Yves here. IM Doc, whose father was a public health official, anticipated the findings of this study which found that faith in institutions is essential to implementing public policies. As he wrote in April:
As a young child, I saw my father [a public health officer] struggle through the Swine Flu of 1976 and the vaccine debacle that accompanied that era.
As I grew older, and especially once I entered medicine, he had several heart-to-heart talks with me about a career in Medicine and by extension public health. I can summarize what he told me in two large thrusts. 1) Integrity, truth, and honesty is EVERYTHING in public pealth. Once squandered, it will never return. 2) Public health is 10% science and 90% psychology. Do not ever forget that. You will get nowhere by screaming SCIENCE SCIENCE SCIENCE and you will certainly get nowhere by flashing credentials. And you must have an acute awareness of panic, fear and anxiety. They change everything and your response must always take that into account.
The US has shown a steady decline in public confidence in official institutions. A recently-published study by the Reuters Institute for the Study of Journalism at Oxford found that Americans have the lowest trust in media of adults in 46 countries. The press has been a major channel for messaging about the desirability of getting vaccinated and Covid generally.
And if you have been paying attention at all, the official responses to Covid have been so obviously politicized as to undermine confidence. The flip flop on masks. The flip flop (and maybe flop back) on the lab leak theory). The failure to acknowledge asymptomatic transmission (yet the full court press to vaccinate teens and children would seem to be all about that). CDC chief Rochelle Wallesnky (along with some public service ads) falsely saying the Covid vaccines prevent getting infected. The failure to acknowledge aerosol transmission, and even now, muddled discussions on official sites. The “mission accomplished” approach, over the objections of the national and largest California nurses’ unions. Readers no doubt can add to this list.
In other words, the US has aggressively pre-positioned itself to have difficulty in getting compliance if its wager on the vaccines doesn’t work out as planned and it has to exhort the public to engage in non-pharmaceutical interventions again, like masking up and staying largely at home.
By Katrin Schmelz, Postdoctoral Researcher, University of Konstanz and Thurgau Economic Institute and Samuel Bowles, Research Professor and Director of the Behavioral Sciences Program, Santa Fe Institute. Originally published at VoxEU
Policy interventions may affect beliefs and preferences in counterproductive ways. This column presents panel evidence on COVID-19 vaccination willingness in Germany which suggests that policies that foster trust in public institutions will promote vaccination acceptance. But a vaccine mandate can also crowd out initial willingness. The data suggest that policies affect beliefs and preferences through both framing and learning effects. Beyond the pandemic, the findings may also be applied to other societal challenges such as climate change, where an effective combination of mandatory policies and values-motivated lifestyle changes will contribute to reducing our carbon footprint.
Four decades ago, Robert Lucas rocked economics with a simple observation: taxes and other government interventions in the private economy affect not only the costs and benefits of actions citizens may take (as intended), but also their beliefs about the future actions of others (including the government), possibly in counterproductive ways. For example, announcing stiffer penalties for non-payment of taxes provides an incentive to pay up; but it also may convey the information that non-compliance is common, leading formerly honest citizens to cheat.
Lucas’ point was that policymaking is not simply resetting the dials on a given model of how the economy works, but instead changing the structure of the model itself (Lucas 1976). In 1994, Henry Aaron of the Brookings Institution pointed to “the failure of economists to take the formation of preferences seriously”, and suggested that the Lucas critique be extended to cover preferences as well as beliefs (Aaron 1994).
At the time there was little evidence on which policymakers could draw if they wished to take account of the endogenous nature of preferences and beliefs. But experimental economics has filled many of the gaps (as surveyed by Bowles and Polania-Reyes 2012). The response to COVID-19 vaccinations provides rare new evidence from outside the lab (Schmelz 2021, Schmelz and Bowles 2021).
Framing and Learning: How Policies Affect Preferences and Beliefs
There are two senses in which a policy may alter preferences and beliefs. We term these framingand learning. The first, a short-term effect, is that the incentives or constraints by which the policy is implemented frame the citizen’s decision in a particular way. The psychologist Mark Lepper and his colleagues wrote that “superfluous social constraints”, for example, unavoidably convey information about “the presumed motives” of the policymaker, as well as the reasons why the policy was adopted, and “the relationship” between the policymaker and the citizen (Lepper et al. 1982).
The second sense in which policies may alter preferences and beliefs is a longer-term change in preferences due to learning. By structuring the daily experiences of the citizen – in their interactions with others and the state – a policy may alter the longer-term evolution of a person’s preferences and beliefs (Bowles 2008, Bowles and Polania-Reyes 2012, Schmelz and Ziegelmeyer 2020).
Our Evidence: Enforced COVID-19 Vaccination May Crowd Out Voluntary Compliance
We have found evidence of both framing and learning in citizens’ responses to vaccinations and other COVID-19 pandemic policies.
Our panel of 2,653 Germans, surveyed both in April/May and in October/November of 2020, allows us to track the attitudes of the same individuals during the first and second lockdowns. In both waves, respondents were asked: “If there is an approved vaccine against the coronavirus, to what extent would you agree to be inoculated yourself if: … vaccination is strongly recommended by the government but remains voluntary? … vaccination is made mandatory and checked by the government?” Answers were given on a five-point Likert scale ranging from 0 (“not agree at all”) to 4 (“fully agree”).
While support for voluntary vaccination remained high in the second wave, the fraction fully supporting enforced vaccinations was initially lower and then dropped from 44% to 28%, as shown in Figures 1A and 1B.
Vaccination Willingness Has Declined Among Those Who Lost Trust in Public Institutions
We found that trust in public institutions is a strong predictor of willingness to be vaccinated under voluntary or enforced policies. We measure trust in public institutions by the average of the subject’s expressed general trust in the federal government and specific trust in its truthful information about COVID-19, as well as their trust in the state government, in science, and in media. We term this measure ‘public trust’.
The fall in support for enforced vaccination occurred disproportionately among those whose public trust had declined between the two waves of the survey. This lends some support to the idea that the positive correlation between trust and vaccine support reported in cross-section data (e.g., Bargain and Aminjonov 2020) may reflect a causal relationship. The distrust effect is substantial: a one-point drop in our public trust measure (ranging from 1 to 6.6) would account for 37% of the observed reduction in support for enforced vaccines between the two waves.
This is consistent with evidence from the UK that people in locations where intensive care units were under stress early in the pandemic were more resistant to vaccination later, perhaps because they had lost confidence in medical institutions (Blanchard-Rohner et al. 2021).
Figure 1 Reduced support for enforced vaccination
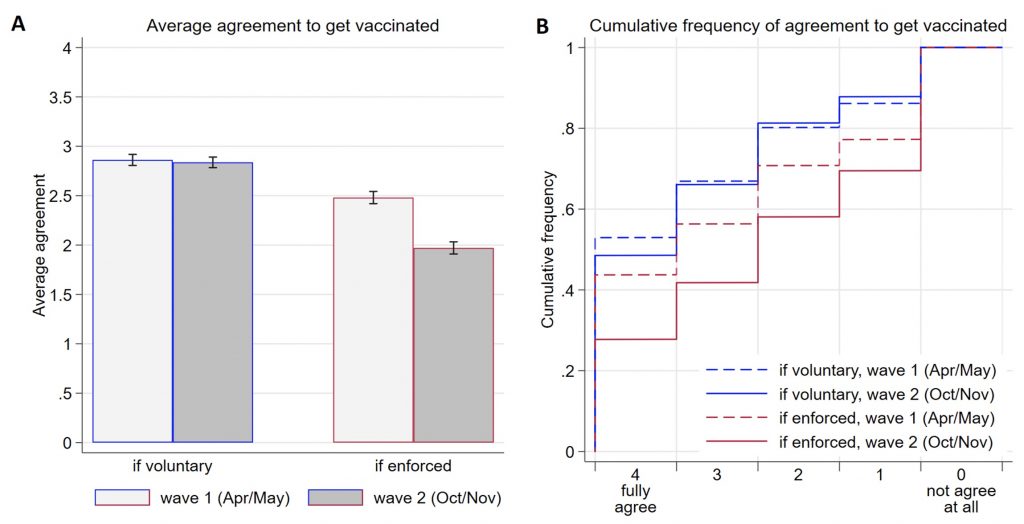
Notes: (A) Average agreement to get vaccinated if it is voluntary or enforced in the two waves of the survey (in Likert scale units). Error bars represent 95% CI. (B) Cumulative distributions of agreement in case of enforced versus voluntary vaccination for the two waves of the survey. For example, the dashed and solid red lines show that 44% and 28% of respondents fully agreed to get vaccinated in case of enforcement in the first and second waves of the survey, respectively.
Why Enforcement May Crowd Out Intrinsic Motivation to Contribute to a Public Good
The fact that enforcement reduces support for vaccinations is surprising in light of what we know from experimental public goods games. Most anti-COVID-19 policies share the fundamental structure of public goods dilemmas where all-encompassing cooperation maximises the wellbeing of all citizens, but since cooperation is costly each individual has an incentive to free ride on others if the level of cooperation is sufficiently high (Gollier 2021).
Experiments with public goods games around the world have shown that in the absence of an option to punish free riders, substantial levels of initial cooperation typically decline as contributors become discouraged or angered by those not contributing (Herrmann, Thöni, and Gächter 2008). But a belief that most others will cooperate – or be punished if they do not – encourages conditional cooperators to do the same (Fischbacher, Gächter, and Fehr 2001, Shinada and Yamagishi 2007). This would lead us to expect that average agreement to follow anti–COVID-19 measures should be higher if a measure is enforced than if it remains voluntary.
But the lesser support for mandated than voluntary vaccinations that we found suggests a different line of reasoning. An enforcement-based approach might be compromised because it crowds out voluntary commitment. Economists term this ‘control aversion’, a particular case of intrinsic motivation being diminished by explicit constraints or incentives (Falk and Kosfeld 2006, Ziegelmeyer, Schmelz, and Ploner 2012).
Our data suggest that this occurs in the case of vaccine willingness. We have identified three mechanisms which might account for this (Bowles and Polania-Reyes 2012).
The first, termed ‘psychological reactance’, is the result of individual strivings for freedom or ‘self-determination’ (Lepper et al. 1982, Rudorf et al. 2018). It is consistent with our finding that the opposition to enforced vaccinations is substantially greater among respondents who reported that it would restrict their ‘freedom’.
Second, ‘moral disengagement’ occurs when the provision of explicit incentives or constraints frames the decision problem as one in which ethical convictions are not salient (Falk and Szech 2013). Voluntary vaccination policies may trigger moral deliberation and the desire to be a good citizen. By contrast, enforcement might relieve the citizen of any need to deliberate, and thus crowd out those moral convictions (Bowles 2016).
Resistance to vaccination provides an example of moral disengagement. In the second wave of the survey, those reporting greater altruism – willingness to help others – were also more likely to support voluntary but not enforced vaccinations. The negative impact of enforcement is greater among citizens reporting more other-regarding preferences.
The third mechanism through which enforcement may crowd out intrinsic motivation is by diminishing trust. Enforcement may signal that the policymaker knows that the vaccine is not something citizens would willingly subject themselves to. In addition to ‘bad news’ about the vaccine, the distrust communicated by enforcement signals low expectations about citizens’ behaviour (Sliwka 2007). In the eyes of citizens, this may result in a mutually distrusting relationship (Bartling, Fehr, and Schmidt 2012, Fehr and Rockenbach 2003), promoting vaccine hesitancy, as our panel data show.
Learning Control Aversion: The Role of Institutions
Because the control-averse reactions shown in Figures 1A and 1B were responses to a hypothetical question about mandated vaccination, we consider them to be temporary framing effects, subject to reversal by reframing the decision, instead of a genuine change in preferences.
But our survey also provides evidence of longer-term preference change.
Respondents who had lived under liberal institutions in West Germany since the end of WWII were more control averse than those who had experienced two generations of authoritarian rule beginning of 1933. Figure 2 shows that the East–West difference is qualitatively larger for older Germans who were at least 20 years old when the Berlin Wall came down (mean age at survey time: 62 years) than for younger Germans who experienced less than 20 years under different regimes (mean age: 35 years). This finding is in line with evidence from an online experiment in a setting unrelated to COVID-19 policies (Schmelz and Ziegelmeyer 2020).
Figure 2 Effect of experience in East (compared to West) Germany on control aversion with respect to anti-COVID-19 policies
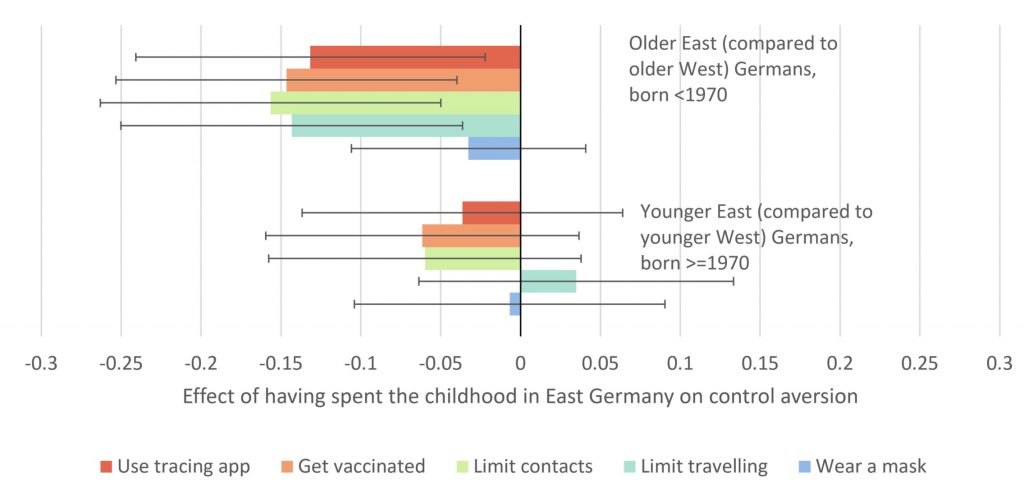
Notes: Control aversion is measured by the difference between voluntary agreement and agreement in case of enforcement in the five domains. Shown are the coefficients and 95% CI on control aversion. For example, the upper part of the figure shows that older East Germans are somewhere between 13% and 16% of a standard deviation less control averse than older West Germans in all domains except for masks.
Older East Germans are less control-averse than older West Germans in all domains except for masks. This is consistent with the effect of mere exposure (Zajonc 2001): those brought up in East Germany prior to 1990 were subject to ubiquitous surveillance, compulsory vaccination, and restrictions on movements.
By contrast, wearing masks is rather exotic and not part of the experience of East (or West) Germans prior to the pandemic. This result is remarkable as it shows that people who experienced the coercive East German regime three and more decades ago are still less averse to enforced anti-COVID-19 measures.
Policy: Putting the Survey Results to Use
Legally required vaccination against measles and other diseases is an essential part of public health policies around the world. COVID-19 vaccination mandates, for example, targeting those caring for the elderly may be an important element of a policy response to the pandemic.
But mandating COVID-19 vaccination may also have a substantial negative impact on voluntary compliance. Given limited state capacities and persistent citizen opposition, ending the pandemic in a timely manner by universal enforcement could be impossible. Moreover, enforcement could bear costs including heightened social conflict and citizen alienation from their government or professional elites. The result could be a downward spiral of public distrust fuelling vaccine resistance, triggering more extensive enforcement and in turn further eroding public trust. Costly errors may be avoided if policymakers understand that citizens’ preferences are not fixed but will be affected by the crowding-out effect of enforcement – in varying degrees depending on the policies, as we have found (Schmelz 2021).
Our findings may bear lessons beyond COVID-19. Consider policies to address climate change. Sustaining environmentalist values will be essential for the passage and implementation of the necessary mandatory policies. Moreover, green social norms will be necessary to promote the lifestyle changes that reduce our carbon footprint, given limited state enforcement capacities in this realm. So, the feasibility and effectiveness of environmentalist initiatives may depend on the ways policies themselves alter beliefs and preferences.
Important considerations to evaluate the wisdom of voluntary versus enforced policies go beyond whether enforcement evokes substantial control aversion and include the level of compliance required for a policy to be successful, the share of citizens who would comply with a policy voluntarily, and the extent to which effective enforcement is feasible.
See original post for references


Key point from the above post:
“Enforcement may signal that the policymaker knows that the vaccine is not something citizens would willingly subject themselves to.”
Bingo. Nail hit squarely on head.
And I’m going to place my slender self out on a limb and say that the vaccine effort is collapsing in the USA. Note the prevalence of bribery since, oh, early May.
At the same time, the Delta variant seems to making itself known here. Will it lead to more widespread vaccination? When we’re hearing about increases in cases, hospitalizations, and deaths in the UK and Israel, two of the most vaccinated areas on the planet, I think that won’t happen.
What will happen? Well, I think that the items discussed in Nick Corbishley’s March 30 NC post will figure prominently:
https://www.nakedcapitalism.com/2021/03/its-time-to-talk-about-ivermectin.html
Experimental economics is largely trash. Mathematical psychology by far has the better record (dating from the 1960s) in testing people’s preferences. Simply Google Antony AJ Marley and his supervisor Duncan Luce (loosely affiliated with the Manhattan project) for proper math.
Daniel McFadden had the good grace to acknowledge in his “Nobel” lecture that the math psych people were where it’s at. Unfortunately subsequent economists have too much ego. Claim new stuff. We knew all this in the late 1960s. I don’t have an iota of respect for Lucas. He never ever acknowledged the work in stated preferences elsewhere.. He’s either incompetent or corrupt.
Its amazing how many ‘breakthroughs’ in economics are little more than simplistic reinventions of what was long known in other branches of research. Economic historians and economic geographers have far more to say about productivity or how to grown backward economies than any micro or macro work.
Bless ypu. The truth in a few simple words.
It sounds like what Robert Lucas actually observed was positive/negative feedback on a real level. Taxes were accepted because people gave government the “benefit of the doubt.” We don’t do that any more because honesty in government has been so corrupted and the population so neglected that nobody, virtually nobody, trusts the government to do or say anything fair or good. The government knows its name is mud, so it gives us screaming twits like Rachel Maddow. But we all, not just government apparatchiks, can sense that ubiquitous, unspoken acknowledgement of what has actually happened (usually we all get screwed) and without a word, maybe some undiscovered language, nobody trusts what the government says. Then the inevitable debacle of handling a crisis like Covid where old lies still linger. It’s a miracle any of us took the damn vaccine at all.
I wonder how Winky’s victory lap is going to affect confidence, White House to trumpet return to normalcy despite delta variant
Return to normalcy?
https://www.newstribune.com/news/local/story/2021/jun/30/springfield-hospital-turns-away-covid-patients/877150/
Springfield hospital turns away COVID patients
thanks for posting this. theres a (sadly not unexpected) twist in this story near the middle where we learn abt inadequate hospital staffing as contract nurses have left for their next “placements”.
but in that story theres a link to another story:
https://www.newstribune.com/news/missouri/story/2021/jul/02/delta-variant-spread-means-missouri-covid-19-cases-could-double-or-triple-july/877490/
which ends with this:
The greatest increase has been in southwestern Missouri. Steve Edwards, CEO of CoxHealth in Springfield, has been outspoken in his contempt for people who doubt the effectiveness of the vaccine or the danger from COVID-19.
His hospitals are treating 74 COVID-19 cases, including four pediatric patients, he tweeted Thursday. The children range in age from a few weeks old to 18.
“If you are making wildly disparaging comments about the vaccine, and have no public health expertise, you may be responsible for someone’s death,” Edwards wrote. “Shut up.”
>….have no public health expertise, you may be responsible for someone’s death
Does this imply people with health expertise (whether they bring up legitimate vaccine concerns or not) are not responsible for someone’s death when they occur? I dont see how this is anything but an effort to shift blame
Of course there is now zero faith in even public health institutions. Almost 2 years on, there isn’t even a transparent, scientific method-adherent effort to find the source of the virus.
I’m not sure if even mention the various hypotheses, and the facts and circumstantial and direct evidence supporting such hypothesis, is even allowed on this website.
And by now it’s too late to definitely prove anything as so much evidence likely has been destroyed or lost to the winds.
And the collapse of faith/trust in public health institutions directly affects people’s willingness to accept claims that are proved by the scientific method but which a layman has not way of independently verifying as they might not even have a high school level understanding of biology or chemistry.
If the lab leak hypothesis is/was not investigated properly by people who are/were more than able to do it, then a persistent lack of convincing evidence that Covid had a natural origin is sufficient to infer that the variant was man-made. This reasoning is as valid as any in scientific inquiry.
Zeynep Tufecki addresses this issue in the Links.
It appears that a definitive answer to the question is unavailable.
I call bullshit. You are treading on very thin ice. No links, just an unsubstantiated assertion. There were plenty of cases not in Wuhan before it broke out there, such as one confirmed in a peer reviewed journal in Italy in Nov 2019.
More generally, the absence of evidence is not evidence of absence.
It took 15 years to find the animal origins of SARS. And there was a TON less international travel in and out of China in 2003-4.
This article might have been mentioned before, but it is worth mentioning again.
Article in Wired latest issue in print version “A Fatal Flaw”. In a quick search, I don’t find a link.
Subtitle “All Pandemic, Long Scientists Brawled Over How the Coronavirus Spreads. Droplets! No. Aerosols!. At the heart of the fight was a Teensy Decades Old Screwup that helped Covid Kill. A team of experts finally tracked that viral error back to its source.”
Describes the scientists and then forensic like analysis to find the “fatal flaw” in the 5 micron droplet theory that prevented the early realization that Covid-19 was spread mostly as an aerosol.
A scientific fact requires institutional and instrumental support. The “fact” of 5 micron drops was the consensus in WHO and CDC which was used to discount the need for masks. Readers here at NC have followed this controversy during the unfolding pandemic.
Bruno Latour in his groundbreaking study at the Salk Institute used literary theory to analyze laboratory life and to describe how scientific “facts” are created and maintained through institutional support. The report on this project was first published in 1979 “Laboratory Life: The Social Construction of Scientific Facts.” In the revised edition published in 1986, the word Social was dropped from the title.
The lesson from IMDoc’s father that “screaming science, science, science” won’t work for public health, has been demonstrated with the experiences from Covid-19. His father also said that once lost credibility, it cannot be recovered. One of the legacies of Trump was the further destruction of institutions, including the institution of science, and undermines intuitions as the places that values are established and maintained.
trump is a symptom of instutional gangrene, not the cause.
rot set in long ago and accelerated post-2008.
blame isn’t solely due to one side. it is trans/omni-party rot and corruption
Agreed, but did you miss the word “further” in Dons comment?
Is not, I suggest, a universal truth. It is true in varying degrees in those places where science butts heads with religious beliefs, where parts of the population of varying sizes and extent have been forced to ‘choose’ between science – (the world is 4 billion years old) – and religious belief – (the world is 6,000 years old) – etc. This leads to ‘science’ being regarded as intrinsically suspect if not downright sinister.
Where religious belief is less dogmatic and gives science some respect, even giving ground in the face of the inevitable, screaming ‘science’ (a’la global warming) can make considerable headway even, and perhaps especially, in the public health field.
Outside of ‘the Bible Belt’ I suggest that the problem screaming ‘science’ has in this particular instance is that the public is very well aware that this pandemic caught science with its trousers down, with its initial confused and even downright wrong initial response, and is now pushing ‘new’ unproven remedies as the solution giving rise to considerable justifiable scepticism as to its credibility. Nevertheless it appears that very many people are prepared to give it the benefit of the doubt by having the jab.
I agree with L Fyne. You give Trump far more credit than he deserves.
A pleasure and an inspiration to see Sam Bowles continue his excellent heterodox work. Sam’s studies of the Prison Industrial Complex remain unsurpassed and completely ignored by the institutionally ensconced. Allow me to note that he published a book on biology and economics with his old URPE comrade Herb Gintis called, A Cooperative Species: Human Reciprocity and It’s Evolution. Truely in the spirit of the great Carl Polanyi. Economic Anthropology…in my estimation the only hope for the dismal science.
Yeah, it is all about trust. Here in Oz they keep on using models to make their decisions with about the pandemic. What do they look like? Don’t know. They’re classified. We just have to take their word for it that their political decisions are aligned with those models. The government, in their infinite wisdom, have decided that vaccines will save us all and are going to threaten people to get a vaccination before they open the floodgates of people coming from overseas that will be able to skip doing quarantine. Sounds like a plan.
Only two problems. There aren’t anywhere near enough vaccines having dropped the ball on supply. The second problem is that to have this herd immunity, the magic percentage of people needing vaccinations is reckoned to be 80%. Is there any country in the world that has achieved that? But as Scotty from Marketing says, they are going to treat this virus just “like the flu” and accept the body count. One thing is for sure, they had better beef up the hospitals and medical system. We are going to desperately need them by next year.
Canada as a whole has just reached 75% of the 12 and older part of the population (none of the vaccines here – Pfizer, Moderna and Astrazeneca – are approved for those under 12) having had at lest the first dose with 22% having had both. Remarkably quick turnaround considering how few vaccinations had been given just a couple of months ago. Seems to be largely supply limited here still. I would guess we’re going to get about 90% vaccination. Hopefully that’s going to work because there doesn’t seem to be much chance of better border controls and quarantine and I get the feeling many of the precautions will be dropped soon.
The most interesting finding of this research is the difference between East and West Germans in their trust of authority. The Ossies are actually more trusting than the Wessies. Go figure.
funnily enough, I had an opposite experience in a far more trivial context. I worked at a retailer in Berlin where we were encouraged to get customer sign-up onto a database (name, email address sort of thing). We were told (and experience confirmed) that Berlin had much less uptake of this than the other stores, all in the west, on account of Eastern reluctance to unnecessarily surrender personal information out of mistrust due to the experience of the DDR years.
So, if trust can’t be regained once lost, and it has been lost, what is the way forward?
imo., to be real, at best prepare for stagnation. don’t expect the state to help you—-regardless of one’s opinion about the role of the state in life (hope i am wrong)
happy birthday america!
Eh. I guess people like the author are expected at this point to write something.
Look, I’ve already stated that I think the normal zillion-years-before-approval of the FDA is just BS. Not because I don’t want everything carefully studied, but because Big Pharm only wants it to look like they carefully studied whatever.
But that’s just me. Most people actually somewhat believe in the FDA or their country’s equivalent. So this article is unknowingly discussing apples (normal drug approval) in the context of a serving of oranges (the OMG we need a vaccine now!) and I don’t know what point that could possibly illuminate. Besides, like I said, the forever need to publish.
The FDA approval process is shorter than a zillion-years. Some problems with a drug or vaccine take time to become known. I recall reading that the present FDA regulations were a result of the Thalidomide tragedy. Some of us believe in some of the regulations the FDA is supposed to enforce, but the FDA itself has become tarnished. The FDA, CDC, WHO, all appear to me as wholly owned subsidiaries of Big Pharma.
We all knew this was coming. Since Katrina we have seen that you cannot depend on the govt. to fix anything, plan anything, help anyone. They do not care. The 600,000 plus people that have died seems to not matter to any of these people. This CDC director is the same as Trump’s CDC director. The CDC and FDA have been a big Pharma joke for years.
We are on our own. I continue to be glad that we have this site as it has helped us navigate the lies. The lie that the vaccine protects the Vaccinated as an example. I am seeing huge numbers of elderly and frail looking persons at the store maskless. People have also been excited about the 4th of July, asking about “our plans” for the holiday. When I tell them I will be in the house as I want to prevent breakthrough transmission etc. I get a look like I just told them some wild Q anon conspiracy. Now that they are also protecting the big Pharma by refusing to release to other countries to make the vaccine. The variant will increasingly mutate.
I’m having similar experiences as you Nikkikat – very few people are wearing masks anymore (I’m not giving up mine when I go in a public place). Friends and relatives believe that as long as they’re vaccinated, they’re safe from getting Covid. I mentioned to someone that being vaccinated is no guarantee you won’t get Covid – she looked at me funny – like what? People will believe what they want to believe. Tonight I head some talking head “news” person say – “now that the pandemic is winding down” – really?
I also notice that sites like CNN, Fox, etc. are no longer giving case counts, number of deaths, so of course, the pandemic must be over. Stuff that isn’t reported just doesn’t exist. Yes, we are truly on our own, and have been for quite some time.
In regard to CNN, has anyone tried to use the formal CNN response form to ask them why they have stopped? I have and am always greeted by a response similar to “We are having some difficulty and are unable to respond to your query.”
I am troubled by this post.
First take a look at the conclusion but substitute one word:
“Important considerations to evaluate the wisdom of voluntary versus enforced policies go beyond whether enforcement evokes substantial control aversion and include the level of compliance required for a policy to be successful, the share of Corporations [citizens] who would comply with a policy voluntarily, and the extent to which effective enforcement is feasible.”
Second I believe the survey has very little to do with the Corona vaccines. The question: “If there is an approved vaccine against the coronavirus, to what extent would you agree to be inoculated yourself if: …” begs the question whether there is an authority that can reliably approve a vaccine for widespread use. For sake of argument assume the FDA is still capable of reliably approving the ordinary flu vaccine. This survey question might be useful for exploring the motivations in populations who do or don’t get an ordinary flu-shot.
The Corona vaccine has not been approved. It has not been properly tested and evaluated. The Government sponsored a free large-scale phase III trial by granting an Emergency Use Authorization [EUA]. How much data is being collected and analyzed for this phase III trial? How much trust is engendered by the Government’s blanket grant of immunity from liability to the Big Pharma vaccine makers? What do policies that foster trust in public institutions have to do with the scattered evidence that the vaccines are neither as safe nor as effective as claimed? Policy interventions may affect beliefs and preferences — policies like deliberately lying to the public?
This post also suggests an intrinsic motivation to contribute to a public good. I am still confused whether the vaccine works at keeping the vaccinated from having an asymptomatic Corona infection and stealth spreading the virus. I think the case for mass Corona vaccination for the public good is weaker than the case for individual good from getting vaccinated, which is already a much weaker case than I would prefer. Policy interventions definitely played a part in my decision to get a Corona vaccination. The “mission accomplished” re-opening hoopla makes it much more dangerous to make even the few trips I make to get food. I also need to get a minor surgery and now seems a brief window when that might be possible with minimal risk, but risk sufficient to risk getting vaccinated. The apparent policy of quashing information about Ivermectin and the relative difficulty and delays in obtaining other than veterinary Ivermectin removes that as a choice for me in making use of this brief window of time before the next wave of the pandemic starts. Part of my decision to get vaccinated was complicated by the contradictory information about whether the vaccines are effective against the new variants. A few years from now will complete the informal phase IV trial and we might be better able to decide how much public good was served by the EUA.
How can they get everyone to believe in free markets?
They need to wait a long time until no one can remember what happened before.
“Everything is getting better and better look at the stock market” the 1920’s believer in free markets
That belief will be gone by the end of the decade.
“Stocks have reached what looks like a permanently high plateau.” Irving Fisher 1929.
This 1920’s neoclassical economist that believed in free markets knew this was a stable equilibrium.
He became a laughing stock.
Better shelve this for a few decades until everyone has forgotten.
Now everyone has forgotten we can use it for globalisation.
A whole new generation of suckers were ready to learn the hard way; it was a complete disaster last time.
The economics of globalisation has always had an Achilles’ heel.
The 1920s roared with debt based consumption and speculation until it all tipped over into the debt deflation of the Great Depression. No one realised the problems that were building up in the economy as they used an economics that doesn’t look at debt, neoclassical economics.
Not considering private debt is the Achilles’ heel of neoclassical economics.
https://www.youtube.com/watch?v=vAStZJCKmbU&list=PLmtuEaMvhDZZQLxg24CAiFgZYldtoCR-R&index=6
At 18 mins.
1929 and 2008 stick out like sore thumbs.
In the 1930s, the Americans found margin lending and share buybacks had artificially inflated the markets and this had lead to the Wall Street Crash of 1929.
What lifted US stocks to 1929 levels in 1929?
Margin lending and share buybacks.
What lifted US stocks to 1929 levels in 2019?
Margin lending and share buybacks.
A former US congressman has been looking at the data.
https://www.youtube.com/watch?v=7zu3SgXx3q4
What was it like last time?
All the wealth concentrated at the top and everyone else had to get by on debt.
Mariner Eccles, FED chair 1934 – 48, observed what the capital accumulation of neoclassical economics did to the US economy in the 1920s.
“a giant suction pump had by 1929 to 1930 drawn into a few hands an increasing proportion of currently produced wealth. This served then as capital accumulations. But by taking purchasing power out of the hands of mass consumers, the savers denied themselves the kind of effective demand for their products which would justify reinvestment of the capital accumulation in new plants. In consequence as in a poker game where the chips were concentrated in fewer and fewer hands, the other fellows could stay in the game only by borrowing. When the credit ran out, the game stopped”
Keynes added some redistribution to stop all the wealth concentrating at the top, and this gave rise to a strong, healthy middle class.
After a few decades of Keynesian, demand side economics, the system became supply side constrained.
Too much demand and not enough supply causes inflation.
Neoclassical, supply side economics should be just the ticket to get things moving again.
It does, but it’s got the same problems it’s always had.