Yves here. Even though experts voice doubts about whether COVID-19 is as well contained as their data suggests, it is still true the the R0, or the basic reproduction rate rate, of an infectious disease is not etched in stone and is estimated by modeling. From a 2019 paper posted at the CDC:
The basic reproduction number (R0), also called the basic reproduction ratio or rate or the basic reproductive rate, is an epidemiologic metric used to describe the contagiousness or transmissibility of infectious agents. R0 is affected by numerous biological, sociobehavioral, and environmental factors that govern pathogen transmission and, therefore, is usually estimated with various types of complex mathematical models, which make R0 easily misrepresented, misinterpreted, and misapplied. R0 is not a biological constant for a pathogen, a rate over time, or a measure of disease severity, and R0 cannot be modified through vaccination campaigns. R0 is rarely measured directly, and modeled R0 values are dependent on model structures and assumptions. Some R0 values reported in the scientific literature are likely obsolete. R0 must be estimated, reported, and applied with great caution because this basic metric is far from simple….
For any given infectious agent, the scientific literature might present numerous different R0 values. Estimations of the R0 value are often calculated as a function of 3 primary parameters—the duration of contagiousness after a person becomes infected, the likelihood of infection per contact between a susceptible person and an infectious person or vector, and the contact rate—along with additional parameters that can be added to describe more complex cycles of transmission (19). Further, the epidemiologic triad (agent, host, and environmental factors) sometimes provides inspiration for adding parameters related to the availability of public health resources, the policy environment, various aspects of the built environment, and other factors that influence transmission dynamics and, thus, are relevant for the estimation of R0 values (21). Yet, even if the infectiousness of a pathogen (that is, the likelihood of infection occurring after an effective contact event has occurred) and the duration of contagiousness are biological constants, R0 will fluctuate if the rate of human–human or human–vector interactions varies over time or space. Limited evidence supports the applicability of R0 outside the region where the value was calculated (20). Any factor having the potential to influence the contact rate, including population density (e.g., rural vs. urban), social organization (e.g., integrated vs. segregated), and seasonality (e.g., wet vs. rainy season for vectorborne infections), will ultimately affect R0. Because R0 is a function of the effective contact rate, the value of R0 is a function of human social behavior and organization, as well as the innate biological characteristics of particular pathogens. More than 20 different R0 values (range 5.4–18) were reported for measles in a variety of study areas and periods (22), and a review in 2017 identified feasible measles R0 values of 3.7–203.3 (23). This wide range highlights the potential variability in the value of R0 for an infectious disease event on the basis of local sociobehavioral and environmental circumstances.
By Bob G
China was clearly in a lot of trouble with Covid-19, but had the contagion contained by February 19th, at least according to their data. They did this by locking down the country and shrinking their economy in the process. This is clearly a strength of a totalitarian regime.
But China also clearly showed the rest of the world how to limit a viral outbreak, and the rest of the world is slowly and reluctantly following the same playbook, to the extent that they are able.
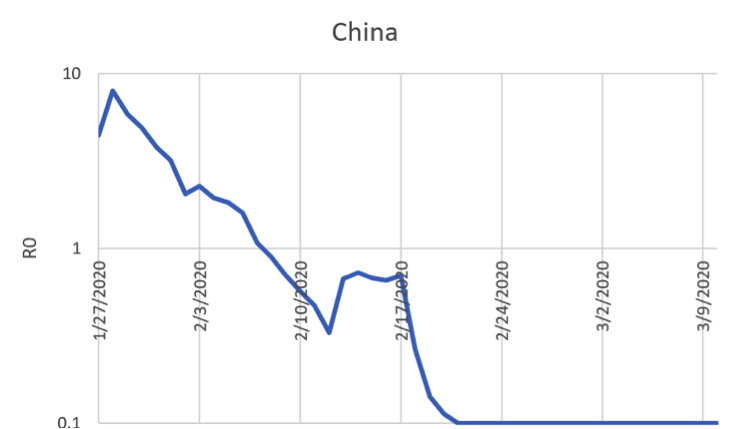
The above graph shows the transmissibility (R0) of Covid-19 in China. When R0 crossed below 1, the number of new infections was declining day-by day. The number of active cases took a number of weeks to work through the system, but they were out of trouble by February 17.
Even though China’s Covid-19 hospitals are mostly emptied out, they are still on lockdown. China still has new cases arising. What is alarming is that many of the newest cases are being imported from Iran. Even in China, only a small percentage of the population has been infected, so few are immune as the virus continues to spread around the world.
We want to know if the pandemic can be controlled. It probably can, at least in countries that are willing to shut down for weeks or months. We want to know if the pandemic can be stopped across the world. That is increasingly unlikely. And we want to know how long we will need to be locked down.
The answers to these questions come down to understanding the transmissibility of the disease. Normally health care experts use R0 (pronounced R naught) to measure the transmissibility of a disease. It tries to measure how many people will be infected by each new infection of a disease. This is a wonderful metric in theory, but a terrible metric in practice. It is almost impossible to accurately measure and is debated for decades. I wanted to find a practical alternative to R0 that can be calculated from publicly available data that would tell us what we really need to know.
I was able to calculate a version of R0 that shows when the disease was spreading uncontrollably in different regions, and the progress the country made to slow this. I simply measured the number of new cases in a region relative to the number of active cases 5 days previously. This is still imperfect in that in early days many cases went undetected so R0 is overstated. It is also not at all clear if 5 days is the average incubation period. Regardless of how one calculates R0, what matters is that when R0 is above 1.0, the disease is spreading, and when it is below 1.0, the disease is contracting. My simplified R0 calculations show the trends by region. The data was downloaded from the Johns Hopkins data sets that they use for their daily reporting.
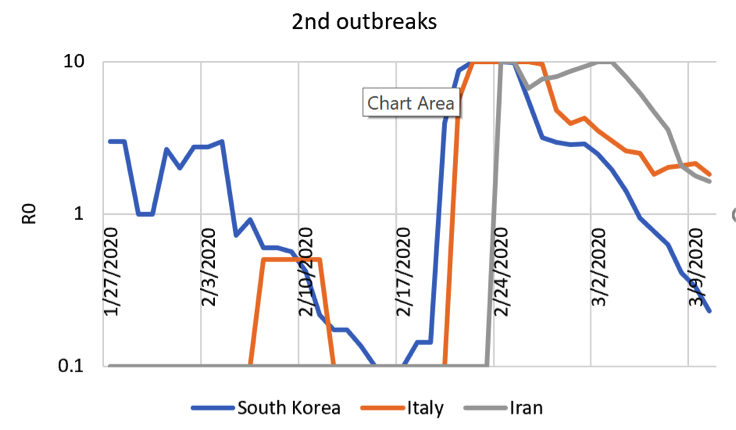
After China had contained the outbreak, it still had time to hop to other countries. South Koreas has already stopped the spread within their country. Italy and Iran have been slower. Italy has a complete shutdown. Iran released its prisoners. Their R0 is around two now, but falling quickly.
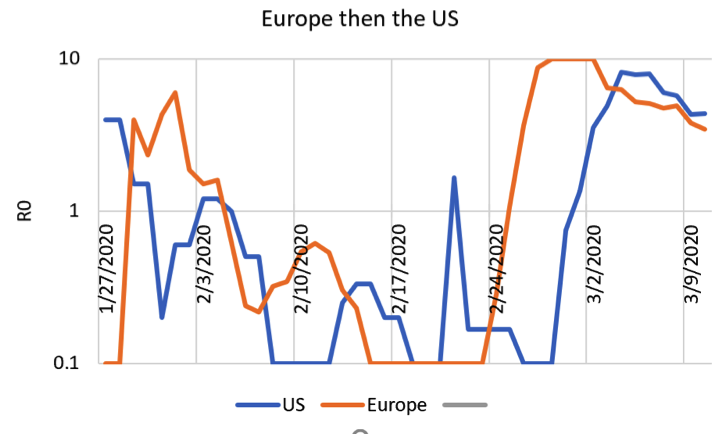
(non-Italy) Europe and the US were hit later, be neither is yet effective. R0 is five, reflective of the fact that the virus has spread everywhere, but the lockdowns have not yet started. I live in Seattle, which has had virtually all the deaths in the US. And out region is already locked down. I am stuck in my home, my children’s’ schools have been closed and my wife spent two days trying to find toilet paper. But all of the Seattle deaths reflected people who were already sick far before R0 in the US started rising again 2 weeks ago.
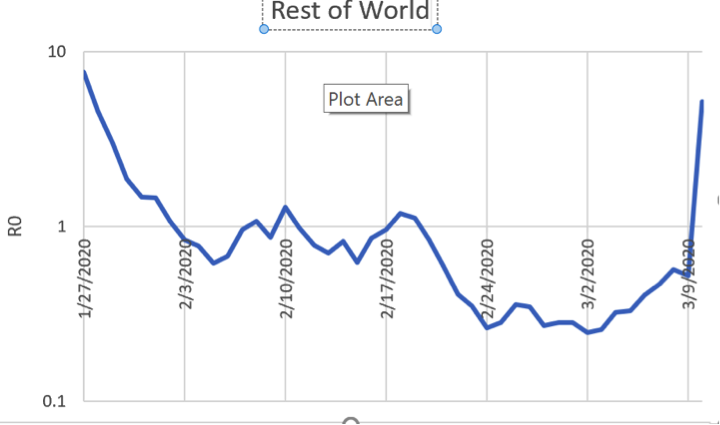
But what is scary is that the rest of the world is just getting hit right now. We do not know if Nigeria or Venezuela or Indonesia will be able to put in social distancing controls on the entire population. I am inconvenienced by being unable to leave my house. Many in America will temporarily lose employment. In the third world people may starve if they cannot work.


Not having read this yet, forgive me If I say some things I have learned these days when in Madrid we suddenly realise that the epidemics is in full swing. Some friends of mine in between 40-50 years old are now feeling the nasty symptoms of what would be called a mild disease (no hospitalization necessary). These symptoms start with what seems a normal caugh that rapidly turns into something nasty with head- aches, some other pains (articulatory for instance, in some cases breast oppresion, fever (37,5-38,5ºC) and a few of them have already been about 6 days with these symptoms. None of them are being tested and for good reason: hospitals are saturated and are risky places. Only if deep fatigue and respiratory problems are felt one has to go to ER. According to a german study that covered mostly mild cases, the immune response starts at about 6-12 days after symptom onset and then improvement starts and virus loads fall sharply.
Please, read this: start NOW cutting sharply social life. If someone feels bad isolate yourself (and your family), keep calm and do not go to a hospital unless you are belong to a risk group or you are feeling severe respiratory symptoms. If you need to go to the supermarket: precautions, masks to be used only inside an discard properly outside (carry a plastic bag with you). Masks if you feel bad to protect your family. If you are okay and weather is fine go outside and have walks, bike rides avoiding gatherings.
For some stupid reason people are hoarding toilet rolls at home. It is said that such attitude gives you a sense of control when you have fear.
To all of you, take care, be helpful, do not panic and react positively.
Thank you for your calm well thought out advice, Ignacio, and very best wishes for all. Always look forward to your comments.
Same here. Keep us posted, and good luck.
I think probably the worst thing about this crisis is the lack of consistent and accurate information, causing people to panic. The Arstechnica backgrounder that Lambert linked yesterday seemed to contradict some other reports. It said the course of the virus is almost always less than two weeks, that you get it by being coughed or sneezed on or from touching virus laden surfaces, that it doesn’t just float around in the free air. It suggested that the disease could be less infectious than many have claimed and that in China most people got it from family members. It does seem that if the disease was already rampant in the US that we would have a lot more sick people in hospitals given the elsewhere claimed fifteen percent hospitalization rate. But as stated in the above report, the R0 could be much less than people think.
So the real crisis is that all of this is just happening too fast and more needs to be known. These drastic measures to buy time seem justified.
In everything I have read, including the many links here, it has always been stated that this virus is primarily communicated through droplets directly inhaled from an infected person. It has never been described as airborne, in the sense that it could be circulated throughout a closed-air system. Hence the efficacy of social distancing.
There was some early speculation here a couple of weeks ago that some individuals could be silently shedding the virus for as long as 28 days–that there could be symptomless disease spreaders. Yesterday’s article seemed to say that transmission was closer to that of ordinary flu and that it might even be less contagious than ordinary flu.
Obviously I’m no expert–just trying to glean info from what’s out there.
Disclaimer: I’m not any kind of expert on any science or medicine, so what I’m writing below is purely derived from information I’ve read from reliable sources and making some educated inferences.
The WHO FAQ says “most estimates” say incubation period (time between infection and feeling first symptoms) is between 1 and 14 days. https://www.who.int/news-room/q-a-detail/q-a-coronaviruses
In the last couple of days I recall seeing some experts (in China, perhaps?) seem to believe that there are outliers where the incubation has been up to 28 days, but this seems uncertain, and even if true, only a very small percentage of people.
I would imagine that R0 of any disease would be heavily influenced by its incubation period. For example, influenza’s incubation period is 1 to 4 days, according to this (first result to a search): https://www.healthline.com/health/flu-incubation-period#incubation-period – that means that COVID-19 can be unknowingly spread for up to 10 days MORE than influenza, before people begin to feel symptoms.
So even if COVID-19 has the same exact chances of transmission per each interaction as influenza, COVID-19 would have more than 3 times as many opportunities to infect others (number of interactions) before the carrier notices symptoms.
Here’s the passage I’m thinking of
https://arstechnica.com/science/2020/03/dont-panic-the-comprehensive-ars-technica-guide-to-the-coronavirus/2/
Thanks for that. I was not aware.
I no longer have the source, I think it was in one of Dr. John Campbell’s video reports, but a credible report out of China maintained that droplets can and do remain air borne for over half an hour and that people can catch the disease at OVER twice the distance as previously thought (which would be over 12 feet). These observations came about from analyzing the video of a 4hour bus ride where a passenger infected was sitting in the back part of the buss and yet infected another passenger who was sitting more in the front – at, over or near 12 feet apart. Moreover, when both of those passengers got off, another person who got on half an hour later was also infected from the remaining air borne droplets. The analysis was apparently very careful (history of each player researched) and thorough to avoid false positives, etc. and relied largely on the way everything in China is so closely monitored.
Adding that in practical terms, (adapted from a comment by Ignacio -though I’m responsible for mangling it) this means to reduce time spent in Supermarkets or other areas with climate conditioning (such as cool air from a closed source – that everyone shares- circulated throughout) and possibly wear masks (not in US) during such periods to be thrown away (such as in a plastic bag) immediately upon exit. Also try as much as possible to work it so you are in such venues when least crowded. Note that masks do not apply in the US because we need to reserve them for medical personnel.
Brooklin Bridge-
The article was posted in South China Morning Post several days ago.
There was some question to the fact the the persons sitting far away from the questioned passenger was already exposed before getting on the bus.
Regardless due diligence is needed.
Right now I am at small town in Utah (St George) and there is resident who is in self quarantine. I traveled here to do a Mountain bike race. Not really feeling motivated for racing. Thinking about how to navigate this pandemic.
Best of “good luck” and I mean it simply. If you are athletic, you already have that going for you.
Perhaps that study is mentioned in this article that summarizes a UCLA report that the droplets can remain in the air for “up to 3 hours.”
https://thehill.com/policy/healthcare/487110-tests-indicate-coronavirus-can-survive-in-the-air
Thank you and best wishes ,Ignacio.
I think you gave good advice.
I add a couple of links about the Covid diffusion.
The first shows, if I get it correctly, that in my country the virus arrived from Munich. This is consistent with what our media reported.
https://nextstrain.org/ncov?fbclid=IwAR1E6Z6TVdFE0-P3GfhjsnVuU7Q475aeAG0JpcXg-Us8IDHdM91DWN0xWvM&label=clade:A2
The second is more global
https://nextstrain.org/ncov
Some good news from Italy!
My friend’s spouse in the Bergamo hospital reports that admission have dropped to the level of discharges! The local hospital system is now stable (at a wartime level of activity, but stability is everything).
Two serial intervals have passed since the Lombardy lockdown last weekend so this means that:
– R0=1 from that weekend (possible from earlier, locally, because of spontaneous social distancing).
– we can expect it to fall below 1 from next week, as incubation periods pass. If it falls to say 0.3, the chains should die out completely within a month (10 intervals) and should probably be low enough for trap and trace to isolate new cases well before that.
This is corroborated by the fall in new cases in the first region to be quarantined, Lodi and Codogno. The epidemic should die out nationally in a week or two.
If you check out the logarithmic plots on http://www.covid19.health (I cannot praise this website enough) you can see the curves bending flat and the daily cases dropping precipitately in Italy and South Korea.
This epidemic is CONTROLLABLE.
Ona related note, the UK government is INSANE to choose to “let her rip” through the population in pursuit of speculative herd immunity. Either the policy will change shambolically in the next few days or the government will fall.
And now some good news from the UK!
Bojo and Brains and the Nudge Unit are on the run!
https://www.theguardian.com/world/2020/mar/13/uk-to-ban-mass-gatherings-in-coronavirus-u-turn
Let’s not let a good crisis go to waste – let’s keep our pitchforks sharp and push them all the way to the left and force an MMT financed relief of people and business and massive investment in integrated healthcare.
This Time It’s DIfferent!
Thank you Ignacio for the lucid, calm breakdown of events in your part of the world and your advice
something Canadian health officials are also recommending and as as my daughter reminded me yesterday, something I have been practicing for my entire life; finally a socially acceptable time to be an introvert ;)
In Karlsruhe, Germany, we have now South Korean style drive through testing boxes. You are not supposed to just go there, but follow this protocol:
If you feel any symptoms, that might be associated with CoVid-19 phone your family doctor. Together evaluate the likihood, that you are really infected. Then make an appointment with the drive through, go there (you can walk or bike there as well, you don’t have to have a car), and let them take a sample. The result will be there in about 24 hours.
The claim is, that
– the likelihood of infecting other people is fairly low, if you keep at least 1m distance to other people during your walk to the testing station
– less protective clothing for the testers is necessary
https://www.ka-news.de/region/karlsruhe/coronavirus-karlsruhe./Erster-Corona-Drive-In-in-Karlsruhe-So-funktioniert-der-Abstrich-durchs-Autofenster;art6066,2508683
Of course you should not just go to the hospital, but testing is important and the Spanish health officials really should try to get a similar solution.
Btw. as well politicians in Germany have been pretty consistently communicated, that you should use the phone rather than go into a hospital or something like that, if you have symptoms.
I was suspecting this. Germany is more or less the European South Korea regarding testing, although confirmed cases are in line with those of France or Spain, Germany epidemics is one step lower. You can tell that watching casualties and recoveries. Early massive testing during the containment phase is good idea to make people aware of the problem, promote isolation and keep R0 lower from the very beginning. (too late for France, Spain or the US IMO: go for mitigation directly)
I think some authorities (and here I include HC authorities who should now better) have erroneously think that tests are just for diagnostics. Quite wrong, it is above all an excellent tool to keep epidemiology on track and help containment.
Someone should tell European politicians about Moon’s approval ratings in Korea now – they are sky high, his handling of the crisis has been very popular (at least so far), despite the best effort of the right wing opposition to politicise it.
https://twitter.com/AskAKorean/status/1238452002193113089
And in further good political news, Bolsonaro in Brazil has just tested positive!
I agree, but we have to recognize the limits of testing. There is a fairly high false negative rate (you are infected but test negative), and sometimes multiple tests are needed for a given patient because the first sample was inadequate. Here’s an excellent summary of this issue. This is why self-quarantine based on symptoms rather than based on tests is important. But you are right, massive testing is needed for other reasons. Too bad the CDC flopped on delivering this crucial need for the American people. Because, you know, WHO is the U.N., and we can’t just use Chinese or WHO tests because we’re exceptional. Now we find out that CDC is ill equipped to oversee massive production and distribution of tests. Something tells me: profits.
Excellent link!
I’m curious about alternative testing. I caught a segment on CNN-I last night, that the Univ of Nebraska had developed a test that could deliver a result in ~4 hours; the approved one, making occasional appearances when its too late to really matter, needs to be mailed off for centralized processing. The U of N people had to jump through a bunch of hoops to use their product locally.
Then, there is the guy who founded alibaba.com in China, who has announced a donation of 500,000 tests to the US. Details aside, I wonder whether they would be accepted, the fatal ego of the US being at stake.
thank you Ignacio, you’ve been wonderful; please be cautious – you aren’t too far from Italy where CV has taken off like wildfire… I’m stunned by how high the death rate there seems to be. They are rationalizing it here by saying that the Italian population is older than most – a good 20% are seniors. I don’t really buy it; I suspect they’ve got a nasty strain of Covid-19. It is just starting to hit here in Utah – the Utah Jazz, naturally. My instincts tell me that if the Jazz players are getting it (2 so far), the entire NBA is as well. And all of their howling fans. So I continue to suspect that the incubation period from well to illness is more than “14 days”. And the above charts seem to be saying so. That nothing can be measured until the immune system kicks in. So with similarities to HIV among their RNA snippets, it will not surprise me if Covid-19 hides away for long periods of time, maybe months. When it takes off in Utah I’ll have a better idea of just how long it takes, dating from 3 days ago. So March 10th. Citizen science, ha.;-)
I think I’m having the Corona right now. Can’t be certain, it could be just the flu.
My symptoms:
Sore throat. Not especially sore at any point, very mild. It feels like there is stuff going on in there, but nothing is coming out and it’s not really irritating. It’s more like the feeling that you keep swallowing because of the feeling, if anyone can relate.
Very little sputum production, so it’s ‘dry’, but I’m not really coughing because there isn’t actual irritation.
No nasal congestion or runny nose, at all.
Feverish feeling or very slight fever, around 36.5 celsius body temp. I don’t actually know what is my standard healthy-feeling body temperature, currently I have just the datapoint from feeling ill.
Headache.
I was feeling pretty ill and confused for 3 days, without any significant fever.
Very slight muscle aching without any physical activity at few places, not the whole body.
Curious hot sensation in my left thumb at times, this is kind of silly one.
I think I had very slight problems of breathing and stinging/cutting feeling below both ribs at few times, but I think these could be my imagination because I have felt them rarely and only very briefly.
So for me the most obvious symptoms were and are currently headache, sore throat, feeling weak/ill and confused. Could be just a flu. I’m little doubtful about the flu because in my recollection most of my previous flus have been hit-like-a-truck fever chills and then the flu clearing relatively quickly in just 2-3 days. This however feels weird slow burning flu with very little symptoms, except feeling ill for 4 days now. I was never really sneezing or coughing at any point. I could easily be out and about with ibuprofen, but I’m choosing to self-quarantine myself.
Can’t get tested because I’m lacking serious symptoms so far and no known contacts to confirmed epidemic areas or local confirmed cases. Although I do have recent contacts to infection dense area not declared risk zone in other european country and the symptoms started manifesting about 3-5 days after the contact.
So it is 1. coronavirus or 2. normal flu and my mind is just playing tricks on me. Unless I end up in hospital later I will probably never find out the truth. Symptoms kind of match flu, but also kind of match Corona. I’m aged between 20-40, no pre-existing conditions that I know of, average fitness and average BMI, so I’m part of cohort expected to have extremely mild infection to the best of my knowledge.
Looks pretty much what I have been reported by my friends. I bet corona but do not panic. 4 days now with symptoms, you don’t report respiratory problems which so far is good news. I believe you are in the midst of it. Isolate yourself and take care.
Thanks for the reply. I still think I am making this up.
My biggest confirmation would be developing pneumonia now, but the thing is I don’t want to get pneumonia. Healthcare refuses to see me with my extremely mild symptoms so I guess I will get tested only if I end up in hospital later. Which I do understand, I would never go to see doctor with mild symptoms like these normally.
However it would be very nice to know whether this is corona or flu.
Actually googled now quickly and my symptoms match this ladies details very well:
https://nypost.com/2020/03/12/woman-who-survived-coronavirus-shares-her-early-symptoms/
Only real difference is the lack of significant fever or fever chills, but for me it started noon. She also did not have coughing or shortness of breath. Also my weird left thumb tingling kind of matches this womans ‘tingling’ of extremities.
Don’t give up. At some point if serum from volunteers is asked you can go and get done a serological assay.
Did you have a temperature of 103 like the Seattlite? Over 20 years ago I came down with the flu/pneumonia? and I had a temperature of 102. That hit me like a truck. But your fever symptoms, fortunately, appear to be rather mild.
It really stinks that people on the cusp can’t get tested easily, or at all.
I didn’t get similar fever, I measured 36.5 several times when feeling feverish, which translates to 97.7.
Currently I’m feeling almost normal feverwise and my temperature is 36.1. So compared to that I had slight fever.
Your symptoms seem similar like mine. A bit of a feverish feeling, but no fever. Low grade cough, but not a lot of irritation. Sneezing: more than regular, but not often. Little bit of soar throat. Heavy head, especially when moving. Slight chest pain when breathing, almost not noticeable. Going on for 3-4 days now. Mornings hardly any symptoms, evenings some more. Didn’t feel the need yet for ibuprofen
Could be a common cold, plenty of that going around.
Hummm. I am starting today with something similar. Some cough and heavy head. Hypocondriavirus or any other thing?. Self-isolated just in case.
Much as I hate to do it, I am sharply cutting my social life. And, yes, I am going for bike rides and avoiding gatherings.
What are the bike rides for? Preventing cabin fever?
You swiped the words right off-a my keyboard, Katy. Preventing cabin fever, depression, and boredom.
Oh, data point from yesterday: I’m brewing up my first batch of beer. Needed bottles. So, I biked over to my favorite brewing supplies store.
Much to my surprise, the store wasn’t a ghost town. It wasn’t super busy either. But the guys behind the counter echoed the sentiment that I shared:
If it’s not a good idea to go out to the bar, I might as well learn how to brew my own.
I’m not their only customer who’s thinking that way.
Thank you Ignacio. Best wishes to you and yours.
Be safe and well, everyone.
There are no reliable data for the U.S. because we lack adequate testing gear. Some testing kits have been distributed but many are incomplete, lacking the necessary reagents.
Here in the SF bay area a few new cases are being reported every day but they no doubt represent a small fraction of the actual infected.
Being a news junkie and among the vulnerable, I saw this coming pretty early on and hope we got a bit ahead of the curve by stocking up and social distancing before the panic buying and shutdown of public events.
To my discredit I must admit to experiencing a certain degree of guilty pleasure in the way this crisis is revealing for all to see, the inadequacies of the U.S. healthcare system and its social safety net. Maybe some good will come of it. May we all survive to see that day.
We don’t have testing because that is what Trump wants: no data on its spread leaking into the news talking heads to interfere with the marketing. It’s not hard to figure this Administration out. Just look at past Apprentice shows. It’s all there.
Weirdly, speaking of marketing, my PBS TV station is still running a plethora of cruise ship and travel ads. At the same time, the local station, KQED, operates one of the more informative, paywall free web pages on Covid-19 developments in the SF bay area.
I never watched The Apprentice but I did listen to an interview on Fresh Air yesterday, White House Knew Coronavirus Would Be A ‘Major Threat’ — But Response Fell Short. The interviewee was Dan Diamond from Politico. It was quite horrifying. I’m opposed to capital punishment but in truth, some people need guillotining.
Although Trumps response has been lamentable there is no evidence any other president would have acted differently. Nancy was busy having her impeachment party rather than spending time working on a containment strategy, she is, or was against suspending The House.
The US and UK response is seriously negligent. In the UK the government is talking about developing herd immunity! The Pols really do see us as cattle.
This may well prove a decisive moment in the US, I think when the population sees the Kleptocrat Class walk away unscathed because they have access to the best medical care and the rest of 99% of the population shelters at home as hospitals are overwhelmed while having to watching loved ones die at home. It will be interesting how the Pols argue against single payer healthcare as the virus rages across the country and the election approaches
Frankly, that’s an outrageous statement. I do not have Trump Derangement Syndrome and I’m no fan of Pelosy. I tend to look at everything in balance and perhaps with a skeptical eye. However, the way that this has been handled would have never ever been done under any other president in living memory, from any party.
How about this for starters (from https://www.snopes.com/fact-check/trump-cut-cdc-budget/):
Then you have the constant downplaying of “it’s just like the flu”. I simply can’t imagine any serious president in my life doing this stuff.
Pelosi has said that they are the Captains and will not abandon ship. If Congress is not in session in the capitol building, no laws can be passed.
It may be time to update the rules & regulations concerning the House & Senate.
SCOTUS can decide cases via phone and email and, as seen after 9/11, can meet at any location to hear arguments.
As for Trump, I can’t remember a President giving such a poor speech to the nation. Even Nixon’s resignation speech was delivered with more veritas.
The man cannot read aloud. His delivery of this hastily-written address was at about the same level as his address after the Iranian rocket attacks.
look at how it deals with climate change, shut down the EPA etc. Enough said. Yes most Dems suck. No they don’t actually do this.
That is the only silver lining we can hope for.
From what I’ve read elsewhere the RO is calculated from an equation whose terms or variables change because dependent upon circumstances or conditions. Taking the equation apart is a good way of understand what the RO is.
Another way of evaluating transmission is using stochastic methods, as Adam Kucharski did in a Lancet paper modeling early transmission in Wuhan: https://www.thelancet.com/journals/laninf/article/PIIS1473-3099(20)30144-4/fulltext
His Twitter stream is worth following, my new morning chore.
Thanks. and that’s much better than the essay by Bob j. They’ve got the code and data online too on github. There’s some real math there. And real data science. I liked it that they “proved” their model by seeing how well it predicted actual data ( though I’ve yet to check whether this was of data unseen by the model ). And most of all they give this :
The factor being : “high individual-level variation in transmission makes new chains of transmission more fragile, and hence it becomes less likely that a single infection will generate an outbreak”.
Now that’s something “actionable” – that much hyped and misused word in data science. And based not on “common” sense but on some science. Hence “testing”, “testing”, “testing”, which sadly the USA federal level agencies have failed, appallingly failed at.
I’ll check out his twitter stream too.
A chain reaction in a fissionable isotope of U or Pt is a good analogy – R0 is the average number of secondary fissions induced by fission of a single U or Pt nucleus. Each nucleus aborbing a neutron (catching the disease) will fission (become contagious) in some time frame which can vary widely between nuclei (infectees) but which is characterized by a well-defined average latency (incubation period). Each fission releases multiple secondary free neutrons which will strike other unfissioned nuclei (uninfected individuals) at some point unless they are absorbed by some material impurity (social distancing or patient isolation) or exit the mass via its physical boundary (national/natural borders). Effective “bending of the infectivity curve” means a chain reaction starts but fizzles out. Not bending the curve, well…
“I am inconvenienced by being unable to leave my house. Many in America will temporarily lose employment. In the third world people may starve if they cannot work.”
A less blinkered version: “I am inconvenienced by being unable to leave my house. Many (outside the bubble) in America will temporarily lose employment and may starve because they have no unemployment insurance, medical insurance or any savings, having been forced into the “gig economy” where there are no workers rights aginst their will by the bi-partisan consensus of indifference in Washington. Growing swaths of sacrifice zone America are third world.”
What a president might look and sound like, if we had one that was
not a sociopath, a buffoon, or an apprentice zombie:
https://www.youtube.com/watch?v=2As11EyIRWc&feature=youtu.be&t=730
Thanks for posting. The contrast with Trump’s shallow, border-minded speech is impossible to deny. He’s serious, thorough, and makes it clear no one will be left behind. Trump’s speech actually had a “we’re gonna think up something” for the working class:
Bernie will be hosting a chat at 2pm EST
https://live.berniesanders.com/
Well, Obama gave us soaring rhetoric™ while bailing out, richly rewarding and legally immunizing the Wall Street fraud cartels, continuing the imperial slaughter and starting more of it (Syria, Libya, Yemen), so methinks you and the West Wing fanboi-set perhaps put too much credence in appearances. The most dangerous sociopaths are the smooth-talking MSM-adored ones, because they get free rein to work their evil magic.
Trump being dismissive of the threat early on surely didn’t help, but he was far from the only world leader who was so. CDC testing-kit #Fail was on them, and as others have noted, once the gravity of the threat is manifest, social distancing is far more important – but of course the same folks blaming Orange Foolius for every misstep in crisis response were also doing so for his shutting down air travel from Europe. Plenty of blame to go around at all levels. Let’s see, in Italy the leadership took the spreading infection far too lightly and now has a national disaster … in Germany we have a well-spoken leader whose “leadership” has consisted of going to parliament and in non-buffoonish terms announcing that “70% of Germans may well catch Covid-19.” Thank you, that was so very well-stated, madam chancellor … but, uh, is there perhaps some things we could actually *do* to reduce that nightmarish estimate?
Examples of effective leadership seem to be the exception, not the rule – China getting praise for shutting half the country down, but hello? The same leadership utterly ignored the clear early warnings from their own experts and went ahead with, among other things, a lavish Chinese new year’s festival banquet in Wuhan, finger food for 40,000 people, which led to an explosion in new cases. “Arsonist turns hero, helps fire crews limit spread of blaze he started” comes to mind.
@OP: But yes, hopefully some of this fine-sounding stuff actually gets turned into legislation that passes both houses and gets signed by the Stable Genius. Oddly, that other DC institution which gets called on a lot in emergencies, the Fed, needs no such congressional or presidential approval to implement its own emergency measures, such as the just-announced $4.5 T (yes, that’s a “T”) emergency liquidity facility to help reinvigorate the Wall Street speculator class. No one ever asks the Fedsters “how will you pay for that?”
This is an excellent discussion of the problems related to use of diagnostic testing in medicine. Anyone who wants to comment on testing needs to be aware of this concept.
https://towardsdatascience.com/statistics-and-unreliable-tests-coronavirus-is-difficult-to-contain-e113b5c0967c
Short version: the utility of a test depends not only on its sensitivity (test is positive when infection is present) and specificity (test is negative when infection is not present). A test with a 90% sensitivity and 90% specificity may be useful to verify infection when infection is highly likely (e.g. patient has all the symptoms, travel history, contacts etc.) but not very useful as a screening test.
For example if the test is used randomly to test 1 million asymptomatic individuals, all of whom are infected, 100000 will be falsely identified as “safe”and if none of the same population are infected, 100000 will be identified as “carriers”. So the utility of the test to determine appropriate treatment of an individual depends not only on the sensitivity and specificity of the test, but also on the prior probability that the person has the infection.
These concepts are essential to determining how testing will be used to determine the response to the pandemic. The problem of false negatives is particularly important in preventing spread. The ideal approach for controlling spread is to treat everyone as infectious, regardless of test results, however this is the approach that inflicts the maximum social and economic damage as non-infectious individuals are subjected to quarantine procedures.
Another obstacle to social distancing in the extremely unequal USA: most single people under a certain age have roommates, at least in major metros.
I have tried to do all the social distancing, but my roommates don’t seem to be. One just came back from the grocery store with stacks of ramen and I wanted to shout at her that the time to do that was last week.
The other roommate still isn’t permitted to work from home. We share a kitchen, bathrooms, front hall, doors in, doors out.
I have yet to read anything addressing this reality, which confirms me in my impression that the media are by and for the highly affluent, especially the older and highly affluent.
I enjoyed this presentation of the math of epidemics, very clear with good graphics:
https://www.youtube.com/watch?v=Kas0tIxDvrg
Can a math person explain to me how any metric, other than confirmed diagnoses and confirmed disease-related deaths, are in any way useful? If no one has the slightest idea of how many people have the disease but are asymptomatic (children, especially) or are slightly sick but with mild symptoms. How can disease burden be estimated without an idea what the total infected by the disease is? It would be one thing to say, “Of people tested, this number have symptoms and this number have died.” Is there some connection between total disease infections (an entirely unknown number) and total population tested (a potentially known number)?
Denmark is closing down – even borders are being closed today, and really tourists would be very disappointed to go here. Everything is closed – schools, universities, museums, libraries, fitness etc.
We have a discussion here. Sweden and UK have chosen another strategy. What is the right thing to do?
This article has convinced me that we may be on the right track.
Coronavirus: Why You Must Act Now
Politicians, Community Leaders and Business Leaders: What Should You Do and When?
https://medium.com/@tomaspueyo/coronavirus-act-today-or-people-will-die-f4d3d9cd99ca
Persistence of coronaviruses on inanimate surfaces and their inactivation with biocidal agents
https://www.sciencedirect.com/science/article/pii/S0195670120300463
I am in the U.K. I have Chinese nationals in my team at work. They are so horrified by the U.K. government approach that some are thinking of returning to China because it’s safer there. They have first had experience of what it takes to contain the disease because they were visiting relatives at new year.
Boris seems to be ignorant of the scientific method and instead is intent on testing his hypothesis on 40 million people. Understandably he is not finding 40 million willing participants in his experiment to generate herd immunity. So there is little democratic support for his strategy and people are essentially ignoring advice and going into lock down if they can without waiting for the government to tell them to.
The problem is the U.K. government haven’t published their modelling nor more importantly, the assumptions that underlie the model.