Yves here. I have to confess to having missed out on the devastating impact that Covid-19 would have on addicts in recovery. This population is likely to make a meaningful addition to “excess deaths,” which is the metric many are using to adjust reported Covid-19 deaths to include ones that were probably missed, such as deaths at home. Clive and QuarterBack may have more to add on this issue.
The problem is, as the medics and scientists will point out, it’s still important to understand who died of the disease, narrowly speaking, as well as who fell victim due to broader societal impacts.
By Markian Hawryluk, the senior Colorado correspondent for KHN, who has written for as the Houston Chronicle, American Medical News and, most recently, The (Bend, Ore.) Bulletin. He has won numerous awards for his health reporting from the Association of Health Care Journalists and the Society of Professional Journalists and, in 2009, won Oregon’s top reporting prize, the Bruce Baer Award for investigative journalism. Originally published at Kaiser Health News
Sara Wittner had seemingly gotten her life back under control. After a December relapse in her battle with drug addiction, the 32-year-old completed a 30-day detox program and started taking a monthly injection to block her cravings for opioids. She was engaged to be married, working for a local health association and counseling others about drug addiction.
Then the COVID-19 pandemic hit.
The virus knocked down all the supports she had carefully built around her: no more in-person Narcotics Anonymous meetings, no talks over coffee with a trusted friend or her addiction recovery sponsor. As the virus stressed hospitals and clinics, her appointment to get the next monthly shot of medication was moved back from 30 days to 45 days.
As best her family could reconstruct from the messages on her phone, Wittner started using again on April 12, Easter Sunday, more than a week after her originally scheduled appointment, when she should have gotten her next injection. She couldn’t stave off the cravings any longer as she waited for her appointment that coming Friday. She used again that Tuesday and Wednesday.
“We kind of know her thought process was that ‘I can make it. I’ll go get my shot tomorrow,’” said her father, Leon Wittner. “‘I’ve just got to get through this one more day and then I’ll be OK.’”
But on Thursday morning, the day before her appointment, her sister Grace Sekera found her curled up in bed at her parents’ home in this Denver suburb, blood pooling on the right side of her body, foam on her lips, still clutching a syringe. Her father suspects she died of a fentanyl overdose.
However, he said, what really killed her was the coronavirus.
“Anybody that is struggling with a substance abuse disorder, anybody that has an alcohol issue and anybody with mental health issues, all of a sudden, whatever safety nets they had for the most part are gone,” he said. “And those are people that are living right on the edge of that razor.”
Sara Wittner’s death is just one example of how complicated it is to track the full impact of the coronavirus pandemic — and even what should be counted. Some people who get COVID-19 die of COVID-19. Some people who have COVID die of something else. And then there are people who die because of disruptions created by the pandemic.
While public health officials are trying to gather data on how many people test positive for the coronavirus and how many people die from the infection, the pandemic has left an untold number dying in the shadows, not directly because of the virus but still because of it. They are unaccounted for in the official tally, which, as of June 21, has topped 119,000 in the U.S.
But the lack of immediate clarity on the numbers of people actually dying from COVID-19 has some onlookers, ranging from conspiracy theorists on Twitter all the way to President Donald Trump, claiming the tallies are exaggerated — even before they include deaths like Wittner’s. That has undermined confidence in the accuracy of the death toll and made it harder for public health officials to implement infection prevention measures.
Yet experts are certain that a lack of widespread testing, variations in how the cause of death is recorded, and the economic and social disruption the virus has caused are hiding the full extent of its death toll.
How To Count
In the U.S., COVID-19 is a “notifiable disease” — doctors, coroners, hospitals and nursing homes must report when encountering someone who tests positive for the infection, and when a person who is known to have the virus dies. That provides a nearly real-time surveillance system for health officials to gauge where and to what extent outbreaks are happening. But it’s a system designed for speed over accuracy; it will invariably include deaths not caused by the virus as well as miss deaths that were.
For example, a person diagnosed with COVID-19 who dies in a car accident could be included in the data. But someone who dies of COVID-19 at home might be missed if they were never tested. Nonetheless, the numbers are close enough to serve as an early-warning system.
“They’re really meant to be simple,” Colorado state epidemiologist Dr. Rachel Herlihysaid. “They apply these black-and-white criteria to often gray situations. But they are a way for us to systematically collect this data in a simple and rapid fashion.”

Before the COVID-19 pandemic hit, Sara Wittner completed a 30-day detox program and started taking a monthly injection to block her addiction cravings. Yet the virus destroyed the support system she had built, including stopping her in-person Narcotics Anonymous meetings and delaying that monthly shot of medication. Wittner died in April, and her death is just one example of how complicated it is to track the full impact of the coronavirus pandemic.(Courtesy of Leon Wittner)
For that reason, she said, the numbers don’t always align with death certificate data, which takes much more time to review and classify. And even those can be subjective. Death certificates are usually completed by a doctor who was treating that person at the time of death or by medical examiners or coroners when patients die outside of a health care facility. Centers for Disease Control and Prevention guidelines allow for doctors to attribute a death to a “presumed” or “probable” COVID infection in the absence of a positive test if the patient’s symptoms or circumstances warrant it. Those completing the forms apply their individual medical judgment, though, which can lead to variations from state to state or even county to county in whether a death is attributed to COVID-19.
Furthermore, it can take weeks, if not months, for the death certificate data to move up the ladder from county to state to federal agencies, with reviews for accuracy at each level, creating a lag in those more official numbers. And they may still miss many COVID-19 deaths of people who were never tested.
That’s why the two methods of counting deaths can yield different tallies, leading some to conclude that officials are fouling up the numbers. And neither approach would capture the number of people who died because they didn’t seek care — and certainly will miss indirect deaths like Wittner’s where care was disrupted by the pandemic.
“All those things, unfortunately, are not going to be determined by the death record,” says Oscar Alleyne, chief of programs and services for the National Association of City and County Health Officials.
Using Historical Data To Understand Today’s Toll
That’s why researchers track what are known as “excess” deaths. The public health system has been cataloging all deaths on a county-by-county basis for more than a century, providing a good sense of how many deaths can be expected every year. The number of deaths above that baseline in 2020 could tell the extent of the pandemic.
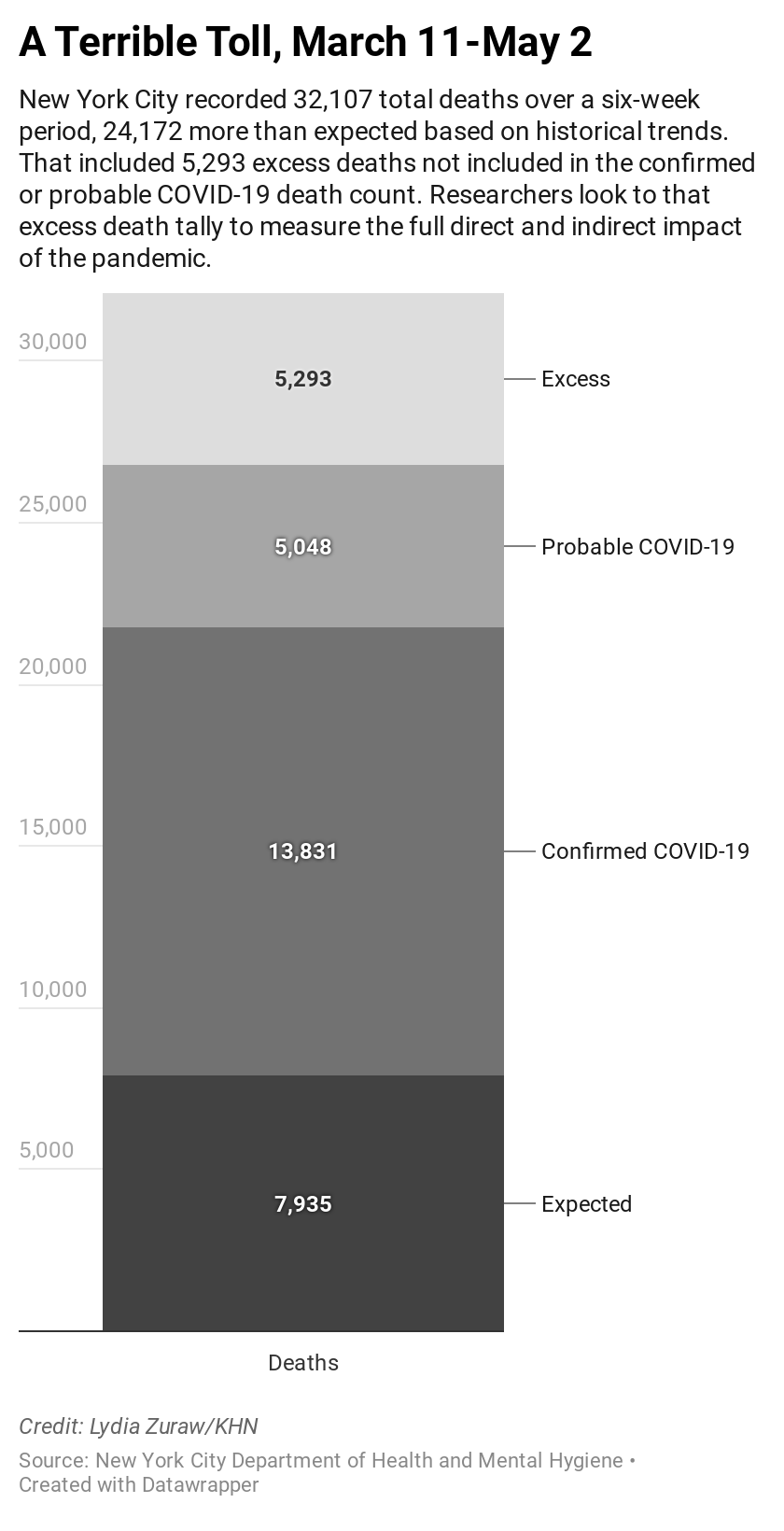
For example, from March 11 to May 2, New York City recorded 32,107 deaths. Laboratories confirmed 13,831 of those were COVID-19 deaths and doctors categorized another 5,048 of them as probable COVID-19 cases. That’s far more deaths than what historically occurred in the city. From 2014 through 2019, the city averaged just 7,935 deaths during that time of year. Yet when taking into account the historical deaths to assume what might occur normally, plus the COVID cases, that still leaves 5,293 deaths not explained in this year’s death toll. Experts believe that most of those deaths could be either directly or indirectly caused by the pandemic.
 City health officials reported about 200 at-home deaths per day during the height of the pandemic, compared with a daily average 35 between 2013 and 2017. Again, experts believe that excess is presumably caused either directly or indirectly by the pandemic.
City health officials reported about 200 at-home deaths per day during the height of the pandemic, compared with a daily average 35 between 2013 and 2017. Again, experts believe that excess is presumably caused either directly or indirectly by the pandemic.
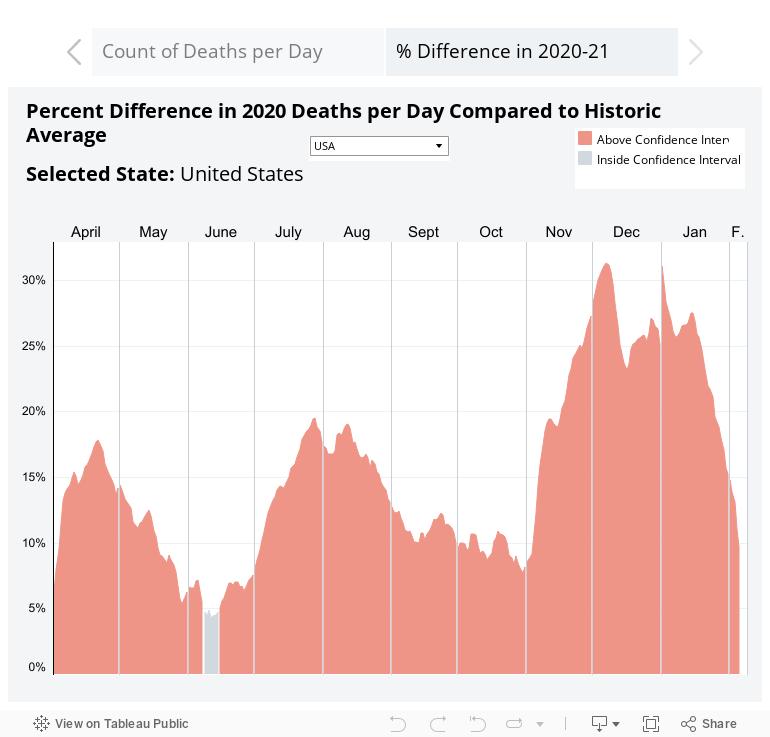
And nationally, a recent analysis of obituaries by the Health Care Cost Institutefound that, for April, the number of deaths in the U.S. was running about 12% higher than the average from 2014 through 2019.
“The excess mortality tells the story,” said Dr. Jeremy Faust, an emergency medicine physician at Brigham and Women’s Hospital in Boston. “We can see that COVID is having a historic effect on the number of deaths in our community.”
These multiple approaches, however, have many skeptics crying foul, accusing health officials of cooking the books to make the pandemic seem worse than it is. In Montana, for example, a Flathead County health board member cast doubt over official COVID-19 death tolls, and Fox News pundit Tucker Carlson questioned the death rate during an April broadcast. That has sowed seeds of doubt. Some social media posts claim that a family member or friend died at home of a heart attack but that the cause of death was inaccurately listed as COVID-19, leading some to question the need for lockdowns or other precautions.
“For every one of those cases that might be as that person said, there must be dozens of cases where the death was caused by coronavirus and the person wouldn’t have died of that heart attack — or wouldn’t have died until years later,” Faust said. “At the moment, those anecdotes are the exceptions, not the rule.”
At the same time, the excess deaths tally would also capture cases like Wittner’s, where the usual access to health care was disrupted.
A recent analysis from Well Being Trust, a national public health foundation, predicted as many as 75,000 people might die from suicide, overdose or alcohol abuse, triggered by the uncertainty and unemployment caused by the pandemic.
“People lose their jobs and they lose their sense of purpose and become despondent, and you sometimes see them lose their lives,” said Benjamin Miller, Well Being’s chief strategy officer, citing a 2017 studythat found that for every percentage point increase in unemployment, opioid overdose deaths increased 3.6%.
Source: Health Care Cost Institute
Meanwhile, hospitals across the nation have seen a drop-off in non-COVID patients, including those with symptoms of heart attacks or strokes, suggesting many people aren’t seeking care for life-threatening conditions and may be dying at home. Denver cardiologist Dr. Payal Kohlicalls that phenomenon “coronaphobia.”
Kohli expects a new wave of deaths over the next year from all the chronic illnesses that aren’t being treated during the pandemic.
“You’re not necessarily going to see the direct effect of poor diabetes management now, but when you start having kidney dysfunction and other problems in 12 to 18 months, that’s the direct result of the pandemic,” Kohli said. “As we’re flattening the curve of the pandemic, we’re actually steepening all these other curves.”
Lessons From Hurricane Maria’s Shifting Death Toll
That’s what happened when Hurricane Maria pummeled Puerto Rico in 2017, disrupting normal life and undermining the island’s health system. Initially, the death toll from the storm was set at 64 people. But more than a year later, the official toll was updated to 2,975, based on an analysisfrom George Washington University that factored in the indirect deaths caused by the storm’s disruptions. Even so, a Harvard studycalculated the excess deaths caused by the hurricane were likely far higher, topping 4,600.
The numbers became a political hot potato, as critics blasted the Trump administration over its response to the hurricane. That prompted the Federal Emergency Management Agency to ask the National Academy of Sciences to study how best to calculate the full death toll from a natural disaster. That report is due in July, and those who wrote it are now considering how their recommendations apply to the current pandemic — and how to avoid the same politicization that befell the Hurricane Maria death toll.
“You have some stakeholders who want to downplay things and make it sound like we’ve had a wonderful response, it all worked beautifully,” said Dr. Matthew Wynia, director of the University of Colorado Center for Bioethics and Humanities and a member of the study committee. “And you’ve got others who say, ‘No, no, no. Look at all the people who were harmed.’”
Calculations for the ongoing pandemic will be even more complicated than for a point-in-time event like a hurricane or wildfire. The indirect impact of COVID-19 might last for months, if not years, after the virus stops spreading and the economy improves.
But Wittner’s family knows they already want her death to be counted.
Throughout her high school years, Sekera dreaded entering the house before her parents came home for fear of finding her sister dead. When the pandemic forced them all indoors together, that fear turned to reality.
“No little sister should have to go through that. No parent should have to go through that,” she said. “There should be ample resources, especially at a time like this when they’re cut off from the world.”


In Sara’s case fentanyl was the killer. Why hasn’t something been done to control the use of fentanyl and the dangerous black market for it? A few years ago they were blaming China for the black market. It could be any manufacturer. After the way Big Pharma has behaved during this Coronavirus Crisis, I’d be willing to believe that they are supplying the black market – they have no integrity at all. And fentanyl is notoriously deadly. WTF? The least we can do is make good anti-drugs and sell them over the counter to dramatically ease the pain of detox. That’s just a no-brainer. Take the market away from the profiteers and save the addicts at the same time. A two-fer.
Think Quaalude. Basically impossible to get these days. Key ingredients are only producible in pharma grade facilities but a 1984 (ish) international treaty super strictly regulates their production and distribution. Not sure why we haven’t replicated/expanded this treaty… oh wait big pharma would loose profits.
Well, the War on Drugs, like Prohibition, are failures. Where there is demand, there will be a market, be it licit or illicit.
What creates the demand for fentanyl?
Manufactured despair.
There can be no doubt that immiserated,guilt shamed populace is the easiest to manage.
The combination of iron,unflinching propaganda and a subliminal, bleak awareness of lack of democratic agency is both cheap and effective.
Source: DEA Intelligence Report Fentanyl Flow to the United States January 2020
Globalization, the grift that keeps on giving…
I know of two people who have died of overdose during this pandemic. One lost his job. The other had been on and off using for a long time. Family thought he’d turned the corner.
I consider them both deaths of despair that are strongly linked to his pandemic. The family says that the lockdown killed their son.
The number of anonimous and sad death stories that are indirect effects of the pandemic must be very large all around the world and many specifically associated with the lockdowns so, “doubly indirect”. Another case for study are the victims of domestic violence that have been shown to increase at least in some places where there is accounting for this during lockdowns.
Job losses are going to be one of the more lasting and damaging consequences of this and will unfold in lots of ways. As unemployment relief is removed during “recovery” probably much faster than the recovery itself, new casualties not coincident with lockdowns or epidemic peaks will appear. IMO these economists that so cheaply talk about dis-incentivation of work are somehow the modern versions of Dr. Mengele though instead of using prisoners, they use the population at large for their “darwinian” (my apologies for Dr. Darwin) social experiments.
I definitely agree.
I can only blame so many people for this, in the end. A virus that kills is a fearsome thing to deal with since it preys on us being social animals. There’s things we can do better, things we can do much better, but I don’t see how we could have gotten around some kind of massive harm, either at the frontend (no lockdown) or at the backend (the years of long tail economic harm.)
this is truly a sad accounting and I am sure just one of many corollary deaths.
It is so obvious that there are “inconsistencies” in just tabulating direct deaths and infections which are critical for understanding the overall extent of infection spread in order to formulate a correct and proportional response. Feature, or bug, be damned–the inconsistencies have the same effect–confusion up and down the chain.
However this statement:
In the U.S., COVID-19 is a “notifiable disease” — doctors, coroners, hospitals and nursing homes must report when encountering someone who tests positive for the infection, and when a person who is known to have the virus dies. That provides a nearly real-time surveillance system for health officials to gauge where and to what extent outbreaks are happening.
directly contradicts the NC Public Radio story I heard yesterday regarding the Meat Processing Plants located in the State of NC and their skirting of “Duty to Report” laws by classifying their Private Tests as just that—Proprietary and therefore exempt from the ‘Duty to Report” (HIPPA was the second reason given). Construction Sites in Charlotte are facing a similar outbreak and have adopted similar “outside the system”testing and reporting–private testing with no reporting.
Although there may be numerous reasons Tyson and others may cite–I have got to believe their Employee Vetting Process is the prime exposure those companies are facing(again and again).
Anecdotal reporting in both Carolinas( because BOTH STATES refuse to release demographic data related to infection(race ok–ethnicity NOT) citing HIPPA again. Greenville County SC is an example with a 9% Hispanic population with 31% of confirmed cases last week.
Regardless, getting demographics in SC means Journalists trolling Zip Codes for data–which certainly is a Feature of the System.
https://greenvillejournal.com/health/covid-19-drastically-affecting-greenvilles-hispanic-communities/
https://www.wltx.com/article/news/health/coronavirus/latino-community-in-upstate-makes-up-30-percent-of-covid-cases/101-59d86441-9e96-4501-8ba9-beb4b76e9876
https://www.postandcourier.com/health/covid19/coronavirus-cases-skyrocket-in-greenville-hitting-hispanic-communities-hardest/article_d3d6393c-b1c9-11ea-9d76-37e79a1ad5fd.html
A buddy of mine is a county sheriff and he says a big reason why liquor stores were considered essential businesses was that they didn’t want people going into withdrawal (DT’s) and ending taking up hospital beds.
Adam1, they were right to call liquor stores essential for exactly the reason your sherriff friend mentioned, it’s an ugly reality.
The income stream of criminal gangs were also affected and they have and will continue to seek alternative sources if income, some of the looting is undoubtedly due to their efforts.
Twice I’ve run into former “bar buddies” on the street and I’ve attended one Zoom reunion of the same and I have to say they look >rough.< These are, and I was until just a few months before the plague, serious bar folk, the kind who come in for happy hour and stay till close because it’s their day off. It’s obvious this group hasn’t slowed down a notch. Blotchy faces, hollow eyes, significant weight gain, the hallmarks of heavy drinking…
My point is I wonder how many plain, regular, non narcotic using drinkers have been pickling themselves at an accelerated pace these last few months. The consequences of such a trend seem obvious…
Drinking during the work day has mostly gone out of style, at least until you could drink in the privacy of your own home while working.
Agreed, assuming you aren’t drinking at home at noon because you’re not working…
The joke going around Ireland has been that they need to open the bars quickly to save everyone from alcoholism.
Given the number of people I’ve seen walk past my window with vast boxes of beer and cider, there is certainly some truth to this.
During the beginning of our local lock downs schools closed about a week before businesses. I remember a meeting shortly before we all went to working remotely where one co-worker commented about the chaos at home with, at the time no real remote learning plan yet in place, kids and everything so uncertain and anxiety driving them nuts. Another co-worker chimed in saying the government is out to turn us all into alcoholics.
Even knowing what we know (collectively) about opioid addiction its hard for me to call an overdose the fault of the lock down. Its relevant to point out that things weren’t so locked down that she couldn’t buy drugs! In the case of this young woman it was a drug overdose, a disease and death of choice. A heart attack seems much less so.
Disease of choice. Not sure you comprehend either or both of those terms.
Barnaby33, someone who has a choice about drinking or using is by definition not an alcoholic or addict.
That’s the nature of the disease, and one reason it is so ugly.
And no, it is not a matter of willpower, ask anyone who has worked with addicts or alcoholics.
This Vast Southern Empire
Slaveholders at the Helm of American Foreign Policy
Matthew Karp
VERY GOOD BOOK!
https://www.hup.harvard.edu/catalog.php?isbn=9780674737259
It’s no wonder that people would be self-medicating, dialing things up a notch .. or to 11 even .. considering that many economic life-lines have been , or soon will be, severed .. seeing as the BigMoney/Power Elites continued to gob at THEIR trough! .. untouched, and unhindered. Thank Nancy&Co. for taking one, or is it 2-4 + Trillion .. (I’ve lost count) for the Team ELITE!
#voiceless votes r us!
I suspect that few of these uncounted deaths need to have happened if the government had encouraged mask wearing on a Japanese scale early in the outbreak. Japan did minimal but strategic shutdown. Mainly schools and large gatherings.
Instead our government lied to us about the efficacy of wearing masks (Dr. Fauci do you hear me) out of fear that purchases would take away from medical professionals, when medical grade were not even needed.
Mask wearing would have been sufficient instead of the less effective shutdown. Now all government credibility is lost.
Failed state America. No leadership. Ruled by ignorant and greedy oligarchs.
For those concerned with this catastrophe:
Our series of online discussions about COVID-19 and drug policy explores how this pandemic has magnified the war on drugs as a public health crisis, how we can sustain progress, which obstacles still remain, and how we can use the current moment to be more aspirational with our policy agendas.
Please RSVP here
http://links.drugpolicy.mkt7185.com/ctt?ms=NDI3OTQyMTkS1&kn=5&r=NTY4MDI0MDkzMTU4S0&b=0&j=MTc4MTk4NTE4MQS2&mt=1&rt=0
to join us for the fourth conversation “New Frontiers: Drug Use, Harm Reduction, and Essential Services in the Time of COVID-19” which will take place over Zoom this Thursday, June 25 from 2-4pm ET.
Another data point is the wife of a relative. She saw her doctor in early March complaining of stomach upset and weight loss. They brushed her off then. She was finally tested in late May. Stage IV cancer. I don’t know if the brush off was due to Covid or not. It should be straightforward to check if the number of cancer diagnoses has dropped during the lockdown and by how much.
Such a damn shame. That Sara Wittner was so young and pretty and now her life is over. What a waste.
The healthcare system is run by unscrupulous tribespeople; that’s why they call it sickcare.
In normal times most are put on ventilators, which are in some state of disrepair, for the money, not because a better outcome is expected. If you can get $100/he, why would you do other jobs for $20/hr?
This is like a gold rush for the hospital functionaries, and the rest can be picked up later. That’s a problem with immorality.
Amoral is a point on a continuum, to deprivation.
Ever see what a broke alcoholic can do to an icu room?
Take digestion through the blood stream and on to the tissues, then reverse it, violently.
This is one of the reasons I’ve been grateful to be an essential worker. Unlimited unstructured time and a government paycheque seem like a dangerous combination for me.
(Tho I’m very much in favour of income supports and the ability to stay home during a pandemic!)