By Lambert Strether of Corrente
CDC, and the public health establishment generally, promote a paradigm of “personal risk assessment” that will enable you to “live with” Covid. Implicit in that social contract is that CDC will provide the necessary data for you to make the assessment; obviously, an individual isn’t going to be personally tracking case counts, or new variants, or dipping into their local wastewater to run tests. Leaving aside the viciously neoliberal and eugenic[1] character of the paradigm, CDC is also failing to uphold its end of the bargain (and not for the first time).
In this post, I’ll examine CDC’s latest betrayal: Its failure to alert the public to a rapidly doubling new variant, BQ.1.* (BQ.1.* includes both BQ.1 and BQ.1.1.) First, I’ll establish that BQ.1.* is a variant that you should be concerned about. Next, I’ll look at the timeline that shows CDC’s failure to warn. Next, I will do a post mortem on whether CDC’s latest betrayal is attribute to persons (“malevolence”) or institutions (“operational incapacity”). Finally, I’ll look into CDC’s operational incapacity more deeply, in particular the CDC’s reliance on a small team of volunteers for its variant data.
The Danger
BQ.1.* is a dangerous variant. It is characterized by rapid doubling time. From Reuters:
U.S. health regulators on Friday estimated that BQ.1 and closely related BQ.1.1 accounted for 16.6% of coronavirus variants in the country, nearly doubling from last week, while Europe expects them to become the dominant variants in a month.
“These variants (BQ.1 and BQ.1.1) can quite possibly lead to a very bad surge of illness this winter in the U.S. as it’s already starting to happen in Europe and the UK,” said Gregory Poland, a virologist and vaccine researcher at Mayo Clinic.
Here is a chart that shows doubling time since the beginning of the pandemic:
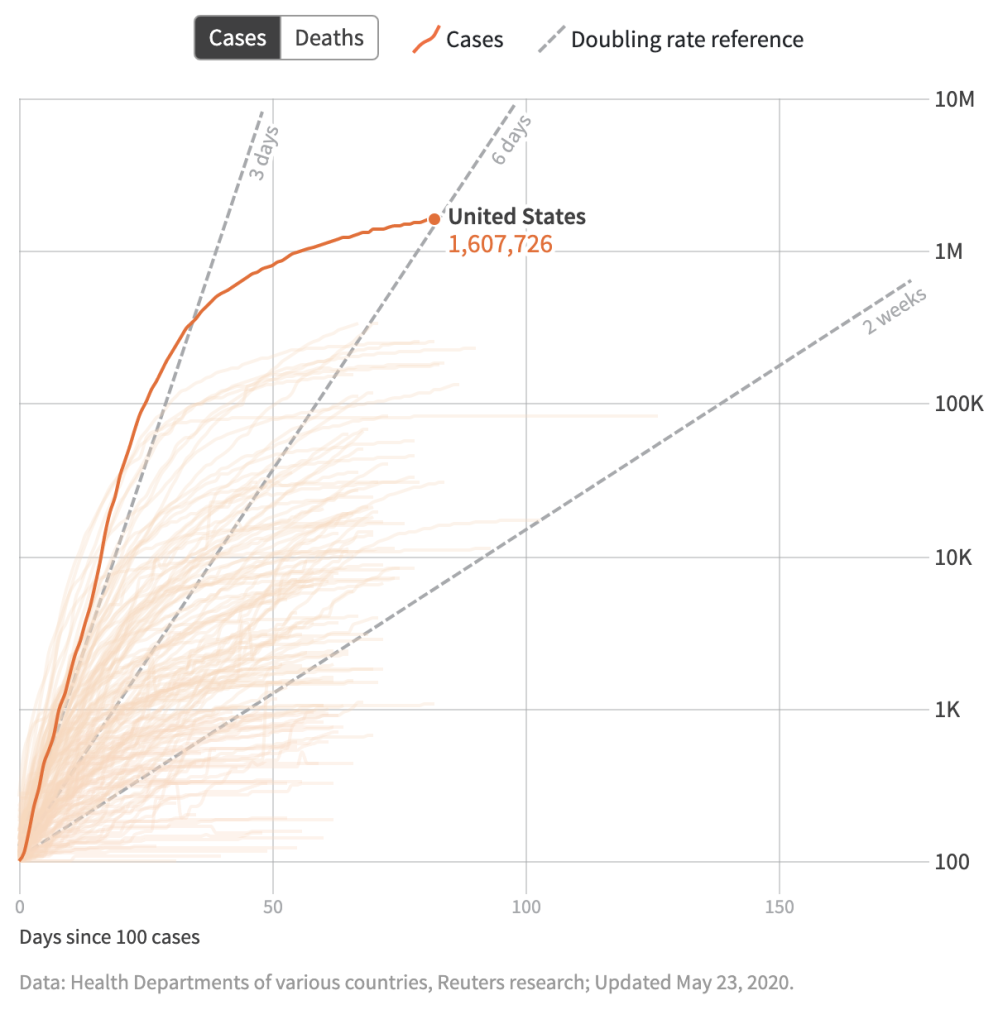
As you can see, even a week is a long time when the virus is getting rolling. To be fair, the United States population is not the same population it was in 2020, when Covid first hit: Many more people have acquired immunity, many more are vaxed, most have different combinations of immunity and vaccination, and so on; we are no longer, as it were, virgin territory. Which makes BQ.1.*’s next characteristic all the more important–
BQ.1.* is immune evasive (that is, previous infection does not protect from a second infection). From Fortune:
BQ.1.1 is thought to be the most immune-evasive new variant, according to Dr. Eric Topol, a professor of molecular medicine at Scripps Research and founder and director of the Scripps Research Translational Institute.
BQ.1.1’s extreme immune evasiveness “sets it up to be the principal driver of the next U.S. wave in the weeks ahead,” Topol tweeted Friday.
On Thursday, he told Fortune that scientists won’t know to what extent it challenges vaccines, if it does, until it reaches 30%-50% of cases somewhere.
“It’s not going to wipe out vaccine efficacy, but it could but a dent in protection against hospitalizations and death,” he said.
(Wait. Since vaccines don’t prevent transmission, I thought protection against “hospitalizations and death” was the reason to het them?
Next, BQ.1.* renders some treatments obsolete. Fortune again:
BQ.1.1 is already known to escape antibody immunity, rendering useless monoclonal antibody treatments used in high-risk individuals with COVID. According to a study last month out of Peking University’s Biomedical Pioneering Innovation Center in China, BQ.1.1 escapes immunity from Bebtelovimab, the last monoclonal antibody drug effective on all variants, as well as Evusheld, which works on some. Along with variants CA.1 and XBB, BQ.1.1 could lead to more severe symptoms, the authors wrote.
Finally, New York City is under the gun. From Becker’s Hospital Review:
Health experts are carefully watching COVID-19 trends in New York amid signs the nation will face a winter surge. The state has seen an increase in hospitalizations over the last month.
Statewide, the daily average for COVID-19 hospitalizations is up 15 percent over the last two weeks, according to HHS data compiled by The New York Times. As of Oct. 20, an average of 3,095 people were hospitalized in New York. On Oct. 2, that figure was 2,614.
The increase in hospitalization rates comes as a pair of omicron relatives dubbed “escape variants” gain prevalence nationwide. The strains — BQ.1 and BQ.1.1 — are most prevalent in New York and New Jersey, where they account for nearly 30 percent of new infections, according to CDC estimates for the week ending Oct. 22. BQ.1’s rising prevalence may be driving the jump in hospitalizations, but scientists say it’s still too early to confirm a causal relationship.
While hospitalizations appear to be trending upward in New York, cases have remained relatively flat throughout the month. This discrepancy highlights the difficulty of monitoring virus activity in an era of unreliable case data and a departure from daily reporting cadences.
(Ya think? How’d that happen?)
For those of us who remember the very first Covid wave in 2020, this is worrisome. From Fortune:
New York is a veritable crystal ball when it comes to COVID forecasting for a couple of reasons: its volume of incoming international travelers, and its robust capabilities to genetically sequence COVID virus samples, experts say.
When a variant gains traction in Europe, as the BQ family has, trackers like Rajnarayanan and Gregory know to look for it in the U.S. The first place they check: New York.
Together, Omicron spawn BQ.1 and BQ.1.1 are “following the same script” as other previously dominant variants—like the original strain of COVID, Delta, and the original strain of Omicron—by starting a swelling in the northeast that could eventually wash over the rest of the U.S., fellow variant tracker Dr. Ryan Gregory, a professor of evolutionary biology at the University of Guelph in Ontario, Canada, told Fortune.
(Well, if the spread follows the pattern of 2020, the first places to track are the Hamptons and the Hudson Valley, as those who can leave, leave.)
If I am to make a personal risk assessment about flying into New York — as indeed many PMC, flying (unmasked) on planes, or attending (unmasked) conferences will do — I really need to know that a dangerous variant is exhibiting doubling behavior there. And I need to now it now, ASAP, because the variant’s doubling behavior means a week, let alone two weeks, is far too long. Unfortunately for many, CDC failed to give timely warning. Let’s look at why..
The Timeline
Here is the timeline for CDC’s “reveal” of BQ.1.*.[2] From Fierce Healthcare (and kudos to them for explaining so clearly a story that has yet to appear in [genuflects] the Times or the Post):
The highly infectious and evasive BQ.1.1 variant not only has a foothold in the U.S., it may have established that foothold weeks ago. The data on the variant have prompted the Centers for Disease Control and Prevention (CDC) to redo previous weeks’ variants tracking charts.
“It’s been hiding in plain sight,” Kevin Kavanagh, M.D., founder of the patient advocacy group Health Watch USA, told Fierce Healthcare.
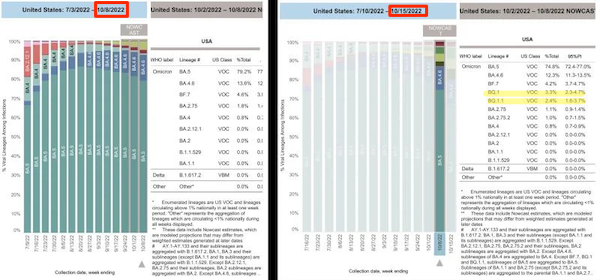
The charts below tell the story. The left shows the first version of CDC tracking data for the week ending Oct. 8, where BQ.1.1 (and its cousin, BQ.1) don’t even appear. The CDC had grouped those data under the BA.5 label, which has been the most dominant subvariant of omicron since early July.
After examining additional data, the CDC this week reconfigured the chart to show BQ 1.1. accounting for 2.4% of new cases of COVID-19 for the week ending Oct. 8 and BQ.1 accounting for 3.3%.
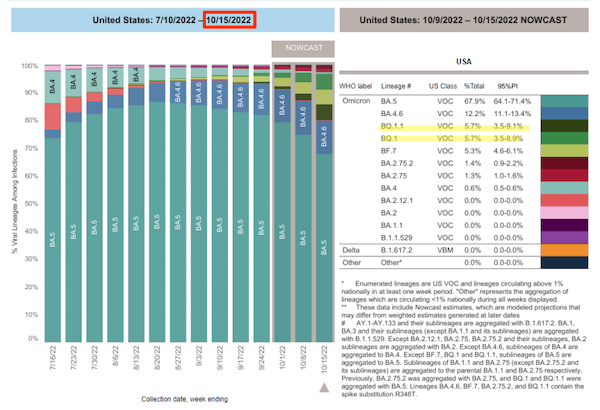
Now look at the chart for the week ending Oct. 15. Both variants now account for 5.7% of new COVID-19 cases in the U.S.
Kavanagh said BQ.1.1 “appears to be doubling every week. Data from CDC appears delayed in being posted on this variant. Once it became apparent in the last few weeks that the variant is having a significant impact, the data were separated.”
So, the doubling behavior of BQ.1.* was hidden by being aggregated with the declining BA.5’s data. At some point after October 8, CDC disaggregated them, and BQ.1.* became visible. Being as charitable as possible to CDC, it got the data out a week late (October 15, not October 8), but as I point out above, a week is too slow. If one wishes not to be charitable, CDC’s internal deliberations took far too long (“it became apparent in the last few weeks”). How did this happen?
The Post Mortem
There are at least to reasons CDC failed to warn the public about BQ.1* in a timely fashion: Malevolence, and operational incapacity.
Taking malevolence first, from WSWS:
On Friday, the US Centers for Disease Control and Prevention (CDC) updated its variant monitoring graphs to show that the highly contagious and immune-evasive descendants of the Omicron BA.5 subvariant, known as BQ.1 and BQ.1.1, now account for a combined 11.4 percent of all sequenced variants.
However, the “update” came one day after epidemiologist Dr. Eric Feigl-Ding tweeted these same data, which he noted were leaked to him from a “CDC-insider source” which informed him that the CDC had been sitting on this crucial information regarding the state of the variants in the US. After Feigl-Ding’s tweet went viral, garnering over 10,000 likes and over 5,000 retweets within hours, the CDC was forced to release the data publicly.
This is among the most significant cover-ups by the foremost health agency in the US since the start of the pandemic. It is clear that the CDC deliberately concealed this vital information from the public for weeks, as part of the relentless propaganda campaign by the Biden administration and the corporate media to falsely claim that “the pandemic is over.”
Well, CDC data drops every Friday, at a stately once-a-week pace. Readers know, I am sure, that I hold no brief for the CDC. However, there’s a good deal of handwaving in WSWS’s post, which I have helpfully underlined; sequence and causality are not the same. In particular, I doubt very much that a Tweetstorm can cause CDC to do anything. If it could, Rochelle Walensky — bless her heart — would be recommending masking because #CovidIsAirborne. I also note that WSWS seems to have no knowledge of how CDC variant data is actually collected.
That brings us to operational incapacity. Reporter Alexander Tin found a transcript of CDC giving its version at a webinar with testing labs on October 17:
NATALIE THORNBURG, CDC [00:22:55] And then last week, we had an update where we added three additional sublineages [including the two BQ.1.* lineages] to the data tracker.
And just a reminder, when we decide the reason we decide to break things out, sublineages out on the data tracker, we have a couple of criteria. One, it has to reach at least 1% prevalence nationally. Two, it has to have medically relevant substitutions. So it has to have substitutions that could show a reduction in neutralization titers, have some effect on– we haven’t really seen diagnostics, but have some effect on diagnostics or therapeutics. But what we’ve really seen most– most often is substitutions that could affect neutralization. And then of course, we need a method for identifying those sublineages.
So early last week, Pango, which is our software that we use to call lineages, released an update that allowed us to call BQ.1 and BQ.1.1 sublineages of viruses, as well as BA.2.75.2
So CDC’s defense is that they did not have the operational capacity to disaggregate BQ.1.* until they got the data from Pango[lin][4], at the usual stately every Friday pace. the Hence the following subtweet directed at Eric Fiegel-Ding:
Virtually all of the underlying seq data are available to the public, and emerging variants are quickly flagged and discussed on scientific forums (& by experts / citizen scientists on Twitter)!
This conspiratorial, clout-chasing nonsense is dangerous and a disservice to us all.
— Duncan MacCannell (@dmaccannell) October 14, 2022
Personally, I lean toward the operational incapacity explanation, because it’s more stupid, and this is the stupidest timeline. Readers may differ! In any case and as usual, The Onion has the story covered: “We Have Coronavirus Under Control,’ Announces CDC Director As Nose Slowly Transforms Into Pangolin Snout” (from 3/05/20 (!!)). But what is Pangolin?
How Pangolin Shows CDC’s Operational Incapacity
Pangolin is a suite of open source software (lead developer; README):
Pangolin was developed to implement the dynamic nomenclature of SARS-CoV-2 lineages, known as the Pango nomenclature. It allows a user to assign a SARS-CoV-2 genome sequence the most likely lineage (Pango lineage) to SARS-CoV-2 query sequences.
It is available as a command line tool and a web application. The web application was developed by the Centre for Genomic Pathogen Surveillance. The command line tool is open source software available under the GNU General Public License v3.0.
(I am assuming that the WebApp somehow uses the command line tool on the backend, hence is GPL’ed, too. Pangolin includes a machine learning component, UShER, also GPLed).
Before going any further, let’s just ask the basic question: Why doesn’t CDC get the Pangolin volunteers some money so that they can speed up their work?! This every Friday drop just doesn’t make it, because the doubling capacity of the virus can outrun it.
Now let’s look at the instituional set-up for Pangolin (and please note that I have nothing but the utmost respect for the skills of the developers, or the power and beauty of their work). From MIT Technology Review:
[the Pangolin project is] a GitHub page staffed by a handful of volunteers around the world, led primarily by a PhD student in Scotland.
Those volunteers oversee a system called Pango, which has quietly become essential to global covid research. Its software tools and naming system have now helped scientists worldwide understand and classify nearly 2.5 million samples of the virus.
Researchers, public health officers, and journalists around the world use Pango to understand covid’s evolution. But few realize that the entire endeavor—like much in the new field of covid genomics—is powered by a tiny team of young researchers who have often put their own work on hold to build it.
Many of the foundational tools for tracking covid genomes have been developed and maintained by early-career scientists like O’Toole and Scher over the last year and a half. As the need for worldwide covid collaboration exploded, scientists rushed to support it with ad hoc infrastructure like Pango. Much of that work fell to tech-savvy young researchers in their 20s and 30s. They used informal networks and tools that were open source—meaning they were free to use, and anyone could volunteer to add tweaks and improvements.
“The people on the cutting edge of new technologies tend to be grad students and postdocs,” says Angie Hinrichs, a bioinformatician at UC Santa Cruz who joined the project earlier this year.
So, just to be clear, CDC has outsourced the essential technology for variant detection to volunteers[5]. (And what is the key characteristic of “grad students and postdocs”? They need to move on.) CDC has bet thousands of lives, perhaps tens or hundreds of thousands, on volunteers. Does that sound like a sensible approach to you? Why the heck, again, can’t CDC get them some kinda budget? What happens when the developer gets a better offer? Or moves to another institution? Do people at CDC think that complex open source software is maintained by little elves? Does this sound like operational capacity to you?[6]
Conclusion
I wouldn’t be so worried if CDC and the public health establishment hadn’t systematically ignored or discredited all forms of non-pharmaceutical intervention, and vax uptake was not at a standstill. But here are are: CDC delenda est. Burn the facilities, plow the rubble under, salt the earth. There’s no excuse for any of this.
NOTES
[1] The ability to assess personal risk is strongly correlated to income, which in turn is driven by class and “social determinants of health” generally. Yves’s helper Betty Jo, for example, who is dedicated to masking, ventilation, and Povidone iodine, won’t be running Bob Wachter’s complex risk assessment algorithm anytime soon; she’s too busy. Hence, stochastic eugenics.
[2] These screenshots have CDC’s NowCast algorithm on. I keep it off, because I don’t trust CDC’s models, based on experience. In some ways, NowCast makes CDC even more culpable; if you have model capable of predicting doubling behavior, why not reveal it?
[3] Here is the argument that CDC should have disaggregated the data much earlier, say on September 24:
2. "(…) with BQ.1 exceeding one percent of all sequenced variants on September 24 and BQ.1.1. reaching that threshold by the week of October 1. By the CDC’s rules, they have to break out these newer strains from all the ones being tracked and list their frequency." pic.twitter.com/J1IvUy6CBt
— Nancy Delagrave | Covid-Stop (@RougeMatisse) October 17, 2022
However, we’d need more evidence that CDC was aware that BQ.1.* had passed the 1% threshold than a screenshot of the current chart, since CDC “backfills” the charts when new variants are disaggregated:
New CDC variant Nowcasts:
– BQ.1 and BQ 1.1 combined are now ~17% of new cases (up from 9.4% last week)
– BA 4.6 consistent from last week
– BA.5 is 62% of new cases (down from 70% last week)Note that CDC has always backfilled as sequences are received.https://t.co/xuOF2fkHPS pic.twitter.com/mYTDDbB32L
— Benjy Renton (@bhrenton) October 21, 2022
[4] The chart in this Tweet purports to show that CDC is slower than private labs:
This chart shows that the CDC is sitting on variant data for 2-3 weeks while state, university, and private labs are getting results and submitting them to a global database within 5-10 days.
The CDC has been sitting on these data for weeks. pic.twitter.com/vThbzVBUbZ
— Dr. Jorge Caballero stands with 🇺🇦 (@DataDrivenMD) October 14, 2022
But I can’t understand the chart, which is why it goes in a note. Readers?
[5] The Technology Review article is 2021, and that is the most recent version I can find. UShER, the GPLed Pangolin component, was run by volunteers in 2022.
[6] Maybe put the United States Digital Service on the case? Not to rewrite the code, but to straighten out the obvious oncoming trainwreck in getting Pangolin maintained? Without, please gawd, privatizing it in Big Pharma’s loving embrace?


Well, from reading about Welensky and her dad’s companies today here on NC, I have a pretty idea why Welensky even has a job and the incompetent government response.
How many people are hospitalized or dying from this new variant? Eric Topol’s data says the death rate: 8 in 100,000 (.008%) in the unvaccinated. Hospitalization 50 in 100,000 (.05%) in the unvaccinated. Those are his charts, not mine, from his substance article from this morning.
I do not care about cases, I care about outcomes. By all means, mask and ventilate, but I just cannot see the concern.
Sorry, can someone please school me if this is wrong?
Well for one thing, the numbers you are citing (https://erictopol.substack.com/p/a-booster-is-your-best-shot-now) are from July 2022 — i.e. the BA5 wave — long before the BQ variants. The only BQ-relevant information is the “anecdata” that “In New York, where there is the highest per cent of BQ.1.1 in the US, there is already a higher rate of Covid hospitalizations than had been seen since the Delta wave.”
So it will take more time to see just how bad BQ is compared to BA. Though at 5-10% of cases if it were significantly worse I suspect we’d be hearing some scuttlebut from medical professionals about a “deadlier” strain.
The word “case” really bothers me, and here’s why:
Exactly what is a case? Is it someone hacking, coughing, and having a runny nose that looks like Niagara Falls? Or is it just a mild round of the sniffles?
My Naked Capitalism-honed critical thinking skills are leaping into action, and they have questions about the definition of “case.”
I believe it’s a confirmed SC2 infection, confirmed either by positive PCR or positive RAT – more likely the latter now. I don’t think symptom presentation has anything to do with the definition of a case. Someone with a confirmed infection – a case – might still be completely asymptomatic. Likewise, an infectee may be completely asymptomatic and not test, and therefore not be a case (on similar grounds, there is a difference in definition between a Case Fatality Rate and Infection Fatality Rate). In the long run, this will be a problem for a disease which can cause sub-clinical damage (to the brain, vasculature etc)
Well, the current outcome has been 3-4 million people out of the workforce with long-COVID. This from Brookings, I think, not exactly a fringe think tank nor one that’s particularly concerned with the fates of working people.
Those questions from the CDC that Brookings Institution used, give me a break.
https://www.cdc.gov/nchs/covid19/pulse/long-covid.htm#technical_notes
I wouldn’t consider that a diagnosis of long Covid at all.
And don’t get me started with all the Pfizer people that are also on the board of the Brookings Institute.
James Smith and Suzanne Johnson are just too, that I found right off the bat.
So your position is the number is too high? Or no such a thing as long COVID? Other sources in other countries also claim long COVID is affecting employment levels. Is this also false?
You posted a dodgy long comment I had to rip out because Making Shit Up. Now you are getting nasty. If you don’t shape up pronto, I will blacklist you. Your behavior has been barely acceptable for a while and I’ve been cutting you way too much slack.
On what grounds, and under what authority?
LC remains a bit of a nebulous entity in the popular imagination, unsurprisingly for such a young and multifaceted disease that we are still trying to come to terms with, but those survey questions accord pretty well with working clinical definitions of LC that have been in place for nearly two years now.
It was many years before the medical community agreed that Chronic Fatigue Syndrome was a condition and not psychological, and then was also quite a while before they agreed on a symptom profile.
> 3-4 million people
Regardless of the exact number, I think a good answer is “an appreciable percentage of the workforce”
> Sorry, can someone please school me if this is wrong?
Vascular and neurological damage even in “mild” cases, cumulative over multiple infections. And, of course, Long Covid. Does this help?
Fierce Healthcare link is broken, I think you mean: https://www.fiercehealthcare.com/providers/highly-evasive-bq11-appears-cdcs-covid-19-variants-charts-first-time
Thanks!
For what it’s worth, BQ.1.1 has a pretty cool nickname that could be useful for anyone trying to track this stuff through media, and there is a lot of coverage of this one, although it’s in Russian:
Nicknamed “Cerberus”: scientists talk about a new type of coronavirus
October 11, 2022
Very little time has passed since the discovery of the omicron variety,a strain of coronavirus known as Centaur or BA. 2. 75, which has infected almost the entire world and reached even to Moscow. And now we face a new threat. Scientists are already talking about the ultra-fast spread of a new version of the same “omicron”, which is unofficially called “Cerberus” (in ancient Greek mythology – a ferocious three-headed dog of the god Hades, guarding the entrance to the realm of the dead). It was given the designation BQ.1.1.
По прозвищу «Цербер»: ученые говорят о новом виде коронавируса – ФармМедПром
pharmmedprom.ru › news-koronavirusa
> BQ.1.1 has a pretty cool nickname
“BQ1” is in fact cool; it sounds like a K-Pop or J-Pop band name
Well, both are infectious, I suppose. Now I really have to worry about what it is doing to our young people– not good!
Somehow this self-made October Surprise, along with Asian AGW rectifying equities & EU gas supply & ensuing inflation/ recession will be blamed on divisive Left purists, or Putin or anysomebody NOT “our” smug, senile zombie kleptocrats lining their bloated pockets?
https://mobile.twitter.com/lorrrraaaaine/status/1584535019615580161
Is there any reason not to aggressively FOIA the [redacted] out of the CDC all the damned time to try to make their
sins-of-omission narrative management more difficultvital communications about public health to be more transparent and more honest? It’s really interesting to watch conservative groups perform targeted FOIA requests to force governmental disclosures, but for a broad public health issue like CDC infectious disease messaging this there seems to be no organization dedicated to the same…> Do people at CDC think that complex open source software is maintained by little elves?
By the premises of neoliberal ways of thinking about “the human project”, public-spirited open-source volunteer collaborations shouldn’t even exist. So yes, these projects have a kind of magical quality to them, from the perspective of very serious people.
—
Thank you, Lambert.
I am greatly encouraged by the people behind Pangolin. Maybe some of them could work for CDC in future, after the current crop of administrators and thought-leaders have been incapacitated with Long COVID.
I, cynic that I am, do have an outre optimism in that I hope for a cadre of these “volunteers” to band together and produce a ‘hack’ that will tangle up and incapacitate Wall Street and the Big Banks. I call it ‘Stoxxnet.’
Has anyone else had the thought that the wave of hackers on the webs is a modern version of the old Anarchists?
>>> (Well, if the spread follows the pattern of 2020, the first places to track are the Hamptons and the Hudson Valley, as those who can leave, leave.)
Why use Covid in 2020? I have seen identical patterns described in all the textbooks and any novel covering an epidemic that I read. Just as diseases tend to get more infectious and lethal if they spread unchecked, which many people should know is also covered in evolutionary biology.
Funny, before the pandemic, I kinda assumed that our betters read books and at least in the CDC were better educated than me. Was that such a stupid assumption?
I remember being warned repeatedly as a kid not to use petroleum distillates in a closed for cleaning or when working on my car while smoking or near an open flame like a pilot light; I always thought “yes, but why would I stupid enough to do so?” Not that l minded being told much as incinerating oneself Would Be A Bad Thing; I always can be stupid at the worst time. Here, we have a society determined to BBQ itself and it’s not a thirteen year old child and there are no older family and friends to stop it.
What on earth makes you think “our society” is not a 13-year-old child?
I know that it is not anymore mature than a 13 year old. A spoiled 13 at that, but that wasn’t always true. That is my point. I have spent the time under Covid disabusing myself of the beliefs that were created from my past memories. After two years, I still wake up, and expect to see what was and not what is.
Our ‘betters’ are just kids playing with matches in a basement flooded with gasoline.
> WebApp somehow uses the command line tool on the backend, hence is GPL’ed, too
Not necessarily. Aside from the Affero variant, the GPLv3 does not treat executable invocation as combination or conveyance, but as mere aggregation, which does not in itself trigger obligations (section 5, “Conveying Modified Source Forms”). I’ve seen plenty of systems do something like this when code needs to be compiled, from online custom firmware generators to professional microcontroller development environments by Microchip and Xilinx.
I believe Lambert was suggesting that if the command line tool were GPL’ed — open-source — then so too might be the WebApp backend which quite probably uses the command line code. That seems a reasonable assumption to me. I rather doubt Lambert were suggesting that the WebApp were open-source as a legal consequence of using GPL’ed command line code — a conclusion you seem to be suggesting.
Please translate your comment into clear human speak.
I check in on this page for New York City, and don’t see that much to be concerned about yet:
https://www1.nyc.gov/site/doh/covid/covid-19-data.page#daily
Interesting that the NYC numbers for 10/22, for example, don’t quite match the NYS reporting for NYC:
https://coronavirus.health.ny.gov/positive-tests-over-time-region-and-county
I’m partial to this NYS data as it has the nice long time series, breaks down by 7day averages and per 100k, and also has variant info and hospitalization time series as well. I noticed the BQ variants in the 10/8/2022 data as their introduction to the series match the slope (roughly) of omicron last winter. I’m eagerly anticipating the bi-weekly update.
https://coronavirus.health.ny.gov/covid-19-variant-data
Being in NYC, I’m well aware of our covid crystal ball status. (When the rest of the country was dismissive about omicron and rapid tests, we were stocking up like squirrels in the first week of Dec 2021, when I already thought we were late too.) I’ve been weary of the fact that hospitalizations haven’t dipped below 820 in NYS since late March 2022, whereas previous waves had much higher peaks in hospitalizations but also much lower valleys.
https://coronavirus.health.ny.gov/daily-hospitalization-summary
Thanks!
Yikes, BQ.1 and BQ.1.1 both more than doubled in 2-3 weeks according to the NYS data summary (not the chart):
https://coronavirus.health.ny.gov/covid-19-variant-data
And we’re off!
“To be fair, the United States population is not the same population it was in 2020”
Also, the “harvesting effect.” Many of the most vulnerable people have already died, and as people become more vulnerable they will die off one by one rather than in a single flood.
True.
One mRNA + One Spike Protein = 1,291 Diseases + Unlimited Ways to Die
https://www.americaoutloud.com/one-mrna-one-spike-protein-1291-diseases-unlimited-ways-to-die/
Dr. Peter McCullough
https://strongandfreecanada.org/truthcast/