Yves here. Biden repeatedly promised to “follow the science” in developing Covid policies. But as has become the norm in American medicine, the science has instead been distorted in the interest of profits and political expedience. This post provides a devastating takedown of the Biden plan to reopen schools with little in the way of additional protections for teachers and students, particularly more ventilation (how about the simple expedient of opening windows?). It explains why Covid cases among children have been severely undercounted and where population-wide surveys were made, children were vastly more likely to introduce Covid into a household than adults. It also shreds the CDC’s astonishing assertion that distancing as little as three feet would be OK.
On the one hand, parents and children are suffering due to the lack of in-person instruction. Keeping schools closed is politically risky for Team Dem, particularly since it is seen as a staunch ally of the (formerly) powerful teachers unions. But simply pretending that schools can implement hand-wave level measures and everything will be hunky-dory is the sort of wishful thinking that is guaranteed to produce problems down the road, just like our insufficient test capacity and unwillingness to enforce quarantines and mask mandates. As a result, how much luck do you think schools and teachers will have in getting children to wear masks properly (particularly not take them off if they start to cough and keep them over their noses), and how much support will they have from parents if they try to discipline the non-compliant?
Lambert almost immediately challenged the CDC’s recommendations on schools for ignoring evidence on aerosol-based transmission. He also found evidence that they relied on a National Academies of Sciences, Engineering, and Medicine report that punted on the question of “indoor air quality of schools” because addressing it might mean spending money! In other words, they refused to consider the issue at all, even low cost mitigations. This article confirms his concerns and adds quite a few others.
Your humble blogger also expressed doubts about Dr. Rochelle Walensky as the new head of the CDC, that she had signed up for Biden Administration priorities (as in she appeared not to have attempted to negotiate the agenda), some of which looked like an impossibly big leap for a weak agency, and others looked unconstitutional. Two particular weaknesses look relevant to this fiasco:
Fighting yesterday’s war
Treating better PR as the solution to way too many problems
There’s much more information in this carefully argued and well documented piece, which I hope you’ll circulate widely. As we’ve been saying from early on, it’s the disease dynamics that are in control. Wanting that not to be true won’t begin to make it so.
By Deepti Gurdasani, Senior Lecturer in Machine Learning, The William Harvey Research Institute, Queen Mary, University of London; Phillip Alvelda, CEO & Chairman, Brainworks Foundry, Inc.; and Thomas Ferguson, Director of Research, Institute for New Economic Thinking and Professor Emeritus, University of Massachusetts, Boston. Originally published at the Institute for New Economic Thinking website

The scale of disaster visited on the world by the COVID-19 pandemic defies any easy summary. But it is safe to say that the question of keeping schools open is among the most fateful decisions facing public authorities. As the pandemic stretches into its second year, it is now becoming among the most contentious.
In the U.S., after some hesitation, the Biden administration seems to be encouraging rapid opening of schools, despite high levels of community transmission in many places, before robust mitigations are completely in place. Many Republican governors and officials also demand the step, including former President Trump in his recent CPAC address. Languishing under lockdowns and zoom or hybrid classes, many exhausted parents, anxious employers, and bored students seem receptive, though polls show widespread reservations about whether premature reopening might trigger new waves of infections. In recent days, more and more states have moved to mandate full in-person classroom instruction within a few weeks.
Accompanying these decisions are organized efforts to recycle earlier studies of school safety[i] designed to reassure skeptics that reopening schools to full-time instruction is really safe, even as new variants of COVID-19 spread that are more contagious and possibly more dangerous than earlier forms. Even the Center for Disease Control is joining this rush to judgment, suggesting that seating students as little as three feet apart might be an acceptable rule for social distancing.
Bitter experience has taught us a great deal since the beginning of the pandemic. Among the most important lessons we have learned is that it is not, in fact, safe to open schools as the pandemic persists without close adherence to significant and stringent abatement measures.
We begin with the most important point as to how we now better understand the risks that eluded us in prior surges of the virus. In those earlier episodes, many people who in fact had the virus showed few indications that they did, even as they went on to spread it to others. This “asymptomatic” transmission was a genuine novelty that researchers only slowly came to grips with.
Unfortunately, the display of coronavirus symptoms is highly correlated with age, thus the younger the student, the less likely they are to show symptoms, or exhibit what are considered “typical” COVID-19 symptoms. The younger students, therefore, were much less likely to be tested. So they continued participating in the school community even as they spread the disease and even having suffered symptoms and long-term side effects that absent a COVID-19 diagnostic determination, were falsely attributed to other illnesses. As a result, the studies commonly cited as supporting school reopening are deeply flawed; they are based on having only tested students who showed symptoms, rather than applying broad screening tests either universally or with true random samples capable of catching the otherwise undetectable asymptomatic spreaders and infected.
The extent of this bias has now been quantified in several studies in the UK, such as the Office for National Statistics Infection and Household Surveys[ii] and REACT-1 Studies.[iii] These studies randomly sampled large numbers of households within the UK at regular intervals regardless of symptoms. The results are dramatically different from the earlier studies, and even from symptom-based testing from the UK during the same time period; they show that contrary to the conclusions from earlier studies based on biased symptom-only testing protocols, in-person schooling is associated with much higher risk than previously thought. A recent study published by the Center for Disease Control (CDC) from Mississippi confirmed these findings; it showed that case-based reporting of infection in children underestimated infection by between 14-68-fold over May to September 2020 compared with serological surveys.[iv]
With the more recent large-scale random sample testing performed in the UK, Sweden, and the US, we now know the following facts:
1. The secondary COVID-19 attack rate – that is, the rate at which the coronavirus spreads – was actually higher for both elementary and high school students than adults when the schools were open for in-person instruction between April to November in England (ONS Household Infection Survey).[v]
2. Both elementary and high school children were far more likely than adults (2x and 7x, respectively) to be the first case in their households rather than the adults between April-December in England.[vi]
3. The spread of infections among school-age children and in the community closely tracked school openings and closures as well as attendance, with the prevalence of infection being highest in these groups compared to all other age groups while schools were open and tiered restrictions for broader society remained in place. Importantly, particularly with the new variants, growth of the pandemic continued in regions where these variants were prevalent even as other institutions were shut down in the national lockdown in November.[vii]These statistics were mirrored in a recent study on the risk of coronavirus spreading in U.S. schools.[viii]
4. Increases in the prevalence of infection among school-age groups preceded rises of infection in other age groups. This has a vital implication; the new studies suggest that infections among children at school do not just reflect infection rates in the community. Rather, they drive increases in infection within the community through spreading from schools into homes, and from there to the broader community.
5. Claims that teachers do not face serious risks are simply false. The risks of infection turned out to be two times greater for teachers of in-person classes relative to those conducting virtual online classes in Sweden.[ix] The study also found an approximately 40% higher infection risk in England in those in teaching occupations compared to those in non-teaching occupations, even when schools were only partly open (REACT-1 study).[x]
6. Several studies also show an increased risk of infection among parents of primary and secondary school children being taught in-person within schools.[xi]
7. The spread of new, more easily transmitted and more deadly variants underscores the true dimensions of the threat from in-person school instruction. With the new B.1.1.7 variant now surging in many parts of the world, variant cases continued to rise with an R=1.45 (compared to an R of only 0.9 for non-B.1.1.7 variants) even during national lockdown while schools were open. R only dropped below 1 – a critical level for controlling the rate of infection – following complete school closures. The numerous outbreaks linked with B.1.1.7 in school settings across the globe over the past few weeks are of grave concern.
8. Between 12-15% of primary and secondary school children had one or more persisting symptoms 5 weeks after infection, according to an ONS survey that took care to examine all infections, including asymptomatic infections.[xii] Before that study appeared, it had been widely thought that because mortality is low among children exposed to SARS-CoV-2, that children are not impacted. Given we know so little about the long-term implications of “long COVID” syndromes, which at least in adults have been often associated with organ dysfunction, it is important to adopt the precautionary principle, and reckon with long COVID related outcomes in addition to deaths.
9. Recent evidence supports the role of mitigations in reducing the impact of transmission within schools. However, it is clear that multi-layered protections are needed, rather than single or a few measures, as the risk reduction is associated with the number of mitigations in place.[xiii]
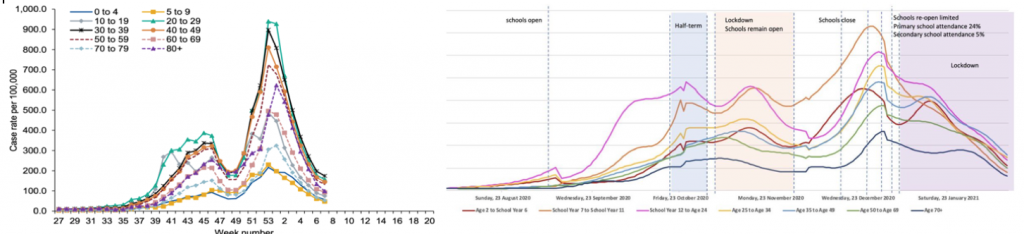
Figure 1 On the left is a graph from an earlier study based only on testing symptomatic U.K. patients that seemed to indicate that children aged 0-19 were the least likely to be infected or carriers of the coronavirus. Such symptom-based data from children are still being used to promote the notion of sage school reopening. The graph on the right shows the data from the large scale ONS study based on random sampling of households across England.[xiv] The latter study catches the large number of asymptomatic carriers, showing clearly that when asymptomatic carriers were counted, those school-age cohorts were, in-fact, the most likely to be infected carriers of the coronavirus. The ONS study also shows the correlation of new case growth in the elementary and high school-aged cohorts with times when the schools were opened for in person instruction and declines over vacation, half-term and shut-down periods.
The coincidence of the rush to reopen with the spread of the new variants of concern to the CDC and the World Health Organization is particularly unfortunate. The new B.1.1.7 variant is both 50% more communicable, and about 30% more lethal than the earlier strains. It is now the dominant and resurgent strain across Europe and is now endemic across the United States. All through the pandemic, the United States has lagged in testing for the virus. It has trailed not only in sheer volume but also in the form of testing: most tests cannot sort out the new more dangerous variants from older forms of COVID-19. Only so-called “genetic survey” tests can do that reliably and they are used only in a few places.
Data from the relatively few U.S. states that use these viral genome survey tests strongly indicate that the now widely reported declining case numbers mask a dangerous, exponential rise in cases of the newer more contagious variants. These appear even now to be turning around the recent falls in total cases in some areas of the country. We expect that in the next few weeks that phenomenon will show more widely.
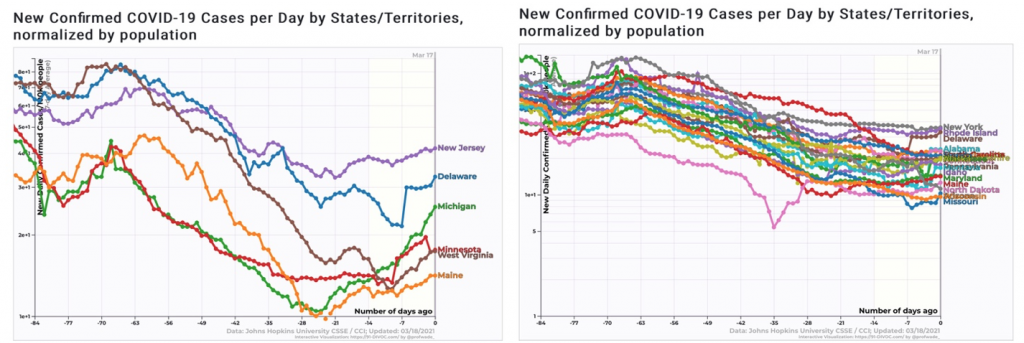
Figure 2 After months of steady decline, we can now see the return of significant growth in new COVID-19 cases across six states where the B.1.1.7 strain is known to be growing in prevalence. Cases are now flat or starting to rise in 21 additional states, and we expect resurgences soon there as well. Relaxation of abatement measures is clearly premature.
Another lingering concern testifying to the persistent impact of outdated science is that so much of schools’ reopening guidance remains aimed at hygienic measures, surface wipe-downs, and plexiglass barriers, all of which are completely ineffective in limiting what we now know is the primary mode of indoor transmission, airborne aerosols.[xv]
The latest CDC guidance suggesting that the risks to students are similar at 6 foot or 3-foot distances and thus that schools can safely reopen with more-or-less normal student seating density and populations in the classrooms completely misses the point. A close analysis of the “3-foot paper[xvi]” the CDC cited shows it to be riddled with errors in protocol, most importantly, that it again relies on data from primarily symptomatic carriers; that it improperly conflates infectious susceptibility with contact rates; and is based on a flawed sampling methodology.
Neither did it measure the actual distancing practices within classrooms, but rather considers guidance at district levels, and only for all schools with attendance greater than 5%. This could mean that schools were wrongly categorized to different distances that were not accurate. Differences in other mitigation measures, class size, or class attendance were also not accounted for. Ultimately, the study is also too small to come to any scientifically supported conclusion, as the results show that the risk of infection among districts with guidance to distance greater than 6 feet could vary from half of those with guidance to distance greater than 3 feet by up to 1.3 times as much.
Most critically, while the authors were correct in saying that there is little difference in risk relative to seating distance, they drew exactly the wrong conclusion from the distance data. Newer science has demonstrated quite definitively that the coronavirus spreads heavily through the air, more so, in fact, than through droplets on surfaces or direct contact. As a direct result, the earlier 6-foot indoor social distancing rule guidance was proven to offer misleadingly false comfort wherever ventilation is poor. A beautifully illustrated and simulated interactive New York Times article highlights “Why Opening Windows Is A Key to Reopening Schools” safely. It’s worth a read, because it also demonstrates clearly why relaxing distancing measures, say to seating students 3 feet apart instead of at a 6-foot distance is not necessarily a good idea.
Contrary to the notion that even 3 feet of distancing is sufficient protection, and 6 feet is overkill, the critical safety issue is that students are all uniformly at risk in poorly ventilated rooms no matter where they are or how they distance. With one infected person in an enclosed and poorly ventilated room, the coronavirus permeates the entire space, putting everyone inside at similar risk regardless of where they sit. The key corrective abatement measure necessary is wholesale improvement in ventilation, filtering, and HVAC systems. Nothing whatsoever in any of the cited studies supports safely moving students closer together.
The Biden administration’s new emergency aid bill contains substantial funding, at last, for states and localities. They could use some of that money to refit ventilation systems in schools and implement rigorous testing programs, and even quickly roll out portable HEPA filter systems. But as of 2020, a GAO study indicated that ventilation and heating systems in slightly under half of the school systems examined required substantial new expenditures to meet code, much less enhanced protection necessary for coronavirus abatement. With substantial federal support only now coming available, properly replacing older ventilation systems with HEPA filters will take time.
And though rapid COVID-19 tests are now available, few public schools can afford the current generation of tests. The simple mathematics of exponential growth and airborne transmission in confined areas means that tests on everybody – students, teachers, and staff, including cafeteria workers and janitors – need to be performed at least twice a week. Testing less often means that the virus cannot be identified fast enough to stop outbreaks from sweeping through schools and that contract tracing and quarantine efforts come too late to be effective. And similar to the VHAC upgrade concern cited above, it will also take time for forthcoming federal aid to flow down to schools and labs to enable frequent and affordable school testing on a national scale. In any case, these tests should not replace robust mitigatory measures within schools, but rather complement a robust, multi-measure mitigation approach.
A reconsideration of the current rush to reopen in-person instruction with less than sufficient mitigations is, therefore, clearly necessary. The understandable hopes for a return to normalcy raised by the stepped-up campaign to vaccinate everyone are premature. The vaccine effort, while gathering momentum, will not reach enough people quickly enough to make opening this Spring safe, without more robust mitigation measures within schools. And the costs of making a rushed mistake based on outdated science will take too long to become obvious.
We understand and sympathize deeply with the pain that the continued delay of reopening causes our colleagues and fellow citizens. But it cannot make sense in the actually existing state of most public schools (or, for that matter, all but the most affluent private schools) to push to reopen without all the critical mitigations, as this will once again potentially lead to educational disruption in the form of school closures and further lockdowns. Better to ensure schools can remain open once they do restart through robust mitigation, ramping up testing, ventilation, and, above all, vaccinations than send new waves of sick students, teachers, and parents to already overstretched hospital and emergency medical facilities in a third resurgence of the coronavirus, and unnecessarily put a generation of students, teachers, and parents at risk of Long COVID side effects.
Reopening most schools now, before most schools lack robust protective measures, and don’t yet have broad ability or finances to conduct frequent surveillance testing to prevent asymptomatic spreaders of the latest, more dangerous coronavirus variants from infecting their community, is thus very unwise.[xvii]
Notes:
[i] Bailey, “Is it Safe to Reopen Schools,” CRPE
[ii] Coronavirus (COVID-19) Infection Survey, UK Statistical bulletins
[iii] Munday, Jarvis, Gimma, Wong, van Zandvoort, “Estimating the impact of reopening schools on the reproduction number of SARS-CoV-2 in England”, CMMID, number.cmmid.github.io
[iv] Hobbs, Drobeniuc, Kittle, Williams, Byers, Satheshkumar, Inagaki, Stephenson, Kim, Patel, Flannery, “Estimated SARS-CoV-2 Seroprevalence Among Persons Aged <18 Years — Mississippi, May–September 2020,” CDC Morbidity and Mortality Weekly Report.
[v] Hyde, “Difference in SARS-CoV-2 attack rate between children and adults may reflect bias,” Clinical Infectious Disease, inacademic.oup.com
[vi] “Children’s Task and Finish Group: update to 4th Nov 2020 paper on children, schools and transmission”
[vii] Gurdasani, Alwan, Greenhalgh, Hyde, Johnson, McKee, et. al., “School reopening without robust COVID-19 mitigation risks accelerating the pandemic,” The Lancet
[viii] Chernozhukov, Victor; Kasahara, Hiroyuki; Schrimpf, Paul. “The Association of Opening K-12 Schools and Colleges with the Spread of Covid-19 in the United States: County-Level Panel Data Analysis,” CESifo Working Paper No. 8929, March 2021.
[ix] Vlachos, Hertegård, Svaleryd, “The effects of school closures on SARS-CoV-2 among parents and teachers,” PNAS
[x] Riley, Wang, Eales, Haw, Walters, Ainslie, Atchison, Fronterre, Diggle, Ashby, Donnelly, Cooke, Barclay, Ward, Darzi, Elliott, “REACT-1 round 9 final report: Continued but slowing decline of prevalence of SARS-CoV-2 during national lockdown in England in February 2021.”
[xi] Vlachos, Hertegård, Svaleryd, “The effects of school closures on SARS-CoV-2 among parents and teachers,” PNAS ;
Lessler, Grabowski, Grantz, Badillo-Goicoechea, Metcalf, Lupton-Smith, Azman, Stuart, “Household COVID-19 risk and in-person schooling”
Forbes, Morton, Bacon, et. al. “Association between living with children and outcomes from covid-19: OpenSAFELY cohort study of 12 million adults in England,” BMJ Husby, Corn, Krause, “SARS-CoV-2 infection in households with and without young children: Nationwide cohort study”
[xii] “Updated estimates of the prevalence of long COVID symptoms,” ONS
[xiii] Lessler, Grabowski, Grantz, et. al., “Household COVID-19 risk and in-person schooling”
[xiv] Riley, Wang, Eales, Haw, Walters, Ainslie, Atchison, Fronterre, Diggle, Ashby, Donnelly, Cooke, Barclay, Ward, Darzi, Elliott, “REACT-1 round 9 final report: Continued but slowing decline of prevalence of SARS-CoV-2 during national lockdown in England in February 2021,”Real-time Assessment of Community Transmission Findings”
[xv] Prather, Marr, Schooley, McDiarmid, Wilson, Milton, “Airborne transmission of SARS-CoV-2,” Science.
[xvi] Van den Berg, Schechter-Perkins, Jack, Epshtein, Nelson, Oster, Branch-Elliman, “Effectiveness of three versus six feet of physical distancing for controlling spread of COVID- 19 among primary and secondary students and staff: A retrospective, state-wide cohort study”
[xvii] Gurdasani, Alwan, Greenhalgh, Hyde, Johnson, McKee, et. al., “School reopening without robust COVID-19 mitigation risks accelerating the pandemic,” The Lancet


I note a couple items missing. First, any discussion of the counterpoint, meaning the cost to young people without in-person education. Shouldn’t there be a cost benefit discussion in an unbiased report? Second, I do not see a reference to a study on the prevalence of asymptomatic spread. I saw something recently, possibly related to in-person schooling in the US, that listed asymptomatic spread as being less than 1% of positives. I continue to look at medrxiv.org and I see no studies showing that asymptomatic spread is a real thing.
What I do find in this are a lot of reference to studies saying “… in England”. What are the data points in the US? This is anecdotal, but the state I live in has had in-person learning for K-12, colleges and universities since the fall session began. Peak cases and hospitalizations occurred months after, not 2-weeks after the re-introduction of in-person education. In my community we had one professor die from C-19. He taught at a university with tens of thousands of students. He contracted C-19 *before* school began in the fall.
In my state, C-19 hospitalizations are currently about 3% of bed capacity, while just under two-thirds are occupied for other reasons. I mention this because lockdowns were about saving the healthcare system. If you look at hospitalization rates in the US as of March 7, 2021 at covidtracking.com, the highest hospitalization rate in the US is for New York. Washington DC and New Jersey are close company. These are hard lockdown locations – obviously. If you look at the 6 states that never locked down, their numbers on case fatality, positivity, hospitalizations and yes unemployment are all better than Florida and the national average.
Asymptomatic transmission, not spread.
> Peak cases and hospitalizations occurred months after, not 2-weeks after the re-introduction of in-person education.
Given that a peak results from a rise followed by a subsequent decline, not sure how this is relevant. More relevant would be the timing of the rise after the prior trough, in relation to the timing of changes in public policy that could affect transmission.
This comes off as if you did not read the post in full, as is required by our site Policies. It makes clear that only the UK (Imperial College) has been testing large numbers of the population (100,000 each time, distributed by age, gender, geography, etc) every six weeks or so. It’s called Real Time Assessment of Community Transmission. We don’t have anything even remotely like that. The UK data is vastly better than anything in the US. Our testing is just about the worst in the world.
And we have pointed out repeatedly that Covid deaths are not a good metric of health costs. Covid does serious ant potentially permanent damage to nearly everyone who gets it. A large scale study in Texas found that 100% of symptomatic cases and 70-80% of asymptomatic cases showed lung damage worse than if they’d been pretty serious smokers. Not clear if that damage will ever abate. Covid also leads to Long Covid (often in asymptomatic cases), heart and liver damage.
Link to the Texas study? I find this incredibly hard to believe.
I have quoted this repeatedly:
https://www.cbsnews.com/news/covid-lungs-scarring-smokers-lungs/
The fact that the lung damage article is from January 15 and that its dire findings have not led to heavily publicized followup studies over the ensuing two months is astounding. I want to get jokey and wonder about CBS’ ratings but, really, what is going on here?
Dr. Bankhead-Kendall is a co-author on this study from July 2020 (Lancet), Mortality and pulmonary complications in patients undergoing surgery with perioperative SARS-CoV-2 infection: an international cohort study. I expect that many of the cases she has seen were also included in that study’s data, and that her comments to CBS reflected patterns she saw throughout 2020.
A quick google scholar search turned up several papers to which she contributed data (at least). In most of those papers the data being presented were from the first half of 2020. It’s likely that other papers are in the works, analyzing data captured later that year.
One notable paragraph from the linked paper: “Mortality in patients with SARS-CoV-2 was mainly in those who had postoperative pulmonary complications, which was about 50% of patients. This rate is far higher than the pre-pandemic baseline; in the POPULAR multicentre, prospective, observational study of 211 hospitals from 28 European countries in 2014–15, the pulmonary complication rate was 8%. In our study, ARDS had the highest mortality rate of the different complications (mortality 63·0%) and occurred much more frequently (20%) than reported in the pre-pandemic African Surgical Outcomes Study (0·05%). In another study of high-risk ASA grade 3 patients undergoing non-cardiac surgery in seven US centres, 0·2% developed ARDS, with an overall mortality related to postoperative pulmonary complications of 2·3%. Even considering differences in the case-mix, the incidence of and mortality associated with pulmonary complications in SARS-CoV-2-infected patients is disproportionately high.”
That’s not a large scale study, that’s anecdata.
if she’s correct, there is somewhere between 24 and 30m folks (that’s the known cases) in the US with irreversible lung damage. And it’s gone completely undetected save for some fine detective work by a “an assistant professor of surgery with Texas Tech University in Lubbock”. What are the odds?
Did you miss:
Chest X-rays are typically not administered casually due to concerns over cancer risk. Modern equipment is supposedly much lower dose and safer and therefore not a big deal, but I personally resist getting an X-ray unless really necessary because I have doubts as to how well machines are maintained.
I imagine there were no shortage of Victorian grandees who sniffed that the “cost benefit” trade-off of water sanitation to control Cholera wasn’t to their liking either.
What drives me bonkers is the continued reliance on “positive case” numbers which are based largely on the very flawed PCR tests. The problems with high cycle thresholds (Ct) are well known, but without knowing the Ct counts for the test results we don’t know if they are run at 35 or fewer cycles (thus reasonably accurate) or at say 38 or 40, which renders them pretty meaningless.
Separately I found today via The Automatic Earth that in the UK the Office of National Statistics (ONS) has apparently been reporting single-gene target PCR test results as positives instead of requiring at least two-gene targets, as specified by the test manufacturers:
Source for the above (emphasis added): ONS Admits Ignoring Manufacturer Instructions in PCR Testing
Original BMJ source: Positive results from UK single gene PCR testing for SARS-COV-2 may be inconclusive, negative or detecting past infections
Again, I cannot trust any widely-reported PCR “positive” test results without additional information. So much public policy is based on flawed testing. And note these false-positive “cases” are affecting the mortality statistics as well, particularly in the UK where any “positive COVID test” within 28 days prior to death counts as a covid death.
“What drives me bonkers is…”
I prescribe a nice cup of tea and a new hobby.
Rest easy knowing you’ve cracked the code, if that makes you feel good.
Trust me, nobody “upstairs” cares what you or I think should be the case, so don’t waste your cpu cycles trying to change it.
Thank you for this post. It is good to read, especially now with all the hype from Biden. As I read this I tripped back to Jr. High and remembered the johns. They were always a mess. Bordering on filthy sometimes. I’d guess this piece by Gurdasani doesn’t go there because the underlying research is so solid regardless. But the stats indicate that 30 – 40% of all adult Covid cases are intestinal; they never turn into respiratory Covid. But that doesn’t mean that intestinal transmission can’t cause respiratory illness (I would think.). And considering that toilets flushing cause aerosols… So maybe these statistics for this post could double-down. Let’s say it’s twice as bad as Gurdasani is estimating. And in response to the plea for more stringent measures, I’d just say it’s virtually impossible, beyond opening the windows. As far as “fighting yesterday’s war” goes, I think therein lies the answer. What do we educate for anyway? To produce a competent workforce. OK. So what are the jobs of the future for these kids. They could well be outdoor jobs; green jobs. Maybe we could give them another year of lockdown, but relieved by lotsa field trips. Exploring an empty lot can be a field trip. Walk along the river. Identify trees and birds. And for that matter, why don’t we change the school-year altogether if we are faced with a new reality of Covid-like pandemics: Let’s “go to school” only in summer when the sun is shining and the breezes are warm. May thru September. And the other 8 months rely on remote learning and a certain amount of self learning. I really do not think keeping kids out of school for another year is a bad thing. I think it is probably the wisest choice. One tele course they need is on learning to learn. Give them tools for analysis; more careful reading skills; etc. Send them both computers – to communicate – and books. And coordinate neighborhoods so friendships can still form. Etc. One good thing – serendipity – would be that kids might get more sleep. They are all sleep deprived these days.
I believe the information in this post portends a growing wave of Corona’s spread, perhaps reaching an even higher wave crest than before. The Government, CDC, and National Academies of Sciences, Engineering, and Medicine, appear all too willing to sacrifice the last remnants of their credibility to accomplish this harm. I can only wonder how members of the teaching profession will deal with this insult to their health and safety. I imagine more than a few aspirants to teaching might be rethinking their goals. I remain amazed at the Corona tests available, their cost, their lack of availability, and their absence from application as the US launches this ill-considered experiment at spreading the Corona virus. The ventilation in schools was a problem before these Corona days. It was hazardous to staying awake in class.
At https://www.microbe.tv/twiv/twiv-734-2/ Daniel Griffin discusses school opening and long covid among children.
“TWiV 733: COVID-19 clinical update #54 with Dr. Daniel Griffin
March 20, 2021
In COVID-19 clinical update #54, Daniel Griffin covers effectiveness of 3 vs 6 ft physical distancing, effectiveness of masks, physical distancing, and eye shields, second vaccine dose completion, alleviation of COVID-19 symptoms after vaccination, vaccine trials in children, and IDSA approval of a mAb cocktail.”
Also see https://www.microbe.tv/twiv/twiv-731/
“TWiV 731: The kids aren’t alright
March 14, 2021
On a TWiV tetramer, we review the ongoing outbreaks of Ebolavirus disease in DRC and Guinea, evidence that SARS-CoV-2 infections in children are far more prevalent than are being detected, and recent long COVID estimates from the UK.”
Much of policy and what is said is driven by both ideology and financial interests, which includes that regarding the virus and pandemic. My cynicism and skepticism is at an all-time high and I assume almost nothing with a high degree of confidence, and even honest experts may be misled by faulty or jiggered data, hidden agendas from established sources, cognitive distortions from political or financial considerations, or psychological manipulation. I’m not sure what to think any more.
I see a huge missed opportunity that’s just a few steps away from my house. It’s a city park, that, for the most part, has been sitting there, empty.
Why haven’t spaces like this one been used for outdoor-based classes? Just in this park, there is a community garden. Great place to learn about botany and agriculture.
The covered basketball court? Wonderful venue for a socially distanced classroom. Plenty of room for a whiteboard or two.
The trees? Horticulture lessons, all day and every day.
And the ball fields? Fabulous places to run around and blow off steam.
These are great ideas. At the very least I would think organized, outdoor Phys Ed classes would be very low risk for pretty big reward. I have no worries about any material my daughter has “missed” bc I can help her learn that. It’s the social aspect that’s really been missed.
not even remotely possible – imagine all the potential liabilities and issues: children sneaking away, easy approach and access for anyone wishing to do harm (child molesters, kidnappers, shooters), bad weather days, etc.
In some districts, teachers aren’t even allowed to keep doors open out of fair of school shootings.
This shows how idiotic America has become. Kids walked to and from school when prevailing crime rates were way higher than now. The odds of a child being kidnapped is 1 in 300,000. The odds of a parent running over their own kid and killing them is 22X greater.
I expect that kids were also more aware of their surroundings in terms of risk assessments… if only to avoid the other gang from school and get pushed around.
I remember when kids had their rifles in their truck because they were going hunting after school. ;-)
Hear Hear Yves and all comments beginning with “I remember when …” I have taught middle school in the US and France and am amazed at what can be learned with “outdoor school”. So much more complexity and interest outdoors than in the classroom, in a chair. During Band class, our Praying Mantis egg sack (Ootheca) hatched. Hundreds of the insects emerged. As I encouraged students to take a few home and release them, they asked (the students, not the mantids) what do we feed the mantids? I replied “they love aphids” – to blank stares. Not one of the 60 kids knew what an aphid was. We set our instruments down to go into “the field” to find thistles covered in aphids.
Upon re-entry to the classroom, thistles in hand, the music and learning were much improved. Their air (wind instruments) was stronger, attention increased, and the joy of being human, either as student or teacher was supremely evident. At day’s end, kids lined up in the Band room to take home a mantis and release it in their garden. I envision outdoor school as the future of education.
More data please from the readers, especially the ones who may be involved with the best private schools:
1) FL schools are open and the Corona rates are down. What mitigation/testing regime is Florida using?
2) What are the big-name private schools schools doing? What mitigation and testing setups? I mean not only boarding schools (Phillips Andover, Exeter, Ms Porter’s, etc), but also day schools– Catholic (especially the DC schools attended by our elite’s kids); private (Sidwell Friends in DC where the Dem. kids go and the three or four famous ones in NYC); Jewish day schools in NYC/Great Neck, LA, Houston, SF, etc. Just possibly this isn’t a crisis for our leaders- only for the rest of us.
3) How is this effecting Ivy/MIT acceptance rates and what do they plan to do next year?
4) Anacdotally, the best private colleges in the midwest (St. Olafs, Carelton, etc) are open with a serious commitment by students, families, faculty and employees to do it right. Why are their plans not being published and copied?
5) How has this affected test scores by location, class, gender, race, etc? Are the private school kids being equally affected (I’d love to hear from insiders on the college acceptance side).
Just goes to show how effective the jailing of even a single data scientist can be.
Governments across this country and the world have been working overtime to suppress the facts about this pandemic in service of multiple failed attempts to “reopen” their economies. They’ve been caught red-handed lying about not only what research shows is the threat to public health, but also what they’re (not) doing about it. Political leaders all seem to have acquired their own “reality distortion” fields, and somehow the public — even more gullibly than the press, who are _paid_ to believe in nonsense — is buying it.
The coverage here on NC, at times almost alone, has been excellent. The evidence of duplicity, incompetence and venality by government and for-profit health has been documented as thoroughly as anywhere, in real time, and without pulling punches. Anyone who reads this blog regularly who can’t accept these truths is probably beyond rational persuasion at this point.
Just like those who lived through the “Kansas Flu” (by now everyone must know it didn’t start in Spain, but was delivered to the world through the medium of the American Expeditionary Force) of 1918 and _its_ equally preventable repeating waves through 1919.
They apparently were bloody minded about masks:
https://www.usatoday.com/story/news/investigations/2020/09/28/florida-schools-reopened-en-mass-feared-covid-surge-hasnt-followed/3557417001/
Florida also seems to eschew fully enclosed buildings when possible. Mid priced hotels often have a lobby in one building and then covered walkways to the entrances to the buildings with rooms, a design you seldom see in CA outside very high hotels where the walkways have beautiful views. I assume this carries over to a lot of other building designs.
Having said that, infection rates are rising in Florida, but not long enough yet to call a trend.
Yves,
I love this site and have helped support if financially, but I totally disagree with this article. The fact that kids still aren’t completely back in school with no masks, etc., is a disgrace. The best comment I’ve heard is that these children are being robbed of their birthright. I couldn’t agree more.
I live in California, where all the clowns can’t actually fit in the car, and my wife is a public school teacher, so I hear all the front line stuff that way. The public comment portion of our school board meetings has basically turned into a continuous haranguing of the board by angry parents telling the board to pull their heads out of their asses and get the kids back in school. Those type of comments outweigh the keep screwing the kids over comments by at least 20 to 1. Take that for what it’s worth, but I seriously doubt any parent would willingly put their child in danger if they thought a classroom was dangerous.
And to top it off, you have the union for LAUSD teachers telling its members not to post vacation pics on social media (it’s spring break time here) because pictures of people out in public being free and not living their lives under a cloud of fear undermines their militant/not validated by science or data position that it’s not safe to be back in the classroom. Politics and stupidity ad infinitum.
The fact that you don’t like the piece does not make it inaccurate. You need to explain why the extensive medical research it provides is wrong. Your position is basically that teachers should get sick and kids should infect their families (did you miss the data that school age kid are 2 to 7 times as likely as adults to infect a household?!?!). How about arguing for improved ventilation and very strict masking rules instead, like kids get sent home?
My poorly ventilated 2nd grade classroom wants a word with you John. And no masks as well? Good lord. It appears everything I’ve been told about airborne transmission was false.
We need a “Madeline Albright Award” ,for policies like this.
Oh, and a “Judy Miller Award” for Journalists.
Editorial nit: first word of the article — “The” — got chopped somehow?
Thanks for running this piece! Very helpful and now bookmarked.
If I thought our political class were really worried about the education of our children, I might be willing to cut thrm some slack on this intense desire to open schools. Remote learning is not effective. But we have mountains of evidence that education is of no real interest. This is about business and money.
Not only are they ignoring inconvenient facts regarding the spread, children’s exposure, but long term damage that can occur in even asymptomatic cases. There has been no massive push to improve ventilation. Hell they aren’t even telling the schools to open the windows.
I think about that one Broadway show where the majority of people working it got Covid. Sure there was singing and no masks but they were together for less time a day than any school. It didn’t matter. It wasn’t just cast and crew. Ushers got it. They would be more than six feet away. But the disease traveled throughout the air all through building.
Some schools won’t have the stagnant closed atmosphere of a theater. But some do have that same limited access to fresh air and older heating and cooling systems. The vaccines only promise you won’t get as sick. So what happens when there are multiple mild cases with long term lung damage. Are there even any studies whether children show any lung and heart damage after exposure, or was the assumption that they were immune mean no one consider children might still be infected but asymptomatic not just carriers.
I worry not just because friends and family are teachers who could be put at risk but because the long term effects of exposure could be so deadly to the children if the immunity assumption is wrong.
Oh well we will know all too soon. Unfortunately if things go south, the same brilliant folks making the decisions now will probably be the ones deciding how to handle the fallout.
Yves,
Thanks for the article.
Agree, it’s top notch as usual. I wish I read it earlier this weekend.
This David Spiegelhalter and Andrew Masters article in The Guardian may be of interest
https://www.theguardian.com/theobserver/commentisfree/2021/mar/14/speedy-covid-tests-are-very-useful-but-not-conclusive
With rapid COVID tests, the false positive rate is low (0.03%-0.1%). However, if the proportion of positive results is very low, then most positive results will probably still be false and the true number of cases will be lower.
The false negative rate for rapid tests is about 50%, so that if the proportion of positive results is slightly higher, then more positives will be missed, and the true number of cases will be higher still.
In the UK, currently about 0.45% of tests are positive, so that the true number of cases is likely to be higher (by 2x(0.45%-0.1%) missed cases).