The information war takes a dark turn as the corporate media transitions from misinformation and obfuscation to outright lies and fabrication.
The campaign against ivermectin is intensifying in the US. Until recently the health authorities appeared to be quite content merely to ridicule those who take or prescribe the drug in order to treat or prevent Covid-19. A couple of weeks ago, the FDA released a now-infamous advertorial on twitter with the heading “You are not a horse. You are not a cow. Seriously, y’all. Stop it.” The subheading: “Using the drug Ivermectin to treat Covid-19 can be dangerous and even lethal. The FDA has not approved the drug for that purpose.”
It’s a subtle message that has been faithfully echoed by the corporate media: ivermectin, a tried-and-tested drug that has won its discoverers a Nobel Prize for the impact it has had on human health over the last 35 years, should only be given to animals. But now the information war is taking a darker turn, as the media transitions from misinformation and obfuscation to outright lies and fabrication.
At the end of last week, a string of American and British outlets, including The Daily Mail, Rolling Stone, Huffington Post, The Independent, Newsweek, The Guardian, and Yahoo News, ran a story about how people who had “overdosed” on the “horse dewormer” were clogging up so many beds in a hospital in Sequoyah, rural Oklahoma, that doctors were having to turn away gunshot victims. The story, sourced to local Oklahoma outlet KFOR, turned out to be completely false. On Sunday, the hospital in question released a statement that the doctor behind the allegations had not worked in its ER for two months. More to the point, the hospital “had not treated any patients due to complications relating to taking ivermectin.” There were no overdoses. And it had turned no patients away.
In other words, everything about the story was false. A total fabrication. Yet many of the mainstream outlets that covered the story did not retract their article. Rolling Stone simply “updated” its piece with the new information. The Guardian inserted a note at the bottom of its article informing readers that Sequoyah NHS had released a statement asserting that the doctor behind the allegations that formed the entire basis of the story had not worked in its ER for two months. In other words, you have to read all the way to the end of the article to find out that its entire content is total bullshit. To make matters worse, The Guardian did not even mention the hospital’s categorical denials that it had treated patients for IVM overdose or that it had turned ER patients away.
The Coming Crack Down
If the goal of all this disinformation is to put people off wanting to get hold of ivermectin, it doesn’t seem to be working, which is hardly surprising given the already desperately low levels of public trust in both US health authorities and corporate media.
There are certain parallels with the furore whipped up over hydroxychloroquine last year. But the case is weaker this time, primarily because IVM is one of the safest medicines on the planet and was widely recognised as such until this pandemic.
One thing that is abundantly clear is that mocking people’s intelligence and comparing them to horses or dogs for wanting to take a certain medicine isn’t a terribly effective way of getting them to change their behaviour. All they appear to have achieved is to invoke the “Streisand effect.” More people are buying ivermectin (for human use) than ever before. In the US as a whole, prescriptions for the medicine have surged 24-fold since the pandemic began, from 3,600 a week to almost 90,000. Between mid-July and mid-August alone, they rose 400%.
In response, authorities are escalating their crack down. On September 1, the American Medical Association (AMA), American Pharmacists Association (APhA), and American Society of Health-System Pharmacists (ASHP) jointly called for an outright ban on the dispensing of ivermectin to prevent or treat COVID-19 outside of a clinical trial.
We are alarmed by reports that outpatient prescribing for and dispensing of ivermectin have increased 24-fold since before the pandemic and increased exponentially over the past few months. As such, we are calling for an immediate end to the prescribing, dispensing, and use of ivermectin for the prevention and treatment of COVID-19 outside of a clinical trial. In addition, we are urging physicians, pharmacists, and other prescribers—trusted health care professionals in their communities—to warn patients against the use of ivermectin outside of FDA-approved indications and guidance, whether intended for use in humans or animals, as well as purchasing ivermectin from online stores. Veterinary forms of this medication are highly concentrated for large animals and pose a significant toxicity risk for humans.
Demonising a “Wonder Drug” (Not My Words)
While it is true that ivermectin was first commercialised as a product for animal health in 1981, fast becoming one of the world’s biggest selling veterinary drugs, it has been used to treat humans since 1987. But most of those humans were in poor countries. As a 2017 article in Nature noted, ivermectin, perhaps more than any other drug, “is a drug for the world’s poor. For most of this century, some 250 million people have been taking it annually to combat two of the world’s most devastating, disfiguring, debilitating and stigma-inducing diseases, Onchocerciasis and Lymphatic filariasis”
“Ivermectin was a revelation. It had a broad spectrum of activity, was highly efficacious, acting robustly at low doses against a wide variety of nematode, insect and acarine parasites. It proved to be extremely effective against most common intestinal worms (except tapeworms), could be administered orally, topically or parentally and showed no signs of cross-resistance with other commonly used anti-parasitic compounds.”
Since the late ´80s more than 3.7 billion doses have been distributed globally in mass drug administration campaigns. All 3.7 billion of those doses were provided free of charge by the medicine’s developer, Merck. The company knew it would not be able to generate profits or even cover costs by selling the drug in the poverty-stricken communities afflicted by the two parasites, so it gave it away. “As much as needed for as long as needed” was the motto. It was a remarkable — and exceptionally rare — gift of generosity from a major pharmaceutical company.
Later on, it was discovered that ivermectin had many other properties. Using the drug as a long-term preventive against onchocerciasis had reduced the prevalence of other parasitic worms known as soil-transmitted helminths, which infect up to 20% of the world’s population and are a common cause of malnutrition and growth impairment in children. It was also discovered to have potent anti-viral effects.
After being used billions of times, this (in the words of Nature magazine) “enigmatic, multifaceted wonder drug” has been shown to have “an extremely good safety profile” — again Nature‘s words — as well as potential applications against a broad spectrum of diseases, from African trypanosomiasis (sleeping sickness) to schistosomiasis, one of the world’s most neglected tropical diseases that afflicts more than 200 million people worldwide; to asthma and epilepsy; to a host of RNA viruses including Zika, dengue, yellow fever, West Nile, chikungunya and HIV. It also appears to have potent anti-cancer properties.
Today, the FDA, with a little help from the media, is doing everything it can to destroy ivermectin’s reputation. At the same time, authorities appear to be clamping down on the importation, distribution and sales of the medicine. They are also beginning to crack down on doctors who have been prescribing the drug, regardless of how much success they’ve had with it.
A Whole Different Story Half a World Away
In Asia, the situation could not be more different. In India the Indian Council of Medical Research (ICMR) — the most important biomedical research body in India and one of the oldest and largest medical research institutes in the world — has added ivermectin in its indication for Covid-19 to its list of essential medicines.
In June, one of three national health regulator in India, the Directorate General of Health Services, (DGHS) overhauled its COVID-19 treatment guidelines and removed almost all of the repurposed medicines it had previously recommended for treating asymptomatic and mild cases, including ivermectin. This sparked concerns that India was about to reverse its approval of ivermectin as a covid treatment. But to their credit, India’s two most important national health regulators — the All India Institute of Medical Science (AIIMS) and the Indian Council of Medical Research (ICMR) — maintained their authorisation of ivermectin.
It’s hard to keep track of just how many states in India continue to use ivermectin as a treatment or prophylaxis against covid-19. Three states that are definitely using it are Uttar Pradesh (population: 230 million), Goa and Bihar (population: 100 million), a copy of whose home quarantine treatment program can be seen here. So, too, is New Delhi.
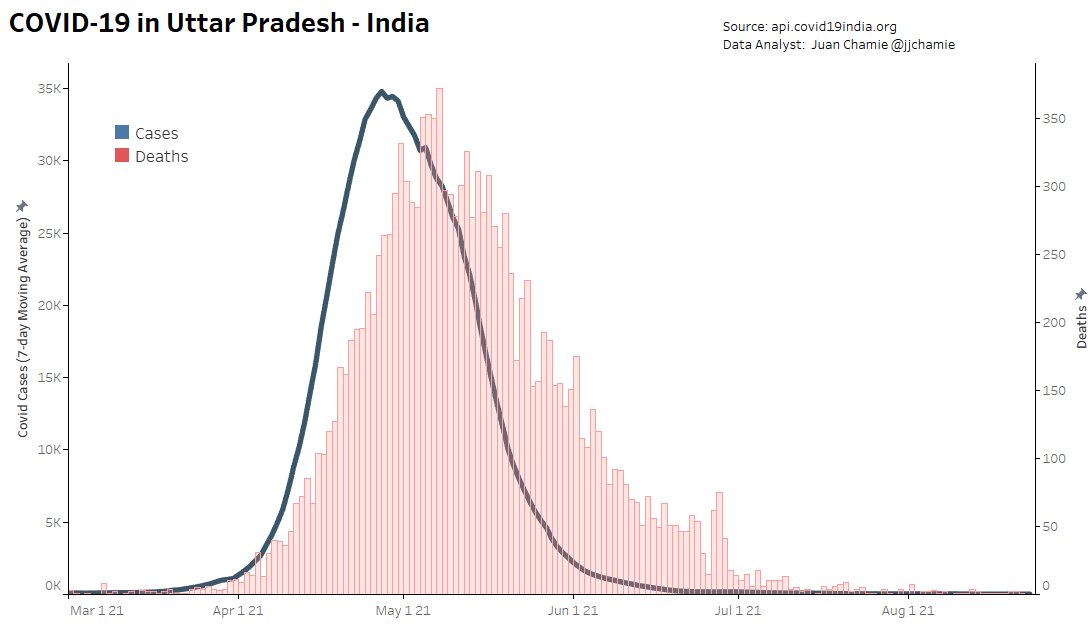
Though the usual caveats apply about numbers being under-reported due to inadequate testing, it’s clear that things have improved across India. Since the country began its last wave of infections, in March, no state has contained the virus as effectively as Uttar Pradesh, India’s most populous region with 230 million inhabitants. If it were a country, UP would be the world’s sixth most populous, sandwiched between Pakistan (5th) and Nigeria (7th). UP has been using IVM longer than any other Indian state, including as a prophylaxis for people who come in contact with the disease. The numbers (both in terms of cases and deaths) speak for themselves. The average number of cases per day over the last seven days was just 28 — in a region with a population larger than Brazil’s! Brazil’s daily average is more than 21,000 cases.
It’s a similar story in New Delhi, where the number of new cases is also close to zero.
Compare that to the state of Kerala, which has stopped prescribing ivermectin and other proven therapeutics and is making exhaustive use of Gilead’s largely ineffective (yet excruciatingly expensive) antiviral, remdesivir. Not only have case numbers barely declined from their mid-May peak but they are rising faster than in any other region. Despite boasting just 3% of India’s population, having one of the most advanced health systems in the country and one of the highest vaccination rates (over 50% of the population has received at least one dose), Kerala accounted for 62% of all of India’s Covid-19 cases in early August. The BBC described the region’s stubbornly high numbers as a “mystery”.
In India, nothing is quite as simple as it might seem, says Jerri-Lynn, who knows a thing or two about the subcontinent, having visited there for long periods:
UP is a large, rural state, with a still largely agrarian economy. It’s part of the northern Indian ‘cow belt’, with low literacy rates, and a distorted sex ratio. It’s the second poorest state in India in terms of per capita income. Kerala is much richer, and has more of a service-based economy; lots of Keralites work in the Gulf states and many send remittances back home. The state has been governed by successive left-wing governments for decades, has high literacy rates, the top female sex ratio in India, and some of its best medical care, particularly on the public health side.
As I mentioned to you before, I believe Kerala recorded the first covid case in India, in a female medical student returning from China — perhaps Wuhan in Jan 2020. The state initially did a good job managing covid and was held up as an exemplar; their contact tracing system was widely praised.
The UP government is notorious for its corruption. Many would take any official UP state figures with large fistfuls of salt. This is not the case for Kerala.
Kerala has by far the highest number of cases in the country while UP has the lowest, but is that because it is testing more and being more honest about the numbers? According to many mainstream reports (including Times of India and India Today), UP is doing more testing than any other state. Can that be true or is UP’s regional government doctoring the numbers? Or is it simply doing a very good job at keeping the virus contained, just like Mexico’s poorest region, Chiapas?
In India’s last brutal wave the turnaround in Uttar Pradesh was so dramatic that even the World Health Organization (WHO) showcased its achievements. In a May 7 article titled “Going the Last Mile to Stop Covid-19” the WHO noted that aggressive population-wide health schemes, including home testing and “medicine kits”, had helped regain control of the virus. The one thing the WHO failed to mention in its on-the-ground reporting is what was in those medicine kits.
The Wonders of Early Treatment
One thing that is that is clear is that many doctors in India try to treat covid-19 as early and as aggressively as possible, whereas many doctors in Europe and North America prescribe nothing more than paracetamol during the first seven days. As I’ve learnt from recent direct experience, this is the equivalent of laying down a red carpet for the virus and telling it to make itself at home and go wherever it wants, do whatever it wants.
“When we started seeing more cases, we decided to take up a door-to-door survey,” Bagalkot District Health Officer Dr Ananth Desai told New India Express in June. “When the health officials noticed people with symptoms during the survey, they tested them immediately and provided them with home isolation kits, which had medicines like Ivermectin, calcium and zinc tablets along with paracetamol. We advised the patients to start with the medication even before their Covid-19 test results came out. With these measures, we noticed that many patients recovered faster. This helped in increasing the recovery rate”.
Besides other factors such as lockdowns, travel restrictions and increased herd immunity, ivermectin has almost certainly played a part in this. But it’s impossible to know just how large a part. The fact that case numbers and deaths have tended to fall precipitously in regions where it is used widely, such as UP, New Delhi, Goa and Bihar, and have tended to remain high in regions where it isn’t, such as Kerala or Tamil Nadu (before it readopted ivermectin in June), does not constitute proof of causation. But when the same thing occurs in so many of the disparate parts of the world where ivermectin is used, a pattern begins to form that strongly supports ivermectin’s efficacy.
That doesn’t mean that it has a perfect record. In Mexico, for example, cases and deaths began surging once again in May, despite the fact that the Institute of Social Security (IMSS), which runs many of the country’s public hospitals, has been using IVM since January, albeit in very low doses. That said, it’s all but impossible to know how many doctors, public and private, are actually using the medicine. In May the newspaper Proceso reported that IMSS had repeatedly clashed with the federal government over its use of ivermectin. In June, the Mayor of Mexico City Claudia Scheinbaum announced that the city’s widespread use of IVM had reduced hospitalisations by up to 76%.
In early August, the results of the first large randomised control trial into IVM use for Covid-19 were released. And they showed “no effect whatsoever” on the trial’s outcome goals — whether patients required extended observation in the emergency room or hospitalization. However, as we noted in a previous article, this was a trial financed by the deeply compromised Gates Foundation, which is heavily invested in the new Covid vaccines, novel treatments and their manufacturers. And the Canadian university that performed the trial, McMaster, is also a major recipient of Gates Foundation funding.
The results of another large RCT trialsinto ivermectin — the so-called PRINCIPLE trial taking place at Oxford University — should also be released in the coming months. Perhaps they will be more flattering.
The case for IVM was also not helped by the discovery of irregularities in a trial conducted in Egypt. That, together with the findings of the Together trial, is now cited by many media outlets as proof positive that ivermectin does not work against covid. To reach that conclusion, they steadfastly ignore the impressive results of many other small trials, the on-the-ground experience of untold thousands of medical practitioners and nurses, and the exceptionally low prevalence of covid in many of the places IVM is being used widely.
Ivermectin Comes Home, to Japan
As the Delta variant has swept through Asia, causing unprecedented devastation, more and more cities, regions and countries are considering authorising the use of ivermectin. They include Tokyo, where Haruo Ozaki, chairman of the city’s Metropolitan Medical Association, has called for ivermectin and the corticosteroid dexamethasone to be used due to the authorities’ failure to distribute vaccines in time. As Lambert pointed out a couple of days ago, Ozaki’s recommendation is for off-label use under “battlefield” conditions:
[OSAKI:] I am aware that there are many papers that suggest ivermectin is effective in the prevention and treatment of corona, mainly in Central and South America and Asia. There is no effective therapeutic drug, although it is necessary to deal with patients who develop it one after another. The vaccine is not in time. At such an imminent time, there is a paper that shows ivermectin is effective for corona, so it is a natural response for clinicians to try using it. Doctor-led clinical practice. That’s why many test papers came out.
On August 13, Ivermectin was added to the Tokyo Metropolitan Medical Association’s home treatment protocol. This is not to say that the whole nation of Japan — whose soil gave birth to the unique and extraordinary microorganism that produces the avermectins (from which ivermectin is derived) — has now embraced ivermectin. Nor is it clear how may doctors in Tokyo are actually using it. But the move could be an important first step, especially if covid-19 cases, hospitalisations and deaths fall.
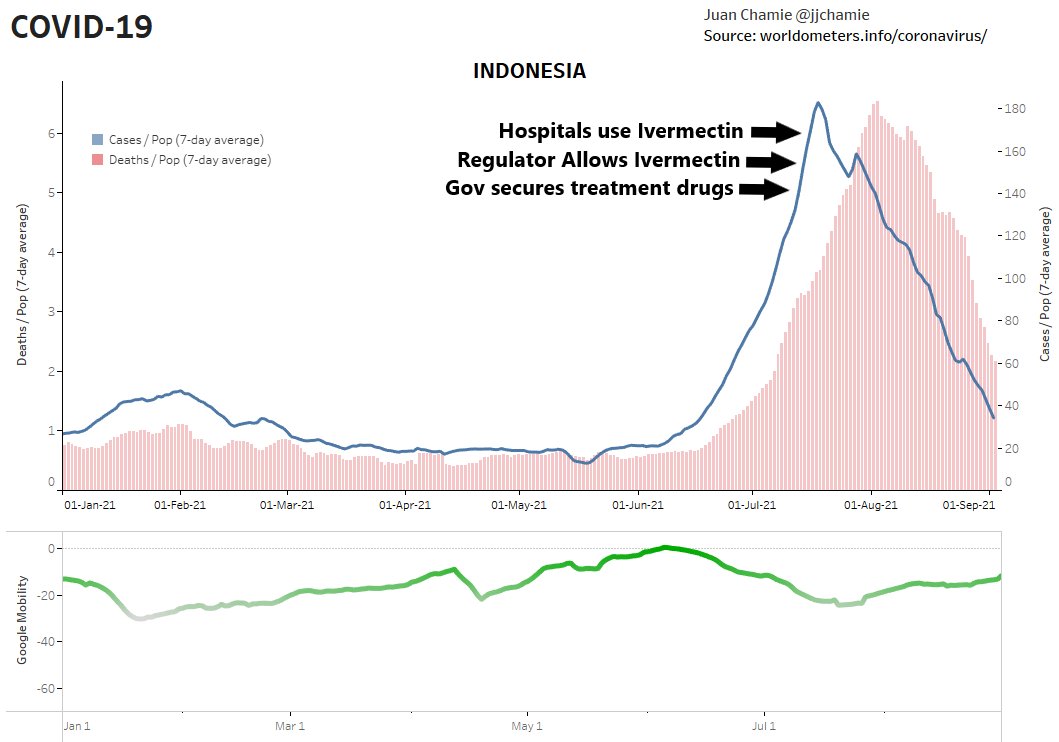
Indonesia has also embraced ivermectin. On July 10, the Indonesian government secured the supply of COVID-19 treatment and created a website showing real time drug availability. Four days later the health regulator authorised the use of ivermectin for Covid-19. Then, on July 22, on July 22 Indonesia’s hospitals began using the drug. By the first week of August cases and deaths were falling.
Meanwhile, Back in the USA…
Pfizer and Merck have announced new trials for their experimental oral antiviral drugs for COVID-19. Merck said in June that the U.S. government has already agreed to pay about $1.2 billion for 1.7 million courses of molnupiravir — working out at $705 per course of treatment — if it is proven to work and is given the green light by regulators. Pfizer, meanwhile, said that if its trial of its “affordable” early treatment pill is successful, it will file for emergency approval between October and December this year.
If the authorisation process is anything like the process employed for Gilead’s Remdesivir, which is included in standard-of-care protocols throughout Europe and the US despite offering next to no real benefits (according to the WHO), and Pfizer’s booster vaccine, Pfizer will be raking in even more money from Covid by the year’s end.
Being able to take an oral antiviral therapeutic for SARS-CoV-2 at home would be a “game changer,” according to Albert Bourla, Pfizer’s CEO.
As I posited in a previous article, one of the main reasons why there has been such fierce opposition to ivermectin is that large pharmaceutical companies are developing their own antiviral therapies that will have to compete directly with ivermectin. Another reason is that if ivermectin were approved as a covid-19 treatment, it could threaten the emergency use authorisation granted to covid-19 vaccines and novel treatments, although the recent approval of Pfizer’s COMIRNATY vaccine may have changed that.
When financial returns are the primary priority in a health care system, this is what you get. Everything is geared to churning out brand new, barely tested experimental medicines as quickly as possible, with scant communication of what potential side effects they may produce. Throw in monopoly control of intellectual property and you have the perfect business model. Whether the new medicines work or not or do more harm than good, they will cost an arm and a leg. And their manufacturers will probably be protected from liability. The patients’ health, well being and welfare are barely an afterthought.


What I find most infuriating and depressing about this whole affair is that we are more than a year past since it was strongly suggested that ivermectin was a potentially useful treatment, and yet we are still left without a single good, high quality study. And we have even less on other low risk compounds such as vitamin D3 or other known immune system boosters. This of course, seems to be deliberate.
Pretty much all the (western) medical power structure has bought into vaccines as the only real game in town. Even normally sane and sensible voices, like Trisha Greenhaulgh, has been repeating the propaganda against Ivermectin. If, as seems very possible, the RNA vaccines prove to be of minimal use, then the loss of public faith in the system will be irreparable for a generation.
This is yet more proof that, as Taleb has pointed out from the very beginning, medical science has a very weak grasp of risk assessment. When you combine this with the malign influence of Big Pharm, we are looking at a scientific (or as Taleb would call it, scientism) failure of historic proportions.
But so many powerful people have dug themselves into their bunker that I doubt the truth will ever emerge. The amount of gaslighting going on, even among the experts, is horrifying.
If, as seems very possible, the RNA vaccines prove to be of minimal use – what exactly are you suggesting here?
Hospitalization rates suggests that though breakthrough infections occur, vaccines greatly reduce the risk of hospitalisation and death including against delta. This includes RNA vaccines. See for example https://t.co/nzyKAF06F4?amp=1.
Are you suggesting the numbers are fraudulent? Or that the analysis is wrong? That there are as-yet unknown long-term side effects? Or what?
According to the CDC definitions of “vaccinated,” which have been changed during the pandemic (you can look them up yourself on archive), someone is not considered “vaccinated” until two weeks after the second dose, which means the following for health care recording: all patients who are tested positive for COVID are NOT recorded as “vaccinated” even if they have had one or more of the vaccines until two weeks after their second dose of the same vaccine. They are considered UNVACCINATED. MEANING: people who only had one dose of any COVID vaccine, people who had one dose of one vaccine and one dose of another, and people who have had both vaccines but two weeks afterward have not passed yet, are considered UNVACCINATED. Furthermore, the CDC changed its PCR policies to use different CT or cycle thresholds for VACCINATED VERSUS UNVACCINATED. The “vaccinated” are to be tested at the proper 25 cycle thresholds rather than higher levels of 35-45 cycle thresholds that yield MOSTLY FALSE POSITIVES. Thus, those who are considered “unvaccinated” because two weeks after vaccine number two has not passed YET, according to CDC testing recommendations, are tested at the higher CT that induce more false positives, along with others who are totally unvaccinated, causing the results to be unequally treated because the testing and labeling protocols are biased. The result is scientific misconduct which will take awhile to uncover and make public, but in the mean time, the information is allowed to be spread, deceiving people into believing false information while the truth is labeled false, reminiscent of the fabricated/fictional Oklahoma Hospital Story that came from one doctor who had not worked in their ER for two months and thus had no basis to claim ivermectin overdoses were rampant OR that others were being denied medical care (UNTRUE).
Sorry if I’m putting words into his mouth, but “minimal use” might refer to the apparently short duration of the vaccines’ effectiveness as seen in the Israel data. Israel started their vaccination program early, bringing their case and death rates down early, but both spiked about six months later.
Are there any ongoing clinical trials for Ivermectin? Have there been any peer-reviewed studies done on its effectiveness? This article is very fuzzy when it comes to actual details.
There are multiple clinical trials abroad for Ivermectin as an anti-HIV med. Most are in advanced stages and Ivermectin is reportedly doing well.
I was actually surprised to learn the above because generally speaking, there is no money whatsoever for clinical trials (expensive!) for an old, cheap, off patent drug. The economics don’t support it.
Similarly, there are doctors to have claimed great success using tetracycline, an old, off patent, cheap, very well tolerated antibiotic as a treatment for autoimmune diseases. The claim that they are “autoimmune” diseases was invented from whole cloth after WWII when symptom-suppressive drugs were developed. The older pre-WWII research path was that these ailments were produced by a pathogen, and one class under investigation was mycoplasma (which aside from three pulmonary mycoplasma that HIV positive patients might get, are never tested for in clinical labs). There’s only “experimental” evidence supporting this treatment protocol. There’s no way anyone will fund clinical trials.
I see you didn’t post my more expansive comment, perhaps it was too heated. My apologies. The point was, if TPTB are going to make an argument against the drug, their argument needs to be based on legitimate grounds, not easily demonstrable falsehoods. Y’all do great work.
Here is a report of a clinical trial by McMaster University, Hamilton, Ontario. They found that the cheap, easily available generic antidepressant fluvoxamine was effective against Covid-19. Ivermectin was not effective. Fluvoxamine costs about $4 for the 10 day course of treatment.
https://brighterworld.mcmaster.ca/articles/antidepressant-fluvoxamine-can-save-covid-19-patients-mcmaster-led-research-shows/
This isn’t even a study. It’s a press release of a not-peer-reviewed study. And they have no basis for commenting on other treatments since they did not evaluate them. One needs to see the study population and the methods section at a bare minimum to evaluate their claims. There is nothing of the kind here, which raises red flags.
I swear, I often learn more from reading comments of these articles (and from reading these articles, of course) than I do from staying abreast of reporting in the mainstream media.
And my thanks to the candidate, Prisoner (“voteforno6”) for posing an insightful question.
There’s this one: https://clinicaltrials.gov/ct2/show/study/NCT04885530?term=repurposed+drugs&cntry=US&draw=2
Apparently Oxford university started a non-laboratory trail and were asking for volunteers back in june. Ivermectin is on the list of possible cures. There are other drugs also being tested. Ivermectin is the one that is hyped more than the others.
Here’s an interesting thread (bit of a rant) from Kory about peer review, major journal publishing, and mentions a DB, RCT by Prof. Eli Schwartz in Israel:
https://threadreaderapp.com/thread/1434741303527579648.html
My take on peer reviewed studies is that these drug companies will find the right peers to agree with pushing whatever drug they desire. And they’ll find the right peers to conclude that “not invented here” drugs to be ineffective. It did not used to be that way.
Check TrialSiteNews. They have the studies done abroad.
There is: https://c19ivermectin.com/
Database of all Ivermectin COVID-19 studies. 113 studies, 73 peer reviewed, 63 with results comparing treatment and control groups. Can search by for Early Treatment, Late Treatment, Prophylaxis, All
> There is: https://c19ivermectin.com/ Database of all Ivermectin COVID-19 studies. 113 studies, 73 peer reviewed, 63 with results comparing treatment and control groups. Can search by for Early Treatment, Late Treatment, Prophylaxis, All
I believe that https://ivmmeta.com/ is superior because it allows you to search by type of trial, e.g. RCT.
There are links to some ongoing trials here: https://www.nature.com/articles/d41586-021-02081-w
I wonder if anyone has seen today’s Substack article by Scott Alexander? He actually went to the trouble of reading the original stories about the Sequoyah incident and had discovered it’s all a lot more complicated than either side is prepared to acknowledge. There are a lot of comments – I haven’t had time to read them yet. As a total non-expert, I’d be interested in what others think.
I am not sure it’s all that complicated. Here’s a link to Maddow who I assume*, as so often, ignited the whole moral panic:
https://twitter.com/ggreenwald/status/1434853272389627906?s=21
Oddly, the Substack article doesn’t mention Maddow, who tied up the whole bad package and put a bow on it.
Anyhow, this isn’t especially on point…
* Caveat that I haven’t done a timeline
Timeline thread:
https://twitter.com/ddale8/status/1434991544306704395
tl/dr: “…1) bad initial local story to 2) unquestioning national aggregation and tweets and then to 3) too-quick denunciations of the doctor whose comments had been poorly contextualized…”
https://twitter.com/ddale8/status/1435229646644187139
This article is certainly useful in illustrating its key point: the power of confirmation bias on *all* sides. Well worth reading in that regard. Yet it starts off this way:
“In case you find this hard to follow: ivermectin is an antiparasitic drug that looked promising against COVID in early studies. Later it started looking less promising, and investigators found that a major supporting study was fraudulent. But by this point it had gotten popular among conspiracy theorists as a suppressed coronavirus cure that They Don’t Want You To Know.”
Is the opening statement true? That is, did it “later” start to look *less* promising? By what criteria? Or whose? That is indeed a crucial question, yet the author seems to think it is settled. This statement itself frames the rest of his discussion.
Granted that in the next paragraph he says this:
“The media has tried to spread the word that the scientific consensus remains skeptical. In the process, they *may* have gone a little overboard and portrayed it as the world’s deadliest toxin that will definitely kill you and it will all somehow be Donald Trump’s fault. It turned into the latest culture war issue…”
This, most of us would agree, is certainly a factual statement, and is the main point of the article (with confirmation bias on all sides at each phase of the story). Again, that is a useful lesson, but nevertheless the possibility that ivermectin may in fact be useful in the treatment of COVID has been rejected. Instead, we get yet another WWF-style clown show.
So… can we “trust the science” or not? The author implies that we can, and that “the science” is skeptical that ivermectin is useful. Is *that* a biased position? Or a “rational” one?
Within the mainstream media context Daniel Dale is usually pretty even-handed as a fact-checker. I just posted the links as a timeline, not an endorsement of any point of view on the substance. Sorry if that wasn’t clear.
I thought your links were quite relevant. Full information should always be welcomed in my view. As I stated above, I also thought Alexander’s observations on confirmation bias were useful — we *all* need to guard against this universal tendency. Nevertheless, it seems ironic to me that Alexander begins his discussion of such bias with an apparent statement of fact which itself could be perceived as biased. Is it? Trying to find out has been very frustrating.
Hi pjay, if I have your attention, I just want to thank you for pushing back on my neutrally given links to the first ivm-critical post on the evidence based medicine blog several months ago. Since then (and having read other things) I no longer trust Gorski or his judgement so readily. I still don’t know if or how much Ivermectin works but man, I hope it does.
In terms of the poisonings, I don’t see anything about the doses they were taking which could have been huge, and cases probably means cases involving it, which may well involve other drugs too. At any rate, no reported deaths, and 1% ‘major effect’.
The poisonings are due to people being too stupid to figure out how to dose themselves correctly, not because it is a veterinary product.
The Rolling Stone story has been debunked by the hospital. No ivermectin OD’s. No space problems. No truth at all.
The poisonings in the pie chart in Scott Alexander’s Substack article – about halfway through the article itself.
One of the oddities of this story is no one did any fact checking, not even Alexander. There are three hospitals in the area of sequoyah hospital, 13 altogether in Sallisaw. Not an overwhelming amount of research.
So the Rolling Stone story was false but not in the way the rightwingers said it was false and therefore gotcha?
I’d say this exercise in on the other handism is fairly lame.
the piece on substack strikes me less as other side-ism and more just a guy trying to make sense of things, which any of us can relate to surely. He might have the thin end of the wedge but I don’t think he’s writing in bad faith.
I mean, the truth matters doesn’t it? Or not.
The Rolling Stone story has been debunked by the hospital. No ivermectin OD’s. No space problems. No truth at all. Now outright lies.
The thing is, focussing on the media dynamic at this small scale misses the bigger point to be made, I think.
You don’t need to be a reader of the grauniad or a viewer of Joe Rogan or Alex Jones to do some basic searches on ivermectin, and a tiny bit of lead-following will turn up ivmmeta.com
And after a few minutes on that site, two things will become apparent to just about anyone: either this is the most audacious, far-reaching attempted conspiracy to commit medical fraud in history, or; those closing rank and claiming that there is “no evidence at all” that ivermectin has an effect on Covid-19 are engaged in a counter-conspiracy.
Either way, it’s a story. A big story. A potentially great story.
And it throws up all kinds of interesting questions, including the limitations of the study-industrial-complex broadly, regardless of what side of the ivm question you fall on. The Elgazzar incident is fascinating in itself (and let’s not mince words; the study was fraudulent. But why? Who would do this? Why wasn’t it caught sooner?). A few days ago someone shared the editorial (BMJ? Lancet?) article that suggested we should perhaps assume medical data was fraudulent unless proven otherwise.
And people are desperate for answers. They would devour any such story. Any journalist worthy of the name would jump at the opportunity to dig deeper into this.
I don’t think we’re going to see any such reporting, and maybe that’s the real issue, in a sense.
On conspiracy, see my response at “Procrustean bed.”
I suppose this is whataboutism, but it’s odd that the people yammering about the poor quality of ivermectin studies don’t comment on the replication crisis in the mainstream, or scientific fraud generally. It’s as if ivermectin is dirty and everything else is clean. That’s a taboo in operation, and nothing scientific at all.
Obligatory note that I am pro-vax, vaccinated, and strongly support the repurposing of existing drugs as a matter of “defense in depth.”
I tuned in KGO radio yesterday to catch the fire news and they had an interview with a Doctor from UC Davis on regarding Ivermectin.
The interviewer led off with a question about how deadly Ivermectin was and the Doctor responded at first by saying the problem was people taking veterinary formulations and overdosing.
That didn’t go over well from the tone the interviewer took, she asked about physicians who prescribed it in a tone of disbelief “Are doctors really prescribing it?” and the physician seemed to pick up on that right away and said “Some fringe doctors are, with mixed results” at which point I turned off the radio..
So IVM only works in some geographical locations, for poor people and people with brown skins…
We are about to see a huge surge in cases in the USA if the pics of college football games is any indication and the streisand effect is real.
Will a slew of dead and crippled children in the USA make a difference?
No.
A recently (Sept 7) updated meta analysis: https://ivmmeta.com/
•Meta analysis using the most serious outcome reported shows 69% [54‑79%] and 86% [75‑92%] improvement for early treatment and prophylaxis, with similar results after exclusion based sensitivity analysis and restriction to peer-reviewed studies or Randomized Controlled Trials.
•Statistically significant improvements are seen for mortality, hospitalization, recovery, cases, and viral clearance. 29 studies show statistically significant improvements in isolation.
I haven’t read it, only skimmed through quickly – it’s long and detailed, and I’m no statistician – thanks to Brian Westva in yesterday’s Links!
Meta-analysis should exclude the Carvallo study, there seem to be major inconsistencies/issues with it.
Thank you, TBellT.
I knew the Egyptian paper was dodgy to put it mildly; looks like that one’s just as bad.
I think I’ll stick to pointing out it’s a very safe drug as drugs go, with known antiviral effects, and there’s a large trial underway. I’ll let the likes of Dr Day make claims for its effects on COVID.
(I would have replied sooner, but we’ve been without electricity most of the day!)
I’d suggest you read this thread, and the linked articles, before putting too much stock into ivmmeta.com.
https://threadreaderapp.com/thread/1422044335076306947.html
I’m an RN, working in the ER for over 15 years. I fully agree that there are significant reasons for all the power players in the health care industry to shade the truth – there’s so much money to be made that it would be inconceivable that there be no perverse incentives.
However, the incentives are huge on the side of those muddying the waters as well, and I think this get missed – the players are much smaller, and their megaphones are correspondingly small. It’s easy to miss that the financial incentives are shared among a much smaller pool of potential recipients, or that sowing discord or confusion can be it’s own reward.
Anyway, I’d recommend a look.
Cheers.
Flea RN, can you expand on this? What exactly would be the financial incentives of those who promote Ivermectin?
I can’t speak for Flea, RN but it’s not hard to imagine really. That is to say, Ivermectin may not make much money for its original patent holder anymore, but it doesn’t come out of the clear blue sky either. All this talk about Big Pharma with no consideration for Small or Medium Pharma. Manufacture, logistics and distribution, etc. – I think it’s blithe to suggest that nobody could stand to gain in pecuniary terms from the potential success of Ivermectin.
I don’t know if that’s what’s going on here. See my
comment above (in moderation atm): either [based on ivmmeta] this is the most audacious, far-reaching attempted conspiracy to commit medical fraud in history, or; those closing rank and claiming that there is “no evidence at all” that ivermectin has an effect on Covid-19 are engaged in a counter-conspiracy.
> a counter-conspiracy
“Conspiracy” is a bit of a Procrustean bed. I don’t think, for example, that it would be useful to frame what happened to Semmelweis as a conspiracy. Professional and institutional incentives, commitment to existing paradigms, and even personal factors or class hatred can all combine to cause the appearance of a conspiracy to emerge.
Yes, I agree, I didn’t mean ‘conspiracy’ in the full-blown CT sense of the word, just wasn’t really sure of a better word to use. Conflagration?
And of course, I don’t really think that if such a story was written that it would necessarily come down conclusively in favour one ‘side’ of that argument of the other; everything is complicated. Reporting is difficult.
But as I say above, the story, whatever it may be, raises all kinds of interesting side-questions, and warrants scratching beneath the surface. There is much worthy reporting to be done on this topic. People are yearning for the best information possible. But we don’t get that. Instead we get the most arrant, vapid nonsense imaginable.
> I didn’t mean ‘conspiracy’ in the full-blown CT sense of the word, just wasn’t really sure of a better word to use. Conflagration?
Perhaps “confluence of interests” (wordy) or faction (too structured). Janine Wedel would I think say “Flexnet” but I’m not sure. I’m not sure what the word would be for a dynamic and temporary subgraph of a Flexnet.
We do need a word. Class interest operates through these things, whatever they are.
We need some good German speakers. They always have a word for anything useful.
Indeed: ‘Interessengemeinschaft’ – community with shared interests. A quite common and selfexplanatory word.
We do need a word. Class interest operates through these things, whatever they are.
Absolutely!
Interessengemeinschaft may be correct, but it’s even longer than confluence of interests, as well as being less than self-explanatory for non-German readers and speakers.
Yes, simply the URL should raise alarms (someone has registered it as a platform – who?)
I suggest looking at the studies themselves instead. The meta analysis studies were linked here at NC not that long ago, and the papers that are quoted on the anti-Ivermectin side are available as well. I read the Lancet study in the latter category and found it quite interesting. They didn’t find evidence to support the hypothesis they were looking for (reduction in viral load after a single dose) but it was very specific and only tested one possible action mechanism. They did not seem to have any hypothesis around symptom reduction (which is the main claimed benefit). They nonetheless saw an effect in that area that was significant enough for them to mention. They finished by noting that although the viral load reduction hypothesis wasn’t supported by the evidence, there did seem to be signs of some clear benefits, and that ivermectin could well have a role in Covid treatment in future and merited further study.
Somehow when this was all fed into the media megaphone, we ended up with the idea that the study had definitively debunked the idea of ivermectin as a Covid treatment and should be considered the final word on the matter. If you read the abstract, neither of those two things is even a little bit true.
Pardon my ignorance, if you ever see this, but why should the URL raise alarms? I’m used to treating some, such as .io, as dodgy until proven otherwise, but any website needs some sort of effort to get it online – why would registering as a platform (I’m using your words, not knowing the right terminology) be cause for extra suspicion?
The problem is when he says “current best evidence is consistent with harm”. Huh? That’s a very bold claim that he asserts with a handwave, and would mean that innumerable doctors around the world, including IM Doc, are engaging in something like medical malpractice. Ivermectin has been used clinically to treat Covid all over the world for over a year now. If there are any covid-specific contra-indications that overturn the drug’s superb 40 year safety record, I’d like to know what they are.
Thank you, Flea, RN.
I thought that site looked a bit odd, and some of its headline numbers seemed too good to be true, though I hadn’t read enough to know what exactly they were referring to. Looks like they were referring to just what you’d expect!
Suffice to say I won’t be posting links to it in future.
(I would have replied sooner, but we’ve been without electricity most of the day!)
I had intended to reply to Ignacio but something went haywire. Anyhow, I hope folks will take a look at that site. I don’t know who has put in all of the work but I think it is important. It is a useful site to refer skeptics to. You can look into the details of the studies as well.
•Meta analysis using the most serious outcome reported shows 69% [54‑79%] and 86% [75‑92%] improvement for early treatment and prophylaxis, with similar results after exclusion based sensitivity analysis and restriction to peer-reviewed studies or Randomized Controlled Trials.
•Statistically significant improvements are seen for mortality, hospitalization, recovery, cases, and viral clearance. 29 studies show statistically significant improvements in isolation.
Studies Prophylaxis Early treatment Late treatment Patients Authors
All studies 63 86% [75‑92%] 69% [54‑79%] 40% [24‑52%] 26,422 613
Peer-reviewed 44 86% [73‑92%] 70% [52‑81%] 43% [21‑59%] 17,082 479
Randomized Controlled Trials 31 84% [25‑96%] 64% [48‑74%] 30% [2‑50%] 6,561 359
Percentage improvement with ivermectin treatment
Admitting some really safe, and inexpensive treatments like Invermectin have great value would diminish fear and slam the brakes on expensive treatments. I do not know this hypothesis to be true, but if there ever is a strong perception that the most influential members of the American medical community plus much of the media has decided that allowing Americans to suffer and die because otherwise it just opens a can of worms regarding activities in 2020, well, what will be found? Under such a hypothesis, “leaders” may be shocked that it is September 2021 and they still can’t move out of the trenches they dug even while all kinds of counties concern themselves with treating the sick effectively.
Perhaps it’s an example of the phenomenon described in a quote attributed to Churchill:
“the Americans always do the right thing, after exhausting every alternative.”
Ivermectin may eventually become a standard anti-COVID therapy in US, but it seems a good bet that this may not happen until after the current $$$ drugs in development have themselves gone off patent.
Many of us will not last that long.
If only the government had a department that focused on health or could fund the research to determine whether or not ivm was effective at treating 19.
Looks like they spend 41b annually to do just that. Who knew?
https://www.nih.gov/about-nih/what-we-do/
In his December 2020 congressional testimony, Dr. Kory begged the NIH to review the IVM data that he and his colleagues had gathered.
The video was deleted by YouTube, but can still be found on the FLCCC website.
Searching the NIH website for Ivermectin finds some interesting results, most of which seem positive:
https://pubmed.ncbi.nlm.nih.gov/33278625/
From the Alexander Substack article:
“I mean, that’s also a pretty cool story, isn’t it? Right-wing news outlets accuse the so-called “liberal media” of bias, then get hoist on their own petard? Seems a bit too cute.”
Alexander cites “right wing news outlets” forgetting that this forms basically the entire current career of Greenwald & Taibbi, who are supposedly above reproach. As the linked Tweet shows, they get to dunk on Rachel Maddow, and that’s all that really matters to these “journalists”.
This is why I don’t trust those guys any more. I’m no fan of Alexander on a lot of things, but this is what I would be expecting from Taibbi/Greenwald if they really honest brokers like people here seem to think they are. They are just as biased as the people the constantly criticize.
The evidence seems to show that: 1.) The so-called “refutation” was by a totally unrelated hospital that never employed the doctor in question; 2.) There is an overcrowding problem in Oklahoma; 3.) It has nothing to do with Ivermectin overdoes; and 4.) Overdoses are going up, but are still basically insignificant. Plenty of blame to go around here, as there is with most issues. It just doesn’t fit into the favored narratives of “stupid Trump supporters” or “evil Democrats censoring everything”.
No, but it DOES fit into the fact that neither the RS journalist nor Maddow actually conducted themselves as journalists and VERIFIED any facts at all — never bothered, for instance, to confirm the doctor’s original statement. He now claims to have been misquoted by the OK TV reporter, though that may well be a self-serving claim, and surely the TV reporter should have — though I’d bet my house does not — contemporaneous notes. Nor did these journalists ever bother to actually call any hospital in OK to find out what was going on.
Basically, they played “Telephone,” and just as in that game, whatever was originally claimed ended up, at the end of the chain, vastly distorted. That’s NOT journalism.
I find it kinda strange that the event allegedly occurred in only one hospital, as from what I can tell there are quite a lot of people out there taking horse de-wormer & the human version in many different places & therefore if it was as bad as we are being told – would it not be logical to assume that there would be many more similar reports ?
If I were an editor, the part of the story where gunshot victims had to wait at a rural hospital would have totally set off my bs detector. From my experience growing up in a rural area, gunshot victims are few and far between. Maybe one per week in a small city, and one per month or longer in a truly rural area (maybe all during hunting season)
FWIW, the picture that ran with the story, the one that showed the gunshot victims patiently standing in line outside the ER, wearing winter coats on a late August day in OK, would have set off my bs detector as well.
A minor citation quibble.
When I see something attributed to “Nature“, I think of the flagship journal Nature itself.
The 2017 article linked by the author is at the nature.com site, but the name of the journal in which it was published is Journal of Antibiotics, which I think is based in Japan.
JA is under the Nature corporate structure (the journal cover says “Springer Nature”, but it is not as prestigious as the flagship journal Nature itself.
—-
A friend is getting some grief from a physician about her interest in ivermectin. The physician apparently is unaware that this drug has human uses. I’m afraid that the media campaign is working.
Here’s safety quote from a 2011 article
https://www.ncbi.nlm.nih.gov/pmc/articles/PMC3043740/
by the same author, Andy Crump, coauthored with Satoshi Omura, who 4 years later won the Nobel for this discovery
“Ivermectin has continually proved to be astonishingly safe for human use. Indeed, it is such a safe drug, with minimal side effects, that it can be administered by non-medical staff and even illiterate individuals in remote rural communities, provided that they have had some very basic, appropriate training. ”
I hope that it is an unrealistic and paranoid thought that perhaps the Pub Med research literature database might at some point be scrubbed to erase visible evidence of the stupidity of this present anti-IVM narrative. A really safe off-patent drug that can be administered by people with basic training — where is the (corporate) profit in that?
I decided this morning to become a full conspiracy theorist. I’m sorry but the total hysteria over IVM at this point has to be prodded by the medical industrial blob or something. The two times I mentioned it either to friends or colleagues, I got shot down as an anti-vaxxer and I didn’t mention the vaccine at all.
If you try to talk about IVM in an even-handed manner, so many labels and assumptions are thrown on you and the conversation is forcefully steered to ‘take the vaccine’. It is creeping me out.
This was done by our medical establishment. They framed the conversation and poured gasoline over the topic.
It’s taking a front-line drug off the table for no reason. If the conspiracy proves true in the next three months, the damage in trust in medical science will be substantial. Then of course so many liberal news outlets will be culpable in this, circling the wagons around the corrupt drug companies.
The final most scary scenario is from PlutoniumKun, that our society can no longer look back in hindsight and learn from this. Just more polarization.
> It’s taking a front-line drug off the table for no reason
Yes. Here is the WHO 2019 (the latest version) list of essential medicines:
https://www.who.int/publications/i/item/9789241210300
Ivermectin is referenced 70 times in this document. “carbapenem ” (include the terminal blank to avoid hits on “carbapenemase”), an example of a class of essential and widely used antibiotics, is referenced 22 times. The class “carbapenems” is referenced 8 times. Imipenem is referenced 17 times. Meropenem 61 times.
Another important antibiotic, colistin, is referenced 11 times.
WHO really likes ivermectin for human uses.
It’s astonishing that there is not more public awareness of the importance of this drug in human medicine.
It’s hard to prefer “ignorance” or “stupidity” to “malice” in one’s interpretation of this.
—–
I’ve read that the early human applications of ivermectin were for tropical parasite diseases, and the countries where these were endemic were too poor for there to be profit potential. The developer, Merck, gave the medicine away at no cost, in what could be regarded to be an heroic act of corporate charity, but which perhaps was also a recognition that the only (corporate) “profit” to be had from the then-known applications of this drug was in terms of “public relations”.
Somehow, I think that they aren’t going to make that “mistake” this time.
Color me cynical.
We need a large not-for-profit pharmaceutical producer.
I am reading “Empire of Pain” by Patrick Radden Keefe. The history of the Sackler family is key to understanding how PhRMA overshadows governmental agencies.
Chapter 3 is “Med Men.” Keefe points out that before WW II, life saving meds like penicillin weren’t patented. Meds were cheap, though limited.
All that started to change as the enterprising Arthur Sackler initially worked for, then took ownership of, William Douglas McAdams Inc., a niche advertising firm that targeted sale of the burgeoning new “ethical drugs” to doctors. The advertising firm employed an army of detail men to doctors’ offices and plied them with direct mail for promotion and brand differentiation that came about in the 1950’s. That escalated to gifts, dinners and speaking fees.
Pfizer was one of their first big clients, where the ad agency (not the drug company) coined the term “broad spectrum” antibiotic in their marketing of terramycin. Subsequent to that success, Sackler’s ad agency was responsible for another newer antibiotic, Sigmamycin that Pfizer developed. Their ads had ringing endorsements by physicians. Problem was that this was fraudulent. These doctors never existed.
Around that time, Sackler ensnared an FDA official, Henry Welch, who helped grease wheels there and promote meds in speeches. Welch got a cut of the biweekly newspaper, the Medical Tribune (which the advertising firm bought large numbers of). $300,000 was a significant bribe in those days. Sackler’s power of influence also extended to the AMA.
You can read some of this at the New Yorker, where Keefe has written about the Sacklers and more here:
https://www.soulask.com/the-history-of-the-clan-who-addicted-the-united-states-to-drugs/
The Medical Advertising Hall of Fame honored Arthur Sackler posthumously in 1997.
We now recognize and abhor the Sackler family’s role in addicting people to first tranquilizers/sedatives (librium and valium), then opioids. The Sackler’s influence was far more invasive. Pharmaceutical lies and propaganda, data mining (IMS Health) and influence peddling that ran the gamut from physician/patient to regulatory capture of agencies–including the FDA and DOJ. All the brainchild of Arthur Sackler.
Ju$t tru$t the FDA?
look, I don’t know about the Sackler article, but looking around on the website you link to, I find a “serious” article titled:
“We’re not from here”: Is the Earth a prison planet and the Moon a station for overseers?
So… Not a place I would look to for information.
Not kidding. Most corporate news copy has its origins as PR for pharmaceuticals, weapons contractors, and investment banks.
I think they only need to hold out until pfizer comes out with a ‘safe’ (i.e. patentable) form of IVM.
Perhaps Ivermectin could be added to one of the expensive new drug formulations as an “inactive ingredient”.
This is what happens when govt. gets in the way.
https://www.yahoo.com/news/judge-says-hospital-cannot-forced-001100148.html
At web site tae the Dr. has great info
This is really bad news and I’ll order some more real soon
Looking on ebay and amazon I’m already seeing price gouging and scarcity of the veterinary product.
Buckerfields, the Canadian farm supply company, has taken it off the shelves here in BC, because people have been grabbing everything they put out. The are limiting supply to people who have aniimals that normally use it.
I can hear the phone calls now, “Hello Vet clinic, can I get permission to buy some of this IVM stuff? What do you mean why? Don’t you think I’m sounding a little ho(a)rse? What do you mean neigh?”
Thank you so much for this in depth discussion. If only the New York Times could be as good as NC!
As for Ivermectin, since it seems to be quite safe there seems to be no motive to be so vehemently against it–no motive other than money that is.
And also power. If the great unwashed start thinking for themselves then who knows what they will do next?
As to the motive to be so so determined to demonize Ivermectin, I have to wonder if it has anything to do with all of the different diseases that Ivermectin has shown promise in treating, including cancer, alcoholism, obesity and others as described in this quote from our article here:
I’ll add this I hope.
https://www.theautomaticearth.com/2021/09/otc-covid-rxs-azelastin-to-zinc/
A number of people I know can not afford to believe that the vaccines might not be a silver bullet or that the Blob’s demonization of IVM is untrue.
This reaction is identical to the families I knew who lost a son in the Vietnam war, they could not afford to believe that the war was unjust and based on a lie because it would destroy their world view.
And yes, these are very well educated people, admitting that the system that has rewarded them very well cares not a whit about their lives or the lives of their children is simply too painful to accept.
A counterhypothesis: perhaps this is another, and even larger “Noble Lie.”
If Ivermectin has only one mechanism of action (MoV) against the the virus SARS-Cov-2 (that is, one directly antiviral MoA, as opposed to not-directly-antiviral mechanisms of treating or palliating COVID disease, which might include things like anti-inflammation), then it is conceivable that widespread distribution of the drug for prophylaxis or single-antiviral-agent therapy could actually promote the emergence of strains of the virus that are resistant to it.
The virus is highly mutable and is already widespread; the risks of selecting for resistance are correspondingly larger than at the beginnings of the pandemic, when there were many fewer people infected.
It might be that it would be better to not widely treat with IVM until there are other antiviral agents available that have different MoAs, with which IVM could be applied in combination therapy in order to reduce the likelihood of selecting for IVM resistance.
(Conceivably IVM itself has multiple independent anti-viral MoAs — I’ve read that it is thought to interfere both with spike function and with viral replication inside host cells, which would greatly ease the worries about selecting resistant strains. Even then, it would be safer to have additional independent targets attacked via combination therapy.)
It might be that IVM is such a useful agent that we mustn’t employ it in ways that would entail significant risk of reducing its usefulness — an annoying and sobering wrinkle in the precautionary principle.
On that theory, the current narrative is a “Noble Lie” designed to protect the future utility of IVM in a world of endemic SARS-ncov-2. Medical establishment discussion of banning use of the drug could, in principle, be intended to prevent loss of future utility of the drug through present use as a single agent that quickly becomes less useful through selection for resistance in the target pathogen.
(I’ll note in passing that the original “Noble Lie”, about the utility of masking, was intended to protect the medical system. Perhaps something like this is happening again.)
It’s a crazy hypothesis, but at this point, truth is at times looking stranger than fiction and it’s hard to know what possibilities are too far out.
We would expect to see this emerge in Africa and other countries where the drug is widely prescribed already. Instead, there seems to be lower covid incidence. I think a major argument against your hypothesis is that is requires the ‘Narrative Elite’ to be both wise and beneficent. It makes a better religious belief than a conspiracy theory, IMHO.
The idea that there could be something “noble” about the establishment attacks on the use of Ivermectin as a COVID treatment seems like quite a stretch.
except that we know it has multiple possible mechanisms of action and antiviral is likely the least important
and i remain agnostic on it. we will never know if it works for covid 19 now. What independent body will fund a good, fair RCT o[n a multipronged approach to treatment?
From the i-MASK protocol*:
The notes go on to say:
This review of the i-MASK protocol shows that there are more strategies for prophylaxis than just Ivermectin. Perhaps in a situation where Ivermectin is so controversial, we can look at something that people can do that may protect themselves and others without being called farm animals. What do you think? Could something so simple be worth a try?
*This information is from the notes on the i-MASK protocol which can be found at the FL
CCC website under the “protocols for covid 19” by following the link in the Box with the following text: “The complete guide for the care of the covid-19 patient”
Here are some the studies they are referring to:
“Effect of 1% Povidone Iodine Mouthwash/Gargle, Nasal and Eye Drop in COVID-19 patient” https://www.bioresearchcommunications.com/index.php/brc/article/view/176
and “Rapid initiation of nasal saline irrigation: hospitalizations in COVID-19 patients randomized to alkalinization or povidone-iodine compared to a national dataset”
https://www.medrxiv.org/content/10.1101/2021.08.16.21262044v1
Those are all interesting ideas. I’m now seeing the FLCCC being attacked on twitter as the bad guys…
Twitter- the final word on science, woke culture and who had the best pictures of dessert today.
https://www.bbc.com/mediacentre/2020/trusted-news-initiative-vaccine-disinformation
Published 10 December 2020
Trusted News Initiative (TNI) to combat spread of harmful vaccine disinformation and announces major research project
At a recent summit chaired by the BBC’s new Director General, Tim Davie, the Trusted News Initiative (TNI) agreed to focus on combatting the spread of harmful vaccine disinformation.
What, exactly, is the TNI doing to combat “the spread of harmful vaccine disinformation”?
They lost me at facebook, google, and the WaPo.
Heh, I couldn’t get past AP.
Here’s a link to a statement from Merck on their current stance for it’s use on Covid 19.
https://www.merck.com/news/merck-statement-on-ivermectin-use-during-the-covid-19-pandemic/
It’s going to need more time prior to approvals as also shown by the Merck link in the article. If it works great. If it doesn’t work then people shouldn’t be self dosing or taking the animal version. Merck is in the business of money, so it’s not going to turn down a revenue stream.
Both the fevered pitch and glaring bias of authors like the one posted is part of the problem. We’ve seen this script play out over and over again with new wonder drug X to deal with Covid prior to having the data to back it up.
Articles like the one above are the whole reason people are self dosing with the animal version in the first place.
The media circus combined with the staggering cost of health care in this country is why people are self-medicating with veterinary drugs, not articles like this one pushing back against said circus. I’d rather get a human prescription. I probably won’t be able to, because my PCP hasn’t heard of the uses in India, Indonesia and Japan, but I’m sure she’s heard the howling from the blob about HoRsE pAsTe. There are plenty of people who don’t have access to a PCP at all, and already self-medicate with veterinary drugs – this is not a new phenomenon.
Perhaps mention to your PCP that a Nobel prize in (human) medicine was awarded to Satoshi Omura in 2015, for his discovery of the bacterial molecule that led to the development of Ivermectin.
Here’s the Nobel press release from 2015
https://www.nobelprize.org/prizes/medicine/2015/press-release/
Avermectin was developed into Ivermectin, used widely first in animals and then, from the late ’80s, in humans.
Fish antibiotics have a been a hot commodity for years due to the cost of health care as you state.
This is not a new phenomenon.
Any evidence that people actually are self dosing with veterinary drug?
And if there is then the obvious solution is to allow doctors to prescribe the human version at the correct dose, not to ban a safe drug (the human version).
The veterinary angle is a self licking ice cream cone. The media tell people not to do something that they never thought of doing until the media told them about it.
Sorry, but a bigger reason that people are self dosing with the veterinary version of “The Drug That Cannot Be Named” is that getting a physician’s prescription for it to use against Covid-19 is well nigh impossible now. When one cannot aford the expensive ‘experimental’ treatments, one needs must falls back on affordable, non standard treatments.
I will make the analogy between the “Drug That Cannot Be Named” and abortion. Under a ‘suppressive’ regime, the wealthy can afford to travel and or bribe their way to the “treatment.” The poor are left to their own devices; often coat hangers and toxic tinctures. The analogy is not exact, because at least the veterinary formulation of “The Drug That Cannot Be Named” does not have to be dangerously toxic if properly dealt with.
“Merck is in the business of money, so it’s not going to turn down a revenue stream.”
Merck doesn’t make any money with Ivermectin, it’s a generic now.
As far as I can tell as a pharmacist in Canada it’s extraordinarily difficult to obtain Stromectol. This has been the case since way before IVM became newsworthy. I was looking for a patient who was convinced she had some rare form of scabies, and it was back ordered and hard to obtain in early 2020.
The hospital can get it but they have different supply chains.
You do realize that Merck is in active tests in Australia, and has had the government purchase thousand of doses presumably to test them of their new oral covid drug. I’m sure you hadn’t missed that Merck has been seriously pursuing a different treatment, one they would have the patent for, not Ivermectin where generic versions can be legally produced.
Meanwhile they have been doing little or nothing to have the cheap drug with the decades long record of being safe deemed a treatment.
You are right about one thing. They are in the business of money, and they want the new drug because that is the one that will make them money. Lesson that should have been learned by the OxyContin debacle at the latest – Do not ever take what a pharmaceutical company says at face value, always look for ulterior motives.
Lack of action by Merck and the NIH are the reason that people are self dosing with the animal version in the first place. Since day 1, almost the entirety of the American focus has been on finding a magic treatment that is 1) profitable and 2.) is not a one shot deal. Keeping Americans healthy has not been part of the agenda for at least two and a half decades as far as I can see.
A brilliant analysis of the strategic thinking of the forces promulgating C19.
Should be of particular interest to financially savvy NC readers.
http://thephilosophicalsalon.com/a-self-fulfilling-prophecy-systemic-collapse-and-pandemic-simulation/
“Joining the dots is a simple enough exercise. If we do so, we might see a well-defined narrative outline emerge, whose succinct summary reads as follows: lockdowns and the global suspension of economic transactions were intended to 1) Allow the Fed to flood the ailing financial markets with freshly printed money while deferring hyperinflation; and 2) Introduce mass vaccination programmes and health passports as pillars of a neo-feudal regime of capitalist accumulation. As we shall see, the two aims merge into one.”
No kidding; just ask Glenn Beck
“Everything should be made as simple as possible, but not simple.” –Albert Einstein (attributed)
In general, people “connecting dots” never describe the nature of the connection rigorously. Adjacency is taken for causality. Hence, the dot connection methodology is very vulnerable to projection:
Structures are seen to exist that are not there…
Hey, there’s a cheap (in generic form, not the “branded” versions) medication that has been prescribed and used over the counter maybe a trillion times now, available in every country, effective for many health problems. For some reason, it is still widely available, even though its safety profile has some bumps and scabs. Here’s the Wiki on it: https://en.wikipedia.org/wiki/Aspirin
Speaking of course of acetylsalicylic acid, the ubiquitous aspirin, the successor to slippery elm bark in the native pharmacopoeia. Not patentable (I think), dirt cheap to produce. I wonder why the Pharma industry and the regulatory structure have not taken on the task of scaring people out of using aspirin because it can cause bleeding, tinnitus, GI problems and the other noted scary side effects, which are well documented, unlike the BS we are being fed in the Global North about IVM.
And one wonders what other legacy meds are out there that might be a specific for Covid. Given the interests and incentives, not likely us mopes will ever know.
It’s not like there are no real global health threats out there, being exacerbated by profligate use and abuse of “miracle drug” antibiotics… https://www.who.int/news/item/17-01-2020-lack-of-new-antibiotics-threatens-global-efforts-to-contain-drug-resistant-infections
JTMcPhee, I was wondering if you meant willow bark instead of slippery elm, which I’ve always associated with properties to sooth the G.I. tract. Doesn’t mean I’m right, of course.
Article on willow bark
Right you are. Aging neurons.
Where I live in Canada the most vocal groups promoting Ivermectin are the most vocal opposing masks,vaccines and social distancing.
Their protests obstructing hospitals are not helping the optics for Ivermectin use.
The local veternary Ivermectin supplies are almost exhausted, all that is left is the horse paste stuff. I do have enough for heart worm protection for the dogs and extra for any other use .
I doubt there are adequate human grade supplies available in Canada for widespread use by the public currently and increasing supplies would have had to start months ago.
links?
When I lived in Thailand I noticed that de-worming medicine for human consumption was sold everywhere – corner shops, Boots, etc. I assume it contains Ivermectin?
I lived there for 11 years and never had worms, BTW.
Not sure about Thailand but I know in Jamaica many people go around barefoot and can get hookworm that way. There tend to be many more parasites in tropical countries so it only makes sense that Ivermectin would be readily available OTC, as it is in Mexico any many other places.
Ivermectin is one of the safest drugs in the world, much safer than acetaminophen and even aspirin (which produces stomach bleeding at a 1% rate)
Not sure if anyone has posted this previously, but there does seem to be some internal conflict going on within the medical profession.
https://aapsonline.org/aaps-letter-to-ama-re-ivermectin-and-covid/?fbclid=IwAR2JdEZ47i92hK2tOobkaizf9uBYNB1oHMoIYl7lBfXM7Jb_1fh8XHxroqc
Indonesia is still forcing vaccination on people though. You might lose your Bansos (Social Aid) if you don’t get vaccinated.
https://www.thejakartapost.com/news/2021/02/15/get-vaccinated-or-lose-your-social-aid-indonesian-government-says.html
Sure that’s an article from some months ago, but friends of mine say that vaccination remains a prerequisite to accessing Social Aid.
Also what’s not mentioned in the article above is the Indonesian government started enforcing what’s known as PPKM Darurat a.k.a. lockdown starting around July 3rd. I’d like to think that Ivermectin played a part but at the same time the lockdown probably played not a small part in the drop of cases.
https://www.thejakartapost.com/news/2021/07/16/govt-bans-idul-adha-festivities-in-ppkm-darurat-areas.html
PPKM is still going on right now, although restrictions have been gradually lifted. Vulnerable people like children under 12 and old people above 70 are still prevented from going to malls, while the rest will need to be vaccinated before they can enter.
Just in from TrialsiteNews mainly focussing on Merck & their campaign to push Vioxx & their attacks on Ivermectin – written by David E. Scheim, PhD, US Public Health Service, Commissioned Corps, Inactive Reserve Blacksburg, VA
dscheim@alum.mit.edu
https://trialsitenews.com/mercks-deadly-vioxx-playbook-redux-a-debunked-smear-campaign-against-its-competing-drug-the-fda-approved-nobel-prize-honored-ivermectin/?
I am looking forward to seeing the results from the current Ivermectin clinical trials. One of them is being run out of McMaster University in Canada. I know a specialist in infectious diseases there, but he was crazy busy even before Covid. I am waiting until the dust settles (?) before asking him about Ivermectin. I think Yves asked about funding sources, and I seem to recall briefly reading that Gates Foundation was funding studies, possibly including the McMaster study. (The article I read pointed out that this presents a potential conflict of interest since Gates supports vaccines.)
I am too busy to fact check the following article, but some of the comments apply to the data from Indonesia above:
https://healthfeedback.org/claimreview/no-data-available-to-suggest-a-link-between-indias-reduction-of-covid-19-cases-and-the-use-of-ivermectin-jim-hoft-gateway-pundit/
The start dates of Ivemectin use in India and also in Indonesia seem to be too close to the drop off in new cases to be the reason for the drop. Even in the Indonesia example above, the hospitals started using it July 22 and new cases dropped by the first week of August. I can understand a drop in deaths in hospitals, but the drop in new cases seems a stretch to me.
Like Jerri-Lynn, I have spent time in India and nothing happens efficiently in the places I have been in, which includes about 30 cities across the country. It is hard for me to believe that the India and Indonesia suddenly got their acts together to distribute Ivermectin information across the entire country….within days of approval of its use for covid. I know some physicians in India and have emailed them before covid; the doctors I know are not good at staying on top of their emails.
It would be great if Ivermectin truly was efficacious, but I would like to wait until I see some trustworthy data. This following post is another example of a study gone wrong:
https://www.theguardian.com/science/2021/jul/16/huge-study-supporting-ivermectin-as-covid-treatment-withdrawn-over-ethical-concerns
re the grauniad, perhaps not… Dr. Tess Lawrie responds:
https://osf.io/peqcj/
The integrity of our meta-analyses of trial data on Ivermectin for prevention and treatment of Covid-19 is questioned by authors of a recent Cochranereview.We agree that misleading information on Covid-19 treatment abounds in social and mainstream media as well as in journal opinion pieces. However, Bryant et al is a non-commissioned research paper that strictly followed PRISMA systematic review guidelines.
Popp et al.itself contains several misleading items. The authors rehearse the outdated objection that whilst Ivermectin slows the reproduction of SARS-CoV-2, “such effects would need major doses in humans”. This conjecture has long been falsified by the results of formal trials and clinical experience worldwide, at 1–3 times the anti-parasitic dose. Professor Chris Whitty (CMO England), has stated: “The drug [Ivermectin] has proven to be safe. Doses up to 10 times the approved limit [200 mcg/kg] are well tolerated by healthy volunteers. Adverse reactions are few and usually mild
…
The effects found in Bryant et al.involved point estimates across trials that were almost universally in the same direction and consistently favoured Ivermectin. Our sensitivity analyses show that, contrary to some claims, the headline mortality advantage is robust to removal of individual trials. In particular, it is robust to the removal of a recently disputed trial, as we show explicitly elsewhere. Moreover a recent Bayesian analysis, systematically shows that the hypothesis of a therapeutic effect remains sustained even after removal of two contested trials. It is inappropriate for Popp et al.to claim that we “misuse established evidence assessment tools as a guise for quality of evidence synthesis”,in reference to work by researchers with extensive experience in evidence synthesis. They further claim that Bryant et al. tried “to create pseudo-trustworthiness” insinuating that we have deliberately tried to create, not solve, public health problems. Open scientific debate is essential, but should focus on material facts and logical reasoning. The basis of the critique of Popp et al. remains unclear
Instead of using all available evidence and presenting appropriate caveats, their own contribution disregards sources selectively and presents threadbare analyses. In a pandemic context, the benefits of Ivermectin almost certainly outweigh any risks, given its outstanding safety profile, negligible base cost, and the existing large body of evidence showing that ivermectin provides benefit in a variety of important clinical outcomes.”
re the grauniad, perhaps not… Dr. Tess Lawrie responds:
https://osf.io/peqcj/
The integrity of our meta-analyses of trial data on Ivermectin for prevention and treatment of Covid-19 is questioned by authors of a recent Cochranereview.We agree that misleading information on Covid-19 treatment abounds in social and mainstream media as well as in journal opinion pieces. However, Bryant et al is a non-commissioned research paper that strictly followed PRISMA systematic review guidelines.
Popp et al.itself contains several misleading items. The authors rehearse the outdated objection that whilst Ivermectin slows the reproduction of SARS-CoV-2, “such effects would need major doses in humans”. This conjecture has long been falsified by the results of formal trials and clinical experience worldwide, at 1–3 times the anti-parasitic dose. Professor Chris Whitty (CMO England), has stated: “The drug [Ivermectin] has proven to be safe. Doses up to 10 times the approved limit [200 mcg/kg] are well tolerated by healthy volunteers. Adverse reactions are few and usually mild
…
The effects found in Bryant et al.involved point estimates across trials that were almost universally in the same direction and consistently favoured Ivermectin. Our sensitivity analyses show that, contrary to some claims, the headline mortality advantage is robust to removal of individual trials. In particular, it is robust to the removal of a recently disputed trial, as we show explicitly elsewhere. Moreover a recent Bayesian analysis, systematically shows that the hypothesis of a therapeutic effect remains sustained even after removal of two contested trials. It is inappropriate for Popp et al.to claim that we “misuse established evidence assessment tools as a guise for quality of evidence synthesis”,in reference to work by researchers with extensive experience in evidence synthesis. They further claim that Bryant et al. tried “to create pseudo-trustworthiness” insinuating that we have deliberately tried to create, not solve, public health problems. Open scientific debate is essential, but should focus on material facts and logical reasoning. The basis of the critique of Popp et al. remains unclear
Instead of using all available evidence and presenting appropriate caveats, their own contribution disregards sources selectively and presents threadbare analyses. In a pandemic context, the benefits of Ivermectin almost certainly outweigh any risks, given its outstanding safety profile, negligible base cost, and the existing large body of evidence showing that ivermectin provides benefit in a variety of important clinical outcomes.”
Behind the Bastards just released an episode on Ivermectin. It seems to be pretty well researched and reasonable, unlike the breathless, hysterical tone of the article above: https://www.stitcher.com/show/behind-the-bastards/episode/part-one-the-ivermectin-episode-86610131
At the risk of re-posting a citation already mentioned…
https://www.covid19treatmentguidelines.nih.gov/therapies/antiviral-therapy/ivermectin/
This piece is fairly neutral. As an institution, NIH will be conservative in its statements. To me at least, it looks like field data is really “noisy” and still needs interpretation from better studies.
We keep paste de wormers on hand as a matter of course for our large animals. Things get really skeezy, I’d probably use the swine dose guidance. They’re a lot like us.
If things get really skeezy — you really should get your dosage and usage guidance from the FLCCC protocol. Use as a de-wormer is different than use against Corona flu.
The Together Trial on IVM has already concluded and the lead investigator, Mills, announced IVM showed “no effect whatsoever”. Dr. Kory, from FLCCC, discusses the Together results in this video:
https://odysee.com/@FrontlineCovid19CriticalCareAlliance:c/outpatients-defeating-the-delta-variant:a?r=663tPbvh6yLkRomB3LipYjgjAJwbkLPX
The main criticism I got from his talk was that the dosage given of IVM was too low & number of days given was too few. The gamma variant of covid was dominant in the state in Brazil were the trial sites were located and Kory says the IVM dosage should have been more to have seen an effect.
Also, what Kory saw of the data showed an 18% relative reduction in mortality for the IVM group, which doesn’t sound like ‘no effect whatsoever’. What Mills should have said was “no statistically significant effect”, which allows for the possibility the lack of result is due to the trial itself and not to IVM. For example, the sample size could have been too small. Possibly, the exact same data outcomes with a larger sample size would have yielded statistical significance.
It’s also troubling that the announcement of the Together IVM results was a month ago and there is still no preprint up on medrxiv as of today, but a more recent Together Trial result on fluvoxamine had a preprint available immediately.
> there is still no preprint up on medrxiv as of today
The paper’s not out, so there’s nothing to go on but a slide presentation. This is exactly like Fauci ramping Remdesivir on the basis of a press release. Wake me when there is a preprint.
Excuse me, but this isn’t anything at all like Fauci touting remdesivir. Fauci has a global soapbox, for one thing, and his conflict of interest was massive. Kory has been shunned and ignored and has far more evidence already on his side re ivm than Fauci ever had or ever will have for remdesivir. On top of that Kory has to defend his besmirched reputation from an absolute corrupt industry and the peons who continue to ignore his work. See IMDocs comment this morning’s about AMA. I think you have double standards, especially when it comes to your interpretation of what a “fine scientist” is. You are quick to point out any perceived weakness in an argument and tell people they should shut up before the info is in or that the sources are insufficient to pass muster with your standards. You have no such problem with the insufficiently effective vaccines or the woefully inadequate data collection that renders almost every conclusion arrived at re covid into a bunch of unprovable and misinforming statistics.
In response to Michael Sharkey’s post:
I am a retired physician and Covid-19 communications to all doctors are controlled through the Oregon Medical Association (the Oregon chapter of the AMA). I am not a member of the OMA and not sure how they got our email addresses, but I am guessing it’s through the Oregon Medical Board.
The OMA Covid newsletters were quick to blast out newsletters against hydroxychloroquine and ivermectin.
OTOH, remdesivir and monoclonal antibodies get the big thumbs up!
The OMA sent out a non-Covid related promotion for Alzheimer’s & Brain Awareness Month on June 29th of this year. The topic: Alzheimer’s Association Welcomes FDA Approval of Aducanumab
The AMA journal, JAMA, makes revenue from drug advertising. The findings in 2014 research suggest that ads are blitzing the Canadian doctors far more. But… advertising of prescription drugs aimed directly at the public is prohibited in most countries, including Canada. We stooges sit through drug commercials with side effects sped read and are vastly more effective in demanding patented meds from our doctors.
https://www.ncbi.nlm.nih.gov/pmc/articles/PMC3885602/
The two Canadian journals sampled (CMAJ, CFP) contained five times more advertisements than the two American journals (JAMA, NEJM), and two British journals (BMJ, Lancet) (p<0.0001). The estimated annual revenue from pharmaceutical advertisements ranged from £0.025 million (for Lancet) to £3.8 million (for JAMA). The cost savings due to revenue from pharmaceutical advertising to each individual subscriber ranged from £0.02 (for Lancet) to £3.56 (for CFP) per issue.
This all has the elements of a future dystopia where in 5-10 years, the Western countries go through a massive die off of people because it would not, could not understand the deadly outcome of using mRNA viruses and shutting down, even criminalizing effective treatments. As the West see millions upon millions get sick and die for the sake of pharma profits, the Global South remains healthy and vibrant as they choose to use alternatives including the Russian and Chinese vaccines. The novel and movie remain to be made. Well, maybe it has actually be made or written. And yes, I am vaccinated with J&J.