By Lambert Strether of Corrente.
Today I’m going to take a quick look at Canadian Medicare and how the neoliberals are using their playbook in that country. I’m really trying to avoid posing as an expert on Canadian politics[1], or as an expert on good faith proposals for refreshing and improving Canada’s single payer system, because I am neither of those things! Rather, I plan to do two things: First, I’ll provide a number of testimonials about the quality of Canadian Medicare. Then, I’ll look at “wait times” as the flash point that neoliberals are using in their persistent, decades-long attempts — funded at least in part by American business interests — to destroy it. But first, let me review the neoliberal playbook for destroying public goods and services (here in a post on the US Veterans Administration):
The stories intertwine because they look like they’re part of the neoliberal privatization playbook, here described in a post about America’s universities:
It’s almost like there’s a neo-liberal playbook, isn’t there? No underpants gnomes, they! [1] Defund [or sabotage], [2] claim crisis, [3] call for privatization… [4] Profit! [ka-ching]. Congress underfunds the VA, then overloads it with Section 8 patients, a crisis occurs, and Obama’s first response is send patients to the private system. Congress imposes huge unheard-of, pension requirements on the Post Office, such that it operates at a loss, and it’s gradually cannibalized by private entities, whether for services or property. And charters are justified by a similar process.
(I’ve helpfully numbered the steps, and added “sabotage” alongside defunding, although defunding is neoliberalism’s main play, based on the ideology of austerity.) We can see this process play out not only in public universities, public schools, the Post Office, and the TSA, but in Britain’s NHS, a national treasure that the Tories are systematically and brutally dismantling.)
Spoiler alert: [2] is “wait times,” and [3] is already taking place (though in the form of inroads and neoliberal infestations, and not the complete dismantling of the system). But first, let’s look at those testimonials.
An amazing thread developed on the Twitter after an opponent of “socialized medicine” deployed the “wait times” talking point, and asked: “Tell me again about how good Canadian health care is.” People were very willing to do so! First, I’ll give a sampling of responses — images, unfortunately, because Twitter insists on including the parent tweet in its Embeds whether I want it or not, and I don’t want the same parent Tweet to show up ten times — starting with Americans who have had the opportunity to compare and contrast the two systems:
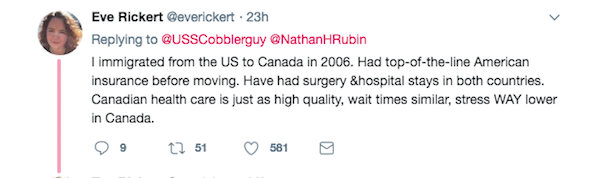
One reason Canadian Medicare is less stressful is that you don’t have to worry about losing everything and going bankrupt:

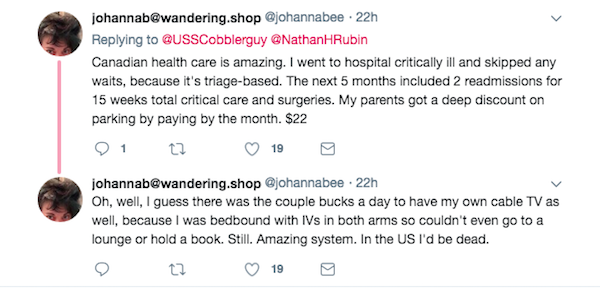
And note that Canadian “triage” eliminates “wait times” for those who are critically ill:
And now here are some Canadians politely dunking on the original poster because their major expense at the point of care was “stress snacks”:
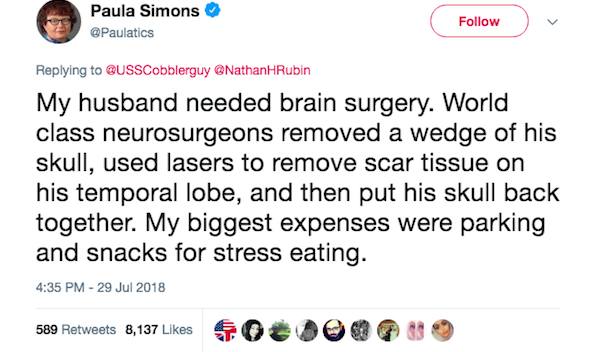
Although, to be fair, parking is a cost, too, besides snacks:
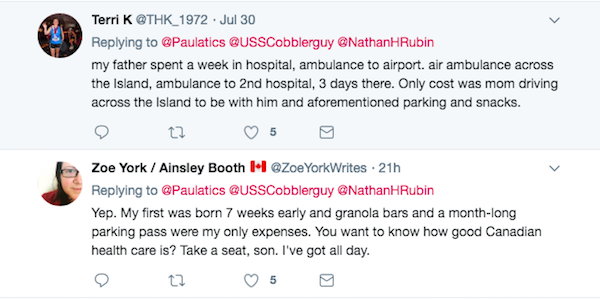
And then there’s the whole concept that you get to keep on snacking and parking, because you’re alive:
Finally, “triage” again:
Let’s sum up that “wait times” argument. To begin with, it’s as anti-social as they come. Suppose I’m waiting in a queue for the bus. What would I think of a person who cut in front of me because they could hand the bus driver a buck, even if those were the rules? Or suppose I’m sitting in my optometrists office with another patient, and they walk up to the receptionist, hand them twenty bucks, and say “I’d like to go first?” That’s the principle involved here. Granted, in this country, the organs of state security are busily trying to make shoving in front of other people because you have money the, er, norm with programs like “Trusted Traveller,” but so far, at least, the practice hasn’t trickled down to everyday human interactions. Et ego in Canada, from the Toronto Star:
At Canada’s Wonderland, you can buy your child a “Fast Lane Pass” so he or she can experience the thrill of pushing ahead of all the other children waiting to get on a ride.
It’s excellent preparation for today’s world of hyper-privilege – where the rich get to buy their way to the front of just about every line.
Wonderland, indeed! Besides being anti-social, the “wait times” argument is anti-care; note several of the testimonials above mention that they got care instantly when they had serious conditions, unlike the poor lady in this country who died while the ambulance people failed to check her vital signs. Heaven knows I have my issues with credentialed professionals, but I would certainly want the queue for medical care to be organized based on medical necessity, and not financial incentives. We have that in the United States, and there are issues with it.
From the quality and principles behind Canadian Medicare, let’s turn to the neoliberal assault, where “wait times” are the wedge issue. The journal Health Economics, Policy and Law gives an overview in 2018 (PDF):
Growing wait times and gaps in access are causing Canadians to question their system. Some 15% of Canadians lack the basic security of a family physician (Health Fact Sheets, 2015). A recent Commonwealth Fund study ranked Canada near the bottom of developed countries with respect to accessibility – behind the US health care system – on some important indicators: half of Canadians surveyed reported waiting more than two hours for emergency room care, compared to 25% of Americans. Some 30% of Canadians said they waited two or more months to see a specialist, compared to 6% of Americans (Schneider et al., 2017). Whilst poll after poll finds strong public support for care allocated on the basis of need rather than ability to pay, Canadians’ faith in medicare has been sorely tested…
Step [1]: Underfund and sabotage. Clearly a resource issue. If the queue is too long, then, within reason, add the human and technical resources to shorten it.
… by long wait times and growing gaps in access to family care and specialists, important medications and long-term care. IPSOS Reid (2003–2010) reports that between 2003 and 2010, Canadian attitudes on the quality of health care services have shifted markedly from positive to negative.
Step [2]: Claim crisis. That’s working splendidly. Step [3] (privatization) is still on the bubble system-wide:
The lackluster performance of the Canadian system may lead to the mistaken conclusion that the basic values underlying medicare are outdated or quixotic. If the core values of access on the basis of care rather than ability to pay are to survive, it is imperative to embrace evidence-based reform that is also grounded in history to better understand the windows of opportunity for change.
Nevertheless, step [3] (privatization) is happening (and in defiance of the law, I might add). From the University of British Columbia Medical Journal:
[T]he private market is not waiting around for the question to resolve itself…. In addition to supplementing the public system, the private system shows signs of infringing upon its domain. An evaluation of 130 private healthcare clinics across Canada found evidence to suspect the possibility of 89 violations of the Canada Health Act, including charging patients for medically necessary services [ka-ching] that are covered by Canada’s publicly funded universal healthcare system. These clinics allow Canadians who are willing and able to pay out-of-pocket to avoid lengthy public system wait times, effectively creating a tiered healthcare system. In 2005, a Supreme Court Case ruling in Quebec allowed an individual to access private health care as a solution to long wait times. (10) This ruling sets a precedent for the nimble private market to fill in the gaps of the public system, pending rulings in other provinces across the country.
And from HuffPo:
Saskatchewan has just enacted a licensing regime for private MRI clinics, allowing those who can afford the fees — which may range into the thousands of dollars — to speed along their diagnosis and return to the public system for treatment [after sucking resources from the public system –lambert]. Quebec has just passed legislation that will allow private clinics to extra-bill for “accessory fees” accompanying medically necessary care — for things like bandages and anesthetics.
$619 bandaids, here we come! C’mon, who doesn’t want that?
Once upon a time, these moves would have been roundly condemned as violating the Canada Health Act’s principles of universality and accessibility. These days, two-tier care and extra-billing are sold to the public as strategies for saving medicare.
This sense of resignation is understandable [an effect of steps [1] and [2] –lambert], coming as it does on the heels of a decade-long void in federal leadership on health care. Throughout the Harper government’s time in office, the Canada Health Act went substantially unenforced as private clinics popped up across the country.
Instead of modernizing medicare, Saskatchewan and Quebec are looking to further privatize it.
In fact, neoliberals are using “wait times” for a Constitutional assault on the entire Canadian Medicare system. From Colleen Flood and Bryan Thomas, “A successful Charter challenge to medicare? Policy options for Canadian provincial governments,” Health Economics, 2018:
Across Canada, laws designed to protect public medicare are subject to court challenges on the grounds that a public monopoly on health care subjects Canadians to long wait times, infringing the right to ‘life, liberty and security of the person’, guaranteed under the Canadian Charter of Rights and Freedoms. By way of remedy, the claimants demand the liberalization of privately financed care, to create a ‘safety valve’ for wait times in the public system. The most prominent of these challenges (the Cambie trial), led by Cambie Surgical Services, a private clinic headed by Dr Brian Day, challenges various laws in British Columbia that prohibit physicians in the public system from extra-billing patients and moonlighting in the private sector, and also prohibit private health insurance for services covered by medicare (parallel private insurance). Although the litigation appears temporarily stalled as the applicants allege they need more financial resources (Mulgrew, 2017), it nonetheless seems likely that in the coming years, the Supreme Court of Canada (‘the Court’) will be called upon to rule on Cambie or a similar Charter challenge, setting an uncharted course for Canadian medicare
The Editors of Health Economics comment:
That Charter rights could be used to undermine medicare is a grave rebuke to the assumption, common among advocates of human rights and dignity, that rights litigation is a positive, progressive force. As Flood and Thomas (2018) discuss in this volume, these Charter challenges will serve either as a wakeup call or death knell for medicare; everything depends on how Canadian governments respond. The courts can permit privatization to undercut equity and access, or they can respond creatively with new legal and policy solutions to improve equity and access, defending the human rights and dignity of all.
I hadn’t thought that there was a Constitutional right to queue jumping for those with the money to do it, but life is full of surprises![2] Oh, and when you hear “wait times,” know that the talking point is part of an international assault.
NOTES
[1] It strikes me, as a rank outsider, that the “pay for” issues occur at the Provincial level (as in principle they cannot at the Federal level, Canada being sovereign in its own currency). Each province has its own plan, and each province (AFAIK) also budgets for health care spending. It occurs to me that this Federal structure has provided the neoliberals with opportunities for attack; they can pick out on province and privatize there, for example. Something to think about for advocates of state level #MedicareForAll in this country.
[2] Once you throw the NHS into the mix, there’s a strong case for internationalizing health care as a universal concrete material benefit. If one really wishes to appeal to the international working class, that strikes me as a stronger case than open borders, particularly after the effects of labor arbitrage are taken into account.
APPENDIX I
Here are the five Principles of the 1984 Canada Health Act:
1) Public Administration
2) Comprehensiveness
3) Universality
4) Portability
5) Accessibility
This is what Canadians mean by “access,” so different from what liberals (and conservatives) in this country mean by it:
must provide for insured health services on uniform terms and conditions and on a basis that does not impede or preclude, either directly or indirectly whether by charges made to insured persons or otherwise, reasonable access to those services by insured persons
These principles are extremely popular. From the University of British Columbia Medical Journal:
[B]etween 93% and 98% of Canadians support the five principles of the Canada Health Act, (12) which confirms strong support for equal access to health services across socioeconomic groups in Canada.
MedicareForAll advocates should make sure that similar principles are written into our own legislation (and not compromised away).


When I retired and moved to a new area I had to wait 9 monthes for my first appointment. Went to a clinic twice to keep my subscription up to date. Sure it was Medicare but more importantly just the lack of doctors in rural areas.
Try getting in to see an endocrinologist or a dermatologist. Months! And that’s not because of Medicare. People don’t want to understand that we already have rationing here. It’s just done by cost and availability.
Where I live in upstate NY there is a problem with getting to see your regular doctor in a short time. If you have an ear ache or some other sudden illness you have to go to a walk in clinic and wait for hours to be seen. The last resort is the emergency room and many insurance policies are fussy about paying for an emergency room visit. To see my regular family doctor requires at least a month of wait time. Before all providers were forced to be employees of one of the two health care system, you could call and get to see your doctor the same day. Health care has become nothing more than a business run by people that aren’t trained in health care. Most are MBA’s and they are telling doctors what they have to do.
I schedule dermatologist appointments a year out. My wife has a three month wait for rheumatology. I have no idea where they got that 6% number.
I’ll add a couple of stories: Last year an acquaintance of mine (USAin) was vacationing in Ireland and slipped on some rocks while hiking near a waterfall, fell and injured his back. The pain got worse that evening so his hotel helped him to a clinic near by. The clinic did x-rays, didn’t like what they saw and sent him via medical transport to the hospital for an MRI that same night. After the MRI, the doctors discovered a hairline fracture and gave him meds and a back brace. On the way out of the hospital he asked “What do I owe you?” He said they looked surprised at the question, but they got the answer to him, about $600 US. With a typical US plan, that would have been many thousands no doubt.
My wife’s cousin who works legally in Japan, fell and broke her leg so badly that she was in the hospital for three weeks. Total cost, about $1k.
Neither of these individuals were citizens of the respective countries, but were still better off than here in the US.
Bottom line, medical care in this country is just another way of extracting excess $ from the general populace. And a great one at that as sooner or later everyone needs care. And as listed above, that is clearly the neoliberal playbook, Medicare and Social Security included.
Lambert as an Ontarian I agree with your take on the Canadian system. What I would add is that it is broadly supported by all major Canadian parties. The current debate is about whether it should be broadened to include drug coverage.
I will attest that in Ontario if you are in bad shape the wait times vanish. If you have a non serious problem that requires a specialist a 3 month wait is my experience.
Ontarian here, and I agree most whole-heartedly. IME, Ontarians, and the other Canadians I have talked with about this, feel about our OHIP or other govt health care the same way ‘Merkins are supposed to feel about their gunz (BTW, I have not heard that from 100% of my US contacts, in fact, from very few). From my cold, dead, hands, and after a hard fight to get me that way.
I cannot understand the heartlessness and barbarism of a country that tolerates bake sales and GoFundMe’s to pay for chemo or ttreatment for gunshot wounds or your kid’s compound fracture.
Another Ontarian, and I agree about the wait times….they disappear if you have an emergency, which is as it should be in correct triage.
I live in a border town and many folk here have relatives/friends in the US (including me). I can say that the horror stories from the US do not go down well. I have been cheered to hear more and more how excellent out healthcare is and that the wait times are fair, there is much less complaining now than usual.
I don’t think there will be any support in my area for privatization, in fact there is a lot of discussion about adding drug coverage and dental care especially for children.
As a Canadian living in Ontario, I had a severe attack of gastroenteristis four weeks ago accompanied by sever bleeding –at least two pints. I was hospitalized immediately for a week. I was seen by about six doctors and three gastrointestinal specialists. I had a CT scan and at lest 10-15 other medical tests. I was on IV for days, normal drip and magnesium drip. I was amazed at the very high quality of care and attention I was receiving.
There are no wait times for emergencies! Triage works well!
My bill was zero dollars and zero cents.
I live in a nation where people –not the dollars they have– matter. Canada’s health care system is a part of my social income, something I can count on when my monetary resources might prove inadequate.
I could not have afforded this care in the United States. Most likely, the ‘ability to pay’ principle would have led to my death.
Think I’ve mentioned that some hospitals around here put billboards on the interstate showing the wait time for their E.R. That might be relevant should you suddenly have a heart attack on the freeway but then another hospital crowned their new wing with fountains and sculpture. Is it a hospital? Or a Sheraton? Clearly the MBA marketing specialists who now run our medicine are having a hard time thinking of selling points to best the competition. A more relevant billboard saying “30 percent less likely to misdiagnose” would be considered a downer.
One hopes Canadians show the good sense to tell these people to take a hike.
Interesting, I just saw a you-tube commentator make the argument that the Canadian healthcare system is so popular, that even the conservatives are not trying to roll it back. Warning! Learning curve ahead.
https://youtu.be/mH9O0MRjvLg
Neoliberalism is sanctioned monopolies under the pretense of free-marketism.
I don’t believe I saw reference to any studies comparing wait times in the U.S. and Canada. Surely the enemies of medicare for all must have something upon which to base their argument.
Right. There are wait times in the US, especially for good specialists.
Exactly. Whenever you hear the words “wait times” your first question should be “compared to what?”
We must always keep in mind the difference in expenditures. The U.S. spends about 18% of GDP on healthcare and chooses to not cover everyone.
Canada chooses to spend about 11.5% of GDP and covers everyone. They could eliminate wait times and every other problem, real and exaggerated, if they chose to spend more.
My experience is that there have been cutbacks to hospitals which have made things somewhat worse than they were decades ago – not really that much worse but noticeable. In the suburbs around Vancouver where I live the fast growth in population hasn’t yet been caught up by increase in hospital facilities so things seem worse than average around here particularly in ER wait times though it must be said that this seems highly dependent upon day to day variations. In the last twenty years I’ve had one quite long wait but all my other ER visits (for myself or when I’ve taken others) have been moderate to short. Even when the ER is very busy though serious injuries have always been taken care of immediately. Neither I nor anyone I know has had to wait very long for non-emergency care. I developed cataracts (at age 47!) last fall and both eyes were done within three months of the diagnosis and that includes the time interval required between ensuring the first eye operation is successful before doing the second one. Single payer just plain works and the U.S. with its much larger and less widely spread population should be able to do it significantly better than Canada. Properly implemented (which is the real trick given how many people there are who would want to kneecap single payer) I would bet that at 10% of GDP the U.S. could have substantially better care than we have in Canada right now.
The Australian situation is similar to the Canadian, where the non-emergency entry point to medical care is a GP (general practitioner) consultation. Under Australia’s MBS (Medical Benefits System) this visit can’t be insured for. The government pays the GP a set fee, and about 80% of consultations are bulk billed. That is, the GP accepts the government rate, which has been frozen lately, as full payment for the service. If there is a top up, a gap payment, this also cannot be covered by insurance.
The private health insurers in Australia, and in particular Medibank, the large government insurer that recently got privatised, have been trying all types of sneaky ways to get around this, including setting up multi-discipline clinics (to avoid the basic GP practice restriction), and trying to offer a ‘guaranteed access’ to a GP within x no of hours depending on insurance cover type.
The government rightly has cracked down on this as introducing a two tiered primary health care system, where privately insured patients get faster access to resources. And with insurance covering the cost, prices will inevitably go up, causing the bulk billing rate to drop and the gap payment to increase, effectively reducing access to these services on price rather than health issues. But that doesn’t stop the insurance companies trying, repeatedly, with, amongst other things, the vocal support of a small pool of academics and the usual neo-liberal think-tanks.
I asked my doc for an MRI for some back pain (over many years, cause unknown).
The wait was really not that long at all in BC – they called once for an appointment; I was not there; they called again in a couple of months – my time availability was actually longer than what they (the hospital) could do.
I have nothing but good things to say about Canadian (BC) health care.
I’ve never really understood the “wait time” talking point. Isn’t the “wait time” for uninsured or underinsured people in the US whose conditions aren’t covered by insurance and who can’t afford to pay out-of-pocket effectively from now until the point they die? What kind of “health care” “system” tolerates that for any portion of the population?
There’s that neoliberal “skin-in the-game” “argument” (see today’s Water Cooler) about how, with free-at-the-point-of-service care, some (likely minuscule) portion of the population might “abuse” the system, but, with all the chatter about “wait times,” not a whole lot of concern, it seems, about the (probably much larger) portion of the population who wait…and wait…and wait (like the refugees in Casablanca) and never get care.
In the UK’s NHS, wait time depends on the condition. If acute they wait time is small. If chronic then the wait time is longer.
In addition they system discourages excessive treatment at end-of-life. Few terminal cases in the UK are treated in by trying to extend line one or two months, unlike the US.
I’m a firm believe in nationalized medicine, because the greatest advances in longevity are the result of well applied public health, clean water, sewage disposal, housing, pre and post natal care, and inoculations.
Better care include banning sugar and HCFS as an additive for food, combined with healthy diets and much, much more exercise. Exercise delivered by not using a car.
It appears to me than many or even most, of the problems on this planet are driven by US Lifestyles, form suburbs to relentless consumerism (aka rent extraction).
Again, can’t help but notice that countries with national healthcare have parliamentary govts (as much as pros and cons are noted).
In British Columbia the “BC Liberals” the so called “free enterprise party” which the voters tossed out last year was very friendly to any public private partnership scam they could design to get tax money to support private corporate ventures. This was a burden on the health care authorities and caused under investment in hospitals care homes (nursing homes) and other health services. Recently it wasn’t so much cuts as much as budget increases that were consistently less than the rate of inflation and rate of population growth with obvious results: longer wait lists and overcrowded hospitals. They did the same thing with education but that’s a different story. The new NDP government is in the process of, hopefully, correcting that. It mainly has meant that patients were backed up in costly hospitals or released to unprepared families, elderly spouses, etc, who were neither physically nor psychologically prepared to handle this. The BC Libs were skilled at underfunding things that remained largely out of sight except for people immediately affected. More money will now be devoted to all this but things move slowly. The NDP with the Greens have a thin majority in BC so they’re risk adverse and don’t want to make any mistakes. More MRI’s more rationalization of care with consolidation of multi disciplinary services at one location, increase use of nurse practitioners (which the doctors always drag their feet on – less money for them) 24 hour clinics instead of emerg depts. So of course, the BC Liberals slow steady squeeze was right out of the neoliberal playbook I watched in the States. Canada needs more doctors, nurse practitioners, etc, to take up the slack in primary care. The biggest enemy in Canada of making a good system even better vs worse leading to calls for privatization is which party gets elected in the provinces, and of course, which party gets to control parliament at the federal level.
Almost all Canadians are very supportive of Canada’s health care system, very proud of it, Tommy Douglas is a national hero, and although they complain about this and that, they maintain a touching (German word alert) shadenfreude over the plight of those poor benighted Americans and their horrible health care system. A knowing glimmer in the eye during that sad shake of the head, oh my.
The main danger, in my opinion, is that Canadians seem to take the continued existence of their Health Care system, which is really very good and cost effective, like they take the rising of the sun every morning – largely for granted. No politician will ever attack the Canadian system they say, and they’re right. Even the Conservatives always say the right things. The way neo liberals North of the border will attack it is in slow steps which is more difficult for ordinary people to see or even imagine. Which makes this ploy the biggest danger to Canada’s system.
Again, I can’t say enough good things about the system. You choose your own doctor, go to which ever specialist you and your GP decide on, care is very good, promt acording to your need. Maybe because I’m originally from America, I’m more naturally critical of things, and the topic was neo lib infestation of the system.
There is also the matter that Canadians spend about half as much per capita compared to Americans on healthcare, yet get better results.
As far as wait times, they are a challenge. The easiest solution would be to:
1. Increase spending on healthcare so that there are more doctors and nurses per patient
2. Increase the amount of residency slots
3. Expand preventative medicine spending
4. Expand coverage of areas not covered (most notably dental care)
Dollar for a dollar, a public system seems far superior than the privatized American system. The reason why neoliberals hate this is because deep inside they know it. That’s why they are desperate to get rid of it. They want people to suffer and rich people to get richer off of this.
I might add that BC does pay for NaturalPathic Medicine assesments including lab tests, eg blood tests for the assessment which also includes Traditional Chinese medicine assessments. All free. And that’s a good thing. But you pay for your own supplements.
Canada needs free Pharmacare which Trudeau promised but has yet to deliver on. Maybe we’ll see something before next year election. And it needs free Dental.
When the Affordable Care Act was enacted in 2014. My wife and I chose one of the plans with Blue Cross – here in California. This was good – since the monthly co-pay was something we could afford. We got health Insurance! Yay!
However, Blue Cross was hard to reach on the phone – hours wait sometimes – and when I had an operation – they tried to add all kinds of charges that were supposed to be included – and even say the doctor that was out of their HMO system – they were not. I had a fight over everything. Not to mention hours long waits to speak to an agent – every time I had to deal with their nonsense… and their awful phone music (it was an ear operation that I had)
Mid 2015: I got a letter from the State of California informing me based on my income they are placing us on Medi-Cal (Medicaid). Uh Oh… What would that be like? would it be Crap? Blue Cross had been a drag (though it was great to have health coverage)…
Turns out- Medi-Cal – administered locally by Central California Alliance for Health – where I live – is Great! Much better than that privately run health insurance.
Medi-Cal has been responsive – easy to reach – and the medical coverage is good for most things… This has made me a believer in ‘Medi-Cal for all’ – It seems like a system closer to what Canadians have. I feel fortunate to have it. (Not sure what will happen next year when I reach Medicare age.)
As an American widower at least in part because of how really F***** Up America’s fabulous healthcare is, whenever I read (the often mendacious or at least misleading) articles about the Evils of Socialized Medicine™️ I get really…annoyed.
We cannot that Evil Socialize Medicine too soon. Of course, there has been multiple serious attempts since at least the New Deal, and that’s only just over eighty years. Any day now…
Further to the barbarism and reverse lottery risk, there’s a growth killing aspect to the US health care problem.
As one of the “not-socialist-but-does-want-civil-society-and-yes-that-includes-effective-no-nonsense-government” fellow travelers on this board, it looks to me like health care costs and risks have become the biggest, though not the only, systematic barrier to a long overdue reinvention of American society and work.
That pool of “reinventors” is now truncated to the young, who have little need for docs and few goods to lose to the reavers in bankruptcy if they do, or else those with a supportive partner with coverage. Parents or oldsters outside the comfortable 20% need not apply.
Put more succinctly, I’d be vastly better off starting a small business, or a second career in my 40s, in Canada, Europe or even the feckless Philippines. Land of the free and home of the brave, not so much.
Everything counts in large amounts.
Shouldn’t no “individual mandate” also carry over to “no emergency room” without satisfactory proof of availabilty to pay?
There are requirements for house insurance, car insurance etc,
etc.
The wait time in a Canadian hospital tends to be roughly six hours, for a non-life threatening injury. To visit a walk in clinic you can expect at least a two hour wait. Unfortunately, the number of people without a family GP is growing. All these imperfections can be traced to one development: our twenty year doctor shortage. For such a shortage to last so long it has to be politically manufactured. Political parties in Canada may say what people want to hear about our health care system, however they are the worst enemies of the same system. Due to the immense popularity of the system with Canadians, our politicians must resort to killing it gradually – death by a thousand cuts. I hate to think how bold they’ll become the moment we have a real economic crisis.
The other pathetic thing is that we’ve been endlessly stealing doctors from India and China yet still have a doctor shortage. Let’s see, 30 million people in Canada, a billion in India and China. I wonder where the greatest need for these doctors is? Like natural resources,the West is good at plundering human resources too. Meanwhile poverty stricken Cuba sends its surplus doctors all over the world. Well Cuba isn’t poor when it comes to its politicians. We got the Trudeaus, they got the Castros. Can’t win them all!
We’ve been plundering MDs but not granting them medical licenses. Many experienced doctors from non-white countries have trouble getting medical residencies (without which they can’t get the license). The Ontario College of Medicine severely restricts these residencies because they think it will drive down their wages (the reason they give is that they don’t trust foreign, i.e. non-white, medical education). Many of these doctors end up downgrading to jobs in the pharma industry or BS like homeopathy or naturopathy. I’ve met and worked with quite a few of them.
JDD over at Richard North’s site has been posting for a while now that the US is imminently about use the WTO DSM against the Canadian healthcare system. The reason is that it is a government provided system and thus falls foul of WTO rules on subsidies as per SCM i.e. subsidies and countervailing measures.
If this succeeds the next case will be against the NHS after the UK leaves the EU.
Thanks for the tip. Do you have a link? (I’ve heard the same logic proposed for TTiP so this is not surprising. These international trade tribunals really need to be reined in; if the Administration manages to cripple them I’ll cheer and deal with any fallout later.
One overlooked social phenomenon that is having a huge impact on Canadian health care is the large numbers of hospital beds occupied by fentanyl mishaps. There are thousands of near overdoses every year in Vancouver alone and the medical system wasn’t designed to handle them all.
In British Columbia there is no affordable housing for young doctors either. Even if European doctors were welcomed with open arms and not cold shouldered by various associations, they would find it really tough to find housing.
Really is a perfect storm and not necessarily something that could be effectively solved through a private system. A private system would make it worse. We have been there through the hijacking of the vast ferry system here. It used to work very well at half the cost, adjusted for inflation, when it was run by the provincial government.
Fortunately for Canadians, we have the threat of a bad example South of the border. No matter how hard corporate interests push for privatization, it is unlikely to happen here.
It means that we will have longer waits for non-essential surgery. I can live with that.
I guess it’s nice that our misery can be put use as warning to others. ?
Thank you Lambert, for good research and analysis on a system that saved my life, and many other Canadians without a huge fee… is there a better reason to love our country?
Was born in New Zealand and lived there for 21 years of my life. Broke my collar bone in ’98. First ER visit I neglected to have surgery on it and see if a sling and time would let it heal (it didn’t). Went back next day, bone had moved per X-Ray. They admitted me, do not pass go proceed to surgery in a couple hours. Pins put in. 4 weeks in to the process one pin came out (pierced the skin… nicely sticking out of my shoulder). Went back to have the pin replaced and then four weeks later to have them all removed.
The total cost for this… wait for it… ZERO FREAKING DOLLARS. Why? Because we all pay in to the system in our lifetime, sometimes (hopefully) you reap the benefits later on in life and are able to live healthy and only need minor assistance late in life. Sometimes you need it earlier. Either way it is a social contract that we as a society understand if we take care of each other we are taking care of ourselves in the long run.
Cue living in the USA for the last 18 ½ years. What a joke our system is. It is about profiteering off the unfortunate medical conditions of others. Every single doctor I have hates the current system, the amount of confusion, the fact they need to keep insurance specialists and practice managers on staff to sort through all the crap. ALL of them feel like they are dictated how to treat their patients by MBA’s and not other doctors.
Back to New Zealand’s healthcare system and that it sucks now (words from my family living there still)! At the hands of the national party (same damn ideology as the Republicans that people kept electing year after year) they have dismantled the funding and the system itself. This is the sabotage part and they have been doing it for over 25+ years. Under fund and the system slowly breaks down, equipment becomes outdated or of ill-repair. Staff training suffers, facility maintenance falters thereby costing more to maintain, renovate or replace.
It is a systematic strategy of destroying a healthcare system. The next nicely gem they like to pull is pushing services and procedures to private hospital systems. So instead of sending someone through the public system, they push them to a private hospital (which in a lot of cases if a true emergency arises with the patient, they get shipped back to the public ER). This strategy is about setting up a false narrative that only private systems effectively in the long run and the “bloated” public system is proof of that and usually succeed with convincing the general population that private is the only way.
It is a con, it is profiteering at the expense of human dignity, well being and financial sustainability (our private health insurance in the USA is NOT sustainable at all). The same tactics are being used against social security (lest us forget GWB administrations attempt to privatize apart of it). Sell to the public that it is not sustainable and they will lose their benefits and push to privatize apart of it.
What a disgusting bunch of “human” beings we share a world with.
One issue with Canadian healthcare where I live (north Toronto inner suburb) is the $50 ambulance fee. Ambulances have been privatised in Toronto but despite the name it’s the hospitals that charge this fee. Fifty bucks might not sound like a lot but it’s a significant barrier for low income people. Taxis aren’t allowed to transport people in medical distress either because of insurance issues so some people either get an uber or pretend they’re okay to the taxi driver. It’s all part of the neoliberal strategy of crapifying the system into crisis and then privatising it, of course.