By Lambert Strether of Corrente.
The other day I was trying to find out why Beto O’Rourke, who claims to support Medicare for All, hasn’t signed on to HR676, the single payer bill before the House. On the Twitter, I was provided this link (from The Ringer, an affiliate site of Markos Moulitsas’ SB Nation sports site). First, the mushy generalities:
[BETO:] So, what’s my vision? Universal health care. And very likely that will involve some form of a single-payer system, some expansion of Medicare, perhaps from where it is right now at 65, all the way down to zero.
Mush. Moving Medicare eligibility down to zero was Ted Kennedy’s approach, before Obama did whatever he did to Teddy’s brain. Perhaps this was the approach O’Rourke would have taken in the Medicare bill he promised to introduce, and didn’t. Now one policy issue:
O’Rourke hasn’t signed on to HR 676, the Medicare-for-All bill that’s attracted 121 Democratic cosponsors, because as he explained at a town hall six months ago, the bill allows for Medicare reimbursement to only nonprofit health care providers, not private providers.
A second policy issue: co-pays and deductibles. From the Texas Observer in 2017:
O’Rourke likes what he’s read of Sanders’ bill [S1804], but disagrees with having no copays for anyone and no premiums for low-income families — he’d prefer everyone pay in to some extent. But O’Rourke said something better than the status quo is needed, whether it’s a version of Conyers’ bill, Sanders’ bill or one he’s drafting himself.
Again, if O’Rourke — harder to type than Beto, dammit — has drafted a Medicare for All bill, it’s still resting comfortably in his desk drawer. But speaking of S1804, O’Rourke’s opponent in the 2018 Texas Democrat primary, Sema Hernandez, says he supports it (letter dated September 3, 2018). However, Hernandez may be far too generous; Current Affairs has a fine summary of O’Rourke’s crawfishing on the issue. And if O’Rourke does in fact support S1804, why doesn’t he say so on his mushy site?
Be that as it may, watching O’Rourke do fakies on health care does show us that the differences between HR676 and S1804 — especially around co-pays/deductibles and reimbursements — will form one flashpoint in the battle between centrist forces like the New Democrats and the left on health care policy. (This is distinct from the usual liberal bait-and-switch and brand confusion tactics last employed in 2009.) And since this really isn’t a post about O’Rourke, emblematic though he is as a figure, I will now turn to the two bills, and compare and contrast them. Here they are.
HR676 and S1804
1) HR676: Expanded & Improved Medicare For All Act, sponsored for a long time by John Conyers, and in the last Congress by Keith Ellison. We don’t know who will sponsor the bill in the next Congress. Here is a list of the HR676 co-sponsors, so you can check to see if your Representative supports the bill, and call and hassle them if they don’t:
Represenatives Adams, Alma S. [(D) NC-12], Barragan, Nanette Diaz [(D) CA-44], Bass, Karen [(D) CA-37], Beatty, Joyce [(D) OH-3], Beyer, Donald S., Jr. [(D) VA-8], Bishop, Sanford D., Jr. [(D) GA-2], Blumenauer, Earl [(D) OR-3], Bonamici, Suzanne [(D) OR-1], Boyle, Brendan F. [(D) PA-13], Brady, Robert A. [(D) PA-1], Brown, Anthony G. [(D) MD-4], Butterfield, G. K. [(D) NC-1], Capuano, Michael E. [(D) MA-7], Carson, Andre [(D) IN-7], Cartwright, Matt [(D) PA-17], Castor, Kathy [(D) FL-14], Chu, Judy [(D) CA-27], Cicilline, David N. [(D) RI-1], Clark, Katherine M. [(D) MA-5], Clarke, Yvette D. [(D) NY-9], Clay, Wm. Lacy [(D) MO-1], Cleaver, Emanuel [(D) MO-5], Clyburn, James E. [(D) SC-6], Cohen, Steve [(D) TN-9], Cooper, Jim [(D) TN-5], Correa, J. Luis [(D) CA-46], Crowley, Joseph [(D) NY-14], Cummings, Elijah E. [(D) MD-7], Davis, Danny K. [(D) IL-7], DeFazio, Peter A. [(D) OR-4], DeGette, Diana [(D) CO-1], DeSaulnier, Mark [(D) CA-11], Deutch, Theodore E. [(D) FL-22], Dingell, Debbie [(D) MI-12], Doyle, Michael F. [(D) PA-14], Ellison, Keith [(D) MN-5], Engel, Eliot L. [(D) NY-16], Eshoo, Anna G. [(D) CA-18], Espaillat, Adriano [(D) NY-13], Evans, Dwight [(D) PA-2], Frankel, Lois [(D) FL-21], Fudge, Marcia L. [(D) OH-11], Gabbard, Tulsi [(D) HI-2], Gallego, Ruben [(D) AZ-7], Garamendi, John [(D) CA-3], Gomez, Jimmy [(D) CA-34], Gonzalez, Vicente [(D) TX-15], Green, Al [(D) TX-9], Green, Gene [(D) TX-29], Grijalva, Raul M. [(D) AZ-3], Gutierrez, Luis V. [(D) IL-4], Hastings, Alcee L. [(D) FL-20], Higgins, Brian [(D) NY-26], Huffman, Jared [(D) CA-2], Jackson Lee, Sheila [(D) TX-18], Jayapal, Pramila [(D) WA-7], Jeffries, Hakeem S. [(D) NY-8], Johnson, Eddie Bernice [(D) TX-30], Johnson, Henry C. “Hank,” Jr. [(D) GA-4], Jones, Brenda [(D) MI-13], Kaptur, Marcy [(D) OH-9], Kelly, Robin L. [(D) IL-2], Khanna, Ro [(D) CA-17], Langevin, James R. [(D) RI-2], Lawrence, Brenda L. [(D) MI-14], Lawson, Al, Jr. [(D) FL-5], Lee, Barbara [(D) CA-13], Lewis, John [(D) GA-5], Lieu, Ted [(D) CA-33], Loebsack, David [(D) IA-2], Lofgren, Zoe [(D) CA-19], Lowenthal, Alan S. [(D) CA-47], Lowey, Nita M. [(D) NY-17], Maloney, Carolyn B. [(D) NY-12], Matsui, Doris O. [(D) CA-6], McGovern, James P. [(D) MA-2], McNerney, Jerry [(D) CA-9], Meeks, Gregory W. [(D) NY-5], Meng, Grace [(D) NY-6], Moore, Gwen [(D) WI-4], Nadler, Jerrold [(D) NY-10], Napolitano, Grace F. [(D) CA-32], Nolan, Richard M. [(D) MN-8], Norcross, Donald [(D) NJ-1], Norton, Eleanor Holmes [(D) DC-At Large], Panetta, Jimmy [(D) CA-20], Payne, Donald M., Jr. [(D) NJ-10], Perlmutter, Ed [(D) CO-7], Pingree, Chellie [(D) ME-1], Pocan, Mark [(D) WI-2], Polis, Jared [(D) CO-2], Price, David E. [(D) NC-4], Raskin, Jamie [(D) MD-8], Roybal-Allard, Lucille [(D) CA-40], Rush, Bobby L. [(D) IL-1], Ryan, Tim [(D) OH-13], Sablan, Gregorio Kilili Camacho [(D) MP-At Large], Sanchez, Linda T. [(D) CA-38], Sarbanes, John P. [(D) MD-3], Schakowsky, Janice D. [(D) IL-9], Schiff, Adam B. [(D) CA-28], Scott, Robert C. “Bobby” [(D) VA-3], Serrano, Jose E. [(D) NY-15], Sherman, Brad [(D) CA-30], Sires, Albio [(D) NJ-8], Slaughter, Louise McIntosh [(D) NY-25], Smith, Adam [(D) WA-9], Soto, Darren [(D) FL-9], Speier, Jackie [(D) CA-14], Swalwell, Eric [(D) CA-15], Takano, Mark [(D) CA-41], Thompson, Bennie G. [(D) MS-2], Thompson, Mike [(D) CA-5], Titus, Dina [(D) NV-1], Tonko, Paul [(D) NY-20], Veasey, Marc A. [(D) TX-33], Vela, Filemon [(D) TX-34], Velazquez, Nydia M. [(D) NY-7], Visclosky, Peter J. [(D) IN-1], Waters, Maxine [(D) CA-43], Watson Coleman, Bonnie [(D) NJ-12], Welch, Peter [(D) VT-At Large], Wilson, Frederica S. [(D) FL-24], Yarmuth, John A. [(D) KY-3]
124 of 194 Represenatives (64%) supported HR676 in the last Congress. There are 40 new Democrat representatives in the the next Congress. If none of them support HR676, the percentage will drop to 53%.
2) S1804, Medicare for All Act of 2017, sponsored by Bernie Sanders. Here are the co-sponsors; I’ve underlined the mooted Presidential candidates, though that will change”
Senators Baldwin, Tammy [D-WI], Blumenthal, Richard [D-CT], Booker, Cory A. [D-NJ], Franken, Al [D-MN], Gillibrand, Kirsten E. [D-NY], Harris, Kamala D. [D-CA], Heinrich, Martin [D-NM], Hirono, Mazie K. [D-HI], Leahy, Patrick J. [D-VT], Markey, Edward J. [D-MA], Merkley, Jeff [D-OR], Schatz, Brian [D-HI], Shaheen, Jeanne [D-NH], Udall, Tom [D-NM], Warren, Elizabeth [D-MA], Whitehouse, Sheldon [D-RI]
(I’m stunned that a Senator named Whitehouse isn’t looking in the mirror and seeing a President.) 16 of 49 Senators (33%) supported S1804 in the last Congress. The Democrats lost two Senators, so if now new Senators sign on, support will increase to 34%.
Now lets turn to the good news about both bills.
The Good News
There’s a lot of good news in both bills — both really would improve the health care system dramatically, making health care a human right in addition to saving a boatload of money — but I’m going to single out one. From a handy comparison chart produced by the Western Washington chapter of PNHP (PDF):

IMNSHO, it’s absolutely necessary, as a first step toward cleaning up the neoliberal infestations in our health care system, to make health care free at the point of delivery, like the NHS or (at least when I was there) Canada. The complex systems of eligibility determination — co-pays, deductibles, “cost sharing,” as the chart calls it — so beloved by liberals are a way to sort those deserving of health care (they go to Happyville) from those undeserving (they go to Pain City). Even leaving issues of justice and health care as a right aside, those fee collecting systems, if left in place, will be morph into new ways to deny people care and to fund credentialed professionals who are in the business of doing that. That’s what those systems are designed to do! O’Rourke, befitting his New Democrat membership, wants those cost sharing systems left in place. They should be eliminated root and branch. S1804 should eliminate that $200 co-pay for pharmaceuticals. It’s not worth keeping.
The Bad News
There is some bad news in S1804 that is not present in HR676: Provider payment, and phase-in. Let’s look at each in turn.
Provider Payment. From the Western Washington Chapter of PNHP once more:
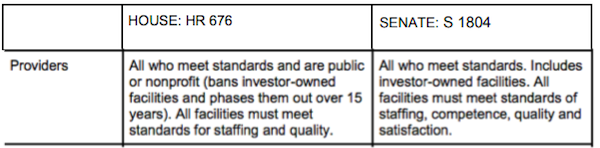
As you can see, HR676 does not allow payments to for-profit providers; S1804 does. (Readers will recall that New Democrat O’Rourke prefers payments to for-profit providers.) That’s a concern. From Steffie Woolhandler David Himmelstein in Health Affairs:
Aligning House And Senate Single-Payer Bills: Removing Medicare’s Profiteering Incentives Is Key
[S1804] largely adopts Medicare’s current payment mechanisms; the House bill’s is modeled on Canada’s single-payer program, also called “Medicare,” which pays hospitals global budgets (much as a fire department is paid in the U.S.) and sharply constrains opportunities for investor-owned care.
These differences haven’t attracted much attention from politicians or the press, and few patients are aware of, or deeply concerned about them. That’s not surprising, since both bills address the lay public’s most pressing payment-related concern: they would drastically shrink (S.1804) or completely eliminate (H.R. 676) out-of-pocket payments for needed care.
But these divergent payment strategies would create very different financial incentives for providers, shaping the culture of medicine and the financial viability of a single-payer reform. The Senate version would, like Medicare, pay hospitals and other institutional providers on a per-patient basis, intermixing payments for current operating expenses with funding for future capital investments and profits. As at present, hospitals’ success, and even survival, would depend on generating profits (“surpluses” in non-profit facilities). Hospitals with a favorable bottom line could invest and add new buildings and programs, while unprofitable ones couldn’t modernize or expand, risking a downward spiral toward takeover or closure.
It’s this profit imperative that drives hospitals’ financial gaming, e.g. upcoding, and concentration on the most lucrative services, such as elective cardiac and orthopedic services, rather than money losers like mental health. This payment mechanism (and S.1804 as a whole) also leaves the door open to investor-owned providers.
(See NC on upcoding here and here.) If you regard the profit motive as a cancer on the health care system, then S1804 could feed the tumor more blood (depending on how hospitals game the new system, as they would have every incentive to do). That doesn’t seem like the optimal course of treatment to choose.
Phase-In. Again from the Western Washington Chapter of PNHP:
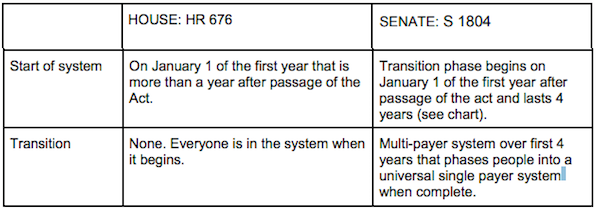
The long phase-in for S1804 gives me the creeps. The players in the health care system are highly unlikely to roll over and accept that the rules of the game have changed (and in fact, S1804’s retention of the profit motive gives them every incentive not to do so.) Four years is — you knew this was coming — a long time in politics, and all the brand confusion and watering down and bait-and-switch tactics used to oppose the bill will then be re-purposed for the phase-in period to delay implentation or even to roll it back (“It’s just too hard.” Here one imagines the avalanche of propaganda and sob stories in our famously free press). Medicare was phased in one year, back in the day when steam-powered computers were driven by punch cards. The health care system will have plenty of “time to prepare” during the debate before passage of the bill (and the more complexity and useless cruft we rip out, the easier preparation will be). There is no reason to assume that players who control the current system are working in good faith, and they should not be given four years to cripple the bill. Sanders should know this.
Conclusion
So, good news, bad news. I can see the political arguments for S1804, in terms of “writing a bill that will pass.” However, if Sanders, as he seems to be doing, hopes to get the bill passed by building a mass movement outside Congress, then there’s really no reason for him to negotiate with himself and begin with a watered-down bill. Having been granted their profits, the providers will then fight tooth and nail against the bill for some other reason. Why not start by forcing them to fight tooth and nail for profit? Let’s see whether O’Rourke and the New Democrats can sell that. Sanders needs to be stand up on this more than he has.

