By Lambert Strether of Corrente.
“”It is common sense to take a method and try it. If it fails, admit it frankly and try another. But above all, try something.” –Franklin Delano Roosevelt
As is well known, the Biden Administration has pursued a “Vax-only” policy from its first days in office (augmented, to be fair, with various over-hyped yet profitable pharmaceutical treatments of less-than-stellar effectiveness; remdesivir, paxlovid). The hallmark of Administration policy has been a thorough-going rejection of a layered strategy (“Swiss Cheese Model“) that would mandate non-pharmaceutical interventions to decrease airborne transmission, whether through recommendations (“3C’s“), ventilation, or masking. (Such is the Democrat commitment to the bit that Acela Corridor media figures are now coming forward to stigmatize mask-wearers, making them objects of derision and hatred; see the New York Times and The New Yorker.) In practice, the Biden Administration has pursued a policy of mass infection, since the vaccines we have now are not sterilizing, and eliminate neither transmission nor reinfection.
The Biden Administration’s Covid policy of mass infection has so far — I will assert for the purposes of this post — been cost-free politically, for a number of reasons: Business support, an incoherent Republican response, denial of airborne transmission by powerful institutional forces in healthcare and academia, a shift in focus from shared responsibility for public health to “personal risk assessment” (engineered by the public health establishment, ironically enough), and destruction of data gathering, but above all through a Goebbels-level propaganda campaign, waged by all components of the Democratic party apparatus and its self-embubbling (hegemonic) PMC class base in favor of “Vaxed and done.” (To be fair, “convenience” and “living your life” are not hard sells for Americans, our culture being what it is. Nor is working through illness. Nor, in least in some strata of society, is a fandom for well-credentialed and highly-placed figures). However, time may be running out.
The Biden Administration’s Covid policy of mass infection has always been vulnerable to facts on the ground. Another surge equivalent to January 2022’s Omicron surge would do it in; so would “something awful” in the form of vascular or neurological (epithelial) damage of an undeniable scale. (Long Covid doesn’t seem to be awful enough, sadly; but that could change, given a solid mechanism and possibly a few celebrities to help with the narrative.) In this post, I’ll first present the case for vaccine escape from recent variants, and then the case for immune dysregulation as a sequel to acute covid. In terms of facts on the ground, the first would create a surge; the second, “something awful.” In either case, even the most coughing, exhausted, several-times-injected, “I’ve got a cold I can’t shake” vaccine militant might be gently led to the conclusion that the Biden Administration’s policy of mass infection has failed[1], and we must try something else.
Vaccine Escape
I started meditating this post when I saw the following article in Cell: “Alarming antibody evasion properties of rising SARS-CoV-2 BQ and XBB subvariants“; “Alarming” is not typically a word that one sees in article titles for professional journals. (I think it translates to “hair on fire”?). From the Abstract (and I’ve gone a little overboard with the formatting just to make the point:
The BQ and XBB subvariants of SARS-CoV-2 Omicron are now rapidly expanding[2], possibly due to altered antibody evasion properties deriving from their additional spike mutations. Here, we report that neutralization of BQ.1, BQ.1.1, XBB, and XBB.1 by sera from vaccinees and infected persons was markedly impaired including sera from individuals boosted with a WA1/BA.5 bivalent mRNA vaccine. Titers against BQ and XBB subvariants were lower by 13- to 81-fold and 66- to 155-fold, respectively, far beyond what had been observed to date. Monoclonal antibodies capable of neutralizing the original Omicron variant were largely inactive against these new subvariants, and the responsible individual spike mutations were identified. These subvariants were found to have similar ACE2-binding affinities as their predecessors. Together, our findings indicate that BQ and XBB subvariants present serious threats to current COVID-19 vaccines, render inactive all authorized antibodies, and may have gained dominance in the population because of their advantage in evading antibodies.
For whatever reason — charitably, the December 13, 2022 publication date, too close to the holiday season — this peer-reviewed study from a top-drawer medical journal has gotten virtually no play in the press.
GM advises us to look at Figure S3, so — even though I feel I’m juggling power tools — here it is (the highlighting is mine. This is an “antigenic map.” The caption explains why the axes are not labeled).
Figure S3 Antigenic map of BQ and XBB subvariants in relation to SARS-CoV-2 variants and sarbecoviruses, related to Figure 2
(B) Antigenic map based on the serum neutralization data from (A). Virus positions are represented by closed circles whereas serum positions are shown as open squares. Sera are colored by group. Both axes represent antigenic distance with one antigenic distance unit (AU) in any direction corresponding to a 2-fold change in neutralization ID50 titer.
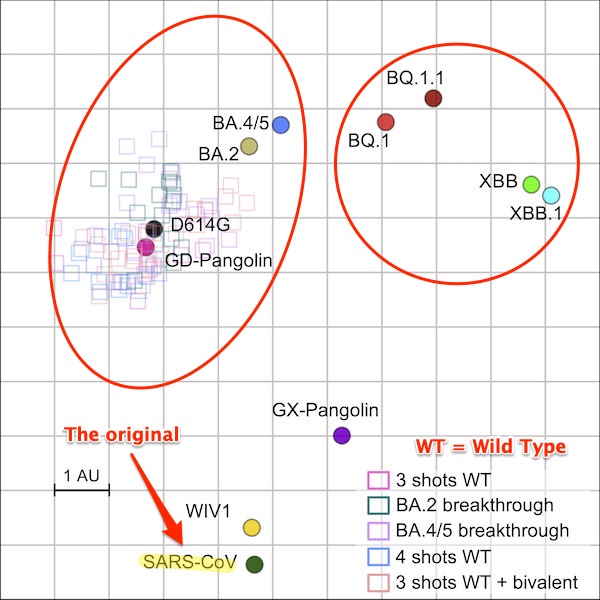
(New subvariants in circle at right; no sera. Old subvariants in circle at left; sera.) In prose:
Our data demonstrate that these new subvariants were barely susceptible to neutralization by sera from vaccinated individuals with or without prior infection, including persons recently boosted with the new bivalent (WA1/BA.5) mRNA vaccines…. The extent of the antigenic drift or shift measured herein is comparable to the antigenic leap made by the initial Omicron variant from its predecessors one year ago. In fact, combining these results with our prior findings on the serum neutralization of select sarbecoviruses, there are indications that XBB and XBB.1 are now antigenically more distant than SARS-CoV or some sarbecoviruses in animals… Therefore, it is alarming that these newly emerged subvariants could further compromise the efficacy of current COVID-19 vaccines and result in a surge of breakthrough infections as well as re-infections. [3]
But, you say, even if the old vaccines don’t work for the new subvariants (BQ/XBB), we have bivalent boosters now, so perhaps they will save us. Sadly, no. First, the Cell study says they won’t (see above), but we can further look at two articles, first from the CDC, and the second from the NEJM.
The first article asks how much of a boost the bivalent boosters give, given “waning immunity of monovalent doses.” From the CDC’s Morbidity and Mortality Report, “Effectiveness of Bivalent mRNA Vaccines in Preventing Symptomatic SARS-CoV-2 Infection — Increasing Community Access to Testing Program, United States, September–November 2022,” December 2, 2022:
Relative vaccine effectiveness (rVE) of a bivalent booster dose compared with that of ≥2 monovalent vaccine doses among persons for whom 2–3 months and ≥8 months had elapsed since last monovalent dose was 30% and 56% among persons aged 18–49 years, 31% and 48% among persons aged 50–64 years, and 28% and 43% among persons aged ≥65 years, respectively.
That doesn’t sound very encouraging.
The second article is a letter in the New England Journal of Medicine, written in answer to a Cell article from February 2022, among others, but not the article quoted above. From “Neutralization against BA.2.75.2, BQ.1.1, and XBB from mRNA Bivalent Booster, December 21, 2022:
We tested serum samples obtained from participants who had received either one or two monovalent boosters or the bivalent booster to determine the neutralization efficiency of the booster vaccines against wild-type (WA1/2020) virus and primary isolates of omicron subvariants BA.1, BA.5, BA.2.75.2, BQ.1.1, and XBB using an in vitro, live-virus focus reduction neutralization test (FRNT).
… Persons who received the BA.5-containing bivalent booster had better neutralizing activity against all omicron subvariants (especially against BA.2.75.2, BQ.1.1, and XBB) than those who received either one or two monovalent boosters, even though the neutralization GMT against WA1/2020 was similar in the cohort that received the two monovalent boosters and the cohort that received the bivalent booster. These responses are consistent with recent observations in persons with breakthrough omicron infection showing broadened neutralizing activity against omicron subvariants. Limitations of this study include the small cohort size, differences in age among the cohorts, the unknown effect of previous exposure to SARS-CoV-2, and comparison of the vaccines at a single time point. These serologic data show an overall neutralization benefit with bivalent booster immunizations.
Comparing the methodology of the Cell study with the NEJM letter is above my paygrade, but that said I think the Cell methodology is superior. Cell includes up to four jabs (not just two), and includes breakthrough infections (Figure 2), so it’s looking at a population that’s far closer to the real world than the NEJM paper. I also don’t know what NEJM’s “better” means in terms of effectiveness. If it means what the MMWR study means (“30% and 56% among persons aged 18–49 years”) that’s not very encouraging, either. Next — and here I’m going to juggle power tools again — the NEJM letter lacks a mechanism. If you look again at Figure S3, BQ/XBB have no sera. So how was the NEJM’s putative “neutralizing activity” to have been achieved? (If we think of antibodies and antigens like a lock and a key, NEJM is not just trying to open a lock with the wrong key, the key is a Shlage, and the lock is a Yale.) Finally, the NEJM study doesn’t mention that the new subvariants ace out monoclonal antibodies, eliminating important treatment options. So I remain “alarmed.”
Immune Dysregulation
Dr. Anthony Leonardi is the foremost proponent of Covid immune dysregulation. This deep dive in the Tyee, “What If COVID Reinfections Wear Down Our Immunity?” gives the backstory[4] and explains the concepts.
By dysregulation Leonardi means three effects of COVID:
- The hyperactivation of many T cells [“one of two white blood cells that defend the body against foreign invaders”], which can prematurely age them
- The exuberant function of those hyperactivated T cells, which can then cause organ damage
- The exhaustion of those hyperactivated T cells, which implies they aren’t winning the battle against viral proteins they are supposed to defeat.
In other words, argues Leonardi, T cells are becoming hyperactivated by SARS-CoV-2 and are prematurely aging, harming organs, and becoming exhausted trying to rid the body of an immune-evasive virus.
Here is a study from Nature, which is alarming because it suggests that Covid can cause immune dysregulation not only in T Cells, but in monocytes, “a type of immune cell that [can] surround and kill microorganisms, ingest foreign material, remove dead cells, and boost immune responses.” Or, as the Cleveland Clinic puts it, “Monocytes are your cell’s firefighters.” They constitute between 2% and 8% of your white blood cell count. That’s a lot! From “Transcriptional reprogramming from innate immune functions to a pro-thrombotic signature by monocytes in COVID-19,” December 26, 2022:
Here, we examine the function of classical CD14+ monocytes in patients with mild and moderate COVID-19 during the acute phase of infection and in healthy individuals. Monocytes from COVID-19 patients display altered expression of cell surface receptors and a dysfunctional metabolic profile that distinguish them from healthy monocytes…. These results identify a potential mechanism by which monocyte dysfunction may contribute to COVID-19 pathology.
On this paper, Leonardi comments:
It looks like Covid suppresses innate immunity toward other viruses and Bacteria
This doesn't bode well for the severity of other infections that aren't even covid
Think of all the people saying "The worst cold of my life"
Mild covid is harming the response to the common cold https://t.co/xwiInnUbIj pic.twitter.com/aKEoH5dpHo
— Anthony J Leonardi, PhD, MS (@fitterhappierAJ) December 30, 2022
Oh. Oh good. (Leonardi might well have mentioned the cases of Strep and resulting sepsis in the UK as well.)
Conclusion
I do not use the word “ruin” in the headline lightly. At the very beginning of our Covid journey, on January 26, 2020 (!!), Nassim Nicholas Taleb and his co-authors wrote “Systemic Risk of Pandemic via Novel Pathogens – Coronavirus: A Note” (PDF):
The general (non-naive) precautionary principle delineates conditions where actions must be taken to reduce risk of ruin, and traditional cost-benefit analyses must not be used. These are ruin problems where, over time, exposure to tail events leads to a certain eventual extinction. While there is a very high probability for humanity surviving a single such event, over time, there is eventually zero probability of surviving repeated exposures to such events. While repeated risks can be taken by individuals with a limited life expectancy, ruin exposures must never be taken at the systemic and collective level.
Taleb defines a “ruin problem” as “one where outcomes of risks have a non-zero probability of resulting in unrecoverable losses.” I suppose it would be possible for some to consider a million people dead from Covid not ruinous — after all, we can always breed more — but taking such risks repeatedly sounds like a very bad idea, especially since we’re taking that risk “at the systemic and collective level.” And taking the same risk repeatedly is exactly what a policy of mass infection does.
If the papers I have presented are correct, the Biden Administration’s policy of mass infection has brought us to the brink of ruin. Vaccine escape is the direct result of the Administration’s mass infection policy. GM writes:
[N]ever before has such a virus received the opportunity to replicate so fast and so much. We’re talking several orders of magnitude more replication than usual. And these are the results.
In the worst case scenario, the health care system is right back where it was in Spring 2020, with no working vaccines. Moreover, it will be overwhelmed not merely with Covid cases — remember “flattening the curve”? Back when collective action was a thing? Good times! — but with all sorts of new infections brought about by Covid’s immune dysregulation abilities, as is happening in the UK now.
Even worse, the subvariants with demonstrated immune escape capabilities (BQ/XBB) are peaking and becoming dominant during the Christmas and New Year’s holiday period, especially on the East Coast, the fons et origo of the first Covid wave in early 2020 (a little in the Hudson Valley and Long Island, as those New Yorkers who could flee did do, and a lot in the rest of the country via air travel, as people who got infected in New York checked Covid in as part of their baggage). Worse than that, the Southwest Airlines debacle has meant that there have been entire families, nationwide, staying 24/7 in airports, which are Covid hotspots, for days. Worse than that, opening up China will — probably already has — expose us to whatever variants have been brewing in immunocompromised Covid patients in that country.
Can’t anyone here play this game? “The pandemic is over.” No, it’s very not. It’s deja vu all over again! How many times do we have to repeat? Maybe try something new? Before it’s really too late?
NOTES
[1] At least as a putative public health measure.
[2] Readers will note we’ve been following the expansion of the The BQ and XBB subvariants in Water Cooler, using both CDC and Walgreens data. (The data for both comes from Pango but we can use Walgreens as a check on CDC’s tendency to hide up-and-coming subvariants in aggregated data). BQ is currently dominant, but XBB is coming up fast. CDC’s NOWCAST model predicts that XBB will dominate soon, which is why many are saying it is already dominant.
[3] There follows some qualifying language that says vaccines work in principle, but for us the point of the study is that they are not likely to work now, which is when we need them.
[4] Having explained the concept, I don’t want to get deeply into the balance of the Tyee article, which you should read if you have not. Suffice to say that the Tyee looks at “six key issues, comparing his statements with what the scientific literature now says or suggests.” In every case, Leonardi was either on the money or still in the running. So he has form. Leonardi has been early and right, not (as NC readers know) always the most comfortable position to be in.


Excellent work, Lambert, and I’m passing it along.
Agreed – excellent work Lambert. I’m not sure there will ever be a political cost to the democrats. I think for there to be such a cost, the electorate has to have a place to turn. And as you state in the post, the repubs have failed to articulate a meaningful and rational alternative strategy.
> I think for there to be such a cost, the electorate has to have a place to turn.
Agreed.
And for decades, the perennial question has been what will that be? I think, maybe from a dash of hopium, that soon they will start paying the cost much like the American Whigs.
However, unlike 19th century political parties, both the Democratic and Republican parties seem to believe and act as if they are the American state and not just political parties. If either party actually starts to be threatened with replacement by another party, Homeland Security (what a fascist label that is) will declare it a terrorist organization and do to it much like was done to the old American socialists and communists.
Yes, thank you, Lambert. I have sent a link to my son and his family (they have a four-month old baby) and he travels regularly between New York, Chicago and Santa Fe and I want him to have the latest and best information on which to act.
Thank you for all the hard work you have done in compilying this important information.
Lambert – Your links in the first paragraph to the New York Times and the New Yorker both go to the Buffalo News which looks like an appropriate article.
Thanks, fixed.
The Buffalo News picked up the Times article, so I’m bypassing the paywall. The New Yorker link is now correct
Since it was Trump and the Republicans who first launched the “vaccines only” approach, based on Operation Warp Speed and ” Real Patriots don’t wear masks”, and since we have a Two Party System, the only way we will escape the bi-partisan consensus on Vaccines Only is if the Republican Party decides to break the consensus.
And since Trump is still the Spiritual Leader of the Republican Party, that means it is up to Trump to break the consensus when he runs for President again. If Trump were to run on the concept of introducing a fully layered containment and reduction approach coming as close as feasible to functional zero, then the Republicans might feel forced to follow Trump’s lead. And if Trump got elected on a platform of “stopping Covid the genuine Public Health way”, he might be able to force that way into existence. Perhaps conduct mass purges at CDC and fill all the emptied places with ” Covid is Airborne” hawks.
Can you really see Trump devoting the necessary discipline that would be needed to effectively pursue it?
Highly unlikely, at best. What’s more plausible is Trump (whose political juju is waning, in imho) trying to advance by stoking further divisions.
Well . . . there went my last hope.
Because if Trump won’t do it, and the Republicans certainly won’t do it without Trump leading the way, and the PMC Democrat Liberals are utterly against it, which at this point they are; then there is no one to do it.
Which means no one will do it.
Which means the minority of Americans who are covid-aware and covid-reality-based will have to keep eachother as safe and less-infected as they can in the midst of a civilization of depraved germ-spreaders. They will have to live like Early Christians in a slowly burning down Late Rome.
Covid is being minimized by private industry, the government and the media. For example, who knows that Pele died from Covid? Almost no one. Things are going to have to get a lot worse before changes can be made.
Pele died of colon cancer.
Cancers can be exacerbated by the covid “vaccines”.
You are asking for me to put you in moderation. Pele died of colon cancer. I can’t have you misinforming readers.
https://www.youtube.com/watch?v=KYVl5wtI598
Well, he wouldn’t have been in the hospital except he caught covid.
https://abcnews.go.com/Sports/wireStory/pels-family-covid-caused-infection-death-imminent-94464919
The claim was he died of Covid and that is false.
Moreover, CNN reported at the same time with more direct quotes from the MDs and family that the Covid infection was weeks before the lung infection and suggests the anti-cancer treatment was the primary cause of his immune system weakness:
https://www.cnn.com/2022/12/05/football/pele-hospitalized-lung-infection-covid-19-spt-intl/index.html
1. The daughter said Pele had Covid three weeks ago, as in he had gotten over it.
2. The hospital fingered the chemotherapy treatment, which is highly unusual, as in it = doctors pointing fingers at themselves.
As for ABC, “Covid” in a headline guaranteed to get more eyeballs than “side effect of cancer treatment”.
shit, ranger agent…why dont we throw in a government that cares about us;n;s, as well
the ghooberment doesnt belong to us
were random noise and cannon fodder and sheep for the shearin
The only way we will get a government which cares about us is if we can conquer the government and occupy and pacify it and staff it with those of us who care about us.
Simple but not easy. And maybe not do-able at all.
Maybe us can conquer smaller units of government at closer more local levels and make those smaller units of government into ours, staffed by those of us who care about us.
In the meantime, the covid-realists can live as much of a covid-cautious life as they can and if they (we?) begin visibly out-surviving the covid deniers and covid dismissers; some among the great masses of onlookers and bystanders may begin to ask us what our secrets are. That would be the time to tell them what we know and how we know it . . . and how the newly-interested may apply it.
> the covid-realists can live as much of a covid-cautious life as they can
One would hope that a clot-free circulatory system and a functioning brain would confer an evolutionary advantage. But perhaps not, or perhaps not fast enough.
Well yes. Why not have him sign up to Bernie’s policy agenda with universal healthcare on top, while we’re dreaming?
I can’t imagine anybody less likely to undertake such a course, especially as it would mean eating a lot of his past words and convincing his supporters to completely reverse position. To be successful, it would also require him to pay close attention to the evidence and learn what works and what doesn’t in practice, instead of just asserting his own idea of reality and expecting to wish it into being. Anybody want to lay odds on that one?
> Since it was Trump and the Republicans who first launched the “vaccines only” approach
I’m not sure of the timeline on this (or how coherent Trump’s policy even was). Certainly, shambolic though the process was, they were at least working to get PPEs. (I remember one story in the New Yorker, the kind of story they can still do well if they luck into it, of a highly competent general who was sent to a mill in Maine to straighten out a family feud that was crippling one of the only firms in the country that could make swabs, for testing. So there were weird pockets of competence.)
IIRC, the CDC (and WHO) were screwing up masks, and telling noble lies, but they were’t arguing there was no need to ever to use them, or actively and deliberately maligning people who wore them. I think the only truly consistent (and malevolent) force — leaving aside Big Pharma and of course capital — was hospital infection control, the “droplet goons” who from the beginning opposed both aerosol transmission and the means to mitigate it, and that faction is AFAIK independent of party. However, it took a long while to fight our way through to some understanding of what was going on there, though, both on the aerosol science level, and on the institutional level, where the difficulties of making a paradigm shift became evident.
I attended the American Geophysical Union fall meeting remotely in Chicago. The AGU gave one of their big prizes (the Bjerknes Prize) to Lynsey Marr who is an aerosols mavin specializing in fluid dynamics. She gave a talk in which the case for aerosol transmission is pretty clear for covid, SARS1, TB, measles, influenza and anthrax. She didn’t mention smallpox which is another nasty airborne transmission. I really despair how she and her colleagues have been fought and ignored by the MDs about this one. This seems to be the big egos of many of the MDs that if you aren’t an MD you have nothing to contribute to medicine.
It does not bode well for all of us. It is also setting back trust in public health enormously. If you want to be an elite, you have to be competent at it, and this seems sorely lacking…
I’m still masking in Montreal. Not many are, principally those of east Asian origins. Vitacore N95’s are pretty comfortable. My only problem with wearing one all day is my runny nose from allergies.
My students in university are showing real signs of physiological stress as they get infected again and again. Scary times without even mentioning the war.
Here’s a link to their work if I can successfully do this. https://www.wired.com/story/the-teeny-tiny-scientific-screwup-that-helped-covid-kill/
i was forced to become an expert on seasonal and environmental allergies by my youngest.
how, pray tell, are you having allergies, if you’re masked all the time?
not being a bitch, for reals…just keeping up the standards
i get that there’s pollen and whatnot in yer hair, and clothes, etc
I am owned by three cats to whom I am rather allergic, hence the runny nose. On the other hand, my feline masters make me laugh alot and bring much joy and warmth on winter (and hot summer) nights;^) They tend to show up and move in. There’s not much that I can do about them except submit and buy cotton handkerchiefs.
> Lynsey Marr who is an aerosols maven specializing in fluid dynamics. She gave a talk in which the case for aerosol transmission is pretty clear for covid, SARS1, TB, measles, influenza and anthrax
The RCT crowd is fighting this tooth and nail. They refuse to reframe airborne transmission as an engineering problem. So Marr remains, in important ways, siloed. (Here is “Parachute use to prevent death and major trauma when jumping from aircraft: randomized controlled trial” (BMJ) if you ever run into an RCT goon. Tell them they just volunteered to be the control. See KLG here on scientific authority generally.)
This may have been cited here before, but Eric Topol has an excellent discussion with Linsey Marr, mentioned supra – he says she’s
a civil engineer and leading authority on air quality, viruses, and the impact of masks. She’s a remarkable explainer and my go-to expert on this topic
It’s a half hour audio with transcript at
https://www.medscape.com/viewarticle/984232#vp_1
I thought I might send it to my wife’s niece, a dentist in Minnesota, in the hope it might have an impact.
Thank you Lambert. I’ve been following the Covid story on NC and Water Cooler since the pandemic’s beginning. This is as important as anything you’ve posted to date. Holy s**t!
Writing from Vancouver. It seems to me that all the public health authorities in Canada and the USA are on the same page: let it rip, get vaccinated, obfuscate aerosol transmission and don’t push masking too hard.
There is going to be a nasty reckoning. To you, Yves, all at NC and in the community, may I extend all best wishes for the new year. Let’s all continue to try our best to avoid being victims of these monsters.
Thank you for this, Lambert. I work for a medical school. The school is hosting a “New Year’s Gala” on January 6 replete with cocktails, and obviously not a mask in sight. At least 300 people are supposed to attend. There was a time when I thought highly of the organization I work for, and the people who run it. Those days are gone.
Brilliant, Lambert. Thanks very much.
So the best course of action was to rely on natural
immunity all along?
Shame on all those who spoke out about viral mutation as a result of mass vaccination.
Science be dammed. Anyone who listens to the government for health advice is now demonstrably loco.
saw this today in memex 1.1:
”I think this is what’s wrong with our political system. It’s organized to get people elected, then the people we elect do the work of big companies. And their work is to squeeze every bit of value they can out of the natural and intellectual resources of the world, and keep it for themselves. If they can kill something that’s worth $100 to reap $1 of value from the corpse, they see that as good business. That’s the approach that has got our species into the climate change corner we’re in. If you burn everything all you’ll have left to breathe are smoking corpses. That’s where we are in everything humans do. That’s why we feel a void for ourselves, collectively. We blame the government, but we’re the ones who believe the lies. We know they’re lying but we believe them anyway.
* Dave Winer, as part of a blog post explaining why he was so disappointed by Obama’s Presidency, despite having supported him in every way he could.
that, right there.
i consider myself a reluctant misanthrope…and yet, i;m a frelling Humanist!
i’m disappointed in my species, such as i’ve encountered.
less disappointed the lower down the socioecon ladder i go…which says volumes, to me.
its the system imposed from on high thats the problem…injected into our minds from kinder…
Enterprise…not Human.
You have this wrong.
Natural immunity is nonsense and anyone who says this in the context of Covid and coronaviruses has discredited himself.
Moreover, the high mutation rate is the result of a high rate of infection. Period. For instance, it’s widely believed that Omicron, which had a sudden, large number of changes to its spike, came about via a protracted case in an immunocompromised individual.
There is no natural immunity to covid. This has been proven repeatedly.
>>Never before has such a virus received the opportunity to replicate so fast and so much.
Actually, wouldn’t this have happened in pre-modern China or Rome, or even in the early modern era? Less people, less travel, but also less sanitation?
It’s like we’ve gone back in time before the germ theory of disease.
Not really, we have 8 billion people now.
It was 500M-1B back then, and not connected, so it mostly stayed in one place, burned through, and then it took time for it to come back.
That’s in general.
But we are talking about SARS viruses specifically.
Those were minding their own business in bats, with populations in the tens of millions and very small body size too. Until 2019…
This is a key point, and I’m not sure how widely appreciated it is: Pathogenic evolution leading to localized extinction or near-extinction of the host species is not only possible, it’s actually quite likely. Selection for short term advantages with huge long-term costs aren’t only a feature of capitalism. At the moment most humans on earth are part of a single web of transmission, and the prospect of something much closer to an extinction event than any of the famous plagues of the past is no mere fantasy.
There is a raft of archeological and genetic evidence proving that the ancient world was *highly* connected, providing little opportunity for a plague to ‘stay in one place and burn out.’ One of the best books I’ve read recently is by anthropologist and archeologist David Graeber and David Wenbrow titled ‘The Dawn of Everything, A New History of Humanity.’ They take the latest research in both fields to support their thesis that it is a mistake to think of pre-historic peoples as lonely bands of hunters forever doomed to inbreeding. Instead, they infer from the evidence, and it’s nowhere clearer than in genomic studies, that humanity has been on the move and intermingling for at least the last 100,000 years. [Note the continued hubbub over Goblecki Tepe, a 13,000-year-old pre-pottery Neolithic monolith site built when said humans were supposedly roving in ‘tiny bands.’] Science is still arguing about the length of time it took the medieval Black Death to reach Europe from its (genetic) origin in Central Asia, but we’d be forgiven for thinking it was a relatively short time if it spread by boat via the Black Sea and the Dardanelles. While I agree we are in a now single web of transmission, we underestimate the connectivity of humans paleolithic, neolithic, ancient and medieval, on all continents in what we now call the Old World. (Pity we have such little interest in examining plagues in the western hemisphere, even though LIDAR continues to reveal vast and sprawling kingdoms.)
There were pandemics in the ancient world as well.
Rome for example suffered from a number of plagues – a well known example is the Justinian Plague.
Plagues would spread throughout the world. The rate may have been slower without modern travel, but the plague still spread.
After the Western Roman Empire fell, other plagues still migrated long distances, a famous example being the Black Death.
See GM above. He is correct in saying there has never been such replication frequency before. Pop sizes, many cities with high pop density, and international air travel. Even as recently as 80 years ago, it would have been unusual to travel 60 miles in one day, when that is now a not-uncommon daily commute distance in the US.
There is plenty of research out there on ancient plagues. They generally travelled slowly – as slow as humans travelled overland or by sea. While insanitary conditions probably favoured water or parasite or fomite transition, it was probably harder for airborne viruses, apart perhaps from very densely populated cities which were relatively rare until the industrial revolution. The wealthy of ancient times usually spent as much time as they could on their country estates for a very good reason.
The slowness of transmission means that diseases usually spread very differently than modern diseases. Studies of the old Irish annals showed that many times plagues in Europe never made it to remote island areas, but when they did it was devastating, presumably because the populations didn’t have their immunity primed. Plagues often lasted for many years, as they moved around slowly finding vulnerable populations. Relatively isolated Japan often suffered horrible small pox outbreaks months or years after the wave had receded in mainland Asia.
I think its likely that the first ‘modern’ plague was the Russian Flu of the late 19th Century, so called because it seemed to have been spread rapidly by the new transcontinental railroads. Its now thought that this was a coronavirus.
in·san·i·tar·y
/inˈsanəˌterē/
– so dirty or ridden with germs as to be a danger to health.
“insanitary conditions”
Okay, that was a giggle, first just wondering how the spelling got past you and spellcheck. It didn’t. Then wondering how it got past me… I’ve never seen it spelled that way before. Then because of one letter, liking it better as an adjective.
The Mayan city of Tikal is estimated to have housed 100,000 people. You can pick a date between 200AD and 900AD to choose its apogee. Depending on your source, ancient Carthage held 700,000 people and ancient Persepolis as many and more. My only point is that history is littered with densely populated cities and with even more ancient densely populated gatherings of peoples. Think Stonehenge and Goblecki Tepe. Could they get on an airplane and fly 3/4 of the way around the globe in hours? No. But there were dense populations and gatherings from Neolithic times forward which were effective in spreading plagues even if they took a decade to burn through a continent.
My 80 y.o. mom managed to dislocate and fracture her arm yesterday. She is okay now, knock on wood, but the emergency room in Norwich, CT was full to the rafters; like nothing she and her friends had ever seen. She did get good care, maybe because she was screaming. Ordinarily she would now hire two friends (one in her 70s; one in her 60s) of her to wait on her day and night. But both of them have been sick for weeks with a bad cold and one of them also had strep throat. Since when do grownups get strep throat?
The Walgreens tracker is very high right now: https://www.walgreens.com/healthcare-solutions/covid-19-index. But as Lambert has said, who goes there? Most people I know don’t bother to test, but if they do test they use a home test.
I go to Walgreens when I want a PCR test, and I’ve referred other people who want PCR tests to Walgreens. They don’t always have PCR tests available, so sometimes I have to try multiple times, or go to a less convenient location. Because the system is not entirely convenient, among my acquaintances, only people who are highly motivated to get PCRs tests go there for covid testing.
How will the elites fare when they march forward, animated by their personal risk assessments, into multiple personal infections by COVID and all the other viral and bacterial and fungal, et al. infections that are floating around and gestating out here? Will they die in large numbers from the primary infections and the effects of immune dysregulation and damage to epithelial and other tissues from the effects of the mRNA “shots” (it’s a lie to call them vaccines? Will the “common cold” take them down?
I wonder how the Russians and Chinese will fare also. This is how species die, I believe. Maybe having not had the blessings of Pfizer and Moderna, which are building huge new capacity to not only ramp up Covid shot production, but touting their tech as maybe a magic solution to maybe most other ills. All protected by the state institutions they own by virtue of “campaign contributions” and other forms of bribery.
Stupid effing humans.
I’m sending this article to all the friends and family I care about, though most of them are believers in the efficacy of “shots” and at the same time, the inevitability of getting the disease. Amazing tenacity of cognitive dissonance.
And thank you for this work. You deserve a medal. Not that, if this analysis is right, it will mean anything going forward.
Have you run across a character named Jacob Dreizin? He has been screaming from the right-wing ramparts of his blog about this for over a year. Used to have a lot of Repub insiders subscribed to his newsletter and now blog. https://thedreizinreport.com/
How can wisdom penetrate the infinitely flexible and apparently unbreachable membrane of the Beltway-Acela-Corporate-Academic Bubble, which nonetheless seems fully permeable to huge flows of money and stupidity?
“Will the “common cold” take them down?”
like in war of the worlds?
one can hope!!
Great article, Lambert. I have to admit I went down the rabbit hole on the Casey Stengel quote link. I wonder what it sounded like when he and Yogi were discussing something?
> I have to admit I went down the rabbit hole on the Casey Stengel quote link
So did I!
Um, I’m not sure what to make of this:
“Covid continues to circulate, with a 22% increase in hospital admissions recorded in England between 7 and 14 December. Dr Stephen Griffin, a virologist at the University of Leeds, said: “The difficulty is that we don’t have freely available PCR tests any more, and a lot of people who are vaccinated [against Covid] don’t necessarily show up on LFTs if they are infected.”” https://www.theguardian.com/science/2022/dec/30/flu-covid-rsv-britain-ill-bugs-viruses
Vaccinated people (who are infected) are less likely than unvaccinated people (who are infected) to show up positive on lateral flow tests???
I have seen different discussions amongst doctors concerned about testing but not anything related to vaccines. Virus is always mutating, so who knows?
No freely available PCR tests is another stupid action in a long line of stupid actions from the UK government where COVID is concerned.
GM does not buy this. Via e-mail:
Unvaxed in UK now thought to be over 25%, how much over is unknown as the ONS data is ‘limited’.
Many studies in UK are showing vaxed up to 3x more likely to be reinfected than unvaxed. All the fears of using a non-sterilising vaccine are coming true.
I agree with the thrust of this article that covid ‘vaccines’ are worse than a chocolate teapot, but I think there is no more truth in the benefit of masking in most ordinary circumstances. They also have now acquired an association with control and lockdowns.
I have to sadly confess a lack of confidence in masks, even though I still wear them on the bus. It’s just that these variants are so contagious I don’t think the masks will protect me. I do nasal washes with providone iodine twice a day if I’ve been among other people. I live alone. I also open the windows on the bus, which are sadly often closed as very few other people seem to think about this.
Many studies showing masks do very well protecting us. Clothe masks have the lowest protection, but they still do about 50%. Only goes up from there. A good N or K95 are great. No mask is 100% but at the very least, you bring down the amount of virus you take in, which helps you when the infection kicks in.
My family and I have been masking since the beginning. We haven’t caught it and I have a 13 year old in a school with 1250 other teenagers. We get boosters and mask.
Thank you for presenting these results, especially the MMWR.
I just saw this Tweet that I guess we’ll see in the Water Cooler soon: Walgreens positivity rate eclipses 40% for first time ever.
https://twitter.com/CovidDataReport/status/1609936405165215745
Speaking of part of our pharmacy duopoly, I got a PCR test at CVS on Thursday morning. It’s Monday evening… no results back yet. Grrr…
> I guess we’ll see in the Water Cooler soon:
Yes, I have’t looked at the charts in some days and I’m anticipating good deal of excitement.
I think I’ll stock up on toilet paper.
> I think I’ll stock up on toilet paper.
Plus N95s or Darth Vader respirators, Povidone Iodine, your various sprays (VirX, etc.) and medicines of choice. It couldn’t hurt to take some precautions. These things are always good to have around the house in any case. (I suppose a prepper might call this form of kit a “Stay Bag.”)
Because of his strategy, Biden will either:
1. Perish because of his old age and reinfection(s).
2. Or he’ll get infected again and his doctors will pump him full of experimental stuff and he’ll survive, Hopefully afterwards they’ll share the secret recipe …
If Biden gets Covid and recovers again, Americans will however think that “if an old man like Biden can survive one or two reinfections, how bad can it be really?”
Excellent writeup, Lambert. Thanks! Scary.
Thanks, Lambert, for another great post on this.
If the existing vaccines don’t work against the new variants, and given that we are supposed to perform “personal risk assessment” on the basis of jiggered data and the deceptions of Big Phrama, I keep arriving at the conclusion that it makes little sense to opt for any of the current boosters, bivalent or otherwise.
The only hope of improvement in this generally horrible situation seems to lie in what Dr. Leonardi already proposed: “an excellent nasal spray vaccine combined with long-term changes to public infrastructure”. However, this raises the question of how we should define “excellent”.
If other readers have ideas about the parameters of “excellent” (i.e., what we should be angling for), I’d be curious to hear.
The scary thing about the CDC/MMWR results is that the bivalent booster was going up against a BA5 dominated world since the results were based on tests run from September 14th to November 11th. These boosters seem to have all the effectiveness of a dog chasing its tail.
And Pfizer’s and Moderna’s fantasy world of boosters every 3 months looks rotten, too, since the results “among persons for whom 2–3 months and ≥8 months had elapsed since last monovalent dose” were a lot worse for the more recently boosted.
https://www.europeanpharmaceuticalreview.com/news/177948/moderna-finalises-plans-for-uk-mrna-vaccine-manufacturing-centre/
Moderna, Inc. has finalised a strategic partnership with the UK government to establish a state-of-the-art mRNA vaccine research, development, and manufacturing facility in the UK.
This milestone follows the agreement in principle between Moderna and the UK Government, announced in June 2022.
The Moderna Innovation and Technology Centre (MITC) is intended to provide access to a UK-made supply of COVID-19 jabs. It also has potential to develop vaccines for other respiratory diseases, such as flu and respiratory syncytial virus.
Fantasy world indeed. I know a professional who had the bivalent booster but then tested positive for Covid, which was described as “the worst cold I’ve had”. A month later, he was still recovering.
This is why I’m wondering about the nasal vaccines, though I assume all are not equal (it seems some are just nasal versions of the vaccine tech we’ve already got, e.g., AZ), and somewhat at a loss of what exactly we should be looking for. Lambert has posted several round-ups of the nasal vaccines (NC, Jul 22, 2021, and Mar 27, 2022), followed up by a study of SA58 spray, just the other day:
https://www.medrxiv.org/content/10.1101/2022.12.27.22283698v1
And a recent article in (yeah, I know) The Atlantic (posted in the 01/01/2023 NC links):
https://www.theatlantic.com/health/archive/2022/12/covid-mucosal-vaccines-protection/672544/
This article, however, sounded a dubious note, e.g.:
The writer of the article sounds very much resigned to endemic COVID, which is perhaps why it didn’t receive any discussion here (or maybe NC readers also have a touch of The Atlantic fatigue; fair enough).
Still, I am wondering if nasal vaccines could help to improve the global picture, and which of the many different projects/products we should be looking out for.
In the meantime, you can swab your nostrils with a 1% povidone iodine solution, or use it as a gargle and nose spray. But probably needs to be done at least 2x a day if you are out and about, so a nuisance compared to a nasal vaccine.
Yeah, I am using that now. The taste was a bit weird but now not so bad. I don’t think it can really get all the surfaces of the sinus, tho, and am not sure about doing that daily.
Is there a commercial 1% Povidone Iodine solution? I’ve seen recommendations for Xclear and tried to research that but all I find is their own studies supposedly proving how well it works which may be true but… Other people we know seem to use everything from saline sprays to neti pots – I guess this is all part of ‘personal risk assessment”..?
No. It isn’t hard to dilute a 10% solution to 1%. I store in a wine bottle with a screwtop.
Hey, I’m ready to try it, but this doesn’t make sense to me…
“Povidone-iodine is a chemical complex of povidone, hydrogen iodide, and elemental iodine.[3] It contains 10% Povidone, with total iodine species equaling 10,000 ppm or 1% total titratable iodine.” [emphasis mine] Wikipedia
Long ago I cleaned milking machines with “Iosan” (Dynachem). Hard on hands skin.
Many questions this site has no info on, though automatically it’ll take you to whatever question. https://www.webmd.com/drugs/2/drug-32658/povidone-iodine-oral-mucous-membrane/details/list-precautions
> nasal vaccines
There is also this concept: A randomized, placebo-controlled trial of a nasal spray solution containing broadly potent neutralizing antibodies against SARS-CoV-2 variants in healthy volunteers (linked to 10/17).
The brand is CoviTrap; I can find it online here, but I’d be more confident with a branded vendor like Walgreens or Boots.
Thank you so much for this pointer. I will investigate !
> Thanks, Lambert, for another great post on this.
[lambert blushes modestly]
IMNSHO, vaccines are exactly what we should be making “personal risk assessments” about (no mandates. We are, after all, allowing them to be injected into our bodies). The non-pharmaceutical interventions should have been mandated, being no risk and high reward.
The Biden Administration — and the (hegemonic) PMC base of the Democrat Party — got Covid policy 180° wrong. And it was their job, especially the (hegemonic) PMC’s job, since their our governing class, to get it right. Instead, we’ve had debacle after debacle, followed by blameshifting, doubling down, and now embubblement:
Fantastic post but I find this comment confusing:
The Biden Administration — and the (hegemonic) PMC base of the Democrat Party — got Covid policy 180° wrong. And it was their job, especially the (hegemonic) PMC’s job, since their our governing class, to get it right.
But, per your PMC class analysis, how does/can the PMC act counter to the interests of the capitalist (profit-seeking) class, since they are in a subordinate position to that class (which is the class that ultimately employs and empowers them)? Also, honest question, how can a subordinate class, or fraction of a subordinate class, be hegemonic?
I think there is an inconsistency in your argument. I think a consistent class analysis would suggest that the PMC (perhaps after some initial confusion about what the class interests of its capitalist masters was) got Covid policy exactly right, which is carrying out the interests of the capitalist class that employs and empowers them. Was there anything in the response to Covid that differed from our capitalist/PMC health care policy in general? Minimize cost-effective prevention, maximize profitable treatment?
>>I keep arriving at the conclusion that it makes little sense to opt for any of the current boosters, bivalent or otherwise.
Something I’m struggling with too. Haven’t gotten the latest booster yet, but thinking of getting it soon. But having some doubts about it. I do have the first two jabs plus two boosters.
Watching our pandemic strategy is like watching a novice win a massive pot in poker in the first few hands but lose all of it in the next 30 minutes to everyone else.
Couldn’t lock it and play conservative, had to take crazy shots just because you were up.
Depressing…..
Thanks for this excellent post.
My most representative professional class friend informed me just yesterday that the covits is turning less and less virulent. This is contrary to my own experience (positive 10/29/ “mild” symptoms, 1 night of fever, 7 days sick, vascular issues from say day 15-45, not mild, and now day 63 or so pretty much normal)
In san diego no masking mostly, expecting a wave but we’ll see…
> the covits is turning less and less virulent
That’s a happy myth, a teleology, that people, especially people with faux expertise, like to believe.
Trivially, there’s no reason to believe that BQ/XBB are less virulent because the data’s not in. (Further, the proponents of “less virulent” have form; they claimed Omicron was “mild” and it turned out not to be.)
Less trivially, there is not the slightest reason to believe that the virus must evolve to be less virulent. To anthropomorphize, all the virus wants and needs is to spread from one host to the next as efficiently as possible. Whether the host experiences “mild” symptoms are drops dead is immaterial to the virus; it will have moved on to the next host in any case.
One more reason not to keep repeating the experiment….
I am not a scientist, but my understanding is since the virus needs live people for opportunities for infection, the fewer opportunities the greater the evolutionary pressure to not kill (and possibly not injure too much); the more opportunities, the evolutionary pressures are for rapid growth and increased lethality. If there are bunches of people around, explosive discharge of bodily fluids onto every one and everything is great even if it almost immediately kills the victim. If almost nobody around, then keeping the victim alive (and mostly well) spreading the virus with some light sneezing is better.
You can think of this as loading the dice for the random mutations that can make a disease more or less deadly. But it is still just chance and most of what the government is doing is loading the dice for worse Covid variants: lack of masking, no quarantines, not increasing ventilation, and encouraging people to gather in large groups. It is almost as if they want to make things worse.
No, this is completely incorrect. Covid is most contagious the day before and 1-2 days after symptom onset. That is way before it kills anyone. Fatality is no barrier to contagion for a virus like Covid that transmits quickly.
As always … yeoman’s service … a strong start to 2023 indeed.
I’ve quote-tweeted Biden’s quod-erat-demonstradum-tweet (via #Twitter) from earlier today with this article.
Following Anthony Leonardi is immensely valuable but so painful when you realize how long he’s been saying these things and how bad things are getting. Good grief.
We need to be defiant in hoping and working for better outcomes for the masses.
This is an invaluable service for us, your readers.
An effective vaccine is a chimera against a virus that mutates naturally by being single stranded genetic material. This is why coronavirus colds keep reappearing. From the beginning of the pandemic, each individual is playing Russian Roullette of being exposed to the virus with sufficient time and dose to get infected. All one can do is reduce exposure and try to keep healthy.
The real shock is that governmental Public Health Services across the world are now totally ineffective. A number worked against the Wuhan virus but all nations have decided to let the Omicron variant rip through their populations.
NGOs took over the global response to the pandemic to increase corporate profits. Neo-Politicians are simply unwilling to spend money to save human lives and prevent illness. But they are willing to finance patent-able drug treatments since they get a cut.
What is scary is the reports of prior COVID infections increasing the likelihood of children being hospitalized with RSV and flu as a result. A highly contagious airborne human immunodeficiency virus freely transmitted in schools is a societal nightmare.
Also, hidden is the impact of long-COVID illness on millions of workers. Blamed on the weather, Southwest Airlines melt-down and Union Pacific two-week embargo of service in Iowa, Minnesota and Wisconsin are due to the lack of workers and the transfer of a business’s wealth to stockholders and managers.
A breakdown of the West is a certainty if the Ukraine proxy world war keeps escalating, if there are rolling electrical blackouts, and if there are not enough workers to produce and deliver goods/food or pick up the garbage.
The vaccines are working super well in Israel. The later’s about to declare the pandemic to be over, https://www.theyeshivaworld.com/news/headlines-breaking-stories/2152771/about-time-israel-to-declare-covid-pandemic-over-downgrade-it-to-flu-status.html
Your claim is not warranted by your link. Plenty of countries (the United States and China come to mind) have declared the pandemic to be “over” (or even endemic) while infection and death were still abnormally high. This has nothing to do with the success or failure of vaccines, and everythingto do with commercial interests. In addition, your link doesn’t even mention vaccines!!
In the meantime, the evidence grows that exposure to outdoor light can help prevent and even treat Covid. In particular, the infrared portions of the light spectrum appear to be the most effective. These are of course, most prevalent at or near sunrise and sunset.
Unfortunately, the shift to LED indoor lights and energy efficient windows that prevent the passage of infrared light basically starves us of the beneficial aspects of light when we’re indoors
A trial for hospitalized patients using 940 nm infrared light had significant benefits including a four day shorter hospital stay compared to placebo was just published. See these two videos:
https://youtu.be/9eEyWlbToI4
https://youtu.be/ZdiUnmpOgqE
If you could just give a link to the study and even quote from it (see Links for how this is done) that would be very useful. Reading is far more efficient than watching and listening.
Thanks!
Perhaps an evocative subheading for the COVID sections of the Links and WC pages could be:
“Something Awful this way comes”
IIRC, the Ray Bradbury book that inspires this suggestion had a happy-ish ending, but evoked a sense of dread throughout much of the story.
So basically, beyond whatever damage SARS-COV-2 itself does, it is also a force multiplier that enables ‘every day’ pathogens that might otherwise be survivable without a significant cost and makes them costly.
Oops.
Happy new year indeed.
Masks and Corsi boxes and when temps allow, open window are your friend! Plus Vit D and zinc and sadly compulsive practices like Neti pots or my fave 1% povidone iodine. You need to use many angles to improve your odds.
Some variation of all of these things I use, but it is tiring emotionally to do this because I have a constant reminder of the CDC and the “healthcare” system consistent incompetence; I worry about my Mom and other members of my family all of whom are fully captured by the PMC lies. Not surprising as they are members, but they might die because of the propaganda being fed straight into their minds; wearing a mask is a reminder of that possibility. Just how often will their children get sick?
I guess the point of my ramblings is that the constant efforts to not get sick, or at least not too sick too often, while seeing my family does not is a dreadful thing. And the efforts, and the information I find, which I would like to pass on to them, seems unsharable. A kind of hell much like that of caring for an addict especially if they can’t even acknowledge the possibility of being an addict.
I can’t even have the satisfaction of being angry at the addict’s foolishness, because of the vast and great efforts being made to make them suicidally ignorant. If it was just their own mind’s BS, I could possibly break through.
So I get to see people I love who are smarter and usually wiser than I…
I want to finish that sentence and I can’t for some reason. What is the point and even if I remain healthy what good is it, if everyone else is not? They could get wise, which is a real possible and would be fantastic, and is an encouragement for me to keep talking, but this situation of multiple epidemics seems destined to keep going on and on. And I am reminded of all this almost every time I mask up.
> What is the point and even if I remain healthy what good is it, if everyone else is not?
“Everybody” is not. The trick is to find the “remnant,” to put it in Biblical terms. As here. Or in school systems that are remasking, as in Boston.
Hey Lambert, found a good analogue for “x has form” in that list of Casey Stengel quotes, in case you’re looking to mix things up:
> “I don’t know if he [threw] a spitball, but he sure spits on the ball.”
Genius!
Good writeup.
I offer 3 things:
1) I don’t think there’s any evidence that the vaccines are less effective in doing their job (preventing severe disease and death), but we still could likely be seeing a blunt force trauma to the healthcare system due to the shear volume of cases we are about to see (again). Due to the tremendous transmissibility growth coupled with waning immunity from both infections and non-boosted vaxees AND almost complete abandonment of mitigation measures.
2) re: China – I’m equally concerned (maybe a little more actually) of the variants this large amount of cases are about to generate in the US. China’s variant of choice, if my sources were correct, is BF7, which was here in September and will certainly be outperformed by XBB.1.5
3) the immune dysfunction issue is a hot topic amongst immunologists. Looking at the flu season, it would lend a pretty large body of evidence AGAINST this theory, because although it started earlier than expected, it didn’t exceed (in terms of severity: hospitalizations) other bad flu seasons we’ve had in recent history
> I don’t think there’s any evidence that the vaccines are less effective in doing their job (preventing severe disease and death),
That’s how “their job” is perceived at this point, because of an extraordinary “whole of PMC” propaganda campaign. The original pitch was that — like the vaccines so many of us had as children — the vaccines were sterilized. That was the only reasonable interpretation of the “You are protected” talking point originally propagate by Biden, Walensky, Harris, et al. When that didn’t pan out, they moved the goalposts.
Lambert:
Japan seems to be a strong counterexample to the idea that stricter measures might prevail.
Cases are at all time highs despite high levels of both NPIs and boosters…
End of Japan COVID curbs triggers surge in visitors to near 1 mln in November Reuters.
They scrapped their curbs.
Anecdotally, I can report that while the practice of masking in public remains the default attitude in Japan, there are more and more people without a mask, even on trains. The right-wing govt has been pushing for a let-er-rip policy, releasing PSAs that it’s okay to remove masks outdoors, even as the current wave of infections is still ramping up. During a visit to my local city office a few weeks ago, I noticed they have a video kiosk in the lobby, with a putative ‘medical expert’ being interviewed in TV news format, and said expert emphasizes the importance of hand washing, with no mention that the virus is airborne. So, the Japanese govt is also onboard with disinformation campaigns. It’s not surprising, I guess, as tourism and hospitality are big business in Japan, and they want all restrictions removed. It’s suggestive that Osaka, a smaller, more right-wing and pro-business city, currently has more active cases than Tokyo (80,122 vs. 53,086).
> During a visit to my local city office a few weeks ago, I noticed they have a video kiosk in the lobby, with a putative ‘medical expert’ being interviewed in TV news format, and said expert emphasizes the importance of hand washing, with no mention that the virus is airborne.
Propaganda works, doesn’t it….
Thanks for the field report. Please continue to keep us posted!
NOTE So, in fact Japan is not a “counter-example” at all. It is, in fact, an example of all the social pathologies we have been documenting in exhaustive detail, brought about by policies of mass infection for profit.
Flew a 10 hour flight yesterday and there were 6 masked on a packed 767.
Seems to me that complaining about this at this point is pissing in the wind.
Two-way masking is superior, besides indicating a healthy society, but one-way masking is not nothing.
I don’t see taking safety measures as “complaining.” That seems like an odd frame to me, equal in value to your putative “counter-example” above.
Adding, why would you want to piss in my wind? Because that’s what deliberately spreading an airborne pathogen is like. Except more deadly, and not a mere matter of common courtesy or basic ethics.