The Seychelles is a tiny country, with a population of less than 100,000 people. It is nevertheless providing a cautionary tale in what happens if you relax Covid protections and rely over-much on vaccinations as your Covid firewall. It’s in the midst of a Covid outbreak so severe that it has had to reimpose lockdown-type measures like closing bars and schools, despite having over 60% of its adults fully vaccinated.
The trigger appears to have been reopening the archipelago for tourism. From Bloomberg:
Seychelles, which has fully vaccinated more of its population against COVID-19 than any other country, has closed schools and canceled sporting activities for two weeks as infections surge…
To date 62.2% of its eligible population is fully vaccinated, according to the Bloomberg Vaccine Tracker. That compares with 55.9% for Israel, the next most vaccinated nation.
Colonel Smithers added via e-mail:
The BBC article [cited below] did not mention that a few weeks ago Seychelles and Maldives opened their borders to tourism, somewhat to the envy of their competitor for tourist hard currency Mauritius.
The big Mauritian hotel operators have hotels in Seychelles and Maldives and have been lobbying for Mauritius to open, too, and cited the example of the pair.
This included getting a doctor heiress to a hotel fortune, amongst other sources of income, to write about the need to open in the island’s largest circulation newspaper. She quoted that 60% vaccination figure as conferring herd immunity, which dad challenged in a BTL comment.
Seychelles and Maldives reported that a few thousand visitors had arrived within the first week of opening and Emirates and Turkish Airlines, with their spokes and hub models centred on Dubai and İstanbul, had been the first airlines to return and to some fanfare.
Seychelles and Maldives have been advertising that they are open for business in the likes of the FT and Guardian and on CNN in the past fortnight. Not just tourism, but people able to and wishing to work from home or just sit out the pandemic for a while in the tropics, not necessarily those with any connections to the archipelagos.
One wonders if variants from around the world which render the current vaccines ineffective have caused this.
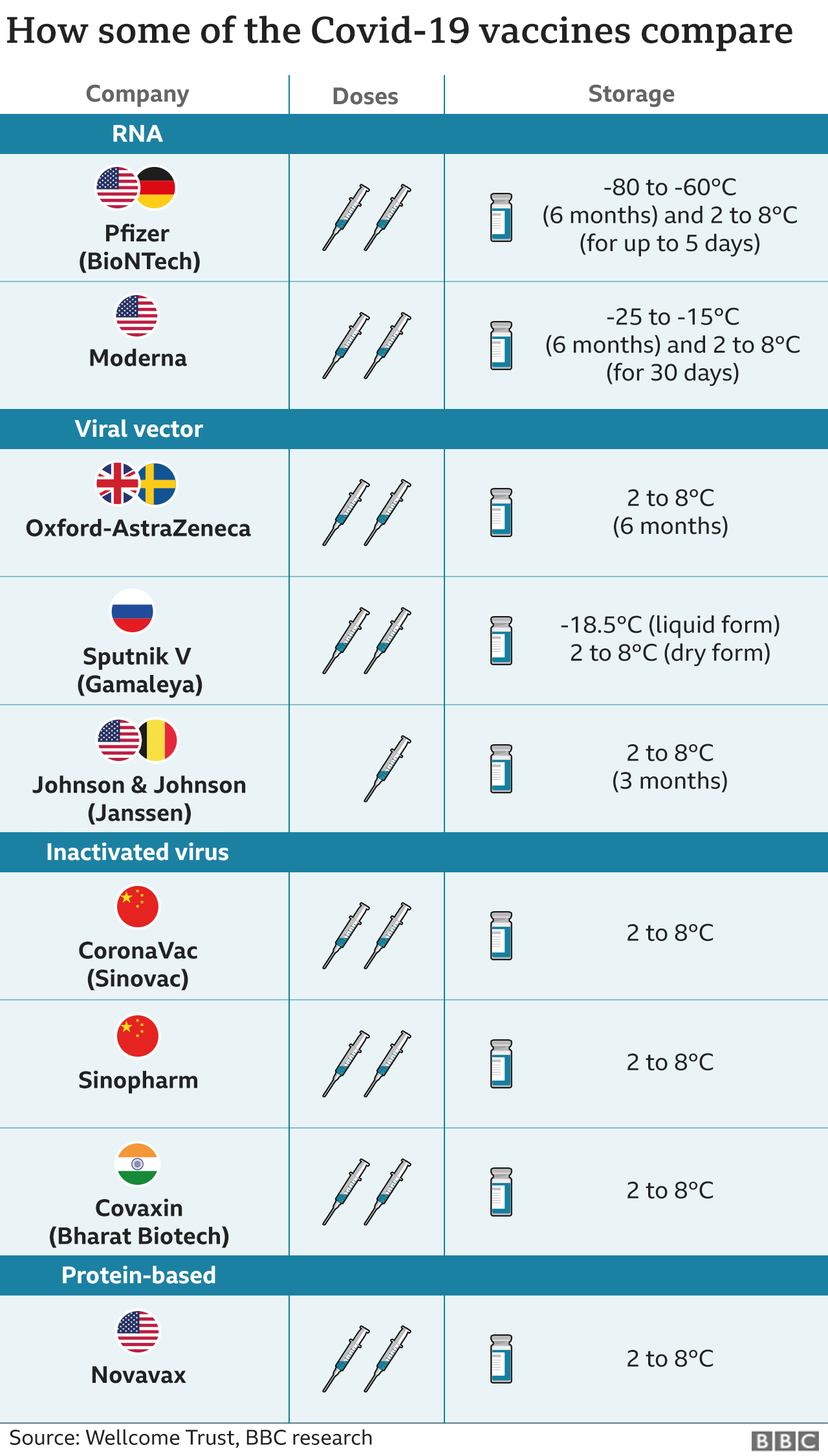
It is hard to blame vaccine choice. Seychelles used Sinopharm, which according to the BBC, has performed well, and AstraZeneca. And as you can see from the chart below, these vaccines don’t require as much special handling as the mRNA alternatives, meaning the odds of spoilage would be lower. From the BBC (hat tip vlade):
The Seychelles, which has fully vaccinated over 60% of its population against Covid-19, is bringing back restrictions amid a rise in cases.
The archipelago of nearly 100,000 people recorded close to 500 new cases in the three days to 1 May and has about 1,000 active cases.
A third of the active cases involved people who had had two vaccine doses, the country’s news agency said….
More than four-fifths of the active cases were among Seychellois people, with the remainder made up of foreigners.
We don’t have more granular data as to whether the bad outcomes occurred heavily among citizens who weren’t far enough past their second shot to have received full immunity. But this is still not a good look. Again from BBC:
By mid-April about 60% of the vaccine doses administered in the country were Sinopharm, with the rest Indian-made AstraZeneca vaccine doses, Bloomberg reported….
Trials in China and the United Arab Emirates have put Sinopharm vaccine efficacy at 79% and 86% respectively.
I have been concerned that the odds of the new variants escaping the current vaccines has been underestimated. Note that experts outside the US have argued that an inactivated virus vaccine should offer better protection against variants than the mRNA vaccines, so the use of an “old technology” vaccine does not seem likely to be the cause of these results. For instance, from LiveMint in March:
India’s mass covid-19 vaccination drive, which began on 16 January, entered its second phase on Monday to include senior citizens and those over 45 years with comorbidities. The programme includes two vaccines. Covishield, developed by AstraZeneca-Oxford University, is based on a recombinant chimpanzee adenovirus vector that encodes the spike protein. Covaxin, developed by Bharat Biotech in collaboration with National Institute of Virology, is an “inactivated” vaccine that uses killed SARS-CoV-2 virus, eliciting an immune response targeting more than just the spike protein. In an interview with Mint, Dr Shekhar Mande, secretary, department of scientific and industrial research and director general, Council of Scientific and Industrial Research, spoke on how the antibody response by a killed virus vaccine is likely to offer greater protection against mutated variants of covid-19, than vaccines generating antibodies against spike proteins….
Interestingly, the breadth of antibody response generated by a killed virus vaccine is likely to offer greater protection against mutated viruses, than vaccines that generate antibodies against the spike protein.
Note that a more technically-oriented article concedes the efficacy versus variants issue while still defending the mRNA approach. From Clinical Trials Arena:
Despite the theoretical potential of inactivated virus vaccines to offer a lead over other Covid-19 vaccine technologies against variants of concern, experts said they are unlikely to be a long-term solution. While it is logical that these vaccines could have better efficacy against variants that have mutations in the spike protein, they come with existing baggage such as relatively lower efficacy versus other Covid-19 vaccines, they noted. And though inactivated virus vaccines have an edge in initiating a T-cell response, the overall value of this mechanism is still unclear in the context of Covid-19 vaccine development, some added.
Hopefully the surge in Seychelles will focus some minds and lead to more caution about reopening. But given animal spirits and business clamoring for income, probably not.


I wonder if SinoPharm has some of the same issues with SinoVax. In Chile I believe they found it offered only very limited protection after a first shot, and even the second shot provided significantly less protection than most of the other vaccines. Chile, of course, also had a major surge in infections despite a very high vaccination rate. I suspect also that the faster the roll-out, the more likely it is that there could be errors – for example, using vaccines that may not have been stored correctly prior to use. The one big advantage slow adopters will have with vaccines is that they are more likely to get things right.
But its pretty obvious here that the key issue is travel and tourism. Most tourists go to the seychelles via the big international hub airports. One can only wonder at the sort of mixing thats going on there. We may not just be dealing with dangerous variants, but a huge stew of different variants all mixing in airports and hotels and then being distributed worldwide. Its the worst possible thing to be doing, an experiment in mass stupidity and all because people aren’t willing to just take a break at home for a year. Mass tourism has been killing the planet for years, now its killing people directly.
Plutonium Kun: Another key issue is the concept of herd immunity (currently much in favor among the nihilist-lite Republicans and the feckless Democratic liberals who rule the U S of A).
(1) Yves Smith has pointed out repeatedly that the coronavirus belongs to a class of virus that are so variable that herd immunity can never be achieved. As you write, the stew of variants means never being able to control infection / virulence. It is time to call herd immunity what it is: Upper-middle-class fantasy.
(2) There can be no herd immunity if the herd is constantly receiving enormous numbers of new members. The idea of quarantine, as developed by the Venetians, was to keep ships out in the lagoon on water for a number of days to see if any cases of “plague” arose. Tourism without quarantines is simply importation of disease.
(3) We saw this last year when the Greeks had an outbreak at the end of the summer tourism season even though they collectively had done very well in controlling the virus during the off-season.
(4) And, yes, flying through Ataturk Airport, which is gigantic, at a time when Turkey is a hot spot, seems, errr, ill-advised.
(5) Which all leads to: Our “betters” have no interest in the survival of the mass of people. Let the repercussions begin!
(1) and (2)…wash, rinse, repeat. Wash, rinse…
Hello Folks, Here is a link to Roy Labs Stats. I have found them quite reliable with …… stats related to Corona virus. Here is their site: https://www.youtube.com/watch?v=NMre6IAAAiU or just “Duck” Roylab Stats.
I bring this up as the stat dashboard is recycled about every minute, meaning that it’ll show deaths per country, case growth rates, recovered, and other ways of observing and calculating the virus – often focussing on regions, hemispheres and of course specific countries. A recent dashboard showed virus mutations. The “estimation” of variants based on current variant permutations was 20,945. I’ll try to paste a screen shot as I don’t know when the variant dashboard will appear again. It was last updated 2020-12-23 though it appeared yesterday.
PS, pasting the pic didn’t work. Now it’s a trust issue :-) Cheers.
I thought the Chinese vaccines were awful and not US propaganda but lots of people with them getting infected in Latin America. I’ll have to do digging, but there was an article on Chile that made it sound worthless. So bad that Chinese “vaccine diplomacy” may be backfiring.
Was that Coronavac and not Sinopharm?
Chile uses Sinovac. The health ministry reports 67% efficacy against symptoms. That’s pretty far behind Sinopharm, not to mention Pfizer or Moderna.
You both need to read a lot more carefully
The vaccine used was Sinopharm, not Sinovac. Sinopharm has higher efficacy.
And on top of that, apples and oranges. Pfizer and Moderna NEVER measured efficacy v. mild symptoms, but v. serious cases and deaths. I have never seen any reports on how they perform in terms of mild or asymptomatic cases.
Even the less-potent Sinovac performs well when compared properly to the mRNA vaccines:
https://www.bloomberg.com/news/articles/2021-04-13/are-china-s-covid-shots-less-effective-experts-size-up-sinovac
I have been wondering about the vaccines versus long-Covid, given that most long-Covid cases seem to start with a “mild” case, which then turns into often severe long-Covid.
I’m guessing there is no information on that question–how many of the “mild” cases not prevented by vaccine turn into long Covid, in vaccinated versus non-vaccinated.
Yes, this! I’ve been wondering about this since the vaccines first received emergency authorization. (Pfizer, Moderna.) If you have a mild case after being fully vaccinated, both doses for mRNA+2 weeks, what portion of people, if any, might suffer from long-COVID?
If it is a small enough number, we might not hear about it for many months or years. But until we know, it is another excellent reason to continue to stay safe.
All of the apples to oranges comparisons are enough to make us all pull our hair out!
We need head to head trials. Large ones powered to see differnces in deaths and long term morbidity! Who wants to bet it wont happen?
It’s not so much the trials per se (although the timing and country selection did make a difference with J&J v. earlier ones), it’s the incomplete reporting of trial data and the inconsistent methods for tracking illness (symptomatic for Pfizer v. everyone being tested weekly for AstraZeneca, as one example). That may be what you meant but there are many variables and some are more easily corrected for than others.
but they did NOT HAVE death and disability as primary endpoints.
Yes, agreed, our Covid brain trust members are very upset that none of the clinical trials or follow-on work has looked at all factor mortality rates among the vaccinated. That is bog standard for all past vaccines, I am told.
It is a true shame. IMO. The rush has not helped.
Both? I wrote specifically that Chile (not the Sychelles) uses Sinovac, which has less efficiency than Sinopharm.
John Burn-Murdoch, data scientist for the Financial Times,, has explained the numbers in a thread:
His conclusion:
As the article states, it’s 62% that are fully vaccinated.
The failure rate among the fully vaccinated is what is troubling here, not the relative levels of infection in the vaccinated v. not.
And the rest of his take is way too confident given the influx of tourists and the high odds of variants driving the upsurge.
Given that the infections among the vaccinated appear likely to be variant driven, we need to see how many actually do wind up not being hospitalized. The old data may not be generalizable to many of these cases, particularly since our IM Doc in flyover reports cases of fully vaccinated patients getting full-blown cases of Covid that did put them in the hospital. One was a very fit man under 60. He also pointed out this, that serious Covid cases among the vaccinated elderly seem to be under-reported:
It’s very important to know which vaccine was used. The J&J has a lower rate of efficacy. Also long term care facilities most likely have different stats with respect to immune system efficiency relative to the general population. The long term care facilities may not reflect the general population.
I’m not saying the care facilities reflect the population. I am saying that there appear to have been a meaningful levels of deaths in these Texas clusters among fully vaccinated people, something the media has been blaring does not happen.
In general, members of long-term care facilities were vaccinated early, and J&J was approved late, so I doubt J&J was used much.
More important, the story that J&J is less effective is exaggerated. J&J went under clinical trial later and in countries with more variants already out and about. So it was subjected to more daunting trial conditions than Pfizer and Moderna.
It also appears that the figure used to hang J&J, as with Sinovac (see above) is overall efficacy. Note that Pfizer did not test all subjects regularly in its trials; participants had to report symptoms and then be tested. So they were set up not to capture asymptomatic cases.
By contrast:
https://www.urmc.rochester.edu/news/story/why-the-johnson-johnson-vaccine-is-more-effective-than-you-think
Let’s see…
Population: 100,000 (nice round number for ease of calculation)
Number fully vaccinated: 62,000 (0.62 X 100,000)
Efficacy of either AZ or SP vaccine: (0.8, this may be overly generous)
Number effectively vaccinated: 49,600 (0.8 X 62,000)
Number ‘ineffectively’ vaccinated: 12,400 (0.2 X 62,000)
Number unvaccinated: 38,000 (100,00 – 62,000)
So of the portion of the population with (presumably) no immunity (un- and ineffectively vaccinated), one would expect about 1/4 of the cases to come from those who were vaccinated but didn’t mount an immune response. Lower efficacy numbers for those vaccines (which are more likely to represent reality) would bias that further towards the 1/3 ratio. The observation that 20% of the infected are foreigners could introduce bias as well, but the direction would depend on their vaccination status.
Thank you, Yves.
For readers, especially those in the medical profession, my father specialises in biochemistry, pathology and toxicology. He’s not a virologist or epidemiologist.
It would be interesting to see more granular data, in particular how many of the already-vaccinated-and-infected had AZ vs Sinpharm.
Remember that SA stopped using AZ earlier this year as it was shown to be <50% effective against the SA variant.
Thank you, Yves.
Further to the map displayed by Yves, along the east coast of Africa and on the islands, some locals of Indian origin have returned from pilgrimage in India. There are also workers from India working on Indian government funded projects, such as the tram in Mauritius. There are similar associated with Chinese funded projects.
PK uses the phrase “stew of variants”. It just does not bear thinking about.
Colonel, thanks a lot for your reporting.
I think that we are collectively failing to understand what can we expect from a campaign of massive vaccination against a respiratory virus and more particularly against a respiratory virus that is transmitted with relative ease amongst humans.
I think I have written about this here more than once, twice, etc. Talking about ‘immunity’ doesn’t make much sense in a case like this. There is not a barrier (except some difficulties the mucosae impose) to virus entry into the upper respiratory tract and as long as viable particles enter in numbers high enough we will be infected even if we have a humoral response (antibodies). It is only that the load will have to be increased if you have some antibodies spread into the URT mucosae. Instead of taking about ‘immunity’ or a barrier we should think about vaccination as inducing quantitative protection. The level of protection will very much depend on the levels of neutralizing antibodies on the nasopharyngeal mucosae compared with the entry load. So, if you have high enough levels of antibodies you can be deemed as ‘fairly immune’. The levels of antibodies in the mucosae depend very much on the levels in blood since these cross the circulatory system to spread around the epithelial tissues of the mucosae.
Unfortunately, to maintain high levels there, where it matters, would require high level antibody production and sustained in time, something our body cannot afford (particularly keeping in mind the many virus serotypes that can enter through our respiratory system). In the best cases you will be fairly immune for some time after the second shot. Sinovac does not distinguish herself by inducing particularly high levels of neutralizing antibodies compared with other vaccines so it may well be the case that one is ‘fairly immune’ just for a short time, let’s say for instance, a few weeks.
But this not the whole story, fortunately. Whether you are fairly, moderately or barely immune to virus entry in the URT when you have been infected or vaccinated before, not totally naive to the Coronavirus, for instance with the Sinovac vaccine your chances to fight the new infection are much better now and there is a range of immune tools that might prevent further progression of the disease into the worst outcomes: you have memory cells that will wake up fast, and with the chance of producing new antibodies against new variants that are somehow different, and you indeed will have a faster cellular response that will help against progression.
I think it would be very important to have a follow up of these new infections in Seychelles and compare the development of severe respiratory syndrome between those vaccinated and infected with those that weren’t vaccinated. IMO, there will lie the real efficiency of the Sinovac vaccine and my guess is that the incidence of severe or fatal outcomes will be very much reduced within those vaccinated.
Your comment is extremely interesting and I thank you for that.
Medicine is not my profession, so maybe I am saying something stupid, but: I haven’t read anything like ‘quantitative protection’ in papers (and I’ve read 100s). Do you have a suitable source?
All I’ve seen is talk about 90% efficacy, but they don’t define efficacy as anything usable. Should we expect to be immune 90% of the time (which would mean everybody finally gets infected) or 90% of the people all the time?
I haven’t found any answer to these basic questions, so I am very intrigued by your interpretation (which makes sense to me, but couldn’t find anywhere).
Still Flying = Total Fail
Why is that so hard to understand? I know, Upton’s sagacious observation is on full display.
Because moneeeeee . . . rots the brain.
You mean traveling instead of flying? I ask bc I thought that, at least in the US, the safety practices that airlines have been using has made flying a relatively safe way to go. It’s what you do after getting off the plane that is the problem. Is that not still true?
First, most, if not all commercial passenger carrying airliners have fully enclosed cabins with heavily recycled air. I’d imagine that airliners would have efficient air filtration systems, considering the exudations and miasmas Terran humans emit. On extended flights, the degree of inter-personal air mixing probably approaches 100%. There have been several graphical presentations of the transmission paths for viruses in enclosed spaces here over the past year. So, the airliner itself, perhaps not so much a factor in virus transmission.
The airports are where the major viral mixing would happen. International airports are huge places, usually enclosed with ‘tempered’ air. The theme of the insufficiencies of the air filtration systems in public spaces has come up here before.
I would compare giant enclosed public spaces to petri dishes. Mix your ‘ingredients’ and see what grows.
Of interest to the ‘curious’ personality type, a long PDF from NASA outlining the computed requirements and ancillary items for a space station. From 1982. Atmospheric considerations are part of section 10.0.
What the NASA document shows me is that we can do the “right thing,” when motivated and funded. At least, we could do so forty years ago.
I am reminded forcefully of the follies of the PMC/Meritocrat politico class when I consider that both the Space Shuttle Challenger and Space Shuttle Colombia disasters could have been avoided if the relevant ‘expert’s’ warnings had been heeded. Both disasters were the result of politically motivated decisions by NASA middle managers, aided and abetted by NASA upper management’s craven careerism.
The ‘national’ response to the Pandemic is of a piece with the Space Shuttle disasters. The Laws of Institutions ‘select’ for cowards and conformists.
See: https://ntrs.nasa.gov/api/citations/19820012330/downloads/19820012330.pdf
> You mean traveling instead of flying?
Ambrit lays it out much better than I could. I mean flying, because of all the mixing and concentration of people during the act of getting to where one is going, and in the case of this post, travellers to the Seychelles flew, instead of drove or swam.
When one travels by car alone or with someone close, the risk is in essence zero of getting it or passing it on and tactics can be used, mask wearing, keeping a distance from other pedestrians at rest areas and spending little to no time going in for a whiz, and forget about the food courts. In other words, I control the risk. On an airport -> aircraft -> airport route that is not possible. So the virus will hop across oceans and continents constantly all day long, every day spreading far and wide.
What one does after getting to your destination is obliquily related. If the purpose of going somewhere is to party your face off in a closed environment, and flying a whole bunch of people to that place is what got everyone together, which this post is a demonstration of, and then a lot of people become ill due to that level of carelessness, the logical conclusion is Still Flying = Total Fail.
Travelling by surface transportation has risks too, but they would spread the virus much slower and as an individual you can mitigate the risks depending on the situation. Flying is the big culprit. Once on board, its a crapshoot that you won’t know the results of for a week afterwards and if infected are now infecting people in your wake.
Ok, given what ambrit and you say, if the crowding and mixing in airports, along with getting there and leaving, is near what it was in 2019, say, then exposure will certainly be a problem no matter what happens on the plane. Thanks.
I’m still trying to wrap my head around the idea of “swimming to the Seychelles.” That would be a major adventure itself.
Did a lot of airport and airline workers worldwide get infected just before the drop off of air travel last year? I could never find any good information. One would think they would be the first ones affected by the spread of the virus.
Slight aside, my sister is a flight attendant who has kept flying through the pandemic without getting sick or testing positive for Covid-19. Jing jing. Then again, she may have an immune system like George Carlin claimed to have, but after several decades of flying.
It’s hard to make sense of all of this nowadays, but I like this site’s (NC’s) attempts.
If aerosol were not a problem on airplanes then why is smoking prohibited?
I think it is as in any confined area. Perhaps since a virus is much larger than CO or even CO2, it is much easier and cheaper to filter out.
This article explains the problems with passenger jet cabin air. https://www.cntraveler.com/story/how-clean-and-safe-is-a-planes-cabin-air
… why do you think?
Here in Switzerland, there are reports from travellers that although the tests are mandatory to board the plane, they are almost never checked. Still, it is more about what you do after as you said.
Slightly Off-topic Travel Query: I am traveling from nowheresville to somewheresville so a friend can have surgery. The trip requires an overnight hotel stay. Can anyone recommend a travel sized (or smaller footprint) and quieter air filtration device to use at the hotel?
Buy a tent?
I have been wondering if there are any CPAP machines with a UV sterilizer feature.
As a microbiologist, humans may be facing a reality that is inescapable. For eons, humans had no defense against infectious diseases except what evolution provided. Pasteur published his germ theory around 1860. Success in developing effective vaccines against scourges to humanity followed and was truly amazing. And as is wont with humans, taken for granted. Look at mortality tables of the 19th century and it is startling to modern sensibilities.
I think we have reached the point that the truth of the matter is that microbes ability to evolve will exceed our ability to mount defenses. The fact that measures against microbial pathogens succeeded so well for so long does not mean that they will continue to succeed.
I am vaccinated, and I have a long list of co-morbidities that put me at great peril. I hope measures can be implemented that will be effective – I like living. But I think the truth of the matter is that humans ability to control the environment is much less than humans suppose. And that is if a significant majority of humans do the rational thing – which considering that the proposition that a significant majority of humans are rational, is a dubious proposition.
Based on what you say, I think that I can guess what comes next. It will be argued that what is needed is a vaccine that will be given at birth and will give that person a beefed-up immunity system. But this one will be different as it will involve a form of gene therapy. So a vaccine that will ramp up a body’s defence mechanism by incorporating and supplanting some parts of a person’s DNA. You can imagine the risks involved but I do not think that people want to go back to the 19th century in terms of diseases. In my extended family, there was young girl that had a bug fly into one of her eyes over a century ago. Within days she was dead of infection. Such was life pre-vaccines.
I was researching the history of a historic building prepping for a pitch to the historical society and in the newspapers from the early 1900’s were many disturbing stories re the perils of life, but one has stayed with me (the other was the 100 lb salmon caught in friday harbor in roughly 1912, which picture I’ve posted here once or twice). Back in the day before drywall houses were lathed and plastered, which from the perspective of modern homebuilding would be tedious in the extreme. Imagine nailing furring strips 1/4″ apart over the entire interior, then mixing what is essentially cement and spreading it on the walls with large wooden trowels. One could get lost in a search of that historical record of plaster. It’s a lost art. At any rate, while reading I came across a story of a kid helping his dad lath a house, he jumped off a ladder and stepped on a nail. Gangrene set in and they amputated his leg after one week, and he died after the second. Tetanus shots have saved a lot of people…
From Spoon River Anthology, by Edgar Lee Masters, 1915. The conceit is that each poem is an epitaph on a gravestone in a local graveyard, written by or about the deceased. This stupid poem has haunted me ever since I read it as a teenager. I’ve urged more people to get tetanus shots than really has made sense.
Charlie French
Did you ever find out
Which one of the O’Brien boys it was
Who snapped the toy pistol against my hand?
There when the flags were red and white
In the breeze and “Bucky” Estil
Was firing the cannon brought to Spoon River
From Vicksburg by Captain Harris;
And the lemonade stands were running
And the band was playing,
To have it all spoiled
By a piece of a cap shot under the skin of my hand,
And the boys all crowding about me saying:
“You’ll die of lock-jaw, Charlie, sure.”
Oh, dear! oh, dear!
What chum of mine could have done it?
For your pleasure, the great Steve Goodman...
Tetanus is a separate disease and it didn’t kill that kid. It was a simple bacterial infection that got him.
I had an acquaintance who worked in a lobster retailer/wholesaler on the East coast in the 2000s. A lobster tail fin cut his upper leg.
Infection set in, one leg was amputated, then the other. He then died.
Antibiotic resistant bacteria is real and it’s killing people today. One of the many tragedies of the 20th century is the feeding of large quantities of antibiotics to farm animals. We’re sure going to miss effective antibiotics.
I think we have reached the point that the truth of the matter is that microbes ability to evolve will exceed our ability to mount defenses.
Especially with a little help from human scientists doing gain-of-function experiments. / ;) (paging Dr. Frankensteen)
For, GOF, look no further than Fauci.
https://www.newsweek.com/dr-fauci-backed-controversial-wuhan-lab-millions-us-dollars-risky-coronavirus-research-1500741
Also, let’s not forget the mining of US and global health by the ‘food’ scientists who design unnutritious food that tastes good. And the behavioural scientists who are more than willing for a $ to research and design methods to sell that “food”. Human health is under attack by science.
All this while the esteemed Epidemiologists, Virologists, etc. stand obliviously and silently by.
I was thinking about the relationship between triple-resistant bugs and covid responses yesterday, and it strikes me as a fine opportunity which we’ll almost certainly squander. We have the opportunity to get ahead of the failure of our medicines and build our calendar around managing those bugs in other ways. The 2020 covid response is all about how we manage disease without having effective treatments.
That is, we’re currently (at least where I am) kind of on board with “lockdown” responses for short periods, but the disruption is worse if they’re unpredictable. However, flu season is not unpredictable. So restructuring our economic activity around a flu season lockdown period each year is totally possible.
If you tie this together with potential responses to productivity increases and persistent unemployment, you could have work 9 months, get paid 12 as a standard. This would be instead of working 4 days get paid 5, which is already being floated and trialled. A month of annual leave a year has us already working 11 months and getting paid 12, adding another two months for lockdown times is not a terrible difference.
Predictable lockdown periods will likely result in the same kind of flourishing of human-centric and healthy activities that we saw in the longer lockdowns last year. Just assuming the flu season is dangerous and acting accordingly will prevent a lot of heartbreak when the particularly bad variants come calling.
There are problems of course. Essential workers don’t get to escape – so we’ll need to recognise that and increase the number of people paid to do those jobs so the two months off can be staggered outside the lockdown period for some of them (to maintain equity in working hours). Increasing employment would of course would require paying essential workers a wage commensurate with the risks of their jobs.
Anyway as I said, of course we won’t do anything sensible like this, so it’s all just daydreams.
You might enjoy William H. McNeill’s “Plagues and Peoples.”
Past is prologue …
If about 62% of the population has been vaccinated and an unknown number infected previously, then I suppose that you can say that this is a real world experiment in what happens if you have a population with a solid measure of herd immunity that still gets exposed to infected people. Based on what is happening in the Seychelles it is not good, particularly in light of the fact that ‘A third of the active cases involved people who had had two vaccine doses.’ This virus just does not give you a break at all.
There is no here immunity on the island. That is why there is an outbreak.
And they always knew that people would still get infected with the virus after the vaccine. And have symptoms. Part of the role of the vaccine is to keep people out of the hospital and dying, which It is currently doing.
What is going on there is concerning, but it’s not alarming in any sense.
Why does 60% fully vaccinated with a vaccine that has roughly 60% efficacy mean herd immunity? That seems to mean that only 36% are protected and herd immunity demands a larger percentage. What am I missing?
You’re not missing anything. He was wrong.
There’s no herd immunity on the island in the outbreak is normal for easing up restrictions during a pandemic. This is nothing to have anxiety about. Except if you live there.
It isn’t clear to me what exactly had been eased up on the island. I can see that they allowed travelers again, and I gather they did not test or track any of them. Yet was mask wearing and social distancing stopped, assuming they were practiced before?
Thank you.
There was no quarantine, test and tracking for visitors.
Social distancing and masks were dispensed with some months ago as the initial lock down was successful.
Appreciate it.
There is no herd immunity for COVID19. Period. As there never was herd immunity to the cold or to the flu.
Even if you were able to vaccinate 100% of the population all in the same day there still would not be herd immunity. I wish people understood this once and for all.
I understand. A benefit of never having finished college.
Thanks Pedro.
I would quibble: There is currently no prospect of lasting herd immunity of the sort that could prevent further epidemics absent competent public health measures to monitor for and suppress the outbreaks that will inevitably occur.
Monitoring and suppressing future outbreaks isn’t “herd immunity.” Not even close.
Instead, it’s using the tried and true methods of disease control that Vietnam, New Zealand and other countries that placed saving lives over economic activity used.
Pedro is right. There is no herd immunity.
The Rev Kev
May 6, 2021 at 9:33 am
https://www.amazon.com/Body-Hero-MD-Ronald-Glasser/dp/0394400135
I happened to read the above book prior to starting to major in microbiology. Just to further my first post, we believe medicine cures disease. The truth of the matter is, if your own body’s restorative functions are impaired, you will not get better. If your immune system is impaired or diminished due to age or health condition, the vaccine is going to be significantly less effective than when provided to a younger person in good health.
https://www.mayoclinic.org/diseases-conditions/flu/in-depth/flu-shots/art-20048000
The people most endangered by Covid are the least protected by vaccines. That is just the nature of the beast. It is better to have the vaccine than not have it, but for a lot of people, the vaccine alone is not enough…
We live with this reality as relates to influenza. Now we have another respiratory disease, that appears to be significantly more serious. This upcoming winter is going to put some stark choices on the table…
If there is not a surge in AZ in June, and then in Florida in July, I will relax. Otherwise declines are just seasonality …
“By mid-April about 60% of the vaccine doses administered in the country were Sinopharm, with the rest Indian-made AstraZeneca vaccine doses”
Indian drug manufacturers adulterate their products. Katherine Eban has written about this problem, based on the efforts of an FDA investigator to fight this problem:
https://www.katherineeban.com/
As I recall, these manufacturers have one standard, for products sold to America, based on what they think they can get away with, and an even lower set of practices for drugs sold to the developing world, perhaps including the Seychelles. They might have shaped up their behavior for the COVID vaccines, given the public spotlight.
Correct me if I am wrong, the personal benefit for the shot is not to prevent you from getting covid but to prevent you from suffering a serious response. Is that correct?
In a probabilistic sense, as what you would expect from your annual flu shot, that is my hunch. But we’ll see.
Was the article from The Atlantic The Liberals Who Can’t Quit Lockdown discussed here on NC?
https://www.theatlantic.com/politics/archive/2021/05/liberals-covid-19-science-denial-lockdown/618780/
I mentioned it in the comments the other day. Didn’t seem to gain any traction, though.
This is fairly obvious from a biological standpoint, and is the reason the most well-protected class of individuals will be those who’ve had the virus as well as a booster in the form of a vaccine. Like me. But read on…
There is very simple reason these vaccines show less efficacy. Inactivated viruses do not make a great source of antigens for live viruses. Think about it. How does one inactivate a virus? Generally this is done by heat-killing–think 65C or higher for an extended period of time. The consequence is that the viral proteins are denatured, meaning (among other things) that their normal spatial conformations are disrupted. Antibodies recognize these 3D structures. So it’s pretty obvious to expect that antibodies raised against denatured proteins are going to be less effective. In addition, to make inactive virus requires production of massive quantities of replication-competent virus under very stringent biosafety protocols. It’s not hard to imagine what can go wrong there.
On the other hand, the mRNA vaccines can use the spike protein sequence and present it in the same native conformation as the virus does. Because the spike protein is only 1 of 29 genes present in SARS-CoV-2, the breadth of antibodies is much less but there’s little risk of anything biologically dangerous. The antibodies that are made are highly effective against real virus, unless the spike protein can mutate sufficiently 1) to escape the allelic variant used in the vaccines while 2) retaining the ability to bind the ACE2 receptor. The most promising course forward is that future boosters are made to address dangerous allelic variants that arise, which is inevitable in the genetic arms race.
(For the record, I am a career academic and do not consult for big pharma.)
Disagree. Cell immunity is likely more powerful with the adenovirus and killed virus vaccines. You are restricting your immunity efficiency to humoral response.
It’s not a one-or-the-other situation. Inactivated virus vaccines definitely do not stimulate humoral immunity as well as other vaccine classes for the reason I mentioned above. If the argument is that inactivated viruses stimulate cell-mediated immunity to a greater degree, that may well be true…but I’d certainly want antibodies to defend against a virus instead of a weaker and generally secondary immune response to viruses.
and yet higher Ab levels have been associated with more severe disease. .
Which is exactly what you’d expect in a properly functioning immune system mounting a response against a virus.
uh, no. these are the patients who do the most poorly
The criteria used to assess the mRNA vaccines in the trials was based on symptom number. They didn’t assess for the most obvious endgame scenarios like hospitalization, ICU admittance, death. They didn’t choose these things as bad outcomes, or in their vernacular, “Primary Efficacy Endpoint.”
Also, the trial participants were all very healthy individuals, as opposed to being a cross-section of the population, as is usual in these trials.
There is no hard evidence to date that the mRNA vaccines prevent infection or transmission. All we know for sure is that they may prevent some symptoms for some people.
Adding, the allegedly high efficacy numbers for the mRNA vaccines are not accurate. Not even close, in fact.
As of a week or two ago, when I last looked into the subject, vaccines that present the ‘fixed’ form of the spike seemed to be retaining in vitro neutralizing capacity better versus variants of concern.
Patient data from South Africa corroborated this for one of the mRNA brands, I’ve forgotten which now. Anyone know of any more recent comparisons?
Is the problem with antibodies to structures other than the spike, or to less than optimal configurations of the spike, that the damn virus may still get jiggy with one of your cells even with the antibodies glommed onto it? Or is it perhaps more a matter of the antibodies lacking sufficient affinity for the actual structures present? Something else entirely?
you cant look at immunity in such a simplified way. that is the problem
immunity is about an entire orchestra coming together in a harmonious way. You are suggesting that if only the violins play their part well the symphony will sound lovely. Just like an orchestra the timing is critical. How fast do the Abs come online. How well targeted are they. When does the cellular system kick in to active NK cells etc etc etc.
“but there’s little risk of anything biologically dangerous”
like the spike for example?
I think I read this link through NC.
If the spike protein from the virus can generate this response, couldn’t vaccines, (including mRNA vaccines) do the same?
https://www.eurekalert.org/pub_releases/2021-04/eb-gcm041621.php
NEWS RELEASE 27-APR-2021
Gene changes might explain long-haul COVID-19 symptoms
Results from a new cell study suggest that the SARS-CoV-2 spike protein can bring about long-term gene expression changes. The findings could help explain why some COVID-19 patients — referred to as COVID long-haulers — experience symptoms such as shortness of breath and dizziness long after clearing the infection.
There is a lot of missunderstanding about how much vaccines on their own can achieve. There will never be herd immunity for thid disease no matter how many people you vaccinate.
We should still be trying to irradicate the disease instead of betting everything on vaccination and simply allowing the virus to circulate.
The flu kills a lot of vaccinated people and mask mandates and the like got rid of the flu but not Covid19. If you think that vaccinating everyone will never happen and you have a recipe for disaster.
“One wonders if variants from around the world which render the current vaccines ineffective have caused this.”
There’s not enough information available to know one way or another of the efficacy of vaccines toward variants. Any information that is available suggests anywhere from 50% to 90% efficacy, and the likelihood is the studies themselves need further evaluation to determine if what they’ve found is really what they’ve found.
It is likely though, in the end, any studies finding lower efficacy results are studies that are too soon after injection, which introduces a whole lot of noise into the results as the three weeks after people are injected are when they are most careless regarding social distancing. But it also takes three weeks for the human immune systems to fully develop a response to the vaccine, and so begin protecting the body from the virus in some capacity. So, it is likely then that this nation probably opened up during the three week window rather than after it, and so have created a situation where discerning what is going on is going to be hell to find out in regards to efficacy.
It is likely then the 70% target that some nations are targeting for reopening should rather be, reach the target, and then wait 3 to 5 weeks afterwards to begin reopening. And if nations are going to be waiting that long, then they might as well just wait for eight weeks altogether, and crush the virus entirely through social distancing and further vaccinations.
But yeah, this probably isn’t going to happen. Nations will reopen despite medical advice, hoping for the best, and not preparing for the worst.