By Lambert Strether of Corrente.
Things are more like they are now than they’ve ever been before.” –Dwight D. Eisenhower
Carpe diem quam minimum credula postero. –Horace
While I support WHO’s standardization of a Covid variant naming convention — the logic is the same as using human-readable URLs, and not incomprehensible numeric dotted quads — I could wish they had not selected the Greek alphabet for their pool of names; every time I hear the name of a variant, I’m reminded of fraternities and sororities. Unlike the hurricane naming convention established by the World Meteorological Organization, WHO’s greek letters have, as it were, no nutritional value. If Delta was named Dennis, we could be making headline jokes about “Dennis the Menace,” for example. Life would be a lot easier. Having gotten that off my not cough-ridden chest, I want to take a look at the Delta variant (née B.1.617.2), first detected in India. The British Medical Journal explains how Delta differs from previous variants in structure and fitness:
What is different about the delta variant?
In some ways the delta variant is an “improved” version of the alpha variant, making it more easily transmissible and more of a concern.
Speaking at the Science Media Centre briefing, Wendy Barclay, professor of virology and head of infectious disease at Imperial College London, explained, “The delta variant has got two important mutations in its spike protein, or sets of mutations. One is at the furin cleavage site, which we think is quite important for the fitness of the virus in the airway. The virus that emerged in Wuhan was suboptimal in that respect, so it transmitted, but perhaps not as well as it might. The alpha variant took one step towards improving that with a certain mutation, and the delta variant has built on that and taken a second step now, a bigger step, towards improving that feature.”
Why is delta able to transmit more easily?
Barclay said that the current data indicated that the virus was “fitter in human airway cells,” meaning an increased amount of the virus in the infected person, and so they may expel more virus out into the air to pass on to the next person. This is supported by the testing data, which show that the CT value (cycle threshold)—the number of amplification cycles needed for the virus to be detected—seems to be lower in samples from delta infected people, meaning they contain more virus.
Another suggestion is that if this variant is better at infecting human airway cells, people may become infected after a lower exposure.
In this post, I’ll wrap up what I was able to collect of what we know about Delta so far. (We don’t know about things that take time to develop, like Delta and long covid, or Delta and fatalities). First, because I’ve tended to bring Covid content down to actions I personally can take, I’ll list Delta’s new symptoms, present some worrying anecdotes, and discuss my personal practices. Then I’ll discuss how Delta spreads, including transmissibility, severity, and vaccines. Finally I’ll ask: “What’s the plan?”
Personal Practice
Importantly, Delta symptoms are different from those we are “used to.” From Medical News Today:
[D]ata from the ZOE Covid Symptom Study — whose scientific analysis is conducted by experts from King’s College London — suggest that the main symptoms of infection with the delta variant are headaches, a sore throat, and a runny nose.
This is a change from official information on COVID-19 symptoms — such as that provided by the U.K.’s National Health Service (NHS) — that lists fever, continuous cough, and loss of smell or taste as the main symptoms of the condition.
Prof. Tim Spector, co-founder of ZOE, warns that SARS-CoV-2 infections are “acting differently now, […] more like a bad cold,” which may tempt people to dismiss the symptoms.
“It might just feel like a bad cold or some funny ‘off’ feeling — but do stay at home and do get a test,” he urges.
(“Do at home and do get a test.” Easy in the UK! In this country, testing is free, except when it isn’t, and treatment is not.) There are worse symptoms in India, not mentioned elsewhere:
Hearing impairment, severe gastric upsets and blood clots leading to gangrene, symptoms not typically seen in Covid patients, have been linked by doctors in India to the so-called delta variant.
Regardless, the really distinctive symptom — loss of smell or taste — is now gone, and symptoms that are “more like a bad cold” are uncomfortably close to an actual bad cold or the flu (which doctors predict will increase now that we’re abandoning masks). People are going to be reluctant to get tested for a case of the sniffles. It’s all the more unfortunate that Delta can comes on faster, at least in China, so there’s less margin for error:
China has uniquely detailed data, however, because it has essentially universal testing in the vicinity of outbreaks, allowing officials to gather detailed information on the extent of cases.
Up to 12 percent of patients become severely or critically ill within three to four days of the onset of symptoms, said Guan Xiangdong, director of critical care medicine at Sun Yat-sen University in the city of Guangzhou, where the outbreak has been centered. In the past, the proportion had been 2 percent or 3 percent, although occasionally up to 10 percent, he said.
And now to the unsettling incidents. Sadly, we have no Delta-specific epidemiological studies, so anecdotes will have to do. First, a hospital in Calgary, Canada:
At the [Calgary’s Foothills Medical Centre] hospital, 16 patients on two units — as well as six health-care workers — have tested positive for the delta variant.
Six of the patients and five of the health-care workers received two doses of the vaccine, while seven patients and one health-care worker had a single dose. All of those infected were vaccinated with an mRNA vaccine…. “[I]n the case of these two outbreaks, only one of the 22 people have required ICU care,” Williamson said in an email. “The majority of both patients and healthcare workers have experienced mild symptoms.” Lynora Saxinger, an infectious disease expert at the University of Alberta, said it will be important to see what the investigation into these cases turns up.
“The things that I’m considering right now are that, a hospitalized population isn’t necessarily representative of the general population,” she said. “Some of that number might be people who would be at really significant risk of having a suboptimal vaccine response because of their medical condition.
I understand Saxinger’s point that hospital populations are not representative (although if I were actually hospitalized that would be cold comfort). Nevertheless, a hospital cluster is disturbing. How did the virus slip past disinfection and ventilation defenses?
The second incident, from Australia, is even more disturbing. From 7News:
A ‘fleeting contact’ has prompted NSW authorities to reintroduce masks across Greater Sydney as one new case of COVID was detected overnight.
The new case was detected in a man who attended Myer [department store] in Bondi Junction on June 12 at the same time another case visited the store.
The first man who tested positive was revealed to be a driver who transported an international flight crew….
NSW Premier Gladys Berejiklian said preliminary advice suggested the new infection may have been transmitted through “fleeting contact” between the man and the driver.
The driver’s infection is deemed to have been “highly infectious”, as he also passed on the virus to a woman who had been sitting outside at a cafe in Vaucluse.
“This indicates that the initial case was highly infectious, as transmission must have occurred through fleeting exposure, noting that the person who caught the infection at the cafe was seated outside and there was no known on-site contact with the initial case,” Chief Health Officer Dr Kerry Chant said.
“Obviously, we cannot rule out that there were some crossover when they were ordering or other things, but again we are highlighting that we have observed these transmissions in settings where we would normally see outdoor dining as a lower risk setting and we would normally see shopping centres as a lower risk setting where you are unlikely to have close contact.”
The driver has the Delta strain of COVID, Chant confirmed on Thursday.
This is an anecdote, not an epidemiological study. Nevertheless, Australia does not have the noise of community spread, so signals are a lot easier to detect, as in another “fleeting contact” in a quarantine hotel, determined to be airborne transmission. So, although video evidence (as in this restaurant case) will probably give us a definitive answer, what we have here looks like a case of outdoor transmission of Delta, which may change a lot of people’s calculations about risk.
As far as my own personal practice, I don’t intend to become the breakthrough poster boy, so I don’t see a reason to change anything for Delta (masking outdoors, Vitamin C, Vitamin D3, povidone following human contact, and Ivermectin as a prophylactic; plus social distancing (and don’t @ me on any of this, unless it’s Delta-relevant)). I use N95 masks (and for those of you who don’t, I’d recommend you up your game and lay in a supply.) The only thing I might do is buy a CO2 meter, for my living quarters and for the rare times I need to be in other enclosed spaces. I will also be more conscious about looking for working fans and outside air — or at least high ceilings — in any other space I enter. We don’t know anything new about Delta surface transmission, so I will continue my non-obsessive cleaning.
How Delta Spreads
Here is a handy chart from Public Health England; I’ve helpfully highlighted the salient sections:
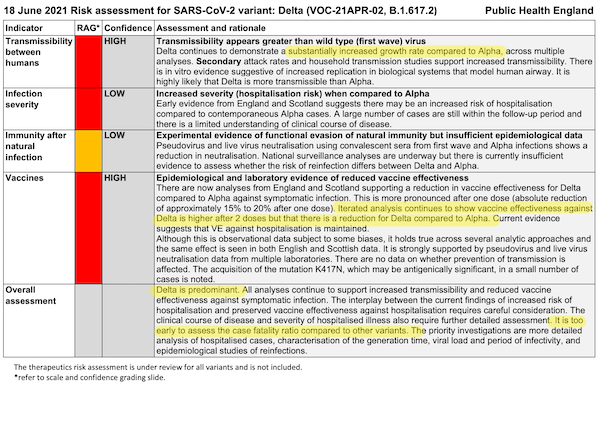
Let’s take each of these sections in turn (sklpping “Immunity after natural infection” and “severity” for “insufficient evidence”).
First, transmissibility. Delta has a higher R0. From BBC:
The cleanest way of comparing the pure biological spreading power of viruses is to look at their R0 (pronounced R-naught). It’s the average number of people each infected person passes a virus on to if nobody were immune and nobody took extra precautions to avoid getting infected.
That number was around 2.5 when the pandemic started in Wuhan and could be as high as 8.0 for the Delta variant, according to disease modellers at Imperial.
(I cannot run down where the 8.0 figure comes from; the Imperial College Delta study I can find has R0 at 1.44. Public Health England’s Dr Susan Hopkins suggests 7.0). Eurosurveillance, if I read this chart, proposes a lower R0, but still higher than any variant so far enountered:
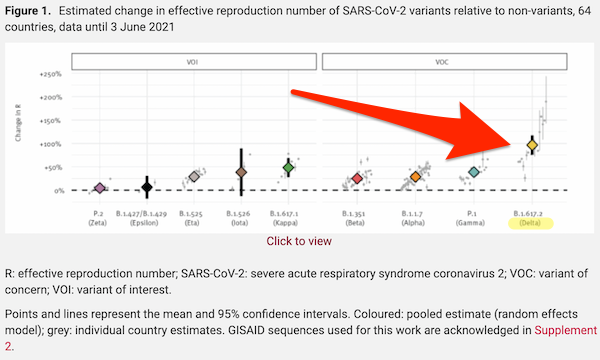
All agree that Delta is more transmissible. As a result, Delta dominates where it is introduced. Eurosurveillance once more:
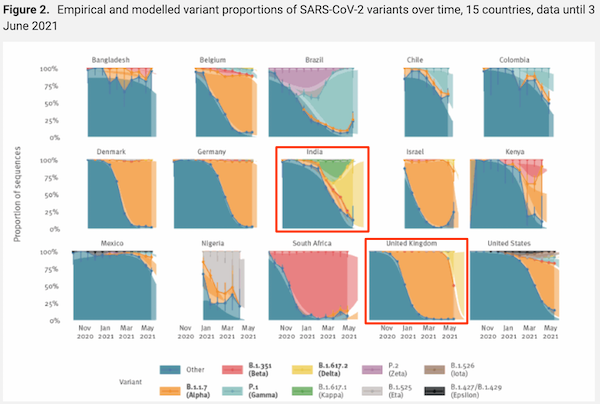
Delta has been spotted in 74 countries, including the United States, where it’s doubling every two weeks. In some Western states, Delta may be responsible for 29% of cases.
As a result of Delta’s increasing dominance, the horizon of herd immunity may recede still further. From Deutsche Welle:
Adam Kleczkowski, a professor of mathematics at the University of Strathclyde in Scotland, likens “herd immunity” to a forest fire running out of dry wood. When there is not enough left to burn, the fire runs out of fuel and disappears. When enough people are resistant to the coronavirus, either through infection or vaccination, the virus cannot spread, and the pandemic stops growing and starts to decline.
The faster the virus spreads, the greater immunity it will take to slow the infection rate. “That shifts this number up. We might need as much as 85% immunity to slow the Delta variant,” Kleczkowski said.
But, he points out, percentages such as this are only estimations. “They are based on limited data. It is not completely clear what percentage we need to reach,” he said.
More disturbingly, Delta is behind a surge among youth in the UK:
Young people are behind the surge, with a 5-fold higher rate of COVID-19 test positivity among children 5 to 12 years (0.35% prevalence) and adults 18 to 24 (0.36% prevalence) than in those 65 or older. People younger than 50 were 2.5 times more likely to be infected than older people (prevalence, 0.20% vs 0.08%), although the researchers noted that infections seem to be growing at a comparable rate in both age-groups.
Second, vaccines. From the Lancet:
Considering the whole population cohort (rather than just hospital cases), the test-negative analysis to estimate vaccine effectiveness in preventing RT-PCR-confirmed SARS-CoV-2 infection showed that, compared to those unvaccinated, at least 14 days after the second dose, BNT162b2 (Pfizer–BioNTech vaccine) offered very good protection: 92% (95% CI 90–93) S gene-negative, 79% (75–82) S gene-positive. Protection associated with ChAdOx1 nCoV-19 (Oxford–AstraZeneca vaccine) was, however, substantial but reduced: 73% (95% CI 66–78) for S gene-negative cases versus 60% (53–66) for those S gene-positive (appendix p 6). These estimates were obtained from a generalised additive logistic model adjusting for age, temporal trend when the swab was taken, and number of previous tests using splines plus sex and deprivation. As there was a trend in vaccine uptake and a trend to increasing Delta variant, the temporal adjustment with a general trend might not fully account for these changes. Also, no formal significance test to compare the vaccines was done.
So, at least not a vaccination debacle. Now, what are we doing about all this?
What’s the Plan?
Molasses-brained CDC, naturally, only declared Delta a variant of concern 30 days after WHO. Meanwhile, just when Delta starting to surge, the Federal Government and the States are systematically dismantling Non-Pharmaceutical Interventions and public health measures generally, when (as of June 16, only 44% of the population is fully vaccinated). Some might view these decisions as sub-optimal. From the British Medical Journal:
Does delaying the easing of covid-19 restrictions make a difference?
Yes, because it allows more people to receive two doses of the vaccine. Barclay said, “Any delays, just from a purely scientific basis, will help, because they will allow more time for people to get the second dose. And also just having the second dose is not quite enough. You need to get around seven days after the second dose for the vaccine to really boost the immune response up to the levels that you’d like it to be.”
The final stage of lockdown easing in England, which had been expected to be on 21 June, has now been delayed to 19 July.
One member of the NC Covid Brain Trust comments:
Once again, I have no idea what the plan is here. Fauci and Co. are not idiots, they have overseen the study of these viruses for decades, they know what is coming. Which means that it has been communicated to the politicians too.
So what happens when the booster campaign has to start due to the ICUs starting to fill with fully vaccinated patients, and when the even more lethal future strains appear, I have no idea. Current messaging is one of complete and final victory.
Pass the Victory Gin, I suppose. Around the non-functional but theatrical plexiglass….


“Gamma”
https://news.google.com/articles/CAIiELiBkMy1o6J5F3dLXP6XHk0qMwgEKioIACIQpzoRSNLEm6QR–MasMLSAioUCAoiEKc6EUjSxJukEfvjGrDC0gIw1anKBg?hl=en-US&gl=US&ceid=US%3Aen
I’m not sure “fortress vaccine” is as non-debacle-ish as is alluded to above:
https://www.nbcboston.com/news/local/more-than-500-breakthrough-infections-reported-in-mass-in-under-3-weeks/2406851/
More Than 500 Breakthrough Infections Reported in Mass. in Under 3 Weeks
Especially considering that we’re being actively told NOT to test vaccinated individuals…
https://www.msn.com/en-us/news/topstories/cdc-says-that-fully-vaccinated-people-no-longer-need-to-be-tested-for-covid-19/vi-AAKl4KC
CDC Says That Fully Vaccinated People No Longer Need To Be Tested For COVID-19
Like the FAA, it sure seems the NIH, FDA and CDC are happy to fly the public into the ground so long as it supports the industry they “regulate”.
Ever watch Dan Gryder’s YouTube videos? He’s a retired Delta Air Lines pilot and is an air safety advocate. Suffice it to say that he is no fan of the NTSB. He proves it through his air crash investigation videos.
You may want to look more into Mr Gryder’s past as far as newspaper articles and pilot forums.
“Gryder got to the end of the runway and attempted to take off, but he was out of gas.”
Thanks. Now it’s time for Slim to rethink Gryder’s perspective on things.
No worries. I have some history dealing with alarmists in the FAA, pilot and technicians groups and can recognize their personalities. I enjoy working with the quiet professionals in the three groups (and the aircraft manufacturers) who try to find a way to expediently correct a perceived safety problem once it has been recognized. It is not a matter of hiding a problem but fixing it or mitigating it before anything else happens after the fault is identified, even if it means grounding airplanes until correction.
Some famous quote from a some military NCO: “You, you and you panic. The rest of you follow me.”
One member of the NC Covid Brain Trust comments:
Once again, I have no idea what the plan is here. Fauci and Co. are not idiots, they have overseen the study of these viruses for decades, they know what is coming. Which means that it has been communicated to the politicians too.
The plan is obvious. Profit, rinse, repeat. Though, Kary Mullis was quite clear in his interviews that he thinks Fauci is an idiot. I suspect he was more correct than people would like to admit.
Fauci is a clever criminal. He’s been working this grift since the AIDS days. Forgot he was assocaited with that? You got cancelled once upon a time for suggesting HIV was not AIDS. “Household contacts can transmit AIDS,” is what he said. Remember the panic that ensued? The hysteria? Here we go again.
Just how are they not idiots? Just how is Fauci clever? From the little I understand, we have gotten a good setup for a very infectious, truly deadly variant that will undo all past efforts. If they were truly honest about the risks, and about what needs to be done, not only would there be greater success in dealing with the disease, people would likely accept any failures.
This bs not aerosol transmission, don’t use Ivermectin, forget about financial assistance, and so on, does no good. It doesn’t even put off a reckoning by much. People will lose whatever faith that they have left and get angrier, if that is possible.
Well . . . what if that was the secret goal, in furtherance of the secret agenda? “Clever” does not have to mean “good” or “ethical” or “moral” or “honest”.
But that is just it, I cannot see how it might be good for any secret agenda, unless it is to unified the majority of the population in disgust, hatred, and rage, thereby causing the possible civil war we are all worried about.
Perhaps, it might be useful in something like short circuit any possible resistance preparations, the destruction of modern civilization, or start something for the business opportunities, or some other crazy, whacked nonsense, but then the like deadliness and evasiveness of a the possible Hell variant would be dangerous to everyone. I don’t think you can make a vaccine for something that doesn’t exist yet. Although if one was willing to live or be quarantined in an environmentally sealed habitat for who knows how long they might be safe.
Yes, I know that I am really focused on this, but unless it is just some nihilistic love of the Evilhul, I am honestly baffled. Maybe we need the The Shadow: “Who knows what evil lurks in the hearts of men? The Shadow knows!
I come back to the question I have asked every now and then for the last couple of years . . . if the Global Overclass wanted to reduce the human population by 7 billion people or so over the next 100 years and make it look like fate or an accident, what methods might they use?
I would “just” raise the living standards and status of the worlds women. The more discretionary freedoms a women has, the less babies she will have.
Failing that, affordable sex bots that cooks and cleans would be my fallback.
The Problem with culling the population with a pandemic is that maybe it is not the people one needs to have around to adjust ones “smart” exercise bike and head freezing facility, who will survive in the end. Maybe those people who can take the most virii and prosper, they became like that through 60 years of civil wars and living in sewers with no infrastructure and that lot will just nick ones stuff and then cook a gnarly meal with ones liver?
In my experience, there are some organisations, where the dumbest of the dum-dums will rise to high power, simply because they are so stupid that they cannot be bored to despair with those many-people project meetings featuring 1h-per-person, bi-weekly, PowerPoint presentations over ones latest “achievements” – those “results” always measured in effort and never in deliverables – that is the “essential product” of the organisation!
They have Infinite Stamina, everyone else will leave, or get serious about their substance abuse to get through each day. When the slot opens, they are right there, spry and fresh!
> A clever criminal
W. H. Auden, “September 1, 1939“:
Clever, but not sapient, let alone wise
We’ll, Biden has vowed no new lockdowns, especially as the midterm calendar is approaching. Further, he also said that if you are fully vaccined, “the delta variant is unlikely to result in anything.”
Apologies, I cannot li l to the Yahoo news article. I got it from drudge but is is now whacky.
First, thank you Lambert for assembling the article. I liked how you broke it down, what we know, with discussion of the anecdotes as well (yikes that Alberta hosp.), and finally what’s the plan.
That last section might be divided between “what is the best plan for us as individuals?” and “what is the plan of pharma, the cdc, et al?”
Well, looking first at the latter, it appears that (here in the Usa anyway) all the public health chips have been bet on vaccination. Not surprising and consistent with many other decisions (like approval of the new alzheimer drug), and private for profit vs public health care systems. What’s that mean the plan is for the Fall when it’s flu season and Delta is predominant? 1. Booster shots. 2. shots for children 3. Much illness and deaths among the unvaccinated, and those with weak immunity (80+ in long term care?).
Let’s hope Gamma (nee P2) and Delta don’t evolve. And what is that new variant that is growing in Brazil?
On effectivness vs Delta, I found a study by Public Health England and published in the Lancet, reported in greater detail by the Guardian here:
Key findings for Pfizer (currently the most effective vaccine): protection against Asymptomatic and symptomatic is down to 79%. Vs Symptomatic alone is 88%, vs hospitalization, w 2 shots and 2 weeks, is 95%, and against mortality is “expected to be promising”.
Personally, I’m not throwing out my n95 masks or air filters. And I do find the CO2 monitor useful.
I predict here in the Usa the hesitant will be getting their shots come fall, hopefully not to late.
With the variants incubating in the population (including the 21%+ of vaccinated ), what will be the outcome for those countries with little vaccine available?
As you noted, the U.S. again has thrown all its weight into one Covid solution (let’s call it Plan A) with no consideration of a Plan B.
This has been our country’s great downfall of late, assuming that our great plan will work out with no Plan B in mind.
The whole of the Iraq War was one plan–get rid of Saddam, democracy appears. Hence, we’ve been stuck in that war for nearly 20 years. Afghanistan was virtually the same predicament–kill Bin Laden, crush the Taliban, democracy appears. Never once do we consider, “what happens if Plan A doesn’t work out?”
If I learned anything new from the Iraq and Afghanistan wars, it’s always have a Plan B.
I think you are misinterpreting Plan A.
Plan A is let ‘er rip through the unvaccinated, blame them for the problem, scare some into getting the vaccine, rinse, repeat.
If that’s the plan, there is no need for Plan B.
Note: as with drone strikes, there may be some collateral damage, but we just write that off as part of the deal and pretend they were unvaccinated.
We are governed by Underpants Gnomes
Emergency management and the powers related to are largely left to the states, so President Biden is not going to announce a lockdown, even if he wanted to if he doesn’t have the power to implement it on a national level.
Secondly, there are also political considerations–people are not going to tolerate lockdowns in perpetuity, especially if they cannot work from home and are not considered essential–in other words, those who stand to lose their livelihoods in a lockdown.
It doesn’t help that state unemplyoment systems and small business asisstence have been plagued by problems–they have been hit by rampant fraud while legitimate applicants can’t get the help they need in timely manner.
Most governors and other officials, including in Blue States, know full well the hardship lockdowns create–shutting down business literally takes people’s livelihoods away–and are only going to reimpose them as a last resort: i.e. if there is a danger of hospitals overflowing and the medical system collapsing.
I’m still disturbed by IM Doctor’s statement a couple of days ago that for the past two weeks, the only patients of his that had caught covid were ones who had been vaccinated. And that none of his unvaccinated patients had caught covid in that time frame.
There would surely be a disincentive to track vaccine breakthrough cases if this is a thing. If people could track infection rates in the vaccinated versus infection rates in the unvaccinated side by side, they might find out that the vaccines make people more likely to catch the new variants (but perhaps not be made as badly ill, at least for now). I take it that that would count as ADE. This is pure speculation on my part; I am no expert at all; I would love to be corrected if what I wrote is flawed.
I’m sticking with Ivermectin; my plan is to wait til the turn of the year to see if ADE shows up. Of course without data, maybe I won’t be able to tell.
Question for you both you and Lambert (That you probably can’t answer on the internet, but…). How are you getting Ivermectin? The only medical group in my region has been forbidden from prescribing, even though many individual practitioners don’t agree. Are local doctors giving this to people prophylactically?
Yes, how do we get this stuff? I see it’s readily available for animal usage. Is this what people are using?
Eeeeh…I think that is compounded differently? Not sure. It’s not recommended.
Of course it’s not recommended, per the helpful Google search engine; what is recommended is that you get the vaccine. Trot right in; they’ll give you a Krispy Kreme as your reward.
look of FLCC website…they have resources
https://covid19criticalcare.com/guide-for-this-website/how-to-get-ivermectin/
The FLCCC folks have really been at frontline of treatment since March of last year
Related ..
Monday, June 14, NIH Treatment Guidelines Panel changed their recommendation on Ivermectin from “against” to “neither for nor against”.
I am aware of several provider groups who had previously stated they would prescribe if/when NIH no longer recommended against. In theory, all US doctors “should” be more open to prescribing under modified guidance. And this is a step towards FDA emergency use approval.
Had the WHO consulted me, I would have suggested they use Roman emperors for the names instead of the Greek alphabet. We would currently be discussing the symptoms and spread of SARS-CoV-2: Claudius, and hoping the next one down the list doesn’t live up to its namesake.
Why not name these strains after incompetent leaders during this pandemic? So you could say ‘Man, I thought that the Trump strain was bad but the Boris strain is even worse. And the future incoming Bolsonaro strain is guaranteed to be even worse than that!’
That outbreak in Sydney is concerning as not only has it spread through ‘fleeting contact’ but because the Premier of that State – Gladys Berejiklian – has the same policies of fighting this virus as that of the Prime Minister. A sort of ‘Nah! it’ll be fine’ approach with an insistence that no matter how bad infection rates are in a neighbouring State, hers must always remain open. As well, ‘Ms Berejiklian yesterday urged people living in the eastern suburbs to modify their behaviour but has stopped short of adding restrictions to gatherings or mandating masks.’ Yeah, masks are a quick, cheap, immediate way to help slow any spread of this virus but she does not want to do that because reasons. I am at present looking at Sydney with a lot of concern as not only am I from there originally but I can see that it will not take much to have a massive outbreak due to dud leadership-
https://www.abc.net.au/news/2021-06-18/nsw-covid-next-steps-after-sydney-outbreak/100223740
This virus does not give you a break nor does its younger Indian cousin. But after 18 months of this pandemic, far too many leaders and medicos still have not learnt this lesson. Too busy trying to talk up their portfolios I guess.
Thanks for your list of personnel practices. Due to the purposeful lack of off-patent drug treatments, no cheap universal tests, inadequate contact tracing, and no comprehensive stage 3 trial surveillance of the mRNA injections, the future is very murky, indeed. Keeping isolated is not long term solution but is the only one readily available to Americans, if they can afford it, other than the jabs.
It is quite incomprehensible after the deadly public health debacle to date that the CDC, NIH, FDA and the White House are now doing victory laps. They are using every trick in the book, except the truth, to try to raise the percentage of Americans vaccinated. It must be that the meritocracy is so wedded to identity politics to divide and rule, they cannot see anything beyond their own propaganda. If the mRNA vaccine campaign fails to sterilize the variants, and with no Plan B, and with the undercurrent of unrest in air travel, urban shootings, and Portland Oregon; these all indicate that another lockdown next winter will tear the USA apart.
The meritocracy seems to be the quickest and the loudest when it comes for calling for lockdowns, perhaps because they don’t stand to lose their livilhoods–many of them came work from home–whereas for many others it’s a bit more complicated.
At the same time there is no guarantee there will be another lockdown. Between the hardship lockdowns cause and the mess that was unemployment and small-business assistence programs–these system were hit with fraud while legitimate applicants struggled to get help in time–there may not be the political support in the United States for any more.
I’d say the odds of more lockdowns in United States are low unless things not only get worse than they are now but reach a point where there is a risk of the medical system collapsing.
I detect a switch, the pro-lockdown posture was a set up to promote vaccines, make it as miserable as possible with the vaccines as the path to freedom, now that there are vaccines, the incentive switches, and they will be extremely loathe to lockdown the vaccinated.
Has anyone heard anything about how Ivermectin has performed against the Delta variant? I remember that Ivermectin was approved as part of the treatment protocol in India about a month ago, so there should be some data forthcoming. I realize it’s too early to have had that data analyzed, but I wonder if there’s been any antidotal Whispers? Anything?
This is the latest thing I could find with a Google search, an oddly Meandering article which talks about when the Indian Medical authorities stopped Ivermectin, along with other treatments that were being used, in late May. https://www.aljazeera.com/news/2021/6/17/families-grapple-as-indias-health-bodies-change-covid-guidelines
I also found this article which reports the Indian government’s claims of having never followed through with Ivermectin treatments (!!!!): https://m.timesofindia.com/city/goa/govt-stand-on-ivermectin-contradictory/amp_articleshow/83414047.cms
Finally, I’m pretty sure that this article or one similar to it has already been posted here: https://theprint.in/india/bar-association-serves-legal-notice-to-who-chief-scientist-over-ivermectin-guidelines/676672/
> Has anyone heard anything about how Ivermectin has performed against the Delta variant?
If this anything, I haven’t seen it.
Thanks for the links
Got to be too soon, surely. Professor Eli Schwartz has completed and only recently published a study which he started June last year which has to have been against the then circulating variant. The results suggest Ivermectin can be beneficial – 72% of patients who were treated with it had cleared the virus by day six of the treatment, compared with 50% in the control group. The patients treated had mild or moderate disease. Studies like this take months – Schwartz felt able to brief orally about their findings only in February this year.
Delta variant has been around for only a short while, becoming apparent in India in ,what?, February. If it is any comfort, those who claim some knowledge of Ivermectin seem to think its method of working (essentially blocking the viruses IIUC) is not particularly dependent on the precise characteristics of the virus. But I doubt anyone really knows.
Interestingly, in Ireland (the Republic) rates of delta has been going down, while its increasing in Northern Ireland.
Northern Ireland has a significantly higher and earlier vaccination rate (albeit with a focus on getting the first shot), while the Republic is lagging, although is stricter on a firm 1 month period between shots. Things will probably even up by around late July. The Republic is mostly using Pfizer and J&J, in the North I think its mostly AZ.
The success in the Republic (so far, nobody things it will last) has apparently been due to a focus by local public health teams to track and eliminate Delta outbreaks. I suspect there has also been an element of luck in that it doesn’t seem to have gotten a grip in schools yet.
So if you use Ireland as a useful example of vaccination vs conventional public health measures, the latter is doing better against delta so far.
Our pols, as usual, are Getting away with murder. I wonder what lies ahead?
To add to the discussion yesterday about YouTube’s suppression of non-officially sanctioned narrative, I’m able to hear all (I think) of Eric Weinstein’s audio productions via podcast, including his, I guess controversial, discussions of Ivermectin use and the possible dangers of taking the vaccines. I use the podcast app “Castbox” on my Android phone. I subscribe to his podcast “DarkHorse”. It’s all there. I don’t have any idea how podcasts are controlled, can be suppressed, where they’re hosted from, or anything, but at least currently, you can get the audio versions of Eric’s productions using Castbox on an Android.
I am just going to say something that hit me as I read your comment…..
Did you ever once dream in your youth that in the USA such comments would be necessary? Working around on the fringes to hear a discussion about a topic that has been censored and suppressed by the powers that be? This is what we used to hear in our childhoods about what was going in the USSR…..
Deeply disturbing – but thank you for your comment.
Thanks, Doc. Even a few years ago, say 15 (which for me now is just a few), I had not the slightest idea that the current level of free speech censorship would be dreamed of, let alone actually occur. I wouldn’t have thought, either, had I bothered to imagine it, that the censorship would happen under the direction of corporations with, I don’t know, tacit?, sanction of the nominally governing bodies. These are strange, disturbing times that I don’t think and of us hoi polloi, anyway, ever anticipated.
Catapult the samizdata.
I’m not thrilled with Weinstein via something I admittedly think is guilt by association but I still take as evidence.
I think you mean Bret Weinstein doing the Dark Horse podcast. His brother Eric is managing director of Thiel Capital. This puts me into a mobius strip, because I’m sympathetic to the ivermectin discussion, but Thiel is Thiel and among many others, funds through the Founders Fund, the dystopian Citizen policing app (Lambert brought it up on water cooler,) as well as Palantir, Taskrabbit (the FF did , at least), Paypal, Facebook, Thiel is Thiel.
So is this too flimsy? I don’t think Bret and Eric are far apart. We have a problem with startups slotting in to absolutely everything. An ivermectin advocate can make an ivermectin startup that flies a flag for disruption, that they are disrupting the stranglehold of the majors. If the subject matter of what they actually do in the world is made of ivermectin, they may do some good for their customer, but the tenor and approach are a larger problem. The Jonas Salk quote about patenting the sun is seen as so quaint. Startup people are the opposite end of the spectrum – they run on IP and I see both Weinsteins, Glenn Loury, people who have been through some kind of confrontation with woke and for a year or two were associated under the semi-jokey label Intellectual Dark Web, Harris too, as very sympathetic to Hayek and the use of market-based solutions to do things. This rubs off on what I think when Bret Weinstein talks about ivermectin; I watched the recent broadcast with Kory for instance.
On the R value of 8, this could be from Professor Paul Hunter who mentioned that figure as his estimate in a conversation with Dr John Campbell which can be found on the internet among Campbell’s other videos. Hunter is a Professor of Medicine at East Anglia University.
I recall the early estimates of Ro including a high of 8 at the beginning of COVID. Maybe the early estimates tend to be high.
Non-paywalled link for the article about Delta in China from the NYT (I think):
https://news.yahoo.com/chinas-latest-outbreak-doctors-infected-154327292.html
Over the past year it seemed like covid generally took longer to spread than expected in the US. People let their guard down because the hospitals in flyover didn’t immediately get overrun like the ones in Manhattan. I have relatives in rural Missouri, for example, who are only now experiencing widespread infections in their area among the unvaccinated, who had largely dismissed covid by now due to political affiliation (it’s Trump country) and having remained largely untouched by the pandemic so far.
I feel like we’re in a bit of a lull right now, as infections drop due to vaccination while delta or other variants that might evade the vaccines have yet to ramp up.
This summer up until fall is probably a good time to get out and do any of the things you’ve been wanting to do but avoiding due to the pandemic. Based on the past year, my gut feeling is that it won’t be until winter that things will start to get ugly.
My gut feeling as well is the winter flu season looks iffy.
Another reason we are in a lull is the general impression that its over, thus less testing, less cases etc. It’s only when hospitalizations pick up, and the hospitals will usually test for covid19, that we’ll notice the lull is over.
Hoping to get a little summer travel in before delta become dominant in another 4 to 6 weeks.
Like you I dread what the Fall promises. I got the first shot and hope that is enough so I can take care of a few doctor’s appointments and have a couple of minor surgeries without having to fly through too much flak.
I was putting off the second shot, but this post induced me to get it this morning, 9 weeks after the first Pfizer. No side effects at all. Not eve a sore arm.
Mid-May, in Belgium, in a town called Nivelles, a cluster was detected in residents of a nursing home. They had all been vaccinated in January 2021 with the Pfizer vaccine. A first contamination was detected incidentally when a resident had to be hospitalized for a reason other than covid. Generalized tests were organized which revealed: 1/ a cluster of variant alpha in the staff 2/ a cluster of variant delta in the residents. Concerning the delta variant cluster, the first tests revealed 24 contaminated residents (https://www.lalibre.be/regions/brabant/vingt-quatre-residents-des-tayons-a-nivelles-testes-positifs-60a7484e9978e20c60df441c). One week later, despite the isolation measures, there were 55 infected residents (https://nivelles.be/actu/article/1775-communique-a-propos-de-la-situation-sanitaire-de-nos-tayons-maison-de-repos-du-cpas-de-nivelles_1775.html). By June 7, there were 68 infected residents and 9 deaths (https://www.rtbf.be/info/regions/detail_nivelles-neuf-deces-a-la-residence-nos-tayons?id=10777634). On June 14, there were two more infections (70 in total), the number of deaths had increased to 12, and 5 people were still hospitalized (https://www.rtbf.be/info/regions/brabant-wallon/detail_douze-morts-du-covid-a-la-residence-nos-tayons-a-nivelles-une-enquete-epidemiologique-pour-tenter-de-comprendre-ce-qui-s-est-passe?id=10783082). The Belgian Ministry of Health is investigating why the vaccination did not work. One hypothesis is that there was a problem with the vaccine batch.
Lambert:
Thanks for never letting the seriousness of the topic deter your amazing deadpan!
[lambert blushes modestly]