By Lambert Strether of Corrente.
B117[1] is the Covid variant shortly to become “dominant” in the United States. Where did it come from? Outside the United States. That makes border control, especially for air travel, of paramount concern. It’s not. Or else B117 wouldn’t be here! That’s basically the post, which is pure common sense as soon as you see it. But allow me to elaborate. First, I’ll briefly summarize the origins of B117, and first spread to the United States. Then I will describe how other Japan and Vietnam have successful controlled it, though [drumroll] border controls, among other techniques. Finally, I will contrast what other countries are doing to what we are doing, and conclude. (All in all, yet another case study for How the West Lost COVID, if preventing the virus from spreading be the appropriate metric for success.)
The Origins of B117
At Virological.org, we find “Phylogenetic evidence that B.1.1.7 has been circulating in the United States since early- to mid-November,” which gives a brief history of the origin and spread of B117:
When SARS-CoV-2 emerged in China late December 2019 and early January 2020, there was little circulating genetic variation as it was exported across the world. This made estimating the number and timing of introductions difficult. Since then, the virus has accumulated mutations (as all RNA viruses do) in a (largely) clock-like manner, diversifying into a myriad of lineages. One of these lineages, ‘B.1.1.7’, first arose in the UK in September after an episode of heightened mutation, likely within a single host. This lineage has continued to evolve over the last several months while rapidly increasing in frequency across southeast England and elsewhere. …. The rapid increase in the UK has made export increasingly likely, and, as of 1/17/2021, the lineage has been detected in 55 countries, including the United States.
“[A]n episode of heightened mutation, likely within a single host” likely means an immunocompromised individual. From Science, “U.K. variant puts spotlight on immunocompromised patients’ role in the COVID-19 pandemic“:
In June, Ravindra Gupta, a virologist at the University of Cambridge, heard about a cancer patient who had come into a local hospital the month before with COVID-19 and was still shedding virus…. That made it hard for him to shake the infection with SARS-CoV-2.
…When Gupta studied genome sequences from the coronavirus that infected the patient, he discovered that SARS-CoV-2 had acquired several mutations that might have allowed it to elude the antibodies.
Now, his analysis, reported in a preprint on medRxiv earlier this month, has become a crucial puzzle piece for researchers trying to understand the importance of B.1.1.7, the new SARS-CoV-2 variant first found in the United Kingdom. That strain, which appears to spread faster than others, contains one of the mutations that Gupta found, and researchers believe B.1.1.7, too, may have originated in an immunocompromised patient who had a long-running infection. “It’s a perfectly logical and rational hypothesis,” says infectious disease scientist Jeremy Farrar, director of the Wellcome Trust.
In terms of the social determinants of health, it’s intriguing that B117 originated in Kent, the sort of place where immunocompromised are likely to be found. From Patrick Cockburn in the London Review of Books:
But it was becoming clear that, whatever the effectiveness of lockdown in other parts of the UK, it wasn’t working in this corner of Kent. The surge in infections moved inexorably inland towards where I live in Canterbury, fifteen miles from Margate and ten miles from Faversham.
It wasn’t surprising that Swale and Thanet should be badly affected: these are areas notorious for their poverty and likely to provide an ideal breeding ground for the virus. They are prime examples of coastal Britain, depressed places where failed hotels and B&Bs have been chopped up into one-room flats and where few can work from home because their jobs won’t allow it; the homes, in any case, are too small to work in. Years of austerity had already cut back the funding and benefits on which such towns depended. People were vulnerable to the virus here because their health was poor before the pandemic and their access to healthcare limited: in Swale the ratio of GPs to residents is lower than anywhere else in England. Inequality is extreme: a woman living in the most affluent ward in Thanet will live on average 22 years longer than a woman living in the most deprived ward.
One thinks at once of deindustrialized flyover and deaths of despair.
Be that as it may, B117 is not a good lineage to have been detected. From the Journal of the American Medical Association, “SARS-CoV-2 Viral Variants—Tackling a Moving Target“:
Epidemiological studies indicate that the B.1.1.7/20I/501Y.V1 strain is 30% to 80% more effectively transmitted and results in higher nasopharyngeal viral loads than the wild-type strain of SARS-CoV. Also of concern are retrospective observational studies suggesting an approximately 30% increased risk of death associated with this variant.
Unfortunately for us all, B117 travels by air. From bioRvix[2], “Phylogenetic analyses of SARS-CoV-2 B.1.1.7 lineage suggest a single origin followed by multiple exportation events versus convergent evolution”
[O]ur analyses point to an origin in and spread of the VOC B.1.1.7 from the UK. As for the virus’ initial and subsequent spread, global connectedness and high levels of human mobility undoubtedly facilitated VOC B.1.1.7 dissemination. The swift global spread of VOC B.1.1.7 illustrates that current restrictions are insufficient to prevent the spread of new and emerging variants. Similar to Ebola, HCV and HIV, countermeasures to SARS-CoV-2 spread should be developed with a broader perspective than the national level. Otherwise, without population immunity, successful local reductions in SARS-CoV-2 burden will be counteracted by imported infections that set off new waves of viral spread, possibly exacerbated by novel phenotypic characteristics of the imported strains
Yikes. With that background, let’s find out how B117 came to the United States.
How B117 Spread to the United States
B117 came to the United States by air (and not by, say, ocean liner, by surface transport, or by hopping the border). From medRxiv, “Genomic epidemiology identifies emergence and rapid transmission of SARS-CoV-2 B.1.1.7 in the United States“:
[W]e investigated the prevalence and growth dynamics of this variant in the United States (U.S.), tracking it back to its early emergence and onward local transmission. … Our phylogenetic analyses indicate that there have been multiple introductions of B.1.1.7 into the U.S., with the earliest dating back to the end of November, 2020. These analyses revealed large clades of closely related SARS-CoV-2 lineages clustering within individual states, as well as national spread indicated by several smaller clades defined by mixtures of samples from patients who reside in different U.S. states. These findings are consistent with community transmission following several of these introductions, including spread across U.S. states.
… [O]ur TMRCA [median time to the most recent common ancestor] estimates coincide with increased periods of travel, where the U.S. Transportation Security Administration reported over one million travelers crossing checkpoints for several days during the peak Thanksgiving season (November 20-29, 2020) and for twelve of eighteen days surrounding the Christmas and New Year’s holidays (December 18, 2020 to January 4, 2021) (TSA, 2021), providing a likely explanation for how B.1.1.7 may have been introduced via international travel and spread across the U.S. via domestic travel.
From the New York Times, summarizing the above study in “Virus Variant First Found in Britain Now Spreading Rapidly in U.S.”:
The first case turned up on Dec. 29 in Colorado, and Dr. Andersen found another soon after in San Diego. In short order it was spotted in many other parts of the country. The variant was separately introduced into the country at least eight times, most likely as a result of people traveling to the United States from Britain between Thanksgiving and Christmas.
(We will have an individual case when we look at the United States response, below.) Of course the variant arrived by air. How else? Now let’s look at how two other countries handled the appearance of B117.
How Other Countries Have Handled B117
First, Vietnam. From the Financial Times, we see the advantages to citizens of not living in a failed state like our own:
Vietnam’s ability to contain its first wave of infections, thanks to vigorous contact tracing, strict quarantine requirements and border controls, has allowed most aspects of normal life to resume.
Nevertheless, the variant arrived. By air. From Channel News Asia:
The two [B117] patients reported earlier in the day include a support staff worker at Van Don international airport who was responsible for taking infected passengers arriving from abroad to COVID-19 quarantine facilities.
The other case is a factory worker who came into contact with a Vietnamese national who later travelled to Japan and tested positive there for the new UK variant of the virus, which has been determined to be much more easily transmissible.
Interestingly, Vietnam tested travelers across internal borders, quarantining them if necessary. From VN Express, “Hanoi tests all arrivals from areas with coronavirus infections“:
Hanoi said people who arrived from Hai Duong Province, the country’s Covid-19 epicenter, and areas with active cases in 11 other cities and provinces would be tested for the coronavirus.
Hanoi’s Health Department said Thursday it would perform Covid-19 tests on people coming to Hanoi from areas having reported infections since the new wave hit Vietnam late last month.
People subject to the tests include those coming from Cam Giang District, Hai Duong’s biggest hotspot, since January 15, and other places of Hai Duong since February 2.
HCMC and some northern localities have also mandated a 14-day quarantine or even barred entry for people coming from Hai Duong.
It looks to me like the cases at Van Don international airport were all from Vietnamese nationals, since Vietnam’s restrictions for foreigners are rather draconian. From the United States Embassy in Vietnam, “COVID-19 Information“:
On March 17, the Vietnamese government announced that they will work with relevant ministries and agencies to consider gradual resumption of international flights; however, there has been no official guidance at this time. As of today, the Vietnamese government continues to suspend entry into Vietnam to all foreigners, including people with a Vietnamese visa exemption certificate. This policy has very limited exemptions for diplomatic, official duty, and special cases, including experts, business managers, foreign investors, and high-tech workers of businesses involved in important projects as determined by the Government of Vietnam. Family reunification is not one of the exemptions.
Travelers currently allowed to enter Vietnam, including Vietnamese nationals and diplomatic, official duty, and special cases, including experts, business managers, foreign investors, and high-tech workers of businesses involved in important projects as determined by the Government of Vietnam, and their family members, are subjected to mandatory quarantine upon arrival.
(The quarantines are free.) A discussion of Vietnam’s testing strategy, with a chart of their success:
Vietnam has beaten their third wave in under 2 months.
How? A key strategy has been third-degree contact tracing.
1️⃣ Cases isolated
2️⃣ Close contacts quarantined
3️⃣ Contacts of contacts must stay home for 14 daysResult: just 2572 cases & 35 deaths.
➡️ https://t.co/wUzWXRgGzq https://t.co/49svqO3cHr pic.twitter.com/Ag6aynPoP6
— Dr Zoë Hyde (@DrZoeHyde) March 21, 2021
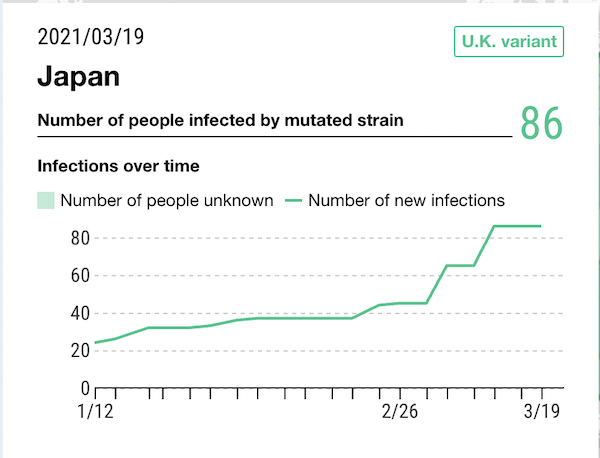
And now, Japan, whose first case of B117 arrived — and I know this will surprise you — by air. From Euroweekly, “British Traveller Violates Quarantine Rules And Infects Tokyo Residents”[3]:
The Ministry of Health, Labor and Welfare announced on Sunday, January 10, that three men and women in their 20s have been infected in Tokyo with a mutant strain of the new coronavirus that is prevalent in the United Kingdom.
Two of them were having dinner with the British man in his thirties, who is said to have tested positive after arriving from England on December 22.
The Brit was supposed to be observing a quarantine period at the time, however, he went out for dinner with about 10 people, although it seems that there are no other people infected.
Of the three men and women, two became ill on December 30 and January 2, respectively, who were confirmed to be infected with the mutant strain.
ABC gives the Japanese government’s response. “Asia Today: Japan halts all foreign arrivals over UK variant“:
Japan is barring entry of all nonresident foreign nationals as a precaution against a new and potentially more contagious coronavirus variant that has spread across Britain.
Japan is also suspending the exemption of a 14-day quarantine for Japanese nationals and resident foreigners in a short-track program that began in November. The entrants now must carry proof of a negative test 72 hours prior to departure for Japan and self-isolate for two weeks after arrival.
Lest you think that “self-isolate” is lax, here are the rules. From Timeout Tokyo:
As of March 18, inbound travellers must install three apps on their smartphones before departing for Japan: the government’s Cocoa Covid-19 contact tracing app (for iOS and Android), the government’s OSSMA location confirmation app (for iOS and Android), and Skype. If travellers don’t have a personal smartphone, they must rent one at the airport.
The revised quarantine measures have come into effect since Friday February 5. Additionally, foreign residents who break quarantine rules will be penalised and could have their residency status revoked. This report also states that from February 13, authorities will be allowed to impose fines and legal penalties on those who break the quarantine law, which may include a one-year imprisonment or a fine of up to ¥1 million.
The inbound travellers must also have undergone testing. From the Japan Times, “With emergency extension for Tokyo area likely, Japan expands border control measures“:
All people coming from abroad are required to undergo tests for COVID-19 prior to their departure for Japan, submit proof they have tested negative upon arrival and observe a 14-day quarantine. However, with the change, people arriving from Austria, Belgium, Brazil, Denmark, France, Germany, Italy, the Netherlands, Nigeria, Slovakia, Sweden, Switzerland and the United Arab Emirates will be required to self-isolate for the first three days at facilities designated by the government. After that period, they will be required to undergo tests for the novel coronavirus once again, and only those who test negative will be able to self-isolate at home or at a hotel of their choice for the remainder of the quarantine period.
These measures seem to have done the trick. From Nikkei Asian Review:
Of course, Japan has the Olympics coming up. Good luck to them, is all I can say.
I began with Vietnam’s strong response, then Japan’s somewhat weaker response, which brings me to the weak response of the United States.
How the United States Has Handled B117
We’ve seen how Vietnam and Japan brought B117 under control through a combination of border controls (both international and domestic) and quarantines (combined with existing systems for contact tracing. Since the United States can’t do contract tracing, we won’t look at that). Let’s see how the United States stacks up, at international and domestic borders.
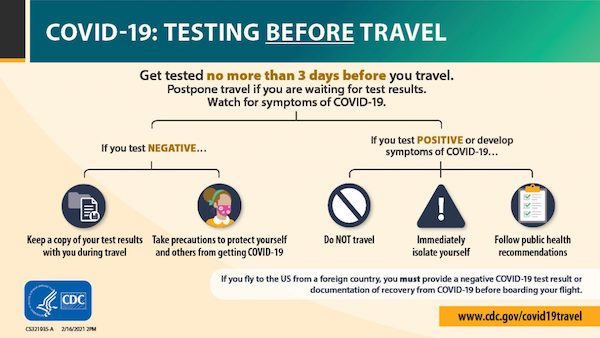
Here is an example of one B117 international-travel case from the CDC’s Morbidity and Mortality Weekly Report, in “Travel from the United Kingdom to the United States by a Symptomatic Patient Infected with the SARS-CoV-2 B.1.1.7 Variant — Texas, January 2021:”
On December 30, the patient disclosed a runny nose during the pretravel interview but was cleared to fly from London to Dallas [!!], Texas the same day. Upon arrival in the United States on December 31, the patient stayed overnight in a hotel and then drove home (approximately 8 hours). On the way home, the patient stopped five times, including twice for food, twice for gas, and once at a grocery store. Throughout the international and domestic travel period, the patient reported trying to maintain physical distance from others and wearing a cloth face mask, except while eating or drinking. The patient began self-quarantine upon returning home, which was broken twice for a medical and testing appointment.
Notice the complete absence of a mandatory quarantine. I have to quote a lot more so you can see what’s not there:
This case demonstrates how a variant of concern, in this case B.1.1.7, might be translocated between communities through travel. At the time of this person’s travel, CDC had an order in place requiring proof of a negative SARS-CoV-2 test ≤3 days before departure, or documentation of recovery from COVID-19, for all air passengers boarding a flight to the United States from the United Kingdom (3). Subsequently, on January 12, CDC issued an order expanding this requirement to all international air passengers arriving in the United States, effective January 26, 2021 (4). Because of the lower sensitivity of some SARS-CoV-2 antigen tests (5,6), the potential for false-negative results when nucleic acid amplification tests (such as RT-PCR) are administered shortly after infection with SARS-CoV-2 (7), and the subsequent potential for exposing others after a test is administered, predeparture testing should be considered one component of a comprehensive travel risk management strategy. Properly timed testing, both before and after travel, together with self-monitoring for symptoms, a period of self-quarantine after travel, use of a well-fitting mask, hand hygiene, and physical distancing, are critical elements of this strategy (8). Persons should not travel if they are experiencing symptoms compatible with COVID-19 or if they have received a positive SARS-CoV-2 test result and have not met criteria to discontinue isolation,¶ have had close contact with a person with suspected or confirmed COVID-19 and have not subsequently met criteria to end quarantine,** or have a pending SARS-CoV-2 viral test result.
Notice that CDC does not recommend quarantine (leaving the matter, as the notes show, to states and localities).
This case is from a US citizen (as with Vietnam), so let’s look more closely at CDC’s current restrictions for US citizens. When leaving the foreign country for the United States:
These are only paperwork requirements, and in the absence of some validation and enforcement process, easily gamed. NC reader AM flew to Scotland and back in October 2020, and described the paperwork as “theatre.” Do any readers have updated information? When returning from the foreign country to the United States:

More theatre. And “self-isolation”/”self-quarantine” requirements are entirely voluntary (!), as is testing (!!), very much in contrast to Vietnam and Japan.
Now, to be fair, the United States does “suspend or limit” entry to citizens of several countries.

However, the list is weirdly arbitrary; we do not limit Indonesia, which has a bad, albeit improving, Covid problem, or Malaysia, which has a lesser but significant one. By contrast, Vietnam and Japan have blanket bans, which are simpler to administer and harder to game.
As far as domestic travel in the United States goes, here’s a handy map of putative restrictions:
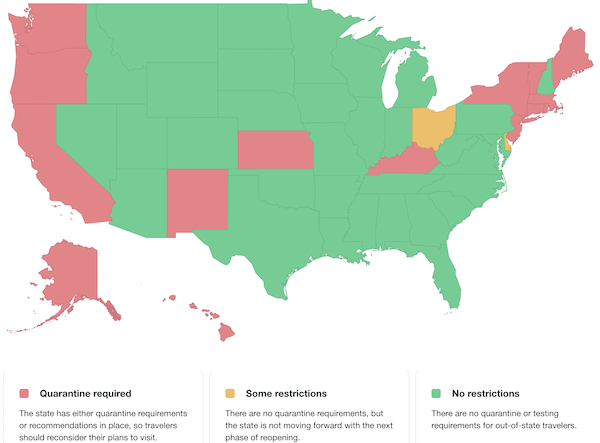
(Here is a list of state restrictions with detail in prose.) Hilariously, the restrictions bear no relation to variant spread whatever:
I would also like to hear from any readers who actually experienced travel restrictions moving from state to state. I would bet it’s all theatre. (Though you would think somebody would get the bright idea of “Covid Traps,” exactly like Speed Traps!)
Conclusion
So, here we are, with the more contagious and lethal B117 variant spreading. From the International Business Times, “Doctors ‘Pleading’ With Public As Air Travel Spikes For Spring Break“:
Public health officials are alarmed by spiking air travel rates, warning that Spring Break travel is premature at this stage in the vaccination effort. The winter COVID-19 surge was driven by holiday travel, and doctors worry that fair weather and vaccine progress could convince vacationers the pandemic is over just as variants loom, CNBC reports.
Air travel rates have reached their highest levels in a year, with one million TSA screenings per day since Thursday. That’s not as high as it was before the pandemic, but it is enough to concern health officials.
“I’m pleading with you, for the sake of our nation’s health,” CDC Director Dr. Rochelle Walensky said Monday. “Cases climbed last spring, they climbed again in the summer, they will climb now if we stop taking precautions when we continue to get more and more people vaccinated.”
Pleading! And we’ve seen the same pattern before: Success, followed by relaxation, followed by renewed failure. From the Guardian., “US experts warn new Covid variants and states reopening may lead to fourth wave“:
“Everybody’s focused on the big declines in the number of cases, pretending the plateau is not really substantive, and oblivious to the impact of B117,” a highly transmissible variant first identified in the UK, said Dr Peter Hotez, a vaccine researchers and dean for the national school of tropical medicine at College of Medicine in Houston, Texas.
The potential plateau, highly transmissible new variants, and decision to reopen when vaccines have reached relatively few people “has all the makings of a fourth wave, and gives me a lot of pause for concern,” said Hotez.
The Administration could, of course, have enforced 14-day quarantines for all international flights without exception:
We wouldn’t need to limit flights from overseas for fear of #B117 variant of #COVID19Aus if we had a nationally coordinated quarantine with consistent infection prevention control procedures. These should have been developed with the close oversight of National expert bodies.
— Dr Vyom Sharma (@drvyom) January 9, 2021
It’s too late to stop B117, but maybe that will stop the next variant, if it evades vaccines.
The Administration could, of course, still restrict domestic travel:
He could have ended air travel into and out of Texas and Mississippi as a warning to other states to stay in compliance with CDC requirements, it wouldn't be adequate, but it would be better than what he's done thus far.
But even that was too much for business interests.
— james_roe (@james_roe) March 15, 2021
There are 117 international airports in the United States. That means that there are 117 points to choke off the entry of the virus into the country by air. That’s 117 testing facilities, 117 quarantine facilities. That’s about half the number of facilities run by the country’s smallest hotel chain, Hilton Worldwide. It’s very hard to believe that the United States doesn’t have the operational capacity, or the money, to set up such a system. And yet nowhere in the political class, or in the public health establishment, are border controls and quarantine even on the radar. They go unmentioned. A failure to learn? A failure of imagination? Lack of nerve? Lack of desire? Rule #2 of Neoliberalism? The business of America is business, after all….
NOTES
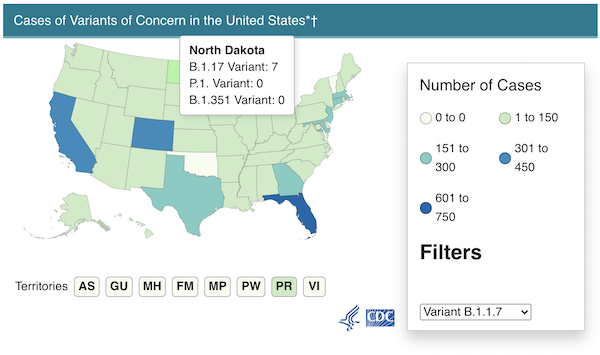
[1] More correctly, B.1.1.7 (lineage), a Variant of Concern (VoC) but that’s a lot of characters to type. Also, B117, for me, has a penumbra of lethal connotation, from World War II bombers like the B-17. B.1.1.7 has other monikers: 20I/501Y.V1, VOC 202012/01. Here is a handy chart:
Covid-19 – Highly contagious B.1.1.7 variant spreading fast in US even as total case stabilize.https://t.co/BRNIh5PCBt#COVID19 #B117 pic.twitter.com/2AgVNmpEBn
— Daily Market Pictorial (@MarketPictorial) March 13, 2021
[2] The paper was withdrawn by the authors for insufficient acknowledgement of the contributions of others, which I take to mean that the content is OK.
[3] In a more pandemic-riddled world, behavior like this might end up being a casus belli.


Preaching to the choir here, but the US – and the wider west is a FamilyBlogging joke … I remember this tweet shared on #NC to begin the year:
Foreign worker returned to South Korea and spent 24 hours in quarantine
We are led by the very worst people. Our lives are to labor and consume. And the state exists to support the plutocrat class.
Fin.
“We are led by the very worst people. Our lives are to labor and consume. And the state exists to support the plutocrat class.”
Yep.
Seriously, what’s the point anymore?
They don’t even hide it. “Objectivist’ Libertarians will tell you the only proper function of the state is to protect private property. Which ultimately means keeping your grubby little mitts of it.
“I would also like to hear from any readers who actually experienced travel restrictions moving from state to state…”
Spring Break…Weeeeee-whoop-whoop!
NYC has troops and staff at Penn and Laguardia who require proof upon reentry that you’ve completed a covid survey asking where you went and telling you to quarantine if needed. The sheriff then calls or texts you every few days to make sure you’re completing your quarantine. However, you can just say you are and then not do it without repercussion (at least so far)
They don’t require proof of a completed survey. My last 2 trips through Laguardia (both in 2021), there were National Guard in camo gear making speeches but not stopping anyone. Prior three trips (2020, on 2 the first 2 they were pretty serious about getting forms, the third not so much). And no one followed up with me, not once.
What I think is worse is NY also requires a negative Covid test w/in 72 hours. Zero checking for that.
We’re all vaccinated, 5 weeks after the second shot.
Arrival at Syracuse airport Friday required a completed form on a phone or hard copy. The NG asked for supplemenal ID. Tracers called the following day. Identical to travel experiences 4 prior trips. Official quarantine notice was emailed the day the tracer called.
Obviously one could lie on the forms.
On April 1 vaccinated persons will not be subject to quarantine. Not sure why that is a magic date…
“Live Free or Die” has become “Live Free and Die”. It’s doing this country in.
A shoutout to our experts – “We who are about to die salute you.”
Experts Experts, Choking smokers. Don’t you think The Joker laughs at you?
This issue is whether the powers that be are really prepared to give up international travel. They are their benefactors in many countries have little desire to do so.
Among the many disservices the WHO did at the start of the pandemic was its vocal insistence that shutting borders was not a solution and would hinder rather than help. That runs contrary to common sense and has been shown quite extensively to be incorrect. Compartmentalisation is an extremely effective control be that in a hospital, by household in lockdowns, by state or by country. Most countries who have stopped the virus have highly restricted international travel.
Of course such solutions are short term (initially short term was envisaged to be months, now its years). A long term solution is vaccine and acquired immunity effectiveness and allowing the virus to become endemic while minimising its impacts.
The COVID response across the world seems to have been and often still is lackluster and accompanied by a denial of realities. This has been a theme often even in ‘successful’ countries. In Australia there is zero community spread currently, but there is still plenty of misplaced optimism.
I believe Japan’s solution for the Olympics, if they are held at all, is to limit spectators to those in Japan, and keep the athletes quarantined.
Yes. International spectators have been barred:
https://www.cnbc.com/amp/2021/03/20/international-spectators-to-be-barred-from-entering-japan-for-olympics.html
I thought that news was so uncharacteristic of the Japanese – until I read this post.
I am behind on this, but on a practical level, is it best to assume the virus will become endemic? The purpose of a vaccine then is not to prevent you from becoming ill, but to lessen the effects if you do? Perhaps greatly decrease the lung damage among the majority of the stricken, which has been discussed on NC?
I think Lambert’s post aptly demonstrates that where there is a will, there is a way. It would be tougher for countries that have let the disease run rampant but my personal thought is that it is still within the realm of possibility.
2 or 3 weeks of very hard quarantine(40 days would be best), real track and trace, real border control.
If the non ACE2 strains take hold then there will be larger animal reservoirs for both cross species infection as well as a larger mutation space.
Quarantine during winter would have been best, I don’t think my fellow Americans will cede their freedoms for their health in any other season.
https://www.biorxiv.org/content/10.1101/2021.03.18.436013v1
Have fun vaccinating the mice!
Endemic is essentially guaranteed.
I don’t know that mice worry me that much. A mouse won’t generate enough viral load to infect a human.
But those NYC Norwegian rats, when they get a good diet, can become pretty hefty. They seem like a more worrisome vector to bigger critters. And I would assume mouse to rat isn’t that big a species jump.
Very likely Yves, that the jump will be pretty seamless, I’d suspect they are already carriers.
I’m no expert on the NYC rats, but the Chicago ones are fairly cat-sized as well. I’d be pretty surprised if they weren’t able to infect people from time to time.
Rodent vectors *could* be a very dangerous mutation laboratory depending on how rapidly they clear the virus.
The situation in continental Europe is identical as in the usa. I was surprised to read about community spread of both South African variant here very soon after it was discovered around New year
How did it get here? By air of course. But I thought international travel was restricted? No, there are no restrictions, and the few rules we have, like self(!)-isolation, are not enforced.
I really don’t understand why politicians don’t shut down international travel when most of society is shut down. It seems easy to do compared to shutting down schools, restaurants,…
i wonder if that question alone illuminates the answer…
The European situation is a mess – the irony is that it would have been better organised if Covid was an animal disease like Foot and Mouth, as there are much stronger transnational arrangements to deal with agriculturural diseases and pests. Animal movements are tightly controlled and monitored, people are not.
But realistically, its very difficult to know how you can isolate the EU as an entity. Not all countries are part of the EU and there are numerous open borders between countries within and outside the EU, and every country has different laws and operational capacity to address people coming into the continent. I’ve heard many stories of non Europeans picking the ‘easiest’ access point to travel and then taking buses and trains across borders to get to their destination. I know of one outbreak in the west of Ireland that came via Iraq via that method.
That said, they didn’t even try, it was clear that the political authorities decided early on that strong controls on movement into and around Europe (EU and geographical Europe) was not practical, and even stopping northern Europeans having their sunshine hols on the Mediterranean was politically too unpalatable. The second surge in the UK and Ireland (prior to B117) almost certainly came via Spanish holidaymakers.
All true, but I’d add that the “open borders” obsession within the EU governing class has also been a major factor. It’s so much an unquestioned norm that governments found their brains seizing up when they tried even to imagine closing borders. I forget which idiot it was who smirked that ‘viruses don’t have passports”, but in a just world he would have been taken out and shot some time ago.
Did someone actually say that? Wow. But then again, I’ve seen even some high profile virologists say things like ‘with proper precautions, there is no evidence to support stopping air travel’, to which I’ve always wanted to ask whether virus’s have wings to help them cross continents.
But to your point, yes, I think there was a real brain freeze at the idea of stopping travel within Europe. As I said elsewhere, I find it bizarre that the Irish government can deem it politically and ethically acceptable to limit people to within 5km of their homes on pains of a stiff fine, but not do anything except politely request people not to fly to the Med for their holidays.
A quick Google search (which I couldn’t be bothered to do before, sorry) brings up scores of examples, including academic papers and political speeches. Macron said something close to that, but, to be fair, it was in the context of the need for a common European approach, and the avoidance of “virus nationalism” rather than a remark about open borders as such. Here’s a corking example, though:
“there are disadvantages to travel bans, said Steven Hoffman, a professor of global health law and political science at York University who uses legal and public health expertise to advise governments on pandemics.
“They don’t work,” Hoffman said. “They undermine the public health response. They undermine trust in governments and violate international law in the process.” The reason travel bans and restrictions don’t work, he said, is that if people want to travel, they’ll find ways to do so. Instead, it’s best if people travel through “official channels” that can be monitored and made safer by identifying cases and their close contacts.
“Viruses don’t carry passports. They don’t respect border officials,” Hoffman said. “They certainly don’t prefer one country’s citizens over another.”
Because of course if you were trying to get from Spain to the UK and there were no flights you’d swim, wouldn’t you ….
I really wish someone would have given some of those people a copy of William McNeills book from the 1970’s ‘Plagues and Peoples‘. Its an extremely well known and widely read book, it was on my undergrad Geography course from long ago and I still have a much thumbed copy on my bookshelf.
Back this time last year, when I first saw that WHO wasn’t advising travel bans, I had a look through their website and the research they were quoting in support. It was astonishingly theadbare stuff, mostly research on border movements in Africa during ebola outbreaks. How anyone thought that this was relevant to covid* when there was literally several millennia of human experience that travel restrictions was an effective means of stopping pandemics defies belief. Among other things, I think it confirms that some basis in history education should be essential for every branch of science or the humanities (including of course, economics).
*oh wait, I forgot of course, it couldn’t possibly be spread through aerosols.
TBH, there were attemptes to close the borders.
I know that a year ago CZ, Poland, Slovakia and Hungary at least closed the borders (including stopping flights). Except it led to a bit (well, way more than a bit) of a problem, where very shortly they had to make exceptions for:
– trade (long distance freight)
– emergency services
– cross-border workers (say a lot of nurses in near-border German hospitals is from the Czech republic)
– a bunch of other people.
All of which were misused.
In practice, there was people-smuggling going on as well – we went for a walk near the German border and in the couple of hours we saw a few cars full of people clearly going over the border.
Technically, right now you’d travel only on business, but in practice every few weeks there’s a case of someone who got back from hols from wherever (like Zambia) bringing in a new mutation, so it’s not that well policed.
Good report this but there is not a lot to take hope in. Just last year during the first year of the pandemic, nearly 400 million people flew both domestically and internationally in and out the US which is about about 65 million more than the population of the United States itself. So as a vector for spreading any new variant of this virus, it will defeat most measures taken. I think that the only way to stop it is for each State to isolate and as each State clears itself from this virus, it can connect with another virus-free Sate but we all know that this solution will never work for the US if for no other reason than the number of States and the commerce between them all.
The focus is on the B117 right now but I wonder about the next variant coming down the pipeline – and the one after that. What if one emerges that is super lethal? As for air travel, maybe the CEO of QANTAS was right in saying that after people have been vaccinated, governments are going to insist on proof of vaccinations before international travelers are allowed to enter. And that this will supplement the expensive 14 day mandatory self-quarantine. Maybe that should apply domestically as well. In reading this post, I could not help but think of Max Brook’s novel “World War Z” and how the virus in that book spread. And the conclusion that I came to was that if there was ever a zombie virus, that we would not be any more successful containing such a virus much less the present Coronavirus-
https://thehill.com/policy/transportation/aviation/544237-qantas-ceo-governments-are-going-to-insist-on-vaccines-for
> I think that the only way to stop it is for each State to isolate and as each State clears itself from this virus, it can connect with another virus-free Sate but we all know that this solution will never work for the US if for no other reason than the number of States and the commerce between them all.
I think it would work. Air travel and especially mass air travel is a recent phenomenon. Certainly China is doing just fine without it, thank you very much.
I thought about it for a while but I do not think that it would survive a legal challenge because of the freedom of travel under US law. And I can’t see 50 States giving this right up either for the duration as it would be a huge power shift to the federal government which they may never be able to claim back-
https://en.wikipedia.org/wiki/Freedom_of_movement_under_United_States_law
I work at a restaurant that used to get a lot of international tourists. Brits, Germans, Italians, French, Spanish, Australians, Japanese. I haven’t seen a Brit, Italian, German, or Aussie in a year. Weirdly, still get some French, Spanish and Japanese. I ask myself how the f- did you get here and with your kids? There’s a year long international pandemic and you just had to come to Memphis to eat bbq? I haven’t eaten in a restaurant in a year, even though I work in one, yet you flew in a sealed metal can with a hundred people across oceans to eat here. Thank you, but Jesus just stay home.
My R&R old homie says I must have been watching late 20th century metal bands when I told him it’d be a cold day in Hell when I got into a flying aluminum death tube.
But please, do carry on with hand washing Kabuki, Hudson sprayer ballet, bleach wipe melodrama and all the other ritual virtue signalling so that WE CAN GET BACK TO NORMAL and as one red state harridan yelled, “….get these muzzles off our face.”
Be sure knock real loud on our bunker door, we’re watching old videos of how things used to be.
The U.K. only recently imposed hotel quarantine on travellers from “red list” countries but that still isn’t stopping these variants getting into the community. Here in our suburb of London, the South African variant has been detected supposedly with no travel links.
Something is not working. Are people lying about where they’ve travelled to avoid quarantine? Are people being infected while in transit as they mix with people from all different destinations?
Yeah that red list is a joke. No European country is on it, nor is US. But of course these scary African and South American countries are banned:
https://www.gov.uk/guidance/transport-measures-to-protect-the-uk-from-variant-strains-of-covid-19
Compare with current Covid rates:
https://www.nytimes.com/interactive/2020/world/coronavirus-maps.html
Nice work again from the country that gave the world B.1.1.7.
Still Flying = Total Fail
As for reopening schools, and three feet is the new six feet, what is a rational person to think when the so called experts are clueless or deliberately lying. If there are two students and a teacher in a classroom and one of them has covid, the other two have really high odds of getting it which violates jawb one – don’t get if and jawb two – don’t spread it if you do have it.
I do have to give the experts some credit though. They asked eclownomists what to do and they were told to assume a proper ventilation system.
Just some anecdotes – I’ve friends from Japan and Vietnam and China who’ve been trying to get home from Ireland for visits. Japan is quite straightforward – you have to quarantine and isolate, but it seems to rely quite a bit on individual responsibility, although the act of that British idiot will no doubt make them far more wary of non-Japanese. With possibly good reason, the Japanese government assumes its citizens follow instructions, but others don’t. I’ve heard that the treatment of workers from poorer countries like the Philippines is less gentle than for westerners. The government is desperate for the Olympics to be a success, but they’ve bowed to the inevitable and have barred foreign tourists for the period. Japanese Covid rates have undoubtedly been higher in the past than the’ve admitted, but the very strong community based health system seems to have done an outstanding job in keeping a lid on it over the winter. But they still have some confused policies – bars and cafes remain open, but they are banning outdoor sakura parties, which makes no sense to me.
Vietnam has been super strict and they’ve benefited from this. They are not gentle with people who choose to travel, and the quarantine hotels are apparently pretty awful. The assumption of rough treatment has been an effective way to persuade Vietnamese inside and outside the country not to even consider travel unless its absolutely necessary. My friends mother was supposed to visit Europe and Canada this time last year, but has not even attempted to revive her travel plans.
China makes you pay for the quarantine hotel which is a major disincentive to travel (don’t even think of making an exception). Most Chinese abroad that I know have opted to weather Covid in China rather than outside if they could afford to, for most, thats proven a very sensible judgement. Interestingly, the price of flights to China has stayed very high, while flights to Japan are very cheap, which I assume is down to the Chinese government simply stopping most routes to keep up capacity, while the Japanese have been trying to keep routes open for the Olympics. That does mean, I suspect, that flights to Japan won’t be packed, unlike Chinese ones.
Europe is, if anything, in an even greater mess when it comes to travel than the US. Geographically and politically of course Europe is a nightmare to control internally and externally. Many governments simply haven’t bothered. Travellers into and out of Europe are often picking the ‘weak spot’ as their entry/exit point.
Ireland has had a particular problem as while theoretically being an island is very useful, the situation with Northern Ireland and Brexit has made coordinating an island wide response to restrict movements impossible. But the failure of the Irish government to put in place stricter airport controls is inexcusable and probably mostly down to the power of the airline industry. It seems the Irish government can stop people travelling more than 5km from their home on a bike, but not stop them taking a Ryanair flight to Mallorca. Fear over the Brazilian variant seems finally to have forced action (there is a large Brazilian population here). Several cases have been identified and isolated at Dublin airport. This means, of course, that they weren’t identified and isolated at their transfer airport (there are no direct flights).
I’ve heard anecdotally from two medical friends that B117 came to Ireland not via the airports or border, but via the regular ferries to Britain before Christmas. There was a clearly identifiable pattern. The two previous outbreaks came via aircraft. The first, in February/March last year, was very strongly associated with upmarket school ski trips to Italy/Austria. The second smaller surge in October was associated with a Spanish variant (so far as I’m aware, it originated with agricultural workers in Spain over the summer), which was almost certainly brought either directly or via the UK from people who insisted on taking summer breaks to Spain against advice.
Anyone who paid any attention to the epidemiology always knew that air was THE transmission vector, because it’s too fast to be stopped effectively for highly-transmissible diseases.
I have seen some studies on how bio-terror could be essentially unstoppable because of the air routes, the only problem (for the terrorists) was that there was no “good” pathogen. CV has many bits of the right pathogen (aerosol spread, high infectability rates), but is not deadly enough.
I really wish I’d kept a record of the link, I can’t find it now – but around this time last year I saw a study from Singapore on an early office outbreak. It was entirely obvious, even to an amateur like me, that only aerosol transmission could have created the pattern seen (essentially, one half the office along one side of the building caught it, the other didn’t). Or at the very least, the spread made no sense if it was caused by droplets and/or hand contact, there had to be something else at work.
The failure of medical authorities to accept this evidence for many, many months is inexcusable (and there are still very influential holdouts, not least WHO itself). I’ve linked below a great twitter thread on this subject.
There was an early outbreak in a Singaporean bank – I think this is what you remember – but the striking anisotropic pattern of infection that ruled out ballistic droplet infection in favour of long-distance airborne infection was the outbreak in a South Korean call centre, which came with a handy seating plan of infection down one side of the building in the air currents but not the other.
https://wwwnc.cdc.gov/eid/article/26/8/20-1274_article
Incidentally, here is a report on an nice piece of research tracking 59 infections from a single flight into Ireland from a Middle Eastern hub airport last summer.
Just to add to the other excellent links above, there is a very interesting twitter thread here from Deepti Gurdasani also check the embedded tweet from Jose-Luis Jimenez.
Its become increasingly clear that the failure by WHO and broader public health authorities in the West to accept the evidence that Covid is spread primarily, if not exclusively, by aerosol was a catastrophic error, and the failure to admit this error is costing thousands of lives. Trisha Greenhalgh in particular has been fighting this fight since the beginning and has gotten nothing but grief from the scientific establishment over it. She’s been proven right.
The belief that “respiratory diseases were spread by large infected droplets through person-to-person contact or contaminated surfaces” has remarkable persistance in view of the growing antiquity of classic studies proving otherwise:
“Air Hygiene in Tuberculosis: Quantitative Studies of Infectivity and Control In a Pilot Ward”, Richard L. Riley, et al. (Received for publication November 28, 1956) [first page accessible at: https://www.atsjournals.org/doi/pdf/10.1164/artpd.1957.75.3.420 ]
“Aerosol Transmission of Rhinovirus Colds”, Elliot C. Dick et al.(published 01 September 1987) [available at: https://academic.oup.com/jid/article-pdf/156/3/442/2412440/156-3-442.pdf ]
If the CDC and WHO are “following the science” — what science are they following or perhaps science of what vintage? The results of the experiment reported in the rhinovirus paper should be hard to ignore.
A lot of these gain-of-function mutations like B117 have probably [almost certainly] arisen multiple times, independently of each other, in a variety of places around the world.
If that is the case, travel restrictions might have slowed, but would not have stopped, the spread of B117, P1, et al — for the simple reason that these mutations are not one-offs, but rather are the result of the virus doing it’s natural evolutionary thing.
The good news is that this virus may have pretty much exhausted it’s range of possible gain-of-function mutations, and if that is the case, the end of the road for the virus may be getting nearer.
Governor Ron Desantis has been refusing to release data about the presence of covid 19 variants in Florida, the number of cases and the locations. Local newspapers have had to sue his admininstration to get access to that data, just as they did to get access to the weekly White House Covid 19 Task Force reports that were issued to each state. These reports often contained urgent warnings and suggested pandemic mitigation strategies that ran counter to Desantis’s reopening agenda. They were meant to be taken into consideration and shared with the public. He recently held a livestream broadcast of a covid 19 roundtable discussion with the authors of the Great Barrington Declaration. It was a self congratulatory celebration of victory over the pandemic, praise and a unanimous acknowledgment that his management of it was an outstanding success. It was support and vindication for what he’s been doing and saying, and a doubling down on all the elements of the herd immunity approach. Some of the statements made and conclusions reached; Masks don’t prevent the spread of covid 19 and they may even be harmful. Contact tracing is of no value. Lockdowns have been a complete failure, causing far more harm than good and Sweden is proof of that because, among other things, the number of covid 19 deaths they had is low compared to the U.K. There’s much more of the same in the discussion. I find it extremely appalling and don’t understand how such behaviour is seemingly taken in stride.
One thing that the pandemic has shown us is the quality of our elected officials. Those that are more geared toward people are certainly different from those who think that the economy is the most valuable thing on earth. It is a real eye-opener!
Yes. As our Humble Bloggers like to say, these times have been clarifying.
I think this comes from an old Nova on pandemics. I thought it was mildly interesting that a gene inherited from crossbreeding with the Neanderthals has given some europeans/descendants a natural immunity to the black plague. And then I thought about how long it might take to develop such an immunity without inheriting it. (After all the black plague is still with us, compliments of prairie dogs usually.) The “immunity” would come from both sides, both a virus that is all mutated out and more or less dormant, and the species that fought the same battle genetically over centuries. And then I got sick thinking about not just the centuries but the millennia involved. Because the Neanderthals would have interbred with modern humans for tens of thousands of years in the middle east and then in southeast Europe… before. Before the black death struck the Europeans beginning in the 7th C. with Attila and successively countless times after that; eliminating people who could not fight it. Century after century. So it is somewhat reassuring that, even though I don’t like the idea of genetic engineering, it’s nice to know we can actually do it. I only hope we are very very careful. It would be foolish, imo, to get too enthusiastic like the Israelis did a few years ago when they claimed they now had the science to eliminate all viruses. Not sure the context of that claim. But I am sure we’d soon find out that it’s just not a good idea to eliminate “all” the viruses.
In my experience, the US travel restrictions have been on the honor system, with some government follow-up.
I flew to Denver from Newark and back last October, the information I voluntarily gave up eventually made its way to the county Public Health Department, with one follow-up phone call.
Compare this to my experience in Taiwan and Hong Kong during non-pandemic times, where the customs and immigration forms had health questions, and the airport had temperature screenings and would pull people aside for follow-up.
I have a friend who moved to Taiwan beginning of this year, with his spouse and three kids. Took a few months to get the visas, as none of them are Taiwanese nationals, though his parents are. All of them quarantined in the designated hotel for two weeks. They got daily checkups, three meals delivered per day, and welcome/goody bags.
my husband and i flew nyc to rome today. we had to have rapid tests 48 hours before flight in order to board at jfk and were again tested (rapid) on arrival in rome. everyone flying into fiumicino is tested, even before going through customs. (i can’t testify about domestic flights.) you sit and wait for results before proceeding to customs and baggage claim. most flights are italian citizens, of course; we qualify for entry as residents. i was impressed with how there were no options but to be tested. we saw only one woman sitting apart in a booth looking dejected who may have failed. i wish i’d asked statistics on failures but was too impatient to get ‘a casa.’
we’d been vaccinated over a month ago in nyc but this would not get one exempted from any of the testing.