Yves here. On the one hand, it’s a step in the right direction to see some policy thinkers grappling with the issue of aging and the rising need for long-term care. On the other hand, the thinking is still blinkered. First, it’s fuzzy at best on the fact that some elderly people can still get by at home with part-time care (it talks about different levels of need but it’s not clear if these are all within institutional settings or not). Of course, they might live longer that way. Second, there are also community options that could be integrated with part-time care. For instance, in Italy, one town I visited briefly had what amounted to a day-time elder care center, a sitting room with a TV, hot and cold drinks, light snacks, reading material, game boards, and a nice view. It looked comfy and the door was open, so I suspected they also welcomed people from the ‘hood stopping by to visit if they had the time and inclination.
I suspect it was designed just like child day care, for working families that had an elderly parent at home and were worried about leaving them alone all day…or maybe the older relative was extroverted and wanted to be out with other people.
Third, however, this post fails to acknowledge that proper long-term care violates Lambert’s second rule of neoliberalism: “Die faster!” The US discovered with the advent of long-term care insurance that funding an industry of retirement centers did keep older people healthier and therefore living longer.
Fourth, it does not consider the impact of long Covid on disability and therefore long-term care demand. It’s not hard to imagine a lot of people will either stop working earlier than expected and/or will have to go to part-time work.
By Rainer Kotschy, Postdoctoral Research Fellow, Harvard T.H. Chan School of Public Health and David Bloom, Clarence James Gamble Professor of Economics and Demography, Harvard T.H. Chan School of Public Health. Originally published at VoxEU
Declining fertility rates and longer life expectancies are producing an ageing global population. This column investigates the challenges that rapidly ageing societies pose to systems of long-term care. To avoid shortages in the workforce, the long-term care industry should endeavour to improve working conditions while also recruiting workers from a larger pool. Investing in disability prevention and rehabilitation are also promising avenues to absorb pressure from growing long-term care needs.
Declining fertility rates, increases in life expectancy, and the progression of large-sized cohorts into older age are driving rapid population ageing globally. In developed and emerging countries, this phenomenon – among myriad health and economic concerns – will raise disability prevalence in the population and dramatically increase the need for long-term care (LTC). Combined with a reduction in informal care (driven by the erosion of traditional family structures) and the widely varying coverage of public social security benefits and private insurance, “most developed countries” will see “a growing dependence on long-term care to provide post-acute care following a hospital stay” (Costa-i-Font et al. 2017). An ageing populace that increases demands on public healthcare systems while simultaneously reducing the number of contributors to said systems exacerbates these challenges.
Figure 1 Population ageing in selected countries
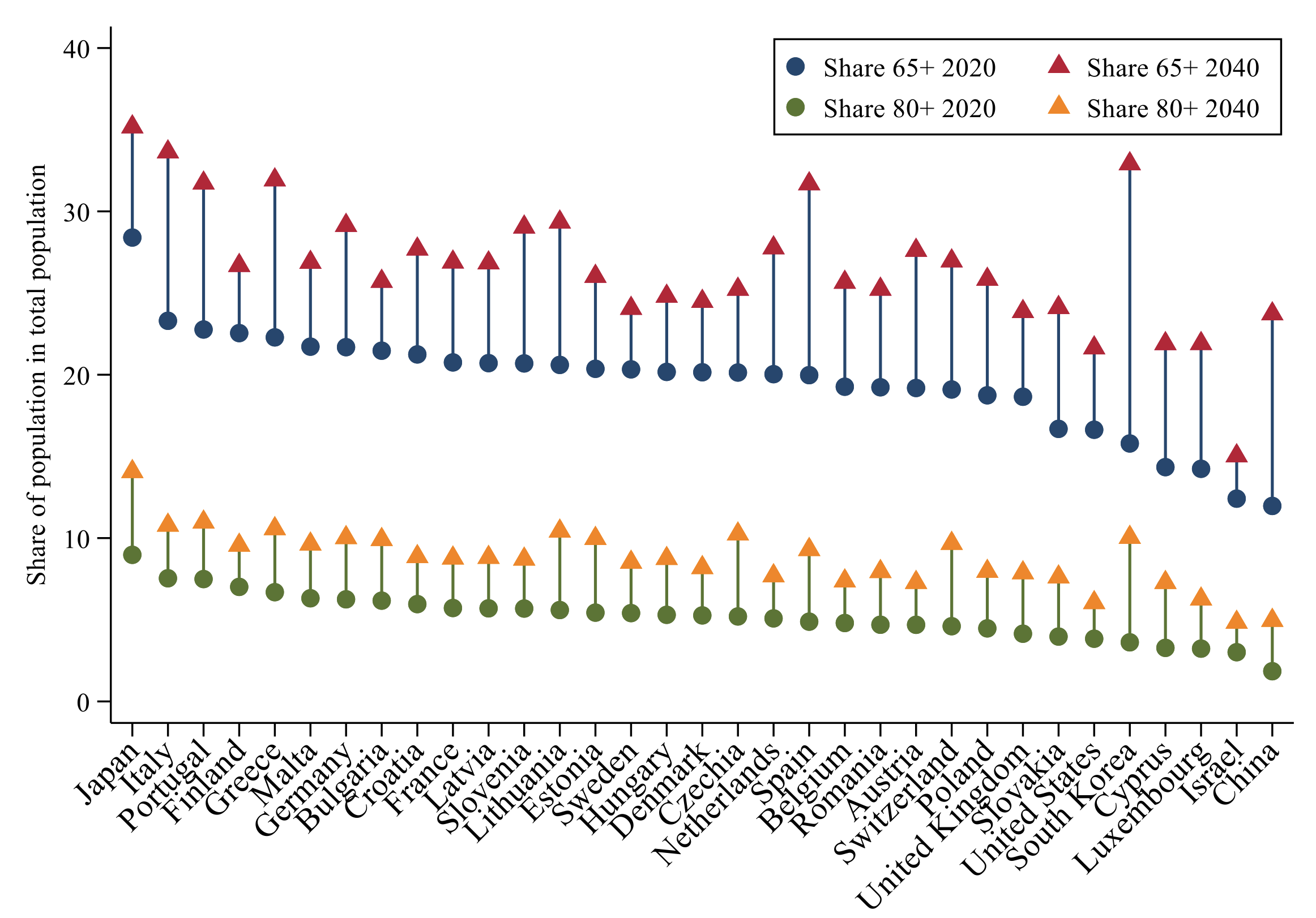
Note: The figure depicts in % the share of persons aged 65+ and 80+ in the total population. All displayed countries are ageing, but the speed of ageing differs considerably across these countries.
Source: authors’ calculations, see Kotschy and Bloom (2022) for details and data sources.
Existing healthcare structures are not designed to meet recipients’ long-term care needs and are ill-equipped for the looming surge in demand. Some countries have implemented social long-term care insurance to facilitate their citizens’ access to adequate care. However, even those systems face considerable challenges in light of population ageing, thus requiring extensive policy reform. Japan, for example, introduced a Long-term Care Insurance Program in 2000; by 2011, long-term care expenditures had doubled from four to eight trillion yen, with government projections forecasting a continued increase to 20 trillion yen by 2025 (Shimizutani 2013). Addressing these challenges by reforming care policy is particularly tricky because measuring informal care has historically been difficult, and because previous reform attempts prove that informal care decisions are sensitive to government subsidies (Costa-i-Font 2018, Barczyk and Kredler 2018). Specifically, when formal care is subsidised but the policy does not anticipate citizens taking advantage of these subsidies, LTC markets will be overwhelmed while informal care converts to formal care. Therefore, reform-minded policymakers must be knowledgeable about the long-term care needs of their constituents, highlighting the importance of health and retirement surveys. To that end, we employed the U.S. Health and Retirement Study and two of its harmonised sister studies – the Survey of Health, Aging and Retirement in Europe, and the English Longitudinal Study of Ageing – to determine the share of ‘frail elderly’, defined as those aged 65+ and those aged 80+ who have at least two limitations in their activities of daily living (ADL) or instrumental activities of daily living (IADL).
Figure 2 Share of elderly with disabilities in selected countries
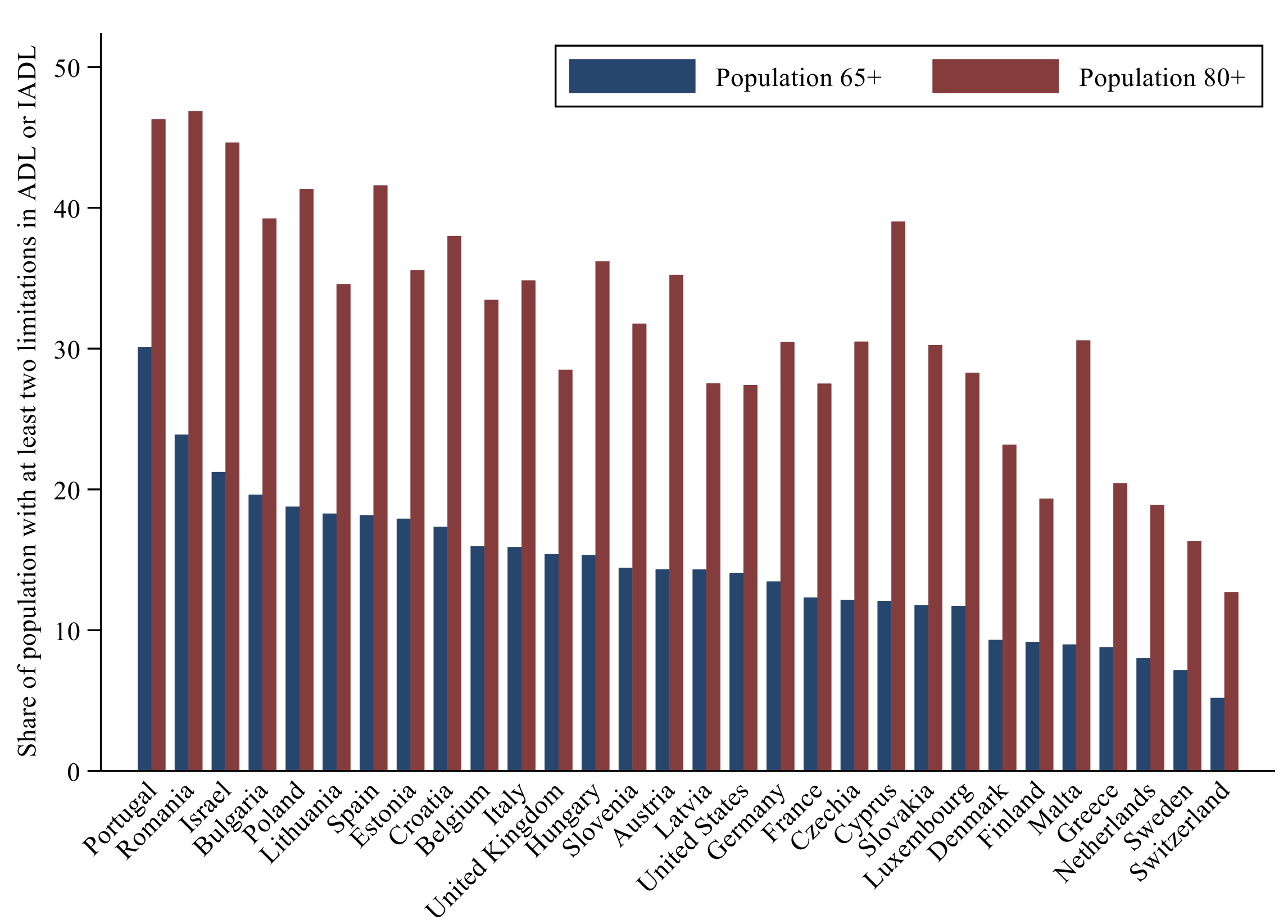
Note: The figure depicts the share in % of persons aged 65+ and 80+ with at least two limitations in ADL or IADL. Values for the United Kingdom refer to England. The figure shows that countries differ considerably with respect to disability burden and that this burden increases significantly with age.
Source: authors’ calculations, see Kotschy and Bloom (2022) for details and data sources.
Examining 30 developed countries, we found that 14.5% of those aged 65+ have two or more limitations in ADL or IADL, which increases to 31.7% for those aged 80+ (Kotschy and Bloom 2022). While these developments are worldwide concerns, the trends display considerable heterogeneity across countries: Southern and Eastern Europe, for example, are ageing very quickly and have a substantial associated disability prevalence among the elderly. Combining projections of demographic composition with the disability share roughly approximates prospective care demand. This projection exercise suggests an increase in care demand of 47%, ranging from 33% to 75% across countries (Kotschy and Bloom 2022).
Figure 3 Projected demand for long-term care in selected countries
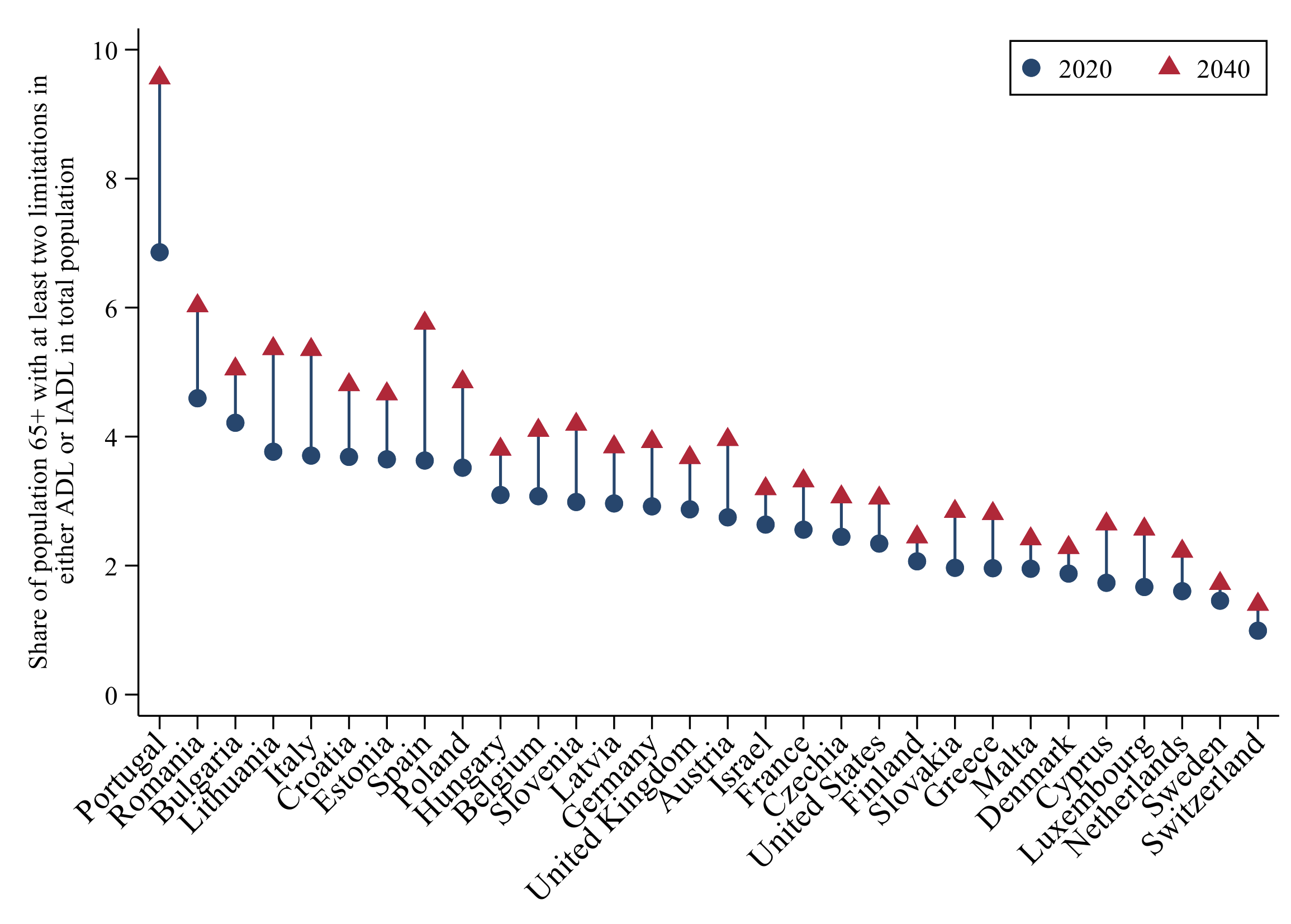
Note: The figure shows the projected increase in care demand, as measured by the share of the population composed of persons aged 65+ with at least two limitations in ADL or IADL in %. The figure reveals considerable differences in this increase, depending on the speed of ageing and the prevalence of disability among the elderly.
Source: authors’ calculations, see Kotschy and Bloom (2022) for details and data sources.
Ageing-Related Challenges for the Supply, Quality, and Costs of Care
Beyond the question of how governments and consumers will pay for increasing long-term care needs is the simple question of whether supply will be sufficient to meet the burgeoning demand. While the number of care workers increased in roughly half of OECD member states between 2011 and 2016, that growth has kept pace with ageing in only a few countries (OECD 2019). To avoid shortages in the long-term care workforce, the industry should endeavour to improve working conditions (offering better pay, enhanced career advancement trajectories, and the use of respite care to provide temporary relief for primary caregivers) while also recruiting workers from a larger pool, including the specific targeting of training for the unemployed, for foreign workers, and for men, who are typically underrepresented in the field. Some countries have made strides in these domains. Germany, for example, has launched policies to improve working conditions and is attracting foreign workers through international collaborations with its Federal Employment Agency (Federal Ministry of Health 2021). Japan has channelled unemployed workers to the long-term care sector, helping the country add 320,000 care workers in a five-year period (OECD 2020). And in Israel, more than half of the long-term care workforce was born elsewhere (Asiskovitch 2013). Unsurprisingly, these countries are among the few where care worker staffing has kept up with the pace of ageing.
The field might suffer growing pains during this workforce expansion if the quality of care suffers for reasons that include the lowering of educational requirements and the scarcity of competition. Potential solutions include licensing professional care workers, as they do in South Korea, or regulating the tasks that care workers can perform, as they do in Israel (OECD 2020). Germany, Israel, Japan, the Netherlands, and South Korea have enhanced training and mentoring programmes to improve long-term care workers’ education (OECD 2020). In addition, Germany has emphasised geriatric training in its nursing curricula. While competition among suppliers is theoretically a boon to curb costs and secure quality, it likely has modest beneficial effects because effective competition is limited in the context of ageing, where demand outpaces supply (see Yang et al. 2021 for a literature review).
If the long-term care workforce does not grow fast enough, informal care must assume most of the care, which can reduce labour supply as friends and family forgo employment to provide care. This development can inadvertently counteract policies that promote female participation in the workplace, as women typically provide most informal care. Policymakers should be encouraged to pursue potential relief measures designed to reduce the economic burden for informal caregivers, such as supporting direct cash payments from recipients and providing social security contributions.
Population ageing also imperils access to adequate care, as it increases the demand for cognitive, dementia, and psychological services. Current benefit assessments and eligibility requirements do not necessarily reflect the heterogeneity in disability and likely overemphasise physical functioning. Some long-term care systems have implemented different care levels based on physical, mental, and cognitive functioning, with a focus on differentiation with respect to care needs. In Japan, beneficiaries are sorted into one of five care levels; in the Netherlands, they receive benefits based on care needs that are organised by functional domains (Joshua 2017). Because equity is an important component of access, long-term care systems should include means-testing or social support for the least affluent to provide equitable access to care. One feature the aforementioned countries share is compulsory long-term care insurance, financed by payroll contributions (Germany and Israel) or by a combination of payroll contributions and taxes (Japan, the Netherlands, and South Korea). As access to care is codified as a legal right motivated by the concept of human dignity (e.g. Nordenfelt 2004), governments might face legal and ethical challenges if they fail to provide universal access to care.
Finally, reform attempts inevitably encounter a trade-off between care quality and costs, often rooted in policies designed to determine eligibility criteria: deciding whether to grant benefits to more beneficiaries or to grant more benefits per person. More efficient service provision is essential to containing costs of the growing use of LTC services. This approach can be addressed through market power, as in Israel, or by decentralising service delivery and putting provision in the hands of local municipalities, as in the Netherlands (Hasson and Dagan Buzaglo 2019, Maarse and Jeurissen 2016). Integrating general healthcare and LTC services, such as aligning admission criteria for LTC facilities and hospitals, could address service gaps and overlaps.
Policy Implications
Population ageing will increase the demand for long-term care. Investing in disability prevention and rehabilitation are promising avenues to promote wellbeing and to absorb pressure from growing long-term care needs. Such initiatives are not quick fixes, but implementing them could create the necessary momentum to address health challenges. The more successful the prevention efforts, the lower the cost and the demand for LTC services, with increased individual wellbeing conferring benefits that could reverberate throughout the health and economic landscapes (Bloom et al. 2018). While most of the countries investigated for this study support rehabilitation programmes, robust prevention initiatives are rare; Japan is an exception, having implemented a preventive strategy at the community level while emphasising community activities and meeting places that can foster the personal autonomy of an ageing populace (Yamada and Arai 2020). Germany and the Netherlands, meanwhile, aim to promote telecare and the redesign of living environments to encourage healthy, independent ageing (European Commission 2019).
As the Figure 4 shows, prevention efforts to reduce the burden of disability still constitute a small portion of health expenditures. However, prevention efforts – along with boosting rehabilitation spending, bolstering LTC worker recruitment, enhancing LTC efficiency, and ensuring equity of access – could mitigate the effects of an ageing population and provide fiscal relief for stressed LTC systems. A stronger emphasis on illness prevention in reform agendas seems highly desirable.
Figure 4 Preventive care spending by government and compulsory schemes as a share of national health expenditures in 2018
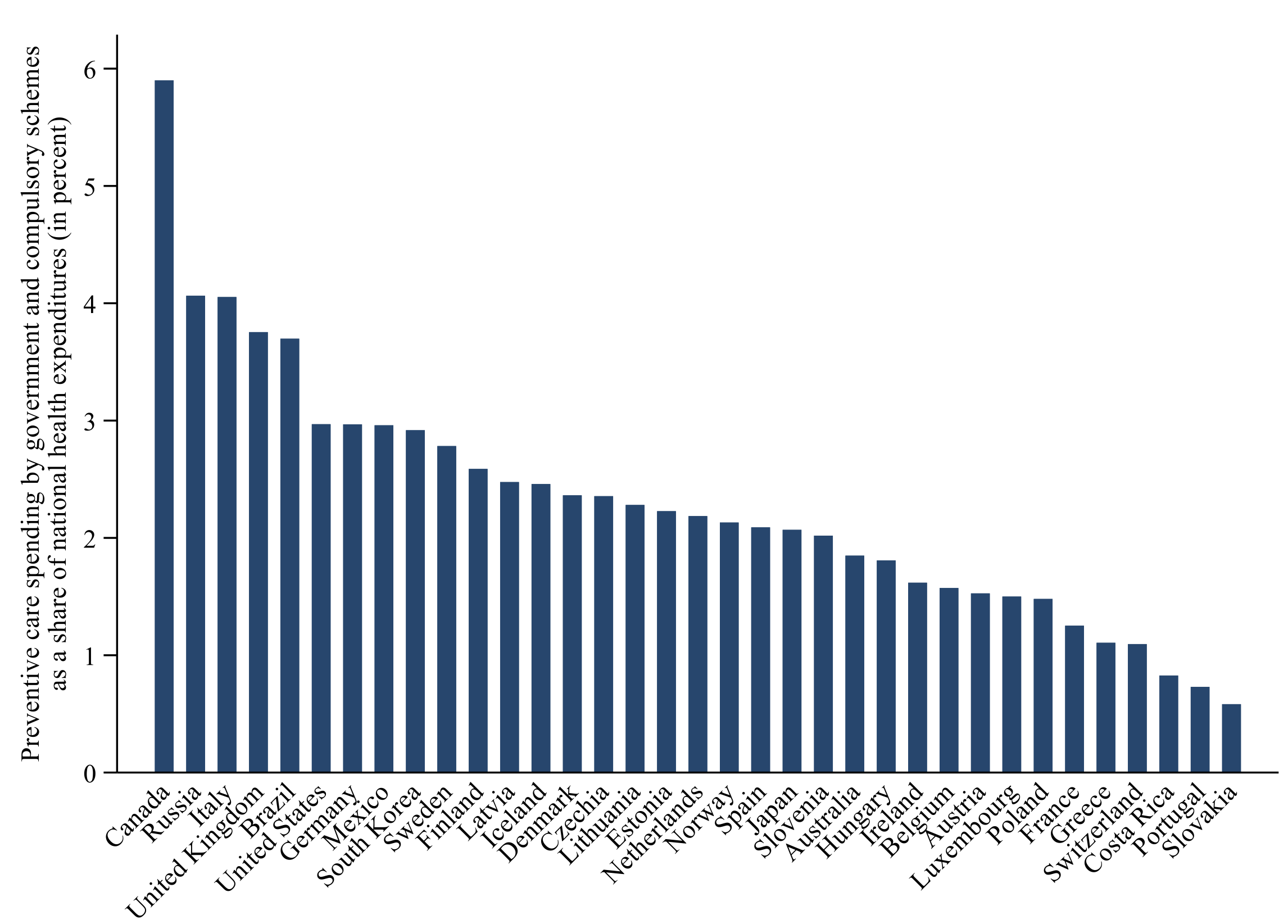
Note: The figure shows that preventive care spending amounts to only a small portion of national health expenditures, ranging between 1% and 3% in most countries.
Data source: OECD.Stat (OECD 2022), extracted on 27 April.
See original post for references


Don’t forget long covid, with likely massive influx of (younger) dementia patients.
Indeed, funding this from the private sector for profit is a challenge. The LTC market is troubled.
This ought to be a universal benefit, along with dental and vision…
https://www.forbes.com/sites/howardgleckman/2019/04/01/another-shock-to-the-long-term-care-insurance-industry/?sh=4446bf00385e
“Spare me the bullshit of mental illness,”
says guy who just approved $40 billion war fund
Sea to shining sea, this open air mental hospital.
Every Kingdom of Raytheonistan worker could be allocated to elderly care for a zero net impact. But caring for a semi-mobile octogenarian with mild dementia would certainly be a problem for someone who’s entire day is spent torqueing screws to mount widgets to chasses. Righty-tighty, click, wash rinse repeat, check please.
IIRC, in The Deficit Myth chapter discussing the Job Guarantee and full employment fiscal policy, Prof. Kelton mentions long-term care as one of the things that a JG program could fund, that the private sector is not able to do well on its own.
Me thinks that between the ‘greying of America’ dynamic and the incapacitation or debilitation of a portion of the working population through long COVID, we are going to see a significant work force shortage overlapping with the growing need for LTC.
—-
A somewhat snarky thought arises, that the food price inflation and shortages may actually help with “disability reduction”. How? There seems to be (in my observation, admittedly a very narrow field of view) growing interest in at-home food production. If home gardening becomes a thing again (as it was during the world wars — the “Victory gardens”), it will probably have beneficial effects on population physical fitness. A sibling who has interacted with many elderly patients tells me that the centenarians among them were all gardeners earlier in life. It seems to be beneficial for preserving functional strength, which is important in avoiding debility and reducing fall risk in the elderly.
It has mental health benefits, too.
To the spades!
I can envision a system of one person monitoring ten or twenty folks remotely and interacting as appropriate. I was watching a show on NHK yesterday about “influencers” in China and that as many as 500 million people there are interacting regularly on their phones with them.
https://www3.nhk.or.jp/nhkworld/en/ondemand/video/2022319/
I am looking at a site called ElliQ, which calls itself the “sidekick for healthier, happier aging”. It looks like a Siri type service custom tailored for older adults.
https://elliq.com/
Add to that all of the people with early onset dementia due to covid.
We definitely have the wrong mindset to address the problem of aging. But I honestly cannot imagine what the “right” mindset should be in this absurd country. Warm, dry, clean, comfortable, entertainment optional, properly diagnosed and medicated, properly fed, rolled out into the sun on a nice day. Achieving all that basic comfort for a cranky old cadaver who regularly poops her pants is very labor intensive. And who hates labor? The United States hates labor. Yet, somehow it just isn’t profitable enough to design good robotics and facilities. In fact, nobody wants to think about it. Charlie Munger says it best: Show me the incentive and I’ll show you the result. So sex and money are probably out – what else is there?
What else? Fear of get’n changed by a robot? Fine tuning such a machine would be a task commensurate to teaching drones not to shoot friendlies (impossible?). Talk about clocked hrs Pubs wouldn’t want to shell out for. And then there would be the supply chains needed to keep the contraptions functional. But I’m hoping you didn’t mean all this.
Recognize the fear, + mass movement demanding labor intensive. They’re more like pushing incentives rather than pulling…I’ll stick with these.
I think we have the storyline for a blockbuster black comedy.
I know the phenomena a little [I said “a little”], so right now the whole picture’s ticking me off too much. If I knew you, you might write a line, and I’d just say, “Yep.”
You hit on the CRUX OF EVERYTHING (thanks), but I think robotics is a vain hope. In fact, I know it is.
Have you heard Kate Willet saying why she doesn’t date 23 yr olds? I don’t know what to bring in here from developmental psych, but I’ll tell you about me. In 7th grade I got exposed to hard jobs, dairy was one [this was 60s]. Though I thought it was an abrupt exposure then, considering my whole life, actually it was a gradual exposure, so I was luckeee (that’s one key to it all, gradual). Humans need the challenges; that seems to be the upshot of everything…as much as I wish human labor was so little necessary that govs might just buy guitars for all those not stimulated enough by trimming chickens or bolting on widgets 20 hrs a week (just check out robotics at “chicken place” if you wanna get freaked out).
DiEM25 & Progressive International with all their ideas have failed to see the jabs weren’t saviors [better vetted ones might have helped; heck, these might have helped some but the evidence doesn’t look good]. Cuomo & the nursing homes–that was where Progressive Int should have taken the cue, and conceived an entire plan of change. But I guess folks in the homes weren’t young enough to count. No, we need a CCC of nurses. It’s unbelievable those orgs are so removed from nursing homes they didn’t make that episode the fulcrum…that and the dud jabs, what worse double whammy outrage could anyone expect? Like you more or less point out though, it would be difficult to say, “Go back and learn how to work,” but maybe if there are enough blackouts out west people will get away from the screens, and the realization’ll dawn on’em.
We’ll need that CCC when the next bad ass variant comes round [needed one by 2020 actually]. How do you convince the MICIMATT in DC? Dunno; they’re about as far into some la la land out past the foreground of what’s in the looking glass as you can get.
Helloooooh MICIMATT. Get your butt back here.
This should have been the key issue where “labor intensive” suddenly made sense to everyone again. And from there people would have seen it makes sense in all kinds of businesses. Things are reversed. Possession of the phones cheap is the be all and end all. Try to go conquer China with China-Yeltsins to get those phones! Has the nation lost its mind?? No, the real imperative is provide jobs that maintain quality of life.
As a low-income 76-year-old, I look at long term care with horror. It will be one thing if I’m allowed an in-home nurse to visit and house help on my fixed Medicare income. It will be quite another if the state decides to institutionalize me in what have been repeatedly found to be low quality Medicare Nursing Homes. At the thought of being tranquilized and backhanded if I get out of line, I have already prepared the prerequisites for a gentle exit prior to that decision.
Due to the horrific hoops I’ve had to jump through maneuvering through our health insurance, oops, ‘care’ system, I’m under no illusion that the U.S. will do jack squat for people like me.
Living the Dream in the Shining City on The Hill !!!
I am in the same river, my boat is upstream a few bends. If it is any consolation, there are many of us facing these facts. I think Covid brought much of it into focus for most of us that are awake (Woke or not). 12 inches from our noses.
I concur with your observations about ‘our’ government by, of, and for the people doing absolutely nothing for any of the least among us.
I wish you more than your fair share of peace, grace, and not-bitter solace.
I am so so sorry.
This. I have just spent 5 weeks navigating the medical and rehab ( nursing home) systems due to a post vaccine septic kidney. It’s not worth it.
Ana in Sacramento
I’m sorry to hear that, Ana, and completely understand. In 2002 I had a terminal cancer diagnosis. (Yay! I beat the odds.) But as I navigated my way through the byzantine halls of hospitals and clinics, I used to say to myself, ‘Feet on twelve, liver on three, ears, eyes and throat in Building C, Suite 400 …’
We are treated as parts, each one a vein of plunder for one specialist or another, no matter how thin or, oops, pyrite. Meanwhile the low-paid aides and CNAs upon whom we truly depend can be surly or merely sullen. That’s why when a truly compassionate aide appears, people start talking about ‘angels.’
At least now, after more than 50 years of advocating for single payer, when I tell a doctor our health insurance – oops, care – system is a cl*&^#$k they nod their heads and agree.
Small comfort.
We need open source 3D printer plans for devices that people can assemble and use themselves to end their lives humanely when they choose. I’m not talking about those big pods, either. Something small that can gradually replace air with CO or nitrogen.
Recently read a very interesting call to arms on elderly care in Canada:
Neglected No More, The Urgent Need to Improve the Lives of Canada’s Elders in the Wake of a Pandemic
by Andre Picard
Apparently NY, CA, and some of the better USA states are 4 fold worse shape than Ontario, so I shudder to think about what the rest of the USA is like now, much less where it’s going with over 50% of Americans with no real savings.
Switzerland has a program started around 2015 that sounds interesting. https://www.zeitvorsorge.ch/ . You spend time caring for elderly and “store” that “time” in a “bank”. When you need care, others will spend time caring for you. (I don’t know German to understand videos, so only read translated webpages). While a lot of details of this nascent program need to be worked out, it is a non-financial solution that may be better-suited for this financialized world.
Given the declining birth rates and rapid aging of the population this sounds like a ponzi scheme.. unless immigration is drastically increased — which would be a solution to most of the problems associated with the dwindling labor force as the current population ages
Nobody in the Anglosphere [including the usually omniscient NC commentariat] seems to pay any attention to the fundamental source of the long-term aging care problem.
Age stratification! Which starts in elementary school and perpetuates until the end people’s of days. For an interesting explanation of this in in Western society, I highly recommend Wednesday Martin’s Primates of Park Avenue.
Anybody who has lived in the “developing” [towards what, I might ask] world in a multigenerational family setting finds the whole Anglospherical approach to aging and old people ludicrous to the point of insanity.
Agree, I’ve had 3 grandparents in retirement homes and I have zero desire to go there. If I’m not surrounded by family, I’ll clock out when I can’t take care of myself.
A big red flag in the article: the uncertainty whether supply will meet demand! “Demand” in economic terms means “entity (person or corp) with willingness and ability to pay”. But when most people read demand, they just think about the human need for support. If we could reduce the need for expensive care by encouraging communities and long term relationships with people and place, and also reward labor more than capital owners, there’s be plenty to go around. But with so many people desperate for work, I guarantee those with cash will find supply of labor.
There are so many old people with so much to give.. I feel so sad every time I go into a retirement facility. Both for the old people and the young.
My father recently died of Covid, among other things, he had a number of health issues including kidney failure. He was taking care of my mother who is 83 who has moderate dementia while living in an assisted living facility. With a bit of help from the facility this was a relatively low cost way to go. The problem is that three months in he died. To this day my mother thinks he is still alive and waits for him.
So my brothers and I have her in memory care in a city on the west coast. Not one of the most expensive cities by any means. I’m an accountant and I’ve calculated the cost of care for her expected lifespan to be north of 800k before we talk about any other medical issues. Fortunately they sold their home last year so they have the proceeds of that and a 400k LTC policy which is paying now or would be paying if the facility would fill out the damn forms without me having to prod them. Now I can’t believe that the average American has anywhere near this amount of assets, or the foresight to have a LTC policy, assuming the insurer doesn’t go bust. No wonder so many quit there jobs and take their family members in.
My brothers both travel constantly, or are overseas for their jobs, so they can’t. I would have liked to try home care for as long as possible. I was planning on retiring by now, but that went out the window when my wife’s job was sent to China and I’ve been killing myself to make the lost income back up for the last decade. So there we are.
p.s. For those that think they will exit early, and I’m one of them, purely to save the family money, if you have dementia or Alzheimers, it’s very unlikely you will have the facilities to do this, or even realize you are impaired. It’s tragic.
Very similar with my father, who got dead last September. We’d been estranged, when Covid hit the assisted community they were in degraded, so he reached out. My stepmum has early Alzheimers, plus some meds that make here sweeter, and I promised him I’d take care of her. He bought a house a couple of blocks away.
So Janet & I are there twice a day, which we’re good with. It’s an anchor point in a tempestuous world. What makes it work is taking the perspective that we are here to
Love and Be Loved.
Which is lacking from industrial health care. When Janet became a Nurse-Manager at a nursing home, they were under sanction from JCAHO. She got it better by doing things like buying cushioning to decrease bedsores. As soon as the sanctions lifted, they fired her and put in a drunk who cut the expenditures, and executive bonuses ticked up. Marginal revolution, cyclic misery.
“For those that think they will exit early, and I’m one of them, purely to save the family money, if you have dementia or Alzheimers, it’s very unlikely you will have the facilities to do this, or even realize you are impaired. It’s tragic.”
It’s truly a farce, isn’t it! I live in Washington state which has a Death with Dignity law. The best I can hope for is a) die in my sleep or b) get diagnosed with something that will take me out within 6 months so I can choose the date.
And all of this horror is only and solely due to MONEY. What a crap civilization.
Yes, life and death have been monetized in this country. Your only value is what can be extracted from you, which is the tragedy of for profit, market based health care in this country. And one that I’m most frustrated with, as I can choose not to consume on many levels, but I’m getting older and despite making reasonably good choices, your body gives up as you get older and you are stuck dealing with the system, which again, see my first sentence.
But surely covid is effectively a way to reduce that growing future demand?