By Lambert Strether of Corrente.
The World Health Organization (WHO) has just released a draft version of “Respiratory pathogens: pandemic preparedness guidance” (PDF). Here is the announcement:
🆕 @WHO Respiratory Pathogens Pandemic Preparedness Guidance
Through technical consultations with countries and partners, @WHO has led the development of the draft Respiratory Pathogens: Pandemic Preparedness Guidance👇
Draft for input (deadline 18 Dec)https://t.co/0c7fiotocY pic.twitter.com/wsRWsGerYb
— Maria Van Kerkhove (@mvankerkhove) December 12, 2022
Kerkhove is an infectious disease epidemiologist, and COVID-19 Technical Lead, Emerging Diseases and Zoonoses Lead, WHO Health Emergencies Programme. Of course, if Kerkhove was both a scientist and had the clout, this infamous tweet would no longer be up:
FACT: #COVID19 is NOT airborne.
The #coronavirus is mainly transmitted through droplets generated when an infected person coughs, sneezes or speaks.
To protect yourself:
-keep 1m distance from others
-disinfect surfaces frequently
-wash/rub your 👐
-avoid touching your 👀👃👄 pic.twitter.com/fpkcpHAJx7— World Health Organization (WHO) (@WHO) March 28, 2020
But it is. So that’s where we are with WHO.
That said, WHO exists, has influence, has a $6.72 billion dollar budget, people still listen to them. It even does real work, when it devises nomenclatures — or coordinates the effort to eradicate smallpox. So WHO’s deliverables, like this one, must be examined.
Now, it’s been a long time since I’ve read a do cument by an international standards body seriously. And I’m not familiar enough with WHO institutionally to construct a thorough-going critiique. (I am certain that CDC should be burned to the ground, the rubble plowed under, and the ground salted; but I am not so certain with WHO.) However, this draft is published with a call for comments, so I will do what most commenters do: Begin by scriibbling notes in the margin. There are my comments, based on little more than a cursory reading.
Page 9: Executive Summary
[1] More aspiration. I don’t know how to translate this into WHO-ese, so I”ll just say: The United States under the Biden administration crystallized an approach to pandemics that included (a) Vax-only (with limited treatment options), (b) “Let ‘er rip”, (c) personal risk assessment, and (d) active sabotage of non-pharmaceutical interventions. The lessons learned were: (1) In the United States, government policy can slaughter a million people with no riots, and (2) propaganda really really works. So as for “key lessons of Covied-19”: Isn’t it pretty to think so.
[2] That word “guidance.” It seems not to mean what “guidance” means when there’s a regulatory effort in the United States, where guidance can be either a rule or regulation, or a recommendation. WHO seems not have even the latter power. From Naked Capitalism:
For the moment, the WHO’s legal framework – the so-called International Health Regulations (IHR) – does not grant the organization inspection, policing or enforcement powers against its member States. In other words, it cannot force member States to follow its guidelines. But that could also be about to change. As the Politico article reports, talks are under way to establish a “global pandemic treaty” that will give the WHO more powers to “strengthen pandemic prevention, preparedness and response.”
(The “global pandemic treaty” has not passed, as of this writing. More on WHO’s constitutional and normative powers here.)
Page 7: Glossary
[1] The wording throughout is aspirational, not to say delusional fanciful. “Ensuring,” “providing,” “strengthening,” “proactively building,” ” developing” all describe the world was WHO wishes it to be, not as it is. For example, “Access to countermeasures”: Anybody who’s experienced the American health care system can spot the sleight of hand that converts “access” in the term to “equitable access” in the definition. (Also, who wrote “ensuring synergy”? McKinsey? And what editor let it pass?)
Page 8: Glossary
[1] This thinking about surges is provider-centric. Transmission and infection within a population can surge, but only some fraction of that population will “demand” services. But as we see with Covid, even “mild” cases that do not require increased capacity — at least during the pandemic — may have serious long-term illl effects.
[2] Federalism is, by definition, not collaborative; the United States, China, and Russia, all great powers, have their own versions of federalism. Further, “public service delivery” is often privatized. Finally, NGOs often play signifcant roles. I think what WHO means to say is “whole-of-state-and-civil-society,” but that’s not what they wrote.
Page 25: Essential Workers
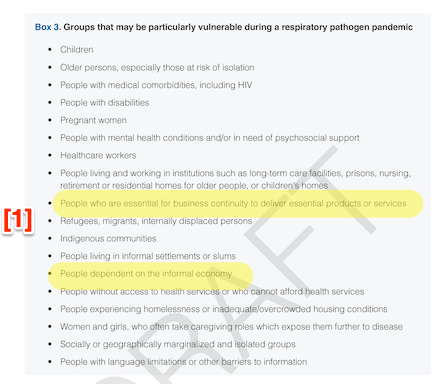
[1] Heaven knows I don’t want anyone to get Covid, certainly not children or elders. But this is a laundry list. I have highlighted the two bullet points for workers (or, as WHO says, “people”). It would have been nice if WHO had mentioned “essential workers” — “people” could be construed to mean the WFH class of emailering laptop types, or even executives, who are essential at least in their own minds — and especially health care workers. According to NBER, “data on 800,000 commercially insured individuals in Philadelphia suggest that during lockdown essential workers were 55 percent more likely than others to get COVID-19.” According to BMJ, “Healthcare workers [are] 7 times as likely to have severe COVID-19 as other workers.” Essential workers, and especially healthcare workers, are, then “particularly vulnerable,” as WHO puts in the headline, and yet WHO gives no guidance that applies specifically to them.
Page 26: Airborne Transmission
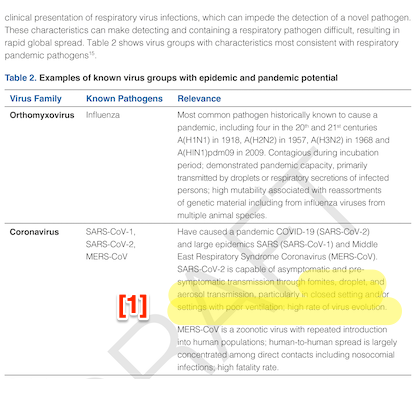
[1] “Transmission through fomites, droplet, and aerosols.” First, since aerosols are Covid’s major mode of transmission, aerosols should be first. Second, since there is only “limited evidence” for transmission via fomites and droplets, they should be placed in a parenthetical and qualified. It looks like the droplet goons still hold sway at WHO, since this wording is all about institutional clout, and not about science at all.
This is as good a time as any to mention that the word “airborne” does not appear in WHO’s so-called guidance at all:
Not does the word “mask,” certainly an odd omission for a document with the word “respiratory” in its title. Does WHO believe that virions are carried to the nose and lungs by tiny Maxwell’s Demons? As opposed to being breathed in with the air?
Page 29: Pandemic Story Arc
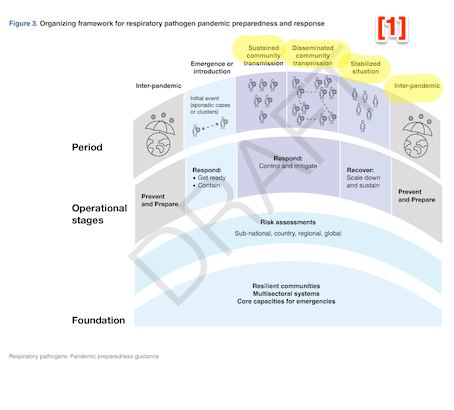
[1] The visual presentation — an arc from low, to high, and back to low, — suggests that a pandemic goes through a linear progression, beginning at “inter-pandemic” and ending at “interpandemic.” Covid does not seem to behave in that way. Due to (IMNSHO) immune dysregulation from Covid infection, we are now experiencing a “Tripledemic” of RSV, flu, and Covid, such that providers are at pandemic levels of stress. The model implicit in the graphic cannot give an account of this phenomenon.
Page 43: Infection Control
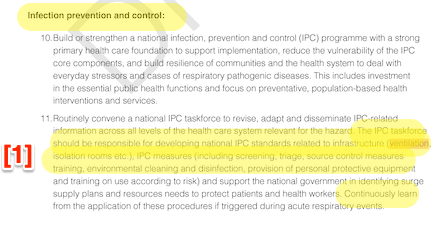
[1] The Hospital Infection Control community fought both airborne transmission and masking tooth and nail, within their own institutions, when advising governments, and in standards bodies, and is still doing so (see the bogus study from Loeb, et al.). They shouldn’t be in charge of a lemonade stand, let alone developing national IPC standards. Of course, TINA, but can we at least acknowledge their role? However obliquely? (See, e.g., Canada’s Dr. John Conley.)
Page 60: Case Studies
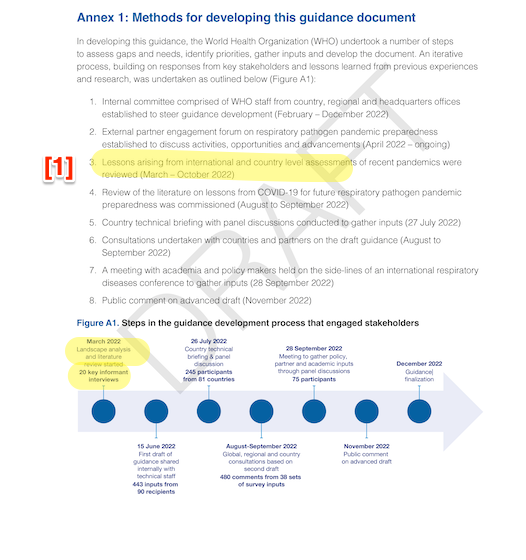
[1] The “landscape analysis and literature review” seems to consist mostly of experts talking to themselves. WHO mentions case studies. The case studies examined for this guidance took place in Germany, Iran, Nigeria, Pakistan, Puerto Rico, Somalia, Vietnam, Uzbekistan, two NGOs (C-TAP and the Pan American Health Organization) and the Caribbean. Where, for good or ill, are China and the United States? Where, if you don’t want to examine Anglosphere debacles, are Japan, South Korea, Taiwan, or Thailand? If the case studies are inadequate, as they are, then the methods for developing the guidance are inadequate, and the guidance is inadequate, being based on the experts WHO is talking to, as opposed to experience on the ground.
Page 65: Ventilation
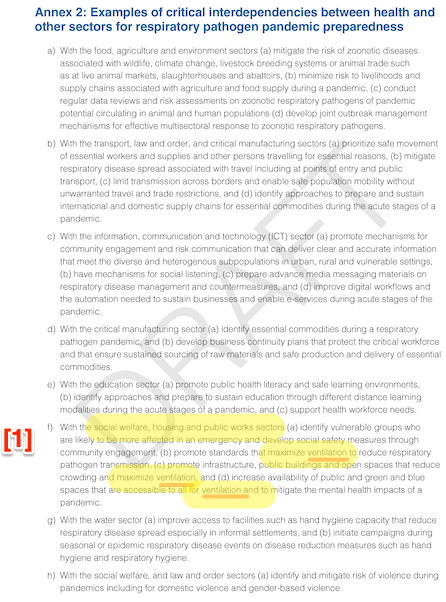
[1] The only other place where the word “ventilation” appears is in Infection Control (p 43). This guidance is even more absurd, because it pertains only to “social welfare, housing, and public works sections. WHO doesn’t even mention ventilation in the workdplace! Looking at page 25, we’ve already seen how WHO gave short shrift to workers, but this really takes the biscuit.
Page 69: Panic
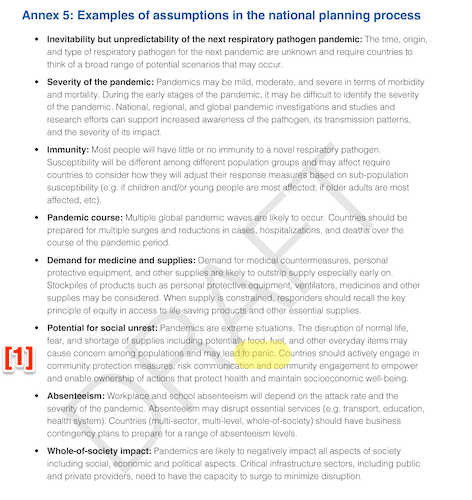
[1] Rebecca Solnit, before she became “Rebecca Solnit,” wrote a wonderful book titled A Paradise Built in Hell: The Extraordinary Communities That Arise in Disaster: “Panic is rare, looting is essentially insignificant, people are not terrified and trampling each other to flee from a disaster scene, but in fact are trying to manage a situation. We may in fact revert to some sort of primordial civility.” Dull normals don’t panic. Elites panic; Solnit shows that the looting and fires after the San Francisco earthquake only happened after the troops arrived.
Page 70: Triggers
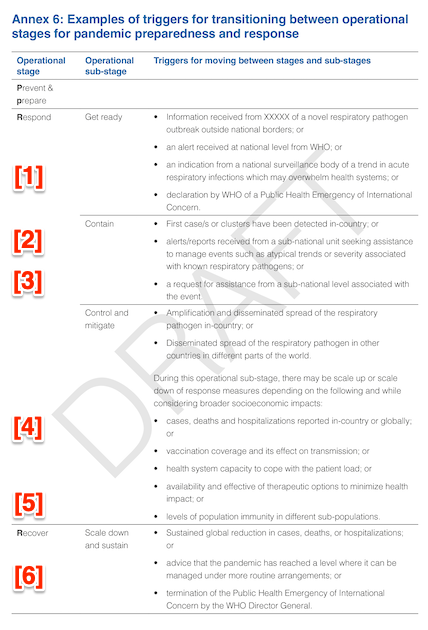
Once again, WHO is being delusional aspirational. I know this is “guidance,” but guidance needs to take some account of the operational capabiity of those guided. In the United States, for example:
[1] in my recollection, alerts came from scientists and news reports (the “XXXXX”?) not WHO or standards bodies;
[2] first cases were in the United States weeks before we detected them;
[3] little assistance was given by CDC to the states, especially since CDC butchered testing;
[4] all reporting was spotty, cases being especially bad because no contact tracing was done;
[5] levels of immunity in different populations were not tracked;
[6] if our current arrangements are “routine,” we might as well just throw in the towel.
Conclusion
I would send this back for a complete rewrite. At a minimum, there should be a science-based theory of transmission for Covid. The selection of case studies should also be adequate. Somehow, I don’t think that will happen, but a blogger can dream.


Thanks for this. This document is in keeping with what hasn’t worked out so well, so we can look forward to moar of the same, I expect. Comments likely to be ignored, as it’s all theatre. Is my cynicism showing?
“No one is safe until everyone is safe” as an axiom defies any logic. I’m left with:
What does “safe” mean? I notice it is not in the glossary.
What if the cost of “safety” is reduced “safety”?
Do both instances of “safe” have the same meaning?
What sort of terrible acts have been committed throughout history in the name of “saving” people?
“Whole of society” pandemic impact should be as focused on “solution” of the guidance. Is it not clear now that much of what was done may have had a worse impact than doing nothing?
I also appreciate the wording of “active sabotage of…” which was so abundantly clear – and would include natural immunity and cocktails of (existing) multi-pronged antiretroviral drugs.
Could say so much more but frankly I’m disgusted.
The WHO gets a lot of funding from the Bill and Melinda Gates Foundation (who is invested in Big Pharma and CocaCola, among other things) so you can expect the WHO to concentrate on things that make money for BPharma, and not have any particular interest in say, making safe workplaces, or even eating a healthy diet. No money in that….
I’d say the WHO needs to be burnt and salted as well. Remember they dragged their feet for calling a pandemic, and argued against travel restrictions. We are better off without them.
Yeah, it’s always a case of follow the money. The WHO could have given scientific recommendations but their donersdid not want to be on the hook for actually implementing any of it and thought that having people just pretend it was gone would be cheaper in the long run.
Note to Lambert: The very last bit of this post seems to have been chopped off when it says-
‘UPDATE I tried to do WHO’s survey on the guidance, but it’s broken; it’s chastising me for failing to provide my institu’
> The very last bit of this post
Removed. Danged autosave. The survey is unbelievably clunky and not meant for the general public.
> I’d say the WHO needs to be burnt and salted as well.
That’s certainly my impulse, but I don’t know enough about their internal workings to say. Institutionally, they are in an impossible position, with a mandate for healthcare as a right, globally, and the constitutional right to make treaties but dependent on state (and, worse, private) funding, and having no ability to inspect or enforce.
And you have to give WHO points on smallpox. So I am not sure they are irredeemable.
1. Covid is not Aotborne:
2. Covid is transmitted when people exhale.
Isn’t that a contradiction?
> Isn’t that a contradiction?
It is, one that CDC has not resolved either, I assume due to both factional/paradigmatic conflict in the institution itself, and direction from the Biden Administration.
“Not Airborne” ranks with the best examples of instruction sheets naively translated from other languages. The favorite example in our home was an ad by vendors of a high friction surface material.
It has a photo of a desktop phone, and the proud statement, “ Your sliding phones are gone forever!”
Who knew the HVAC industry was so powerful?
Pun intended.
Thanks as always. It’s disheartening and vexing in equal measures. There is no intention whatsoever to actually deal with the spread of the disease. Instead the same obfuscating language – purposeful sins of omission.
I wonder what they’re gonna do if MERS gets spread from Qatar?
Via The Lancet:
“The Qatar FIFA World Cup 2022 and camel pageant championships increase risk of MERS-CoV transmission and global spread”
Excerpt:
“MERS-CoV was first reported as a new human pathogen from Saudi Arabia in 2012.6 MERS-COV is the most lethal of the three zoonotic coronaviruses (ie, MERS-CoV, SARS-CoV, and SARS-CoV-2) that have caused human outbreaks.7 As of Nov 1, 2022, 2600 people have been reported to have laboratory-confirmed Middle East respiratory syndrome (MERS), including 894 deaths (ie, a 34% case fatality rate), globally from 27 countries.8 Although the majority of infections have occurred in the Middle East, eight countries in Europe have also reported confirmed infections, all with travel links to the Arabian Peninsula. In May 2022, Qatar authorities reported to WHO two individuals with MERS, of whom one died.9 Both had primary MERS-CoV infections, contact with camels, and had consumed raw camel milk. With MERS-CoV being endemic in camels in Qatar, the simultaneous hosting of the FIFA World Cup 2022, and the camel beauty pageant, poses an enhanced risk of transmission and globalisation of MERS-CoV.”
We’re family-blogged if this gets out …
A quademic? Interesting in a horrible way. Anyone betting on quindemic? It looks like each epidemic gives another disease a chance to become an epidemic by overloading our already collapsing medical system or am I wrong?
Assuming that Western civilization will still be a going concern fifty years from now with my family’s lifespans, I could possibly still be alive to read the history of today’s planetary clusterfluck; I do wonder what it will say.
I just got to say that seeing all the bad reasoning, panicked and/or corrupt opportunistic decision making, stupidity, fear, greed, paranoia, and ineptitude that I have read about for years in history more believable seeing it as it happens now. Another March of Folly in real time!
> . . . if this gets out . . .
Still Flying = Total Fail
> Page 65: Ventilation
I should have added that WHO seems to think that bringing in outside air is enough. “Ventilation” also comprises HEPA filters, CO2 monitoring, and (possibly) up-and-coming UV technology.
It’s as if somebody said “We’ve got to get the word ventilation in there!” and so they did, but never did any actual research. (This may also be due to the undue influence of Hospital Infection Control, who have a whole paradigm for ventilation, and assume it’s a solved problem (and no need to spend more money on solved problems). So, and as usual, they apply the paradigm for their own institutional setting to the world as a whole, and it just doesn’t work.
Apparently a work produced by a committee is only as intelligent as the committee’s stupidest member. If produced by multiple committees, the stupid is multiplicative ……
My question is – Have all the institutions of the west been corrupted? Has the corruption proceeded through the ether and infected everyone within ?
Thanks, Lambert, for wading through this disheartening task.
It shows how these high institutions are influenced by important players. If they stick with the droplet theory is because it fits the interests of HC providers not wanting to do the necessary investments to prevent airborne transmission. Easier and cheaper just cleaning surfaces.
KNOCK! KNOCK! KNOCK!
The sound of another head banging on a desk.