Yves here. This is an important post, since it documents yet another way that the foundations of supposedly civilized life are eroding in America, here access to hospitals because money. And the headline is too charitable as to why this is happening now. It’s not because rural hospitals are suddenly seeing decay in their economics. It’s because bigger hospitals are buying them and shuttering them, presumably because they believe they can force folks in these low-population areas to travel to see specialists and get surgeries. But what about emergencies? And what about those who are in hourly jobs and simply can’t take a half day or day off just to see a specialist, let alone to get testing and care.
This article does not incorporate the idea of private equity squeezing patients by buying up speciality practice like ER doctors and hospitalists, but I have to believe that plays a role.
Note in particular the map of states with a lot of rural hospitals at “immediate risk” of closing. Ugly.
By run 75411. Originally published at Angry Bear
This is an interesting take on small hospitals and also covering smaller hospitals in small towns or rural areas. It is an issue as the larger hospitals buy them up. Rather than invest in them, they close them down. One reveal is those hospitals closings coming as a result of what private insurance pays for patient care.
This is an issue which both state and federal governments. should be addressing.
Why are 600+ rural hospitals at risk of closing? advisory.com. Commentary taken from:
“Rural Hospitals at Risk of Closing,” chqpr.org. Center for Healthcare Quality and Payment Reform.
Things are changing more rapidly. Smaller hospitals are under an attack of high costs and less revenue. As a result, many are closing leaving the small town and rural residents without medical care or having to drive long distances in emergencies. As reported by Healthcare Quality and Payment Reform:
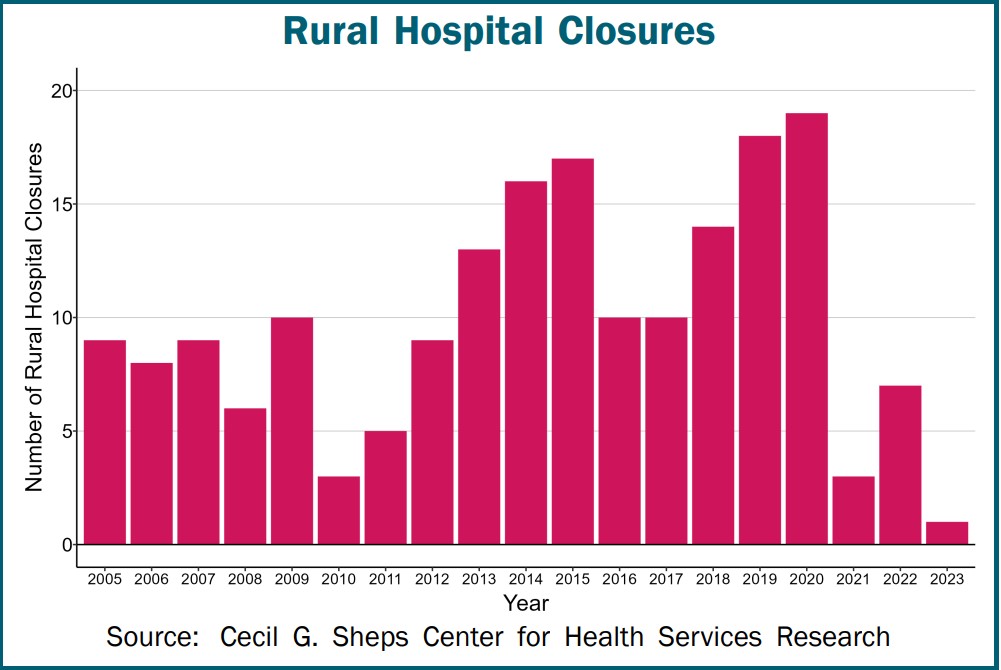
Many people across the country could not receive hospital care in their community when the pandemic began. Over 150 rural hospitals closed between 2005 and 2019. An additional 19 rural hospitals closed in 2020, more than any year in the previous decade. The closures are not resulting from the pandemic, but by financial losses in previous years. Ten more rural hospitals closed in 2021 and 2022. The closures decreased in 2019 due to the special financial assistance hospitals received during the pandemic. The pandemic aid has ended and closures are likely to increase.
Hundreds of Hospitals are at Risk of Closing
Six hundred rural hospitals or ~ 30% of all rural hospitals in the country are at risk of closing. At risk because of the serious financial problems, they are experiencing:
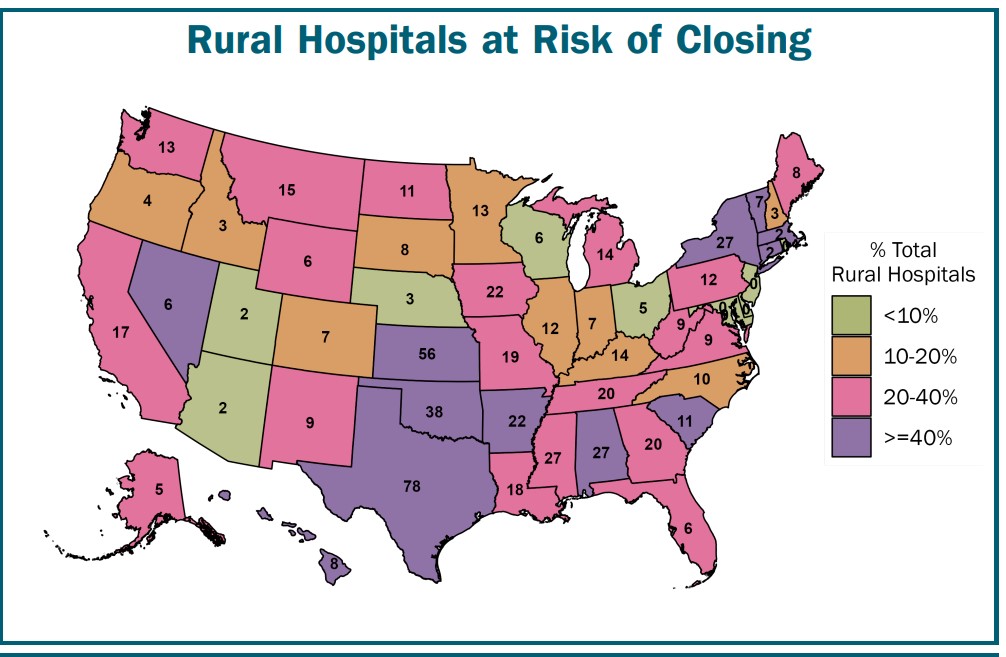
Losses on Patient Services: Health insurance plans are not paying these hospitals enough to cover the cost of delivering services to patients. The losses will likely be greater in the future due to the higher costs. All hospitals and particularly small rural hospitals are experiencing such because of inflation and workforce shortages. Many of these hospitals have received grants, local tax revenues, or profits from other activities offsetting losses on patient services in the past. However, there is usually no guarantee these funds will continue to be available in the future or whether they will be sufficient to cover costs.
Low Financial Reserves: If the hospitals do not receive grants or other funds to cover losses on services, the hospitals would not have sufficient net assets (including pandemic-related funding, but excluding buildings & equipment) to offset their losses for more than 6-7 years.
Many Rural Hospitals Are at Immediate Risk of Closing
Over 200 of rural hospitals are at immediate risk of closure. This due to the severity of their financial problems:
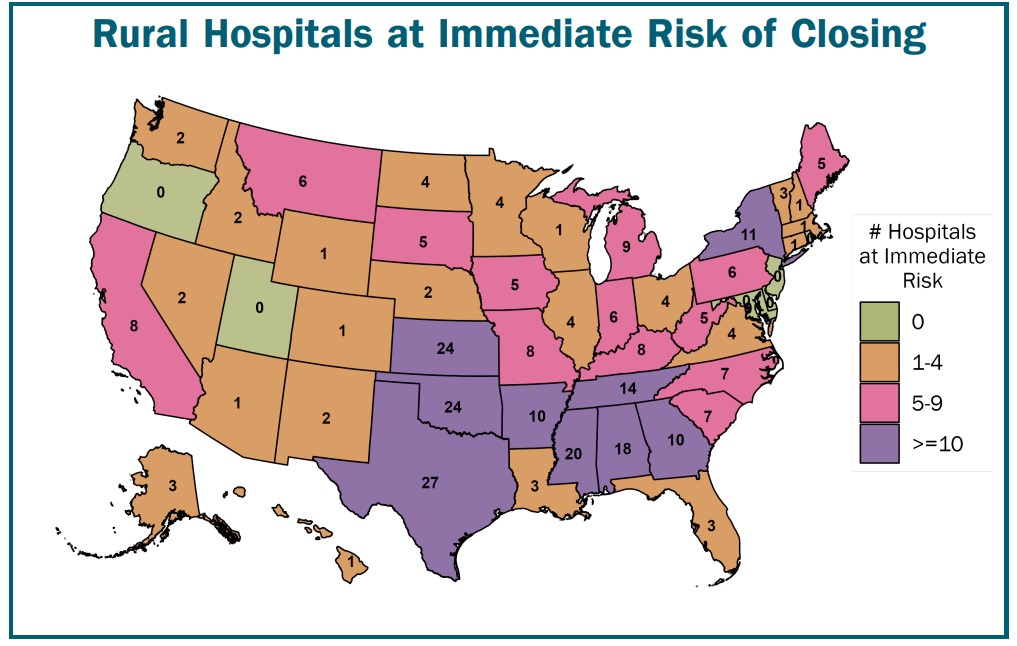
Inadequate Revenues to Cover Expenses: These hospitals lost money delivering patient services over a multi-year period (excluding the first year of the pandemic). They are unlikely to receive sufficient funds from other sources to cover those losses after federal pandemic assistance ends.
Very Low Financial Reserves: The hospitals have more debts than assets, or the hospitals’ net assets (including pandemic-related funding and excluding buildings & equipment) could offset their losses for at an ~ 2-3 years. (Fewer rural hospitals are at immediate risk than prior to the pandemic because of the federal pandemic aid they received).
Access Reduction and increasing Disparities for Rural
Most of the at-risk hospitals are located in isolated rural communities. Closure of the hospital would mean residents of the community would ravel a long distance for emergency or inpatient care. Also in many small rural communities, the hospital is the only place where residents can get laboratory tests or imaging studies. It may be the only or principal source of primary care in the community. A closure of the hospital would cause a loss of access to many essential healthcare services.
What I like about this article is it adding a different viewpoint of why small hospitals are in financial trouble is the next portion of the article. The next two topics come as a shocker.
Closures Are Caused by Inadequate Payments from Private Payers
The primary reason hundreds of rural hospitals at risk of closing is private insurance plans are paying them less than what it costs to deliver services to patients. As shown, although the at-risk hospitals are losing money on uninsured patients and Medicaid patients . . . losses on private insurance patients are the biggest cause of their overall losses.
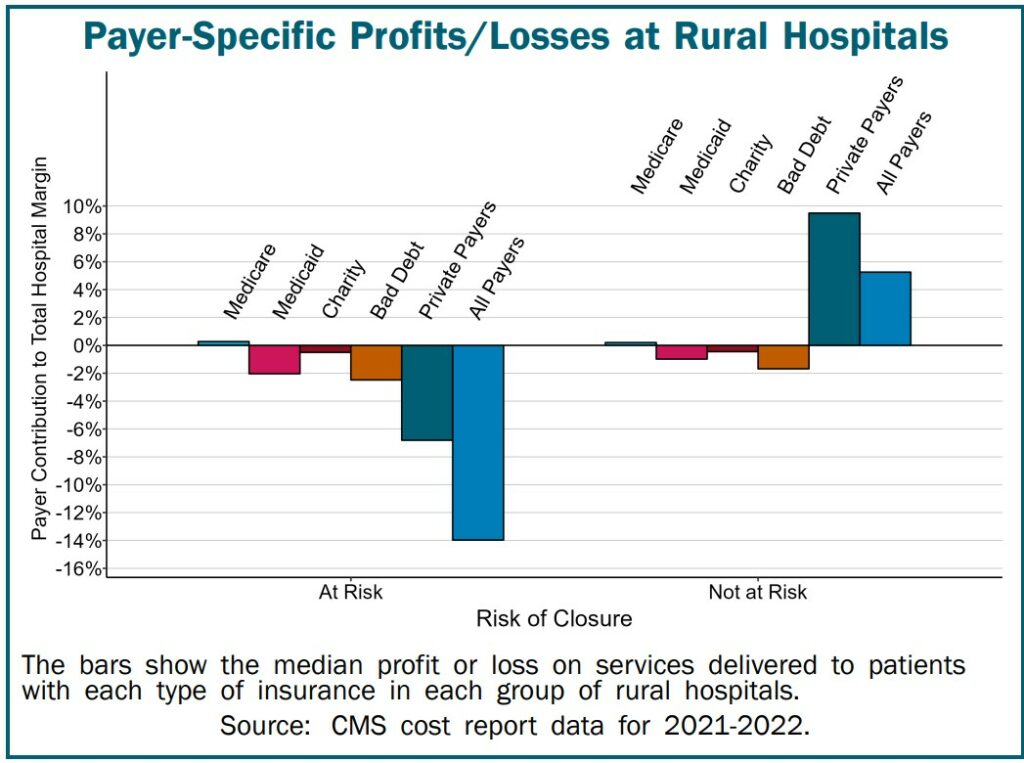
Conversely, many rural hospitals not at risk of closing because they make profits on patient services. They receive payments from private health plans covering the costs of delivering services to the patients with private insurance. Those payments also offset the hospitals’ losses on services delivered to uninsured and Medicaid patients.
Note: Medicare is not one of the causes putting rural or small hospitals at risk.
Preventing Rural Hospital Closures
Changes are being called for in both the amounts and method of payment for rural hospital services in order to prevent more rural hospitals from closing in the future. Rural hospital closures threaten the nation’s food supply and energy production. The reasoning are the locating of Farms, ranches, mines, drilling sites, wind farms, and solar energy facilities are located primarily in rural areas. They will not be able to attract and retain workers if the workers cannot get adequate healthcare services.
Requiring Healthcare Services to Cover the Cost of Services in Rural Communities
Payments that are sufficient to cover the cost of services at large hospitals will not be adequate at small rural hospitals because it costs more to deliver healthcare services in rural communities. This is not because rural hospitals are inefficient, but because of the smaller number of patients served relative to the fixed costs of the services. For example, a small rural community will have fewer Emergency Department (ED) visits than a larger community simply because there are fewer residents, but the minimum cost of staffing the ED on a 24/7 basis will be the same, so the average cost per visit will be higher.
The biggest problem facing small rural hospitals is inadequate payments from private health plans. Most “solutions” for rural hospitals have focused on increasing Medicare or Medicaid payments or expanding Medicaid eligibility due to a mistaken belief most rural patients are insured by Medicare and Medicaid or are uninsured.
In reality, about half of the services at the average rural hospital are delivered to patients with private insurance (employer-sponsored insurance and Medicare Advantage plans). In most cases, the amounts these private plans pay, not Medicare or Medicaid payments, determine whether a rural hospital will have to close.
Rural hospitals should not be forced to eliminate inpatient care in order to receive higher payments for other services, as is required under the federal “Rural Emergency Hospital” program. This would make it harder for rural residents, particularly the elderly, to receive prompt, high-quality care when they are ill.
Increasing payments to levels sufficient to prevent closures of the at-risk hospitals would cost about $4 billion per year. This would represent an increase of only 1/10 of 1% in total national healthcare spending. Most of the higher spending would support primary care and emergency care, since the biggest causes of losses at most small rural hospitals are underpayments for primary care and emergency services. Spending would likely increase as much or more than this if hospitals close, because reduced access to preventive care and failure to receive prompt treatment will cause residents of the communities to be sicker and need more service in the future.
Create Standby Capacity Payments to Support the Fixed Costs of Essential Rural Services
The financial problems at small rural hospitals are caused not only by the inadequate amounts paid by private health insurance and Medicaid plans, but by the problematic method all payers use to pay for services. Small rural hospitals are not paid at all for what residents of a rural community would likely view as one of the most important services of all – the availability of physicians, nurses, and other staff to treat an injury or serious health problem quickly if the resident experiences an injury or problem. Having health insurance that pays fees for ED visits, laboratory tests, or treatments is of little value if there is no Emergency Department, laboratory, or treatment capability available in the community for the resident to use.
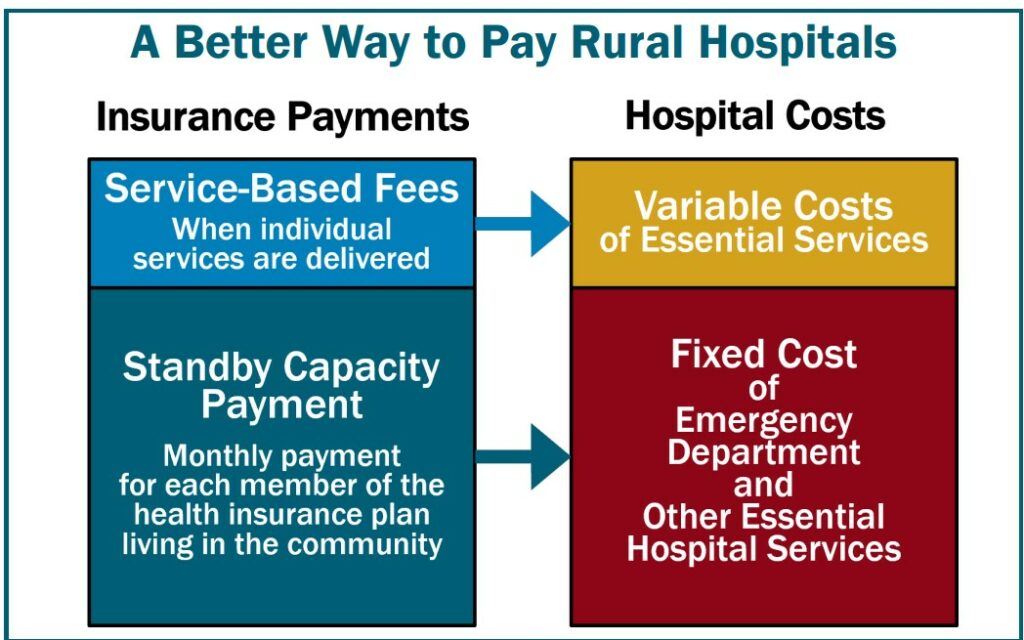
In order to preserve and strengthen essential hospital services in rural communities, small rural hospitals need to receive Standby Capacity Payments from both private and public payers in addition to being paid Service-Based Fees when individual services are delivered. The Standby Capacity Payment would support the fixed costs of essential services at the hospital, and the Service-Based Fees would cover the variable costs of those services.
More details on this approach are available in A Better Way to Fund Rural Hospitals.


Once Bill Gates gets his Frankenplants, self-driving tractors and robot bees in place, humans will have to leave farm country. It will be so toxic, it will be dangerous to remain there. See? Problem solved.
Thank you for posting this. My wife works at a local rural hospital on the north coast of CA. Because the hospital needs earthquake retrofitting that is costly, rumors are that the hospital will simply be closed instead. I certainly hope that does not happen, the local community will be devastated and many people will be out of a job.
The hospital is the largest employer in this town of roughly 7,200, and also serves the surrounding rural coastal communities. The next nearest hospital is 1.5 hours away.
I forwarded this article to my wife, who is at work right now. I asked her to forward it to the director of the hospital as well.
This article juxtaposed with that bit of information about the 99% chance of developing Long COVID paints a dark, dark picture ahead…
Thanks for this post.
This erosion of rural hospitals has been going on for 20+ years. There are many reasons. No one at the top govt levels seems the least concerned about this devastation. I think of it as the slow de-contenting of America.
I like “derezzing”.
Derezz definition: (science fiction, of an image) To disappear, or dissolve into pixels..
Could this have anything to do with closures?
“Gov. Gavin Newsom announced a budget deal Sunday that includes funding to expand Medi-Cal – California’s state-subsidized health insurance – for low-income, undocumented residents ages 26 to 49. It is expected to impact roughly 700,000 people across the state. The program is expected to start by Jan. 1, 2024.
That means once this latest expansion starts, California will become the first state in the country to remove immigration status as a barrier to health care.”
https://www.kcra.com/article/california-budget-expanding-medi-cal-undocumented-residents/40439713
Not at all, as was pointed out, this is a long-term process nationwide.
But the Gaviner and his wealthy cronies need to have the taxpayer pay for their slave labor on their vineyards, farms etc. Public subsidies are for the rich, taxes and prison are for the “little people”.
Besides, having slaves die young from a simple preventable health issues is not good for PR or good for business – who else is going to pick grapes for slave-wages in the 100-plus degree weather?. So Gaviner can feel good about himself, what a nice guy eh
I live in an upstate NY county of around 100,000. We used to have two separate operating hospitals.One of the hospitals bought the other one. Shortly after they closed it and turned it into a huge nursing home. Locally we no have no choice. The nearest other hospital is almost an hours drive away.It was NYS that forced this to happen.
Left out of the discussion is another significant cause, perhaps the significant root cause,…..the tort system. Because these hospitals are rural they have low volume. So consider, for example, a child’s wrist fracture, which is a common occurrence. Years ago when the rural hospitals were dominant a local GP or ER doc would reduce the fracture and put it in a spliint without fear and with backing of their malpractice carrier. Now if an orthopedic surgeon is not available, and this is common because there is low volume, the child is referred out of the ER to the medical center perhaps an hour or two away. The reason is litigation. If the parents are not satisfied about some aspect of it like a minor residual deformity, or occasionally worse, they almost always sue. And the settlement amounts are not trivial. For a child 250 to 500K for a mild residual deformity would be in the ball park. For an adult with a 30 percent reduction in forearm rotation an easy 200K. Throw in defense and plaintiff fees and you are looking at 7 figures. And this extends to other specialties like cardiology with angina (chest pain), now stroke which requires immediate intervention and childbirth. And for some years the US government has had a national data bank on malpractice cases open to all hospitals and physician employers. Even if there is a minimal settlement it goes into the data bank and the doctor’s permanent record which is the kiss of death for a practitioner if they ever need to get another job. So they refuse to settle which generates tons of litigation with helps the legal profession from another angle. So what happens is the ER becomes a defacto peripheral office of the medical center an hour or two away. Because at trial if the medical center expert says that the result is the best that could be achieved that is going to trump the statement of an expert that the local doc at the local rural hospital achieved the best possible outcome given the circumstances. And the bottom line from the plaintiff attorney is always that the local doctor had the option to refer the patient and chose to treat it less than optimally. Less than optimal care at Massachusetts General or Johns Hopkins or UC Davis or Stanford is not viewed by juries as less than optimal as often as perhaps at a local rural hosptial on the California coast with an ER doc and family practitioner as the treaters. And this referral of all complex cases out to the medical centers starves the local hospitals of the high dollar revenue cases like joint replacement (now done for hip fractures often), spine surgery (mostly useless but high revenue), cardiac surgery, oncology, significant trauma. And so the patients must endure long drives to the big centers, or helicopter fllights they are billed for in cases of stroke or angina, or polytrauma etc., to enjoy the potential benefits of litigation. The only solution would be massive tort reform……like perhaps no fault malpractice insurance…..and some sort of modification of the data bank. But then local doctors would take on cases occasionally that would beyond their skill set and then there would be occasional worse outcomes. And at an individual level Americans want the right to sue, without paying for it, if an outcome is not ideal. No other country has such a legal system. So it boils down to the fact that rural small hospitals are basically nursing homes, at best, that have to have a baseline of expensive equipment which costs a ton of money and is underutilized so they are not economic. And I have worked in both the medical centers and the small rural hospitals.