Yves here. KLG discusses an important new paper in the BMJ publication, the Journal of Medical Ethics, on Covid-19 vaccine mandates. It comes down against them for a host of reasons, including risk of net expected harm for some populations, questionable net public health benefit based on vaccines not reducing transmission of current variants, and “lack of reciprocity,” meaning effective inability of anyone harmed by the vaccines to recover monetary damages. It also highlights that coercion can produce a loss of trust in public institutions and other vaccines.
I hope you will circulate this article widely.
By KLG, who has held research and academic positions in three US medical schools since 1995 and is currently Professor of Biochemistry and Associate Dean. He has performed and directed research on protein structure, function, and evolution; cell adhesion and motility; the mechanism of viral fusion proteins; and assembly of the vertebrate heart. He has served on national review panels of both public and private funding agencies, and his research and that of his students has been funded by the American Heart Association, American Cancer Society, and National Institutes of Health

Board, Ernest; Vaccination: Dr Jenner Performing His First Vaccination, 1796 ; Wellcome Library; http://www.artuk.org/artworks/vaccination-dr-jenner-performing-his-first-vaccination-1796-125729
The story of Edward Jenner and his invention of the smallpox vaccine has been a fascination of mine since I saw an illustration based on the painting above, which represents the first vaccination of a child (James Phipps) against smallpox, in The Golden Book Encyclopedia my parents bought for my siblings and me a long time ago. Ours was not a house full of books, but these were there, soon to be followed by the 1965 edition of the World Book Encyclopedia.
At about the same time I was obsessively re-visiting the story of Dr. Jenner, I received my smallpox vaccination. If memory serves, I remember getting this shot from a school nurse in the first or second grade, each class lined up trying to be brave at the sight of those rows of sparkling glass syringes on the table (The TB skin test was even worse, perhaps because it was easier to watch the needle pierce the skin of your forearm!). My reaction to the smallpox vaccine produced a large, dark scab and then left a scar on my upper arm that those of us of a certain age remember well. But we were in no danger of smallpox thereafter.
The same is true for polio, which was still very much a frightening possibility at the time. My family lined up with the entire local community at my elementary school to receive the Sabin oral polio vaccine, administered as a blue/purple spot on a sugar cube. I was recently talking to a long-time friend about this. She remembers the identical experience at her elementary school on the other side of town and told me she wanted to ask for another sugar cube.
Notwithstanding the recent controversy over the completely manufactured link between the MMR vaccine and autism, vaccines have prevented millions of deaths from smallpox and countless cases of polio, diphtheria, pertussis (whooping cough), and tetanus (DPT vaccine), with few associated injuries. These diseases could be terrifying to my parents’ generation and those who came before them. Newer vaccines against chicken pox and human papilloma virus (HPV) will prevent millions of cases of disease associated with these common viruses. Like many of my contemporaries, I have had measles, which meant two weeks in a darkened room with no television as a first grader.[1] I was told I also had the German measles (rubella), but I do not remember that. I do remember the chicken pox and mumps, however. But I never had to worry about stepping on the proverbial rusty nail and getting tetanus, because when that inevitably happened I got a tetanus shot. More recently I had a recent bout with an HPV-related illness that was unpleasant but has turned out well. So far. All things considered, I would rather have had the vaccines. They work!
So, when the world was confronted with the news of an epidemic of severe respiratory disease in China in late 2019, a vaccine was the natural response to SARS-CoV-2 and what was later named COVID-19. Operation Warp Speed was a remarkable effort that led to the availability and widespread use of the Pfizer/BioNTech and Moderna mRNA-based vaccines and the Johnson & Johnson/Janssen adenovirus-based vaccine.
Unlike the vaccines for the former childhood diseases of my youth, these vaccines have been a disappointment. They prevent neither systemic disease caused by SARS-CoV-2 or transmission of the virus from one infected person to another. There is evidence they lessen the severity of disease in some COVID patients.
But as the original SARS-CoV-2, sometimes referred to as “wild-type,” has evolved through a series of variants, the basic concept of a vaccine against SARS-CoV-2 has become “problematic.” Although virologists, and especially Big Agriculture with its (immoral) CAFOs (Confined Animal Feeding Operations), have known for a long time that lasting immunity to coronaviruses is difficult to attain, either through previous infection or vaccination, this simple fact has not become more widely understood during the current pandemic.
To a first approximation, RNA viruses such as those in Family Coronaviridae evolve rapidly because replication of RNA genomes is more error prone than DNA genomes and these errors provide the raw material for evolution (defined here as random variation followed by selection for variants that replicate faster or in different tissues, for example).
Nevertheless, we have what we have, and most of us have gotten the two “jabs” of one or the other available mRNA vaccines. Whether what has been primarily an all-vaccine-all-the-time strategy is the correct path to end the pandemic is an outstanding question for another time.
A pressing question for now is whether subsequent “boosters” beyond two shots should be required. Which brings us to today’s subject, provided in an open-access paper published recently in the Journal of Medical Ethics (BMJ) by Kevin Bardosh and colleagues: COVID-19 vaccine boosters for young adults: a risk benefit assessment and ethical analysis of mandate policies at universities (pdf).
Yes, this paper concentrates on booster mandates for young adults who are attending college, but it also illuminates where we are currently in the biomedical and social responses to the COVID-19 pandemic and what we as a society should be thinking about as we move forward through a pandemic that, despite rhetoric to the contrary, is not over.
What follows is a series of highlights from this paper, which I encourage those so inclined to read. Although the terminology gets thick at times, the data presented are clear and the rationale for the authors’ conclusions are straightforward. The bibliography is also extensive and most of the papers are freely available (at least those I consulted). I have included several block quotes and a figure that cannot be adequately summarized otherwise, hopefully not in violation of fair use. It should also be noted that institutional requirements regarding COVID-19 vaccination and boosters remain a work in progress as new information becomes available, but this does not detract from the overall message of the study.
COVID-19 booster shots have been controversial from the beginning of the current vaccination regime for the good and simple reason that a required series of boosters is not within the common experience of a society that by and large has come to appreciate the importance of vaccination to public health, notwithstanding yearly flu shots that are chosen ahead of time to work against the expected variants of influenza virus in the upcoming flu season.
Moreover, regarding COVID-19, as noted above the vaccines have not worked as we have come to expect of vaccines. They prevent neither disease nor transmission, and while they are said to reduce severity of disease, it is not entirely clear that better patient outcomes are not due to improved clinical management as healthcare providers have learned how to better care for these patients. The coming COVID wave, if it arrives as feared, may answer some of these questions.
According to this paper, COVID-19 booster mandates for young adults/university students have been controversial primarily because of a lack of clear evidence that:
(1) Boosters provide a meaningful reduction in risk of hospitalization in healthy adolescents and young adults, and
(2)Previous infection confers significant protection against hospitalization due to re-infection (up to 64% of young adults have circulating SARS-CoV-2 antibodies)
It is also true that young people in general are not as likely to experience severe outcomes upon infection with SARS-CoV-2. This, however, does not rule out sequelae to infection such as systemic organ damage and what has become known as long COVID. Perhaps the most important aspect of these mandates for a population in which the risk-benefit calculus is not well established is that the social consequences will be the further erosion of trust in governmental and scientific institutions?
According to the authors, four ethical considerations must be met for a mandatory vaccine:
- The disease is a grave threat to public health
- The vaccine is safe and effective
- Mandatory vaccination has a superior risk-benefit profile compared to alternatives
- The level of coercion required is proportionate
Taking these in order:
(1) COVID-19 is most definitely a grave threat to public health. More than 1,000,000 people have died of COVID-19 in the United States, and as of 1 January 2023, according to the World Health Organizationthere have been 651,918,402 cases of COVID-19 and 6,656,601 people have died of COVID-19, with 778,879 new cases in the past 24 hours. At this rate, there will be 284,290,835 cases in 2023. At a death rate of ~1% worldwide, that means nearly 3,000,000 people will die in the coming year. These numbers are ridiculously precise, but their import is obvious.
(2) Whether the COVID-19 vaccines are safe and effective is still a matter of debate. As I wrote in an unpublished review of mRNA vaccines two years ago, these vaccines are an experiment, albeit a necessary experiment in the face of the pandemic. The results are equivocal at best, and as will be seen below, even more equivocal for the adolescents and young adults.
(3) My answer to this is the same as for “safe and effective.” As outlined in the paper, the data are inconclusive for adolescents and young adults.
And (4), the level of coercion required is proportionate, which gets deeper into the ethics of COVID-19 booster mandates.
To quote directly from the paper:
Proportionality is a key principle in public health ethics (emphasis added). To be proportionate, a policy must be expected to produce public health benefits that outweigh relevant harms, including harms related to coercion, undue pressure, loss of employment and education and other forms of liberty restriction… mandates may be justified for older but not younger people, among whom such policies are not proportionate given a lack of clarity that benefits outweigh harms. Such ethical assessments should rely on empirical data: thorough risk-benefit assessment requires quantification (where possible) of relevant risks and benefits for the group affected by the policy. With respect to poor outcomes due to COVID-19, the most consistent predictors are age and comorbidities such as obesity. Similarly, age and sex are prominent risk factors for vaccine-associated reactogenicity and serious adverse events (SAE) such as myocarditis, which is more common in young males. Vaccine requirements should therefore be predicated on an age-stratified and sex-stratified risk-benefit analysis and consider the protective effects of prior infection.
Again, neglecting long-term consequences of COVID-19, a one-size-fits-all approach to COVID-19 vaccination may be problematic. It is not clear that all of these factors have been considered, and to support this conclusion we can go to the data presented in Figure 1 (resized for readability in this format but unmodified).
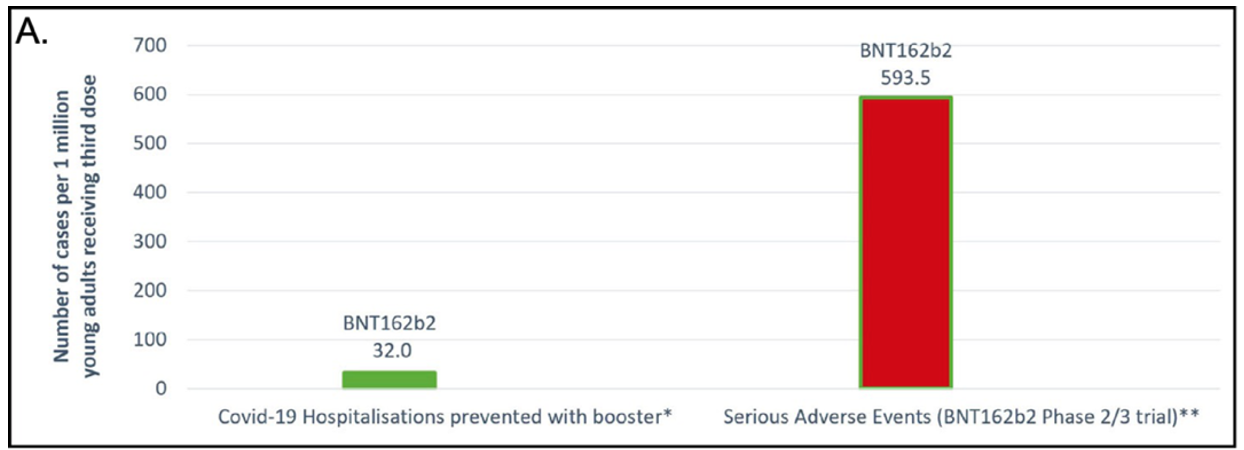
Figure 1A shows that, according to the authors’ analysis of the available data, for every 1,000,000 young adults receiving the third dose of the Pfizer/BioNTech mRNA vaccine (BNT162B2), 32 hospitalizations will be prevented and that 593.5 serious adverse events (SAE) will occur (1:18.5). SAE is defined as any of the following: death, life threatening at the time event, inpatient hospitalization or prolongation of existing hospitalization, persistent or significant disability or incapacity, congenital anomaly/birth defect or a medically important event, based on medical judgment. 32 out of 1,000,000 hospitalizations prevented is very low on the risk-benefit scale, while 593.5 SAEs per million could/should be considered significant, depending on the nature of the common SAEs associated with the booster.
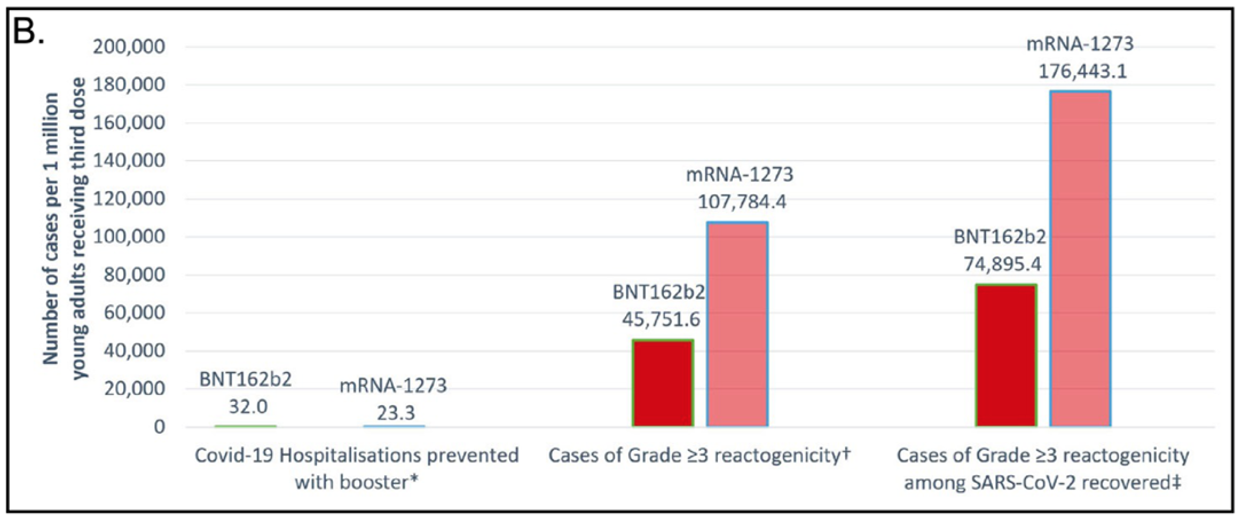
Figure 1B compares the Pfizer/BioNTech booster with the Moderna (mRNA-1273) booster. The Moderna booster is shown to prevent fewer hospitalizations than the Pfizer booster: 23.3 versus 32. This is a good example of the difference between relative risk/effectiveness and absolute risk/effectiveness. One could say that the Pfizer vaccine is about 39% better than Moderna (9/23=0.39), but the absolute improvement is from 0.0023% to 0.0032%, or 0.0009%, which has no practical significance. The numbers for Grade 3+ reactogenicity are more significant, and Moderna is “worse” than Pfizer: 11% versus 4.6%. Grade 3+ reactogenicity is defined as local/systemic adverse events that prevent daily routine activity or require the use of a pain reliever or require an emergency room visit or hospitalization. The values increase to 18% and 7.5% for those who have been previously infected with SARS-CoV-2 (based on reported seroprevalence in young adults).
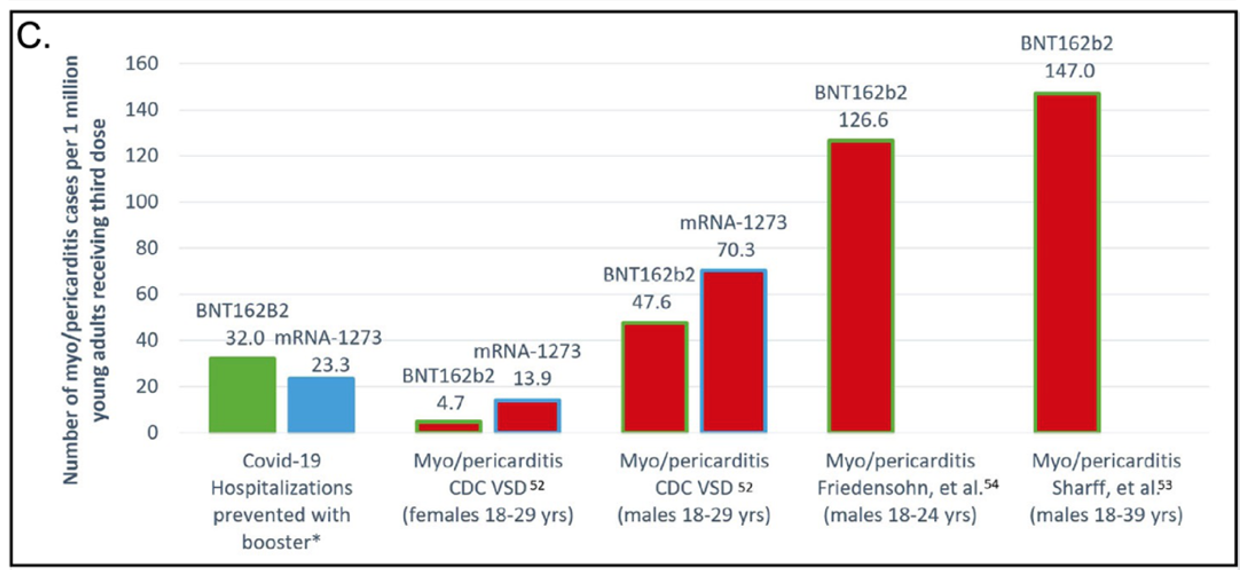
Figure 1C gets into the substance of the controversy surrounding mandates for young adults. The red bars show that myo/pericarditis (serious inflammation of the heart or the membrane surrounding the heart) increases significantly with both boosters, especially in males compared to females. From the paper:
For our estimates, and assuming a precautionary stance, we have used active surveillance rates or population-based rates. For males aged 18-29 years we consider the rate 1 in 7000 to be the most reliable because the method relies on CDC definitions and databases.
Further along:
Per million third doses of mRNA vaccine administered, 23.3 – 32 hospitalizations may be averted while 47.6 – 147.0 cases of myo/pericarditis may be caused among young males aged 18 – 29 years…Thus, to prevent a single hospitalization among males aged 18 – 29 years, we estimate between 1.5 and 4.6 cases of myo/pericarditis…For adolescents aged 16 – 17 years…we expect 6.3 cases of myo/pericarditis among males and 1.4 among females.
And more from published studies:
(V)accine-associated myocarditis has been found to occur in as many as 1 in 2652 males aged 12 – 17 years and in 1 in 1862 males aged 18 – 24 years after the second dose (and as high as 1/1300 after the second dose in a BNT1626b2 – mRNA-1273 combination.
The severity of these cases is often not trivial, and
69% – 80% of those diagnoses with vaccine-associated myo/pericarditis had findings consistent with cardiac inflammation on MRI testing 3 – 8 months after the second dose. The potential long-term impact of scar tissue on heart conduction remains unknown.
A study of this kind has obvious limitations and the authors address these, which include reliance on sponsor-reported and CDC summaries of adverse events (AEs), for example.
Nevertheless, their conclusion that “caution is warranted” seems very sound given the conflicting responses to and recommendations for the management of the pandemic from independent government and international agencies (e.g., CDC, NIH, FDA, WHO) during the past three years. Thus, it is hard to argue with their conclusion of the likelihood that “real-world severe or serious AEs may be greater than those reported in the RCT data because standard trials are underpowered to detect rare AEs and there may be selection bias” among trial recipients who may have had a bad experience during the primary series of inoculations. As pointed out in the paper, these data are usually collected after drug approval and use, which means that post-marketing data are critical for determination of the ultimate effectiveness of the vaccine, or any other intervention or drug.
The authors present five ethical arguments against universal booster mandates:
- Transparency. Risk-benefit analysis should be stratified by demographic factors and updated in a timely manner. According to this paper, no such assessment has been published to date: “(T)here has not been any RCT specific to evaluating boosters in young adults (and) CDC relied on data from an older cohort with a median age of 42.0 – 51.7 and incorrectly assumed that the benefits would also outweigh risks for younger age groups.” This assumption is unlikely to be true.
- Potential net expected harm. The reasonable likelihood of a net harm argues for the ethical case against booster mandates in the young. Updated policies have been developed for other vaccines as post-marketing data has become available, including adult boosters for tetanus and diphtheria; influenza, dengue fever, rotavirus; plus adenovirus-vectored COVID-19 vaccines due to thrombosis, primarily in younger women. And uncertainties remain for mRNA vaccines regarding menstruation and fertility and shingles.
- Lack of proportionate public health benefit. Boosters provide “limited lasting reduction in probability of infection or transmission, hospitalization, and limited expected benefits to young healthy individuals, especially those who have already been infected…(thus the)…coercive mandates themselves are not counterbalanced by a large public health benefit.” The emphasis on vaccines as the primary tool in the anti-COVID-19 toolbox also probably vitiates efforts for alternative and complementary non-pharmaceutical interventions as well as the development of anti-viral medications. But this is another issue altogether. Anti-viral compounds in combination (HAART) have made AIDS a manageable chronic condition for most HIV-infected individuals in the absence of a vaccine 40 years after the beginning of the AIDS epidemic. Yes, HIV is a much different virus causing a much different pathology, but the solution was not a vaccine.
- Failure of reciprocity. Vaccines in the US are generally covered by an injury compensation program for those who are harmed by the vaccine. This is not true of COVID-19 vaccines, which are still administered under an Emergency Use Authorization (EUA). If the shots are mandatory strong protections are warranted. So far, very few claims for injury compensation have been approved in the US, and there seems to be an undercurrent of outright denial that these vaccines may cause problems.
- Wider social harms. Mandates must be supported by a “compelling” public health justification. In the absence of such, coercion will lead to “long-term negative consequences on trust in society and institutions and vaccine confidence in general, including vaccine hesitancy for routine pediatric and adult vaccines, a problem which predated the pandemic and is considered one of WHO’s top 10 threats to global health.
The conclusion to this analysis of the ethics of mandatory COVID-19 boosters is that:
(1) Mandates should be repealed
(2) Pathways to compensation for those injured should be provided, and
(3) Regulatory agencies should require independent scientific analysis, with open access, to clinical data that provides risk-benefit conclusions in an age- and risk-stratified manner, especially for any new vaccines prior to their approval and use.
The authors stress:
This is needed to begin what will be a long process of rebuilding trust in public health.
All research is provisional, and the responses to this article are likely to be interesting. But I see little to add to their conclusions at this time, although they do diverge from the current institutional and governmental/political consensus.
Except one more thing in closing. A recent paper in Science Immunology (22 December 2022) on the effects of repeated boosters using COVID-19 vaccines suggests a Class switch towards non-inflammatory, spike-specific IgG4 antibodies after repeated SARS-CoV-2 mRNA vaccination. A complete description of the functions of antibody classes can be found here.
Although it is a simplification to say these results indicate that repeated mRNA vaccine injections lead to the development of “immune tolerance” of the spike protein analogous to tolerance of allergens, this is an interesting result that may be relevant to the issue of COVID-19 boosters, scientific and otherwise. As one might imagine, this paper has elicited responses in the 11 days since publication.
Many of these, from several sides of the resulting argument, can be found on Twitter using “IgG4” as the search term. Caveat emptor! I am not nor have I ever claimed to be an immunologist, but this seems to be something to watch from the Slough of Despond that is the COVID scientific literature, which now includes 321,974 references in PubMed using “COVID” as the query on 2 January 2023.
_____
[1] Confirmed after the death of my mother when I found my first-grade report card in a box of photographs. Three things in that document stood out: 12 consecutive absences due to the measles, the calligraphic handwriting in blue fountain pen ink of my first -grade teacher, and the year-end comment in which she diagnosed me at age 5-6 as someone who “could use his time more wisely.” Teachers, they are indeed wise and exceptional people!


Finally, a beginning to the implementation of a saner public health policy as regards Covid.
As any ‘graduate’ of a 12 Step program will tell you, the first ‘step’ towards a “cure” for any problem is to first admit that there is a problem. It is a real shame that, after three years, we, as a society, are just entering that “First Step.”
I’m ‘sending’ this to my relatives. They already think I’m a nutter. What do I have to lose?
Stay safe.
I was looking at the link in the article to the
recent paper in Science Immunology (22 December 2022).
“However, the large number of breakthrough infections caused by the Omicron variant indicates that current vaccination regimens do not confer sterilizing protection…”
Until it is admited that sterilization was not mandatory for the approval of the shots and that they were known to be non-sterilizing since 2020, I just see alot of the same ground being retread.
Yeah, at last the beginning of a wider discussion of harm vs benefit ( the probability of each to be more exact) . And organized by various cohorts ( like the different age groups, and those already infected and recovered and so on) at that.
A couple of issues still stand out to me – the term “public health”. Who is the public here ? One doesn’t quite have to go to the extremes of Maggie Thatcher’s “there is no such thing as society” – but some sub-grouping of similar sets should be incorporated instead of this single category of ‘public’.
Then there’s “how to rebuild trust”. I’m surprised there is no immediate mention of “fire the ones responsible”. Not because of revenge but “to encourage the others” and to get people more with-it into positions of authority, and to prevent the all too predictable behavior of foot-dragging and downright gaslighting that we get from those responsible.
I’d also include fixing the financial motivations here, for big pharma and all those in the tentacles of that poisonous squid but welllll that’s taking on capitalism and that’s a might beast to have a bun fight with.
This is all we’ve done in the past 3 years, heck its all we’ve done since the GFC. Think hard on this:
“We’re an empire now, and when we act, we create our own reality. And while you’re studying that reality — judiciously, as you will — we’ll act again, creating other new realities, which you can study too, and that’s how things will sort out. We’re history’s actors . . . and you, all of you, will be left to just study what we do.”
I have to say, the figures in those charts for Myo are pretty shocking. I knew there was a serious issue, I didn’t realise that the risk/benefit balance was that skewed. That the cardiology profession is not raising the alarm over this is…. well, I should say surprising, but it really isn’t.
I think its fair to say that the medical/public health profession has always been reluctant to trust the public with clear unbiased information – if you read the history of polio its pretty clear that there was a consensus that keeping the public blinkered on possible bad effects from the vaccine was considered justified, and maybe it was giving the risk/balance with that disease.
But there is an inbuilt assumption among many professionals that the general public just don’t understand risk, which repeated studies show is not true. That people don’t understand statistics well is not the same thing as not understanding quite sophisticated concepts in risk. Not to mention that repeatedly studies have shown that many doctors and scientists often have their own deep epistemological problems with statistics and risk.
I really don’t see any justification in the vast majority of cases (there may be some exceptions, polio being a well known one) for being less than truthful and open with the public – but there seems a very deep cultural problem within multiple levels of the science/health community that continuously comes up with reasons for equivocating with data. Nothing of all to do with professional gatekeeping and status of course.
The science/health community or the political/business community? Or do I repeat myself?
Here in America the medical profession has always been a capitalist affair and sounds like the same is becoming true in the UK with the NHS. The above article is all well and good but the assumption that decision makers are only thinking about health in these matters ignores the reality that profit making businesses have their own risk/benefit calculation involving the health of their shareholders. Therefore the first step toward ethical medicine would be to stop pretending this isn’t true and to pass laws to guarantee that it isn’t true.
So perhaps what makes Covid different from Polio or Smallpox is that this medical/business entanglement is much more so than it once was and it isn’t a conspiracy theory to regard anything coming out of Big Pharma with suspicion. At the very least government shouldn’t be declaring that suspicion itself illegal. The vaccine mandates–for this disease–have always been wrong. Some of us have had the luxury of being able to avoid them and Covid as well. And I still wear a mask to stores–thereby exercising my good old American free choice.
I think there is much, much more at work than just capitalism, at least in its most literal application. Of course the profits going to some companies is a major source of bias, but I do think that intellectual gatekeeping within various branches of the science/medical field has had a malign influence on public health over decades or centuries. Max Weber wrote about this a century ago (maybe not directly on public health, but in general). I think the shrinkage in access to the PMC has if anything exacerbated the need for internal ‘signalling’ within all professions that they are players in the game.
I still haven’t seen the cardiac split between vaccine and no Covid versus vaccine and Covid (before, after, or both). But maybe it’s finally in this paper.
And calling AIDS a manageable chronic condition is something of a gloss – if you intend to be read by ordinary folk.
Agreed, that would definetly be nice to see.. so nice in fact that I imagine Pfizer would have published it if they had reason to believe it would increase demand for their product. Part of this storyline the whole time has been that certain data pieces that should exist for us to draw a conclusions were never bothered to be collected
This paper is pretty much all we have about COVID related pericardial and myocardial issues…..It remains the best and broadest one that I know of. Done in Israel in one of their big huge systems. It is from April of this year. Any others I have seen are very much smaller or very poorly done.
https://pubmed.ncbi.nlm.nih.gov/35456309/
This is the conclusion –
We did not observe an increased incidence of neither pericarditis nor myocarditis in adult patients recovering from COVID-19 infection.
This is pretty much it at this time. There are several papers out there as KLG referenced above about vaccine myocardial issues – but this one is the only one done reliably with regard to COVID itself.
Unfortunately, this paper is not optimal in any way shape or form. It is a retrospective lookback. That is never the best way. It does have going for it a huge cohort.
The best way to do this kind of work is to actually collect data prospectively as you are going along. With both the vaccines and COVID itself, if this has been done – it has not really been reported. It is yet another sign of complete incompetence. It is what we keep saying over and over again. If this data exists, it needs to be released immediately. A group of good epidemiologists could come up with answers in an afternoon with a pencil sharpener.
Arent there a number of other heart related risks that comes with Covid? Even if Covid doesnt increase the risk of myocarditis, I still think its fair to question the other cardio events that those vaxxed/vs unvaxxed experience.. Although as I noted, cynically I would bet Pfizer did question that and the fact that nothing is being reported is potentially telling
I think it is very likely.
Unfortunately, the myocarditis issue is what I am focused on like a laser.
I have become concerned with the two I have already had in my practice. Both young men. Both very athletic. Both onsets very timed to the vaccine administration – not COVID. And although they are improved, they are not in any way back to baseline. I have no known patients with myocardial damage from a COVID infection.
As I have stated many times before, I fear that this right now is only being seen in a more athletic cohort. It makes me very concerned that the Nintendo crowd may have some issues and just do not know it yet because they are not pressing their hearts.
There is a precedent out there called rheumatic heart disease. It too infiltrated so many in the pre-antibiotic era and they only really started having issues when they became much older – in time for me to care for them as a young doctor. They are largely all gone now. Rheumatic heart disease is not the same as COVID, don’t get me wrong – it is just there is an absolute precendent for this kind of thing in the past. And the symptoms in many do not show up for a long time. As I stated – I am focused on the vaccine. That I think is causing problems for certain. COVID may very well be doing it as well. COVID infection is a much LOWER dose of spike antigen than a vaccine causes. It may cause its damage, therefore, in a much more insidious manner. WE JUST DO NOT KNOW.
COVID may very well be causing some/many of these clotting and vascular issues we are having – I am convinced because of the timing I am seeing with patients in my own world that the vaccines are as well.
Again, real studies need to be done. These are pressing issues – and the fact that this work is not being done is a real “sign” as you say. I would also consider it incompetence at best, a crime at worst.
Thank you, IM Doc. Very much appreciated.
Although I was a professor of non-clinical health, much of this makes sense to me and worries me immensely….particularly given my own cardiac history and the fact that when my current hospital got their hands on my scans from my hospital taken 20 years ago (upon diagnosis) they have suddenly done a “warp speed”.
Thank you IM Doc. Is it fair to paraphrase your comment as follows:
Young athletic people physically push themselves; present with symptoms; and can be clinically diagnosed – these are the visible victims of vaccine myocarditis or pericarditis damage.
Non-athletic types may also have suffered vaccine damage to their hearts but: do not notice symptoms; do not present to a clinician; and do not receive diagnoses – these are sub-clinical cases.
The potential extent of such sub-clinical cases is unknown.
Yes – that can be said. That is but one logical conclusion of the reason it is happening in athletes more commonly. There are others.
I am not at a place where I can find it now. But just recently there was an article published about the presence of cardiac damage markers after vaccination. The number of people who demonstrated this was frighteningly large. This is called a signal. It is not a certain problem and it may mean nothing. However, much work needs to be done PRONTO about this. But yet nothing has been released to the public about this, if it has been done.
An age and status controlled cohort of recent COVID infections needs to be evaluated in the same way. As well as an age and status controlled cohort of the unvaccinated and asymptomatic. This kind of study and data is the only way we are going to know for sure there is a problem. And if the problem is the vaccines? COVID? Both? One more than the other? neither? —- AGAIN these are the kinds of things that should have been embarked upon the moment these signals started turning up – not just in our VAERS but also in the Israeli studies – they were the first to report an issue in the summer of 2021.
@IM Doc
Here is an interesting new(2023) article in the American Heart Association Journal based on patients to Massachusetts General for Children and Boston Children’s Hospital:
Title: Circulating Spike Protein Detected in Post–COVID-19 mRNA Vaccine Myocarditis
https://www.ahajournals.org/doi/epdf/10.1161/CIRCULATIONAHA.122.061025
Yes – I was at a Zoom Conference where this was discussed today. And all I can say right now is there are many questions and few answers.
It is not understood if these findings are important. Some of them seem to be very concerning.
As I have said repeatedly, much very rapid work needs to be done. To begin the work and the recognition of what is going on, we must first begin to acknowledge the problem.
IM Doc, You’re absolutely right. I think this describes the study you allude to:
<a href="https://m.youtube.com/watch?v=vveMHtVk_mY"
which doesn’t yet seem to be in print. Shockingly, results suggest some degree of myocardial injury universally post booster, meeting the threshold for myocarditis in 3% (but not necessarily with symptoms, and, therefore, described as subclinical). The long term implications of this subclinical myocarditis are unknown but numerous cardiologists have linked resulting scar formation to an increased risk of dysrhythmia in the adrenergic setting (exercise), potentially manifesting with sudden death.
I’m screaming into the void here on an old article, but
The idea that one’s exposure to spike protein is greater from the vaccine compared to infection is counterintuitive to me.
I dread trying to Google this because of the amount of garbage I would have to wade through.
Does anyone have a link to a study ?
As a medical professional I have started basing my vaccine recommendations on the assumption that these people will otherwise be infected with covid, given the let it rip Beyblade strategy. ….. I’ve never been fully comfortable with this idea and so that’s why I’m asking.
“We did not observe an increaed incidence of EITHER pericarditis OR myocarditis in adult patients recovering from COVID-19 infection.” is less confusing to this reader as “neither” introduces negativity.
setting aside all its other limitations, isn’t the Israeli paper about post-acute myo/pericarditis? The paper itself says:
There’s abundant literature confirming significant observed myo/pericarditis at acute Covid infection (that is to say, not post-acute, contra the Israeli study referenced) – including in 2020 well before vaccination – and this literature cannot be handwaved away with a general “very much smaller or very poorly done”, particularly in contrast with the manifest limitations of the Israeli study you cite. The idea that that study and the line you quote dispositively shows no or very little myo/pericarditis in (pre-vaccination) covid infectees, at the time of infection is… surely not right, as the paper did not set out to investigate that in the first place?
And while I am not denying the reality of post-vaccine myocarditis, my understanding is that not all, but the overwhelming majority of it is “mild” and self-limiting (see one summary here, source is obviously pro-vaccine but I am taking his summaries of the studies’ conclusions at face value). Which, as CoryP alludes to (and others like Raymond Sim have elsewhere), hardly makes sense. The idea that the vaccines are causing all this trouble and the virus itself isn’t strikes me as fanciful? Presumably it’s not the adjuvants doing this, so surely it’s the spike? How could the limited spike produced by the vaccines possibly be doing so much more damage than the spike produced by the virus itself en masse, as some would apparently now have it? It’s also not necessarily true that the sudden death by heart failure that we’re now seeing – assuming it is in excess of the pre-covid baseline, and I suspect it is – is specifically caused by myocarditis or pericarditis alone.
As I’ve explained before in comments, we also have numerous erstwhile Zero Covid control countries like Australia who had a year of vaccination with very little or no co-circulating virus, followed by a year of mass infection. There was no excess death signal accompanying the mass vaccination campaign in (heavily vaccinated) Australia. It simply wasn’t there. (Australia and many other countries have their own VAERS analogues by the way, and Adverse Event reports were openly solicited from the general public throughout the vaccine campaign as well as monitored by technical experts – hence the rapid throttling of the deployment of AstraZeneca in Australia due to clotting risk when we had very little alternative mRNA supply). Excess death trends were thrown into sharp relief from Jan ‘22 onwards when we opened the floodgates for Omicron, and continued all year per actuarial data, coinciding with infection waves (booster uptake continued through 2022 but booster uptake was relatively low here compared to the first two shots). Moreover, for years now, we have always seen, internationally, that excess deaths in general correlate with waves of the actual disease, and not vaccination campaigns.
Tangentially, but: the idea that myo/pericarditis in vaccines is more severe than covid itself is of course one that someone like Vinay Prasad and the various other goober-grifter-frauds – cited with miserable regularity and depressingly uncritically here by an alarming number of commenters – needs to lean on very heavily as he has been saying for years now that it is important to infect children asap to get us to endemicity or whatever, which besides being scientifically illiterate was idiotically reckless blather predicated on the false assumption that Covid is no big deal for kids, as we blithely force infection on all the world’s children. More straightforwardly, it is not in Prasad’s material interests to shift from his vaccine fearmongering to pointing out more obvious and banal truths: that covid is actually really quite serious, obviously more serious at a far greater scale than vaccine harms by any sensible standard you care to use, and people should continue to wear a respirator whenever possible, because the minute he says any such thing, he will literally lose money as his paying followers will desert him, and his newfound media prominence as well. many such cases.
@PlutoniumKun
I am surprised that you are surprised.
Vinay Prasad was highlighting this issue on Substack over a year ago. Tracy Beth Hoeg, one of the authors of the paper discussed above, has also been highlighting this issue for over a year on twitter. This is only to mention two, there were many others – they were all sidelined.
The medical establishment has disgraced itself in its refusal to honestly engage with the data as it has rolled in and to reappraise.
It is true that the medical profession has disgraced itself.
Some examples:
“The @Delta letter is cosigned by @CarlosdelRio7 [president of the Infectious Diseases Society of America] @henrytingmd — two physicians with industry ties who seem content with throwing their HCW colleagues under the bus.”
(“Delta CEO asks CDC to shorten the recommended COVID quarantine: “the 10-day isolation for those who are fully vaccinated may significantly impact our workforce and operations”)
Vinay Prasad (anti-mask, anti-testing):
https://twitter.com/dontwantadothis/status/1608652844139442180?s=20&t=sIWBVt_sP9Dp5WZwbYzkHA
https://twitter.com/TheDesignFlaw/status/1600508694717923328?s=20&t=sIWBVt_sP9Dp5WZwbYzkHA
Thank you very much for this fine summary KLG.
I have been teaching medical ethics for years. I have been teaching students for years that the principles of ethics are extant not just for the protection of patients but also for the protection of practitioners. This whole interlude has taught me another aspect that I will have to add from now on. These principles are there for the protection and survival of the very profession itself. This lesson will now be learned and the price will be very high.
These mandates of experimental drugs went against the very essence of two of the most important statements of our ethical code as a civilization – The Nuremberg Code and the Helsinki Declarations. More importantly, they were a slap to the face of one of the guiding principles of medical ethics since Hippocrates – that of patient autonomy. As a physician of the late 20th Century, I have heard my whole life that paternalism was the great evil of our profession, that autonomy of patients must reign supreme. And then this happened. It was as if an entire profession was completely brainwashed in the blink of an eye. No thinking allowed.
Not only did the mandates happen with the complete acquiescence and encouragement of the profession and the ethics chairs in its most prestigious centers, we actually took it a step further. Something not even I saw coming. The demonization of the unvaccinated will be a branded Scarlet Letter for my profession from now on. Young doctors online laughing about scolding the unvaxxed as they were intubating them, ER doctors online demonizing grieving mothers of VAX injured kids thousands of miles away. I can go on and on. This egregious behavior was not only not reprimanded, it was held up as an example for others to emulate.
This is now just beginning the detonation phase. I saw a tweet this weekend of a young critical care doctor who was one of the main instigators of this malfeasance toward the unvaxxed last year. She said that even if the vaccines are poison ( an interesting comment to make from this crowd – precipitating much thought on my part all weekend) she would happily and righteously do it all over again. I DID IT OUT OF LOVE FOR HUMANITY AND I WILL DO IT ALL AGAIN – I DID NOT DO IT OUT OF HATE LIKE THE ANTI VAXXERS DID. First of all, she needs to go back and look at all the tweets and posts of her and her compadres, and then really contemplate the meaning of hate. Secondly, her statement above may very well be the epitaph for the current iteration of this healing profession.
I am unable to even begin to remotely process the soul place from where these people come. It has been profoundly depressing to me as an ethics professor the behavior of these younger doctors. I thank God to this day none of my students seem to be out there in the vanguard. They would have gotten a phone call for sure.
I do think we should all reflect on this line of thinking so prevalent in our world. It will be the death of us all.
The intense skepticism now being thrown at me all day about tried and true procedures and meds like kid vaccines is becoming alarming. We in this profession have no one to blame but ourselves. The quietness last year spoke volumes to all around us.
Again, KLG, awesome piece for the ages.
And as this all unwinds, may God have mercy on us all. This health care system is already in deep trouble. This engendered distrust may be the terminal event.
Thank you for this IM Doc. I and many others were deeply offended by the behaviors you describe. And let’s not forget that Biden, that nasty, corrupt, etc, threatened the unvaxxed with a “winter of sickness and death”. No apologies of course.
On top of that, millions of Americans’ income and livelihood were directly threatened and many ruined. And even now, at this late date, the pressure to get vaccinated to be employed persists and people are being forced to get the covid “vaccine”.
We have entered a dark era when such coercive behavior is sanctioned and rewarded. There is a serious rot in the moral fiber of our society, and it has rotted from the top down. Where this goes from here is anyone’s guess but I fear it gets worse, not better, because once again there has been no price to pay for failure and destruction.
And I was one of those people. Was the winter of 2021-22 a winter of sickness and death for me? Nope. I’m still here.
OTOH, I think that I lost a photographic assignment last May because of my, ahem, status. Was in quite the conversation with a local institution then, suddenly, radio silence.
This is one of those institutions that requires the thing that this article talks about. Methinks that my contact did a social media search and found that Slim isn’t exactly worshipful of this thing.
Any-hoo, I am grateful to what I learned here on NC. It strengthened my decision not to take the thing. Instead, I’ve been working on improving my health, and this effort is paying off.
So, once again, thank you, Naked Capitalism!
From my experience, those “people” meaning the un-vaxxed are still getting blamed. On several occasions in the not to distant past I mentioned that the pandemic is “not over” and in fact the numbers are now getting worse.
Common answer; that’s because all those *pick a name* won’t get the shots. It’s all their fault this is not over. Many then go on to explain how these people are the scum of the earth.
What a mess.
@IM Doc
Thank you for this. Was surprised you didn’t comment on Lambert’s piece a couple days ago :
Biden “Vax-Only” Strategy of Mass Infection Lies in Ruins, Destroyed by Vaccine Escape, Immune Dysregulation. I felt the piece danced around the issue of the vaccines themselves.
@KLG
Thank you very much for this!!! I feel this is the first time NakedCapitalism has fully addressed the failings of the vaccines themselves and vaccine mandates outside of broader political/public health policy.
I agree with Ahimsa’s final paragraph, ” the first time Naked Capitalism has fully addressed the failings of the vaccines themselves and vaccine mandates”.
A special thanks to IM Doc for his first critique (12-2020) of the vaccine trials which solidified my mistrust of big pharma.
I answered your earlier “dance around” comment and you just doubled down on it. I hope you find the happiness you seek elsewhere.
The medical profession still had quite a bit of moral capital before Covid. I still value the work of surgeons who are exposed to negative feedback loops: kill or maim too many patients on the table and you’re not going to be a surgeon for too long. But my attitude towards pill-pushing physicians is beneath contempt now, and that will not change. I still go to them when I need a note from my mommy to get a medication that preserves my life. But if they try to tangle with me on things not supported by data (statins, for example), they’re going to get a withering earful.
The only physicians I’ll trust without knowing them are ones fired for not taking the mRNA therapies or who suffered for opposing them. Everyone else is guilty until proved innocent.
Two questions that most pro-vaccine proponents with whom I engage simply don’t want to countenance are:
1. Did mass population-wide vaccination campaigns against a coronavirus (which are notorious for rapidly evolving and mutating) during widespread waves create an enviroment with selective evolutionary pressures promoting variants and vaccine escape? In effect undermining and ultimately proving counterproductive in the fight against the novel virus.
see section of KLG’s post:
2. Has repeated dosing (particularly of the novel mRNA vaccines) resulted in immune imprinting or immune intolerance in a huge percentage of our adult vaccinated populations.
see KLG’s post:
I am glad KLG could raise those issue in this post, it’s the kind of thing that used to get people censored on Twitter and YouTube.
I am of the opinion that the vaccine mandates here (New Zealand) were a disaster. I was against them at the time, but had some trouble articulating why, and was at odds with most of my peer group, who tended to side-eye me as a possible anti-vaxxer if I tried to raise the subject.
Even the supporters (and there were many at the time) had to admit that it was a pretty major departure from the principle of patient autonomy. It was mostly hand-waved away by pointing out that we weren’t technically requiring them. I’d say that is sophistry given that they were required to hold most jobs, participate in public life, or venture into public spaces (we did at least exempt essential services like supermarkets and hospitals).
The main problems in my view were that (a) they did not deliver the promised result and (b) they were a huge expenditure of political capital for minimal or no gain. It was very clearly promised that if we all met the vaccination targets and complied with the mandate, we could expect to be protected from Covid and go back to living a ‘normal’ life. It was clear even from evidence at the time (Provincetown) that this was a pipe dream, and Omicron blew it completely out of the water. Supporters claim it could have succeeded with Delta and Omicron changed the game, but there was always going to be a new variant. There is really no plausible argument under which we can claim it was justified to restrict people’s freedoms so drastically in the name of public health, when we are tolerating vastly higher infection and death rates right now with no restrictions at all and claiming it’s no big deal. Essentially the argument is that mandates were justified because back then we were scared and now we aren’t.
So we were left with a group of people who were being denied some pretty fundamental rights for basically no good reason. This was a pretty traumatic experience for most of them (some have written about the experience) and there was a distinct lack of support or empathy for any that spoke up. On the contrary, they were vilified and demonized. Even now, most people who supported the mandate still claim it was needed, and don’t recognize the cognitive dissonance of accepting vastly higher infection rates with no restrictions right now. Meanwhile, the only group that was willing to provide support, validation and emotional comfort to these people was the anti-vax community. Is it any wonder that the parliamentary occupation and explosion of CT groups was the result?
Excellent post, as always.
Far too many people in the medical industry (1) told people early on that the experimental vaccines were risk free and everyone should take them, without discussion of the nuanced risk inherent in ANY medicine or vaccine, and (2) kept telling people to take the vaccines after the risk profile became blatantly obvious. Those people have lost ALL credibility and I will never listen to them again on any issue. Fortunately this is “only” perhaps 90-95% of physicians and putative public health experts.
I am forgiving of those people who looked at the experimental vaccines as a potential life-saver with major uncertainties, and cautiously recommended them to the elderly or those otherwise at high risk from Covid-19.
But few mandates applied to the elderly and high risk. Most mandates applied to working age people at moderate to low risk. The worst and most offensive, immoral mandates by far applied to college students and school children, at essentially zero risk of death or serious illness. How many of those young people now have radically shortened life expectancy? Turbo-cancer? Infertility or sterility? Chronic debilitating conditions? Even one is too many, but the likely number is in the range of seven or eight figures.
This has been the worst catastrophe in the history of medicine, and we’re probably still in the early stages of recognizing it. There’s no question that all of the mandates were and are unethical. There might be some meaningless questions of degree, for example the unethical mandate on hospital workers in the US, where there is some logical justification yet not enough relative to the risks, compared to the mandates for schoolchildren in some states, which are tantamount to genocidal child abuse.
Does COVID infection in these age groups cause X-carditis at a lower rate than the vaccine does (in which case what is the mechanism) or is it just that the booster does not reduce the incidence of X-carditis in COVID cases?
I think the more relevant calculation is not the “vaccine-induced” versus “CV-induced” rates subsequent to exposure to the respective stimuli (a relative risk calculation), but rather “absolute incidence” of the respective outcomes (absolute risk calculation). The relative risk could be quite favorable for the vaccine and it might still be a bad choice for those who are able to significantly lower their risk of contracting the virus through NPIs.
Exposure to the vaccine is 100% for those who receive it, compared with a possibly much lower risk of contracting the virus if the NPIs one implements are effective.
Actually, its moreso that the exposure to vaccines is 200, 300, or 400%+ when you factor in boosters. If this was a one and done vaccine we could begin to make the analysis expr suggested.. even though there is that progressively smaller group of unvaxed/No Covid group that should factor into the analysis as you note
Agreed. Perhaps an appropriate “absolute risk” calculation could compare frequency of adverse outcomes (such as myocarditis) on a defined time scale, such as the recommended interval between boosters. On that comparison, the booster “risk of exposure” would be 100%, which could be compared with “risk of infection” over the same time period, depending on what NPIs one (and one’s associates, neighbors and community) were using. Then one would factor in the “conditional probability” of the concerning outcome.
One of the things that has been grievous to me is that it seems that many people who have received the vaccination and boosters assume that they can safely dispense with NPIs. This posture, it seems to me, is like embracing both the 100% “risk of exposure” to the vaccine (for those who are treated with it) and a high risk of contracting the virus — since the vaccines are not sterilizing. So it isn’t “either get vaxxed or contract CV”, but rather “get vaxxed and run a high risk of still contracting CV”.
Lambert is always emphasizing “layered defense”. It seems that a distressingly large proportion of the population doesn’t understand this concept, or isn’t willing to go to the trouble of implementing additional protections.
I think the risk of long COVID is undervalued here. Even if the vaccine reduces the chance of long COVID by only 10-15%, I believe it’s still the right choice to risk a vaccine adverse event.
With 4 doses and a 10-30% chance of long COVID, you risk a 0.24% chance of serious adverse event to reduce your risk of long covid by 1 to 4.5%, assuming a 100% chance of getting COVID once.
Agreed that this is an additional complication.
I would urge to “layer” NPIs on top of pharma interventions such as vaccines for protection from Long COVID.
The thought is simply that one way to delay acquiring Long COVID is to delay COVID itself, and NPIs can do that.
3M Aura N95s can be purchased at Amazon for $1.15 each if purchased in case (240/case) quantities. Pool funds with friends, get a bunch, and share them.
I’m not a statistical wizard, but if I was a male between 18 – 29 and have a chance of 32/million being hospitalized as opposed to 147/million chance of myocarditis, I’d put my bet (and life) on my hospitalization chances. I just don’t get why this is so complicated. Oh well, call me an anti – myo, Trump loving, fanatical right wing, election denying, Ukraine flag waving, Jan 6th insurrectionist kinda woman.
In a similar vein:
TWiV Special: Bivalent boosters with Paul Offit
A thirty minute discussion
“Paul Offit returns to TWiV to discuss why the bivalent booster dosing story should be a cautionary tale of how not to move forward in this pandemic.”
Thank you KLG for your effort and I concur with your assessment. One thing I think we should think about when talking about vaccines is that it is not the same challenge to try to protect against viruses that enter and infect initially in the upper respiratory tract and are transmitted airborne (despite CDC stubbornness) as efficiently as COVID, Flu or RSV among others. Prior to COVID, risk assessment analysis led to the recommendation of flu vaccines (never mandate) only for the elder and some studies showed that repeated vaccination in this case, year after year, might result in immune fatigue in this cohort and weaker immune responses with time. We have never run for boosters like crazy every few months until COVID and this has been done with little if any previous evidence of their utility. We focus on Nab in sera and we really don’t know what is going on in the places that matter for entry: the URT mucosae.
It is fair to say, though that the 2021 vaccine campaigns were useful and prevented a lot of hospitalizations and deaths but time has gone, virus evolved rapidly and we cannot simply get ahead of it with vaccines. In fact we are very much behind the curve and IMO vaccine mandates do not make any sense. In fact they didn’t make any sense even in 2021 and from a practical point of view vaccine based COVID policies were counterproductive in the sense that allowed more transmission between overconfident vaccine recipients. It may sound quite counter-intuitive but mass vaccination probably resulted in better virus spread associated with lower sense of risk.
In regards to the last paper on IgG4 keep in mind this is only “interesting” scientifically and a primer for much further research on the role of such antibody subclass but the paper doesn’t give a clue on what kind of protection these give compared to the usually dominant IgG1 and IgG3 and for instance what titres of such subclass would produce significant reduction of disease severity etc. Bear in mind that much of the spread of COVID within our bodies goes directly from cell to cell without the need to release lots of particles to infect new cells, and these antibodies without (or with less) cell-killing effector properties might avoid inflammatory reactions but at the same time might give very limited protection. In fact what the paper says is that our immune system, after repeated exposure to the Spike antigen (via vaccination or infection) tries to reduce the damaging inflammatory responses associated. It somehow underlines that Spike protein based vaccines are by themselves somehow damaging.
Just to end, I am quite pro-vaccines, but with proper risk/benefit assessment and this ratio has been climbing steadily since mass vaccinations started.
re: ” It also highlights that coercion can produce a loss of trust in public institutions and other vaccines.”
Where to begin…. NIH? CDC? FDA? HHS? Basically the entire federal public health apparatus? Before these last 3 years I never questioned them. They were the GoodHousekeeping Seal of Approval, so to say. Now? My trust in them has vanished. I know there are still many dedicated lower level people who believe in and work toward public health and the public good, but the lower level people don’t make policy.
Hell yeah, the nadir was when I lost trust in first the Federal Aviation Authority and then the NIST ( National Institute of Standards and Technology) and the UL kitemark private company Underwriters Laboratories. This was all in the 2000s in the aftermath of the various mis-investigations into the twin tower collapses.
Yes, it’s quite the web of lies over this last decade or so. Great show last night with Glen Greenwald’s interview of Jimmy Dore. Start at 28 minutes for the fun part. Link: https://rumble.com/v23rbyc-jimmy-dore-on-mccarthys-speakership-bid-squad-hypocrisy-ukraine-and-more-sy.html
They run through the various levels of deceit. Go IM Doc, go NC!
That is a fantastic interview, thanks for the link!
Yes, thank you!
Amazing that you can see this kind of opinion piece on WSJ now.
Think of all the doctors who warned us and were pilloried mercilessly by the media.
https://www.wsj.com/articles/are-vaccines-fueling-new-covid-variants-xbb-northeast-antibodies-mutation-strain-immune-imprinting-11672483618?mod=opinion_trending_now_opn_pos2
Thanks very much for this post. Excellent paper.
“All things considered, I would rather have had the vaccines. They work!”
For a man who understands the nature of the web and provides links to so many important points, a link to the gold standard of scientific truth, the RCT for some of the vaccines that “work” would be useful here. I particularly appreciated that Pfizer ran such a large RCT for the mRNA treatment and I’ve been able to calculate the relative risk reduction from their data, and yes, it was over 90% effective at the time they reported results. Of course, the absolute risk reduction said that for every 22,000 people we inject with mRNA, we can expect one fewer death in six months from Covid. It was only when got the rest of the data that we found out there were more deaths in the mRNA group than the placebo group. To save one death from Covid in the mRNA group we lost a few people to “other” causes.
AS IM doc points out, the entire medical profession has shot its credibility over this issue. I no longer accept “vaccines work” from medical authorities, because their definitions of “work” differ from my own. Show me the RCT, let me probe the data, let me calculate the ARR, not the RRR, and I’ll accept.
an aside:
“the entire medical profession has shot its credibility over this issue.”
The WHO pandemic treaty update, where the WHO will control all the signatory nations’ pandemic responses if signed an passed, is exactly not the solution to the problem. The WHO’s response throughout has been no better, often worse than the US and other countries. I have less trust in the WHO than in the FDA.
Caveat that I’ve been a medical skeptic for probably 30+ years mostly due to my own family’s medical history. Multiple members of my family have had allergic reactions, bad side effects, treatments that made things worse along with non and/or mis-diagnoses. This included issues with normal vaccines for both my Dad and my son.
We had covid early and it wasn’t as bad as a normal flu for us. When the covid vaccines were introduced, we decided to take wait and see approach since we’d already had the disease. I respected other people’s choices on deciding to get the vaccine including my parents. Most of them just did what media, their doctor etc told them to do to so they would be safe and then to “protect grandma”
Fine…but then they wanted to give it to teenagers. In June 2021, I reviewed the deck the Cdc that had put together that showed the myocarditis signals in teenagers and thought no way for my kid.
Then the mandates happened. I pretty much lost my mind about this. I ended up quitting my job (govt contractor ) in Dec 2021 so I wouldn’t have to either lie to get a religious exemption (my company was approving them) or get the jab. Here in California, we couldn’t go to many events at that point without a vax card. This was happening when there were breakthrough infections happening left and right so it was pretty obvious that the vax didn’t stop transmission.
It is just in the past few months that the industry that both my husband and I worked in have dropped vax requirements from their job listings although not entirely.
My son couldn’t attend an in-state college and went out of state to avoid the vax requirement.
The only thing I didn’t lose faith in was my friends and family. They are ALL (with a single exception) vaxxed and know that we aren’t, but we didn’t have any of the issues that I’ve heard about. We were included in holiday celebrations, invited to activities. After the initial discussions, we just had to avoid the whole subject,and I’ve had to accept that I can’t have a real discussion on any real topic (don’t even think about bringing up Ukraine) without MSM talking points just being repeated.
I’m pretty cynical about just about everything these days.
A friend used to warn me that there was no such thing as too cynical, Laura. It’s great that your family still welcomed you despite not being vaxxed.
Your situation recalls what was for me the big stopping point on vaxxes: the idea that one should take the things even if recovered from Covid. I recently recovered from two days with Covid: 103 degree fever and done, and I’m not young, thin, female, or all that healthy. They blew a propaganda campaign of fear and didn’t take steps, as often pointed out here at NC, that could have prevented spread because there was no easy profit for anyone in them (imagine paying the billions paid to Pfizer to HVAC blue collars and getting a real health improvement out of it instead). I wouldn’t take the risk of them now for anything.
And I’m questioning almost everything else.
Haven’t had energy to do much recently due to long covid. The “mysterious virus” everyone round here in middle of UK fits new covid variant much more than flu. Our household all still suffering….. Over 2 weeks after initial infection and still ill. My autoimmune issues back into overdrive….. Alopecia most “obvious”…. When biopsied in August, the physician said “scalp biopsies like this are all I’m doing these days” and showed me scar of his OWN biopsy done after covid infection.
Tired of all this. Even worse, the Tories now say mask use is something you do if YOU are the problem (flu etc). Today on busses etc picking up my vital meds I had 6 people make “quiet” comments about me…… When *I* am the clinically vulnerable person….. My congenital heart problem is back and I’ve been called back (Monday) to have a continuous monitor fitted.
After THAT Channel 4 A&E documentary yesterday the hospital is desperately trying to recruit…… Bit difficult when I can type in badly ventilated office (no mask mandate) or work at supermarket at bottom of scale for MORE MONEY AND MORE FRESH AIR. We are really in trouble. Clinicians – interested in your views on UK Channel 4 documentary on ER (QMC Nottingham) first broadcast yesterday (Tues 3rd). Got serious stick on twitter……
If I’m banned forever so be it….. But I’m furious at the UK authorities, tweeting the following – I’m just trying to help and follow the advice from the docs on NC:
Happy to help @TeamNUH get crucial letters to patients/GPs typed more on time. How’s about paying more (and I have extra skills to justify this & other things – see my h index) so @sainsburys doesn’t beat you. I just want ADEQUATE VENTILATION AND MASKING. Protect your employees.
I’ve really appreciated your contributions here over time, Terry and I’m sad to hear you’re doing so poorly. I hope it passes.
It would be great if someone could make a two page chart, divided into two columns, showing “Dominant Narrative” in one column compared with “Science & Reasonable Inferences” in the other column. If time permits, adding citations to relevant authorities for each proposition. Maybe this could be a group project. I, and I assume other laity, are in positions to effect policies and practices at local (for me, Chicago) institutions and public spaces. Having a myth-busting handout would be useful. Ciao
Paul Offit, inventor of the Rotavirus vaccine, and a dissenter on the issue of boosters on the FDA advisory panel on vaccines, has much in common here. To me, as a physician, the most troubling was a study from Thailand, that looked at common markers of cardiac injury following vaccination. Of the 300 young men in the study, while none developed myocarditis ( not unexpected – study size too small); 2.5% of study subjects had transient increases in troponin and CPK. To put this in perspective; walking in to the ER with this will earn you a trip to the coronary care unit. So, 2.5% of a population of healthy young men is being subject to immune mediated attack on the heart, the long term consequences of which are ” known unknowns”. One would think that- proceed with caution, would be an appropriate adage. https://www.youtube.com/watch?v=fqtQAVRNowQ&t=3034s
I see Vinay Prasad on the author list. The guy used to write blog posts invoking the Third Reich when talking about how covid suppression policy, complains about the lack of RCTs to justify for mask use, writes for the Brownstone Institute of Great Barrington fame so I’m not terribly surprised that he’d come down negative on boosters. Of course that doesn’t mean that the results aren’t valid, but it raises some red flags.
I agree. I do not read papers, if I do not like any of the authors. Being nice to each other has been an important part of science all throughout history, but lately people like Vinay Prasad and Bhattacharya destroyed that spirit.
People, who invoke Third Reich (and Nurenberg code that came out of it) are using hyperboles to describe a thoughtful response to a serious pandemic. The current situation is very different from what the Nazis did, when they blamed a sub-population for carrying disease to generate fear among the population –
https://www.jta.org/archive/typhoid-is-endemic-jewish-disease-nazis-say-in-issuing-warsaw-ghetto-rules
The issue is that the Nuremberg Code and other decrees like it were a direct result of activities of villains like Dr. Mengele among many others. Among all that I have read about the Nuremberg Codes in my life, the thing that stands out is that the vast majority of German physicians recognized that what he was doing was evil, and yet because of the environment they were in, they chose to ignore it and not say a word. Put another way, had Mengele’s colleagues stood up and renounced him and all the others, I doubt the villains would have been able to be as effective in committing their evil deeds.
So, our forebears in ethics, in the immediate aftermath of the atrocities met in Nuremberg to codify a simple question – “What can we do so this never happens again to our descendants?” They thought and fought long and hard – but at the end of the day, decided on basic structures to stop the evil at its inception. Basically, enact rules to disable any individual or country FROM TAKING THE FIRST STEP DOWN THE SLIPPERY SLOPE. Your comment is equating that first step ( and their desire to “nip it in the bud”) to the atrocities that followed from the first step. That is not appropriate.
One of those rules was to NOT allow coercion of any kind of experimental therapy or research. And that makes perfect sense given what had happened in those concentration camps.
To equate the Nuremberg Code to the Third Reich is, in my opinion, completely out of bounds. I absolutely loathe all the “this person is Hitler” talk running wild in our discourse today. It is toxic. But the Nuremberg Code and its tenets were a response to Hitler, and for the most part have held up well for a few generations to protect all of us in the West. The fact that these vaccine mandates are a direct rejection of the Nuremberg Codes should give us all pause. I would have never dreamed it possible to contemplate just 5 years ago. But we now live in a society that has also thrown out other treasures like the First Amendment, so it is no longer surprising. People who are discussing ethics in our society, especially medical ethics, should have every right to invoke the Nuremberg Codes without fear of being blamed as a Nazi fabulist. Those codes are among humanity’s highest achievements.
I suspect there’s quite a bit of sarcasm in JMG’s comment. His final link makes an analogy between Nazis blaming a small sub population, Jews, for typhus, and leaves unstated the constant demonization of “the unvaccinated” for the current pandemic.
bingo
Kunstler agrees with what IM Doc says about the future of medicine –
https://kunstler.com/clusterfuck-nation/repentance/
” I’ll tell you what will happen: medicine as we’ve known it is going to collapse, along with most other activities in our society. Apart from ethical offenses against the public in the single instance of the Covid-19 emergency, doctors and their administrative cohorts have stealthily surrendered to a racketeering business model that had already badly damaged the practice of medicine before Covid-19 came on the scene.
Remember: as a general principle, organisms and systems often assume their greatest size just before the go extinct or fail. That’s exactly what you’re seeing in the conglomeratization of hospitals in the USA. If the idea was to remove redundancies for the sake of “efficiency,” then they did exactly what destroys ecosystems. Anyway, the net effect of all that hospital consolidation was just to make access to health care much more difficult for the average citizen, and the only benefit was to make multi-millionaires of the executives who run the hospitals.”
Also, John Michael Greer alludes that maybe we are entering the endgame regarding covid vaxxes –
https://ecosophia.dreamwidth.org/215249.html?thread=38096849#cmt38096849
“One of my readers referenced this in discussing a comment on yesterday’s Magic Monday open post. He quoted his mother (vaxxed and boosted) as saying the following in a discussion of the vaccines:
“Even if the Covid-19 vaccine kills me, it was a good deal, and given the chance, I’d do it again even knowing that it would cost my life.”
Has anyone else seen anything like this? I find such utterances profoundly creepy, to use no stronger language. Wasn’t the point of the vaccines to save lives? The Twitter post is very obviously virtue signaling — notice the telltale insistence that the people on her side were acting out of love and those who disagree with her could only have been acting out of hatred — but Anon’s mother’s comment doesn’t even have that element.”
re: Even if it kills me, etc.
There are a sudden spate of those declarations showing up on twtr and other social media. They don’t really make sense. I have my doubts about their source(s).
adding: Things aren’t always what they seem. / ;)
https://sfstandard.com/technology/these-doctors-pushed-masking-covid-lockdowns-on-twitter-turns-out-they-dont-exist/
Yes, it appears the tweet I was referring to is now questioned as being a fraud.
Very concerning. I would say that is often seen in a group that is trying to discredit its opponents – get them to say things that are inappropriate.
That tweet may very well be a fraud. The problem is that I am seeing this same kind of thinking pop up in multiple locations. If this is a fraud, this may very well be some kind of organized thing, See above.
And the other disturbing thought I had when I began to contemplate the authenticity of the Tweet is that I believed it. Why? I do not need Twitter or the Internet – very similar if not worse statements have been made to my face over the past 3-6 months. This is all really becoming quite a dreadful show. Not encouraging for the future for my kids.
IM Doc, The author of the tweet you mentioned in your earlier comment is a real doctor, not one of the fake accounts mentioned by flora.
Her posts –
https://med-mastodon.com/@SolNataMD
Her profile –
Dr. Natalia V. Solenkova
https://health.usnews.com/doctors/natalia-solenkova-841718
based near Miami Florida.
I cannot locate the exact comment, but her tone in general matches the text you posted. She may have deleted the comment after getting a bit more public attention than expected.
The tweet attributed to her was fabricated. Rogan himself apologised for this.
Seems she went private after copping a lot of abuse as a direct consequence of that fabricated tweet.
forgot to add that she took her twitter account private –
https://twitter.com/SolNataMD