By Lambert Strether of Corrente.
The CDC, newly headed by Biden appointee Rochelle Walensky, has issued guidance on school re-opening. From the Associated Press:
The Centers for Disease Control and Prevention released its long-awaited road map for getting students back to classrooms in the middle of a pandemic that has killed nearly 480,000 people in the U.S. But the agency’s guidance is just that — it cannot force schools to reopen, and CDC officials were careful to say they are not calling for a mandate that all U.S. schools be reopened.
Officials said there is strong evidence now that schools can reopen, especially at lower grade levels….
The guidance was issued as President Joe Biden faces increasing pressure to deliver on his promise to get the majority of K-8 schools back to in-person teaching by the end of his first 100 days in office. He acknowledged that the goal was ambitious, but added, “It is also a goal we can meet if we follow the science.”
This post will follow the science; it’s an open question, however, whether CDC did, as we shall see. There are two key documents:
1) Operational Strategy for K-12 Schools through Phased Mitigation (“Strategy“) (updated Feb. 12, 2021), which provides guidance to the schools, and
2) Transmission of SARS-CoV-2 in K-12 schools (“Transmission“) (updated Feb. 12, 2021), which documents “the science” upon which the guidance is (putatively) based. (Readers may wish to jump to the Appendix, where Table 2 lists, categorizes, and provides quotations from the 61 sources cited in Transmission. Scanning the quotations may provide an approximation of the science as CDC understands it, at least with respect to Covid, schools, and children. I will use select citations from Table 2 in Table 1, when I take a look at CDC’s use of epidemiogy.)
There are two central issues with Strategy. The first might be labeled its Central Dogma. The second is the action items in Strategy. Here is the CDC’s Central Dogma:
The occurrence of SARS-CoV-2 infection in schools reflects transmission in the surrounding community.
That is, schools themselves are not drivers of transmission, but rather, as it were, passive recipients of it. This is certainly disputable, for example in this recent thread on Montréal:
6) Dr. Drouin noted that Montreal schools have become a driving force in the spread of the #coronavirus since reopening last month, blaming them for the increase in #COVID19 cases among the 0-to-17 and 35-to-44 age demographics, the latter being parents.
— Aaron Derfel (@Aaron_Derfel) February 11, 2021
See also this recent thread on the UK:
A few things to note:
1. The infection rates among primary & secondary school children closely follow school openings, closures & levels of attendance. E.g. We see a dip in infections following Oct half-term, followed by a rise after school reopening. pic.twitter.com/dqyfAhtPPu— Deepti Gurdasani (@dgurdasani1) February 18, 2021
I will have more to say about reasoning from other countries to this one later in the post. But for now, consider these two tweets as prima facie evidence that the CDC’s Central Dogma is open to question. We will pass on from that topic to the central focus of this post: The CDC’s action items. From Executive Summary of Strategy, here they are:
You will notice immediately that aerosol transmission is omitted; the message of Strategy is that aerosol transmission can be ignored because it is not an “essential” element. This message is getting through; from an acute summary of Strategy in WaPo, “The CDC’s plan to reopen schools seems to prioritize expediency over teachers’ health“:
Here’s what the guidance does well. Unlike the Trump administration’s watered-down recommendations that were couched in language such as wearing masks “if possible,” these new guidelines are clear on many points. They lay out five mitigation measures that every school should implement: masking, distancing, hand-washing, cleaning and contact tracing. The part I like the most is how the CDC has divided schools into four categories based on degree of covid-19 transmission in their surrounding communities. At low and moderate levels, full in-person learning can occur; at higher levels, hybrid or reduced attendance is recommended.
Again, the CDC’s “mitigation strategies” omit discussion of aerosol entirely (even to ventilation). Frankly, I was gobsmacked. I hate to deploy terms like “criminal malpractice,” so I won’t, but such was my level of gobsmacked-ness. Further, if you accept, as I do, the SARS-COV-2 can be transmitted by aerosols, the CDC Transmission document — “the science” backing up the recommendations — rests on a very modest epidemiological base. Let’s consider first the CDC’s suppression[1] of aerosol transmission.
The CDC Suppresses Aerosol Transmission: Why?
First, let’s define our terms. From an excellent article in Journal of Hospital Infection, “Dismantling myths on the airborne transmission of severe acute respiratory syndrome coronavirus-2 (SARS-CoV-2)“:
There is little doubt that SARS-CoV-2 is transmitted via a range of airborne particle sizes subject to all the usual ventilation parameters and human behaviour. To clarify the terminology used in this article, therefore, droplets are particles that fall to the ground (or any surface including vertical surfaces) under the influence of gravity and/or the momentum of an infected person’s exhaled air; and aerosols are particles that remain suspended due to size and/or environmental conditions.
I would summarize this by saying that particle behavior is what matters, not arbitrary size constraints. Aerosols float, like cigarette smoke. Droplets are ballistic; they fall, like tiny loogies. Hence, whenever you hear somebody advocating a distance measure, like the six feet recommended by Strategy, you’re hearing someone protecting against droplets, but not aerosols, because aerosols can float for long distances. Aerosols, again like cigarette smoke, gradually fill up any closed space into which they are emitted. El Pais has an especially vivid discussion of this in “A room, a bar and a classroom: how the coronavirus is spread through the air“:
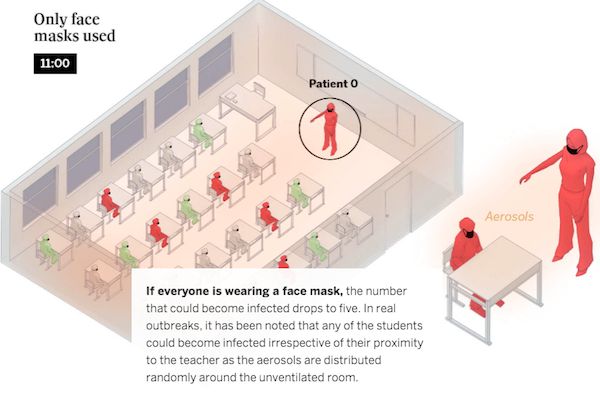
(The figures are based on the Covid Airborne Transmission Estimator developed by a group of scientists led by Professor José Luis Jiménez from the University of Colorado.) I saw that El Pais article cited innumerable times on the Twitter by people reacting to CDC’s aerosol-suppressing guidance, so I imagine at some point the CDC and the White House will become aware of it.
Now, to be fair, aerosol vs. droplet transmission has been a bit of a paradigm shift for the public health community (con vs. pro)[2]. However, until CDC Strategy came out, I had thought that aerosol transmission was settled science; that the shift had occurred. El Pais once more:
In the spring, health authorities failed to focus on aerosol transmission, but recent scientific publications have forced the World Health Organization (WHO) and the CDC to acknowledge it. An article in the prestigious Science magazine found that there is “overwhelming evidence” that airborne transmission is a “major transmission route” for the coronavirus, and the CDC now notes that, “under certain conditions, they seem to have infected others who were more than six feet [two meters] away. These transmissions occurred within enclosed spaces that had inadequate ventilation. Sometimes the infected person was breathing heavily, for example, while singing or exercising.”
Now, however, the CDC is backsliding; of the many institutions and publications supporting aerosol transmission I”ll pick Harvard’s T. H. Chan School of Health, since Walensky is surely familiar with it:
4/ The decision to open schools is complex, controversial, & emotional. Everyone wants students & teachers to be safe. The gist of all reputable reports on school re-opening is a layered approach, but critical to address the airborne component of spread. https://t.co/aQTHnv57w7
— Dr. Alex Huffman (@HuffmanLabDU) February 13, 2021
But why the backsliding? (Walensky’s message discipline is such that she didn’t mention either aerosols or ventilation in her interview on Face the Nation.) I believe the answer is to be found in the source cited in the very first footnote of our second document, Transmission. From The National Academies of Sciences, Engineering, and Medicine, “Reopening K-12 Schools During the COVID-19 Pandemic: Prioritizing Health, Equity, and Communities,” at section “The Role of Airborne Transmission of COVID-19“:
In the process of writing this report, the committee repeatedly returned to conversations around the role of airborne transmission of COVID-19. As described in Chapter 3, indoor air quality in U.S. public schools is notoriously poor, which can have innumerable deleterious health impacts on students and staff. However, because there is not yet scientific consensus on the role of airborne transmission in the spread of the virus, it is also unclear how the indoor air quality of schools matters in the spread of COVID-19. Given the considerable cost associated with updating aging facilities, it is particularly important to understand the exact role of airborne transmission such that stakeholders can assess the relative value and utility of that investment.
Needless to say, this is a budgetary — hence political — constraint, not “the science.” Nor could it be! And sadly, by reducing the question of aerosol transmission and indoor quality to facilities they enable the CDC to deny children, parents, and teachers simpler methods of mitigation:
5/ Zilch on use of single-zone portable HEPA air filters to supplement ventilation, boost equivalent ACH, or help reduce concentrations of aerosol particles when students are out of room, which lowers levels on return & can signif' lower daily dose. Incredibly disappointing.
— Dr. Richard Corsi (@CorsIAQ) February 13, 2021
Shoddy work all round.
The CDC’s Epidemiology Is Weak
Now let us turn to “the science,” as presented in Transmission. Let me explain why, while I respect the other methods of scientific work being done with Covid — statistical work, aggregator reports, metastudies, and miscellaneous narratives — I find epidemiological studies — with index cases, seating and airflow diagrams, contact tracing, etc. — essential. For a policy maker, no doubt all the methods listed are important. But for me as an individual, they are not enough. A metaphor may help. For a World War I General asking his soldiers to go “over the top,” a likely casualty rate will have informed his decision. But the soldier needs to know the actual ground; where the barbed wire is, when to duck the machine gun fire, etc. With Covid, I would want to know the actual ground, too, no matter the odds: For example, I know it makes no sense to sit downwind from an air conditioner in a closed space, even if it makes sense to enter the closed space in the first place. Only “shoe leather” epidemiology can provide such answers. For example, I would certainly want to know whether the windows in my child’s classroom could be opened, if they can be, and whether they are.
However, epidemiology, being of the ground, is necessarily localized and not global. For example, here is a description of schooling in Norway from an American who spent a year as a teacher there.
After every 45 min or so of lessons, students spend 10 to 15 minutes playing outside or in common areas– as many as five or six times a day. At many schools teachers hold on to the students’ cell phones all day in a “cell phone hotel” and encourage real play during break times, like a short pick-up game of soccer or foosball or just jumping around with friends for a few minutes. And during this time, someone always opens a window to let in a little fresh air, even in December.
Obviously, that’s a well-ventilated school (and one that dilutes any aerosols that are to be found). And yet, I doubt very much whether any of the global, statistical work that includes data from Norway takes these facts on the ground into account. How would they now? And yet, given that aerosol transmission is “the science,” those facts are essential. With that in mind, let us look at all the epidemiological studies in Transmission, extracting the relevant rows from Table 2 in Appendix 1:
Table 1: Epidemiological Sources in CDC’s Transmission of SARS-CoV-2 in K-12 schools
| 45 | Finland | Epi | School | Art | Ot | 07/30/20 | Transmission of SARS-CoV-2 following exposure in school settings: experience from two Helsinki area exposure incidents. Preprint. MedRxiv |
| When the index was a child, no school transmission was identified, while the occurrence of an adult case led to a 16% AR. Further cases were evidenced in 3 families, but other transmission chains were plausible. It is likely that transmission from children to adults is limited. | |||||||
| 60 | France | Epi | Choir Room | Art | Fi | 12/23/20 | High Rate of SARS-CoV-2 Transmission Due to Choir Practice in France at the Beginning of the COVID-19 Pandemic. J Voice. |
| The characteristics of the viral transmission via close human contacts was probably enhanced by the act of singing, at a phase of intense circulation of SARS-CoV-2 in the population at this period. We report in our study the role of asymptomatic infection carriers initiating a silent chain of transmission of the coronavirus, leading to a cluster under the circumstances of the rehearsal. This study confirms that the transmission of the virus from asymptomatic cases is very efficient. | |||||||
| 41 | Germany | Epi | School/ECOC | Art | Fi | 09/10/20 | Transmission of SARS-CoV-2 in children aged 0 to 19 years in childcare facilities and schools after their reopening in May 2020, Baden-Württemberg, Germany. Euro Surveill. |
| Child-to-child transmission in schools/childcare facilities appeared very uncommon. We anticipate that, with face mask use and frequent ventilation of rooms, transmission rates in schools/childcare facilities would remain low in the next term, even if classes’ group sizes were increased. | |||||||
| 23 | Israel | Epi | Household | Art | Fi | 08/2020 | The Role of Children in the Dynamics of Intra Family Coronavirus 2019 Spread in Densely Populated Area. Pediatr Infect Dis J. |
| Our investigation demonstrated significantly lower rates of COVID-19 positivity in children compared with adults residing in the same household. | |||||||
| 36 | Israel | Epi | School | Art | Fi | 07/23/20 | A large COVID-19 outbreak in a high school 10 days after schools’ reopening, Israel, May 2020. Euro Surveill |
| The high school outbreak in Jerusalem displayed mass COVID-19 transmission upon school reopening. The circumstances promoting infection spread involved return of teenage students to their regular classes after a 2-month closure (on 18 May) and an extreme heatwave (on 19 May) with temperatures rising to 40 °C and above [6] that involved exemption from facemasks and continuous air-conditioning. | |||||||
| 48 | Italy | Epi | School/ECOC | Art | Fi | 12/2020 | Secondary transmission of COVID-19 in preschool and school settings in northern Italy after their reopening in September 2020: a population-based study. Euro Surveill |
| The overall secondary case attack rate was 3.2%, reaching 6.6% in middle and high schools. More timely isolation and testing of classmates could be effective in reducing virus transmission in this setting. | |||||||
| 52 | Norway | Epi | School | Art | Fi | 01/2021 | Minimal transmission of SARS-CoV-2 from paediatric COVID-19 cases in primary schools, Norway, August to November 2020 |
| This prospective study shows that transmission of SARS-CoV-2 from children under 14 years of age was minimal in primary schools in Oslo and Viken, the two Norwegian counties with the highest COVID-19 incidence and in which 35% of the Norwegian population resides. | |||||||
| 40 | Singapore | Epi | School/ECOC | Art | Fi | 06/25/20 | Novel coronavirus 2019 transmission risk in educational settings. Clin Infect Dis. |
| The data suggest that children are not the primary drivers of SARS-CoV-2 transmission in schools and could help inform exit strategies for lifting of lockdowns. | |||||||
| 55 | South Korea | Epi | Fitness Center | Art | Fi | 05/15/20 | Cluster of Coronavirus Disease Associated with Fitness Dance Classes, South Korea. Emerg Infect Dis. 2020 |
| During 24 days in Cheonan, South Korea, 112 persons were infected with severe acute respiratory syndrome coronavirus 2 associated with fitness dance classes at 12 sports facilities. Intense physical exercise in densely populated sports facilities could increase risk for infection. | |||||||
| 56 | South Korea | Epi | Fitness Center | Art | Fi | 08/10/20 | Epidemiological Characteristics of COVID-19 Outbreak at Fitness Centers in Cheonan, Korea. J Korean Med Sci |
| Zumba is an exercise fitness program which combines aerobic exercise with music, and Oriental and Latin dance moves.5 In the fitness centers where the Zumba classes were held, a large number of students had taken classes in a relatively crowded space, although ventilation systems were working properly. … [T]he droplets produced by exhalation or cough of a patient during the exercise have higher chance of reaching the nose, mouth or eye of other class participants directly, as well as remaining on the surface of the exercise equipment and later transmitted by contact. | |||||||
| 57 | US, FL | Epi | School Gym | Art | Fi | 10/16/20 | An Outbreak of COVID-19 Associated with a Recreational Hockey Game — Florida, June 2020. MMWR Morb Mortal Wkly Rep |
| The study was unable to determine exactly where exposure occurred, but hypothesizes it was at the evening hockey game, due to the heavy breathing that occurs, the lack of masks covering the mouth and nose, the transition from ice to bench where players continue heavy breathing or in the locker rooms and lack of other common exposures or time spent together. | |||||||
| 58 | US, FL | Epi | School Gym | Art | Fi | 01/26/21 | SARS-CoV-2 Transmission Associated with High School Wrestling Tournaments — Florida, December 2020–January 2021. MMWR Morb Mortal Wkly Rep |
| An outbreak arising from a Florida high school wrestling tournament in December 2020 had an attack rate of at least 30% (38 of 126 tournament attendees who were tested) and a secondary attack rate of at least 9% (41 of 441 close contacts of the 38 COVID-19 patients) | |||||||
| 39 | US, NC | Epi | School | Art | Pr | 1/2021 | Incidence and Secondary Transmission of SARS-CoV-2 Infections in Schools. Pediatrics. |
| In the first 9 weeks of in-person instruction in North Carolina schools, we found extremely limited within-school secondary transmission of SARS-CoV-2, determined by contact tracing | |||||||
| 59 | US, WA | Epi | Choir Room | Art | Fi | 05/15/20 | High SARS-CoV-2 Attack Rate Following Exposure at a Choir Practice — Skagit County, Washington, March 2020. MMWR Morb Mortal Wkly Rep. |
| Transmission was likely facilitated by close proximity (within 6 feet) during practice and augmented by the act of singing. | |||||||
You will observe there are 14 epidemiological cases in all. Recalling the example of Norway above, we throw out all the examples except those from the US. Four remain, which I have helpfully highlighted. Two are gyms, which are nothing like classrooms in their patterns of ventilation, both in Florida (!). One is a choir room, ditto. One remains.
Therefore, as far as school re-opening classroom epidemiology in the United States goes, Transmission depends on one case. Transmission is an enormous inverted pyramid whose apex is a single point. I have to say that balancing act doesn’t fill me with confidence.
Conclusion
Politico summarized the CDC’s reopening strategy in “Biden’s follow-the-science mantra on school meets political reality“:
Biden administration officials insist that the White House is grounding all of its policy decisions firmly in the best available evidence. They say the president receives a daily state of pandemic update from his Covid response team in his daily briefing book. And indeed, the Biden administration has taken care to give health experts like Anthony Fauci and CDC Director Rochelle Walensky leading roles in managing the response, and solicited constant input from its health agencies and outside public health groups.
Well, no. The budgetary concerns of “stakeholders” aren’t science, aren’t a mantra, and aren’t evidence, either. If Biden’s response team isn’t including aerosols and ventilation in his briefing books (the same issue occurs in other contexts) I want to know why. Ditto for soliciting constant input, because it doesn’t look like CDC reached out to aerosol experts at all. And then Politico continues:
Biden transition officials spent weeks crafting plans for safely reopening schools based on public health best practices, including proposing a massive new Covid testing regime and hundreds of billions of dollars in funding to help retrofit classrooms and overhaul ventilation systems.
No, they didn’t, because without taking aerosol tranmission into account, you don’t have best practices; you have tepid guidance like opening windows “to the extent possible.” But even more weirdly, if overhauling ventilation systems is going to be a line item in the budget, why in the name of all that is holy did CDC carefully suppress aerosols from its guidance? Or fail to do any serious epidemiological work on it?
The CDC already has two strikes against it: It catastrophically butchered the test kit rollout[3], and it butchered the software development for VAMA (the Vaccine Administration Management System). Now Walensky whiffs on school re-opening. Is that strike three? It’s hard to avoid the conclusion that the CDC is completely dysfunctional, and that Walensky, despite her warm personality, is unlikely to have the administrative and institutional chops to fix what’s wrong.
NOTES
[1] The CDC does mention ventilation in its “Health Facilities” section: “Improve ventilation to the extent possible such as by opening windows and doors to increase circulation of outdoor air to increase the delivery of clean air and dilute potential contaminants.” Sounds discouraging. Nor is aerosol tranmission mentioned. Why then open the windows?
[2] Here is an entertaining thread on the history of droplets v. aerosols from that same Professor Jiménez.
[3] Of the many shifting stories, here is the latest.
APPENDIX
Table 2: Complete Sources in CDC’s Transmission of SARS-CoV-2 in K-12 schools
Legend:
The Note column keys to the footnote numbers in SARS-CoV-2 in K-12 schools.
Abbreviations by column: Method: Model, Statistical, Epidemiological, Aggregation, Metastudy Narrative; Type: Article, Editorial Letter Revview Study Status: Preprint, Fininal, Other.
Citations are to linked title and publication only, for space purposes.
Beneath each source row, I’ve placed a quotation taken from that source. Scanning the quotes may give a sense of where “the science” is, as CDC conceives it.
| Note | Country | Method | Venue (Epi. Only) | Type | Status | Date | Citation |
| 1 | — | Agg | Art | Fi | 07/15/20 | Reopening K-12 Schools During the COVID-19 Pandemic: Prioritizing Health, Equity, and Communities. Consensus study report from The National Academies Press. | |
| In its final recommendation, the committee identifies four areas of research that are urgently needed to fill the existing gaps in evidence: (1) the role of children in transmission of SARS-CoV-2, (2) the role of reopening schools in the spread of SARS-CoV-2 in communities, (3) the role of airborne transmission of COVID-19, and (4) the relative effectiveness of different mitigation strategies in schools. | |||||||
| 2 | Nar | Edi | Fi | 07/29/20 | COVID-19 and School Closures. JAMA | ||
| Given the strong connection between education, income, and life expectancy,9 school closures could have long-term deleterious consequences for child health, likely reaching into adulthood. School closures also affect parents’ ability to work. | |||||||
| 3 | Australia | Sta | Art | Fi | 09/25/21 | COVID-19 in Victorian Schools: An analysis of child-care and school outbreak data and evidence-based recommendations for opening schools and keeping them open. Report from Murdoch Children’s Research Institute and the University of Melbourne. 2020; Published 2020 September 25. | |
| Infections linked to [Early Childhood Education and Care (ECECs)] and schools peaked at the time when community transmission was highest during July and then declined in August, suggesting that infections in ECECs and schools are driven primarily by transmission in the broader community. | |||||||
| 4 | US | Sta | Art | Fi | 04/10/20 | Coronavirus Disease 2019 in Children — United States, February 12–April 2, 2020. MMWR Morb Mortal Wkly Rep | |
| [R]elatively few children with COVID-19 are hospitalized, and fewer children than adults experience fever, cough, or shortness of breath | |||||||
| 5 | — | Mod | Let | Fi | 06/16/20 | Age-dependent effects in the transmission and control of COVID-19 epidemics. Nat Med | |
| We estimate that susceptibility to infection in individuals under 20 years of age is approximately half that of adults aged over 20 years, and that clinical symptoms manifest in 21% (95% credible interval: 12–31%) of infections in 10- to 19-year-olds | |||||||
| 6 | China | Sta | Art | Fi | 03/16/20 | Epidemiology of COVID-19 Among Children in China. Pediatrics | |
| Children of all ages appeared susceptible to COVID-19, and there was no significant sex difference. Although clinical manifestations of children’s COVID-19 cases were generally less severe than those of adult patients, young children, particularly infants, were vulnerable to infection. | |||||||
| 7 | US, UT/WA | Sta | Art | Fi | 01/01/21 | Symptoms and Transmission of SARS-CoV-2 Among Children — Utah and Wisconsin, March–May 2020. Pediatrics. | |
| Children and adults had similar secondary infection rates, but children generally had less frequent and severe symptoms. In two states early in the pandemic, we observed possible transmission from children in approximately one-fifth of households with potential to observe such transmission patterns. | |||||||
| 8 | US, UT/WA | Sta | Art | Fi | 01/01/21 | COVID-19 in Children: Looking Forward, Not Back. Pediatrics | |
| In this study, the researchers found that 20% and 17% of households had potential child-to-adult transmission and child-to-child transmission, respectively, but numbers are too small to draw definitive conclusions. | |||||||
| 9 | China | Sta | Let | Fi | 04/23/20 | SARS-CoV-2 Infection in Children.NEJM | |
| In contrast with infected adults, most infected children appear to have a milder clinical course. Asymptomatic infections were not uncommon.2 Determination of the transmission potential of these asymptomatic patients is important for guiding the development of measures to control the ongoing pandemic. | |||||||
| 10 | — | Agg | Rev | Fi | 06/17/20 | Children are unlikely to be the main drivers of the COVID‐19 pandemic – A systematic review. Acta Paediatr. | |
| Children are unlikely to be the main drivers of the pandemic. Opening up schools and kindergartens is unlikely to impact COVID-19 mortality rates in older people. | |||||||
| 11 | — | Agg | Rev | Fi | 12/2020 | COVID-19 in children: current evidence and key questions. Curr Opin Infect Dis | |
| Important questions remain unanswered regarding why children have mild disease compared with adults; how children of different ages contribute to asymptomatic community transmission of the virus; and the pathophysiology of and most appropriate investigation and treatment strategies for the novel hyperinflammatory syndrome. | |||||||
| 12 | — | Agg | Rev | 09/01/20 | Severe Acute Respiratory Syndrome Coronavirus 2 (SARS-CoV-2) Infection in Children and Adolescents: A Systematic Review. JAMA Pediatr | ||
| The rapid spread of COVID-19 across the globe and the lack of European and US data on pediatric patients require further epidemiologic and clinical studies to identify possible preventive and therapeutic strategies. | |||||||
| 13 | — | Agg | Rev | Fi | 04/06/20 | Epidemiology and clinical features of coronavirus disease 2019 in children. Clin Exp Pediatr | |
| This review summarizes what is currently known about COVID-19 in children and adolescents. | |||||||
| 14 | — | Agg | Rev | Ot | 01/12/20 | Why is COVID-19 less severe in children? A review of the proposed mechanisms underlying the age-related difference in severity of SARS-CoV-2 infections. Arch Dis Child. | |
| In this review, we discuss proposed hypotheses for the age-related difference in severity of coronavirus disease | |||||||
| 15 | Europe | Sta | Art | Fi | 06/25/20 | COVID-19 in children and adolescents in Europe: a multinational, multicentre cohort study. Lancet Child Adolesc Health | |
| COVID-19 is generally a mild disease in children, including infants. However, a small proportion develop severe disease requiring ICU admission and prolonged ventilation, although fatal outcome is overall rare. | |||||||
| 16 | US | Sta | Art | Fi | 10/02/20 | COVID-19 Trends Among School-Aged Children — United States, March 1–September 19, 2020. MMWR Morb Mortal Wkly Rep | |
| Underlying conditions were more common among school-aged children with severe outcomes related to COVID-19: among school-aged children who were hospitalized, admitted to an intensive care unit (ICU), or who died, 23%, 38%, and 33%, respectively, had at least one underlying condition. | |||||||
| 17 | US | Sta | Art | Fi | 01/22/21 | COVID-19 Trends Among Persons Aged 0–24 Years — United States, March 1–December 12, 2020. MMWR Morb Mortal Wkly Rep | |
| COVID-19 cases in children, adolescents, and young adults have increased since summer 2020, with weekly incidence higher in each successively increasing age group. | |||||||
| 18 | Iceland | Sta | Art | Fi | 06/11/20 | Spread of SARS-CoV-2 in the Icelandic Population. N Engl J Med | |
| In a population-based study in Iceland, children under 10 years of age and females had a lower incidence of SARS-CoV-2 infection than adolescents or adults and males. The proportion of infected persons identified through population screening did not change substantially during the screening period, which was consistent with a beneficial effect of containment efforts. | |||||||
| 19 | — | Met | Art | Fi | 12/01/20 | Household Transmission of SARS-CoV-2: A Systematic Review and Meta-analysis. JAMA Netw Open | |
| [G]iven that individuals with suspected or confirmed infections are being referred to isolate at home, households will continue to be a significant venue for transmission of SARS-CoV-2. | |||||||
| 20 | China | Sta | Art | Fi | 06/26/20 | Changes in contact patterns shape the dynamics of the COVID-19 outbreak in China. Science | |
| [C]hildren 0 to 14 years of age are less susceptible to severe acute respiratory syndrome coronavirus (SARS-CoV-2) infection than adults 15 to 64 years of age. | |||||||
| 21 | — | Met | Art | Fi | 02/01/20 | Susceptibility to SARS-CoV-2 Infection Among Children and Adolescents Compared With Adults: A Systematic Review and Meta-analysis. JAMA Pediatr. | |
| In this meta-analysis, there is preliminary evidence that children and adolescents have lower susceptibility to SARS-CoV-2, with an odds ratio of 0.56 for being an infected contact compared with adults. There is weak evidence that children and adolescents play a lesser role than adults in transmission of SARS-CoV-2 at a population level. | |||||||
| 22 | — | Agg | Rev | 10/29/20 | On the Effect of Age on the Transmission of SARS-CoV-2 in Households, Schools, and the Community. J Infect Dis | ||
| There is some evidence that given limited control measures, SARS-CoV-2 may spread robustly in secondary/high schools, and to a lesser degree in primary schools, with class size possibly affecting that spread. There is also evidence of more limited spread in schools when some mitigation measures are implemented. | |||||||
| 23 | Israel | Epi | Household | Art | Fi | 08/2020 | The Role of Children in the Dynamics of Intra Family Coronavirus 2019 Spread in Densely Populated Area. Pediatr Infect Dis J. |
| Our investigation demonstrated significantly lower rates of COVID-19 positivity in children compared with adults residing in the same household. | |||||||
| 24 | Italy | Sta | Art | Fi | 06/30/20 | Suppression of a SARS-CoV-2 outbreak in the Italian municipality of Vo’. Nature | |
| The experience of Vo’ shows that, despite the silent and widespread transmission of SARS-CoV-2, transmission can be controlled and represents a model for the systematic suppression of viral outbreaks under similar epidemiological and demographic conditions. | |||||||
| 25 | — | Met | Art | Fi | 12/06/20 | A meta-analysis on the role of children in SARS-CoV-2 in household transmission clusters. Clin Infect Dis. | |
| Children are Infrequently Identified as the Index Case of Household SARS-CoV-2 Clusters | |||||||
| 26 | US, NY | Sta | Let | Fi | 05/20/20 | Nasal Gene Expression of Angiotensin-Converting Enzyme 2 in Children and Adults. JAMA. | |
| [C]ompared with younger children, ACE2 gene expression was significantly higher in older children. | |||||||
| 27 | — | Nar | Let | Fi | 05/06/20 | The immune system of children: the key to understanding SARS-CoV-2 susceptibility?. Lancet Child Adolesc Health. | |
| Children are more vulnerable to other infections; thus, the important question arises—why are children less susceptible to COVID-19 disease compared with adults? So far, there is no evidence of a lower degree of expression or function of the SARS-CoV-2 receptor (namely ACE2) in children. Thus, studying the innate immune system of children might be the key | |||||||
| 28 | US, NY | Sta | Let | Fi | 11/05/20 | Distinct antibody responses to SARS-CoV-2 in children and adults across the COVID-19 clinical spectrum. Nat Immunol | |
| The clinical manifestations of SARS-CoV-2 infection in children are distinct from adults. Children with COVID-19 rarely exhibit severe respiratory symptoms and often remain asymptomatic | |||||||
| 29 | Israel | Sta | Art | Fi | 02/11/21 | The role of children in the spread of COVID-19: Using household data from Bnei Brak, Israel, to estimate the relative susceptibility and infectivity of children. Preprint. MedRxiv | |
| [T]he fraction of children among the confirmed cases has been found to be low in many countries can be accounted for by two (nonexclusive) hypotheses: (1) Children display milder symptoms than adults when infected, so are less likely to be tested in a typical testing policy triggered by symptoms, (2) Children are less susceptible to infection than adults. Our analysis of the data obtained in this study lends support to <em>both</em> hypotheses, and indicates that both have a role in explaining the observed epidemiological patterns. | |||||||
| 30 | South Korea | Sta | Art | Fi | 10/2020 | Contact Tracing during Coronavirus Disease Outbreak, South Korea, 2020. Emerg Infect Dis | |
| Of 10,592 household contacts, 11.8% had COVID-19. Of 48,481 nonhousehold contacts, 1.9% had COVID-19. | |||||||
| 31 | China | Sta | Art | Pr | 07/24/20 | Infectivity, susceptibility, and risk factors associated with SARS-CoV-2 transmission under intensive contact tracing in Hunan, China. Preprint. MedRxiv | |
| Our findings support the hypothesis that children can effectively transmit SARS-CoV-2 and highlight how pre-symptomatic and asymptomatic transmission can hinder control efforts. | |||||||
| 32 | UK | Sta | Art | Fi | 08/24/20 | SARS-CoV-2 infection and transmission in educational settings: a prospective, cross-sectional analysis of infection clusters and outbreaks in England. Lancet Infect Dis | |
| Overall, SARS-CoV-2 infections and outbreaks were uncommon across all educational settings. Staff members had an increased risk of SARS-CoV-2 infections compared to students in any educational setting, and the majority of cases linked to outbreaks were in staff. | |||||||
| 33 | Europe | Sta | Art | Pr | 11/13/20 | Age differential analysis of COVID-19 second wave in Europe reveals highest incidence among young adults. Preprint. MedRxiv | |
| [W]e analyze data of incidence by age groups in 25 European countries, revealing that the highest incidence of the current second wave is observed for the group comprising young adults (aged 18-29 years old) in all but 3 of the countries analyzed. | |||||||
| 34 | Italy | Mod | Art | Pr | 12/18/20 | No evidence of association between schools and SARS-CoV-2 second wave in Italy. Preprint. MedRxiv | |
| [S]chool closures in two regions where they were implemented before other measures did not affect the rate of Rt decline. In schools, despite the high frequency of tests per week, secondary infections were <1%, and clusters in a representative November week infrequent. Thus, our prospective analysis does not support a role for school reopening as a driver of the second wave of SARS-CoV-2 epidemics in Ital | |||||||
| 35 | US | Sta | Art | Fi | 01/04/21 | The Effects of School Reopenings on COVID-19 Hospitalizations. Technical Report from the National Center for Research on Education Access and Choice (REACH). | |
| The study is the first to examine how reopening schools in-person has affected COVID-19 hospitalizations. We found no evidence that reopening schools in-person or in a hybrid form increased COVID hospitalizations in the 75 percent of counties that had low COVID hospitalization rates during the summer, prior to reopening schools. Our results suggest that it seems safe to reopen schools when there are no more than 36 to 44 total new COVID hospitalizations per 100,000 people per week. | |||||||
| 36 | Israel | Epi | School | Art | Fi | 07/23/20 | A large COVID-19 outbreak in a high school 10 days after schools’ reopening, Israel, May 2020. Euro Surveill |
| The high school outbreak in Jerusalem displayed mass COVID-19 transmission upon school reopening. The circumstances promoting infection spread involved return of teenage students to their regular classes after a 2-month closure (on 18 May) and an extreme heatwave (on 19 May) with temperatures rising to 40 °C and above [6] that involved exemption from facemasks and continuous air-conditioning. | |||||||
| 37 | Germany | Sta | Art | Fi | 09/2020 | Surveillance of COVID-19 school outbreaks, Germany, March to August 2020. Euro SurveillSurveillance of COVID-19 school outbreaks, Germany, March to August 2020 | |
| Only few and mostly small COVID-19 school outbreaks had been reported in Germany overall, suggesting that the containment measures are sufficient to reduce spillover into the community. | |||||||
| 38 | US, MI/WA | Mod | Art | Fi | 2/2021 | To What Extent Does In-Person Schooling Contribute to the Spread of COVID-19? Evidence from Michigan and Washington. Report from the Center for Education Data & Research (CEDR), National Center for Analysis of Longitudinal Data in Education Research (CALDER), and Education Policy Innovation Collaborative (EPIC). | |
| Using a variety of regression modeling strategies , we find that simple correlations show in-person modalities are correlated with increased COVID cases, but accounting for both pre-existing cases and a richer set of covariates brings estimates close to zero on average. | |||||||
| 39 | US, NC | Epi | School | Art | Pr | 1/2021 | Incidence and Secondary Transmission of SARS-CoV-2 Infections in Schools. Pediatrics. |
| In the first 9 weeks of in-person instruction in North Carolina schools, we found extremely limited within-school secondary transmission of SARS-CoV-2, determined by contact tracing | |||||||
| 40 | Singapore | Epi | School/ECOC | Art | Fi | 06/25/20 | Novel coronavirus 2019 transmission risk in educational settings. Clin Infect Dis. |
| The data suggest that children are not the primary drivers of SARS-CoV-2 transmission in schools and could help inform exit strategies for lifting of lockdowns. | |||||||
| 41 | Germany | Epi | School/ECOC | Art | Fi | 09/10/20 | Transmission of SARS-CoV-2 in children aged 0 to 19 years in childcare facilities and schools after their reopening in May 2020, Baden-Württemberg, Germany. Euro Surveill. |
| Child-to-child transmission in schools/childcare facilities appeared very uncommon. We anticipate that, with face mask use and frequent ventilation of rooms, transmission rates in schools/childcare facilities would remain low in the next term, even if classes’ group sizes were increased. | |||||||
| 42 | US, WI | Sta | Art | Fi | 01/29/21 | COVID-19 Cases and Transmission in 17 K–12 Schools — Wood County, Wisconsin, August 31–November 29, 2020. MMWR Morb Mortal Wkly Rep. | |
| Among 17 rural Wisconsin schools, reported student mask-wearing was high, and the COVID-19 incidence among students and staff members was lower than in the county overall (3,453 versus 5,466 per 100,000). Among 191 cases identified in students and staff members, only seven (3.7%) cases, all among students, were linked to in-school spread. | |||||||
| 43 | US, MS | Sta | Art | Fi | 12/18/21 | Factors Associated with Positive SARS-CoV-2 Test Results in Outpatient Health Facilities and Emergency Departments Among Children and Adolescents Aged <18 Years — Mississippi, September–November 2020. MMWR Morb Mortal Wkly Rep. | |
| Among children and adolescents aged <18 years in Mississippi, close contact with persons with COVID-19 and gatherings with persons outside the household and lack of consistent mask use in school were associated with SARS-CoV-2 infection, whereas attending school or child care was not associated with receiving positive SARS-CoV-2 test results. | |||||||
| 44 | Australia | Sta | Art | Fi | 10/21/20 | COVID-19 in schools and early childhood education and care services – the Term 3 experience in NSW. Report from National Centre for Immunisation Research and Surveillance (NCIRS). 2020; Published 2020 October. | |
| Three larger outbreaks occurred, all in high school settings. Factors that may have contributed to these outbreaks include attending school while symptomatic, a non–school-related overnight retreat and participation in a music group. All outbreaks were rapidly contained with NSW public health response strategy. The likelihood of cases in educational settings is related to the level of community transmission of SARS-CoV-2. This is consistent with findings from Victoria, Australia4 and from international studies. | |||||||
| 45 | Finland | Epi | School | Art | Ot | 07/30/20 | Transmission of SARS-CoV-2 following exposure in school settings: experience from two Helsinki area exposure incidents. Preprint. MedRxiv |
| When the index was a child, no school transmission was identified, while the occurrence of an adult case led to a 16% AR. Further cases were evidenced in 3 families, but other transmission chains were plausible. It is likely that transmission from children to adults is limited.\ | |||||||
| 46 | Ireland | Sta | Art | Fi | 05/28/20 | No evidence of secondary transmission of COVID-19 from children attending school in Ireland, 2020. Euro Surveill | |
| [E]xamination of all Irish paediatric cases of COVID-19 attending school during the pre-symptomatic and symptomatic periods of infection (n = 3) identified no cases of onward transmission to other children or adults within the school and a variety of other settings. These included music lessons (woodwind instruments) and choir practice, both of which are high-risk activities for transmission. Furthermore, no onward transmission from the three identified adult cases to children was identified. | |||||||
| 47 | Australia | Sta | Art | Fi | 08/03/20 | Transmission of SARS-CoV-2 in Australian educational settings: a prospective cohort study. Lancet Child Adolesc Health. | |
| SARS-CoV-2 transmission rates were low in NSW educational settings during the first COVID-19 epidemic wave, consistent with mild infrequent disease in the 1·8 million child population. With effective case-contact testing and epidemic management strategies and associated small numbers of attendances while infected, children and teachers did not contribute significantly to COVID-19 transmission via attendance in educational settings. | |||||||
| 48 | Italy | Epi | School/ECOC | Art | Fi | 12/2020 | Secondary transmission of COVID-19 in preschool and school settings in northern Italy after their reopening in September 2020: a population-based study. Euro Surveill |
| The overall secondary case attack rate was 3.2%, reaching 6.6% in middle and high schools. More timely isolation and testing of classmates could be effective in reducing virus transmission in this setting. | |||||||
| 49 | Spain | Nar | Let | Fi | 10/05/20 | COVID-19: Social Irresponsibility of Teenagers Towards the Second Wave in Spain. J Epidemiol | |
| This situation is beginning to occur also in other countries, such as Japan. A recent study shows that the majority of young adults who start outbreaks are asymptomatic, when they are not yet aware that they can infect other people, and they do so mainly in situations where they breathe hard and there is little social distance, such as singing in karaoke bars, screaming in pubs, or working out in gyms | |||||||
| 50 | — | Nar | Edi | Fi | 01/26/21 | Data and Policy to Guide Opening Schools Safely to Limit the Spread of SARS-CoV-2 Infection. JAMA. | |
| [T]he preponderance of available evidence from the fall school semester has been reassuring insofar as the type of rapid spread that was frequently observed in congregate living facilities or high-density worksites has not been reported in education settings in schools. | |||||||
| 51 | — | Nar | Art | Fi | 12/11/20 | Summary of Guidance for Public Health Strategies to Address High Levels of Community Transmission of SARS-CoV-2 and Related Deaths, December 2020. MMWR Morb Mortal Wkly Rep. | |
| No single strategy can control the pandemic; rather, a multipronged approach using all available evidence-based strategies at the individual and community levels can break transmission chains and address high levels of community transmission; reduce related illnesses, long-term sequelae, and deaths; and mitigate the pandemic’s economic impact. | |||||||
| 52 | Norway | Epi | School | Art | Fi | 01/2021 | Minimal transmission of SARS-CoV-2 from paediatric COVID-19 cases in primary schools, Norway, August to November 2020 |
| This prospective study shows that transmission of SARS-CoV-2 from children under 14 years of age was minimal in primary schools in Oslo and Viken, the two Norwegian counties with the highest COVID-19 incidence and in which 35% of the Norwegian population resides. | |||||||
| 53 | Switzerland | Sta | Art | Pr | 12/26/20 | Surveillance of acute SARS-CoV-2 infections in school children and point-prevalence during a time of high community transmission in Switzerland. Preprint. MedRxiv | |
| In a setting of high incidence of SARS-CoV-2 infections, unrecognized virus spread within schools was very low. Schools appear to be safe with the protective measures in place (e.g., clearly symptomatic children have to stay at home, prompt contact tracing with individual and class-level quarantine, and structured infection prevention measures in school). | |||||||
| 54 | US, IL | Sta | Art | Fi | 12/30/21 | Data-Driven Reopening of Urban Public Education Through Chicago’s Tracking of COVID-19 School Transmission. J Public Health Manag Pract | |
| By combining local data from a large urban private school system with national and international data on maintaining in-person learning during COVID-19 surges, Chicago believes in-person public education poses a low risk of transmission when the operational burden imposed by the second wave has subsided. | |||||||
| 55 | South Korea | Epi | Fitness Center | Art | Fi | 05/15/20 | Cluster of Coronavirus Disease Associated with Fitness Dance Classes, South Korea. Emerg Infect Dis. 2020 |
| During 24 days in Cheonan, South Korea, 112 persons were infected with severe acute respiratory syndrome coronavirus 2 associated with fitness dance classes at 12 sports facilities. Intense physical exercise in densely populated sports facilities could increase risk for infection. | |||||||
| 56 | South Korea | Epi | Fitness Center | Art | Fi | 08/10/20 | Epidemiological Characteristics of COVID-19 Outbreak at Fitness Centers in Cheonan, Korea. J Korean Med Sci |
| Zumba is an exercise fitness program which combines aerobic exercise with music, and Oriental and Latin dance moves.5 In the fitness centers where the Zumba classes were held, a large number of students had taken classes in a relatively crowded space, although ventilation systems were working properly. … [T]he droplets produced by exhalation or cough of a patient during the exercise have higher chance of reaching the nose, mouth or eye of other class participants directly, as well as remaining on the surface of the exercise equipment and later transmitted by contact. | |||||||
| 57 | US, FL | Epi | School Gym | Art | Fi | 10/16/20 | An Outbreak of COVID-19 Associated with a Recreational Hockey Game — Florida, June 2020. MMWR Morb Mortal Wkly Rep |
| The study was unable to determine exactly where exposure occurred, but hypothesizes it was at the evening hockey game, due to the heavy breathing that occurs, the lack of masks covering the mouth and nose, the transition from ice to bench where players continue heavy breathing or in the locker rooms and lack of other common exposures or time spent together. | |||||||
| 58 | US, FL | Epi | School Gym | Art | Fi | 01/26/21 | SARS-CoV-2 Transmission Associated with High School Wrestling Tournaments — Florida, December 2020–January 2021. MMWR Morb Mortal Wkly Rep |
| An outbreak arising from a Florida high school wrestling tournament in December 2020 had an attack rate of at least 30% (38 of 126 tournament attendees who were tested) and a secondary attack rate of at least 9% (41 of 441 close contacts of the 38 COVID-19 patients) | |||||||
| 59 | US, WA | Epi | Choir Room | Art | Fi | 05/15/20 | High SARS-CoV-2 Attack Rate Following Exposure at a Choir Practice — Skagit County, Washington, March 2020. MMWR Morb Mortal Wkly Rep. |
| Transmission was likely facilitated by close proximity (within 6 feet) during practice and augmented by the act of singing. | |||||||
| 60 | France | Epi | Choir Room | Art | Fi | 12/23/20 | High Rate of SARS-CoV-2 Transmission Due to Choir Practice in France at the Beginning of the COVID-19 Pandemic. J Voice. |
| The characteristics of the viral transmission via close human contacts was probably enhanced by the act of singing, at a phase of intense circulation of SARS-CoV-2 in the population at this period. We report in our study the role of asymptomatic infection carriers initiating a silent chain of transmission of the coronavirus, leading to a cluster under the circumstances of the rehearsal. This study confirms that the transmission of the virus from asymptomatic cases is very efficient. | |||||||
| 61 | — | Agg | Art | Fi | 08/27/20 | Droplets and Aerosols Generated by Singing and the Risk of Coronavirus Disease 2019 for Choirs. Clin Infect Dis. 2020;ciaa1241. Published online ahead of print 2020 Sep 18. doi:10.1093/cid/ciaa | |
| While social distancing is effective in normal social interactions, singing can produce a substantially larger number of respiratory droplets and aerosols than speaking, as it is louder and sustained for longer durations | |||||||


I’ve posted this before, but two HVAC engineers I talked to mentioned they don’t think a given school’s existing ventilation system can be retrofitted to air exchange every three minutes without running afoul of energy usage/efficiency regulations. This would put policy makers in a space that can’t be easily negotiated without expenditure.
My personal hobby horse is changing the school year to have outdoor instruction in the summer and remote learning over the winter. Mix and match hours of operation to your local climes.
A neighbor is teaching an eight-week adult education class in a nearby park.
It’s for people who are interested in becoming certified in permaculture, and the class looks to be fully enrolled and socially distanced. People are sitting far apart from each other and the instructor is, well, in front of the class but not right next to any of his students.
I know that such a class wouldn’t be possible in Chicago right now, or, what the heck, in Texas, but it is happening right here in Tucson on Saturdays and Sundays.
It’ll be possible in Texas by Tuesday.
> This would put policy makers in a space that can’t be easily negotiated without expenditure.
As I point out in the conclusion:
I think many books will be written in the future on the topic of why the western medical establishment is so resistant to the aerosol theory (unlike in Asia, where they seem to have simply assumed it would be a factor). When I raise this question with my medical relatives, I don’t get any straight answer that I can understand at all. I don’t think the answer can be found in corruption or money, as I can’t see where the motive might be – I think it’s ultimately an epistemological failure, based to a large degree in the history of medical and public health science. But it is absolutely infuriating to see that a year into this, the same mistakes are being made.
> I think it’s ultimately an epistemological failure, based to a large degree in the history of medical and public health science.
This thread (from note 2) has some theories. There really is a paradigm shift needed, In addition, hospitals don’t like new capital expenditures on HVAC any more than schools do.
> it is absolutely infuriating to see that a year into this, the same mistakes are being made.
Worse, having been unmade, they are now remade.
I remember back in January 2020 watching a video from Wuhan, where government workers were chastising a maskless elderly women on a bus, while they were causally touching the bars and handles on the bus with bare hands. ‘Such idiots’, I thought, ‘don’t they know about fomites?’ I think that certainly a paradigm shift is needed, but it seems that it had already taken place in Asia, where there seems to have been a strong assumption from the very beginning that aerosols were at least as likely to be a mode of transmission than droplets/fomites.
First, Aerosol IS covered by CDC: “Respiratory etiquette” addresses “covering your cough”.
I tried to get noted epidemiologist Julian W. Tang interested in my inventions (all since rejected by USPTO – that is just what they do now) which addressed all the leakage which takes place when sneezing/coughing with and without masks (no, does not involve sealing mask perimeter- they allowed dozens of those patents, all essentially the same). 99% effective per independent lab tests.
His contention was that talking/singing etc. net/net spread more aerosols than coughing and sneezing does. He MIGHT be correct, but that runs counter to 50 years of research.
Earlier versions DID receive patents, but hospital buying group had NO interest (pre-covid) unless they felt pressure from infection control people. And those people do not get promotions for spending more money. Research how profitable treating hospital Acquired infections is.
The USPTO has won the battle, and the war; Day trading crapified Stocks has been much more rewarding than beating my head against patent examiners.
What are you talking about?
Meant to echo/support your conclusion as a setup for what i intended to be my real payload, the outdoor instruction + remote learning. This would allow policy makers to cheap out on retrofitting but still take measures that could possibly mitigate aerosols. Maybe buy time as a stop gap until all factors can be assessed.
I understand your thesis to be that there is gatekeeping at CDC about virus transmission modes in schools and you’ve presented literature and a strong case addressing aerosol. The public may not want to deal with it at this point due to fatigue and uncertainty about how COVID is actually affecting the young. I am still terrified that the effects might be cumulative or risk increased with each reinfection of same variant or new variant. I think this uncertainty absolutely warrants maximum precaution but here we have precaution fatigue and a strong desire among a significant portion of the populace to return to normal.
I feel outdoor instruction can thread the needle, reducing risk of aerosol transmission while allowing a step towards normality.
To veer toward current political trends, I think our congresses time might be better served by not having a 9/11 style 1/6 commission, but rather a 9/11 style COVID commission. To the average person on the street, is 1/6 a greater risk to their live and livelihood, or is COVID? The charts we see in water cooler everyday are indicating a big drop in cases, but the risk of resurgence of original or variant still exists imho.(by the way, I recall a link I saw right around inauguration that discussed guidance to labs to reduce testing cycles because it was thought that the current amount of cycles at the time were oversensitive, it seems like a fundamental change in testing protocol would have a significant effect on the charts, maybe distributed over time as more labs adopt the new protocol(note this is speculative)).
In short, I support your thesis and conclusion.
From which I conclude that achieving ‘herd immunity’ through means separate from but perhaps in addition to vaccination, was the unstated policy of the Trump administration and remains the unstated policy of the Biden administration. [Are Americans under 16 even eligible for vaccination?] The transition from one administration the next seems to have entailed, in this area, just replacing the use of political rhetoric to obscure a persistent policy with scientific rhetoric.
Thanks for this, Lambert.
What a shame US can’t afford to provide good ventilation and good air quality in the facilities that its young spend a large portion of their lives in.
Oh, wait.
I guess the MMT people haven’t made much progress yet at Dept. HHS or its subordinate institutes.
And I suppose that, from the perspective of our rulers, the political undesirability of letting the governed know that the government can afford to make things better is a weightier matter than whatever objective goods might be achieved by actually making things better.
> And I suppose that, from the perspective of our rulers, the political undesirability of letting the governed know that the government can afford to make things better is a weightier matter than whatever objective goods might be achieved by actually making things better.
Everything’s going according to plan.
Hammacher Schlemmer portable filter, “hospital grade” for a 1,500 foot (no typo) room is $1000.
https://www.hammacher.com/product/hospital-grade-air-purifier
That’s capital R retail.
I am sure a school system could find a cheaper equivalent version and get an even better deal by buying in bulk.
It is baffling. HEPA and masks would likely do the trick.
A free-standing, unbaffled filter is remarkably ineffective. With its input so near its output, air is mostly recycled in a loop from the high-pressure zone at the output back into the low-pressure zone at the input. To effectively ventilate a room or filter room air, a fan must be placed within a close-fitting circular opening along a wall or window or else be fed from without through a close-fitting conduit. This is standard HVAC procedure. The worst possible installation is conveniently shown in the company advertisement, of a stand-alone filtration unit placed in the corner of a room.
Hospital ERs are full of these devices….I’ve seen them. Along with dentist’s offices.
You are basically discussing air exchange, not a filtering device as air cleaner. Why not just thrown open windows? I don’t see your approach as any improvement over that.
Why can’t they be fairly effective if the filter is changed very frequently?
I have four large (2 foot diameter) hospital grade HEPA air filters made by Honeywell in my home. They are designed to pull in air from all sides and blow it out the bottom horizontally in all directions as a fairly strong blast across the floor to disperse the clean air across a room. They work very well. In allergy season when I turn one on at high speed the effect on my nose is noticeable in a few minutes. Once a room has been cleared of allergens they can be left on at low speed to take care of new allergens seeping into the room. That is a different problem than aerosols being emitting from someone next to you, so perhaps the highest setting would need to be used in schools which would raise noise levels some. They certainly would remove viral aerosols to a large extent, exchanging all the air in a large room maybe once or twice an hour; that’s one of the reasons why they are used in hospitals:
https://www.nytimes.com/wirecutter/blog/can-hepa-air-purifiers-capture-coronavirus/
https://www.epa.gov/coronavirus/will-air-cleaner-or-air-purifier-help-protect-me-and-my-family-covid-19-my-home
The EPA page above says a HEPA filter alone is not enough, but can be part of a good safety strategy.
Scientist_4_of_6 is correct that if you are sitting next to an infected person and the HEPA filter is far away the filter is not going to help you as much, but it will still help to some extent in keeping the concentration in the room lower. Whether that plus masks and other measures reduces risk to acceptable levels is hard to know without a large well designed study. Even if the risk is acceptable to the government, affecting a small percentage of the population, is that risk acceptable to families? Some children will still get infected and bring it home. The fact that your family was unlucky is not much comfort. There are HEPA filters that also have UVC lamps inside them, sterilizing the air as it passes through (cheaper models may produce ozone from the UVC lamp if they are poorly designed). Honeywell sells their big HEPA filters started at about $200 and up. Filters are recommended to be replaced every 6-12 months usually, though it depends on the local environment; for my home I find they last for years. They really cut down on dust accumulation also!
So, policy advice from the CDC is still being directed and written by political commissars rather than scientists or scientismists or even scientitians.
Good to know.
> So, policy advice from the CDC is still being directed and written by political commissars rather than scientists or scientismists or even scientitians.
I tbink that institutional inertia has a lot to do with it. Science proceeds one funeral at a time. Or one housekeeping, but so far Walensky seems unwilling to do that.
I’m starting to feel like I’m in Bizzaro World’s Bizzaro World.
This is the sort of post that I love here at NC, and why I’m so happy to support the site. Thank you.
Ditto. Awesome post. That letter to the triumvirate of Zients, Walenski, and Fauci is a masterpiece. And Jimenez is my hero.
Sadly, as Samuel Connor intimates above, much as it may seem like the health, educational, and economic benefits to the citizenry of containing the pandemic are legion, there are still far too many poors among us for that.
Never let a crisis go to waste…
> This is the sort of post that I love here at NC,
[lambert blushes modestly]
Absolutely. In my case, the post captures and elaborates my thinking on this issue for, oh I dunno, the last eight or ten months. During that time, outside of aerosol scientists, I’ve seen very little “conversation” about aerosols and how they relate to recommendations for restaurants and schools. Here’s the one local article I found regarding air filtration in restaurants: https://sanantonioreport.org/air-filtration-technology-clears-the-air-for-some-san-antonio-businesses/
The cynical side of me observes that no one wants to seriously engage with this issue, because mitigation looks expensive. In that way, it’s similar to the lack of attention to treatments, e.g., Ivermectin and various other cheap medications. I end up having to do my own research and make my own “guidelines” in absence of competent institutions.
> mitigation looks expensive.
Mitigation for the ordinary person in the street is expensive only in thought.
We are open 4 days a week. If the parents want to, they could have their children in school the entire four days.. we have a hybrid model (2 days a week) as well as a four day a week model.
We have 60% of the students who don’t come in all week. By choice. We take all the recommended precautions. I have a 6 ft long stick that I use to measure distances between students. They still don’t want to eat the cat food.
At this point, trust in government is so low that if the CDC is doing a sloppy job no one is going to listen
Our schools are starting to open too. The last survey that went out had about 2/3 of parents choosing 100% virtual (as is our family), even though there is now an option for in-person school.
I find it interesting that so much of the media focus is on reopening schools, yet when parents are given a choice, most of them prefer to be cautious. I suspect the push for in-person schools is coming primarily from business pressure, not families, and, as usual, the media amplifies their perspective.
The response of the US government to the coronavirus pandemic has been abysmal from the start. CDC prohibiting Washington State from testing for the Wuhan virus. It distributed a faulty test. No PPE was available for the evacuation of Princess Cruise passengers.
A year later there has been no improvement. Basically, to reopen schools, aerosol transmission is overlooked.
The life expectancy of Americans has decreased by a full year due to the pandemic. The biggest decline since WWII. Americans are literally at war with virus, but its government is not. The cause is the same as the blackouts in California and Texas, the ruling Elite is simply unwilling to spend the money on planning and upgrading infrastructure to save American lives.
Australia, New Zealand, NBA, and NFL are examples of where public health measures to prohibit the transmission of the virus work. Schools could reopen with daily testing, safety upgrades, bubbles, local public health supervision, reporting and paid safe quarantines, no questions asked. But Dr. Anthony Fauci stays on as the White House Medical Advisor. No change. He is paid the big bucks to increase corporate profits. Not to give information, supplies, money and planning to save American lives; one community at a time and until finally the whole nation eradicates the virus.
Instead, it is not surprising that today Pfizer said they are developing a third shot for the South African variant. Another money maker.
Mike the Mad Biologist, who in addition to being a biologist is a public school teacher, has a better opinion about the CDC Guidelines. However, he has doubts as to anyone will follow them
https://mikethemadbiologist.com/2021/02/17/some-thoughts-on-the-cdcs-new-school-guidance/
> a better opinion
I enjoy Mike’s old school blog, but I think he’s mistaking civility for content. It is possible, I suppose, to offer good guidance even if one’s science is bad, but in this case, the CDC offers poor guidance and bad science when good science and good guidance is available to them. CDC erased erase aerosol transmission, and with it opening windows, filters, HVAC tinkering, etc. They do this while posing as an authoritative source and polluting the media with what in any other context we would label disinformation — cf. Fauci’s Noble Lie — and thereby deny parents knowledge they may need to protect their children. All so as to avoid offending budget stakeholders. It’s unconscionable.
I apologize for my lack of tact in the comment you replaced with your own. And also for causing you the work of deleting it.
There is the another side of the coin.
Here, during the last 12 months, kids were supposed to be in school for 10 of them. In reality, at best, they spent 3 months at school, and 7 distance learning. Some less, because last spring the distance learning wasn’t mandatory, as there was quite a few people who just didn’t have the equipment (now schools are supposed to help with that, don’t know how it works in reality).
That has very substantial impact on the kids and the society, in many ways. For one, it’s very likely to have a significant impact on widening the inequality, both because high-socioeconomic families are more likely to supply extra home-schooling than low ones, absence of school meals (in the UK, this was an issue that a footballer had to force the meal-snatching Tories to do), lack of social contact etc. etc.
I know of many parents who would happily brave Covid to get kids into schools, as they believe that even catching it (in the family) would likely have less impact on their kids long term than missing school for this long. Businesses can get their support moneys and loans. But there’s no, absolutely no way, of returning to the kids their childhood and schooling at the right time.
So, the questions here are:
– can we open the schools reasonably safely? (and what does “reasonably safely” mean?)
– if no, who are going to sacrifice – the kids, or the vulnerable?
The second question is very much a moral call question, where there is no one good answer IMO.
Yes, its a horrible situation. Its very stressful for the kids and parents.
Here in Ireland, the schools have been shut since the New Year. The impact on kids will be highly variable, there are obvious impacts based on socio economic features, but there are many other factors involved. One friend thinks her two girls may have benefited hugely from the free time and space to explore. An American friend here who has been homeschooling since this started (they were moving and changing school so it seemed logical to just sit things out for the transition) tells me that while her kid is doing ok academically, she is desperately lonely from lack of contact with other children.
I was listening to a radio show this week interviewing older kids, those in their last year. Again, the impact seems highly variable. Some seem to have thrived under the challenge and are inventing new ways of working with other pupils (there has been a big rise in study vloggers, a new thing to me), while others are giving in to despair.
As you say, there are no easy answers. Its pretty clear that the science is against those who argue that sending the kids back won’t make the pandemic worse. But that has to be balanced against a whole suite of other issues, including the health of teachers (a junior school teacher friend of mine is on the verge of a breakdown under the stress and worry).
What does occur to me is that there are a lot of old style rural school buildings here with high ceilings and double aspect windows, which can easily be made reasonably well ventilated so long as the weather is not too cold (we rarely have air con here, its never that hot). Maybe they knew what they were doing a century ago. More modern urban school buildings are far more problematic.
> So, the questions here are:
– can we open the schools reasonably safely? (and what does “reasonably safely” mean?)
– if no, who are going to sacrifice – the kids, or the vulnerable?
Those are good questions, and good science should serve the public as the public answers them. Unfortunately, good science is exactly what the CDC did not provide!
Indeed. TBH, I don’t know about anyone who did, and the best answers one can find to the first one is “For any definition of reasonably safely that includes not worsening the situation, and does not assume impossible *), the answer is ‘no’.”
So it pretty much always gets to the second question – of how much worsening are we willing to accept at what price.
But there it seems to be that the extremes tend to win, although always under the guise of the “common good” while ignoring, and not even discussing the tradeoffs. And IMO it’s a question that is critical, but of course, which pols want to make a choice where one or other reasonably powerful group will get hurt?
*) either theoretically, like “kids are immune, so who cares”, or practically “let’s install super-strong air-circulation devices in every classroom”, “use natural circulation in all weather, including freezing”
Another way this guidance from CDC is harmful is that it limits the scope of what is practically possible. It’s rather hard for Congress to appropriate money to fix air handling / sanitization in needy schools if the CDC guidance doesn’t include any definition of what success looks like to work against. So let’s have another few thousand people shipped off to the sandbox instead. Priorities are on display.
I should have said that CDC doesn’t admit there’s a problem to solve, much less set a target.
I have chimed in here before on this about my and my daughter’s situation. We’re in a large West Coast city school district which has been closed for close to a year. No in-class learning whatsoever.
During this time, as an ‘essential worker’ I was able to get my daughter into the boys and girls club along with a lot of other kids, to do remote “learning”. It’s ages K-early teens.
There, at the boys and girls club, they do school together, eat together, play and do recess together, study together… In other words, they are IN SCHOOL! Ii’s just not in a school district building. And it’s every day, not any kind of one day off-one day on, or half a classroom or whatever.
And they have not had one issue with covid.
“And they have not had one issue with covid.”
Are they testing everyone? If not, you have no idea how many kids have had covid, or more importantly, how many have passed it on to vulnerable family or community members.
Schools are have been open all year where I live.
Things seem normal.
Mid Missouri.
My son’s public school in suburban Maryland looks to be reopening in early Spring. Thank god because I’ve had to quit my job to be home with him and virtual learning is the worst for young kids. I was pleasantly surprised to learn that they’ve replaced all HVAC filters and installed air cleaners in every room. Kids will be spaced out and can only attend school every other week to make room for everyone. It’s a start. There is no reason that restaurants and gyms should be open and schools closed.
The problem is that school attendance is compulsory, which can expose individual administrators, the board of education, and the political subdivision to a civil suit from a parent(s) who is compelled under pain of fine and imprisonment to sent their child into an unsafe environment.
Our school (k-2) opened in sept and has stayed open since. 100% open, full time. 11 kids per class, masks. social distance. We had option to choose 100% remote which I did for my first grader.
The school has had many cases of covid among students and faculty. (Mostly students) .
They only quarantine CDC defined “close contacts “, not the entire class when there us a positive.
They are supposed to start pool testing but it’s (ready for this?) Voluntary. What’s the point if it’s not random?
Anyway, their go to line is “there has been no proven case of in school transmission so we remain open”. Well, I don’t buy it. They aren’t contact tracing for source of infection so how do they know??
It’s all so bizarre and as someone who leans to the cynical point of view (I’m too smart not to) …I dont buy it or trust it.
So we stay home.
My sister said her high school was on the precipice of closing from hybrid because the math and science departments were eating lunch together. This is a good high school. Kids want to talk to their friends and are loud.
As an agency, the CDC has been a servant to corporate interests since inception. During the malaria days, they were lock step with the chemical companies when it came to dumping large amounts of DDT and other chemicals (including just spraying motor oil) into ponds and streams in the south, side effects be damned. They eliminated malaria in the United States, though, which has to count for something.
Later, one of their patrons was the chairman of the board of Coca Cola, through Emory University. Along with the malaria legacy, that’s why the agency is located down in Atlanta.
Here’s a podcast about the CDC’s beginnings and how their relationship with Coca Cola and Emory evolved into a kind of three part partnership: https://soundcloud.com/tinderboxpodcast/out-flew-enza-cdcs-sweet-beginnings
Not directly related to schools but I listened to the Michael Osterholm podcast yesterday and he mentioned the CDC not acknowledging aerosol transmission, The salient point was that by not acknowledging aerosol transmission OSHA can’t check ventilation and I immediately thought of food processing plants and other workplaces where social distancing is difficult if not impossible.
Regarding Norwegian schools, a neighboring municipality, Nittedal, had outbreaks at two schools recently; one a primary school and the other a middle school. From Aftenposten:
https://www.aftenposten.no/norge/i/gWz0a0/mutanten-vil-dominere-hele-landet-frykter-fhi-i-nittedal-faar-kommune (The mutant will dominate the entire country, FHI fears. In Nittedal, the municipality receives help from Oslo and Lørenskog).
–14 cases of infection during the weekend, followed by 11 cases on Monday, have caused the alarm to go off in Nittedal. The outbreak is believed to be due to the British mutant virus.- About half of those who have tested positive are 7-year-olds who go to 2nd grade. There is also a teacher and a sibling at an upper secondary school who have tested positive, he says. (He being the municipal heath physician).
–A teacher and three other students who have been in close contact with the youth at Hakadal ungdomsskole, have tested positive for the coronavirus, he says.
Thanks for the long form takedown. I didn’t have the energy to dig into it. My daughter is a teacher slated to go back in the classroom for the final eight weeks or so of school. I can only hope the vaccination she is getting due to being a teacher will be sufficient – her classroom doesn’t even have windows, much less ones that are openable.
One small positive thing in the CDC guidance is that they are finally talking about community prevalence, something I’ve been tracking for months. If the prevalence were under 0.010 % (10/100k), it would be reasonable to go back to classes assuming a strong test/trace/quarantine policy.
Oregon counties, colored by CDC guidelines.
1) the R value in UK by age cohort is now highest in 5-12 year olds and 19-24 year olds. The young adults are likely either rule breakers or zerohour workers, possibly both. The children are old enough to be infected but too young to be left at home so they go into school, which is open for “key workers’ children”, a very flexible group that apparently includes the county council legal staff, a pen that you would think could be pushed from home. Younger children are in nursery but appear genuinely less susceptible.
2) I wonder if aerosol transmission is just too close to the miasmatic theory of disease for Western Medicine to take it seriously…?
Regarding HVAC issues…
The ASHRAE recommended number of air changes per hour for aiding in infectious disease control is 6 ACH. That means completely replacing all the air in a given volume every 10 minutes. That fails within many systems capabilities to do so, provided the system has the available controls to do it. It becomes expensive though because that means you’re wasting the energy to condition that air and then you need to condition a new volume of air, throw that outside too…and so on.
Along those same lines, most facilities like schools have economizer operations where they exchange incoming fresh air with conditioned air, or take advantage of other environmental benefits to freely cool or heat air as needed. These operations will mostly have to be disabled in order to prevent contaminating the incoming fresh air. That kind of change can require recommissioning a system and making other changes because dampers and control options may have to be disabled.
Finally, lots of people have discussed increasing the system filters to a higher grade, like MERV 13. Not every system can handle that that, because the higher the grade of filter, the greater the pressure drop across the filter, which means a fan may have to work harder to push air through the system. The increased demand on the system can cause the fan to burn out. It can also reduce the number of air changes per hour depending on the design of the system. These filters also become potential biohazards and need service technicians who know how to safely remove and change them and will need to wear full tyvek suits and respirators while they do the work.
Opening windows isn’t necessarily an option in some cases either. I’m not talking about whether windows can open or not. Opening windows can create issues with humidity and it can create pressure imbalances in the system. Pressure imbalances can cause doors to slam shut and other problems in a building. Humidity issues can of course lead to mold.
Long story short, it’s not a trivial thing to figure all this out.
There are calculations on the new variants needing exchange every 3 minutes due to their increased infectioness. Based on my understanding of your comment, existing systems in schools cannot meet that. So in my mind, outdoor instruction w/ modified school year is the only way to accommodate in person instruction without incurring energy and infrastructure costs. My operating assumption is that repeated COVID exposure to young and old could turn out to be harmful.
I would be interested to see any reference to requiring an ACH of 20 to handle this situation. There’s also been limited to no evidence that these variants of concern are much more transmissible. As Vincent Rancaniello and others on TWIV, and multiple clinicians have been saying these supposedly deadly variants aren’t doing that in the wild.
All that being said, yes, you’re correct. If we do need to fully exchange the air in a space every 3 minutes that would be very difficult to do inside any building. Your best bet would be to diffuse the contamination in a large volume of air which would make it much less likely to develop concentrations that would infect people. So we could hold class in a warehouse with no ceilings on the classroom space. Maybe that would give a purpose to all these malls that no one is using right now?
Lisa M Brosseau: “Losing my patience with CDC and the medical establishment. I posted questions and comments about aerosol inhalation on the JAMA network interview with Walensky and got shut down by the person managing the Q&A.”
https://mobile.twitter.com/brosseau_lisa/status/1362183795466792962
Cidrap bio: https://www.cidrap.umn.edu/about-us/staff/lisa-m-brosseau-scd-cih
Why do everybody pick on schools? I am in Delaware and literally every other thing, bars, restaurants, churches, casinos, malls, private sports, EVERTHING is open but public schools. Education is essential. Everything else should be closed and schools open. America has lost it’s mind.