nonsense was. It was an invitation to the virus to mutate. And mainstream public health science, with its emphasis on ‘flattening the curve’ can’t get away lightly either. The only strategy that has worked so far with Covid has been complete suppression – i.e. the ROK/Taiwan/Vietnam/China/NZ/Aus approach. And even this may fail if new variants can get into those countries.
I think these new variants will make the first half of 2021 a really scary time, perhaps much worse than what we saw in 2020. Here in South Africa our own variant is wreaking havoc: triage tents set up in the parking lots of hospitals, record daily infections and deaths, hospital bed capacity at near breaking point, all elective procedures suspended indefinitely. Re: Complete suppression, this demands measures that are politically unviable in those countries that pride themselves on the elevation of individual rights to heights heretofore unknown in human history, where constitutionally enshrined rights ally with political/ideological zealotry and powerful business lobbies to place governments in straitjackets.
What didn’t work to contain the less infectious variants from 2020 is surely not going to work containing these new super strains in 2021, a point neatly summarized by Yves, yet this rather obvious tidbit seems completely lost on politicians around the world. It seems to me that democracy, at least in some respects, will have to be placed in chains for a period, otherwise the virus will continue to unfurl itself and blanket entire populations, with consequences too catastrophic to even contemplate.
I hope that whatever stopped the first waves hitting Africa too hard apply to the new variants.
I know that the ship has passed for complete suppression in most countries. I just regret that for whatever reason, it never became part of the narrative in so many countries (WHO, I think, has to take particular responsibility for this).
But you are right of course that so much of the discussion on ‘rights’ was completely hypocritical. It also lacked historical basis – there is a long history of very repressive laws working to suppress disease (TB being a particular example).
Just realized from your comment – what happens when this mutation reaches India?
Or Brazil, for that matter. This new strain is going to be a disaster in multiple places that are already struggling with the original.
Antibody prevalence in India is the highest reported in the world – could be up to 30 or 40 % in urban areas. So as long as this variant does not escape immunity, there may be substantial protection.
I think the main thing that stopped much of Africa from getting hit hard is that many african countries are largely rural, and even alot of the more urban regions have much of the people spending alot of their time in the cities outside rather than inside. The virus spreads much easier indoors.
Also not all of Africa has been so fortunate: South Africa is being hit incredibly hard. Not quite sure why they’re specifically having such a relatively hard time.
South Africa is the closest incarnation of western-style liberal democracy on the continent, that’s good during normal times, but terrible during a pandemic. Instead of being decisive and going all-in to enact effective abatement measures, the government has to be mindful of the plethora of legal challenges that the libertarians in our midst inevitably lodge, resulting in half-measures disguised as “balancing lives and livelihoods” (the mantra favoured by said libertarians). The business lobbies demand that the masses be hauled back to work to keep the economy churning, government relief packages are criticized as “money being frittered away”, high risk sectors like alcohol being temporarily banned is framed as “denying the fiscus of much needed tax revenue”. In other words, South Africa, while the most advanced economy on the continent and in theory the best equipped to handle the pandemic, is being bedeviled by the same issues that handicap an effective response in much of the west.
As I posted sometime ago, if only Chris Hani had lived to lead… Things would almost certainly be radically different.
SA is first world in so many ways, but abject poverty and destitution. Obviously the wealth is there to make things right (just like the US), but kleptocrats simply can’t be bothered.
Great point about the TB response. This is something unappreciated by a lot of the “rights” brigade, that history has called for the temporary curtailment of individual freedoms to subdue a rampaging disease.
I can speak from personal experience about this. I was a nurse looking after a young farm worker from Mexico whose leg got dragged into the augur of a rice harvester, in the neurological wing of a hospital in the Central Valley here in California. The leg was ripped clean off, but he survived, with a lot of neurological damage that needed extensive care and attention. In particular, one had to get very close to him to lift him and position him with minimum of pain.
Anyway, I got TB from him, and the law required me (obviously) to give up my job immediately, go into quarantine, take a pill each day for a year (that I reacted badly to), and undergo numerous X-rays and evaluations for the next year, and once a year for nine years after. This was back before Reagan defunded rural hospitals, so fortunately my county paid for all this. When my lungs were declared clear, I was able to return home, but it was made clear that if I stopped taking the medicine, or the X-rays showed anything wrong, that both I and my wife would have to quarantine and go through the same process. This was the law, and still is, AFAIK.
The irony was that around that time, HIV and AIDS was spreading, but being mostly ignored. Another nurse I worked with died of AIDS from a self-jab, but it was some time before the connection was made; so, losing my job this way may have saved my life, who knows?
The second irony is that due to the political fuss made by the community mainly suffering from HIV/AIDS, the proposals to extend the TB law to those who might carry/transmit this deadly communicable disease was squashed, and so the disease flourished mightily–purely for political reasons! If sufferers had had the same restrictions those with TB have, it would not have become the widespread disaster it did, only brought under control when the multi–drug regimes were discovered and put into widespread use.
Forgive me if I’m being pedantic, but I have two nitpicks
1) The human receptor to which SarsCov2 binds is called ACE2, not Spike. It sits on the outside of our cells: in the lungs, throat and inside of the nose, but also in many other tissues like our gastrointestinal tract, kidneys and for men, testes. Spike is the virus protein that binds to ACE2, and this binding is the first molecular host-virus interaction at the cellular level.
2) I’ve seen lots of speculation but no evidence – but please correct me as I’ve not been following that closely – about the underlying mechanism that causes the new UK variant to be more infectious. The mutations are all in the Spike protein, which makes it likely that something about the interaction with ACE2 has changed. My money would indeed be on Spike binding more stronly to ACE2 due to these mutations, making it ‘stickier’ if you will.
However absent evidence of this I would hesitate to use such terms especially in communications with the general public. The reason is that it’s easily misinterpreted. I’m a member of Nextdoor, a social media site, and people were spreading information supposedly coming from doctors that the new variant is stickier necessitating more handwashing, better washing of groceries, etc, while I would be much more worried about airborne transmission.
(I’m not questioning the increasingly strong epidemiological evidence that indeed it increases transmission – and using early tentative evidence as an argument for increasing lockdowns / vigilance is certainly warranted under the precautionary principle).
Many thanks by the way for consistenly staying ahead of the curve in your Covid coverage. This is truly exceptional in the current media landscape. This post is another excellent example.
Just to follow up on this, there might now actually be some evidence of the kind I had in mind.
A study was posted 3 days ago (not peer-reviewed yet) that takes the kind of mechanistic approach that I had in mind: they measured in the lab how well ACE2 and the receptor binding domain of Spike bind to one another, and found that certain mutations increase binding by a lot. One of these mutations also occurs int the UK and South-African variants. But the caveat is that the UK variants contained a number of mutations in Spike, I believe 13, while (if I understood correctly) this paper tested single mutations at a time. But it’s certainly suggestive that this mechanism is indeed key.
(They also suggest that an artificially created Spike with mutations that make it bind very tightly to ACE2 might be a potent SarsCov2 inhibitor, i.e. preventing the virus from binding because the receptor is already occupied).
Preprint here on biorxiv: https://doi.org/10.1101/2021.01.06.425392
and some discussion here: https://twitter.com/BallouxFrancois/status/1348707529220628489
So would common BP meds like ace inhibitors function as “artificially created spikes” – something that blocks the real virus from locking on to the site?
Way over my pay grade – sorry!
Good line of thought, but situation is very complex and heavily looked into and data are unclear on whether they are helpful, neutral or harmful. As of now, recommendations are to keep taking the drugs if you are already taking them.
I agree with your assessment regarding N95 masks. Without the proper seal, they probably aren’t much better than surgical masks if they’re even better at all. Recall that the best “loose” mask materials are those that (1) filter well; and (2) don’t restrict airflow too much. I haven’t worn an N95 but imagine that without the seal, more air escapes from the leaks than with a double-layer T-shirt mask. I really have no idea though.
Thinking about masks and transmission mitigations inspired me through the following chain of thoughts:
* that so-called “aerosol” transmission (and maybe fomites too) may become a more significant transmission mechanism than it already is
* that for a given space, maximum safe occupancy vs. ventilation throughput may be significantly lower
* that this situation is likely to be a lot worse for “front-line” workers, school children, and any others who occupy indoor spaces with strangers for long durations
* that this may substantially diminish the efficacy of partial lock-downs vs. current conditions
It looks like INET (quoted above) is reporting exactly that—diminished efficacy of partial lock-downs.
What really amazes me is how little attention this seems to be getting in the media, not to mention all the mixed messaging from the usual authorities. It certainly wasn’t a good look for CDC to debunk the notion that “mutant strains are spreading in the US” shortly before the Columbus strain was discovered. It’s like it’s January 2020 all over again. Maybe “hindsight is 2020” is the ultimate cosmic joke. 2020 the year we’re doomed to repeat until we get it right, like in the movie “Groundhog Day”.
My wife & I are the only ones we’ve seen wearing N-95 masks, everybody else we’ve encountered since March have been seen wearing vastly inferior masks/bandannas/whatever. And it isn’t just us, i’ve seen few N-95’s worn on the sidelines of NFL games by coaches, staff & players.
I shouldn’t have, but we needed a few things and popped into our local small supermarket, where 3 employees including the checker were sans mask, along with 3 customers unshod. That’s it for us, we’re not going there again, too risky.
This during a period when the only hospital serving a quarter of a million of us is bursting at the seams with Covid patients, as their staff is being ravaged by the virus, requiring a bevy of travelling nurses to fill in, and in a bit of added drama for the employees there, a rumor is going around that each of the travelling RN’s are receiving $2500 a day for their services, while everybody else earning say 1/5 or 1/7th as much in pay for doing the same tasks are wondering if they’re so much chopped liver in comparison.
As in the Spanish Flu, we’ll soon have people dying @ home all over the place, and what do you do with all the corpus delecti?
I have two old N95 masks left from the 2000s, made in USA by 3M. the build quality is incredible compared to the cheap-o KN95s.
I had around a dozen from my stash, and had used them exclusively when weed whacking, as little divots go into your mouth & nose if not covered up. They’d get all sweaty and after maybe a week’s worth of use, into the trash it went. A box of 30 N-95’s set my back $19 way back when.
I also had 4x nice blue model N-95’s that were obviously more cush than the white ones, and I sent my mom a couple, leaving one for my wife & I, which we saved for ‘dress occasions’.
I had laser surgery on my retina last month, and wore the brand new blue one, which elicited ‘wow, nice mask’ exclamations from nurses @ my beck & call. We’re talking about a $2 mask!
Early on in the Covid saga, 3M laid off 2,900 people in December 2020, followed by another 1,700 in August.
You’d think they’d have all the demand you could imagine, producing N-95’s but no.
Probably sold the factory (and/or equipment) that made the masks after they shut production down…
Having worn a few non-fitted N95s, I do think they are better than surgical masks. Breathing takes a teeny bit of effort v. none with a surgical mask. Surgical masks are supposed to reduce transmission by nearly 80%, N95s nearly 100%.
But the issue is N95s are supposed to protect the wearer from contagion. I’m not sure how good a job they do when they have a a gap in the seal on the sides or under the chin.
Also I just tried an N95 with headbands, as opposed to ear bands. Way tighter. For me, they probably approximate a fitted N95.
while i was getting my test last week in the parking lot of the little local clinic, i picked the nurse’ brains about all manner of covid related things.
among them were availability of tests.
when i asked if they were rationing tests, she paused, with eyebrows screwed up under her bonnet:”now that you mention it, that’s exactly what we’re doing”(implication: it’s being called something else in her world)
she said that the rapid pcr test…for which they have a little expensive desktop machine…is extremely limited, namely, the reagents. so this is reserved for people like my wife, who are at high risk, and whom need to know RFN.
I got the regular PCR(with a smaller, softer and less alarming swab than the one i got in , i think, april)…which they send away to a corporate lab, and has results in 3-5 days(mine took 4).
the rapid antigen test(which my youngest took) is the least reliable…but even these are being rationed.
one is eligible to get a test if one has symptoms, or is in close contact with someone who has the covid….and as stated, criteria much relaxed with high risk, like cancer patients…much more proactive and damn the torpedoes.
all of this is in a tiny county, with one town, 45 miles from other towns, and 100+ miles from a city of any size.
brother, in kingwood north of houston, reports that it’s easy to get tested, there…although he also has really good insurance, which may or may not factor in(he also works from home, and has adequate means to take 2 weeks off if need be…perhaps rendering him psychologically more comfortable with getting a test)
as far as vaccines, go…the clinic got 100 doses 3 weeks ago…ran out…and are expecting 200 between now and next week.
eligibility relies on criteria that is opaque, and hard to find, and “the line” for obtaining a shot is run through the county judge’s office, for some reason.
(same county judge who admits to artificially lowering the official case counts to avoid a mandatory mask order(didn’t want a mini- last wednesday in his office))
I’m not eligible for a shot…nor are the boys. wife is.
it’s the moderna shot, and several of the nurses, etc that i’ve talked to are leery of it…one told me to make the boys wait for a regular-ish vaccine, rather than these experimental offerings…and she’s not a maga, nor an hysteric(known her for 20+ years).
everything i’ve said will only get orders of magnitude worse with a variant that’s 70% more transmissible.
a slight uptick in mask wearing in town…based on my limited movement, of late(i’ve been for cigs once, and feedstore once…and got in and out in a hurry, and took care not to breathe on/touch anyone—other trips, i remained outside. )
but that slight uptick is hardly adequate.
i am not optimistic.
I have some N95 masks that fit really well (and the only way is trial and error, buying these expensive masks in small sets of 10-20 and then testing them), as proved by the fact that I can’t smell air freshener when I have one on.
But the challenge is when I am putting it on quickly.
The other day I wore one into a bakery and the smell of bread immediately wafted in.
It’s just hard to live like you live in a disease ward. You want to get out of the house and end up in an even more stressful situation.
As for N95 vs. surgical mask: the last time I got my hair cut, I wore an N95 under a surgical mask and didn’t smell anything. Something like 1 in 50 people in my town had a diagnosed Covid infection in December, so I thought it was worth it.
Man, that B117 curve is just exponential in growth and this article made really uncomfortable reading. There is only one way that this is going to end and that is by triage – a battlefield concept. I fear that this will become the new buzz-word this year as ‘social-distancing’ was last year. Thuto in a comment above mentioned its use in South Africa already. How will that play out in practice? So people that turn up, if they can, with Coronavirus will be immediately sorted out by a doctor – or perhaps a heavily-burdened nurse. If you do not look too bad, you will be sent home to work your way through it – or not. Those a bit sicker might get sent to one of several leased hotels with some modicum of supervision and perhaps treatment. If you are really sick but are relatively young or look like you might make it, you will be allowed in as the whole hospital is now essentially a huge ICU unit. For those too old, too sick, too weak or whatever, you will be sent back home as there is no use squandering the remaining medical resources on you. It will be brutal but without the resources or people to deal with what is coming, there will be little choice.
I read somewhere that two masks can make leakage worse because the reduced airflow through the mask then puts increased pressure on any leak sites in the mask, increasing rather than decreasing leakage. I don’t know if that is correct.
I have been wondering about the issue of cleaning out ones nasal and mouth cavities as a way to perhaps reduce viral load and thus both severity of possible illness for you, and transmission of virus for others. There have been a few articles about this, and also about the question of whether the nose has a lot more receptors than the mouth, in which case it might make sense to pinch off your nose, say with a swimming nose clip, under your mask. It does make you sound funny, and would be for short human encounters only, but hey, desperate times…..
I have been working on a list of my requirements for various providers (dentist, doctor, physical therapy, blood donation place, etc.) whom I would like to return to someday, which I plan to share with them. In addition to all of them and myself being vaccinated, and the other standard stuff, it really comes down to ventilation to protect me from their exhalations, and also the exhalations of their other patients/clients.
I am very surprised the government did not offer a liability “safe harbor” to businesses–do X on ventilation, etc., document it, and we will provide you a safe harbor. A lot more businesses could have stayed open this way, it seems. I am also surprised there has not been an explosion of entrepreneurs running around making businesses “Covid safe” (and certifying them as such), again using ventilation above all as the tool.
But now with a more infectious strain, even such measures may be out the window.
We do not give medical advice but per your line of thinking: a small scale “observational” study using an OTC mouthwash in Japan with 0.5% povidone iodine found that people with actual confirmed Covid who gargled with it 4X a day had 1/4 the hospitalization rate compared to a group with confirmed Covid selected to be demographically similar.
The reason this is plausible is povidone kills Covid in vitro faster than just about anything: 15 seconds. Even isopropyl alcohol takes 30 seconds (washing with soap is 20 second due to mechanical action of soap breaking down lipid exterior of Covid).
I looked up various studies and they had tested nose sprays and gargles with povidone iodone of up to 2.5% concentration. Use of up to 5-6 months had no ill effects (they didn’t test beyond that).
Having said that, povidone iodine kills lots of stuff, presumably including gut bacteria, so even more so that with normal gargles, it’s a good idea to try not to swallow it. And the one counter-indication would be if you have a high thyroid, since the iodine could increase T4 to T3 conversion.
To my knowledge, you cannot get a povidone iodine nose spray or mouthwash in the US. However, I have made my own home brew by diluting 10% povidone iodine with water to 1%. I gargle 2X a day and use it as a nose spray (occasionally, when I think I’ve been in a risky situation for the next few days). The gargle is foamy!
Thanks so much. I Looked around a little, it appears a company called Halodine has started selling both a 1.25% providone-iodine mouthwash and a 2.5% nasal spray, for crazy amounts of money ($25 for 2 ounces of mouthwash, $24 for six single use nasal swabsticks).
But the bigger question is why are not this or similar approaches being tested, and if effective at reducing transmission and/or illness, being pushed to the masses as part of the whole approach to Covid? Seems they would be pretty cheap, in the scheme of this.
Here is an article about a lipopeptide swab preventing transmission in ferrets:
https://www.biorxiv.org/content/10.1101/2020.11.04.361154v1
(probably I found this on NC to start with…….)
Here in Arizona, the governor is being urged to increase mitigations. Specifically, mask mandates and curfews. Not the first time he has been urged to do such things.
Link: https://www.kgun9.com/news/coronavirus/several-healthcare-providers-send-united-message-help-us-stop-covid-19-spread
Thanks NC for re-posting that plot, I think a picture is worth 1000 words in this case.
There is also an excellent thread from a few days ago that illustrates the issue
https://twitter.com/DrEricDing/status/1348080234265006082
Turns out last year was just the warm up for the real situation. Extremely grim and there’s no avoiding it by now.
The ‘spike’ structure seems to be changing in the new Corona variants. I thought the mRNA vaccines “targeted” proteins in the ‘spike’ — lead to human cells manufacturing and excreting spike proteins as antigens. Is it unreasonable to wonder whether the vaccines might not work at all on some of the Corona variants? Don’t Corona viruses tend to conserve the structure of the virus shell? If so, is there some reason the proteins in the virus shell weren’t selected as the “target”?
Further speculations — considering the logistics problems characteristic of the current mRNA vaccines I remain puzzled by the insistence on using human cells as the ‘factories’ for producing Corona proteins to act as antigens. The mRNA vaccines have been used in mice to produce antigens and if mice why not some other organism? I thought it were possible to manipulate yeasts or e-coli to manufacture drugs and presumably would be capable of manufacturing Corona proteins. I would expect there are techniques for separating yeasts or e-coli from the drugs they are used to produce — and I think there are also techniques for purifying the extracts. In fact didn’t Pfizer achieve its prominence by developing somewhat analogous processes for producing penicillin on a large scale — growing Penicillium, fungi in large tanks. GMO yeasts can used to produce plant based drugs [“Complete biosynthesis of noscapine and halogenated alkaloids in yeast”, https://www.pnas.org/content/115/17/E3922%5D
Is there some reason mRNA lipid capsules couldn’t be used to manufacture Corona proteins which might be extracted and purified to obtain relatively stable Corona proteins to use as antigens in a more conventional vaccine?
I think one of the ideas was to streamline new vaccine development. Just plug in the new mRNA sequence to your carrier mechanism and you are good to go, theoretically. No intermediate step of protein production, purification, etc. if it works it could be helpful for new strains.
I have read of that as a stated advantage of the new mRNA vaccines. That is fine and dandy … once it has been tested much more thoroughly. I am leary of messing around with the machinery in my cells. I do not believe the science is as well understood as claimed. If something goes wrong I would far prefer to toss a batch of yeast than wonder what new wonders my body might surprise me with. And I did begin my comment wondering at the logistics problems — which would be much easier to control inside a vaccine factory.
The reason to manufacture virus proteins in human cells is that most proteins exposed on the outside of a cell are glycosylated – that is, they have had sugar molecules attached. Yeast (a simple eukaryote) and bacteria don’t attach sugars the same way as mammalian cells so the proteins they make often don’t “look right” and won’t bind correctly. The proteins may not fold correctly either. Some proteins don’t have as much processing and you can produce them in bacteria, e.g. insulin.
mRNA lipid capsules don’t contain the cellular machinery to make proteins. Cells do.
You can think of the spike protein as a key, and the ACE2 receptor as a lock. The original covid strains had a key didn’t fit the lock that well and had to be jiggled to open up. The new strain has a key that fits better.
The vaccines were designed to work against the spike protein because it sticks out of the virus. We are all hoping it works against the new spike protein as well! This is an enveloped virus (it buds out with a little of the cell membrane) so the nucleocapsid protein is not exposed and isn’t as good of a target.
Regarding the footnote: On Fridays I volunteer at the local animal shelter. The work is mostly chores and some dog walking. I shave and put on a KN95. With some activities such as walking up the stairs from the basement I get light-headed and have to slow down or stop to recover. I had no such effects from using a surgical mask or cloth mask. Perhaps my soft, spherical face allows a better fit than for you Yves.
I’ve been to my dentist twice since xmas week and twice also to an endodontist. I was carefully examining how they are masked since I don’t have the option. They all had a surgical mask on top of another mask that wasn’t a surgical. Where I could get a good look, it looked like a respirator underneath. This was reassuring because my experience with surgical masks is that a lot of air passes around and not through the filter material. I have elastic cloth masks bought on Amazon that have much better fit than the surgical masks but I don’t trust the cloth as much as the KN95 in potentially contaminated air.
I’m seriously considering suspending my visits to the shelter. My work is useful to the staff and animals but I’m not sure it’s the responsible choice given current stats in Boston.
Btw, Yves, It’s not clear where the quote from Hubert Horan’s assessment via e-mail ends.
Thanks for your comment. If you are getting lightheaded from your K/N95 you probably have a very good seal. Early on, someone in a hospital attached a hospital-grade oximeter to himself and kept piling surgical masks on his face. He got to 6 masks with no change in his blood oxygen level. He quit at 6.
I just tried an N95 with the headbands and found the fit was way tighter. So that might be the way to go for people who think other types aren’t snug enough.
To pick up points made by both Thuto and PK, then if this analysis is anything like correct, we are headed for a period when people are going to have to be bluntly told, and even coerced into, doing things they don’t want to do, because the alternative is death.
This is something completely outside the current western mindset, especially in Europe. where the concept of Human Rights has been pushed to the point where happiness itself is pretty much regarded as a right. After the initial shock had worn off, we started to see articles appearing saying things like “the struggle against Covid must not be at the expense of fundamental human rights.” There have been any number of earnest calls for a “balance” to be struck, as though this was somehow possible. You can understand why: HR campaigners have nothing of any importance to say about the crisis (after generations of becoming more and more influential) and it’s the only line of business they have.
But it’s not possible even in theory, in my opinion, to compare these two things: it’s not even apples and oranges, it’s more like apples and aardvarks. I suppose some mad economist could try to set up a marginal preference exercise asking people to choose between units of human rights and numbers of dead, but it obviously wouldn’t work. You can’t measure HR in any meaningful quantitative sense, and even if you could, on what basis could you actually compare the two? Like it or not, I think we are probably headed for a time when a lot of customary rights will have to be sacrificed: that might mean control of movements, compulsory ID cards, compulsory vaccination, compulsory sequestration of the contaminated, mass incineration of corpses and other unpleasant things.
In Europe at least, we have completely lost the reflex of sacrificing freedoms in time of crisis, and there are many who appear to believe that existing freedoms represent some forever untouchable normative standard which must be maintained irrespective of the consequences. (The ghost of Immanuel Kant is still twitching and still causing trouble.) Governments are going to be politically reluctant to go against the HR discourse, especially as reflected in the ECHR. The latter contains provisions for suspension, but the chattering classes and the media will scream at any such suggestion. In France there are already over a hundred administrative law cases pending against the governments handling of the crisis (not unmerited, it must be said) and several Ministers have had their homes and offices searched by the Police for incriminating material. This can only get worse. I just hope the ECJ stays out of the party.
Excellent points. To be fair, it would be far easier asking the unwashed to temporarily hand over their rights in the name of a higher communitarian goal if there was a semblance of trust in authorities, and if those authorities hadn’t spent the best part of last half century telling us that there’s no such thing as a society.
I’m not talking ‘right’ to not wear masks, more like right to protest which seems to be curtailed now in UK.
Trust is a key point. TK of the Ask a Korean Blog and Twitter feed has been making that point about Korea – contrary to assertions in the western media ROK is a low trust society. But people followed the advice of the government because they trusted it in this particular situation (everyone except the right wing evangelicals).
They were able therefore to put in place very strong restrictions without any significant public pushback, and when they did crack down on the churches, it was with public support. The government was partially lucky that it happened on an upswing of popularity for the Moon administration, but it also communicated extremely well, so enhancing trust. This is a key point about those countries which have had relatively strong restrictions without public pushback, such as Norway, Denmark and New Zealand. Its not just in democracies – Vietnam did it as well – primarily I suspect because even Vietnamese who don’t like the Party there at least trusted it to manage the response correctly, and they did an outstanding job in mobilizing communities to self police.
Also, with the UK in mind, it doesn’t help waffling on and on and about theoretical scenarios and reacting before the results of the last batch of interventions have come in.
The UK government suffers from both ADHD and verbal diarrhoea, they just can’t sit still and shut up for the time it takes before the numbers come in. And that makes people tune out.
In Denmark they “sticks to the plan” for 1-2 months at a time, there is nothing like the UK’s “Everyday brings a new initiative”.
As we’re getting into scientific details (good!), may I pose a question to the knowledgeable. I have read multiple times about the exposure levels required to contract COVID. The implication is that one needs to accumulate an amount of virus in order to become sick. In my simple mind, a single virus particle can invade a cell, replicate by the help of the cell machinery and thereby be enough to bring on full-blown COVID in an individual.
Can someone address my misunderstanding or confusion here. Thanks readership.
Without making any particular claims of being knowledgeable beyond the knowledge of an interested layman — I’ll take a stab at answering your question.
I think you could model catching the Corona flu as two processes matched against each other. Model the infection process as virus particle(s) infecting cells and causing the production of more virus particles which go on to infect more cells. The human body mounts an opposing process detecting the virus particles as antigens and producing antibodies and other agents of the immune system. I don’t understand enough to do more than wave a hand at — T-cells and other cells in the blood that go around ingesting antibody tagged virus particles. A smaller number of virus particles means a slower infection process that might not be able to overcome the body’s immune system. More virus particles means a faster infection process. Although the simple model I described greatly simplifies the actual processes involved in infection and in the manifestations of symptoms — I think it is adequate for understanding how the virus ‘load’ — the number of virus particles in an exposure — affects the probability of experiencing an infection. Think of the virus load of an exposure as the initial condition for starting the infection processes.
Would that not suggest that the quickest way to stop the pandemic is to attempt to give everyone controlled, low-grade infections, at least those without comorbidity.
That sounds a lot like that hardy perennial, herd immunity.
Except the virus is not so stupid as to fall for it: If “those with low comorbidity” are the only “food” available, it will simply evolve to produce more virus with what it’s got, it will get more infectious and it will hit “those with low comorbidity” harder.
“Heard immunity through natural infection” is just bullshit. Which is Sponsored by the Koch Brothers.
So we know it is garbage.
PS:
Wife tested positive today, this is likely the more infectious strain because we already had The Corona Classic in February 2020.
She is ill like with the flu, for me it’s more like an “alert”, the “I know I have taken something but it has not really kicked in yet”-feeling.
It is a bit trippy for me. I have a Tinnitus that changes with rapid head movement and crazy dreams. No fever. Blood Oxygen % is Okay.
We have food and everything for at least 6 weeks so we don’t have to go out.
Just now read you comment. Hope things go well with you and your wife. Must be tough after having gone through it last year but at least you are set for the next six weeks to wait it out.
That’s what conventional vaccines do.
What Ames said above. You just explained to us how all vaccines work, as if vaccines were a new thing nobody had thought of previously.
Also keep in mind that it’s a stochastic process. While in theory it’s possible that a single virion will make you sick, given the barriers it needs to overcome to do so the odds are well stacked against it. Thus, the higher the viral load, the higher the chances get that some (or many!) of them establish a local infection.
I think of it as the moment a virus particle comes in, the starter’s pistol goes off. The virus has a doubling time, 1,2,4,8,16 etc. The immune system has a fixed lag. If the virus starts off with 50 particles VS 1 million makes a big difference in how out of control the infection gets before the immune system organizes its response.
> In my simple mind, a single virus particle can invade a cell, replicate by the help of the cell machinery and thereby be enough to bring on full-blown COVID in an individual.
I know I linked to a study on precisely this point, I believe in vitro (because how on earth could you test this in vivo). But I can’t find it….
The number of viruses (“effective dose”) was quite small, IIRC in the four figures. I cannot find how many viral particles a droplet, let alone an aerosol particle, contains.
I think in the body the number would vary greatly, depending on where the viruses had the luck to land, whether in a small particle inhaled deep into the lungs, in the nose (defended by mucus), in the mouth (defended by saliva).
Traveled to New Orleans for 3 days, somewhat unwillingly. My mom is 93, has dementia but still recognizing me. She has serious heart disease and sleeps 20 hours a day. Residents and staff in her small facility were vaccinated with Moderna on Friday.
Knowing of the impending B117 blowout by March and her continued deterioration I made a “now or maybe never” travel risk assessment.
We have well fitting N95s which provide a Modicum of safety.
Mask use on my AA flights appears good, but plenty of gaiters, cloth and paper masks. Maybe 5% have K/N95 masks.
Went for a maskless run yesterday morning on the levee and kept plenty of distance from others. Yet a woman jabbering loudly on her phone passed me about 20 feet away and I got a good whiff of perfume . Lesson learned!
Most appalling was the New Orleans gate areas. 50% with no masks or masks pulled down. A number were legitimately having coffee or snacks. But half were maskholes. Fortunately the airport is maybe at 10% capacity this morning .
What it particularly disturbing Is the minimal MSM coverage of the huge new B117 risks. This is not to minimize The current political coverage that’s important. But MSM coverage of the potential B117 doom is scant. Even on long from news websites you have to dig; seldom anything above the fold. Like February, this is “Deja vu all over again”.
This will be so bad…
We have our vaccination #1 scheduled for next week.
The news in this post is very disturbing though not unexpected. The US badly mishandled the Corona pandemic even after it had been given examples of reasonably effective public health control measures used with relative success to handle the pandemic in several countries of the Orient. With new variants of the Corona virus showing up — which should not be a surprise to public health officials or our Medical Industrial Complex — the US is even less ready to handle the challenge. Trump or Biden, republican or democrat, I fear we will very soon miss the safe and easy times of 2020. I like to believe the Biden administration will be an improvement over Trump but that is a very low bar to clear and very little consolation as the situation worsens beyond any small improvement I expect from Biden’s administration. And if this is how the US meets a challenge like the Corona pandemic I have little hope the Government will be of much help for dealing with the much greater challenges the rest of this decade promises.
Great! Another virus on the way. Just what we need. Remember the shortages of everything last March? It’s happening again. Went to Costco, then Walmart, one toilet paper bundle per customer, but also canned soup, pasta, other things, even batteries, gone.
Everything from car plant shutdowns because of a lack of semiconductors, to toilet paper and masks is threatened in the supply chain. Obtain what your family needs while it’s easy.
Would you rather have a lower credit card bill and empty cupboard, or a higher bill and enough food and supplies to mean you don’t have to leave the house for 6 months?
Thank You Yves…for putting comments back on. So much learned in the comments!
Yes, that goes for me too. This post was spectacular. It looks like B117 is just the vanguard of the mutations. Two new ones in Ohio, etc. It sounds to me like we need to focus immediately if not sooner on doing a “Covid shot” every year, just like the flu shot. As well as good, effective medicines to reduce severe symptoms. I’m a firm believer in mask wearing – the thicker the better. I’ve been wearing a 4-layer fleece scarf that is big enough to tie snugly, covering all the vents and then tuck down my shirt. And I’ve been wearing surgical gloves when I go shopping or to the post office. In my frustration yesterday I went surfing and found a YouTube interview with my favorite author – Edward Steele. Virologist, immunologist, geneticist. He says that the virus is everywhere, there is no escaping it so hand washing and masks are imperative. He also says, that based on scientific understanding of virus behavior that the speculation that Covid 19 is biowarfare is just pure nonsense. This virus is behaving just like any other and now (after a bit of a lag – interview was done a few months ago) has started to mutate. So this looks to me like it really is OMG for a while. And it will happen just like the flu, every year. Since it is an altogether new virus, we are all getting much sicker than we would if it were an old regular. He didn’t have much faith in the vaccines, but what else can we do? Medicines would be a good alternative imo. I’m thinking this must be the proverbial second wave that people refer to when talking about the Spanish flu. The mutation phase?
I saw a very long interview with a pandemic expert in early March last year, just as things were getting underway (sorry I can’t remember who..). He was quite clear that this virus was going to go endemic and that we’d be in an influenza type situation where we’d be looking at regular vaccinations (yearly or more) and that it might take close to 10 years to reach a new equilibrium of co-existence. So yes, I think that’s coming true and that we’ll be getting covid shots 1-2x year for the forseeable future, and there will be some natural selection going on :(.
I am very optimistic about vaccines being a critical part of the solution, but since this is a new illness and new vaccines (and technology) there will surely be some growing pains.
Thanks for this. I remember back in January of last year, it seemed like Naked Capitalism was the only place taking covid-19 seriously, while other news outlets seemed to barely mention it, or were downplaying the severity. The idea that it would effect the US was not being discussed seriously.
Using the general rule of thumb that the writers and commenters at NC are smarter than me, I began stocking up on some supplies and tried to prepare as best I could. Seeing it discussed here gave me a few weeks head start, and I managed to get myself situated before it was even on other people’s radar. At the time it was an odd feeling checking out at the grocery store with a cart full of rice and canned goods when everyone around me was going on about business as usual. Then later in March, there were widespread shortages and I was lucky to have planned ahead.
This post is giving me an eerily similar feeling. I already have food, masks, and general supplies stocked up, and I don’t know how I could avoid the public any more than I already am currently, so I don’t know how much more I can do to prepare for what’s coming this time.
It’s always good to hear from Hubert Horan, a hero in my eyes because of his series of articles about Uber.
My money is on the mutation allows a 2nd receptor in addition to ACE2. Two doors in explains the explosion more than “stickiness”.
I focus on this sentence:
I think it’s very good to focus on what we all need to do personally — stockpile, for example, before it’s too late. However, I think the prospect of catastrophic damage — what Taleb calls “ruin,” and of what Smith urges any nation has “a great deal of” — isn’t, as it were, priced into our thinking (let alone Mr. Market’s).
Imagine that Warren Mosler’s proverbial man with a gun — the man who turns litter into money — gets Covid. What then?
To me, stockpiling enough to last 6 months or a year might be as futile in the long run if we’re looking at something that could last as long as one of our recent wars (I plead with you to start from Z and go backwards in choosing) and then it wouldn’t be enough, as if you were a smarty in Holland in 1940, but what good did it do in 1944?
That said, its a good idea, but also think out in terms of how you can feed yourself. I have 100 fat cows within a few miles of me owned by locals who would prefer to sell to locals, a fruit cocktail in the valley below, with an an orchard in mid grow.
Learning how to grow things is learning patience, in itself a worthy pursuit.
Most Americans are not in such a position, living in places where the ground may not thaw until May and cannot grow their own food, many have no store anywhere near them, no local farmers willing to sell to them. “Want a few bushels of GMO corn, or silage, or soybeans?” Your kids will love that!
Food if stored in cool conditions is edible well beyond its expiration date. Pasta, soap, fertilizer, clothing, firewood, motor oil, sporting equipment, electronics, sawblades, car tires, etc, might mean rough survival. What would you say to your children starving to death in a protracted emergency? “We didn’t want to clutter up the garage with stuff and not be able to park the car in there?”