As readers know, I have long urged, following the science, that Covid is airborne, and that its main mode of transmission is via aerosols. (I was initially persuaded by an epidemiological study, now consigned to link rot, that showed a seat diagram on a Chinese bus with the index case and how many were infected. It seemed clear that neither fomites nor hacked up droplets could be the cause, since the seats were widely separated. Many more such studies followed. No such studies followed for fomites or droplets.) On April 30 — after enormous efforts from aerosol scientists — WHO changed its guidance to reflect that Covid is airborne. On May 7, CDC followed. So, after more than a year, we have finally agreed Covid’s mode of transmission. It is to be hoped that science-based mitigation measures — especially ventilation — follow.
In this post, I will first look at what WHO and CDC actually said. Then I will look at helpful materials produced by the aerosol scientists and their allies during their battle (which may prove helpful in further battles to come, especially in schools and workplaces). Turning to institututional slash political factors, I will look at why WHO and CDC delayed so long, and how the Biden administration seems oblivious to the paradigm shift from droplets to aerosols (going to far as to push useless, even dangerous, plexiglass shields).
What WHO and CDC Actually Said
First, WHO. From “Coronavirus disease (COVID-19): How is it transmitted?“:
The virus can spread from an infected person’s mouth or nose in small liquid particles when they cough, sneeze, speak, sing or breathe. These particles range from larger respiratory droplets to smaller aerosols[1].
- Current evidence suggests that the virus spreads mainly between people who are in close contact with each other[2] typically within 1 metre (short-range). A person can be infected when aerosols or droplets containing the virus are inhaled or come directly into contact with the eyes, nose, or mouth.
- The virus can also spread in poorly ventilated and/or crowded indoor settings, where people tend to spend longer periods of time. This is because aerosols remain suspended in the air[3] or travel farther than 1 metre (long-range).
People may also become infected by touching surfaces[4] that have been contaminated by the virus when touching their eyes, nose or mouth without cleaning their hands.
Further research is ongoing to better understand the spread of the virus and which settings are most risky and why.
Some notes: [1] The word “aerosol” actually appears. Good! [2] The “close contact” frame does not take superspreading — as on the Chinese bus — into account. [3] Here, superspreading is implicit, but not stated. [4] Dogma. Covid rarely spreads through fomites.
Now, CDC. From “Scientific Brief: SARS-CoV-2 Transmission“:
The principal mode by which people are infected with SARS-CoV-2 (the virus that causes COVID-19) is through exposure to respiratory fluids[1] carrying infectious virus. Exposure occurs in three principal ways: (1) inhalation of very fine respiratory droplets and aerosol[2] particles, (2) deposition of respiratory droplets and particles on exposed mucous membranes in the mouth, nose, or eye by direct splashes and sprays[3], and (3) touching mucous membranes with hands that have been soiled either directly by virus-containing respiratory fluids or indirectly by touching surfaces with virus on them[4].
Some notes: [1] Needless to say, this is a highly political document. CDC seems to need to think of aerosols as “respiratory fluids,” bless their hearts. [2] The word “aerosol” actually appears. Good! [3] Droplet dogma. [4] Fomite dogma. Note that CDC carefully does not say which mode is the primary mode.
And CDC again, for the layperson, in “How COVID-19 Spreads“:
COVID-19 spreads when an infected person breathes out droplets and very small particles[1] that contain the virus. These droplets and particles can be breathed in by other people or land on their eyes, noses, or mouth. In some circumstances, they may contaminate surfaces they touch[2]. People who are closer than 6 feet from the infected person are most likely to get infected.
Some notes: [1] The word “aerosol” is suppressed. [2] Fomite dogma.
Since this is CDC, we expect the deliverable to be sloppy and half-assed, and so it proves. From the University of Maryland School of Public Health, “Statement of Scientists in Response to CDC’s May 7th Announcement Recognizing Inhalation Exposure“:
[The “How COVID-19 Spreads” document] will lead people to continue to think that maintaining distance is sufficient to prevent transmission.
We know that transmission at distances beyond 6 feet occurs because of superspreader events, careful studies of smaller outbreaks, and the physics of aerosols. It can easily happen indoors in a poorly ventilated environment, when people are not wearing masks..
There is clear consensus among aerosol scientists and epidemiologists that inhalation of small aerosol particles, including at distances of greater than six feet, is a major driver of the COVID-19 pandemic. To slow transmission and save lives, it is crucial that CDC update its guidance and recommendations to address and highlight the importance of improved ventilation and using NIOSH approved respirators, especially in indoor locations where the virus may accumulate in the air. .
Moreover, OSHA must issue an Emergency Temporary Standard to control workplace exposures, including inhalation exposure, as soon as possible in order to protect workers and reopen the economy safely.
Nevertheless, CDC did speak the unspeakable word — aerosols! — so that is a victory.
Helpful Materials for Air Breathers
I cannot summarize the history and politics of the battle to recognize aerosol transmission because I was not in those rooms.[1] However, I can highlight the literature that I found most illuminating along the way. (As Mr. Rogers says: “Look for the helpers.”). The literature falls into two buckets: Scientific Communications, and Scientific Papers.
Scientific Communications
First, University of Colorado aerosol scientist masterfully circumvented the United States press with this article in the English language version of El Pais: “A room, a bar and a classroom: how the coronavirus is spread through the air.” It’s one of those mobile-friendly interactive pages, but it is still worth a read even today. Here is a classroom situation:
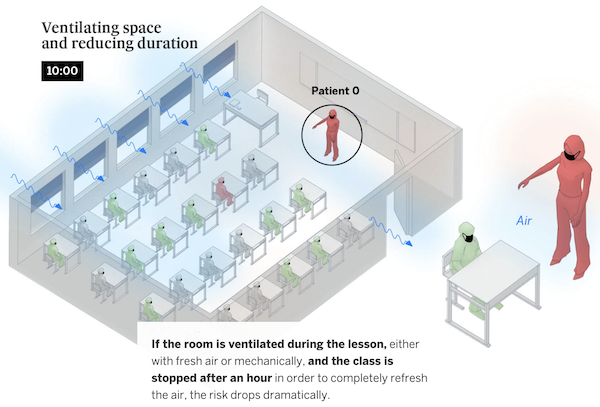
I saw this paper cited many times in discussions of school reopenings on the Twitter, so at least some parents may have been able to protect their children from CDC’s miserably inadequate school reopening guidance, which did not consider aerosol transmission in the United States, not even in its scientific references.
Second, this wonderful article in the Lancet, “Ten scientific reasons in support of airborne transmission of SARS-CoV-2.” Here are two of the 10 points. Recall that neither droplets nor fomites can give an account of superspreading events:
First, superspreading events account for substantial SARS-CoV-2 transmission; indeed, such events may be the pandemic’s primary drivers. Detailed analyses of human behaviours and interactions, room sizes, ventilation, and other variables in choir concerts, cruise ships, slaughterhouses, care homes, and correctional facilities, among other settings, have shown patterns—eg, long-range transmission and overdispersion of the basic reproduction number (R0), discussed below—consistent with airborne spread of SARS-CoV-2 that cannot be adequately explained by droplets or fomites. The high incidence of such events strongly suggests the dominance of aerosol transmission.
Sixth, viable SARS-CoV-2 has been detected in the air. In laboratory experiments, SARS-CoV-2 stayed infectious in the air for up to 3 h with a half-life of 1·1 h.12 Viable SARS-CoV-2 was identified in air samples from rooms occupied by COVID-19 patients in the absence of aerosol-generating health-care procedures13 and in air samples from an infected person’s car. Although other studies have failed to capture viable SARS-CoV-2 in air samples, this is to be expected. Sampling of airborne virus is technically challenging for several reasons, including limited effectiveness of some sampling methods for collecting fine particles, viral dehydration during collection, viral damage due to impact forces (leading to loss of viability), reaerosolisation of virus during collection, and viral retention in the sampling equipment. Measles and tuberculosis, two primarily airborne diseases, have never been cultivated from room air.
Third, this handy chart from the British Medical Journal, “Two metres or one: what is the evidence for physical distancing in covid-19?”:
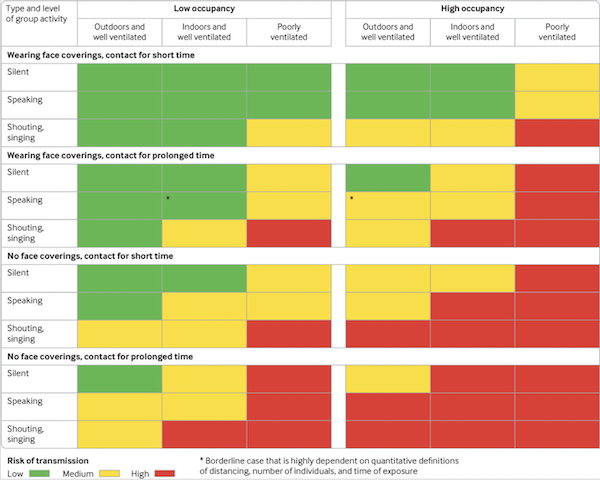
(Tricia Greenhalgh has aggregated translations of this chart here.) I like this chart first, because it’s small (as opposed to that ludicrously ginormous CDC chart I printed the other day) and second because its simple: Actions (singing, breathing, masking, not masking) on the vertical axis, built environment on the horizontal. The famous Skagit County choir practice superspreading event, for example, is at bottom right (red, unsafe). Singing, no masks, prolonged contact, high occupancy, poorly ventilated. A silent walk with your friend in the park, both masked, would be top left (green, safe)
Scientific Papers
We have all linked to many, many papers on aerosols, but this paper (I hope) is extraordinary: “Indicators for Risk of Airborne Transmission in Shared Indoor Environments and their application to COVID-19 Outbreaks.” (I say “I hope” because the math is over my head; I hope some maven in the readership will give it a go.) In essence, the authors have devised a formula for calculating the risk of indoor transmission, based on a set of parameters. They then aggregated and tabulated a large number of aerosol studies and threw them against the formula, with parameter values taken from real events as documented by epidemiological studies. From the body of the paper:
An important advantage of the simplified risk parameters is that their values can be calculated
for outbreaks that are documented in the scientific literature. Values for documented COVID-19 outbreaks are shown in Table 1 (rE and rB are estimated based on the likely types of activities in each case (33, 37, 44), see Table SI-2 for typical values). Also included are values for outbreaks documented in the literature for tuberculosis and measles, which are widely accepted to transmit through the air, and an influenza outbreak that was clearly due to airborne transmission.
The authors then took the formula and turned it into a calculator:
12/ If you want to calculate the risk parameter for your situation, you can do so with the COVID-19 Aerosol Transmission Estimator, freely available online.
(Modify sheet "Master-choir" — will transplant to the others)https://t.co/t9qPriPMYX pic.twitter.com/twCY1XzbtT
— Jose-Luis Jimenez (@jljcolorado) May 2, 2021
Here is the calculator. It made me scream and run; the calculator needs to be made usable by, say, an HVAC person in a school (and not a high-priced consultant). But that’s what software is for, so this is a mere implementation detail.
The Disgraceful Response of the CDC (and WHO)
Here I can do no better than to quote a great slab of Zeynep Tufecki’s “Why Did It Take So Long to Accept the Facts About Covid?” in the New York Times, which you should read in full:
Why did it take so long to understand all this?
One reason is that our institutions weren’t necessarily set up to deal with what we faced. For example, the W.H.O.’s Infection Prevention and Control (I.P.C.) global unit primarily concentrates on health care facilities. Many of the experts they enlisted to form the Covid-19 I.P.C. Guidance Development Group were hospital-focused, and some of them specialized in antibiotic-resistant bacterial infections that can spread wildly in health care facilities when medical personnel fail to regularly wash their hands…. Further, in some countries like the United States, they tend to have extensive engineering controls to dampen infections, involving aggressive air-exchange standards, almost like being outdoors. This is the opposite of modern office and even residential buildings, which tend to be more sealed for energy efficiency. In such a medical environment, hand hygiene is a more important consideration, since ventilation is taken care of. Another dynamic we’ve seen is something that is not unheard-of in the history of science: setting a higher standard of proof for theories that challenge conventional wisdom than for those that support it.
As part of its assessment of the virus’s spread, the W.H.O. asked a group of scientists last fall to review the evidence on transmission of the coronavirus. When reviewing airborne transmission, the group focused mostly on studies of air samples, especially if live virus was captured from the air, which, as mentioned above, is extremely hard. By that criterion, airborne transmission of the measles virus, which is undisputed, would not be accepted because no one has cultivated that pathogen from room air. That’s also true of tuberculosis. And while scientists, despite the difficulties, had managed to capture viable SARS-CoV-2 in three studies that I’m aware of, the review noted that the virus was detected only intermittently in general, disputed whether the captured live virus was infective enough and ultimately said it could not reach ‘firm conclusions over airborne transmission.’ The lead author and another senior member of the research group previously said they believed transmission was driven by droplets.
The skepticism about airborne transmission is at odds with the acceptance of droplet transmission. Dr. Marr and Joseph Allen, the director of the Healthy Buildings program and an associate professor at Harvard’s T.H. Chan School of Public Health, told me that droplet transmission has never been directly demonstrated. Since Dr. Chapin, close-distance transmission has been seen as proof of droplets unless disproved through much effort, as was finally done for tuberculosis.
Another key problem is that, understandably, we find it harder to walk things back. It is easier to keep adding exceptions and justifications to a belief than to admit that a challenger has a better explanation.
…[T]he initial public health report on the [Skagit County] Mount Vernon choir case said that it may have been caused by people “sitting close to one another, sharing snacks and stacking chairs at the end of the practice,” even though almost 90 percent of the people there developed symptoms of Covid-19. Shelly Miller, an aerosol expert at the University of Colorado Boulder, was so struck by the incident that she initiated a study with a team of scientists, documenting that the space was less full than usual, allowing for increased distance, that nobody reported touching anyone else, that hand sanitizer was used and that only three people who had arrived early arranged the chairs. There was no spatial pattern to the transmission, implicating airflows, and there was nobody within nine feet in front of the first known case, who had mild symptoms.
The Biden Administration Stumbles
Finally, we come to the Biden administration, which seems completely unaware that a paradigm shift in our understanding of Covid’s mode of transmission is occurring. I presented this video once, but it still frosts me, so I’m going to present it again:
President Biden: "You guys are impressive."@POTUS and @FLOTUS visit an elementary school in Virginia pic.twitter.com/Ohs38tcBW6
— The Hill (@thehill) May 3, 2021
First, as should now be obvious, plexiglass screens don’t protect school children from aerosols, because the aerosols, just as cigarette smoke would, go around the barriers.
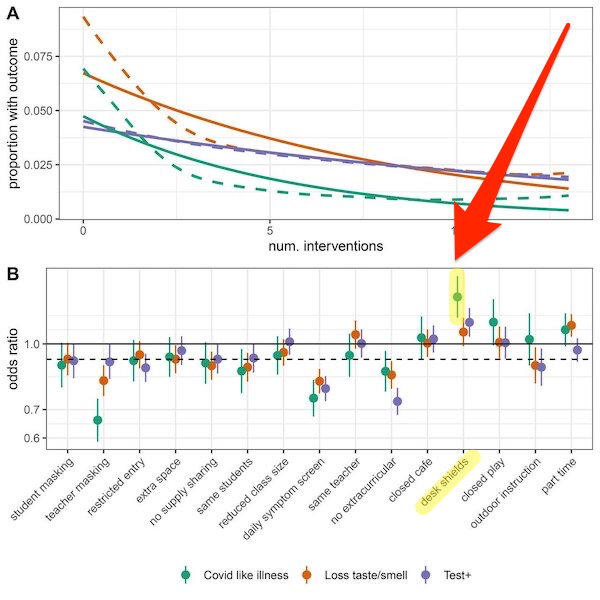
Second, plexiglass screens may actually increase the danger of Covid transmission. Here is a handy chart from Science, “Household COVID-19 risk and in-person schooling“:
Here is a video from one of those helpful aerosol scientists explaining why:
I have been lots of questions about plexiglass barriers–this is the best visualization that I have seen. They are designed to block big droplets produced in sneezes and coughs. Aerosols float right around them and can actually concentrate near a person sitting on the other side. https://t.co/0jKd0fk32s
— Kimberly Prather, Ph.D. (@kprather88) December 17, 2020
And we have a real-life example. From medRvix: “Weekly SARS-CoV-2 screening of asymptomatic students and staff to guide and evaluate strategies for safer in-person learning,” the Conclusion:
In this school district with layered mitigation measures, in-school transmission was rare. The program identified a cluster with in-school staff-to-staff transmission and spurred enhancement of safety strategies.
And here are some of those enhancements:
First, review of heating, ventilation, and air conditioner (HVAC) systems, including assessment of airflow in the main office using smoke, suggested airflow impedance in the main office area attributed to plexiglass dividers with sidewalls; these structures were rearranged.
As I read the study, then, plexiglass dividers actually contributed to an outbreak.
When I see that [family blogging] Biden video, I want to ask “Who did this?” The room is poorly ventilated. Plexiglass dividers are at best useless, at worst dangerous. It’s a dangerous place for students to be! And yet we have a President “modeling behavior,” as we say, based on an obsolete paradigm for transmission. So all over the country school districts are going to be buying plexiglass barriers instead of fixing their ventilation systems! Ron Klain, Biden’s chief of staff, was sold to us as a pandemic expert based on his Ebola Czardom. Was Klain asleep? Not paying attention? Advised by some droplet goon at Walensky’s CDC? Fondling his West Wing box set? Who knows. What a debacle!
Piling debacle upon debacle, we know have this idiotic statement by Fauci. From CNN:
Sunday on ABC News, Fauci was asked whether it’s time to start relaxing indoor masks requirements. Fauci replied, “I think so, and I think you’re going to probably be seeing that as we go along, and as more people get vaccinated.”
Madness, because as aerosol theory predicts, and fomite and droplet theories do not, indoors spaces are the most dangerous spaces (see Greenhalgh’s helpful chart above). We don’t know, for any given space, how many people within in will be vaccinated. We also do not know how many have been vaccinated and are still capable of asymptomatic spread — and hence, in a closed space, of becoming superspreaders. Fauci should be focusing on ventilation, which actually makes people safer, instead of playing Philosopher King and using some people’s desire to unmask to manipulate them into getting vaccinated.
Conclusion
Concluding, the intellectual victory needs to be fought out on the ground of mitigation (which, above, both Biden and Fauci butchered). From the Toronto Globe and Mail:
A transition to an airborne approach revolves around a simple and powerful concept: COVID spreads by breathing shared air, and infectious air accumulates indoors.
Primary mitigation strategies shift from two metres distancing and handwashing to ventilation and high-quality masks. Monitor ventilation using portable carbon dioxide monitors, open windows and emphasize improvements in ventilation or air filtration when ventilation systems are poor. Distancing remains important but high-quality respirators should always be worn while indoors. All breaks and meals where masks will be removed must be moved outdoors or, when outdoors is not possible, in large well-ventilated rooms with maximal distancing and small numbers of people.
While airborne transmission is now acknowledged, changes to infection prevention strategies and efforts to increase public awareness are lacking. These changes will reduce onward transmission in high-risk settings and provide opportunities for a return to normalcy in some spheres: outdoor activities (where aerosols are rapidly dispersed) and even some indoor spaces with guidance on how to eliminate aerosol combined with proper masking.
Shifting to an airborne prevention approach will be life-saving for people working in high-risk essential jobs, and for the families to whom they bring home the infection. It will also impact overall epidemic control and help guide a safer more sustainable economic reopening.
One of the nice things, of course, about mitigation strategies like this is that — unlike today’s vaccines — they’ll work when the next airborne pandemic comes along. We sure dodged a bullet that Covid wasn’t as contagious as measles. Eh?
NOTES
[1] I can say that the aerosol advocates reminded me very much of MMT advocates. It may be that the pleasant group dynamics gave both thought collectives some leverage to effect their desired paradigmatic shifts.


As readers know, I have long urged, following the science, that Covid is airborne, and that its main mode of transmission is via aerosols.
Indeed, you have, and kudos for this. My comments on the WHO, et al, will remain, um, self-muted. / ;)
“I was initially persuaded by an epidemiological study, now consigned to link rot, that showed a seat diagram on a Chinese bus with the index case and how many were infected.”
That study was, for whatever reason, later retracted.
I remember its disappearance. From your retraction watch link:
So my thought was that the reason for the retraction was political, or geopolitical.
In any case, the case primed me for later incidents, e.g. Skagit Valley.
I wouldn’t be using that language — it can be seen as an excuse for what has happened so far, i.e. they just did not know, but now they are seeing the evidence and having to change their mind.
In reality, there is no paradigm shift — it was well known that it was airborne from the beginning by everyone who bothered to look into it.
Including by the government.
Remember those Bob Woodward revelations about Trump? One of the things Trump had said was “you just breathe and you catch it”. Which very clearly indicates that Trump himself knew it was airborne in January/February 2020, and that means the people around him, who told him that, knew it too.
So the CDC has been deliberately lying since the beginning, the WHO has been deliberately lying, Fauci has been deliberately lying, etc. etc.
This ^^ .
Which is why we should keep wearing those [family blogging] masks and remaining socially distant.
It’s airborne.
And, if I or anyone else reading this comment catches COVID, I think we’re entitled to the same level of treatment that Trump had last fall.
The thing that did it for me was the COVID due to airflow in a chinese restaurant, followed by a study of a high rise apartment building sharing a common chase.
This document prepared by Jose Luis Jimenez and other scientists has a lot of information about how to protect yourself from aerosol transmission: https://docs.google.com/document/d/1fB5pysccOHvxphpTmCG_TGdytavMmc1cUumn8m0pwzo/edit
Just want to thank you for all your work on this!
Ignoring aerosol transmission is part and parcel of an incompetent corrupt government that serves and protects greed not the people. Likewise, the CDC ignores the breakouts of COVID-19 in fully vaccinated persons. Yes, the number of cases is significantly less and symptoms are not as severe. But deaths have been reported and more long-COVID cases are likely. The transmission by asymptomatic vaccinated carriers of the new variants to the unvaccinated and those without a booster shot appears likely. There will be significant populations of unvaccinated next winter in the USA and especially the rest of the Americas who cannot afford the jabs, hesitant, or turned off by the politicization of the pandemic.
It is criminal negligence by the Biden/Harris Administration not to use the decrease in numbers of COVID cases this summer and fall not to test, contact trace, quarantine, mask, social distance, and personnel hygiene, all at once, to eradicate the virus and avoid a fourth spike, an economic collapse, and more unrest next year.
I think Fauci said he was worried there were not enough masks for health care workers so he played the aerosol down. I think he and our leaders live in such a pampered world that it never occurred to them that they could just tell people to make their own with vacuum cleaner bags between layers of old T shirts. You could make a 95 mask with the top of a soda bottle and a vacuum cleaner bag as well. Since when are Americans incapable of making their own masks at home? It was just a failure of imagination.
I don’t think it would be effective to eradicate the virus in the US without eradicating the virus in the entire world
Let’s not throw the baby out with the bathwater though.
Just because most of the spread is airborne, and this has been denied for so long by the powers that be in order to serve the economic interests of the ruling capitalist class at the expense of public health, it does not follow that one should not be paying attention to surfaces.
The problem is that first, fomites are almost impossible to contact trace, so there are not that many well established examples, and second, while regular-fabric face masks are not good at keeping aerosols out, they are good at keeping droplets in.
So the usual sources of fomites have been largely eliminated — under normal circumstances, people cough, sneeze and spit all over surfaces and those surface are as a result coated with germs. Fomites for this virus arise from respiratory droplets (this is not Ebola) and occasionally from fecal matter, and by definition aerosols float and droplets drop.
Mask wearing has eliminated much of the fomite generation, but that situation will presumably return once people stop wearing masks.
While fomite contact tracing is difficult, it has nevertheless been demonstrated on multiple occasions, and it is also well known for other viruses and this one has been shown to survive well on surfaces, i.e. there is no reason to think it does not spread that way. We have examples of elevator buttons, garbage bin lids, and other stuff of the sort, and my personal favorite — a sewage pipe bursts and contaminates the ground with fecal matter, which is then carried on people’s shoes into their homes, which leads to infection with SARS-CoV-2 (think about how far fetched that sounds, yet it did happen).
So I personally do not plan to stop wearing gloves in high-traffic public areas any time soon.
> So I personally do not plan to stop wearing gloves in high-traffic public areas any time soon.
I think you are wise. Generally, I do add a qualification to the effect that fomite transmission is certainly possible in cases where there are sanitation issues. And yes, I wash my hands a lot. But so far as we know, the cases of fomite transmission are very, very low.
This is a reminder to carry my trusty alcohol spray bottle to the gym. 30 seconds kills Covid. I spray things I will handle, wander away for a bit and then come back. And wash my hands a couple of times too.
Problem with gloves is gloves can transmit fomite junk to your face too. Maybe as a researcher you are disciplined enough and have big enough supplies to strip them off and don new ones regularly, but most mere mortals don’t.
I like gloves to help keep me mindful of what I am doing–avoiding Covid. I put that as priority one, but it is always battling my old “normal” ways of doing things. I use the clear plastic, slightly oversized disposable ones made for food handlers–but there is the key–once they are on, I treat them as if they were my skin, so if I would apply sanitizer to my skin, I apply it to the gloves instead. (cuz I’m sometimes too lazy to change gloves). And I try to remain aware of what I’m touching, in succession–so doorhandle, could have a fomite, then keys, whoops…..
Of course, with my Narwall mask, can’t touch any facial membranes, so there is that too……
I stopped going to the Gym. Too dangerous because of the puffing and wheezing from exercise.
I ride a cycle in the open air, with very few encounters with other people mask, and hope that sunlight kills the virus.
I have a well developed reflex to never touch my face with gloves on after many years of working in labs. So having gloves on helps, at least to me, to not touch my face. They also have a smell, so it is easy to notice when they are close to your face. And, of course, you are masked too.
Also, they can be washed a lot better than hands — hands have a lot of nooks and crannies that are difficult to reach (thus the long and complex surgical hand washing routine), gloves are smooth. So if you have XL gloves and you normally wear L gloves, you can wash them while they are on your hands, then remove them and reuse them. (this can’t be done so easily with the ones that are your size and thus fit tightly). They will last through 10-15 cycles of that
P.S. I stashed some XL gloves in early February last year for that reason — research has been hit quite hard with shortage since then and they have not been seen anywhere for months, we only get smaller ones now…
Amends in advance but the whole thingy has the perfumed airs of a on the trot insurance disclaimer, w/ a vestige tail of Science, too gab about in some distant court room or media PR [evolution vs creation lvl lawyering] in the possible future … I mean that is how the neoliberal market[tm] works …
On top of all that Dr. AIDS made bank and obviously was Flexian enough to get invited to all the right parties and functions and now has the misfortune of having to play media science guy[tm] to a splintered nation whilst political factions are having a theatrical production of the Hunger Games for style points – too the aforementioned. Just imagine the pressure perceived or received by C-corps and the financial sector to not mess with the plate spinning world record attempt …. whoooo boy …
For some reason I’ve got the old episode of ‘Awful Truth’ playing in my head, the kidney drama, duplicitous contract which both states yes and no to transplant and how that all rolled … yet now we all act surprised – ????
> On top of all that Dr. AIDS made bank and obviously was Flexian enough to get invited to all the right parties and functions and now has the misfortune of having to play media science guy[tm] to a splintered nation whilst political factions are having a theatrical production of the Hunger Games for style points
“the old is dying and the new is struggling to be born….”
Lmmao …. @ link … and GBD[???] is that the drug that killed River Phoenix I presume …
Well, not directly. We have systems for that. Frankly, CDC and WHO did a pretty good job at that, if one is inclined to ignore Hanlon’s Razor, with their denial of aerosols.
PIXIES – Gouge Away
https://www.youtube.com/watch?v=FiUNDeuBbi8
My life suxz … I went to a concert … nothing changed … and people payed for the experience …
Its a poetry that wreaks my soul, but in its destruction I must persist, not for myself but others, till final gasp….
I wonder if years from now, that medical historians will be able to analyze the death rate for countries like the UK, Germany, US, etc. compare it with those countries that took precautionary methods like masks, social distancing, contact tracing, etc, that would be effective against aerosol spread, and then work out how many excess deaths there were because the WHO and the CDC slow-walked all recognition of aerosol transmission of this virus. In fact, not only did they refuse to recognize aerosol spread but the establishment used their clout to suppress studies showing aerosol spread. Unforgivable that.
I saw a doco on the pandemic the other night and it was bizarre the number of people that thought that a virus in China would never reach their part of the world whether the UK or Iceland. And I am including actual doctors here. It was only when family members died that they began to wake up to say oh yeah, this is real now. They saw countries like China and other countries get on top of this virus and yet they refused to learn the lessons. Turns out that the medical authorities in most countries in the world were not fit for purpose. Surprise!
COVID, being the greatest crime against humanity in modern history since The Holocaust (which it will likely greatly surpass in body count — we are already approaching 10M deaths accounting for the lack of proper counting in poorer countries), deserves its own Nuremberg trials. Because all of this death and suffering was deliberately allowed to happen, and that was openly admitted — it has been lost to the rapid flow of history in the months since then, but prominent heads of government were openly saying “such and such number of you are going to die and we are not going to do anything to stop it” in early March 2020, and subsequently only locked down whenever there was such a threat and for only as long as necessary to avoid the unacceptable for PR purposes situation of people dying outside of hospitals because there is no space inside the hospitals (deaths inside a hospital were perfectly OK, and their number did not matter).
So basically everyone in power in the countries that let it spread, plus, of course, the corporate big shots who told them to do that, should be on trial the same way the Nazis were after WWII — the Nazis exterminated millions and intended to do the same to many more with the goal of taking over the natural resources that those millions were in possession of, and what is basically the exact same thing was done here too — properly dealing with COVID would have required redistribution from rich to poor, that could never be allowed, so the poor had to die in large numbers instead, and not only that, but there was another huge upwards transfer of wealth engineered too (why let a good opportunity go to waste?).
Naturally that’s a taboo topic though, and it will never happen because the people responsible are the ones in power.
And scientists will not breach that subject either, because it would mean people at the WHO and the CDC going on trial too, and they just cannot accept that their buddies there could do anything wrong.
I’ve literally had the conversation multiple times with other scientists, both older and younger, about how the WHO and CDC lied deliberately on countless occasions, and how they have no credibility left whatsoever as a result, and the reaction is always one of bafflement — how could the WHO and CDC not be reliable? That does not compute. Yeah, sure they made mistakes, but they are honest and good people, etc. You point to them to the long list of very clearly deliberate lies that killed millions, and they just refuse to accept it.
And tragically, a month or so ago, the NY Times ran a story about various PPE startups on the verge of bankruptcy because no one has any idea that they’re selling N-95s, with proper approvals, because for example Amazon and Ebay are banning listings and hospitals prefer to buy cheaper N-95s from Asia through existing supply chains. (I assume GPOs play some role in this; now there’s an anti-trust target if there ever was one; they’re actually exempt!)
How appalling.
I live in East London in an artists collective. The building is a decommissioned Salvation Army hostel that was specifically designed to minimize air flow for the sake of fire prevention.
I have been in a running battle since March 2020 with both the landlord and the London Fire Brigade.
In 2018, there were 261 fire related deaths in the UK. Since the pandemic began, there there been nearly 130,000 deaths attributed to Covid.
No matter how much state-of-art scientific research I threw at them proving that maximizing air flow was the simplest way to minimize Covid transmission and exposure, both adamantly insisted that regulations require that fire doors be kept shut at all times.
I offered to only keep the doors open between 8:00 a.m. and 10:00 p.m. and to appoint monitors to make sure the schedule was scrupulously maintained.
Nope. Regulations require that the fire doors must always be kept shut.
Someone once derisively said that England is a nation of shopkeepers. I’m beginning to believe that it is a nation of bureaucratic box tickers.
And all those people who caught Covid, especially severe cases (as the intensity of the illness is directly proportionate to virion exposure) or died, are in no position to complain.
But at least the regulations were strictly adhered to.
Great recapitulation. Thank you.
I personally could never see how the virus would not be present in aerosols and therefore avoided breathing other peoples’ air from near day 1.
Watching the all over the map politicians, including Fauci, who could never speak a sentence without a qualifier was interesting and disheartening.
Zeynep Tufecki has somewhat paralleled Lambert in calling out aerosols and may accrete a following that will get ahead of the next pandemic. Check her out.
Breathe safe.
Anybody have data on how if at all aerosols travel in airplanes?
Short answer is that airplane air is continually recycled and they have very high quality filters, so your main risk is from aerosols that haven’t been recycled yet. This typically means from passengers within a few rows of your spot.
It is a notoriously difficult problem to study owing to the difficulty of pinning down the plane trip itself as the transmission vector (as opposed to the airports or other activities before or after the flight). Here is one study (not peer reviewed at publication time) that did so with some rigor.
It does seem clear that the filters must work, otherwise every plane flight would be a superspreader event. However they aren’t instantaneous, and the risk is definitely higher than most of the airlines are representing.
Long-haul flights are also more dangerous, because it’s possible to pass the Covid test before boarding, and the develop viral load on the flight itself. There was a case of an flight via Dubai (?) to Ireland where this happened; caused a superspreader event in Ireland.
I think this is the study you are referring to – newspaper summary here.
This from the NYT applies to ivermectin, fluvoxamine : “Another key problem is that, understandably, we find it harder to walk things back. It is easier to keep adding exceptions and justifications to a belief than to admit that a challenger has a better explanation.”
It would cost a lot of money to install real and workable anti-aerosol ventilation into millions of currently unventilated, underventilated, and anti-ventilated buildings. But that just means that there is a lot of opportunity to spend a lot of money up-ventilating all those buildings. It could be a lucrative and jobs-jobs-jobs creating part of the Biden Infrastructure Plan.
If somebody with powerful influence over the Joemala Administration could convince President Joemala about that, then we might get that pro-ventilation spending done and get all that counter-aerosol ventilation installed.