By Lambert Strether of Corrente
Last Friday, the CDC published “Outbreak Associated with SARS-CoV-2 B.1.617.2 (Delta) Variant in an Elementary School — Marin County, California, May–June 2021” (“Outbreak”). This got a lot of play in the Northern California press, with a good deal of reporting done (or at least original stories written), because the study was led by Marin County Public Health, and they with other California epidemiologists and experts wrote the study up and then submitted it to the CDC, which accepted it. Good for them! However, there is a question “Outbreak” does not ask, and that the press did not ask. Carefully avoiding spoilers — though few NC readers will be surprised at the plot twist — I will first quote the “Outbreak” on the incident. Then I will switch into media critique mode, and present the headlines from Northern Califonia. After that, I will present the implications drawn from the outbreak by the press (which are more broad spectrum than the headlines). Finally, I will give the unasked question from “Outbreak” a thorough airing, and conclude.
Here is what “Outbreak” says in the “Investigation and Findings” section:
The outbreak location was an elementary school in Marin County, California… Each grade includes 20 to 25 students in single classrooms. Other than two teachers, one of whom was the index patient, all school staff members were vaccinated (verified in California’s Immunization Registry). The index patient became symptomatic on May 19 with nasal congestion and fatigue. This teacher reported attending social events during May 13–16 but did not report any known COVID-19 exposures and attributed symptoms to allergies. The teacher continued working during May 17–21, subsequently experiencing cough, subjective fever, and headache. The school required teachers and students to mask while indoors; interviews with parents of infected students suggested that students’ adherence to masking and distancing guidelines in line with CDC recommendations (3) was high in class. However, the teacher was reportedly unmasked on occasions when reading aloud in class. On May 23, the teacher notified the school that they received a positive result for a SARS-CoV-2 test performed on May 21 and self-isolated until May 30. The teacher did not receive a second COVID-19 test, but reported fully recovering during isolation.
The index patient’s students began experiencing symptoms on May 22. During May 23–26, among 24 students in this grade, 22 were tested…. Twelve (55%) of the 22 students received a positive test result, including eight who experienced symptom onset during May 22–26. Throughout this period, all desks were separated by 6 ft. Students were seated in five rows; the attack rate in the two rows seated closest to the teacher’s desk was 80% (eight of 10) and was 28% (four of 14) in the three back rows…
On May 22, students in a another classroom, who differed in age by 3 years from the students in the class with the index case and who were also ineligible for vaccination began to experience symptoms. The two classrooms were separated by a large outdoor courtyard with lunch tables that were blocked off from use with yellow tape. All classrooms had portable high-efficiency particulate air filters and doors and windows were left open. Fourteen of 18 students in this separate grade received testing; six tests had positive results. Investigation revealed that one student in this grade hosted a sleepover on May 21 with two classmates from the same grade. All three of these students experienced symptoms after the sleepover and received positive SARS-CoV-2 test results. Among infected students in this class, test dates ranged from May 24 to June 1; symptom onset occurred during May 22–31.
So that’s the outbreak. Here are the headlines:
- CDC: Unvaccinated Marin County teacher caused big COVID-19 outbreak in school San Francisco Chronicle
- CDC study finds unvaccinated Marin Co. teacher infected 22 elementary school students with COVID ABC7
- CDC report confirms unvaccinated Marin County teacher was source of Delta variant outbreak KTVU
- CDC study shows unvaccinated teacher started Delta COVID outbreak at Marin school KSBW
- One Unvaccinated Teacher In Marin School Seeded COVID Outbreak That Infected Over a Dozen Students, Their Siblings, and Parents SFist
- How 1 unvaccinated Marin County teacher started a delta variant outbreak: CDC study KRON4
There is a unanimity of opinion by the headline-writing editors that the source of the problem was the index case: the unvaccinated teacher. Indeed, that’s without justification — that is, is not only a matter of aghastitude — given the “Implications for Public Health Practice” in the Summary section of “Outbreak”:
Vaccines are effective against the Delta variant, but transmission risk remains elevated among unvaccinated persons in schools. In addition to vaccination, strict adherence to multiple nonpharmaceutical prevention strategies, including masking, are important to ensure safe school instruction.
(I presume the Summary is tacked on to the submitted study by CDC.) Now let’s turn to the bodies of the stories, where there is a broader spectrum of opinion than in the headlines. In the same order as above:
The rash of infections highlights just how contagious the delta variant is, underscoring “the importance of vaccinating school staff members who are in close indoor contact with children ineligible for vaccination as schools reopen,” the CDC report said.
However, Lam-Hine said that it’s impossible to know if the unmasking was the cause of the outbreak or if it was a combination of small lapses in the protective measures.
“When there’s things that are very high risk, you have multiple levels of protection, and when one fails, you hope that the other three or four that you have in place hold up,” he said. “In this case, something didn’t line up.”
ABC7:
“We had someone let their guard down,” said Mary Jane Burke, Marin County Superintendent of Schools.’
Luz Pena [reporter]: “Do you believe teachers should be mandated to get vaccinated?”
Mary Jane Burke: “I do, I do.”
KTVU (FOX):
The CDC says 18 of the 27 cases were sequenced, and they all were found to be the Delta variant.
The CDC says that this incident illustrates just how contagious the Delta variant is.
Nothing on interventions, pharmaceutical or not.
KSBW:
The report, released Friday, emphasizes the significance of vaccination and “strict adherence to multiple nonpharmaceutical prevention strategies, including masking” in ensuring the safety of students and teachers now that in-person learning is the norm at Bay Area schools.
UCSF chair of medicine Bob Wachter used this study as a case study of why a vaccine mandate is necessary for teachers.
“I doubt this teacher wanted to infect half of her class or thought she was putting them in danger,” Wachter said in a tweet Friday. “But she did and she was.”
In a case that illustrates both how essential vaccine mandates are for schoolteachers and how contagious the Delta variant can be in an indoor classroom setting with unvaccinated students, the Marin outbreak holds lessons that should be learned nationwide.
At the time of this outbreak, another occurred in Marin County that was centered in San Anselmo and Fairfax. Health Officer Dr. Matt Willis said at the time, because both outbreaks lasted only two weeks and appeared to be stopped short by the vaccines, “This is what herd immunity looks like.”
Assuming “herd immunity” for respiratory viruses is a thing; we simply don’t know (and Fauci’s nimble goalpost moving hasn’t helped).
The CDC recommends for all eligible people to get vaccinated – especially teachers who are in close contact with ineligible students They also recommend staying home if showing symptoms, getting tested routinely, and wearing face masks inside.
Note that “close contact” is not a means of transmission.
So, we have a rich bouillabaisse of opinion, with teacher vaccination mandates predominating, but also the contagiousness of Delta, and non-pharmaceutical interventions, including masking. Marin County’s Lam-Hine, the corresponding author for “Outbreak,” has, to my mind, the best perspective of all: “When there’s things that are very high risk, you have multiple levels of protection, and when one fails, you hope that the other three or four that you have in place hold up.” However, there is one level of protection after vaccination that none of the reporting mentions; it’s as if masking and social distancing were the only forms of non-pharmaceutical intervention. Ironically — and this is the plot twist — Lam-Hine’s “Outbreak” also fails to give adequate consideration to it. That level of protection:
Ventilation. How effective was the ventilation in the school room?[1]
At least in my recollection, aerosol transmission broke through to the mainstream in this lucid and compelling interactive article in the English version of El Pais, “A room, a bar and a classroom: how the coronavirus is spread through the air.” Here is a graphic about aerosols in schools, directly on point “Outbreak”:
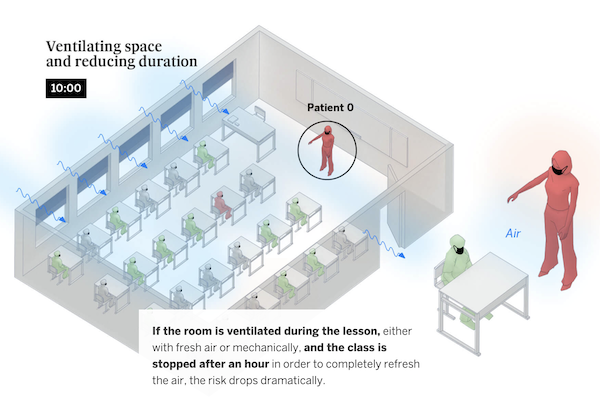
And here is “Outbreak’s” seating chart, which shows, like El Pais, a pattern of transmission extremely suggestive of aerosol transmission from a superspreading teacher to multiple students:
(So apparently being one of Chris Arnade’s “back row kids” is no guarantee of protection, although the front row kids are worse off.) SFist describes the “Outbreak” seating chart admiringly:
Much like an early study out of China that illustrated how the airborne coronavirus spread in a restaurant, the CDC study provides a map of where the teacher’s desk was located in relation to students’ desk, and where each of the infected students sat. Students in the class, included many in the front two rows of the classroom, began showing symptoms on May 23 and 24, and subsequently tested positive. All told, 12 out of 24 students in the class were infected and tested positive, including several in the back rows of the class. The infection rate for the front two rows of the class was 80%.
These transmissions occurred despite students adhering to mask protocols, the presence of an air filter at the front of the class, six feet of distancing between desks, windows left open on both sides of the classroom, and the door of the classroom being kept open.
I too, admire seating charts; I find epidemiological diagrams far more persuasive than models[2]. But I have questions. I note that the diagram indicates open windows, an open door, and an air filter. From the text of “Outbreak“:
All classrooms had portable high-efficiency particulate air filters and doors and windows were left open.
“Outbreak,” in other words, answers the question: What was the physical arrangement in the room?[3] However, the question that needs to be answered is: How well was the room ventilated?
In terms of physical arrangement, were the windows and doors always left open? How do we know? Were the windows small and high up[4], so a good draft would not be possible? What brand of HEPA filter was used, and was it suitably sized to the room? Were the filters running at all times? A fan or Corsi box was apparently not thought necessary, but why? And who decided? In terms of metrics, why on earth were no CO2 measurements taken with the room populated and under protocol? And what are the Air Changes per Hour? Saying that a room is well ventilated because there’s a HEPA filter in it is like saying children are learning music. Joseph Allen of the Harvard T.H. Chan School of Public Health tweets:
— Joseph Allen (@j_g_allen) August 27, 2021
And how on earth did CDC’s editors allow this paper to be published without revisions? Perhaps because the policy objective of mandating vaccines for teachers — so happily propagate in the headlines — is of over-riding importance to them, and not [genuflects] the science?
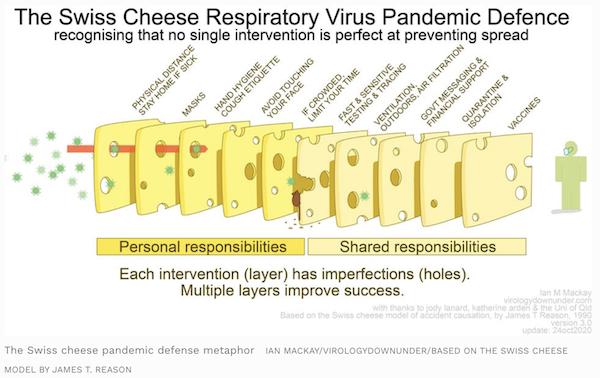
The CDC supports, as Marin County’s Lam-Hine correctly points out, a layered strategy against Covid:
CDC recommends a layered approach to reduce exposures to SARS-CoV-2, the virus that causes COVID-19. This approach includes using multiple mitigation strategies, including improvements to building ventilation, to reduce the spread of disease and lower the risk of exposure. In addition to ventilation improvements, the layered approach includes physical distancing, wearing face masks, hand hygiene, and vaccination.
This layered strategy has been characterized as “The Swiss Cheese Model (of which California educators are aware, at least in Bakersfield):
It is, therefore, deeply ironic that “Outbreak” fumbles its analysis of one of the layers: Ventilation. From the data in Outbreak, we cannot know — pace Bob Wachter — that this is “a case study of why a vaccine mandate is necessary” because we cannot know, from the information before us, how the room was ventilated.[5]
It is also ironic — and I suppose here by “ironic” I mean teeth-grindingly typical — that even though CDC says that it supports a layered strategy, they can’t adjust their messaging accordingly. For example, all they had to do was add two words (which I have helpfully underlined) to their “implications for public health practice”:
Vaccines are effective against the Delta variant, but transmission risk remains elevated among unvaccinated persons in schools. In addition to vaccination, strict adherence to multiple nonpharmaceutical prevention strategies, including masking and ventilation, are important to ensure safe school instruction.
If CDC had done that, all the coverage would have picked that wording right up, as they did the existing wording.
If I were a parent, I would find this whole episode enraging, because none of the players are upholding what, in the Swiss Cheese model, is labelled a “shared responsibility”: Ventilation. I cannot go before the school board and argue for improved ventilation to protect my child based on “Outbreak,” its press clippings, or CDC’s messaging.
Finally, nobody should construe this post as being anti-vax; I am vaccinated and pro-vax. That said, vaccination is but one layer, and multiple layers of protection are critical, in the age not only of Covid, but of variants and breakthrough cases. Vaccinations are not a magic bullet, no more than forms of treatment, favored or disfavored. What I dislike about the press coverage of “Outbreak” is that it makes us more stupid, by reinforcing the PMC’s single-minded focus on vaccination alone. What I dislike about “Outbreak” is that it had the chance to make us smarter, and didn’t. And I dislike the CDC for both reasons.
NOTES
[1] It’s rather remarkable that CDC can present a study that assumes aerosols as the primary mode of transmission en passant, without actually using the word — perhaps the Marin County officials were savvy enough to avoid it — and without incorporating aerosol transmission into their messaging (“It’s like cigarette smoke”) or indeed admitting any error.
[2] The Chinese restaurant study, if the study SFist refers to is the one I am thinking of, was considerably more rigorous than “Outbreak.” The study authors broke down CCTV film to rule out fomite tranmission.
[3] Compare “Outbreak”s “portable high-efficiency particulate air filters” to this followup study on the Skagit Valley superspreading event:
Limited information is available about the heating and ventilating system; what was learned from personal communications is summarized here. The Fellowship Hall is heated and ventilated with a mechanical air heating system including an outdoor air intake and air recirculation. The air handling unit has a relatively new commercial forced-air furnace (see Supplemental Information for the system capacity details). The furnace is installed with an outside make-up air function and it also has a separate combustion air intake, which is standard for gas appliances. But it is not known how much outside make-up air was supplied to the building that evening. The furnace is also outfitted with a MERV 11 filter, which has a rated single-pass efficiency of ≥30%-65% for aerosol particles of diameter 1 µm or larger.29, 30 Three supply air registers are situated 2.4 m above the floor on one wall with a single return on an adjacent wall, just above the floor (~0.15 m). Someone in the front office reportedly turned on the heating system prior to the rehearsal to warm the space, and the thermostat was set to 20°C (68 °F). It was about 7°C (45°F) outside, so the heating was on at the start of the rehearsal, but with so many people in the room, it did not need to stay on to maintain a comfortable temperature. During the entire rehearsal no exterior doors were open. It is not known whether the forced-air furnace fan operated (only) under thermostatic control or whether it ran continuously.
“Portable high-efficiency particulate air filter” seems awfully vague by comparison. What was the rating of the filter?
[4] CDC does not name the school at which the outbreak occurred, nor do the stories linked. There was an outbreak in the May timefrom at Our Lady of Loretto School in Novato, Marin County; “Outbreak” appears to have happened in that school. If so, I am dubious that the windows open fully. Via Google Maps:

The state of California requires all businesses to implement a Site Specific protection plan. I looked at Our Lady of Lorretto’s. It is replete with hygiene theatre. I searched the document for the strings “venti,” “window,” “door,” “filter,” “MERV,” and “air.” “Door” appears once in the context “car door.” “Air” appears once in the context “We will air on the side of caution.” (There is a standard template for schools, which does mention ventilation, but Our Lady of Lorretto did not use it, perhaps because they are Catholic.) At some point, given the open windows and doors described by “Outbreak,” and the filter, their plans changed, but I can’t find any documents explaining why or when. This concerns me, because of Our Lady of Loretto is as fanatical about hygiene theatre as their protetion plan indicates, ventilation may have been an afterthought, and carelessly implemented (as indeed the teacher lowering her mask would suggest).
[5] Yes, I know that Delta is extremely contagious, statistically, and I know that “fleeting contacts” in Australia were sufficient for transmission. However, to the best of my knowledge, those fleeting contacts were not between masked people. It does indeed seem likely to me that aerosol spread from the unmasked and unvaccinated to the masked is the case here, but because of “Outbreak’s” methodological sloppiness on ventilation, we cannot know.


“We will air on the side of caution”
They unintentionally created the slogan of the Good Ventilation Movement! It even beats “To air is human”.
hahahaha!!!
right? They won’t err on the side of correct spelling. Which is a shame for a school.
That is too rich.
I love it
Area sports statistician chimes in:
So a Blue Check Mark™ isn’t a guarantee of quality?
Pandemics don’t build character, they reveal it.
From a friend in Knoxville, TN-
Parents are suing KCS. Zero contact tracing and 10k kids out friday…. Schools don’t even have appropriate cleaning supplies and in many cases covid has them down to one janitor per school. Grainger county schools closed suddenly because they literally don’t have enough staff or bus drivers to even run school.The ICU beds are almost maxed out in both regular and children’s hospitals here and the national guard is here at two of the largest hospitals helping out.
The CDC doesn’t seem very transparent. How do they make their decisions and by who? Maybe a peer review process is needed.
As I recall, the Chinese quarantine infected people and everyone they have interacted with until they are certified as COVID free. It doesn’t sound like they were very aggressive about this in Marin County.
The Chinese took some incredible steps this last round when they were facing a rise in cases that spread to most of the provinces, and it looks like they managed to stop it yet again. They were not only quarantining positive cases in quarantine facilities but were enforcing home quarantines for even some fleeting contacts such as those in an apartment complex. They resorted once again to quarantining whole residential apartment buildings when positive cases show up in the building and cases were spiking in the area. Its pretty incredible to me that most Chinese citizens are mostly cooperating. I understand when they implement the most strict quarantine measures in an area the residents are provided food and other necessities. And someone comes around taking requests for other necessities like medications, etc. Im curious to know if the government is paying people for loss of income every time an area is forced into quarantine. I imagine there is some kind of scheme in place to make people whole but have not come across any reliable info.
The school is Willow Creek Academy in Sausalito. The husband of the teacher had relatives who visited from China the preceding week.
Deja Vu all over again.
When will they ever learn? At least everyone is wearing a mask.
Huh? We have been topping 100,000+ new cases a day driven by delta v. What does that have to do with China? Deja Vu is right, except its for the level of denialism and scapegoating from the early days under the orange man admin. Now its happening under the dopey, sleepy man admin in charge.
> The school is Willow Creek Academy in Sausalito
Needs a link or at least some logic.
Maybe those in favor of vaccinations, among whom I count myself, should stick with the message that being vaccinated vastly improves your chances of not becoming seriously or deathly ill when–not if–you become infected. Not the “happy days are here again” we’ve been primed to hope for, but at least we’ll be around to continue lodging our existential complaints and political critiques.
Assuming some considerable amount of outside air must replace inside air to achieve adequate ventilation, how difficult and expensive is it to ventilate larger buildings in hot, humid, and/or very cold weather or, as is the case here at the moment, where the air is rendered unfit to breathe because of wildfire smoke?
Living as I do in one of world’s milder climates, I’m currently doing fine holed up in my room with an air purifier, humidifier, and air conditioner, which I use only about 20 days per year. While I’ll see a bit of bump in my utility bill, I imagine the costs in harsher climates would be considerably more. Still, that might be cheaper than the hospital bills we’re currently running up, not to mention all the suffering and dying.
“Maybe those in favor of vaccinations, among whom I count myself, should stick with the message that being vaccinated vastly improves your chances of not becoming seriously or deathly ill when–not if–you become infected. Not the “happy days are here again” we’ve been primed to hope for, …”
To naked capitalisms immense credit there has not been any of that triumphant, delusional discourse here when victory was more or less declared couple months back. . Far more clear eyed and honest.
Former school teacher here.
1) We all had to prove vaccination with at least the MMR. I continue to be amazed that Covid vaccination for teachers or healthcare workers is controversial. Even if vaccines’ value against onward transmission were negligible, what are the students going to do while you’re out sick for 2 to 8 weeks?
2) I just noticed that every classroom ventilation diagram show the students lined up in rows. Is that a requirement now for school re-opening, to enhance distancing and improve ventilation?
Row seating hasn’t been the standard since the 1990s at least.
The goal is a mix of small group, pair, and individual work with the desks normally rearranged to accommodate. If students are only able to engage in individual work, that is a big degradation of the learning experience that negates some of the value of in-person learning.
You are apparently not up on the menstrual cycle disruptions the vaccines can cause, including generating heavy periods in women who stopped menstruating years ago. They are more common than the “rare” (as in less than one in a million) blood clots that got everyone freaked out for a while with J&J.
These cases include some women losing their periods entirely. We’ve heard of two cases like that when our contact base skews heavily male and older. Oh, and they have gone to doctors for treatment, and the specialists have no clue.
From a recent post (the “Katie” is a PhD and research scholar, and the press commonly demeans professional women this way, rather than using a honorific and a last name):
Some doctors are pooh-poohing the results as “emotional stressed out women” but heavy and early periods are not a typical stress reaction. Light and/or late is what results. And why would being vaccinated be a stressor, particularly relative to all the other Covid stressors floating around?
The CDC has been utterly silent on this issue, which only feeds worries.
Many reproduction-age women will not risk their fertility to get a vaccine. I’ve heard through multiple channels of nurses quitting hospitals over a vaccination requirement for this reason. I assume the same will prove out at schools.
You had to prove immunity either by record of MMR vaccination or by titer test. Even with the MMR vaccine with its long proven record of high benefit/low risk, it’s prudent to go with the titer test if you have reason to believe you have immunity not reflected in your vaccine record. Young teachers should have this option for the Covid vaccine.
This issue will remain with boosters since many vaccinated people had or will have Covid prior or subsequent to vaccination.
There seems to be an assumption in all of these articles that the vaccines are sterilizing.
That the vaccine isn’t sterilizing was just a month ago a widely disseminated fact that has become one of a number of unmentionable elephants in the room as, I’m just guessing here, it detracts from the wonderfulness of vaccines. Perhaps the assumption in the PR department is that “the vaccine may likely save your life” isn’t sexy enough.
And the teacher could have caught the virus from an asymptomatic person – vaccinated or unvaccinated.
The teacher would have just needed to be around them long enough at the right time to catch the viral load.
I’m old enough to remember the rollout of the measles vaccine. ISTR that it was in 1965. By that time, I’d already experienced and recovered from both types of measles. And I *think* that my parents also had measles when they were children.
In short, the *Pennsylvania* Slim household had immunity to the measles.
However, a nearby shopping center hosted event called End Measles Sunday. Since this was in Pennsylvania and the Blue Laws that closed most retail businesses on Sundays were in effect, there was no problem with holding a mass vaccination event in the shopping center parking lot.
Note the name of the event: End Measles Sunday.
It wasn’t Reduce Your Child’s Risk of Serious Illness Sunday or Mess Up Mom’s Menstrual Cycle Sunday. It was an event that was about eradicating this terrible disease called measles.
In the weeks and months that followed, I never heard anything about kids or adults who got the shot but came down with measles anyway. Or people experiencing oddball side effects.
And we kids were a bunch of blabbermouths, a trait we’d gotten from our parents. If something was amiss, we’d certainly be talking about it.
The reason there weren’t many breakthrough measles infections was that the virus was not saturating public spaces the way Covid is now, due to widespread natural immunity on top of vaccinations.
No vaccination is 100% effective and these vaccines are getting a lot of virus thrown at them.
As for concerns about MRNA vaccines, how did J&J get thrown under the bus like this? It’s like it’s been memory-holed.
Perhaps it is not so much delivering the spike protein making instructions by Mrna vs. by an engineered adenovirus that causes the worst side-effects, rather the making and releasing of said spike proteins throughout the body.
What chance is there old fashioned attenuated virus vaccines developed in other places (like the Chinese ones?) will be approved for US use?
When did large numbers of people get the J&J shot? I remember Virginia Governor Northam, a MD, had a J&J shot when it came out but it was after my first Modern, March 8th which puts me six weeks out from six months from my second shot. There really was an solid two months of large numbers of people getting shots, some even longer. I sort of remember the J&J shot being out just not available.
Not that many people especially the more vulnerable populations had J&J shot comparatively. I checked there are stories out there about boosters for J&J, but I suspect this is people asking about their own shots.
> If I were a parent, I would find this whole episode enraging, because none of the players are upholding
> what, in the Swiss Cheese model, is labelled a “shared responsibility”: Ventilation. I cannot go before the
> school board and argue for improved ventilation to protect my child based on “Outbreak,” its press
> clippings, or CDC’s messaging.
But that would cost money. We can not do the right thing if it would cost money! We should do everything we possibly can, including Academy Award winning hygiene theater, however useless, so long as it is inexpensive. Because money is more important than everything else. We can not spend money to save ourselves harm, it would be impractical!
See also all cries to reopen ever, why you haven’t put solar panels in your roof, insisted on a EV, or done other right things.
I’m not a communist yet, but damn if humans aren’t depressing and very, very predictable.
I suppose I should go see about that industrial strength HEPA filter I bought for my daughters class room but haven’t given to the school yet….
I live in the Bay Area and I had the same thought when I read the headlines i.e no one’s saying anything about ventilation.
Well this is after the CDC that went from “we are all going to die!!!” to “let’s open everything up” in two weeks time.
Also, there is no mention of the utter debacle of coronavirus testing in the USA. There would be no outbreak at all if there had been a school bubble like professional baseball and the teacher had a quick free accurate antigen test before leaving for work and if positive being paid to stray home for 2 weeks until infection free. In addition, if daily testing is coordinated with comprehensive contact tracing and quarantines plus social distancing, masks, personal hygiene and ventilation; coronavirus would be eradicated in the USA in two months. China, Taiwan and New Zealand are doing it.
Shaming the unvaccinated is public/private propaganda required to avoid Americans blaming the ruling class for their corruption and incompetence.
> the utter debacle of coronavirus testing in the USA
I should look for a world ranking of testing. I bet we’d be pretty low.
GM commented that all efforts at quick testing were halted late last year when the “decision” was made (somewhere) to “let it rip” and go endemic.
MIcheal MIna, who was involved in some early testing development, and a staunch advocate last year, has gone silent on the issue.
Just like Dr John Campbell, who was very impressed with Tess Lawrie’s meta on IVM, has gone silent on it. His only comment on the UK opening up “Apparently we aren’t going to do antivirals…”
Not to get all foily, but there is stuff going on behind the scenes.
What if there a people who catches the virus is going to be a superspreader whether they are vaccinated or not or asymptomatic or not?
While others won’t be?
Is everybody really capable of being a superspreader?
I don’t really like the term, but just a wild consideration…
“if there are people who catch”….
Writing whlie rolling out of bed…
Yes, and this is probably true of almost all airborne respiratory diseases. It’s only suprising if you don’t ‘believe in’ airborne transmission.
The phenomenon is very much one of ‘wrong place, wrong time’, less so one of the individual characteristics of the infectious agent and very much less those of the infected individual.
The incessant push for vaccination introduces lots of noises and prevent doing the correct thing. The index case was symptomatic by May 19th… without reporting!!! This is the biggest mistake and it should be researched why the teacher didn’t report. Fear about getting fired, because was not vaccinated? Showing symptoms the incumbent still went to the classroom on 19th, 20th, 21st (this day finally went for PCR test), and May 22nd On 23rd he was notified positive and apparently didn’t show up. The pupils started showing symtoms by 22nd suggesting they could be infected by 18th-21st.
1.The moment a teacher shows symptoms compatible with COVID, he or she should communicate the school and stay home without needing a positive test. Precautionary principle. This wouldn’t have prevented all the contagions but possibly most of them. Parents should have been notified: there is some risk SARS CoV 2 has entered the classroom. PCR tests conducted on all pupils by 19th or 20th. Now, with Ag tests available, the teacher could have done it by himself the first day showing symptoms and communicate to the school the result.
2. The classroom mates and their families should be informed, masks made mandatory for them both indoors and outdoors and each family could decide whether their children might stay home for a couple of days or not. For instance if you have someone at home that might be vulnerable take special measures. Notify the school at the onset of symtoms or any positive/negative test.
For me the conclusion to take about this outbreak is not mandatory vaccination required but proper notification and contact tracing protocols that seem not to be in place. If there is a protocol and, for instance the teacher was mandated to report any symptom and didn’t this would be her/his fault, rather than the vaccination status. There must be flow of information. In this way you might limit the size of the outbreak and control it. Yet, the only conclusion taken by the media is vaccination, vaccination, vaccination!
I can tell, by my own experience that not hiding the truths is the best way to prevent spread.
> not hiding the truths is the best way to prevent spread
No doubt. What is this “testing and contact tracing” of which you speak?
> The incessant push for vaccination introduces lots of noises and prevent doing the correct thing
“Fundamentally, nothing will change.” I think that’s the real politics of vax, hence the desperate assumption that sterilizing immunity was in the cards in “our vaccine journey” (modulo something clever with the mucosal immune system).
Hahahahahaha!
“Fundamentally, nothing will change.”
Yup. God forbid we do something anything truly radical proportional to the scale of the threat we face.
There is a now a modeling literature on mean residence time distributions of viral aerosols (aided by computational fluid dynamics), that emphasizes the key interaction of viral concentrations in biological fluids, droplet size, humidity, and overall volumetric air exchange rate (AER). A recent paper[1] concludes that increasing AER is key, as residence times (thus risk of individual uptake) decrease monotonically with increased ventilation rate. IOW, effectively decreasing overall transmission risk may be more a function of really dialing up the ventilation, and not so much trying to capture ultra fine particles (small droplets more likely to be blanks, larger particles settle rapidly).
1. https://onlinelibrary.wiley.com/doi/10.1111/ina.12868
I think the bottom line is that U.S. measures against COVID are not adequate at all. Americans are going to be jumping through these half-measure hoops until they get fed up and get really serious about stopping the disease. We don’t seem close to that point.
6 Questions To Ask Your Colorado School About COVID And The Air In Your Child’s Classroom
I don’t think I’ve seen this linked here: https://www.cpr.org/2021/08/27/colorado-schools-covid-air-filtration/
Fantastic article! Thank you
Second
The prevailing story is the only story our captured media is interested in. Adequate ventilation in buildings that were never designed to have fresh air costs too much. Masks are scary. Testing, Contact tracing, quarantine, etc is too expensive (an not just because sick leave is too much for employers, employees are left in the lurch)
So our misleadership class have decided inadequate vaccines will have to do because nothing can fundamentally change as Lambert and others have noted. And any scary out breaks must be because of someone not vaccinating. (Mark my word any outbreak that cannot be played that way will be ignored or downplayed as a non life threatening aberration before fading from public view.
(I think they are quickly reaching critical cognitive dissonance, but that may be just me.)
Aside from the vaccinated there is no evidence that Covid-19 existed. Covid-19 is never isolated. See Jon Rappaport citing even the CDC saying no isolated virus. No nation, no lab has an isolated virus. Autopsies are not done on the dead. The PCR test is fraud. The CDC, WHO are criminal organizations. Vaccination with EUA is criminal.
https://noqreport.com/2021/08/28/deaths-in-80-vaccinated-uk-up-tenfold-from-this-time-last-year-when-zero-were-vaccinated/
The talismanic value of the vaccines has become quite incredible. When the data clearly shows that the vaccinated can be just as infectious as the unvaccinated, what is the point of enforced vaccinations for a public health standpoint?
Certainly they have value at preventing serious disease, but they certainly do not prevent infection (reliably), don’t even prevent pretty serious disease in many cases.
And if you wait long enough, data seems to show that the protection largely disappears (at least, the easy to measure antibodies do).
So like holy water, they are being pushed as magical.
A vaccine “passport” proves what? exactly? You might be less likely to get really sick if you get infected. Nothing more than that. Meaningless from the standpoint of protecting others.
I notice that the Marin layout meant that the kids near the windows were better off and the ones downwind of the teacher on the way toward the door all got it. The only explanation that I can see why huge vent ducts were not put on the ceiling and vented to the outside via one of the windows is that there would be a large increase in HVAC energy costs to condition the incoming air being moved through the hallways. But, come on, this is Marin County, damp and foggy in the morning and rarely very warm or cold. Suck it up parents- and administrators; make the kids bring sweaters.
I just came back from a five-day convention in Houston. OK, I’ll admit it; it was the world gathering celebrating the 75th anniversary of Mensa. Maybe 1,200 people in a Hilton hotel. In the elevators everyone was masked with no exceptions I saw. In the large meeting rooms people were usually separated by two seats and maybe an empty row; ~75% were masked and when I wasn’t I sat away from people. People were very considerate. The Hilton had almost uncomfortably cold, dry air from 20-30 feet above around the sides of rooms and a fast turnover rate. The hotel staff was masked at all times, even in the back-room kitchens.
In the huge hospitality room (½ of a ball room) everyone entering had to have a mask on; in line to get food everyone was masked. At the 6-7 seat round tables most people were separated by one chair and had masks off. The ventilation was as good as in the meeting rooms.
A number of the speakers touched on Covid but by far the most informative for me was Dr. Subinoy Das, an ENT doctor and apparently a researcher in Ohio. His lecture was titled “The Science of Smell Loss. With apologies to Dr. Das for any mistakes I’m making, here, based on my notes, are some comments:
1) One virus particle doesn’t give you Covid. You need to take in a significant load of particles The worst case is an infected person yelling or singing in a confined and poorly ventilated space who expels a huge package of aerosolized particles singing and yelling. Air turnover is the key, which is why outdoor events with even a slight wind appear to have minimal transmission IF the people are properly spaced (the last sentence is my interpretation of what he said in a roundabout way, so take it with caution).
2) Covid does not directly attack the nasal smell receptors; but it rapidly (within 1-2 days) can destroy the support cells and stop a person from smelling. Dr Das was a bit disturbed that this was not being used as a test. Temperatures usually go up on the 4th and 5th day- very late; a simply alcohol swab held under the nostrils and sniffed can detect many (most?) Covid on the second day. If you can’t smell it you probably have very early Covid, which is far easier to treat. Luckily, the support cells are constantly being regenerated, so the loss of smell slowly is reduced and often ended within 60 days. For those who continue to have loss of smell, there are fairly simple ways to retrain the sense of smell; look up “olfactory training”.
3) Mouth breathing and nose breathing lead to different results. Nose breathing produces laminar flow, so the Covid particles are more likely to go straight to the lungs. Mouth breathing is less laminar and many particles lodge in the throat. If the viral load is low, this may produce a sore throat and the antibodies are more likely to multiply fast enough to contain the Covid- almost like a mini-vaccination. There appears to be little-or-no skin to skin transmission.
4) High viral load and immune systems that are weak and slow to react give Covid a head start. When those immune systems finally react on approximately the 8th day they overreact producing a “cytokine storm” which can damage organs and lead to death. The old, the immune compromised, the overweight, the under-exercised, diabetics and smokers are at serious risk. The conclusions I draw are that the recycling of air and the weakness of the inhabitants may be responsible for the sad early disaster in the nursing homes.
There appears to be little-or-no transmission by hands or surface contact. Aerosols are what matter. Large particles drop out of the air quickly but the small ones stay aloft for some time and don’t drop. Thus my conclusion that large overhead air intakes that empty a room of air rapidly and outside air intakes are almost mandatory. Lambert is right. The good news is that a decent HVAC crew can install ducts in a school over a weekend. The big increases in Covid in the humid south appear to be caused by low turnover of air in conditioned spaces. In very hot or cold regions this could be a real problem because of cost and new HVAC equipment. But it may only mean kids in MN may have to leave their coats on in 55 degree rooms and in Arizona they may sweat a bit in 80 degree rooms. And no screaming and yelling in the corridors or in the schoolyard.
And masks do make a difference by both reducing the viral load breathing in and by reducing the load sent out by those infected.