Our mini-fundraiser for Water Cooler is on! As of this hour, 148 donors — our goal is 250 –have already invested to support Water Cooler, which provides both economic and political coverage, to help us all keep our footing in today’s torrent of propaganda and sheer bullsh*t. Independent funding is key to having an independent editorial point of view. Please join us and participate via Lambert’s Water Cooler Tip Jar, which shows how to give via check, credit card, debit card, PayPal, or even the US mail. Thanks to all!
By Lambert Strether of Corrente.
Most of the liberal Democrat opposition to TrumpCare, both in its House and Senate manifestations, has focused on how many people would be thrown off the rolls; for example. (Left opposition to TrumpCare focuses on creating the universal direct material benefit of Medicare for All.) This is a smart tactic, because it piggybacks on press coverage (fueled by the headline numbers from the CBO reports), and it reinforces the psychology of loss aversion. It’s also photo- and protest-friendly[1]. Strategically, I don’t think it’s so smart, for reasons I’ll get to in a moment.
In this post, I want to take a less analytically impoverished approach — to be fair, I haven’t invested most of my time over the last six months ginning up a Red Scare and fomenting a war with Russia, unlike liberal Democrats — by looking at the BCRA’s Medicaid caps[2]. Medicaid caps will permanently crapify the program, and hence are far worse than one-time cuts in the rolls, bad as those are. (The distinction is equivalent to fighting Tory hospital closures in the UK, and recognizing that the Tories are playing a long game, and wish to destroy the NHS altogether by selling bits of it off, both so their cronies can profit, and because ideologically, they’re neolibeals, and that’s neoliberals do.)
Here is an explanation of how Medicaid caps will “work” under the BCRA. From an important post in Health Affairs, “The Downstream Consequences Of Per Capita Spending Caps In Medicaid“:
Recent federal reform proposals from House and Senate republicans would change the current financing system in which the federal government guarantees a share of total program spending to states to one limiting federal cost exposure by setting a per capita cap on federal payments to a state.
A change in the Medicaid program to a per capita cap financing system is included in the House-passed American Health Care Act (AHCA) and in the Senate-proposed Better Care Reconciliation Act of 2017 currently under consideration. With the Congressional Budget Office estimating that the Medicaid proposals in the AHCA will cut federal Medicaid spending by 25 percent by 2026, much attention has been given to the effects of such cuts on decreasing the number of individuals enrolled in Medicaid and increasing state budgets. Much less attention, however, has been given to a related but critical question: How do the reforms affect who enrolls in and gets care under Medicaid? From the lens of economics, we draw an analogy to per capita payments in health insurance markets and explain how the currently proposed reforms threaten the core programmatic purpose of Medicaid by incentivizing states to limit care and coverage to the states’ most vulnerable residents.
And:
Federal funding for Medicaid creates a national safety-net[3] health insurance program. Without federal funding, one might expect a classic “race to the bottom” among states to reduce state spending (and the accompanying taxes) by weakening their Medicaid programs. Federal policy for Medicaid prevents the race to the bottom by conditioning funding on both state spending and on the fulfilment of certain safety-net requirements, such as eligibility for statutory categories of individuals and benefit and access requirements.
(You say “race to the bottom” like that’s a bad thing!) Here’s how the caps would work:
It is not hard to envision Medicaid, under a per capita spending cap system, working as poorly as the early version of Medicare Advantage. While states are not for-profit insurers, as they grow to understand that it is financially difficult (or even impossible) for them to enroll a disproportionate number of sick individuals in Medicaid, they will likely shift enrollment efforts to less “risky” groups, such as the healthy and the young. States may be less eager to enroll or reenroll sick Medicaid recipients. Such incentives could, for example, manifest in the form of fewer enrollers at and less streamlined enrollment procedures for safety-net hospitals. At the same time, states may be much more likely to send enrollers to schools or community health centers where they can find young relatively healthy children and families. Alternatively, states could take a page out of the Medicare Advantage playbook and modify the services they offer to make them more attractive to young families and less attractive to older, sicker individuals.
Won’t that be great? Dealing with Medicaid is going to be like dealing with a private health insurance company, because under the BCRA, the incentives are so similar! (And because conservatives, like Tories, play the long game, a crapified Medicaid will be ripe for ultimate abolition.) And yes, this will happen:
A key question is whether or not such economic incentives are strong enough for states to act upon. The case seems clear that they are. While per capita cap proposals do specify different payments for each eligibility group, there is enormous variation in spending across and within eligibility groups in a given state that creates obvious “winners” and “losers” from the state’s point of view.
(Do note that nobody at Health Affairs has taken out their Communist Party card; it’s a well-respected, mainstream publication.) Kaiser Health News makes the same argument in “What Could a Medicaid Per Capita Cap Mean for Low-Income People on Medicare?” The structure of the AHCA is a bit different, but it too has caps:
Policymakers are giving serious consideration to [converting] Federal financing for Medicaid [into] a per capita cap model (such as under the AHCA) or block grant, both of which aim to limit and make more predictable federal spending on Medicaid and provide states more flexibility in their management of Medicaid spending. …
Under current law, the federal government matches state Medicaid spending at a rate determined by a formula set in statute. Federal spending increases in response to the rise in the cost of providing care to enrollees, with no limit on total federal contributions.
In contrast, under a block grant or per capita cap model, federal Medicaid spending would rise at a specified growth rate, irrespective of the actual rise in Medicaid spending in a state.
Translating, caps would make it impossible to fund health care for an epidemic under Medicaid. Jackpot! More:
Limits on federal spending could put pressure on states to limit Medicaid spending over time, if Medicaid spending increased faster than the growth in federal contributions.
Creating a race to the bottom. And:
The impact of a block grant or per capita cap would also depend on underlying costs drivers that may vary across states. For example, states that experience a relatively rapid increase in labor costs (e.g., for nurses and home care workers) may have greater difficulty absorbing costs than other states, if federal contributions are capped. The effect for any given state would also vary with the growth in average health care and long-term care costs per person, and states in which Medicaid costs grow relatively rapidly would be more challenged than other states to find the resources to care for their residents.
Bonus points for screwing the unions!
Finally, Brookings makes the important point that we shouldn’t confuse the BCRA “cap” with capitation (bad as that is under HMOs/ACOs). Looking at data from the 2000s:
Due to the “one-sided” nature of the AHCA’s per capita cap, there would have been no winners among the states, only losers. States receive reduced federal matching funding if their spending is above the AHCA cap in a given year, but do not receive additional federal funding relative to current law if spending is below the cap… This means that no state would have received more funding under a per capita cap than under current law in any year. This is an underappreciated feature of a per capita cap, which greatly magnifies the federal budgetary savings from the proposal. It is also an important difference relative to true capitation or block grant proposals under which a state would receive a fixed payment for each enrolled individual or for the program overall.
I’m sure there’s plenty more wrong with the BCRA caps, but if dull normals like Brookings, Kaiser, and Health Affairs have, well, concerns about it, I think we can conclude it’s pretty bad (and those of you with moderate Republican Congress critters might consider focusing on the cap when you chat with them during the coming recess).
Let’s now turn strategy, to the reasons liberal Democrats find it difficult to focus on capping (and gutting) Medicaid, preferring instead to focus on enrollment. Those reasons are implied by this chart from the CBO’s cost analysis of the BRCA, presented yesterday, which I have further annotated (in blue):
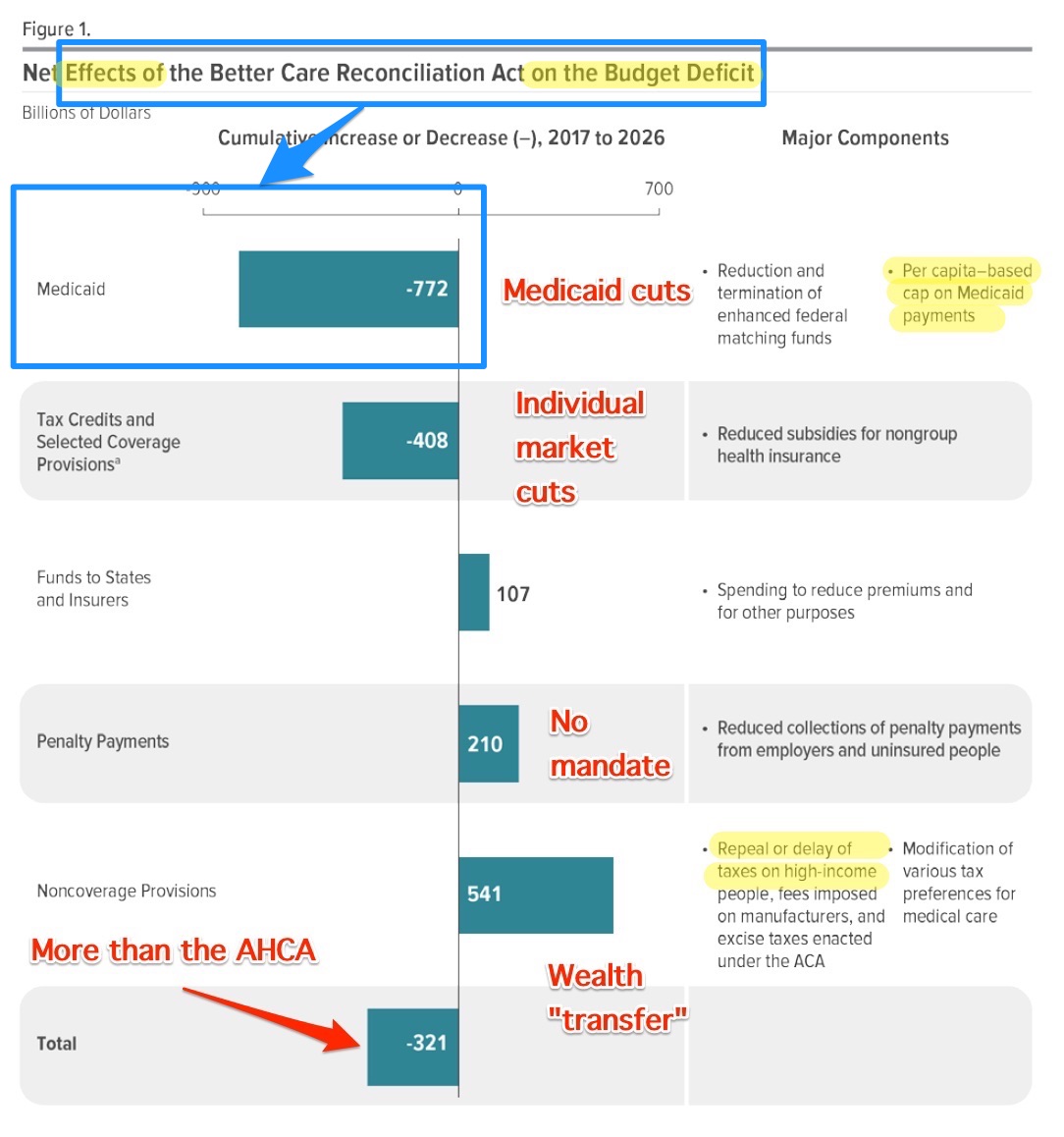
Even assuming policy good faith by the Republicans — I know, but bear with me — on Medicaid cuts, they have to answer as Willie Sutton did when asked why he robbed banks: “That’s where the money is.” That is, given that Medicare is not (yet) on the cutting block, “bending the cost curve” on Medicaid is the only place where deficit reduction can be seen to be made. And the Democrats are in zugzwang; they have no good move. The Republicans argue that cutting Medicaid is essential to reducing the deficit, and have proposed a method to do so. In response:
1) Liberal Democrats cannot argue that ObamaCare bent the cost curve, because it did not (spending decreased during the Great Recession, for obvious reasons).
2) Liberal Democrats cannot argue that the reducing the deficit is less important than saving lives by providing health care, because they don’t believe it; they believe in “fiscal responsibility.”
3) Liberal Democrats cannot argue that Medicare for All is the better alternative to both the ACA and the AHCA/BCRA even though it would save the country — although not the Federal budget — well over $400 billion dollars a year and thousands of lives — because they don’t believe that, either (“never, ever”).
4) Liberal Democrats have yet to answer the question why it’s terrifying that 540,000 people will die in the next decade under the AHCA/BCRA, but not terrifying that 320,000 will die under the ACA. They have no moral standing at all.
In short, liberals cannot address the central conservative concern (again, assuming good faith) of deficit reduction, since in fact they agree with conservatives. Hence, they open themselves to Medicaid cuts (“the money has to come from somewhere”). And liberals cannot address the central left concern of universal coverage, because (assuming good faith) they don’t believe in it.[4] So they are left in the incoherent position of supporting existing and partial enrollment, while accepting the key rationale that prevents them from expanding it. No wonder they’re in trouble, electorally.
Conclusion
In a post this short, I don’t think I need a lengthy peroration. Again, I think the well-supported position that Medicaid caps will create a race to the bottom between the states, ultimately destroying Medicaid, would play well with “moderate” Republicans (like, for example, Susan Collins), so be sure to mention it when you communicate with your Congress critters over the recess, or when you write your letters to the editor.
NOTES
[1] Rant: Here is a typical liberal headline from Slate: “Americans With Disabilities Should Be Terrified.” Maybe some consultant told these guys that “terrified” was good for clicks; I don’t know. Suffice to say that I’m sick of headlines like this, even if they’re true. Imagine I’m in a crashing plane. Do I want the flight attendants running up and down the aisles screaming “Be terrified! Be terrified!”? Or do I want real information that will help save lives? I wish liberals, and especially those in the political class, and especially those in the press, would stop projecting their own terror at lost power and influence onto the rest of us. They’re creating the worst kind of echo chamber.
[2] One baseline for how bad the health care debate still is: Eliminating Medicaid estate recovery (see NC here, here, and here) still isn’t on anybody’s radar, at least in the Beltway. Fix that for us, wouldja Neera?
[3] Note that the “safety net” trope is directly opposed to the concept of universal direct material benefits. The policy concept buried in the trope is that most can make it across the tightrope safely, and only a few will actually fall and need the net; this view is a wee bit optimistic in 2017. Also buried in the concept, if we go by experience, is the idea that as you fall through the air, thinking happy thoughts on the way down, you will encounter a series of gatekeepers and rent collectors who will ensure that you really are falling, are worthy of landing in the net, as opposed to on the ground, will fall onto the right part of the net, and so on. Supporters of health care as a universal benefit don’t think there should be any such tightrope in the first place.
[4] To be fair, the liberal Democrat base of credentialed gatekeepers and service providers derives material benefits from the artificial complexity of ObamaCare, which is, in a way, a jobs guarantee for them. So there’s that.


So what we seem to have here is like the Clinton welfare “reforms” of Clinton Era I (Bill). Neoliberal destruction of programs under the cover of fiscal responsibility.
The liberal class has a coda di paglia, as the Italians say, which means that their tail of straw prevents them from going too close to the fire. I would reinforce that the liberal coda di paglia is self-affixed. They can take it off at any time–but then the money stops flowing in their direction. [This certainly explains the likes of Manchin and even Booker.]
Quoting the rant (or why I believe in reading endnotes): “Do I want the flight attendants running up and down the aisles screaming “Be terrified! Be terrified!”? Or do I want real information that will help save lives? I wish liberals, and especially those in the political class, and especially those in the press, would stop projecting their own terror at lost power and influence onto the rest of us.”
FDR knew full well how corrosive fear is. On the other hand, I note in my own behavior that the less I bother with the fear-mongering, the more I realize that I have a duty to try to act. Not hopey and changey and scaredy duty. The duty is more along the lines of Samuel Beckett: We have to act because we have nothing else.
> even Booker
“Even”?
Folks have been saying all along that Democrats are just Republican Lite. Sounds about right to me. Both parties are nothing but corporate whores.
They’re both neoliberals (markets first).
markets
firstfist.And, drum rolllllllll!, The most evil and powerful of them all!
, “Mr/Ms Market”
(would sell It’s own Grandparents down the river!)
Here is a list of the runner ups;
The Infernal Names
Abaddon—(Hebrew) the destroyer
Adramalech—Samarian devil
Ahpuch—Mayan devil
Ahriman—Mazdean devil
Amon—Egyptian ram-headed god of life and reproduction
Apollyon—Greek synonym for Satan, the arch fiend
Asmodeus—Hebrew devil of sensuality and luxury, originally “creature of judgment”
Astaroth—Phoenician goddess of lasciviousness, equivalent of Babylonian Ishtar
Azazel—(Hebrew) taught man to make weapons of war, introduced cosmetics
Baalberith—Canaanite Lord of the covenant who was later made a devil
Balaam—Hebrew devil of avarice and greed
Baphomet—worshipped by the Templars as symbolic of Satan
Bast—Egyptian goddess of pleasure represented by the cat
Beelzebub—(Hebrew) Lord of the Flies, taken from symbolism of the scarab
Behemoth—Hebrew personification of Satan in the form of an elephant
Beherit—Syriac name for Satan
Bilé—Celtic god of Hell
Chemosh—National god of Moabites, later a devil
Cimeries—Rides a black horse and rules Africa
Coyote—American Indian devil
Dagon—Philistine avenging devil of the sea
Damballa—Haitian Vodou serpent god
Demogorgon—Greek name of the devil, it is said should not be known to mortals
Diabolus—(Greek) “flowing downwards”
Dracula—Romanian name for devil
Emma-O—Japanese ruler of Hell
Euronymous—Greek Prince of Death
Fenriz—son of Loki, depicted as a wolf
Gorgo—dim. of Demogorgon, Greek name of the devil
Haborym—Hebrew synonym for Satan
Hecate—Greek goddess of the underworld and witchcraft
Ishtar—Babylonian goddess of fertility
Kali—(Hindu) daughter of Shiva, high priestess of the Thuggees
Lilith—Hebrew female devil, Adam’s first wife who taught him the ropes
Loki—Teutonic devil
Mammon—Aramaic god of wealth and profit
Mania—Etruscan goddess of Hell
Mantus—Etruscan god of Hell
Marduk—god of the city of Babylon
Mastema—Hebrew synonym for Satan
Melek Taus—Yezidi devil
Mephistopheles—(Greek) he who shuns the light, q. v. Faust (Greek)
Metztli—Aztec goddess of the night
Mictian—Aztec god of death
Midgard—son of Loki, depicted as a serpent
Milcom—Ammonite devil
Moloch—Phoenician and Canaanite devil
Mormo—(Greek) King of the Ghouls, consort of Hecate
Naamah—Hebrew female devil of seduction
Nergal—Babylonian god of Hades
Nihasa—American Indian devil
Nija—Polish god of the underworld
O-Yama—Japanese name for Satan
Pan—Greek god of lust, later relegated to devildom
Pluto—Greek god of the underworld
Proserpine—Greek queen of the underworld
Pwcca—Welsh name for Satan
Rimmon—Syrian devil worshipped at Damascus
Sabazios—Phrygian origin, identified with Dionysos, snake worship
Sammael—(Hebrew) “venom of God”
Samnu—Central Asian devil
Sedit—American Indian devil
Sekhmet—Egyptian goddess of vengeance
Set—Egyptian devil
Shaitan—Arabic name for Satan
Shiva—Hindu the destroyer
Supay—Inca god of the underworld
T’an-mo—Chinese counterpart to the devil, covetousness, desire
Tchort—Russian name for Satan, “black god”
Tezcatlipoca—Aztec god of Hell
Thamuz—Sumerian god who later was relegated to devildom
Thoth—Egyptian god of magic
Tunrida—Scandinavian female devil
Typhon—Greek personification of Satan
Yaotzin—Aztec god of Hell
Yen-lo-Wang—Chinese ruler of Hell
Well said. Those runner ups have been busy busy busy nonetheless.
Medicaid also funds training of doctors, nurses and others in hospital settings. A large percentage of funding for training hospitals in cities like New York comes from Medicaid. Last I read it was close to 30 percent of our hospital budgets throughout New York. Those covered by insurance here will experience repercussions as funding is cut to training programs at the major city hospitals which completely depend on billions in medicaid dollars both through reimbursements and additional funding to programs. I assume that would affect anyone who wants care at one of these big name tertiary care centers that may serve the well off in clinics that are still subsidized by medicaid dollars. Still the uninsured are hurt the worst.
A major issue too is that under Medicaid long-term care, institutional care is mandatory while home care isn’t. So while home care is cheaper, states will feel the need to comply with this rule and will cut home care funding first.
That is a major reason why you saw the ADAPT protests. We could see people with disabilities warehoused. They also repeal Community First Choice, which was a Medicaid option in ACA that allows states to provide home care without a wait list for services in exchange for an extra 6% FMAP boost.
Protests
Toomey’s Senate office. 7 arrests
https://twitter.com/kira_lerner/status/880109079997419520
Cotton’s Senate office
https://twitter.com/JStein_Vox/status/880111792776728576
ADAPT at Gardner’s Denver office
https://twitter.com/JStein_Vox/status/880050569704075264
Kira LernerVerified account @kira_lerner 4m4 minutes ago
Hard to walk through the Senate halls today without bumping into a health care protest
https://twitter.com/kira_lerner/status/880116969890033664
Still holding to the theory that per capita Medicaid grants are analogous to the long-running Medicare “doc fix,” which Congress would waive each and every year.
CBO is obliged to score the budget according to existing statutes, so Medicaid per capita funding casts a rosy glow on the out years, even if everyone knows an annual waiver is in the cards after poor folks start getting wheeled to the curb in front of the hospital to expire outdoors.
Surely Medicaid caps are a convenient fiction that Democrats can get behind … for the greater good. After all — as Lambert ably delineates — it’s not as if they have any ideas of their own.
Worried? Here, have a big wooden bowl of Nancy Pelosi word salad:
> Surely Medicaid caps are a convenient fiction that Democrats can get behind … for the greater good.
Yes, that’s what really worries me. A “Grand Bargain” that caps Medicaid in the coming years. Even if the BCRA fails, it will have succeeded in dragging the Overton Window back rightward, or rather, toward the conservative apex of the Strether Triangle of conservative, liberal, left.
I think selling things like mandatory work and drug testing sells much much easier. The real savings could come through limited formularies but obviously that is a nonstarter. One thing i dont understand about your analysis: the cherry picking you mention is already a part of the process in all the States that have Medicaid managed care.
Thanks for this post. Clearly explains a very important point that is getting no press coverage.
As for the Dem estab options on effective push-back….. you’ve ably documented the reasons they have none. Reminds me of this reported exchange between Churchill and a socialite:
“Churchill: “Madam, would you sleep with me for five million pounds?”
Socialite: “My goodness, Mr. Churchill… Well, I suppose… we would have to discuss terms, of course… ”
Churchill: “Would you sleep with me for five pounds?”
Socialite: “Mr. Churchill, what kind of woman do you think I am?!”
Churchill: “Madam, we’ve already established that. Now we are haggling about the price”
Lambert, you say the Medicaid caps will permanently crapify the BCRA. How is it possible to crapify pure S**t?
I wrote: “Medicaid caps will permanently crapify the program.”
Medicaid is a program. BCRA is a bill.
From what I gather, the caps would apply first to the actual recipients of capitation services rather than the privatized PROVIDERS of the managed care. The PROVIDERS grift has been codified in the various state agreements allowing privatized managed care. The 55-65 yoa clawback for capitation services will doubtless recover some of the costs. Managed care PROVIDERS will be the last to suffer from the per capita caps.
fellow Washingtonians, at 5 PM we are going to from a human chain around the US Capitol to call for the preservation of healthcare.
Really, “the preservation of healthcare”, since you are not “forming a human chain” for Medicare for all or single payer, you are calling for the preservation of private insurance subsidies.
What a noble cause, er, I mean group of unpaid health insurance lobbyists.
You realize 2/3 of Americans cannot come up with $1000 dollars to cover an emergency, and the average lowest deductible on the bronze plan in 2017 on the ACA market is over $6000.
I hope the chants in this human chain match what it is actually trying to preserve. “Save insurance company profits”, “bigger dividends”, “better executive pay now”.
I hope people realize realize this “human chain” (thankfully it’s utterly ineffective, and pray tell what happens if there aren’t enough people to ring the capital? Will every one just mill about to get their dose of virtue signaling) is trying to preserve suffering and private subsidies and don’t show.
Single payer please.
ABCRACADABRAH!
I don’t think both Reps and Dems really care about deficit, particularly Reps. They just think everything should be privatized. Deficit is the excuse.
yes privatization is the only alternative to government, and conservatism has a patriotic based that considers all government bad because we rebelled against an oppressive government hundreds of years ago and replaced it with a skeleton version that efficiently met the needs of the day of a nation composed of no embedded kleptocracy.
Today we are a kleptocracy full of rent seeking leeches that will do anything immoral for a buck as long as it is legal, so the role of government must now be expanded to remove that dynamic where we cannot regulate it. It is demonstrated that we cannot regulate health care away from the leeches so government must take it over.
It is the necessary, lesser of evils is how republicans need to progress in their view single payer.
https://consortiumnews.com/2017/06/23/deep-history-of-americas-deep-state/
not just “today”
The only thing they DONT want to privatize is the military. Everything else, let the market figure it out, apparently.
Pssssst. They have already privatized the military.
I am someone who relies on Medicaid for homecare, under Medicaid long-term managed care in New York State. I’m supposed to receive other services which are never delivered. There is so much corruption sloshing around in the current system, comprised of fund distribution without any required oversight. Yet our governor handwaves how wicked the GOP are for suggesting Medicaid cuts. If the liberal governors were genuinely concerned about poor patients, they should raise the monies to make up the differential. They’re certainly giving away scads of money now to ‘healthcare’ rent extracting middlemen.
So the solution to corrupt middlemen and politicians is to let poor and middle class americans die? That’ll learn ’em!
No, and that’s not what I said. You also seem to ignore the fact that I will be directly impacted by any cuts. It seems liberals have no desire to root out and destroy corruption, which diverts (steals) funds from the poor and middle class, thereby denying them necessary services so they in effect die. Is that not clear to you? Once again, the GOP are up front on their intentions, the liberals pretend they care but don’t want professionalized corruption interrupted.
Thanks so much for this report, Lambert. You would think that U.S. citizens would catch on to the word games played by U.S. politicians: ‘Better’ Health Care Act, Contract for America, et al. If any proposed policies contain words that sound like Madison Ave’s “New and Improved” sales techniques, you might wanna hit the ground running and get the hell away from that policy as quickly as is humanly possible. But, no, it would seem that there truly is a “sucker born every minute,” doesn’t it? Single. Payer. Now. I will be looking up that P.O. Box to send you a couple of bucks for the Water Cooler. Same for Yves over at NC for her “links.” My days wouldn’t be the same without you guys to fall back on.
Lambert, I catch your drift here, but it’s discouraging to hear you continue to harp on the Democrats, as feckless as they may be. Implicit in your argument is the dubious logic that if the choice is between a plan the leaves 324k and a plan that leaves 550k uninsured, it doesn’t matter which gets implemented. Which is a poor argument. There is no plan that insures everybody on the table, in the works, at hand.
No matter what we do, everyone is going to get sick and die. Suffering is inevitable. To posture like you know how to solve this gordian knot of healthcare in the US, and in the meantime knock down the only significant party who’s trying to move the needle in the other direction is childish.
The main reason you see Dems harping on these numbers is that this is a simple numerical argument to make, and at least think one can understand. To most people, including myself, the nitty gritty of health policy is eye glazing material.
I commend you for bringing some analysis to the debate here that looks more closely this nitty gritty. But I’m befuddled by your sneering contempt for the Dems, which you dish up (rhetorically) far more than you do at the Repubs. Your rhetorical stance seems to be, well, the Republicans are hopeless, it’s hardly worth wasting good sneering contempt on them. More satisfying to do it to the hypocritical Dems, because, um, they pretend to be good.
The point is, your prefered solution to health care, single payer, is not close to being politically viable. To attribute this state to the greed and stupidity of the “neo-liberals,” lacks nuance, and is not effective criticism.
A more interesting line of inquiry, IMO, is trying to understand the social dynamics that underlay the current situation, without just throwing up your hands and attributing the cause to stupid, greedy people.
I have found the coverage of the CALPERs governance issues on this site illuminating, because they contribute to the understanding of that system on a functional level.
One of the problems with the notion of setting up a system that drastically undermines, or eliminates, the current status of the insurance companies as being key gatekeeper/middlemen in the system, is that a lot of people work in the insurance industry. Big policy ideas that are going to decimate a whole sector of industry are just not going to be implemented, without some very deft political work being done.
I say this as someone who is concerned that the course of governance, overall, in the US has taken a severe turn for the worse. If one is really happier with the Republicans running the show, then I can totally understand why they would harp on the Democrats, and look to weaken them. But if not, in the mind of the public, criticism of the Democrats, whether from the Left or the Right, just weakens them, and opens the doors wider to the cynical opportunists who run the Republican Party.
One of the most concerning aspects of what I see happening is that one thing Republicans tend to have an interest in, and aptitude for, is ruthlessly maintaining and expanding their power. Despite the utter political ineptitude the Republicans when it comes to governing in a constructive way, it seems they are going to dominate for the foreseeable future.
I guess it’s a fine line between constructive criticism vs passive aggressively tearing down one’s most plausible allies.
> passive aggressively tearing down one’s most plausible allies.
Where am I passive aggressive? And surely, given the Democrat Establishment’s record of betrayal on so many fronts, they deserve a good deal more than sneering contempt. If that’s all I’ve conveyed, I need to work harder.
I take sneering contempt than a shovel upside the head which is what the GOP proposes.
Can’t wait to watch the pitchforks come out nationwide.
The per capita caps are about defunding progressives.
California received about $5 billion in Obamacare federal subsidies to help pay healthcare premiums for about 1.2 million individuals. But California’s big bucks came from Obamacare’s “Medicaid Expansion,” where the state received about an extra $15 billion to expand its Medi-Cal coverage by 3.5 million individuals.
As a result, California now has about 13.5 million individuals enrolled in Medi-Cal, or about 34.5 percent of the state’s 39.1 million residents. But with only 31 states and the District of Columbia participating, the total U.S. Medicaid expansion was 14.4 million individuals, according to the Kaiser Family Foundation. That means California captured over 24.3 percent of Obamacare’s Medicaid Expansion funding.
Of the 68.9 million individuals currently enrolled in Medicaid, California has 19.6 percent of all U.S. Medicaid enrollment and receives 19.6 percent of Medicaid funding, according to the Medicaid.gov website. But under the Republican Senate’s restructuring, that would change dramatically.
The Republican Senate’s restructuring of Obamacare does allow federal Medicaid funding to be “block granted” to each state, so California could develop its own socialized medicine benefit program. But the Senate’s restructuring coverts Medicaid funding from an unlimited number of enrollees, to a “per capita cap” funding amount based on the state’s population.
Given that California currently has 12.4 percent of the nation’s population and 19.6 percent of the nation’s Medicaid funding, the Senate Obamacare restructuring proposal would “reallocate” 7.6 percent of national Medicaid funding on a per capita basis to the other states.
That means that California would lose 37 percent of its $82.0 billion in Medicaid funding to the other states. That amounts to a California being at risk of losing $30.3 billion in federal funding.
Rather than pushing for Single Payer–which would put Republicans on the defensive and empower excitement across the country–the Democrats are following their usual losing strategy of pretending that the current situation is great. People know the current situation sucks, which makes them more amenable to alternatives, even if those alternatives are worse.
b1daly,
It is absolutely appropriate to highlight that those in power are simply arguing, posturing over how many people to NOT cover. Any plan that does not cover everyone fully, to the same extent, is simply arguing over who it’s OK to harm, who’s unimportant.
This notion “politics is the art of the possible” or similarly expressed is nothing but propaganda to keep the status quo largely in place. This is a fundamental issue of morality, one is not good simply because they offer only to cut off a finger while the other wants an entire leg. Neither is acceptable, given only those two options one should rightly spit in the face of the offerer.
Settling for what we’re told is possible, the best out of a number of poor options, is in part how we have gotten where we are today. On issues of fundamental morality such as this, when given no good options by the system, the only moral response is to smash said system, at the very least to not grant legitimacy to the charade.
Healthcare, education, basic survival needs, clean air, clean water, these are non-negotiable items, their funding source, the monetarily sovereign federal government, is non-negotiable as well. To accept anything less is to be complicit in every harm caused as a result.