“Report back to me when, uh, I don’t know, when it makes sense.” —Burn After Reading
By Lambert Strether of Corrente
As readers know, I’m a humble Covid tape watcher. I don’t believe any of the numbers are as accurate as (say) an income statement [snort], but I have had confidence that I could discount the bullshit and at least form sufficiently useful narratives to answer questions like: Are we rising, peaking, or declining? Is my area safe? Is an area I want to travel to safe? If I get sick, what are the odds I won’t survive? For example, if Los Angeles County is a rapid riser county, it probably doesn’t make sense to fly there. And so forth. My motive is reader service (with myself as a reader). Now, however, I’m not so sure I can discount the bullshit properly, and that makes me queasy. And I’m not the only one:
In the wake of a flurry of warnings from officials over a potential COVID-19 resurgence in the United States, there are growing concerns among health experts that dwindling access to public data, the shuttering of COVID-19 testing sites and with an increasing number of people using at-home tests instead, it could leave the nation vulnerable to unforeseen upticks.
“Comprehensive case data is critical to an effective response. As we have seen throughout the pandemic, lack of data leads to poor decision making and ultimately costs lives,” Dr. John Brownstein, an epidemiologist at Boston Children’s Hospital and an ABC News contributor, said.
Worse, the CDC reform proposals seem geared to handing more power to an agency that has shown itself to be completely dysfunctional. Maybe clean house before starting a renovation?
First, I’ll quickly go through the metrics I’ve been using. (Readers are welcome to suggest new metrics, and new sources. However, I think continuity is also important. Plus, I’m aware of the new CDC dashboards, but I’m not sure their value-add goes beyond presentation, and in some cases the presentation is not that good.)
Case Count
Contra CDC and many Covid minimizers, I think case cases are the most important metric, more important than hospitalization. That’s because you can suffer vascular and neurological damage, or get Long Covid, without necessarily going to the hospital. In addition, case counts are much close to a leading indicator than hospitalization, and since Covid cases can multiply exponentially, getting as much lead time on a case explosion as possible is important. Here are the case counts for the last four weeks from the source I regularly use, 91-DIVOC:
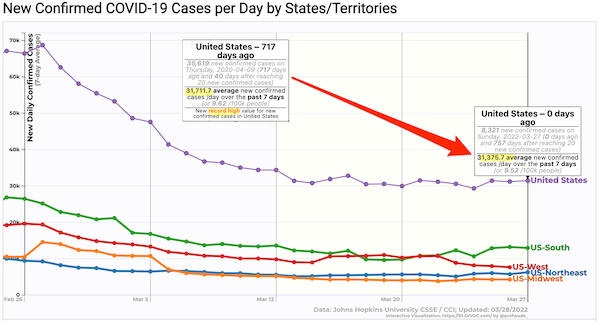
This looks mightily and flatly reassuring (as long as you’re willing to accept that the new normal of average daily cases is equal to a record high in the first peak, in April 2020. But are these numbers right, and are the case count curves really flat? Probably not:
[Researchers] found the use of the [at-home] tests more than tripled when the omicron variant was spreading rapidly, increasing from an average of 5.7 percent to more than 20 percent among people with symptoms. While test use surged, the tests weren’t used consistently across the U.S. population — it varied by race, age, income or education. For example, the researchers found that white people were approximately twice as likely to report at-home test use, compared with those who identified as Black. In addition, adults in their 30s were more likely to report at-home test use than people in their teens and 20s and those ages 75 and older. At-home test use also increased with higher levels of household income and education — people making more than $150,000 a year and those with a postgraduate degree were the most likely to report the use of at-home tests.
At home tests aren’t likely to be counted:
“Home testing leads to marked underestimates of case numbers,” Dr. Robert Wachter, chair of UC San Francisco’s Department of Medicine, said in an email. “Clearly many hundreds of thousands of people are now diagnosing themselves with positive home tests (generally plus symptoms) and these are not reported.”
Even if you do try to report your results, the information isn’t likely to move the needle on the public’s understanding of the virus. That’s because they’re not included in the data health officials use to produce their reports and policies.
So the more people test themselves at home, the less the official numbers about new infections and positivity rates (that is, the percentage of tests that detect the virus) will provide an accurate picture of the public’s health.
So the case counts are bad. How bad? We don’t know. We did have an enormous Omicron peak. We are now not nearly at peak level. But where are we? We don’t know. It makes me queasy that we don’t have this simple, basic information. I have, however, collected a number of unsettling anecdotes. Perhaps readers can supply more.
Anecdotes
Note that all these cases are closed spaces, crowded places, and close contact. So as one would expect:
Film crews:
Everyone in the film&TV industry is regularly tested, some people three times a week. NYC film crews now seeing a surge in cases. We are the canaries. Trust me, wear your mask and avoid large indoor gatherings.
— thomas Jr. 🛠 IATSE STRIKE! (@t_NYC) March 24, 2022
Game Developers Conference (GDC):
Ugh. Seeing the chatter about a lot of folks catching COVID at GDC this week is disheartening. Please do the right thing and notify the people you met closely with and use the appropriate contact tracing channels. There were a lot of maskless folks. 😔
— Shawne Benson (@shawnethegirl) March 26, 2022
School:
A month after Vermont dropped masking in schools, 6/14 counties have medium or high transmission under the new CDC community levels. Universal school masking is needed now to ensure safe and stable in-person education for all. https://t.co/HrisYtwbLJ pic.twitter.com/ZB7KjVWg2w
— Anne Sosin (@asosin) March 26, 2022
(More on “community levels” later.)
Daycare center:
So a friend of mine’s toddler got Covid at daycare – diagnosed by PCR test. The whole family (one more young child and two parents) then all got symptoms. They just assumed they all had Covid – but didn’t go for tests so didn’t report it.
Anyone else hearing similar stories?
— Kate M (@ComissionerKate) March 27, 2022
And of course my perennial bugaboo, air travel:
Oh my god
Spoke to someone (not a patient) who got a flight back home from a European country last week KNOWINGLY with Covid?!!
Just because he didn’t wanted to isolate abroad.
So now EVERY SINGLE person on that flight has been exposed & at risk?!
🤬
— Neena Jha (@DrNeenaJha) March 26, 2022
Because freedom. Sure, those are just anecdotes. But there seem to be rather a lot of them.
Waste Water
As readers know, I’ve been very enthusiastic about wastewater detection, and the CDC stood up a National Wastewater Surveillance System. Unfortunately — hold onto your hats, here, folks — CDC seems to have butchered the data collection:
The federal government paid LuminUltra, a private commercial lab, more than $6 million to assist states that couldn’t monitor sewage on their own, but the company struggled to build trust with local operators who weren’t always aware of what the federal government was trying to accomplish. Mark McIntosh, the vice president of applied services at LuminUltra, said the CDC would have gotten more for its money if it had relied on local labs instead of a large, national company….. The hope was to build a system that could identify coming Covid case surges and detect new variants. And moving forward, it could pick out other public health threats, such as growing resistance to popular antibiotics, upticks in opioid use or the appearance of a virus that could cause the next pandemic. But 18 months since the effort began, only a dozen states — California, Colorado, Illinois, Missouri, North Carolina, New York, Ohio, Rhode Island, Texas, Utah, Virginia and Wisconsin — are routinely submitting data to NWSS, according to the CDC. Even then, the information from some of those states is thin. California, which has 39 million people, has 23 collection sites on the CDC’s NWSS dashboard, most of them clustered in the Bay Area. More than half of New York’s nearly 60 sampling sites have no recent data on the dashboard, meaning the CDC doesn’t have at least two data points from the last 15 days to calculate a percentage change in viral concentration…. CDC officials believe a wastewater surveillance system can work even if all states do not participate, noting that it is designed to supplement other public health surveillance efforts — not act as a singular watchdog. “Having more sites sampling wastewater allows for a more robust national surveillance system, but we know that one of the biggest advantages of NWSS is that it gives local health officials specific, actionable information about what’s happening in their community so that they can take steps to protect the public’s health, if needed,” a CDC spokesperson said.
What a horrid example of handwaving and excuse-making from the CDC spokeshole. The system is called “National.” That’s a lie; it’s not. And that’s somehow good?
Worse, CDC butchered the dashboard it built:
8/ This pattern, where the CDC dashboard (below) indicates dramatically rising viral concentration but the state-level data do not, is happening in sampling sites across the country. pic.twitter.com/5Rs6I0s1cO
— Pandemic Prevention Institute (@PPI_Insights) March 16, 2022
First, why the discrepancy between state data and CDC’s dashboard, when the CDC’s data is supposedly derived from the state? Second, a 1000% increase isn’t especially useful, unless I know the baseline.
Hospitalization
Hospitalization — central to CDC’s horrid “community levels” metric — would seem to be relatively straightforward. After all, billing is involved. Sadly, no:
Hospital trick: patients admitted with covid in 10-12 days become post-covid & no longer counted as hospitalized covid patients. ICU is full of post-covid patients that are here for 30, 40, 50 & more days. Not counted in the official stats.
— Dr. Natalia 💉😷 (@SolNataMD) January 24, 2022
Commumity Levels
We reviewed CDC’s new community levels metric — which I shall not be using — at NC here:
The formula is stupid. The message conveyed by the “Low” (Green) level is low risk. To move the community level from Low to Medium (“Yellow”) risk, the load on hospitals must increase. But hospitalization is a lagging indicator. So there will be a window for Covid to spread while infection is increasing, but hospitaliation is not, while the level remains Green. In that window, people will not be encouraged to mask up, no community measures will be taken, and so on. Note again that people can catch Covid, avoid hospitalization, and still come down with Long Covid later. As one primary care doctor remarks:
… both justifying the relaxation of public health protections now and about justifying too little, too late policy responses in the future when surges re-emerge.
— Andrew Goldstein #EndVaccineApartheid (@AndrewMakeTweet) February 25, 2022
Personally, I’d stick with case numbers, underestimated though they are, rather than CDC’s new formula. It’s almost as if…. It’s almost as if…. CDC wants you to get sick.
Worse, CDC butchered the data when implementing its “Community Levels” metric in California:
Federal health officials who reported that nearly half of Californians live in “high-risk” counties for COVID-19 were relying on old data, and only a small number of counties now fall into that category, according to local officials.
At stake is whether counties considered high risk should keep indoor masking requirements under new guidance from the U.S. Centers for Disease Control and Prevention or follow the state’s lead in removing nearly all mask requirements..
Kamlesh Kaur, a spokesperson for the Stanislaus County Department of Public Health, said the county was surprised to be designated high risk by the CDC. The most recent COVID-19 case rate for Stanislaus County is about 13 times lower than what the CDC reported on Friday, she said.
The CDC’s estimates appear to be outdated by more than a month.
“I’m not sure when (the CDC) received their data. They are showing a little over 200 cases per 100,000 residents. Right now our cases are at 18.2 per 100,000 residents,” she said.
Deaths
From the Guardian:
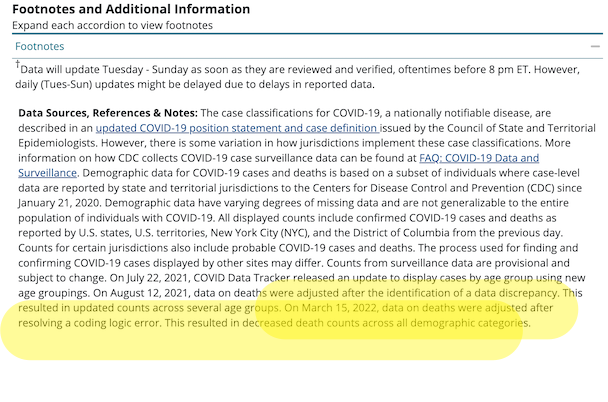
Last week, after reporting from the Guardian on mortality rates among children, the CDC corrected a “coding logic error” that had inadvertently added more than 72,000 Covid deaths of all ages to the data tracker, one of the most publicly accessible sources for Covid data.
The agency briefly noted the change in a footnote, although the note did not explain how the error occurred or how long it was in effect.
About that footnote:
Here is the footnote (you have to scroll to the bottom of the page and then open an accordion). I have helpfully highlighted the relevant portion:
The Guardian continues:
The problem stemmed from two questions the CDC asks of states and jurisdictions when they report fatalities, according to a source familiar with the issue.
One data field asks if a person died “from illness/complications of illness,” and the field next to this asks for the date of death. When the answer is yes, then the date of death should be provided.
But a problem apparently arose if a respondent included the date of death in this field even when the answer was “no” or “unknown”. The CDC’s system assumed that if a date was provided, then the “no” or “unknown” answer was an error, and the system switched the answer to “yes”.
This resulted in an overcount of deaths due to Covid in the demographic breakdown, and the error, once discovered, was corrected last week. The CDC did not answer a question on how long the coding error was in effect
Readers may wish to comment on the CDC’s coding style. Of course, what do a few tens ot thousands of deaths matter, when there are so many? However, when a coding shop commits errors like that one, you can be sure there are others just like it.
Excess Deaths
David Wallace-Wells writes on the importance of a “single metric.” That metric is excess deaths:
There is one data point that might serve as an exceptional interpretative tool, one that blinks bright through all that narrative fog: excess mortality. The idea is simple: You look at the recent past to find an average for how many people die in a given country in a typical year, count the number of people who died during the pandemic years, and subtract one from the other.
As a measure of pandemic brutality, excess mortality has its limitations — but probably fewer than the conventional data we’ve used for the last two years.
And to the extent that the ultimate impact of the pandemic isn’t just a story about COVID-19 but also one about our responses to it — lockdowns and unemployment, suspended medical care and higher rates of alcoholism and automobile accidents — excess mortality accounts for all that, too. In some places, like the U.S., excess-mortality figures are close to the official COVID data — among other things, a tribute to our medical surveillance systems.
Could there be “coding errors” in the CDC’s calcuations for excess deaths? We don’t know. One thing we do know, and I’ve been irritated about this for months:
Look at the qualifications in that drop-down. And the ginormous typo, helpfully highlighted….
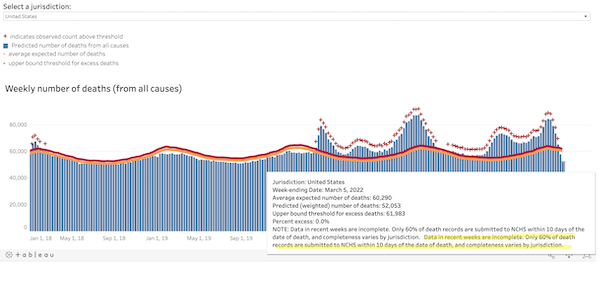
We know that CDC’s copy editing processes are slow. But this error has been present as long as I’ve been running that chart. To me, that’s a sign that nobody at CDC is looking at the excess deaths chart at all. Does that mean they’re not looking at the algorithm?
Conclusion
FiveThirtyEight reviews the history of various datatypes as they came into salience. They conclude:
For two years we’ve tried to make sense of COVID-19 trends with metrics that were fundamentally impaired by our chronically decentralized and underfunded public health system. Looking back, it’s remarkable how poorly we started, how far we’ve come and how far we still have to go. If the country doesn’t want to repeat its mistakes, it will have to take radically different actions the next time a health crisis hits.
The great and the good of public health, including Ezekiel Emmanuel — with a little help from The Blob — put together a report that proposes many such actions. Here, from “Getting to and Sustainin the Next Normal: A Roadmap for Living with COVID,” are the “Health Data Infrastructure Strategic Goals:
1. Empower and fund the CDC to rapidly develop standardized, national, real-time, comprehensive, and secure data platform(s) to monitor respiratory viruses and illnesse
2. Direct HHS to establish consistent national data standards by identifying critical metrics, defining them clearly, and establishing collection, linkage, and reporting requirements.
3. Direct HHS to financially incentivize or require real-time reporting from states, localities, health providers and at-home testtakers, to include secure and de-identified test results, vaccination status, vaccine breakthrough and re-infection status, age, sex, ethnicity, race, job, workplace, and other essential socio-demographic information.
Lol, income is not on the list? Roll on, neoliberalism!
4. Direct and fund the CDC to accelerate insight generation and provide open access to data.
5. Direct HHS and the CDC to design health infrastructure to promote health equity and mitigate racial, ethnic, occupational and gender disparities.
I have to question whether CDC — at least without a thorough housecleaning that would involve gutting the management team after forcing them to testify before Congress or, better, The Hague — is institutionally capable of achieving any of these goals, but that is a topic to go into later. However, I do want to call out something that Emanuel and crew got right. I underlined it: “Open access.” The data behind the dashboards should be open and accessible to all (and not just to hospitals or professionals). Another crew of the great and the good, writing in the Hill, has a terrific metaphor for how such a system should work:
The National Weather Service relies on a decentralized network of satellites, radar sites and local data to model and predict severe weather events. Their authority to do this does not flip on once a storm begins. Storm trackers are always on the lookout with coordinated streams of real-time data that are consolidated, analyzed and publicly shared, enabling them to alert communities and save lives. In contrast, the CDC has had to rely on uncoordinated data agreements because the agency lacks the legal authority to systematically ensure public health reporting before a health threat strikes. We wouldn’t attempt to predict severe weather like this, so why do we try to forecast the spread of deadly diseases this way?
The key is not only that the data be open, but that it would be interoperable (unlike, say, fifty states reporting data in fifty different ways (as Cory Doctorow suggests for the platforms). if the data were interoperable, citizen scientists could go to work on it, app developers could code to it, data reporters could dive into it, and so on. Much more powerful than CDC going into the dashboard business. Let a million dashboards bloom!


Nothing here.
It’s there now; an Internet outage at the worse possible time.
day care tweet is missing – duplicated the following tweet twice.
Fixed, thanks.
Literally while reading this, I received a recorded call from a state health official, urging booster shots. Nothing in the call about non-pharmaceutical interventions to slow spread. They’ve got one tool in the toolkit, and are willing to let it rip.
Exactly.
OTOH, a certain doctor is writing a book. It’s about early treatment and how it could have saved millions of people. And, yes, I know. It’s an Amazon link, but that’s the only info I have on it. Here goes:
https://www.amazon.com/dp/151077386X/
“Could Have Ended the COVID Pandemic”
Treatment is not a substitute for prevention. Is it treatment or preventative? In my interaction with Ivermectin proselytizers I get constantly shifting answers on this.
Personally I’m skeptical of any miracle solution to the pandemic, whether it be repurposed medicine or vaccines. Think it’s been pretty clear from the beginning that is going to take a layering of many different pieces, swiss cheese model, not some silver bullet.
And sorry for double posting but what’s with the past tense of “have”, does Dr Kory consider the pandemic over?
Yes, it’s fanciful crap to believe that mass Ivermectin would end the pandemic. There is no credible evidence showing this.
As GM has said, SARS2/Covid is a solved problem. There is an algorithm that has worked in quashing the contagion every time it has been used to date. It doesn’t involve ivermectin, or vaccines for that matter. But we can’t implement it in the west now because reasons.
You get shifting answers because no serious studies have been done. I agree, some skepticism is in order, but the fact that we dont know definitively if IVM could have ended the pandemic because a couple million dollars couldnt be allocated to the subject is tragic
It is surely one of the most studied drugs of the last two years. Surely that study would amount to at least couple of million?
The demonisation of it is stupid, but there is no mechanism by which Ivermectin could end the pandemic. At best it could slow it. Like the intramuscular vaccines.
Anecdote: I got a call from the NYC Health and Hospitality Dept. (?) informing me that I’m eligible for my booster shot. I told the young lady no thanks and goodbye. Now I’m wondering if I am on some kind of list, well, other than the list they already had me on. How is it they came across my info? Who is sharing this data with whom? Who is safeguarding this information? Do the boosters even help with Omni-cron? Why do I keep getting phone calls in Mandarin? A flaming shit-show on wheels…
@jr
most likely a scam, they got your phone number like they get your email, and they try to monetize it, so always ignore cold calls
if you didn’t sign up for contact ahead of time? it’s a scam
they never reach out to us deplorables to do anything other than cheat us
Health and Hospitals is actually a (huge) provider network, albeit puBlicly owned. If, perhaps, you got a shot at one of their facilities, it would be in their records. Similar to doctor’s office calling to remind you about other periodic health issues, they’re just have a bunch of hospitals and clinics.
If % positive and the total number of tests administered both go up – trouble.
One is up; other is flat – bad.
One is up; one is down – neutralish
One is flat; other is down – good news.
Both down – great news.
I use the above heuristic to get an idea of the direction. Only time it went to shit was when they changed how many cycles they run on the tests in a lab – otherwise pretty solid.
It’s a good approach, but I gave up on positivity a long time ago because, testing accuracy aside, I didn’t think we knew the number of tests, and now we really don’t know the number of tests.
I’ve been thinking a lot about this lately, as I see no one wearing masks nearly anywhere anymore in western NC.
What I’ve also been thinking about is, I don’t know how to determine risk level even with accurate case counts. Just as an example, and I realize the flu is not SARS-COV-2, I’ve never had the flu in my life, and only got a flu shot 3 or 4 years in my life and never altered any behavior when flu was spreading, while going out into heavily crowded spaces, eating out, all the usual situations you might avoid today. So what would a similar dashboard look like for the seasonal flu? Was I playing Russian roulette then? If I decided to “live my life” now, even with an accurate case count as a barometer of danger, how do you translate that into a risk assessment?
It’s impossible to ascertain what level of caution is prudent, so I go exclusively to the grocery store only and always wear an N95. Better safe than sorry. But would I be rolling a D20 or a D100000 if I decided that for myself the pandemic is over, much as the Establishment has?
I’ll feel a lot better if/when we have intranasal vaccines available.
To me the wastewater treatment data is or will have to be good enough. I am sure it could be better. We have a septic tank so people like me will never be counted, but this is what statistics is for. Insisting on counting everyone is naive. The biggest risk is that sewer sampling introduces some bias common to urban dwellers that is unrepresentative, but given what fraction are now urban in this sense, it may just be a rounding error.
The points about timeliness of hospital cases is correct but the rest is overblown. The article is mostly about lack of trust in institutions. We can see this bias in things like surrounding “coding error” in quotes. Is there any way in which this is not a plausible coding error? No. Only in the sense that design of social science questionnaires is fraught with danger because they are frequently misinterpreted by interviewees and too rigid to capture what is really going on. What this is not is a conspiracy. It’s a bungled design, and honest mistake, and no more sinister than the backhoe operator who punctures a gas line and burns down your apartment.
My advice is to stick with the data and keep the speculation, particularly the speculation involving trust, out of it until you have evidence of malfeasance.
My read on the Hospitalization section and tweet is that the amount of currently hospitalized patients because of COVID may undercounted, maybe hospitals are only supposed to report active COVID cases. I don’t think they will be missing the COVID codes upon discharge from the hospital.
jawing with nurses and doctors while i’m hanging around in san antonio, the gist is that they’ll keep wearing their masks, whether it’s required, or not.
of course, those parking lots are next to generally cancer related facilities.
i figure that healthcare people, on the ground, wearing masks into the coffee shop down the street is a pretty good indicator that it ain’t “over”.
that said, just took mom to eye doctor in kerrville….a place taken over from the hippies in the last 50 years by the worst kind of militaryesque “conservatives”.
in the office, no masks were required…and mom and i were the only one’s wearing them.
the socioplolitical nature of that town…i think…likely plays into the decision to not even speak of masks.
docs and nurses there 1, may be hyperconservative, themselves…and/or 2, not want to deal with the spittle spraying hordes when they do require masks(that’s what happened to my county government mid-2020)
when i go to the beer and cig store, i half the time fail to mask up…nobody in there, and i’m in there for under 5 minutes.
similarly, if the feed store is busy, i’ll mask up…and glare right back at them.
i don’t really go anywhere else(aside from the cancer san antone trips…masked upon entering anywhere*)
(*and, on masking on that trip…frelling public restrooms. we stop at a truck stop in Comfort, Texas, because they have immaculate restrooms.
but that said, given what i’ve known about aerisolised fecal material coincident with flush toilets, i’m more than happy to wear a mask,lol)
Thanks for the response Amfortas, I wrote a decent reply last night but messed up right at submit time…
Hope this change of topic doesn’t blind side you but have you and your wife considered FECO as a last ditch effort? Or even juicing non-decarboxilated leaves? Read good things about the chocolate tonic strain…
> It’s impossible to ascertain what level of caution is prudent
Yes, and we are simultaneously being told it’s our personal responsibility to protect ourselves. A classic double bind! Worse, those whose motives are to protect others are being systematically disempowered and vilified.
Perhaps that can be a partial guide for us about which scientists, doctors, other health-connected people to trust.
If they are vilified by agents of the mainstream Spread Covid Everywhere establishment, perhaps that is evidence that they are trustworthy for the purposes of learning some truth about covid and maybe even some ways to protect against it.
Some data points in my neck of the woods:
1) My small liberal arts college stopped requiring indoor masking on 3/16. The undergrads were away on break and return today. In the 12 days since the indoor mask mandate ended, cases among graduate and professional school students have doubled.
2) I would say masked vs unmasked at the grocery store in said college town was 70/30 with most using N95s.
3) Masks starting to reappear in some of the small shops closer to home.
I think on Saturday I had commented that most on our two research floors were masking. Today, that number has dropped quite a bit. The group next to us is no longer masking, and I just walked by an unmasked person coming from another floor to use a core facility. The undergrads came back this weekend, too. I wouldn’t be surprised if this ends being a replay of last year.
Also, a friend south of Sydney in the Illawara region has finally gotten covid. He said it’s like “a really bad flu”. For him to say that, it must be pretty bad.
Oh and they’re re-opening the gym on campus to faculty and staff on April 4th. It’s been students-only for quite some time now.
The key is not only that the data be open, but that it would be interoperable (unlike, say, fifty states reporting data in fifty different ways (as Cory Doctorow suggests for the platforms). if the data were interoperable, citizen scientists could go to work on it, app developers could code to it, data reporters could dive into it, and so on. Much more powerful than CDC going into the dashboard business. Let a million dashboards bloom!
There is nothing technically infeasible about this at all – what you’re describing is just a public API, and the CDC would theoretically be in charge of administering the databases. Here are the APIs the government already runs. You’ll notice our friends at the CDC are not represented, of course! The FDA looks like it has a decent API and promotes usage of it by the public.
Why this stuff hasn’t happened so far is probably due to political and funding reasons (see, for example, there was formerly at some point a program to get open source tech people to utilize the APIs, but this has since been archived as read only, so it isn’t being actively updated). Probably the CDC already spent all their dashboard funding on that stupid command room with the big screens and showing their useless metrics. Looked nice on the news when they interviewed Walensky tho, so that’s what is important.
I expect careerism in the bureaucracy has a second order selection preference for data selection and presentation forms that suppress bad news.
Not overt data suppression, but selection of methods and techniques that put the best face for the individual career of the individual bureaucrat on the systemic outcomes from the system resulting from the prior selection biases.
This is a governmental administrative parallel to a lethally profitable death and disease industry we call “healthcare”. “They really are trying to kill us.” It’s not personal, its a business and the government is shaping the market to ensure it’s continued contribution to GDP…until it doesn’t.
There is that. I think another factor here is just how the government thinks of and handles data in general, and where the responsibility for that lies. I’m wholly unaffiliated with the gov so my experience with them and their tech is through the lens of being a former employee of several different big tech behemoths who worked with various gov entities as a supplier. My perception was that, just like with big legacy corporations, there are very technically adept small teams within big organizations that are at the mercy of funding on an annual or bi-annual basis. These teams may be able to accomplish quite a lot if they have a well-defined project roadmap and clear definitions on what is and is not possible to do with the data, and if there are no sticky questions about that data being public. With something like health data (from a hypothetical CDC epidemiology status API) there are questions around personally identifying data, and those questions are still generally poorly-defined at the public health level as in, what consititutes PII for that data set and how can it be made programmatically available from distributed entities in the field? That requires standardization and systems for collection or enforcement, which they can build if there is the political will to answer those questions so the API can be built. Which there clearly is not. Outsourcing the wastewater data and building a fancy command center with big screens was easy and there was political will. They don’t even know how to ask the right questions to get the right answers to get to where a public health public API could be made.
> They don’t even know how to ask the right questions to get the right answers to get to where a public health public API could be made.
See my comment below; institutionally, the worker bees at CDC are incapable of advocating for this. In fact, they probably believe it’s a bad idea (“My state is special”).
The tech you’re looking for is the Fast Healthcare Interoperability Resources standard. This standard is mandated for several types of organizations in the US including medicaid and health plans, and is of interest to many other organizations. Google has teams building tools to make it easier to implement, for example, because they want health companies paying for their hosted healthcare apis. But ‘easier’ is relative, and the standard comes with tools for comparing different uses for a reason… and it still doesn’t solve at-home tests.
Ah, HL7. I was hoping somebody would mention it. It doesn’t seem like there are many implementations, sadly. But perhaps with Google’s muscle behind it?
Speaking as someone doing the FHIR work, I don’t know if I would rely on that wikipedia article for much. For example, Epic supports FHIR and the Interoperability and Patient Access final rule (CMS-9115-F) is a real thing, so the US has picked this standard and is moving towards it. But ‘easier’ is still very very relative.
> Probably the CDC already spent all their dashboard funding on that stupid command room with the big screens and showing their useless metrics
I should make fun of that.
Perhaps somebody with actual experience at the CDC — surely we have somebody in the readership? — can correct me, but this is how I envision case data handling at the CDC:
There are, say, fifty cubes (headcount 50), one for each state. (Perhaps the cubes are by regions, I don’t know). Each cube has the responsibility for the data in its jurisdiction (California, Idaho, the Midwest, whatever). The jurisdiction sends its data to the proper cube, whether electronically, by mail, by fax, by phone, or some mixture of all of these. The cube dweller then aggregates the data, possibly communicating back to the jurisdiction for clarification and correction. The cube dweller also fills in any gaps algorithmically. The cube dweller also converts whatever data format their jurisdiction is using to the standard data format used by CDC, and sends it up the line to be aggregated with the work product of all the other jurisdictions, from where it is distributed to CDC’s customers, displayed on dashboards, and so on.
Notice:
1) Inputs from jurisdictions are not standardized. “Normalization” happens in the cubes
2) Personal relations between jurisdiction and cube matter
3) Integration of processes across cubes is very difficult since each cube has its own methodology.
In short, the system doesn’t scale and is very difficult to change.
Further, you can see from the spokeshole’s remarks that CDC not only believes this is how things are done, it’s how things ought to be done.
but this is how I envision case data handling at the CDC:
Based on my interaction with gov entities I think the data handling is probably more like:
– the office or team that handles this data is much smaller, less than 20 people (call this the ‘CDC data team’);
– they have a rudimentary system of automated data collection, possibly part of another, bigger CDC data collection program, that includes a database with various siloes/tables/lakes just for this team’s use;
– each state or region or hospital or whoever has agreements to report into the CDC’s data collection system already (possibly due to prior agreements on other various gov programs, like VA inclusion), and those entities, which probably constitute less than 30% total of hospital or patient care centers, already had some form of automated data collection and sharing to this CDC database prior to the pandemic;
– adding new entities into this automated collection system is time-consuming, because every entity has their own idea about what data should go in for collection. the CDC data team does not have time to handle this, so they plead for administrators who take over your ‘cube’ role defined above;
– CDC financial administration – the people who approved the command center and big screens – see the cube workers and the data team as cost line items. The understand expenses like buying a big screen or a dashboard creation software subscription that relies on an underlying database. They have sales guys from Tableau and Salesforce trying to call them weekly to talk about what their software can do for the CDC during the pandemic. The have sales guys from wastewater sampling calling and offering the same. Sometime in mid 2021, when it became clear that Hot Vaxx Summer was a dud, the CDC admin signs off on expenses to create the command center and the dashboard creation software as a ‘fair compromise’ between fully overhauling the CDC data collection process and outsourcing the entire thing. To do otherwise would mean hiring a much larger data team, figuring out the database infrastructure requirements (more money! more time!), possibly hiring a software development team, and who knows what would happen to the cube workers… How could administration possibly justify that to (whoever they report to)?
So yes, CDC delenda est, but we’re solidly in Il Gattopardo territory here, where the only way for ‘things to remain the same’ (CDC still has credibility for public health) then ‘everything must change’ (if you’re gonna rely on data to make decisions better make the data infra , collection and systems are up to the task, otherwise they’re subordinate to petty office concerns).
All of them will be reporting using some mutant species of Microsoft Excel or CSV, because “standard software that we happen to have” is what “standardisation” means in practice.
For each data source, someone like me then writes a “data adapter”, in Python, that picks out the data and cleans it up as best one can into a “standardised CSV”, and maybe even logs some of the errors that can be detected, then spools it off to some cloudy URI, where other stuff picks it up.
Eventually someone manually goes through the import failures into the $Big Legacy System and then we have our data. Then the interminable haggling starts over licensing and communications stuff, about using data and getting it out again.
Finally a web page displays some coloured blobs. Nobody knows what they mean, which means that “communications” properly did their actual job of rolling the turd in glitter!
Oh, and, Logistics works very much in the same way!
> Probably the CDC already spent all their dashboard funding on that stupid command room with the big screens and showing their useless metrics
I should make fun of that.
Perhaps somebody with actual experience at the CDC — surely we have somebody in the readership? — can correct me, but this is how I envision case data handling at the CDC:
There are, say, fifty cubes (headcount 50), one for each state. (Perhaps the cubes are by regions, I don’t know). Each cube has the responsibility for the data in its jurisdiction (California, Idaho, the Midwest, whatever). The jurisdiction sends its data to the proper cube, whether electronically, by mail, by fax, by phone, or some mixture of all of these. The cube dweller then aggregates the data, possibly communicating back to the jurisdiction for clarification and correction. The cube dweller also fills in any gaps algorithmically. The cube dweller also converts whatever data format their jurisdiction is using to the standard data format used by CDC, and sends it up the line to be aggregated with the work product of all the other jurisdictions, from where it is distributed to CDC’s customers, displayed on dashboards, and so on.
Notice:
1) Inputs from jurisdictions are not standardized. “Normalization” happens in the cubes
2) Personal relations between jurisdiction and cube matter
3) Integration of processes across cubes is very difficult since each cube has its own methodology.
In short, the system doesn’t scale and is very difficult to change.
Further, you can see from the spokeshole’s remarks that CDC not only believes this is how things are done, it’s how things ought to be done.
I thought you meant cube as in data cube
I could imagine the cube dwellers wandering forever in the Escheresque landscape of malformed statistical data. Sad cube dwellers!
Lambert, you’ve got the air travel tweet twice, but no daycare tweet.
Lambert, this post is absolutely terrifying. Not only does no one have an idea what is actually going on, everyone is going to act as if nothing is going on because warm fuzzy and the shitstorm of disinfo and the NYT didn’t tell me to brush my teeth today so I ain’t gonna take the precautionary step. Dr. Wen should be in prison too, I’m truly sick of her smug, professional “smile”. Is there any clearer sign of a degenerate society than prostituted doctors?
Unlike liberal headline writers, I don’t write to get “terrify” in the headline (and another thing to be terrified of, and then another, and so on). If fear were not adaptive, it would not have arisen in nature. If you hear a twig snap behind you in the jungle — anecdotally! –it’s rational to feel fear. The question is how to convert the fear into motion and action and, one hopes, safety. I think step one is to think carefully before following the CDC’s advice on anything.
To be clear, I wasn’t being accusatory, just declaiming to the gods. Nor do I think you were being intentionally provocative. I appreciate the “straight, no chaser” approach to the truth NC serves up and as always I appreciate your hard work.
I used to share this quote with my students all the time – and I will share it now with everyone here – it is a very simple quote – but is absolutely true –
‘When a doctor does go wrong, he is the first of criminals. He has the nerve and he has the knowledge.’
Sherlock Holmes
The Adventure of the Speckled Band
Sir Arthur Conan Doyle
The Strand Magazine
February 1892
Thanks for this Doc and all your good work here. I seem to recall an old black and white film from years ago in which a bunch of young med students were goofing about in a class. The professor shut them down harshly and if I recall one got a bit wise.
The professor then demanded the student pick a term from the textbook. He did so and the professor immediately recited the definition and treatment from memory. He then addressed the whole class and reminded them that they are one of the few people in society who have the ability to kill someone and not pay any price or something to that effect.
An anecdote from the biography of Richard Burton comes to mind (a ripping read btw). An MD was trying to take the piss out of him at a dinner party, asking “So, Burton, how do you feel after you’ve killed a man?”
“Quite jolly, Doctor,” came the immediate reply, “how about yourself?”
Paging Dr. Shipman – with an estimated body count of 250 victims-
https://en.wikipedia.org/wiki/Harold_Shipman
Thanks for all your hard work, Doc. Even here in the Southern Antipodes it is appreciated.
I can practically feel the anxiety floating off the NC pages. I don’t think it’s helping anyone. Try the following breathing practices. They cut right through the fear and build lung and immune system capacity.
Pranayama breathing is quite easy to master and very invigorating: https://www.doyogawithme.com/content/pranayama-wake
This is an amazing breathing technique that is rather hard to do at first but is excellent: It feels almost like a Bene Gesserit “Fear is the mind-killer” exercise. https://www.youtube.com/watch?v=0BNejY1e9ik&t=650s
I’m working up to doing both exercises twice daily first thing in the AM along with my workout routine, and then in the PM before bed. Also be sure to practice breathing through your nose rather than your mouth at all times. Your nose is an awesome filtration device and naturally cleans, warms and humidifies the air you breath. Try reading Breath: The New Science of a Lost Art by James Nestor. Trust your own body more and help it grow stronger every day. Yoga stretches for the shoulders and chest also help you open your lungs and your heart. Do Yoga with Me has many excellent short videos that you can do throughout the day, even at your desk. Peace.
My breathing practice is masking up and avoiding sharing air when possible, especially by breathing outside air. When indoors, I use a CO2 meter.
But thank you for psychologizing a systemic problem! It’s the American way.
Oh come on, Lambert. Knowing that our gov and agencies et al are corrupt as hell doesn’t mean you can’t protect yourself as much as possible. A mask is not enough. Breathing practice is not psychology it’s physiology. Just try it.
How DARE you talk down to Lambert. Even worse, just repeating an attempt to censor the site shit-coated in insulting New Age pandering.
And it’s misinformation.
I will not tolerate it.
There is ZERO evidence that “breathing practice” reduces the odds of contracting a pathogen.
And a fitted N95 mask does, to an enormous degree.
Stop selling snake oil at the expense of approaches that make a huge difference.
It can help reduce stress, however
Breath is important and one doesn’t need to new age it
> A mask is not enough
Yes, a layered strategy is important (I gave some examples in my response).
I’m certainly open to the idea that breathing practice is protective. I’m not opposed to any placebo effects provided by amulets, prayers to the Virgin, incense, or Eastern religious practices; however, absent evidence, it’s all just woo woo.
I suspect you’ve posted this in the past, but what CO2 meter have you been using?
Aranet4.
Thanks!
I’ve been noticing the same thing. Anxiety floating off the NC pages.
How do I handle it? Well, I just go out into the world and live my life. Yeah, I do carry a mask that I can put on if I’m going to be inside for a while, but that’s about it.
Life’s too short. Let’s enjoy the time we have here.
Me too now, spent last two years keeping small circle of friends. Then got covid from double/triple vaxxed company. My doctor thankfully previously gave me a script for you know what (got another one for next time) and came away with hopefully no further complications. I have to say I feel much more safer now that I have natural immunity. Hope it lasts.
You should never be thankful for getting Covid. Every time you get it, it imposes a cost on your body.
Would you rather be anxious and take precautions or relaxed and have suffered permanent Covid damage due to being cavalier?
I see this as a false choice.
As an analogue, I cycle daily. It is well established that wearing head protection greatly reduces head injuries if you have a bad accident. Still, I’m not wearing one. Not because I consider myself cavalier, but because I consider the risk of that head injury small enough that it is not worth the inconvenience of the helmet to me.
For Covid I’m pretty much in the same boat. I consider the risk of getting hospitalized or long Covid to be low enough that I don’t really worry about it. Yes, I can be unlucky, so be it. I won’t let that fear dictate my life.
Having said that, I don’t oppose all kinds of Covid measures and will mostly follow them. But to me the important metric is the hospitalization rate. As long as the health system can easily cope, I see no strong reason for severe measures. And I’m well aware that can easily change if a more severe variant arises, but we’ll cross that bridge if and when that occurs. No need to worry about that now.
Of course that risk assessment is personal. If you consider that risk high enough to go that extra mile on protection yourself, I will respect that. Just as I respect people who do wear a helmet while cycling. But for me that is a personal choice. With Covid my choice unfortunately will impact yours, but that is where the government regulations come in. They more or less represent the community choices, which I will respect.
First, you are incorrect in your risk assessment. Getting Covid is not a one-shot deal. Immunity from infection lasts only six months or so, and often much less with Omicron (many reports of reinfection a mere month after the first).
The more often you get it, the more damage to your body, and greater risk of bad outcomes, particularly cancer. IM Doc says he and other MDs are seeing a marked rise in cancers. There’s one type of thyroid cancer, for instance, where he had seen only 2 cases in his prior 30 years. He knows of eight cases personally in the past year.
Second, if you think damage to your heart or your lungs or your brain is no biggie, there’e no reasoning with you because your position, despite your claims of rationality, is profoundly illogical. You are a textbook case of hyperbolic discounting that economists call hyperbolic discounting, greatly undervaluing future costs and benefits. Your are ignoring risk that could put you in a hospital or have you permanently impaired not that far down the road, say after 2-3 Covid cases, because you’d rather have a good time now.
And your mis-assessment of risk does impose costs on all of us via higher health care costs.
On the point of risk, you are confusing two types of risk – personal and societal.
If you don’t wear a bike helmet you are (arguably, I’m not going down that rabbit hole), increasing your personal risk of being injured or killed.
But thats not the same type of risk as, for example, riding your bike very fast through pedestrian crossings without stopping. Doing that you are putting yourself at risk – and you are also putting innocent pedestrians at a similar risk of injury or death. This is why in most countries wearing a bike helmet is a personal choice, while cycling recklessly through a pedestrian crossing is illegal.
With covid, there is no ‘personal’ risk. If you get it, you are putting other people at risk. This is why only a holistic public health approach makes sense. But instead, we are transferring the responsibility to individuals. Its as if we allowed drivers to drive at whatever speed they chose, and drink as much alcohol as they wanted, so long as they put on their seat belt.
Used to cycle everywhere in hilly, scary, drunked-up Pittsburgh. Wore a REAL helmet; best friend, died at 52, said it lowered his reaction time? Hit icy streetcar tracks in heavy tracks & THREW myself abruptly at the curb. The semi tractor behind me stopped with a first aid kit. He’d thanked me profusely for keeping him from swerving, as some idiot coming at us had accelerated across the double yellow unknown to me. I was embarrassed but fine. My helmet’s remains were aroun d my neck. Maskless churls make it EASY for us to AVOID narcissistic suck-up hive-minded sociopaths.
As things now stand, the best therapeutic that still works is Paxlovid. Using the website, https://covid-19-therapeutics-locator-dhhs.hub.arcgis.com/, there are few doses available in my area. Plenty of Sotrovimab, now completely useless against Ba2, and Molnupiravir, also not particularly effective. Prophylactic antibody, Evusheld, available here and there, but restricted to narrowly defined high risk groups. I guess it’s just me, my P-100 respirator, and solitary habits against Moloch and the machinery of the night. Fortunately, I am retired and therefore, America, I will not be putting my cisgender shoulder to your mthrphking wheel. Apologies to Allen Ginsberg.
Funny you should mention this. I’ve been wondering about US case counts as well after noticing an anomaly in Covid case numbers and the Covid death rate on the dashboards (sourced by Google from NY Times).
The latest spike in deaths peaked around 4 Feb, at a rolling average of approx. 2500/day. This lags the peak in cases for Omicron by a bit over two weeks, which sounds reasonable. Rolling average of new cases was approaching 1 million/day at the peak, so this translates to a death rate somewhere around 0.25% – kind of high for a ‘mild’ illness, but not wildly out of line with expectations for Omicron (and given all the well-documented issues with US health care, it seems credible to me).
Case numbers started declining steeply at the end of Jan, dropping below 100k per day by mid-Feb and continuing to fall. Death rates, meanwhile, are also falling, but by nowhere near the same magnitude, and are still quite high more than a month after the end of the big Omicron peak. At present the rolling average is sitting not much below 1k/day, which if you compare to case numbers about 2-3 weeks prior amounts to a mortality rate of around 3% if accurate, which seems awfully high.
Looking back, it seems we see this pattern every time there’s a dip in case counts, although not to quite the same extent. I’m not sure what’s causing it. I remember Denmark said that high death rates were a data anomaly – basically, Covid was so prevalent that people dying from normal causes often happened to have had recent Covid infections and were therefore counted as Covid deaths. It could well be something like that, or it could be that during low infection periods it’s mostly the vulnerable and immunocompromised who suffer and mortality really is higher. Or it could be that cases are being systematically undercounted and the death rate is closer to the true story (but if so you’d need an explanation for why that wasn’t happening at the peaks). Looking at excess deaths might help resolve this question, but as you say the CDC chart hardly inspires trust in the data.
> Looking back, it seems we see this pattern every time there’s a dip in case counts, although not to quite the same extent
The distribution of “time to mortality after diagnosis” may have a fat tail; after a surge in cases, that would keep the death counts elevated above what a baseline lagged CFR calculation would suggest based on new cases. There is mention in Lambert’s post of patients lingering weeks in ICU; many of these may not be recovering.
I have wondered if that may be the issue. At one point I looked for a graph of the time between diagnosis or hospitalization and death but never located one.
I don’t doubt that’s a factor, but how much of one is hard to say without better data. It’s certainly one possible explanation, I agree.
Assuming the fat tail is proportional over time, then it may be possible to use the excess deaths vs the case count with a comparison between multiple peaks of different widths to determine the tail shape.
I’ve said for a long time that cases were way under counted. Just like one of the twitter threads noted, one person gets covid symptoms and gets a positive PCR test.
His or her close contacts get covid symptoms and just stay home. Unless they need a test for “official” reasons or they get sick enough to go to the doctor. their cases aren’t counted. I saw this multiple times last year before home tests were available.
Now with the home tests, it is even more true. During the omicron surge, my cousins family all got covid. No official tests at all, just home tests. They all stayed home from work/school according to the guidelines but their cases are invisible from a government perspective.
There are quite a few papers coming out now that argues that a Covid-19 infection does “bump” various “natural causes”, for example heart and circulatory system problems, in any population, and even after “mild” cases (paywalled).
My totally unscientific theory based mostly on my own personal experience with 2x Covid-19 is that this disease Ages people. One “simply” ages about 3-5 years. Every time one gets it, the “permissive action links” for cancer, type 2 diabetes, liver problems, respiratory issues, and circulatory system problems moves a few steps closer to their “open” position. With enough ageing, wrong kind of genetics and so on, “Natural Causes” kicks in and one becomes another statistic.
But, this could happen a long time after the initial infection, the papers so far talk about “increased risks of X up to a year after Covid-19” which is kinda what they have data for also, so it could turn out to be “Forever”.
I think what we will eventually see in Denmark will be a dramatic (2-5%) rise in what are called “lifestyle diseases”, across all age groups, and that the effect will be large enough to shorten the average life-time expectancy.
Still, this will not be bad enough to improve ventilation is schools or hospitals, that was identified and consequences documented as a problem in 2009. I only hope China will do better when we flame out!
Great summary, Lambert. Two years ago at this time I was nearly ready to buy tickets to head east in early June to take two grandkids on a backpacking trip in Vermont, but my gut told me this damn covid thing was rising fast and by June we’d be in the horrors, so I cancelled the trip, heard a few tut-tuts from relatives, but then by June realized I had done the only proper thing. I was then, and still am, very uneasy in an airplane and have avoided any since covid began. So now covid is over, they say, or some say. I am vaxxed and boosted, healthy, have not had it unless totally without symptoms, and my wife and I have lain low. Last week for the first time in two years we went to a gathering in someone’s house, all vaxxed people, her colleagues, very nice, but then we both collapsed for two days because the social interaction so exhausted us.
So this spring I have been considering heading east again, there is an outdoor athletic event back east (rowing) which my oldest friend’s high school crew he coaches is competing in, a hot crew by the way, and I desperately want to go watch him and his girls, plus then going on to see those grandchildren near Boston. Yet, at almost exactly the same time, reading the tea leaves, the China lockdowns, the rises in Europe, the rising curves of cases here in the US with this new version despite the home testing data skew Lambert mentions, I think to myself, do I want to get in airplanes to fly across the country in mid May? Am I thinking of not taking this trip because of a real and reasonable concern about this version of covid or am I using this as an excuse to not travel at all because I have reached the age where the airport experience is close to death? Am I a wuss? Or am I being smart, as I would argue I was two years ago?
So I sent a note to my rowing friend, who himself had covid a couple weeks ago (vaxxed) and had relatively minor symptoms, and I asked him, am I a wuss, and he said, “I’d say you are smart.”
This old dog is going to sit tight right now, plan nothing, and see what happens, as he did two years ago.
no shame in it being both.
over the last 17 years, i’ve shamelessly used my disability to get out of long trips to see people, and other social type things.
because i’m at root a hermit…but nobody accepts that excuse.
for the long trips…it really does hurt like a b&^ch, and i’ll take a week to recover from the 700 mile round trip drive to houston and back.
for the local stuff…well…i’m a hermit, don’t like crowds even sans covid,and generally lay down by 6pm.
if you feel you must avoid stressful situations(i haven’t even driven close to an airport in 30 years), and the counterparty won’t accept “well, that really harshes my mellow…”…then by all means…plead covid.
similar to the breathing advice, above…such exercises are good for anxiety and hyperstress.
use every tool in the box.
> “I’d say you are smart.”
Hopefully
Count me among the frustrated and queasy. I’m an executive director for an arts non-profit with galleries and performance space. Never stopped our mask mandate since we opened back up in July 2020 and fully publicized it to both protect our staff/volunteers and provide cover for other businesses to do the same. When fully closed for the Omicron spike this winter, we came up with a guideline for being fully open, limited opening with masks and capacity caps, and fully closed. Still haven’t opened up the theater yet except for a few isolated events during very low COVID times. NC has been a huge help in finding and interpreting data.
Unfortunately our tiers were based on the 7-day average county-level data from the CDC and roughly tracked with the old categories for community transmission. Now that page still has the color coding of old, but the 7-day data on cases and positivity rate seem to be missing. I assume the next step will be to change the whole country to the “low” color. Finding it hard to fight the good fight, and the performing artists are champing at the bit….
Well, here we are. No preventative measures from a societal perspective (mask mandates gone, very little improvements in ventilation, air filtration etc indoor spaces). All we got are vaccines and for the very sick or very wealthy, Paxlovid – if you get diagnosed quickly! It’s all about money imo. The current system is very profitable and illness is profitable too. So a little covid-19 is fine with those paying our representatives bills. 1 million deaths, life expectancy dropping a few years to 74 for men, and by 3 to 5 years for people of color – no big deal! In the “before times” a drop in life expectancy of 0.1 years was considered a big deal. I bet the drop for the wealthy has been much less of course.
Anecdotally, masks are out of style pretty much everywhere. However, I’ve seen a bit of a rise in better quality masks among physicians. It’s not just about masks though – the zeitgeist has changed. Concern is on the wane, most want to not hear anything about covid. Don’t ask don’t tell as they say. To me this makes any data in the USA highly suspect unless it is something like waste water that is not dependent on much other than people using the toilet, which seems likely not to change?
Luckily “flu season” aka airborne disease spread season is mostly over in N. America for this season. BA2 however, is some say, 50% more infectious than Omicron, so that could overcome people being more outdoors in the Spring than Winter. In some parts of the country, we should expect a repeat of the past few Summers – TX, FL, both had surges in cases in the Summers with heat and people staying indoors in air conditioning. Likely we’ll see a surge there this Summer with BA2, but only in wastewater, excess deaths and maybe a bump up in hospitalizations?
Likely there will be a new worse variant (as in able to out-compete BA2) by Fall 2022. If we are lucky, we’ll have a new nasal vaccine before the Fall. Otherwise we likely will see at least another few hundred thousand deaths through the next year.
Personally, I will try to keep my N95 masking on indoors in public as much as possible, ventilating the house, filtering the air and avoiding large crowds.
I’ve much appreciated the info found here at naked capitalism on covid in general and filter boxes, etc. in particular. Big help!
I had a good run – no Covid, no colds, no flu since March 2020.
In the last 2 months I *mostly* used masks and distancing.
You can see where this is going.
It was in the office I stopped wearing masks – and I’ve going in twice a week since January 2022.
Saturday I got a dry cough and runny nose.
Sunday the rest of the head cold symptoms showed up, in force.
Took the home test. Positive for Covid.
Today I dragged myself through the CVS drive-through to get tested and be part of the case counts.
Turns out I’m a precautionary tale. Ugh.
You must not have been doing your Yoga….
That was so mean, Lambert … just dug my yoga mat from the back of the closet to ROFL.
Lambert, no offense but you’re pussy footing around the issue. There’s a time to call a spade a spade and this strikes me as one of those times. Basically, the data doesn’t seem to be trustworthy. Act like it isn’t!
So what would you do different if the data were good, mask up? Well, you’re masking up regardless, right? So it doesn’t matter what kind of hokum they’re spreading because you, like me, and everybody else, has to take responsibility for protecting yourself. After all, you, and you alone are responsible for you. Like I am responsible for me. Point being, I mask up 100% when I go out.
Note; if I anticipate being in a high risk place I hork before I go and and I hork my nasal cavities upon return, 100% of the time – no exceptions. High risk places, by the way, being defined by me as the doctor’s office, or anywhere I am going to be confined with others.
Finally, I’ve mentioned before the nasal lavage bottles sold by amazon for <$10. I use one of these to hork out my nasal cavities with a saline solution consisting of 3tbsp of non-iodized salt, 20cc of 7.5% Betadine, mixed in a 2L bottle. This mixture resembles the color of tea (not as dark as a Coca Cola, and more brown like tea).
Oh, and I simply don't go out unless I absolutely have to. Haven't been to a restaurant in more than two years. We were spending well over $1000/month on just this activity. No longer. Haven't had a professional haircut during this period, either. My wife or daughter do the best they can for me, and do each other. Sad for these business, but it is what it is.
Interestingly, I was chatting with a pal in Shenzhen and they went through 9-day lockdown last week. As it happens, I think President Xi has been wise to force a lockdown because this lets them get their ducks in a row, test as much as needed, and and because everybody is isolated, then those who get sick call for help but aren't spreading it. I honestly wish we had politicians with the stones to do the same. Maybe then we wouldn't be looking at 1M deaths in America. Of course we're such independent cusses it would never work because, freedoms.
Anyway, I'm definitely not a proponent of let 'er rip.
> hork
Word of the day!
When owls regurgitate the undigestible bits of the food they’ve eaten that’s commonly referred to as “horking” with the pellets from their crops called “hork balls”.
Here’s a photo of a horking owl
On the vein of statistics, here in BC there is data out on the period from Aug/1-Oct/31 2021. This comes from stats Canada.
Excess deaths over 2140
Covid deaths 430
Opioid deaths approximately 600
This leaves another 1100 unexplained deaths over a 3 month period in a population of around 5 million. In the same period the excess death rate of under 40’s was 67% above average. The opioid deaths may be part of long term average as this problem has been here for a few years.
If I was paranoiac, I might think the reason for sending out those home tests is to look like you actually care, while helping to hide the true number of cases because that means fewer people will take the public tests or report their own. Win-win. Then there is the serial faulty reporting and while I am not some specialist, or even that smart, if the company I worked for had put me in charge of similar reporting, say on damage on a type of shipping container, such incompetence would have made them asked if I was either stupid, on drugs, or working for someone else. Pen, paper, ask questions, call, write, and hire whoever was needed, then review and test the program and/or report for however long it took using every possible problem people could think of.
I understand that one should usually ascribe to incompetence, instead of malice, bad actions such as this. However, this is so goofy, I have to ask if they are stupid, using drugs, or have some other goal besides accurate record keeping and reporting needed to protect the public?
This reminds me of the creative ways that statistics in homicides, particularly by the police, and gun use in general have collected and analyzed by everyone; the police do not want it know just how lethal they are and that those they kill deserve it, and both the pro gun and anti gun factions believe winning the struggle rather than the truth is important.
This means everything from not reporting the murders to just lying or being creative in the analysis, often using true facts and numbers to lie about the truth. And it is not just about gun homicides as police department sometimes bump any crime up or down in seriousness to make themselves look good or on funding issues. Rape becomes assault. Murder becomes manslaughter, first degree manslaughter becomes second degree or the other way around. Then there are all those rape kits everywhere in the country that are never tested. Lies about the victims, the perpetrators, and history in general to support their positions with all sides doing manipulations like this. It makes studying the issue difficult especially as I am not a statistician. It does make studying crime in the United States interesting.
It is not necessarily a mass conspiracy, but just small groups and individuals who collective actions sometimes make just small nudges become big lies. Perhaps it is just that too many people think that manipulating facts, or feelings, somehow makes what they want to believe true. Maybe, they believe that propaganda convincing others of something makes it true, regardless of the consequences outside of the believer’s mind. Or some people are just lying and sabotaging everything in the hope Covid goes away? Because money?
i’ve been in the “ascribe it to malice” camp since feb. 2020.
we’re not “citizens”.
we’re not even really “customers” any more.
we’re a herd to be managed and exploited.
ergo, be that goat….the one that always finds the hole in the fence.
I guess being the ornery goat is better than the lamb sent to slaughter. Certainly better than being the customer ready for shearing and perhaps further “processing.”
It would be nice though to be considered American citizens or even(!) human beings again instead of feedstock for Soylent Green. :-(
Humans are varied, we
(are encouraged)should think ourselves as livestock, valued as exploitabe,unvalued as collateral.Thanks as always, Lambert!
Truly horrid stuff from this country’s rancid leadership.
From my late night doom scrolling – turns out our neighbors to the north aren’t much better (via Twitter).
Neolibs straight up “sticking to the plan” …
• By vax alone shall you …
• It’s “mild”
• Isolate for five days – this is the killer IMO … contributes most to sick people spreading
• No “scarlet letter” mask for you … a close second to the above
• Get back to work and the “new normal”
NY state and city looks like their rises are on for real now. I’ve wondered how The UK could be so bad, yet no one’s talking about travel restrictions from there. How many cases per day did South Africa have when travel was cut off?
:: heads over to Flip-the-script ::
LOL
When travel was banned from South Africa to US because of Omicron (11/26/2021), South Africa had a 3,863 cases per day weekly average, or just about 7-persons/100K when normalized for population. On that very same date, the UK was at 48,672 cases per day weekly average, or around 69-persons/100K when normalized for population. Today, the UK is at almost 108K/day average or around 163-persons/100K. Yet the flights keep coming into JFK and many other points east and beyond. As we saw in the tweet above, people are obviously getting on planes sick despite all the PCR requirements. #{DEITY} help us. We’re on our freakin’ own, here.
Canada’s health care system was, amazingly, even more aersosol-hostile than our own. Worse, some infection control droplet goons had important positions at WHO, and blocked aerosol transmission from there.
https://people.com/health/covid-infection-increases-the-risk-of-developing-diabetes-multiple-studies-find/
Isn’t life just great?
>>>As we saw in the tweet above, people are obviously getting on planes sick despite all the PCR requirements.
That is the most disturbing thing of the post. Individuals who know that they have COVID, but prefer to be sick at home because it is more comfortable for them.“I have the Plague, but I really don’t mind exposing and murdering people for my convenience.”