Yves here. If nothing else, be sure to look at the chart, which is the second graphic in this article. It presents a factoid that has been remarkably absent from discussions about affordability and access to healthcare.
One of the authors of this post, John Canham-Clyne, gave us a heads up on some news that will be breaking tomorrow. Since Lambert will be traveling, he won’t be able to include it in Water Cooler but interested readers can check the FAIR website in the mid-late afternoon for their take. From Canham-Clyne:
The sidebar on the rise in employer-sponsored premiums is particularly timely. The 2017 Kaiser Family Foundation/Health Research and Education Trust annual employer survey is due out Tuesday at 12:30, and wlll no doubt be accompanied by Democratic promotion of a “historically low” rate of private sector premium increases. A colleague will be looking at the full study when it lands tomorrow, and we’ll have a quick take on the real rate of premium increases.
By Mike Casey, chair of the Healthcare Initiatives Task Force of UNITE HERE, a union of 270,000 North American hospitality workers and John Canham-Clyne, deputy director of research for UNITE HERE. Originally published at FAIR
Media fixation on small fraction of patients distorts system’s real problems
The recent collapse of Republican efforts to repeal and replace the Affordable Care Act demonstrated that the GOP’s tireless obsessions—free market platitudes and tax cuts for the wealthy—contribute absolutely nothing to fixing the American healthcare system.
Unfortunately, that was the only thing made clear by media coverage of the healthcare debate.
Looking back, we are struck by the degree to which the media’s fixation on a narrative that mocks a small slice of American voters—pro-Trump voters who had new ACA coverage—deflected attention from the frustration of millions of American workers who have struggled with healthcare problems the ACA either failed to address or exacerbated.
The truth is our healthcare system is sick, and the Affordable Care Act has been little more than a bandage on a compound fracture. The ACA cut the rate of the uninsured to an all-time low, and limited the health insurance industry’s most outrageous consumer abuses, both important steps forward. At the same time, 29 million people remain uninsured, most of the non-elderly population who have employer-paid coverage are increasingly underinsured, and costs continue to soar at 200–400 percent of inflation. (See sidebar.)

Atlantic (2/23/17)
Instead of taking a serious look at the flaws in the ACA, and the deep impact they have on the lives of working-class Americans, reporters covering the healthcare repeal saga spent untold hours and column inches seeking out a tiny slice of the electorate for “reporting” that amounted to little more than mockery. Less than 2 percent of the American people both got new coverage under the ACA and voted for Donald Trump. Yet major media outlets obsessively sought out this sliver of the electorate, to ask, in the words of the Atlantic’s Olga Khazan (2/23/17),
a question that’s baffled health reporters in the months since the election: Why would people who benefit from Obamacare in general—and its Medicaid expansion specifically—vote for a man who vowed to destroy it?
Vox’s Sarah Kliff found these voters in Kentucky, more than once. Abby Goodnough and Reed Abelson did too in North Carolina for a front-page Sunday feature in the New York Times (3/7/17). Jessica Contrera found them in West Virginia for the Washington Post (3/11/17). The LA Times’ Noam Levy (2/24/17) found them in Florida. The Kaiser Family Foundation held monthly focus groupswith them in Pennsylvania, Ohio and Michigan, allowing KFF president Drew Altman to opine on the Times’ op-ed page (1/5/17). Like Kliff, ABC (2/27/17) found them in Kentucky, and CNN’s Dr. Sanjay Gupta (1/6/17) went to Florida. Reporting stimulated comment from the Post’s Dana Milbank (12/20/16) to the Times’ Paul Krugman (3/14/17) to influential liberal sites like Daily Kos (1/28/17), Salon (12/15/16) and Digby’s Hullabaloo (3/13/17).
Khazan’s “baffling” question has a simple answer. Trump did not promise to “destroy” Obamacare, he promised to give people better health plans (a promise broken, obviously). Many people can’t afford ACA exchange coverage, made clear in the Kaiser focus groups:
They spoke anxiously about rising premiums, deductibles, co-pays and drug costs. They were especially upset by surprise bills for services they believed were covered. They said their coverage was hopelessly complex. Those with marketplace insurance—for which they were eligible for subsidies—saw Medicaid as a much better deal than their insurance and were resentful that people with incomes lower than theirs could get it. They expressed animosity for drug and insurance companies, and sounded as much like Bernie Sanders supporters as Trump voters.
Most People’s Healthcare Left Out of Discussion
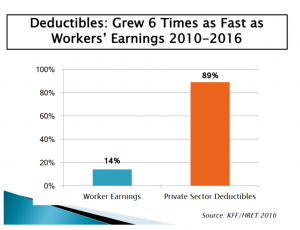
Chart: UNITE HERE
The most damaging effect of singling out this minuscule fraction of the electorate and questioning their motives was the license it gave media to ignore the realities faced by the rest of American working families and to distort the politics of the Affordable Care Act.
Here’s who the media failed to cover: the 177 million Americans who get their insurance through job-based coverage. They are Clinton voters, Sanders voters, Johnson voters, Stein voters and, yes, Trump voters. Media generally overlook the crushing impact the ACA has had on their health insurance. To the extent people with employer-provided insurance are interviewed on healthcare, they are often wrapped in the wrong frame—that their concerns about the ACA are irrational, because the ACA didn’t impact people who were already covered.
This is just a little of what has actually happened across political, racial, economic and gender divisions to the millions of Americans with employer-sponsored health insurance since the ACA was implemented in 2010:
- The ACA imposed an excise tax on their benefits, the simple threat of which caused 73 percent of employers to cut benefits, raise out-of-pocket costs or make plans to do so.
- Their premiums went up more than 3 times faster than inflation. (See sidebar.)
- Their deductibles increased 89 percent, while their compensation went up just 14 percent.
- When they can afford to get care, they see a stranger: 15 percent of Americans lost access to one of their doctors because their insurance network changed in just the last year.
- Even though the US has the lowest rate of un-insurance in our lifetimes, 31 percent of Americans told Gallup they either skipped or delayed necessary medical care last year because of costs, the majority for serious conditions.
- The Census Bureau reports that 11.2 million Americans live in poverty due to out-of-pocket medical expenses.
In short, the majority of Americans who get their insurance through work are facing an escalating crisis of underinsurance, brewing under the ACA and not addressed in the GOP’s proposed replacements. With more than a third of workers carrying deductibles of $1,000 or more, and 20 percent now in plans linked to Health Savings Accounts, few Americans’ benefits look much like 2010.
Shifting Costs to Patients
The deepest flaws in the ACA are the fruition of President Obama and congressional Democrats creating a law that counted on controlling costs by forcing employers to make American workers pay more so they would use less healthcare, instead of having millionaires pay their fair share. In particular, the misleadingly named “Cadillac Tax” is putting enormous pressure on workers’ out-of-pocket costs, based on the false notion that Americans use too much healthcare and that giving employers and workers more “skin in the game” will shrink overall costs—as if shifting costs to the least-powerful players in the system weren’t a recipe for boosting rather than curbing healthcare inflation.
In reality, we already pay more out of pocket than almost anyone else, but go to the hospital and see the doctor less often than the average for wealthy nations. American costs aren’t out of control because we use too much healthcare, they’re out of control because our healthcare system allows corporations to charge too much:
- Hospitals have been on a 20-year merger spree. Now they’re buying up doctors’ practices and charging monopoly prices for both hospital and physician care.
- Drug companies are gaming patent law and charging monopoly prices, refusing to reveal any justification for their larcenous prices.
- Insurance companies are passing provider and drug prices to their ratepayers and skimming billions of dollars off the top of an ever-growing pie.
Media focus on the actual problems with the healthcare system (e.g., Time, 3/4/13) is episodic, in contrast to the drumbeat of coverage of the political wrangling over healthcare.
 These trends are covered, but only episodically compared to the avalanche of coverage of the ACA marketplaces and Medicaid expansion. The New York Times(12/15/15) and others covered a groundbreaking study of 3 billion insurance claims that showed that hospital market power and prices, not utilization, are the primary drivers of private-sector costs. Steven Brill (Time, 3/4/13) has relentlessly exposed extreme hospital prices, and pharmaceutical price-gouging is a national story (e.g., New York Times, 4/26/16). But overall, the media allows Washington politicians to frame the “reform” debate as a false choice between a status quo and Republican reaction—in other words, between a system that punishes working-class Americans and even more punitive proposals.
These trends are covered, but only episodically compared to the avalanche of coverage of the ACA marketplaces and Medicaid expansion. The New York Times(12/15/15) and others covered a groundbreaking study of 3 billion insurance claims that showed that hospital market power and prices, not utilization, are the primary drivers of private-sector costs. Steven Brill (Time, 3/4/13) has relentlessly exposed extreme hospital prices, and pharmaceutical price-gouging is a national story (e.g., New York Times, 4/26/16). But overall, the media allows Washington politicians to frame the “reform” debate as a false choice between a status quo and Republican reaction—in other words, between a system that punishes working-class Americans and even more punitive proposals.
There are plenty of policy tools to combat healthcare corporate monopolies—from Nevada’s first-in-the-nation law curbing Big Pharma’s price-gouging on insulin, to Maryland’s successful hospital rate-setting system, to Hawaii’s employer mandate—or, of course, creating a universal Medicare-for-All (“single-payer”) system. However, all of these require politicians to put working-class Americans before Pharma, hospital and insurance industry profits. Unfortunately, few in Washington, DC, have a taste for any change that isn’t paid for by poor and middle-class families, and corporate media allow politicians to get away with it.
Republicans’ simplistic market nostrums and fixation on tax cuts for millionaires have already run smack into the brick wall of reality. The Democrats’ turn is coming. Standing back and watching GOP infighting may be satisfying, but until Democrats acknowledge the direct harm that their healthcare reforms have inflicted on American families, and the even greater harm that failing to include any restraint on the industry in the original bill has caused, Democrats will continue to suffer apparently mystifying failures at the ballot box.
The media’s myopic focus on a tiny slice of Trump voters, singled out for mockery and disdain, has enabled Democrats’ denial of the true practical and political consequences of a flawed law under whose purview the family fortunes of the majority of Americans have continued to decline.


This is excellent. It is so sickening to hear people like Krugman speak about the 150 million USians who are “generally satisfied with their health care.” I know virtually no one who is, and I live in a prosperous community.
I’m no economist, but doesn’t that mean 150 million Americans *aren’t* satisfied with their health care? That’s kind of a lot.
I for one have been satisfied with my health coverage, but I’ve been on Medicare for the last 9 years.
More, I have a “Medicare Advantage” HMO. with reasonable co-pays, from the insurance company that is owned and controlled by the non-profit hospital system to which I belong. The system — Henry Ford Health System in Detroit — is so large that I have more than enough choice of individual doctors, specialists, labs, and locations, plus now a walk-in clinic for urgent care that I can book online with 30 minutes’ notice — and no paperwork except the multi-page usage reports and annual catalogs that Medicare mandates.
All in, it costs me about $2100 a year. Plus dental, eyeglasses, hearing aids. Under the Sanders/Conyers plans, my savings on hearing aids alone would be a huge improvement — of something that’s already good.
We all should be so lucky. Yes indeed, Medicare for all.
Tens of millions of Americans cannot afford $2100 a year. We need expanded, improved Medicare for All — no premiums, no deductibles, no co- pays. Other countries do it. So can we.
The majority of Medicare Advantage (advantage for insurance cos) policies are sold by one of the five major (crooked) insurance cos. There are deductibles on hospitalization (first week), drugs etc. etc. For the ones where there’s a copayment (e.g. MRI) the crooks of 20%, they won’t tell you how much it will cost. Physical therapy and specialist service copays are also too high. The Sanders plan will (hopefully) eliminate these hurdles and not require an additional premium. The dental and vision care itself is a premium benefit with Bernie Care.
re the great Medicare-Insurance-for-all model:
After repeated requests for a cost estimate I finally received a written cost breakdown for three orthopedic surgeries I’ve needed for several years: Bone spur removal on my heel and elbow from decades-old old injuries and repair of a rotator cuff shoulder injury than I never had fixed because it happened when I was an uninsured private contractor.
Estimated cost: $79,500. My co-pay— $19,900,
For $19,900 I can fly halfway around the world to Thailand, stay in a four star hotel on the beach for a month, receive much more personalized private hospital services, and still have money left in my pocket, Once I’m there, perhaps I should just stay and not return?
Good you don’t pay much for your care.
That is not true for many of us.
Many folks worked overseas.
Should they return to the states, they would be forced to pay permanent penalties for each year they did not sign up for Medicare. In addition to that, increases are also due depending on income.
This makes it certain that America and Medicare are not choices for many highly educated Americans.
Comparing Medicare to French health care shows how inadequate Medicare really is.
In France, there are “SOS Doctors” who come to your home 24/7.
There are also SOS Dentists, SOS osteopaths, etc.
In addition, the labs can come to your home for all those blood tests.
An emergency? Nothing is better here than the “SAMU”. Call and then come
Near Paris, American Hospital is there for all of us.
> It is so sickening to hear people like Krugman speak about the 150 million USians who are “generally satisfied with their health care.”
Krugman purveying disinformation? Say it’s not so!
More seriously, this is a terrific post. (The “why are they voting against their own interests?” compilation is especially good, since that’s been a standard liberal Democrat talking point for, well, donkey’s years. As it turns out, and as usual, liberal Democrats had not concept of how these voters conceived their interests, even on a straight-forward bread and butter issue. This is 1788-level delusion.)
Krugman purveying disinformation? Say it’s not so.
I still cannot get over the “debate” between real economist, Steve Keen, and faux economist, Krugman, on whether or not banks create credit.
If anyone doubted Krugman to be a dunce or charlatan before that, I cannot fathom how they could think otherwise since it.
…Socratic method…issue by issue, perpetrator by perpetrator…
(basis of U.S. law)
Even the right-wing Republicans in my family are increasingly unhappy with their medical insurance and they are also fairly prosperous. The usual tactic of trying to pit middle-class and working-class Americans against each other might not work anymore.
Still, I think the sticking point with voters will be taxation. Some Americans seem willing to put up with bad health care as long as their taxes aren’t going up because they think “well, I am not sick now, so I would rather keep my money from the taxman at this point and I don’t want to pay for anybody else.” Opponents of Medicare for All will harp on taxation and the idea of paying for people who make bad lifestyle choices to try to prevent single-payer from ever happening.
Friedman study (PDF) of HR 676 says 95% of people will pay less out-of-pocket (all but the top 5% of earners).
The tax proposals in the bill and those suggested in the Sanders white paper are progressive.
Republicans favorite comeback on socialist programs is “but how will we pay for it?” This time there is an easy answer, with taxes we can pay for from the premiums and out of pocket pocket expenses we won’t have to pay for any more.
Yes the people that don’t take care of themselves cost the most, but that is actually made worse under the system, for those that can’t afford to maintain their health earlier and cheaper, the whole idea of HMOs. And those that don’t have health care and make bad life choices, health care must not be part of the equation for that, so providing health care is not a moral hazard, and resolves those who end up costing more through use of EMTALA to deal with their problems when it is too late and too expensive.
The long game here is republicans will skeptically vote in favor of single payer. The vehicle to get there is everybody getting screwed along the way.
The only reason the healthcare vampires lose the long game is because they just can’t restrain themselves from trying to suck 100% of the population dry. It will be there undoing.
The proposal is to tax employers to replace part of the break they will get from not having to provide health insurance for their employees. That makes it a no-brainer.
Most Americans are obsessed with saving on taxes because of the constant propaganda. They make poor decisions based on this obsession.
…said propaganda launched by Jude Wanniski, documentation here:
“By 1974, Jude Wanniski had had enough. The Democrats got to play Santa Claus when they passed out Social Security and Unemployment checks – both programs of the New Deal – as well as when their “big government” projects like roads, bridges, and highways were built giving a healthy union paycheck to construction workers. They kept raising taxes on businesses and rich people to pay for things, which didn’t seem to have much effect at all on working people (wages were steadily going up, in fact), and that made them seem like a party of Robin Hoods, taking from the rich to fund programs for the poor and the working class. Americans loved it. And every time Republicans railed against these programs, they lost elections.
Everybody understood at the time that economies are driven by demand. People with good jobs have money in their pockets, and want to use it to buy things. The job of the business community is to either determine or drive that demand to their particular goods, and when they’re successful at meeting the demand then factories get built, more people become employed to make more products, and those newly-employed people have a paycheck that further increases demand.
Wanniski decided to turn the classical world of economics – which had operated on this simple demand-driven equation for seven thousand years – on its head. In 1974 he invented a new phrase – “supply side economics” – and suggested that the reason economies grew wasn’t because people had money and wanted to buy things with it but, instead, because things were available for sale, thus tantalizing people to part with their money. The more things there were, the faster the economy would grow.
At the same time, Arthur Laffer was taking that equation a step further. Not only was supply-side a rational concept, Laffer suggested, but as taxes went down, revenue to the government would go up!
Neither concept made any sense – and time has proven both to be colossal idiocies – but together they offered the Republican Party a way out of the wilderness.
Ronald Reagan was the first national Republican politician to suggest that he could cut taxes on rich people and businesses, that those tax cuts would cause them to take their surplus money and build factories or import large quantities of cheap stuff from low-labor countries, and that the more stuff there was supplying the economy the faster it would grow. George Herbert Walker Bush – like most Republicans of the time – was horrified. Ronald Reagan was suggesting “Voodoo Economics,” said Bush in the primary campaign, and Wanniski’s supply-side and Laffer’s tax-cut theories would throw the nation into such deep debt that we’d ultimately crash into another Republican Great Depression.
But Wanniski had been doing his homework on how to sell supply-side economics. In 1976, he rolled out to the hard-right insiders in the Republican Party his “Two Santa Clauses” theory, which would enable the Republicans to take power in America for the next thirty years.”
https://www.commondreams.org/views/2009/01/26/two-santa-clauses-or-how-republican-party-has-conned-america-thirty-years
Fully agree! An outstanding article.
Essentially (and I believe Yves’ article concurs with my opinion having read and studied the ACA legislation, not parroted stupid stuff from Fake News) is that it was structured as a money transfer from the Middle Class to the poor.
I have heard this sentiment repeated by only one other expert on this subject.
Also, external cost drivers have been greatly ignored:
(1) Private equity leveraged buyouts across the entire spectrum of the healthcare sector;
(2) Hedge fund speculation across the entire spectrum of the healthcare sector; and,
(3) Of course, those mandatory and mandated high-cost pharmaceutical prices.
Yes to this:
> structured as a money transfer from the Middle Class to the poor
… while maintaining and enhancing wealth transfer from both to the rich who own the healthcare industry quasi-monopolies.
But I disagree about “medicare for all”. The issue isn’t who pays, but why are so few getting paid so much for so little? Why are monopolies and trade restrictions being tolerated in this industry which would be shameful anywhere else? Where are the pitchforks and torches?
The actual Trump voter demographic, always quoted, are some of people who’ve gotten the worst end of the stick as a result of the ACA. Self employed tradesmen who might have 1 or 2 helpers are paying monstrously high premiums.
Add to that people who sacrificed say 15 or 20% of their lifetime wages for good benefits and job security, their premiums exploded because of the so called “cadillac tax.”
It’s so purely neoliberal, the Heritage Institute’s healthcare plan is one of their many pieces of legislation that attempt to turn the society into one of only billionaires and paupers, with nothing in between but a 4% professional service class.
Initial implementation of the Cadillac tax was delayed until 2020. It’s retained in Graham-Cassidy but delayed until 2026.
Businesses with fewer than 50 employees are not required to provide insurance. If they choose to do so, they can use the small business ACA exchanges. Those with fewer than 25 employees may be eligible for a tax credit.
I don’t dispute your characterization of the neoliberal ACA, or that premiums are too high on or off the exchanges.
…appears need “neoliberal” historical documentation:
(George Monbiot)
“The term neoliberalism was coined at a meeting in Paris in 1938. Among the delegates were two men who came to define the ideology, Ludwig von Mises and Friedrich Hayek. Both exiles from Austria, they saw social democracy, exemplified by Franklin Roosevelt’s New Deal and the gradual development of Britain’s welfare state, as manifestations of a collectivism that occupied the same spectrum as nazism and communism.
In The Road to Serfdom, published in 1944, Hayek argued that government planning, by crushing individualism, would lead inexorably to totalitarian control. Like Mises’s book Bureaucracy, The Road to Serfdom was widely read. It came to the attention of some very wealthy people, who saw in the philosophy an opportunity to free themselves from regulation and tax. When, in 1947, Hayek founded the first organisation that would spread the doctrine of neoliberalism – the Mont Pelerin Society – it was supported financially by millionaires and their foundations.
With their help, he began to create what Daniel Stedman Jones describes in Masters of the Universe as “a kind of neoliberal international”: a transatlantic network of academics, businessmen, journalists and activists. The movement’s rich backers funded a series of thinktanks which would refine and promote the ideology. Among them were the American Enterprise Institute, the Heritage Foundation, the Cato Institute, the Institute of Economic Affairs, the Centre for Policy Studies and the Adam Smith Institute. They also financed academic positions and departments, particularly at the universities of Chicago and Virginia.
As it evolved, neoliberalism became more strident. Hayek’s view that governments should regulate competition to prevent monopolies from forming gave way – among American apostles such as Milton Friedman – to the belief that monopoly power could be seen as a reward for efficiency.
“Neoliberalism sees competition as the defining characteristic of human relations. It redefines citizens as consumers, whose democratic choices are best exercised by buying and selling, a process that rewards merit and punishes inefficiency. It maintains that “the market” delivers benefits that could never be achieved by planning.
Attempts to limit competition are treated as inimical to liberty. Tax and regulation should be minimised, public services should be privatised. The organisation of labour and collective bargaining by trade unions are portrayed as market distortions that impede the formation of a natural hierarchy of winners and losers. Inequality is recast as virtuous: a reward for utility and a generator of wealth, which trickles down to enrich everyone. Efforts to create a more equal society are both counterproductive and morally corrosive. The market ensures that everyone gets what they deserve.”
https://www.theguardian.com/books/2016/apr/15/neoliberalism-ideology-problem-george-monbiot
Actually, Brookings quite helpfully documented the transfer of wealth under the ACA in a classic “Data Debunks Headline” study in 2014. Follow the link below, ignore the text and look at the graph. It tells you a lot about how Washington views “inequality” and how so many experts equate health care with charity. The Top 10% of the income strata take the smallest hit to their income, while the 7th and 8th deciles subsidize the 9th and 10th.
Link to Brookings study?
…structured as a money transfer from the Middle Class to the poor.
Subsidies alone guarantee this. The subsidies have a sharp cutoff at 4x the poverty level. A family that makes less than $64k gets the full cost of insurance in their subsidy. A family above that limit gets 0.
Im perfectly satisfied with my Medicare Advantage Plan, the only complaint I have about it is the barrage of constant phone calls from them pushing this service and that service that I have no use for.
I don’t think you could invent a system worse than ours. It is the confluence of greed, corporate hegemony, and a bought and paid for Congress. The same Congress that stuck us with Obamacare- and knowing how bad it was going to be for us- opted out themselves. Therein lies the truth.
“If you have to pass a law to make people buy it- it was probably a horrible product to begin with.”
…need understand ACA = corporate-taxpayer subsidies-kickback-contributions to dems, just as Medicare part D = corporate taxpayer subsidies kickback-contributions to repubs….which is largely real reason repubs wish eliminate what was their own invention…
…the “system” killed several friends, one of whom was waiting for HepC medication roll-out…
American health care represents what I despise about the modern world.
1. Politicians with their little talking point lists that ignore reality.
2. Media shills who don’t even bother to address what they don’t understand or cover.
3. Misanthropic plutocrats
4. Lying companies
5. (too many more to list, going to lie down now for a while.)
All better now. TGINC.
If we include diet, exercise and living a relatively stress-free life in a broader definition of health care (more like well-being), then there are even more to dislike or despise.
Even more villains.
Reminds me of Oscar Wilde:
To get back my youth I would do anything in the world, except take exercise, get up early, or be respectable.
Amen to both you and Enquiring Mind!
But until the populace mobilizes to create genuine change, all you will get are the B.S. “fixes” like ACA, that create the appearance of change without addressing the most serious issue: cost inflation due to anti-competitive practices.
Our politicians aren’t ignoring reality. They just care about big campaign donors more than the health of everyday people.
A definition of a psychopath i heard recently. One who understands but does not care.
@Todd: As the Republican party would say, “Hold my beer.”
I wish that were the case.
I wouldn’t even give it the respect of calling it a system. It’s a hodge podge of plans, policies, and band-aids thrown together haphazardly, typically without regard to the bigger picture and often as unintended consequences of unrelated issues (the whole idea of “employer-provided health insurance” as the standard came about as a response to wage freezes during the depression). Yet lawmakers continue to put on this farce of it being a coherent system, rather than admit the market dun goofed.
I’m familiar with the phrase, do not attribute th malice that which can be explained by incompetence, but sorry, I’m not buying it here.
This a result of a long game effort to steer the legislative process to the blood sucker’s benefit. This may not be what some people wanted that voted on this stuff, but it is absolutely by somebody’s intention that we are here. This is no mistake.
Really? A conspiracy?
Quite right, although you likely meant “wage freezes during World War II,” when “fringe benefits” such as employer-paid health coverage spread like wildfire.
Employer-provided health coverage is by definition non-portable and disappears during unemployment (at least for those who can’t afford a COBRA extension). But it’s the cornerstone of the US system, along with nontransparent pricing and nontransparent subsidies of Medicare and Medicaid.
Even when one gets through the hurdle of paying for medical care, a huge hurdle, there is the problem, little talked about, of actually getting decent medical CARE.
We have two community hospitals near me, with large university medical centers not far. Our community hospitals were always very good. First, the smaller one fell apart after being taken over. Then the larger one, a trauma center even, finally caved into joining a large system. The quality of care dropped off dramatically. One doctor admitted to me that, yes, the culture had changed, as did medical secretaries.
I have good insurance (with Medicare), and felt that, as a result, I was over referred, given too many expensive and unnecessary testing procedures, and even unnecessary surgery! All of this occurred while my reason for coming in was ignored, and would have been a rather simple matter. This is not exceptional. I have seen it over and over with others. It is the system that is at fault and even good doctors are trapped in it.
When I was in the hospital for a week, I got to observe first hand. When someone came to do what was basically a customer satisfaction survey, I ended up telling them that the whole model of care was wrong. Ha.
Tell me about it.
Two years ago, my elderly parents were hospitalized after a car wreck. Neither parent was seriously injured, but the hospital wanted to run tests for this, that, and the other thing. I got a lot of practice in saying “NO.”
So, count me as someone who’s just a wee bit skeptical of Medicare. The fact that it would cover all of those tests wasn’t a good enough reason to run them.
…those of us wife R.N., European healthcare (as opposed U.S. health profit) have ability contrast what passes for, U.S.
I was stunned on Sunday evening, Berlin, when wife called doctor to complain of illness…around 35 minutes later, roving doctor knocked, examined her, defined 3 courses of procedure over next days. (She went to her doctor, next day)
As doctors-nurses are state educated through university, they owe back years of Ed in state facility-there is choice-state, or private. (no such choice exists, U.S.) This involves several ways European healthcare holds down costs-the social system benefit. There are also no legal ramifications if-when mistakes are made, beyond doctor appearing before board of peer for strict evaluation. Goal at all times is provision of healthcare, making individual as whole-healthy as possible.
For first time doctors-nurses, subsidized communal housing-apartment dwelling is provided within walking distance of workplace, till social contract-payback achieved…
finally, those “gaming” the system, are removed from system, for designated by offense period of time…we don’t see ridiculous “medical paraphernalia” adds Americans are subject to placing faith in…
> The fact that it would cover all of those tests wasn’t a good enough reason to run them.
One reason why the lack of a global budget in BernieCare worries me. Of course, we await the “death panel” framing…..
I say pass it without it first, then worry about fixing what is broken with the new found authority of the government to act in people’s best interest.
I will say this, the best way to ensure single payer works is for the public employed leaders of that system to be the highest paid positions in all of government, with strict laws on even the appearance of a conflict of interest that could lead to corruption. This would keep the wolves at bay, because that is the greatest enemy to a public run system is corruption.
More anecdata: About 6 years ago my late aunt visited us after work on a Friday afternoon and then complained that she thought she was having a heart attack. Off to the emergency room we go, and within a few seconds the receiving nurse had taken her in for an EKG. No evidence of a heart attack, so we sat and waited for the ER doc to see her. And waited. After several hours she was admitted to the ER department. While he was taking her history it became clear that she was suffering from an extreme case of heartburn/gastritis caused by her earlier meal, which consisted of a platter of fried catfish and a coke. Not good for a 73-year-old who was somewhat fragile. But to be sure, she stayed overnight for observation. Now, my aunt did suffer from heart trouble and had several stents in place, so this was a good precaution. But, the next day her cardiologist and internist visited her during early rounds and decided she should be transferred to the “Heart Institute” for a series of tests, “just to be sure.” These took another four full days, and by the time they were finished her arms were a complete mess of overlapping hematomas from blood draws and IV needles. Suffice it to say that Medicare (plus full supplementary insurance) paid for the entire 5-day hospital “visit.” She liked the attention, naturally. However, it was clear to any sentient being that this was a simple plan to milk Medicare. If she had been 64 and thus without Medicare, there is no doubt she would have been sent home soon after the ER doc diagnosed her troubles, with a prescription for an antacid and a bill for at least $10,000.
Overtesting is bad enough. Don’t get me started on overtreatment.
I got introduced to it young, when I had a knee injury that didn’t get much better in the usual 10 days. I got an MRI. The MD tossed the radiology report at me and said, “You went to Radcliffe. Tell me what you think this means.”
The radiology report said I might have a meniscus tear (which = “operate”) or it could be a possible false positive.
I told the orthopedist, “He said it’s a possible false positive.”
He said, “They all say that to cover their ass. I’ll schedule you for a Friday, I’ll go in and have a look, clean up anything I see. You’ll be walking with a cane by Monday.”
I walked out, thinking, “I’m not having you go on a fishing expedition in my knee.”
But had the guy not been such a jerk and made me read the radiology report, it never would have occurred to me to get a second radiological opinion. I would have gotten a second orthopedic opinion.
A college roommate had married a radiologist. I called her. She put her husband Frank on the phone. He had worked in NYC before they moved to LA.
Frank said, “Read me the report, ” which I did.
He said, “Who signed it?” I read the name.
He said, “I know him. He wouldn’t say ‘possible false positive’ unless he had real doubts. Send me the films.”
An entire team at Cedars Sinai looks at my films. Frank called and said, “Your knee looks perfectly normal.”
As a former Diag Radiologist for nearly 40+ yrs, your experience again confirms, what I have been quoting more times than I can remember at various threads!
In early 90s, several studies came from Rand Corp and Fraser institute that that up to 2/3rd of diagnostic tests and surgeries have NO MEDICAL INDICATIONS! But this being ignored by the AMA and others in medical community b/c there is built in FINANCIAL INCENTIVE in our current fee-per pay service!
There is also what’s called Evidence Based Medicine (EBM) but it gets only lip service!
Medicine has become a huge business, where medical ethics has been replaced by bottom line mindset!
S. Nilavar, MD (ret)
This is the norm with these crooks who milk Medicare. Glad you resisted and did your own homework. That’s what I would do.
Perhaps over-utilization is a problem…driven by eager-for-testing doctors, for public sector patients (those with Medicare).
From the article:
But not when the sick person (like me, for example) is in the private sector and has to pay for it….I rather avoid going to the doctor, only visiting when it is needed, like for regular cholesterol tests and when I am hurt or sick.
Will over-utilization be a problem when everyone is on Medicare or is covered? Hospitals have to make (tons of) money.
That’s why we need these (from the article) when considering Medicare-for-All:
That is, Medicare-for-All alone is not enough. We have combat price gouging and have a rate-setting system. Then, the only rent seeking ways left would to be order too many tests or making the patient over-stay an extra night or two.
Although physicians and hospitals in specific cases treat poorly or too much, systemically, we go to the doctor and stay in the hospital significantly less often than the average in wealthy countries. We often get way too much of the wrong care, and not enough of the right care, but there’s just no evidence that the U.S. cost spiral is driven by using too much health care, especially for non-Medicare patients. Cooper et al, have significantly debunked that notion by examining 3 billion medical claims and finding that the key factor most closely correlated with cost is hospital market power.
As for Medicare-For-All, our Washington experts are so invested in the idea that overutilization is a problem that they’ve made a fetish of “fee-for-service” reimbursement. Canada, France and a number of the other systems who cover all of their residents deliver better outcomes and just more raw utilization than the U.S. at a fraction of our spending while reimbursing through a fee-for-service model, with global budgets.
Meanwhile, in the midst of a system that spends twice as much on average as comparable countries, and nearly 50% more than the runner up, 31% of the population says they skipped or delayed treatment for cost reasons last year.
Overtesting and overtreatment are bad medicine, but they aren’t driving our cost problem. Prices and market power are.
It’s the mighty Wurlitzer.
Btw, utilization/average physician visits in USA = 2.2
Canada maybe 4
Cuba 6
I think Czechoslovakia 8
We’re bending the cost curve.
Not discussed in this post is perhaps the sickest component of the American health care system: the emotional toll it takes on those who must use it. The stress, frustration and anger navigating a complex, often, for most people, incomprehensible system, as well as the strains the financial tolls place on individuals and families. Countless time, probably in the billions of hours per year, are absolutely wasted by the users of this system, the lost value of which is never seems to get noted or addressed.
The American health care system is hostile to the quality of life of every person who must use it, and to a vast number of those who must work in it. Except the most wealthy, of course. It puts financial considerations ahead of everything else, and forces people, often in some of their most vulnerable emotion conditions, to have to spend time away from loved ones to “take care of business” regarding payment, usually before treatment will begin. The takeaway is that money is valued more than people, and that those working in system perform their jobs accordingly.
In no other system in the civilized world is anyone, let alone an entire population, subjected to the ongoing abuse, lost productivity, and diminished quality of life inflicted on those who need to access health care. It is barbaric. Put aside the fact that private insurance and for profit health care is also the most expensive and least efficient delivery of service in the world. Compared to the rest of the world, by any objective measures of patient centered care and compassion, our system is a failure, the worst.
But in America, the rich who control the system prosper, and in America, that is all that matters, and we are reminded of that every time we need health care.
> the emotional toll it takes on those who must use it.
It’s a self-licking ice cream cone! After all, stress leads to illness, which leads to stress…
I really resonate with KYrocky’s comment.
But for Lambert – it’s far more than just the stress – illness plus outrageous costs leads to bankruptcy – which makes it even more difficult to get treatment for the illness – so the illness progresses (to much more expensive =”lucrative” stages), until one qualifies for Medicaid or Medicare… at which point the legalized over-treatment can kick in… but often too late.
Beautifully put. It’s a great article, well written and well referenced, and a terrific comment stream. KYrocky’s remards are an eloquent and accurate characterization, right up to the very last paragraph, to which I would only add this qualifier: that the rich suffer nearly as much as the poor at the hands of this broken “system,” because they are at the other end of the gross misallocation of investigation and treatment, and that is also not a happy place to be, given the existing state of medical knowledge and practice. Those extra needless tests and treatments all have consequences, many of them adverse. Good for the hospital budget! For the patient, not so much.
As fine as it sounds to be able to spend freely on health care, it’s really not; not if the spender doesn’t understand what she is buying. And if she’s not a trained physician, that’s generally the case, because nobody explains anything any more in health care: doctors now are more like carnival hawkers than allies in health. So, for instance, it’s bad to spend six months dying in dehumanizing degradation as a consequence of an “adverse event” during a questionably necessary elective surgery–say, for instance, a joint replacement–knowing that when your estate gets the bill, your entire savings, which represents a lifetime of personal sacrifice and dedication to a productive career, along with self-restraint for the sake of your children’s futures, will be completely exhausted, irrespective of whether it amounted to $50,000 or $1 million. I think even the people who refuse vaccines and antibiotics would opt not to have that experience as a “rich person.” And, it could be avoided with a little clever rationing of health-care resources, such as is done in every humane system in the world.
In addition, the gross misallocation of pharmaceutical resources to “diseases of the rich,” among them diabetes and heart disease medications, and “diseases of the wretched,” among them some kinds of opioids (really everything other than morphine, hydromorphone, and tramadol) and the vast majority of anti-depressants issued after Prozac and Wellbutrin, would be self-correcting, and the rich would benefit greatly from that, as well: most drugs issued now are either patent-prolonging variants or dangerous, pointless replacements for proven, cheap, existing medications.
In the Canadian system, which to me is still the epitome of social justice and efficiency, the rich do best of all. They still do better than the poor, because they can pass envelopes of money under the table to jump the line, but do not suffer needless investigation and treatment. Also, if they jump the line, they are often jumping in front of each other, because the poor needy person still precedes the rich or well-connected eager person.
In the US, a “system” only a sadist would accept, they have found a way to make even the comfortable classes fear their nurses.
Yes yes yes re the anxiety!
I am one of the few with a good health insurance policy, but my insurer Cigna has found new clever ways to crapify it by denying claims…first by imposing a time limit on when they need to be submitted (this is an illegal change in contract terms but you can’t win fights like that) and then they periodically pretent not to have received claims. Since no one else has trouble getting mail from me, the frequency with which this happens mean they are throwing claims out.
So I have to submit claims promptly, and keep records on them so I can call Cigna in case I don’t get paid in a reasonable period of time (they can’t look it up unless you have a set of data items).
A former CIGNA employee once told me what the name of the company actually stands for: “Conned Into Getting Nothing Again.”
Here’s a thought. Maybe it would be a good idea to repeal Obamacare. How could it get any worse, or perhaps if it does we will do something about it.
..forgetting entirely that “something”- healtprofit is “better” than nothing healthcare, for those who can afford nothing…
regardless of fact obama failed entirely-it was always a government subsidy to corporate contributors, as was repub medicare part D…
Their premiums went up more than 3 times faster than inflation. (See sidebar.)
Their deductibles increased 89 percent, while their compensation went up just 14 percent
==============================
And as noted by several commentators, the quality and care they experience is decreasing
And yes, I have posted the below link a zillion times before:
https://www.bls.gov/cpi/factsheet-medical-care.htm
“Although medical insurance premiums are an important part of consumers’ medical spending, the direct pricing of health insurance policies is not included in the CPI. ”
Not to mention co-pays, co-insurance, deductibles, out-of-pocket maximums, etcetera…..does the CPI consider that….or even know it exists???
Are health care prices in general going up, or are prices paid by consumers going up? If price gouging occurs after Harvey or Irma, is that reflected in the CPI?
I don’t know if the CPI is designed to obfuscate health care price rises for the actual consumer (pardon my cynicism, but I think the “unemployment rate” is DESIGNED to hide the true unemployment rate) to protect health care profits for hospitals, drug companies, and insurance companies, but it sure seems that way to me….
And finally, I get so tried of the yammering about how “THE MARKET” is suppose to reduce costs when there is such OVERWHELMING evidence in health care that it does the opposite.
Employment statistics were not designed to obscure the true unemployment numbers, but like the CPI, they have slowly distorted, misinterpreted, and selectively compiled and reported by both the government and by the media. It’s as simple as reporting the U1 numbers and not the more accurate U6 numbers by everyone especially as the latter is a little harder to explain; the large changes in the increasingly dysfunctional economy from when the employment stats methodology was set-up I think (?) before the Great Depression has also been ignored. From what I understand, the process is similar with the CPI, but I understand less about that.
As an example of how not changing methods when reality does, part of the reason the ability of people to pay their mortgages overstated, which meant real, not fake, housing prices was overstated was the Financial sector ignoring the fact that mortgages were no longer issued by local banks who both knew the buyers, not just their FICO scores, and would be carrying those mortgages and would eat the losses if their customers couldn’t pay. Also the home buyers use to have some confidence that if the bank was willing to give them the loan after the arduous process, they could pay and the house was realistically priced. However, loans are no longer issued, and carried, by small local banks, but megabanks that doesn’t know well the area or the customers, and would simply bundle and sell the mortgages to some other business, so they only were interested in getting as much in fees as possible not in getting the loans’ interest payments.
If Big Finance was honest and competent, instead of being financial vampire squids, the changes would have been noted and the algorithms used was have been adjusted. But there was neither the desire or incentives to do so. There were incentives for them not too.
So in the employment stats and CPI there is pressure to not change anything even if the methods used no longer work.
JBird4049
September 19, 2017 at 5:01 pm
“Employment statistics were not designed to obscure the true unemployment numbers, but like the CPI, they have slowly distorted, misinterpreted, and selectively compiled and reported by both the government and by the media. ”
Your right – I get over wrought at this stuff. But the fact that it soooo favors the 1% is, I believe, not a coincidence
so cpi doesn’t account for food, energy, doesn’t account for healthcare, and doesn’t properly account for rents or housing costs ..
Thanks for the excellent article and for Yves for opening comments again.
I’m 64, married to a fellow 65 year old and we have two adult sons and a young grandson. When our family was younger, 25 years back, we could afford catastrophic insurance w/a $2,000 deductible and also accident insurance, which with two active sons turned out to be more useful. The premiums and paperwork quickly derailed this modestly useful system.
I have not been to our family Dr. for at least 5 years, skipping all tests expected from the medical establishment… you can chalk it up to “typical male” stereotypes of head in the sand attitude but it has worked for me, no problems thus far and now hello Medicare!
The only time in my entire life that I have had effective medical insurance and care was when I was a student in college almost a half century ago. I think ACA is a joke except for the poorest and have paid the “fine” since it was foisted on us.
I’m with you. I’m terrified of entering the American “health” “care” “system” because I’m not sure I’ll come out.
So, it’s around 1982 and i’m headed to Auckland on a big old jet airliner, and i’ve got a cold and should’ve never set foot on that plane, but didn’t really know any better, and I arrive in NZ with a horrible flu, and take a taxi to a motel and have either got night sweats or am shivering, but even back then, I knew how onerous healthcare was in the states and am afraid to blow serious dough, but after a couple days I can take no more and call the front desk and ask if they can summon a doctor for me, and an hour later I get my first and only ever doctor visit with him clutching a black leather bag.
He looks me over and tells me i’ve got a nasty flu and need medicine, but i’m in no shape to go get it, so he tells me he’ll go to the chemist for me, and off he goes and 15 minutes later comes back with the goodies, and then tells me “Healthcare is not free in New Zealand, but it’s reasonable, and it’ll be $4 for the visit and $3 for the medicine.”
A couple of years ago I was traveling in Oaxaca (the second poorest state in Mexico) and I had some digestive issues. I went to the local pharmacy for some meds, and they told me I needed a prescription. A doctor affiliated with the pharmacy was next door. I went there and was examined immediately, and to my perception, competently. I got the prescription and the meds and was soon on the mend. Total cost of the whole transaction was a couple of dollars. No claims, no insurance denials. I think all of their customers get the same treatment. Our health care system could use an injection of the humanity with which I was treated in Oaxaca.
I hate going to the doctor too. I go once a year because my employer gives me a discount on my premiums if I meet ever more difficult test results (blood sugar, lipids, BMI, something else). I have to set up a time to get the blood tests. Wait. Take time to see the doctor.
My doctor is actually a great guy though. Serbian. Works in an office with just his wife who is an LPN and administers the office. My doctor and I talk a lot about all the scams in healthcare. He came here thinking America was a great country, and found it was more corrupt than the old Yugoslavia.
America is a weird place.
Here in the UK we have a govt national health service for all but mortgages are done by private banks.
In US you have private health care for rich people and mortgages are done by the govt via fannie mae.
Basically in the UK we ration Health Care by having to wait and certain expensive treatments are not available on the National heath service
In the Us you ration based on money i.e. who can afford it.
their is always too much demand for health care so you have to ration.
I can only assume the US is more interested in money than people’s welfare which is very sad for the richest country on earth.
People don’t understand the degree to which Pharmacy Benefit Managers and health insurers have aided and abetted the Perdue criminal drug cartel by subsidizing cheap, addictive painkillers at the expense of non-addictive solutions that leave patients alert and able to think clearly.
They really, really, really don’t want their “customers” able to fight back, so they remove those good options from their formularies. It’s not a mystery why there are so many heroin addicts in America. It’s a design.
https://www.nytimes.com/2017/09/17/health/opioid-painkillers-insurance-companies.html
See, e.g.:
Private Equity Sees No End to the Drug and Mental-Health Gold Rush Bloomberg
The Hidden Monopolies That Raise Drug Prices The American Prospect
The survey company Press Ganey is also to blame for the opioid addiction problem, Wade. They, along with the corrupt hospital regulatory agency Joint Commission, lobbied hard to have patient satisfaction factored into Medicare reimbursement. And some of their most important survey questions ask about pain management. It asks whether or not the doctor prescribed enough pain meds to relief your pain, and whether or not the nurse gave you your pain meds in a timely fashion. These questions may seem rather harmless, and some may even see this as a win for patient advocacy, but it’s really not on either account. Doctors on the frontlines, as well as nurses on the frontlines, including myself, have been warning for years that such survey questions will help fuel an opioid epidemic in this country. Press Ganey balked at this, including Joint Commission and Medicare. But, hey, this should surprise no one. After all, all three of them are in a revolving door together, getting rich off of Uncle Sam.
So as Press Ganey goes from being a mere million dollar company to a monstrous billion dollar company, think of all the massive amounts of money they have made by helping to get millions of Americans addicted to narcotics. If I personally had any kind of power in Washington, I’d push hard to have Press Ganey handover a sizable portion of their profits selling surveys to hospitals and put it to use treating opioid addiction across this country!
I mentioned this the other day, but my mom gave me her checkbook register from mid 1961 to mid 1962, and adding up all of the checks to Dr. Evers-our family physician, it came to $88 for a family of 6.
My coming out party was $190.
I asked my mom if we had health insurance and she told me nobody had it back then, except for a few that had Kaiser.
Why is a pregnancy 50x as much now?
Good question, but here is the really scary question.
Why is a pregnancy 50x more likely to kill the mother now than when they cost $190?
Lost Mothers
If you click Google News or go to any MSM site, you’ll hear a deafening silence on Medicare-for-all or serious discussion on the dysfunctional healthcare system.
The only chance of real progress is to get the Deplorable Democrats who are not backing Sander’s bill the heck out of office…
Good write up and good comments.
As part of their argument for “streamlining” via tax reform, one Republican talking point has been all the time people will save on preparing their taxes and how much fuller their lives can be with that time.
I have spent more hours fighting just a single incorrect medical bill than all of the time I have spent doing my taxes in 36 years of filing.
Lifetimes of wasted hours are pissed away every day in this country navigating our for profit health care system, but no Republican cares about that.
The point about time wasted on medical bill technicalities versus tax technicalities is worth bringing up, but the generalization about what all Republicans care about is gratuitous. Of course there are Republican voters who get frustrated navigating the current health care system.
This is incredible data to support what I’ve seen, trying to get healthcare for my family in the last 8 years. Huge deductibles, unexpected bills, fighting for coverage on numerous phone calls. All with ‘good’ Employer supported insurance.
But look at what the LA Times published on Sunday: “… most people with employer-provided private insurance say they like it “. Complete rubbish from Doyle McManus. Does Bernie Sanders’ single-payer plan have a shot?
Recently I have learned of two large medical practices in the Chicago area being purchased by hedge funds.
The (old, nearing retirement) partners get a huge bolus of money up front and leave the younger members to deal with being employees of for-profit organizations run by non-MDs.
I just can’t fathom this. Hedge funds. Owning doctors. Who have been sold out for 30 pieces of silver by other doctors. This exemplifies, in a small way, everything wrong with health care in America.
Yes, agreed, an excellent post and very good comments.
Two observations:
(1) I’ve begun reading my Senator’s FB posts’ comments the last few months. He’s a Democrat and supporter of the ACA (not on board with Medicare for All yet). It’s pretty clear from the comments that people are generally extremely dissatisfied, and that includes plenty of posters with insurance through their employers–who almost uniformly blame the ACA for their no-longer affordable premiums/deductibles.
(2) As an American resident abroad for yonks, I’ve seen what an NHS even in a totally broken country is like – yeah, in many ways it’s below American standards in terms of bells and whistles, concierge-type services, but there’s one thing about it that can’t be compared: I’ve never met a single person in forty years who became impoverished as a result of a major illness. Cost of full leukemia treatment, including bone marrow transplant: nothing. Cost of emergency surgery for accident-related injuries: nothing. Cost of orthodontics for offspring #1: nothing.
In contrast, while in the U.S. recently I had a very bad accident. The ER didn’t do anything for the actual injury, but they charged me $1650 for six stitches and the privilege of not being seen by a physician.
This is a seriously, seriously messed-up system.
On a motorcycle trip to Texas (the three sisters if anyone knows of them), my windshield broke off after a bird strike, the upper half of which struck me in the face and slashed my face open. I had the joy of sitting in an empty waiting room for 2 hours (doc was at dinner), finally giving up, buying a tube of super glue at a zippy mart, and gluing my face together in a hotel room. I got a bill for $350 from the hospital. Not quite $1650, but I did feel your pain. BTW, thank you, Texas, won’t be back.
“There are plenty of policy tools to combat healthcare corporate monopolies—from Nevada’s first-in-the-nation law curbing Big Pharma’s price-gouging on insulin, to Maryland’s successful hospital rate-setting system, to Hawaii’s employer mandate—”
Sure, there are plenty of tools but lets not pretend that they are all truly effective. I live in Hawaii and can say that while things are better here as far as coverage and costs than most states, we are far from anything resembling sanity.
What has always astounded me is that the employers of America have never lifted a finger to relieve themselves of the economic burden of employee health insurance. They are allowing the med industrial complex to eat their lunch with excessive cost and making insurance an artifact of employment. Guess they love them Freedom Fries!
“the employers of America have never lifted a finger to relieve themselves of the economic burden of employee health insurance”
Yes they have. They’ve offshored as many jobs as they can. Health coverage is part of the ‘high costs’ they cite when they close up shop here, and re-open in China.
Well documented piece. Has anyone else seen this? Unclear whether this is a solution but at least the incentives potentially line up: https://www.washingtonpost.com/business/economy/experimental-program-in-vermont-pays-doctors-to-keep-patients-healthy/2017/09/17/ddb47cfe-9320-11e7-aace-04b862b2b3f3_story.html?utm_term=.775eaa0ad9d1
Sounds great in theory but I very much doubt it will be accepted by the hospitals and the providers. Payment under DRG group was similar but didn’t survive!
s.nilavar, M.D.
In the era of ‘Ct scans, MRIs, Ultra sound, PET scans, Nuclear Medicine/Radiology,the essence of practicing with bare hands ‘clinical skills’ of ‘HEAR, SEE, & TOUCH has been completely LOST, do the detriment of patient’s interest!
The BASIC ‘clinical’ Medicine has taken a back seat to to all the modern imaging miracles! I should I know! I was a GP before going for training for 5-6 years (with fellowship) to become Diagnostic Radiologist. Practiced in private, University + VA systems in 40 yrs+ time.
To illustrate by my personal experience about 2 yrs ago, at Vancouver Int’l airport. By accident I fell down on an up going escalator and sustained bloody scratches/gashes, all small, over my fore head adjacent to my right eye and below nose. My shirt was bloody all over. Some one stopped the escalator. I got up and rested on a stool. My daughter (practices FP in BC) and my son-in law came who were waiting came running. Para medics on bikes arrived. An ambulance was called in. The para medic cleaned my wounds and put a strip across the cuts. Then he insisted I should go to hospital, get a CT scan etc. But I declined politely and assertivily, was asked to sign a release which I did!
I told my daughter that if any of my’ vital signs including a NEURO CHECK (lose consciousness, not respond to command or sensory stimuli ETC) she should drive me straight to Hospital on the way. Nothing happened to warrant a CT scan within the next 24 hours! Of course I had my daughter-MD!
The point is before CT scan etc, there used a clinical protocol to diagnose serious brain injury. Skull x-ray may or may not show a skull fracture. But even fracture may not reveal injury to underlying brain.
In ER in early 1970s, we are taught about NEURO CHECK – check the consciousness, pulse, BP, reaction of pupils, response to commands or pin prick etc on admission and if needed put on a 24 observation either there or sent home, provided, if the patient had any’ responsible’ adult, with clear instruction to come back if any of the (previously described signs& symptoms) within 24 hrs. I rarely encountered any one who was sent home came back. Of the course the ‘standard of care’ in ER, now has changed.
No one thinks of any of the basic skills (fading way in modern medical education!) but instead rely on imaging which are known to produce false positives or even false negatives. The key point is that doctor is treating a ‘living human being’ and NOT the x-ray, scan or MRI! Just relying on them ‘blindly’ is BAD medicine!
S.Nilavar, MD (Diag Rad ret)
Thanks for the article, observations, and comments…unparalleled…
I contemplated adding to the recount of healthcare/hospital horrors, but became too despondent reading about others.
Long story, short: incompetence abounds in the hospital and it cost close to $1Million. (Most of it paid by insurance, but the physical/mental scars remain.)
Good Health, to all.
As I think once again the discussion around healthcare is focused completely on the wrong issue. Instead of focusing on how to insure a system that is fundamentally corrupt and flawed at its core and look at empowering people to improve their health sometimes with the assistance of their doctor rather than managing the symptoms of illnesses which the overwhelming majority could be eliminated by lifestyle changes including diet. We need to get completely out of this debate and look at the underlying assumptions that are in fact sustaining the racket that we call health. As concerns this I forward you a presentation made by Rob Verkerk from Alliance for Natural Health International on their 8-point Sustainable Healthcare Action Plan at lifestyle medicine conference in Sydney, Australia. I think you will find that if something along these lines were implemented it would completely transform the whole healthcare debate and costs would drop dramatically.
http://anhinternational.org/wp-content/uploads/2017/09/170915-Verkerk_sustainability_ALM17_optimised.pdf