By Lambert Strether of Corrente.
Here is the latest Johns Hopkins “Global Cases” tracker on the spread of #2019-nCoV (I’m using that hashtag in proses, insted of Wuhan Corona Virus, or Corona Virus, because I think it gives me the best hits on the Twitter).
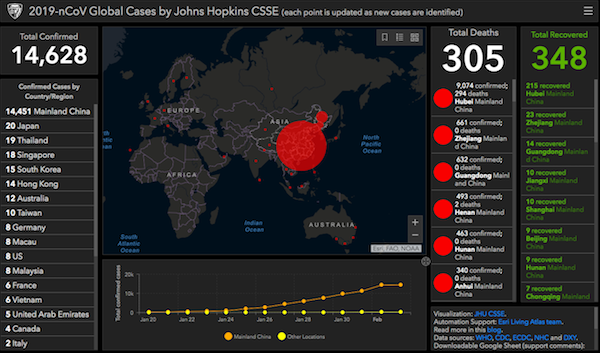
There’s every reason to think that the cases are under-reported, since health facilities where the virus has hit are overwhelmed, and testing kits are scarce; see the story of Zhang Chi’s 10-day quest for treatment at Sixth Tone. (“Fortunately, as president of a local soccer fans’ club with over 1,000 members, Zhang had a lot of friends.” So one can only wonder how the poor and working class are doing.) Numbers aside, the Lancet’s assessment of last week remains in force:
Given that 2019-nCoV is no longer contained within Wuhan, other major Chinese cities are probably sustaining localised outbreaks. Large cities overseas with close transport links to China could also become outbreak epicentres, unless substantial public health interventions at both the population and personal levels are implemented immediately. Independent self-sustaining outbreaks in major cities globally could become inevitable because of substantial exportation of presymptomatic cases and in the absence of large-scale public health interventions. Preparedness plans and mitigation interventions should be readied for quick deployment globally.
In this morning’s Links, I provided a look at the mainstream #2019-nCoV news; here is one addition from Bloomberg: “China’s $22 Billion Injection May Help Ease Global Market Rout”
A $22 billion injection into Chinese markets won’t be enough to prevent the country’s stocks and currency falling on Monday, but it may ease a global sell-off sparked by the spread of the coronavirus.
That’s according to analysts after the People’s Bank of China and other regulators announced a slew of measures to shore up their financial markets when they re-open following the Lunar New Year holiday.
The central bank said Sunday it will use reverse repurchase agreements to supply 1.2 trillion yuan of liquidity on Monday, with the figure coming to 150 billion yuan ($21.7 billion) on a net basis, according to Bloomberg calculations.
“This is well beyond the band-aid fix,” said Stephen Innes, a Bangkok-based chief market strategist at Axicorp. “If this deluge doesn’t hold risk-off at bay, we are in for a colossal beat down. In addition, the PBOC will likely intervene in the currency market, so I would expect them to layer the soothing market balm thick and heavy.”….
In a containment scenario — with a severe but short-lived impact — it could take China’s first-quarter gross domestic product growth down to 4.5% year-on-year, according to Bloomberg Economics. That would be the lowest quarterly figure since at least 1992.
(At least according to David Harvey, China was the force that prevented global collapse after our Great Financial Crisis. If we have another one such this year — not on the horizon, I admit — it seems unlikely they will be able to play that role again.) Anyhow, in this post I’m going to collect some of the more estoric items I gleaned in my travels looking for Links and trying to keep up with the situation generally: Transmission methods, travel bans, the danger of mutation, and the bioweapon CT. I’ll conclude with a brief remark on institutional factors.
Transmission Methods
First, there is the possibility that the virus may be transmitted by touching surfaces. MedPage Today:
[Maria Van Kerkhove, of WHO’s emerging diseases and zoonosis division] said that evidence indicates the virus can be transmitted through the respiratory route, via droplets, and physical contact between people, but also from fomites, as the virus can live on surfaces for a short period of times
Sidebar for the word of the day: fomite:
Any inanimate object, that when contaminated with or exposed to infectious agents, such as pathogenic bacteria, viruses or fungi, can transfer disease to a new host. In addition to objects in hospital settings, other common fomites for humans are door knobs, light switches, handrails, elevator buttons, television remote controls, pens, and other items that are frequently touched by different people and that may be infrequently cleaned.
Researchers have discovered that smooth (non-porous) surfaces like door knobs transmit bacteria and viruses better than porous materials like paper money because porous, especially fibrous, materials absorb and trap the contagion, making it harder to contract through simple touch.
So far as I know, there is no case of #2019-nCoV with a history of fomite transmission, so we will have to look to other viruses for indications. End sidebar.
From the American Society for Microbiology, “Significance of Fomites in the Spread of Respiratory and Enteric Viral Disease” (2007), a review of the literature:
There is now growing evidence that contaminated fomites or surfaces play a key role in the spread of viral infections.
Virus spread by person-to-person contact can be interrupted with isolation of the viral carrier. Yet, isolation may prove to be impractical or difficult if there are many people or if the source of infection is unknown (69). Consequently, interrupting disease spread via indoor fomites is one of the more practical methods for limiting or preventing enteric and respiratory viral infections.
A majority of respiratory viruses are enveloped (parainfluenza virus, influenza virus, RSV, and coronavirus) and survive on surfaces from hours to days….
Studies have demonstrated that viral transfer from hands to surrounding surfaces is possible in 7 out of 10 viruses reviewed. Generally, research evidence suggests that a large portion of enteric and respiratory illnesses can be prevented through improved environmental hygiene, with an emphasis on better hand and surface cleaning practices.
(So clean your keyboards, light switches, etc. besides washing your hands!) For a corona virus, although not #2019-nCoV specifically, from the American Society for Microbiology, “Effects of Air Temperature and Relative Humidity on Coronavirus Survival on Surfaces” (2010):
The potential reemergence of SARS or the emergence of new strains of pandemic influenza virus, including avian and swine influenza viruses, could pose serious risks for nosocomial disease spread via contaminated surfaces. However, this risk is still poorly understood, and more work is needed to quantify the risk of exposure and possible transmission associated with surfaces.
From the American Society for Microbiology, “Human Coronavirus 229E Remains Infectious on Common Touch Surface Materials“:
Animal coronaviruses that “host jump” to humans result in severe infections with high mortality, such as severe acute respiratory syndrome (SARS) and, more recently, Middle East respiratory syndrome (MERS). We show here that a closely related human coronavirus, 229E, which causes upper respiratory tract infection in healthy individuals and serious disease in patients with comorbidities, remained infectious on surface materials common to public and domestic areas for several days. The low infectious dose means that this is a significant infection risk to anyone touching a contaminated surface.
Again, however, we don’t have any kind of case data whatever, so for now I’m putting this into the category of things one might worry about (as opposed to things one should absolutely not do, like standing next to a coughing person from Wuhan for any period of time). Fascinatingly, the article concludes:
However, rapid inactivation, irreversible destruction of viral RNA, and massive structural damage were observed in coronavirus exposed to copper and copper alloy surfaces.
So if your bathroom fixtures are made out of copper, you’re good. Alternatively, one could visit the local home and garden store and experiment…. (Kidding! Copper sprays are poisonous!)
The second route of transmission is a bit less esoteric: Fecal transmission. Once again, from Bloomberg:
The novel coronavirus was detected in the loose stool of the first U.S. case — a finding that hasn’t featured among case reports from Wuhan, China, the epicenter of the outbreak. However, that doesn’t surprise scientists who have studied coronaviruses, nor doctors familiar with the bug that caused SARS.
Squat latrines, common in China, lacking covers and hands that aren’t washed thoroughly with soap and water after visiting the bathroom could be a source of virus transmission, said [John Nicholls, a clinical professor of pathology at the University of Hong Kong], who was part of the research team that isolated and characterized the SARS virus.
A virus-laden aerosol plume emanating from a SARS patient with diarrhea was implicated in possibly hundreds of cases at Hong Kong’s Amoy Gardens housing complex in 2003. That led the city’s researchers to understand the importance of the virus’s spread through the gastrointestinal tract, and to recognize both the limitation of face masks and importance of cleanliness and hygiene, Nicholls said.
I wouldn’t classify face masks as virtue signaling, exactly, but the more I read, the more 19th-Century basic hygiene measures assume salience. (I’m not sure whether fecal matter as such would be considered a fomite, as opposed, say, to the metal handle of a flush toilet.)
Travel Bans
From STAT News:
Travel and trade restrictions can lead to dire economic consequences for countries involved, creating a disincentive for them to quickly disclose potential outbreaks to the WHO or other nations. They can hinder the sharing of information, make it harder to track cases and their contacts, and disrupt the medical supply chain, potentially fueling shortages of drugs and medical supplies in the areas hit hardest by the outbreak. They also send a punitive message, which could contribute to discrimination and stigmatization against Chinese nationals, experts warned.
Any effort and money spent crafting and enforcing travel and trade restrictions also take away already-stretched resources from public health measures that have been proven to be far more effective, experts said. Those measures include providing assistance to countries with weaker health systems, accelerating the development of a vaccine or rapid diagnostic test, and clearly communicating with the public about when and how to seek care.
I’ve gotta say I’m of two minds about this. I accept the argument that a travel ban will only slow, and not stop, the acceleration of a virus (since original propagators will have already been in-country). And apparently the Chinese interpreted Trump’s punitive message all too clearly. Still, if increased social distance is a good method to stop an epidemic, what social distance is easier to increase than that between countries? (Perhaps an exception could be made for scientists and medical personnel.) For example:
[T]ravel has made the world far more interconnected than in 2003, accelerating the rate of infection. China — the starting point for both viruses — has become the world’s largest outbound tourism market and one of the engines driving the global economy. In the intervening years since the SARS outbreak, global airline capacity into China is 3.8 times larger than it was in 2005. China flights now account for 12 percent of total worldwide available seat kilometers versus only five percent 15 years ago, according to PlaneStats.com, Oliver Wyman’s aviation data portal.
Is mass tourism that important?
The Danger of Mutation
One of the issues with viral epidemics is that the viruses mutate, sometimes becoming more lethal. Sadly, there is a path for #2019-nCoV to do this. From, once again, the American Society for Microbiology, “Novel Coronavirus (2019-nCoV) Receptors Show Similarities to SARS-CoV, According to New Analysis” (Jan. 30, 2020):
Decade-long structural studies by Fang Li of the University of Minnesota, et al. have shown how the SARS virus (SARS-CoV) interacts with animal and human hosts in order to infect them. The mechanics of infection by the Wuhan coronavirus appear to be similar. These investigators used the knowledge they gleaned from multiple SARS-CoV strains—isolated from different hosts in different years—and angiotensin-converting enzyme-2 (ACE2) receptors from different animal species to model predictions for the novel Wuhan coronavirus. (Both viruses use ACE2 to gain entry into the cell, but it serves normally as a regulator for heart function.)
“Our structural analyses confidently predict that the Wuhan coronavirus uses ACE2 as its host receptor,” the investigators wrote. That and several other structural details of the new virus are consistent with the ability of the Wuhan coronavirus to infect humans and with some capability to transmit among humans.
“Alarmingly, our data predict that a single mutation [at a specific spot in the genome] could significantly enhance [the Wuhan coronavirus’s] ability to bind with human ACE2,” the investigators write. For this reason, Wuhan coronavirus evolution in patients should be closely monitored for the emergence of novel mutations at the 501 position in its genome, and to a lesser extent, the 494 position, in order to predict the possibility of a more serious outbreak than has been seen so far.
Ulp. Great work on the science, though!
No, #2019-nCoV Is Not a Bioweapon
At least one finance-adjacent blog (not this one) promoted a bioRxiv pre-print entitled “Uncanny similarity of unique inserts in the 2019-nCoV spike protein to HIV-1 gp120 and Gag”, containing the inflammatory passage “The finding of 4 unique inserts in the 2019-nCoV, all of which have identity/similarity to amino acid residues in key structural proteins of HIV-1 is unlikely to be fortuitous in nature.” That paper has now been withdrawn. From Richard Sever, Assistant Director of Cold Spring Harbor Laboratory Press, Editor of CSH Perspectives, bioRxiv Co-Founder:
Authors of disputed “uncanny” 2019-nCoV preprint to voluntarily withdraw preprint:
"It was not our intention to feed into the conspiracy theories…we appreciate the criticisms…and will get back with a revised version” https://t.co/zGcT1440D0— Richard Sever Ⓤ (@cshperspectives) February 1, 2020
Here is what one bioinformatics research had to say about the now-withdrawn paper:
The 2019-nCoV genome does not contain remarkable genomic properties which need explaining, and for which we’d look to some kind of bioengineering as a cause.
The virus has a close 96% sequence overlap to a naturally occurring bat coronavirus, and coronaviruses have been known to jump from bats to humans by way of intermediates before, like the SARS coronavirus. The differences between the genome sequences, including the ones identified by the Indian study, are in variable regions of the genome that we’d expect to differ, and the 4% difference in the genomes is hard to call as “high” or “low,” given that we don’t know exactly which bats the 2019-nCoV strain came from or when it diverged from its closest known ancestor.
Nor is it surprising that the known 2019-nCoV sequences all contain the same genomic changes relative to a known relative. They all came from the same outbreak from the same animal reservoir, i.e. they only diverged from each other a few months ago at most. It’s not surprising that they haven’t evolved very much away from each other.
Nor does the clinical presentation of 2019-nCoV have novel features which need explaining. Its symptom profile, degree of transmissibility, severity, mortality rate, duration, incubation and latent period, ability to jump from animals to humans, and ability to transmit asymptomatically and by skin contact are all within the precedents established by other human coronaviruses.
That is, the 2019-nCoV genome and the way it affects humans have, by themselves, no special anomaly which needs explaining.
(More on 2019-nCoV and bat corona viruses here.) Further, from Infection, Genetics and Evolution, “Full-genome evolutionary analysis of the novel corona virus (2019-nCoV) rejects the hypothesis of emergence as a result of a recent recombination event“:
The levels of genetic similarity between the 2019-nCoV and [BatCoV] RaTG13 suggest that the latter does not provide the exact variant that caused the outbreak in humans, but the hypothesis that 2019-nCoV has originated from bats is very likely. We show evidence that the novel coronavirus (2019-nCov) is not-mosaic consisting in almost half of its genome of a distinct lineage within the betacoronavirus.
Conclusion
There’s been a good deal of dunking on how China’s government and health care system has handled the #2019-nCoV epidemic (or pandemic). For example, from the China Media Project, a really interesting media critique, “As an Epidemic Raged, What Kept Party Media Busy?“. It concludes:
On January 25, there were at last two reports about the epidemic on the right-hand side of the People’s Daily front page. Either of these stories would have merited top billing on the page, but this was not the case. Priority was given instead to a report in the anti-poverty propaganda series, “The General Secretary Visited Hour Home.”
During this key period, from January 21 to 25, many party members, cadres and ordinary people were full of suspicions. They wondered how it was that no member of the CCP Standing Committee had yet managed to visit the scene of the epidemic in Wuhan, something that had happened in the case of both the SARS epidemic and the 2008 Wenchuan earthquake. When people felt fearful and at a loss, why was there all this focus on peace and happiness?
The blame certainly does not fall on the shoulders of the top editors of these Party papers. Since the start of the year, the pages of China’s Party newspapers have been given their “assigned seats.” The activities in which leaders would take part had already been fixed, and the themes to be emphasized had been more or less carved in stone. Inspections, greetings, expressions of condolence, banquet speeches – everything had already been planned. There would be no detracting from the prestige of the “leader.”
The system of the CCP is like a great big elephant. It is difficult for the sudden and unexpected to force any change to its huge and lumbering gait.
All of the deception and miscalculation that has happened in the wake of the revealing of the epidemic has been a source of immense public anger.
However, NC readers have are familiar with and have expressed a rather robust critique of the health care system in the United States. Can we — a country that until last year was experiencing dropping life expectancy — say we would do better than China?


Imagine trying to quarantine the Chicago metro area. That’s the enormity of the task we’re talking about.
I think these fellows will be fine with being quarantined. https://www.esquire.com/news-politics/g30734613/frankfort-kentucky-gun-owners-red-flag-law-protest-photos/?slide=20
More like Dallas-Fort Worth, or Atlanta. Lake Michigan at least creates one physical boundary delimiting ground travel.
Anyone been to Tokyo lately? Paris? London?
A couple of transmission observations:
The fecal route is interesting. Most public restrooms don’t have lids and modern water efficient toilets are designed to be energetic, so they send sprays up into the air where the little droplets can contaminate many surfaces in a bathroom. This should be a particularly efficient transmission route in airports.
https://www.today.com/home/it-necessary-close-toilet-lid-when-you-flush-t143776
People who travel to and from China generally will be on the wealthier side and are likely to be covered in a US healthcare system. If the virus gets into the US uninsured population, then it is much less likely that they will seek medical help quickly, which should also aid in transmission, especially in the US as many other developed countries will be much better prepared to address a population-wide challenge.
Finally, I predict an upsurge in Moscow Mule consumption which has both alcohol and copper (the cups) to prevent transmission.
“ Finally, I predict an upsurge in Moscow Mule consumption which has both alcohol and copper (the cups) to prevent transmission.”
That’s more like it!
the aerosolized fecal plume from ordinary toilets has been one of my peeves since i learned of it.
no lids, even in hospitals.
i’m also peeved by bathroom doors…fire code makes them open inward, so after washing yer paws, you must grab the door the unwashed paw just grabbed.
and there’s a lot of unwashed paws out there.
it’s safer in the woods.
The reason there is a trash bin next to the exit door is to deposit your hand washing paper towel, AFTER you’ve grabbed the handle and opened the door with it. I try and use my shoulder/elbow as much as possible when going through public entry.
> the little droplets
Then there are those stupid hot air dryers, instead of paper towels.
One of my workplaces has eliminated paper towels entirely for expensive hand dryers. You can see the water on the wall and floor underneath them.
And yes my first thought was I was going to have to start carrying a supply of napkins and towels in order to wash my hands there without possible recontamination from my current answer -air drying or wiping them on my pants.
But a TREE died so you could have germ-free digits, Lambert!!
sorry .. the Agony of St. Greta overtook me for a brief & terrible moment ..
IF it gets out of control here, I foresee a nationwide Super Dome after Katrina situation. Tent cities full of sick folks who are left to die and not allowed to leave. Chinese people getting gunned down for sneezing in Walmart. Every man for himself. Empty supermarket shelves. No sign of the brave police who will refuse to go to work / get out of their cruisers. Doctors taking a long vacation en masse. Gas shortages. Mass layoffs. Widespread starvation.
Don’t you?
Is your definition of “out of control” the rate of infection in China (virus spreading, knowing 14K is way lower than actual), or worse?
I think that number in every state ought to do it. What about you?
I think 8 across the country is making people worried. If this moves even into the hundreds, people will start to get scared But I’m not sure about complete mayhem and pandemonium. I was there on 9/11 and there is a calm and sense of cohesion that happens during calamities. But that was different than this.
I do think there will be a market crash and probably a global “something” (retraction, recession, not sure).
What’s the Chinese saying – may you live in interesting times? LOL. The next 2-4 weeks will be very interesting indeed.
This is going to last a lot more than 2-4 weeks given official reactions so far in non-China areas including Hong Kong and Singapore.
9-11 comparison is meaningless too. Beyond the general confusion of the first few days, it was clear it was an external enemy and Americans rallied against that. This is a completely different situation along with different mediums for information transmission and gathering.
Societal trust has gone way down since 2001 along with trust in almost every other institution in the U.S.
This is only one institution that has trust across almost all demographics- the U.S. military.
> Societal trust has gone way down since 2001 along with trust in almost every other institution in the U.S.
And as I keep saying, a valid approach is increasing social distance. So people become even more isolated.
The interesting times quote is great and I use it often but the closest it comes to being an ancient Chinese curse is the saying “better to be a dog in a time of peace than human in a time of war.”
https://quoteinvestigator.com/2015/12/18/live/
It isn’t officially ‘out of control’ yet if you use the Chinese Health Authority numbers but no one seems to believe the 14k ‘official’ number.
Highest estimates from sources I would deem as ‘semi-credible’ was over >150k cases and at least 10k deaths so far.
I’m sure the Chinese really don’t know an ‘official number’ given how large the dispersal was from Wuhan and how many people are holed up dying/dead at home right now due to quarantines on over 60M people.
My sister-in-law and her husband work in Hong Kong in senior roles and both of them were told this weekend to plan to work at home indefinitely starting today.
> My sister-in-law and her husband work in Hong Kong in senior roles and both of them were told this weekend to plan to work at home indefinitely starting today.
Good data, thanks.
Of course there will be problems, but people have an uncanny ability to come together during disasters.
This was written about in A PARADISE BUILT IN HELL, by Rebecca Solnit. She talks about different disasters and the lack of looting and other shenaningans.
No, I don’t. 10,000 people died of the flu in the US in 2019, and that didn’t happen.
Please do the math before making bogus comparisons. There is a reason people are being quarantined for the coronavirus when they aren’t for flus.
0.1% fatality rate for flu v. over 2% for coronavirus. Coronavirus is 20x more deadly.
And it has a high reproduction rate too, as in it is more infectious.
too soon to say for sure it is 2%. .4% was the calculation from that paper you referenced yesterday
https://medicalxpress.com/news/2020-01-wuhan-infected-coronavirus.html
I didn’t reference or link to a paper yesterday, so I have no idea what you are talking about.
And the overall estimate is irrelevant. That figure is an estimate of all infected, which includes the 14 day incubation period. The infection itself is also of comparatively long duration when it kicks in, with it become serious when it does (as in becoming viral pneumonia) at the end. You can’t compare that to deaths due to the fact that the infection level isn’t even close (# officially infected doubling roughly every 2 days) to stabilizing and the long gap between infections and deaths when they occur.
The death rate may prove to be lower as we get better data, as I have indicated, but hospitals in Hubei are so overloaded that pretty much everyone is being turned away, including the very sick. The opening of the new hospital will take the edge off that, but the public health system there still looks to be under siege.
Apologies. The link was in comments. The overall. Estimate is not at all irrelevant. On that you are mistaken it is one piece of the puzzle is all. .
How’s the Rapture Index today?
The Union of Atomic Scientists’ Doomsday Clock is down to counting in seconds, not minutes: https://thebulletin.org/doomsday-clock/current-time/
How many people can even tell the difference between a cold and flu? The pressure to go to work even when we have sick leave or vacation days can be intense. And the lack of information…. Does going to doctor help? What if a person gets stuck in an isolation ward for observation… who pays for that? Or do doctors send people home with a list of instructions? And if we have thousands being held in hospitals — Who pays. Will hospitals hold uninsured?
If people don’t have insurance when then they won’t go to the doctor if they think it is JUST a cold or flu. Even having insurance I had a couple of bronchitis events where I didn’t go to the doctor until I was crazy sick. Hardly able to draw a breath without horrific cough.
So what does #2019-nCoV do to us? Just thinking….
I guess I think a pandemic won’t go well here.
I was reading that Chinese men who were taking an ACE inhibitor were suffering fewer severe complications from CV. I can’t find the report though. Anyone know of this?
if one had to sit it out and basically not go out, what are the essential food items one would need?
If I thought i would have water and electricity, and if I thought the local pandemic would last 3-6 months, and if I thought my best option was to shelter in place, I would buy 50 lbs of dry beans, 50 lbs of dry brown rice, 25 boxes of frozen spinach, 10 boxes of oatmeal, 20 lbs of whole wheat flour, 20 yeast packets, 10 lbs of powdered milk, and some multivitamins. Roughly $200 at Aldi, btw.
I don’t think it’s time to panic, though.
Don’t forget the booze and edibles!
And batteries (and a solar charger). Because who really knows about the grid?
You forgot salt, cooking gas and toilet paper. Actually all sorts of stuff to go on such a list which would be more extensive than most people think.
Flutrackers.com has several forums to cover this exact question. This one is an excellent bet.
https://flutrackers.com/forum/forum/personal-family-professional-emergency-preparedness/ok-what-do-i-do-now
Rice, beans, spices !! dehydrated vegies to add to such .. moar spices ! Pasta .. and sauce, cheeses.
Stopped at Big Lots .. purchased what I like to call EastIndian MREs – single pouched curries & daals .. not bad !
Nuts – home roasted. Potatoes – mash em, fry them, put em in a stew … with a brace of Coneys .. or protein of your choice .. or by themselves – with spices added. Eggs. Alcohol of one’s choice – as, um, er, ‘mouthwash’.. gulp ! Chocolate(s)
Flours – with or without gluten.
Did I mention spices ??
LOL! “East Indian MREs.”
That and Ramen, the lunch of America’s student body. (I got a case of the cheap ones today.) Did we mention spices?
By coneys, I sense you are being “olde schoole” in referring to wild rabbits. (A headlight and a .22 do the job.)
I’ve got a couple of potato vines running across the back of the lot. (In the ‘wild’ part of the property.)
This topic was discussed in comments on today’s links, with links to scientific papers. It seems that Asians may be more susceptible to the virus than other populations due to some susceptibility having to do with ACE2 receptors, and that ACE2 inhibitors appears to mitigate this vulnerability.
Thank you. A comment by JeffC.
I didn’t see this report linked here yet:
https://www.nejm.org/doi/full/10.1056/NEJMoa2001191?query=featured_home
“[…] We report the first case of 2019-nCoV infection confirmed in the United States and describe the identification, diagnosis, clinical course, and management of the case, including the patient’s initial mild symptoms at presentation with progression to pneumonia on day 9 of illness. […]”
Being that this is only a single case, any conclusions drawn should be considered tentative at best. However, the information is still useful. My big take-away from this and other sources is that this coronavirus disease may be like a common cold on steroids. In fact, it may be symptomatically indistinguishable from a cold until it enters its more severe phase where it turns into a nasty pneumonia. The pneumonia may occur many days after initial symptoms appear, so many suffers may assume they merely have a cold until it takes a turn for the worse, right about the time they expect to be feeling better.
If you ask me, this is close to a worst case scenario for a pandemic disease. Not only are the periods of incubation and asymptomatic transmission likely long, but the early symptoms may not be distinctive enough for people to stay home from work, much less admit themselves to a hospital where they might get tested and quarantined.
Also, I want to note that so far it seems that the people who actually need hospitalization for the disease need mechanical ventilation, and this is a highly specialized resource that’s in much shorter supply than mere hospital beds. Even a relatively contained outbreak, could cripple the ICU services in any affected city. This has the potential to directly and severely impact essentially everyone except a handful of elites with exclusive concierge service, whose price may be about to go up a lot. Maybe all those bunkers in New Zealand will be seeing some warm bodies soon?
Your scenario is just about my worst fear. Depending on how many cases advance to pneumonia, it could be really really bad. And with so many people under and uninsured, how do some of them get treatment?
Well if the pandemic cannot be contained and the rate of life-treathening symptoms is high, then critical resources will run out and people will be turned away whether or not they have insurance. Likewise, if you get into a car wreck and the ICUs are full, you might be turned away. It affects the whole system systemically.
Piling on the worry, a global health crisis like this could overwhelm the supply chains for major medical supply staples like antibiotics to treat secondary infections or even seemingly mundane things like disposable syringes and IV bags of saline. I can confirm that the latter are already in extremely short supply, and a pandemic will almost surely cause major shortages. This likely occurred due to a combination of industry consolidation; premature optimization of the supply-chains (just-in-time and “right-sizing” of production capacity); unanticipated recent damage to factories and/or store houses many of which resided in Puerto Rico; and (perhaps) the opportunity noticed by other companies to use PR as an excuse to hoard inventory and jack prices up. Funny that. Maybe we won’t technically “run out” of IV solutions bags, we’ll just get to a point when their too expensive to use on “normal” patients.
While I’m on it: anyone see the last Dem debate where CNN gave Warren the opportunity to promote her idea for government owned pharmaceutical manufacturing? She could have made a hard sell, on the basis of “National Security” (!!!) if nothing else, but instead she withered away and pivoted. What a missed opportunity for her and the Dem party!
Hindsight is 2020 might be the joke of the year because it almost seems like all of society’s past sins and debts are coming due all at once.
The medical logistics lines originate in China and the Chinese are “working from home” … Hm!?
The Dim party’s opportunity lies in engineering a loss to Donald Trump – there will be more donations coming in that way and that’s what the political consultants care about.
> I didn’t see this report linked here yet:
Links, three days ago.
New Zealand has just banned flights from China and if a world-wide pandemic develops may ban flights from anywhere, so your bunker could easily be inaccessible.
“I wouldn’t classify face masks as virtue signaling, exactly”. Agree, but here’s a link to how to properly put on and test a face mask that may add protection:
https://www.cdc.gov/niosh/docs/2010-133/pdfs/2010-133.pdf
Note, N95 masks are also useful for those of us in wildfire prone areas, as they protect against smoke.
Also, for exposed eyes there are several options, wrap around glasses or sunglasses, paintball protection plastic glasses, swimmer goggles, ski goggles, etc.
All the above will increase survival odds if it comes to that. Lets hope we never need to use them.
The count is up to 17,295 cases now. The rate of increase is rising. Possibly due to the deployment of more rapid diagnostic kits.
One gets the impression that there might be a backlog of undiagnosed cases in Hubei province, so the daily changes are hard to interpret. But the jump between 1/30-1/31 and 1/31-2/1 is certainly not encouraging.
The thought occurs that there may not be a lot of spare medical capacity in a US for-profit health-care system that is “right-sized” for maximal RoI from the facilities in each locality.
I wonder what the Cabinet is doing to prepare?
Oh, right:
https://foreignpolicy.com/2020/01/31/coronavirus-china-trump-united-states-public-health-emergency-response/
Lambert mentions a $22 billion injection into Chinese markets. Looks like the Chinese decided to go big and are now injecting $173 billion into the economy to boost liquidity and stabilize the currency-
https://www.asiatimes.com/2020/02/article/virus-toll-over-300-as-china-to-inject-173-bln-into-economy/
A lot of countries like Australia are going to be hit hard by the lack of Chinese tourists spending their money here. If Coronavirus cuts loose, a lot of countries and places dependent on tourism will be hit hard.
PS I keep on seeing references to some sort of football game going on right now. Something about a supper bowl? Maybe Campbells sponsors them.
NZ logging crews have been sent home (presumably without any compensation as they’re all contractors and sub-sub-subcontractors) https://www.stuff.co.nz/national/119236860/coronavirus-strikes-logging-crews-across-new-zealand
Interesting because it’s not directly virus related, rather economic impacts downstream.
Looks very much like it might be to do with export problems more than it is the virus in NZ – because there aren’t any confirmed cases of the virus in NZ. Unless there’s a huge number of Chinese subbies that haven’t been able to get back to work, but that seems unlikely (Filipinos and islanders are way cheaper and easier). Also possible that a link in the domestic supply chain for logging is owned by China and has been affected, given their buy-in across NZ industry over the last decade.
China is the major export destination for nz logging – 48% of export value in 2018 ( https://www.teururakau.govt.nz/news-and-resources/open-data-and-forecasting/forestry/wood-product-markets/ ).
The quote from the industry body is suspect –
I keep wavering on how to put this in prospective. On the one hand, world-wide, there are 3,000 deaths EVERY DAY (1.25 million per year) due to traffic accidents — which rates a big fat so wach-a-gonn-a-do?; on the other hand, if 60% of the US caught it, 2% deaths would be 4.5 million — that’s not good.
So then maybe it’s not so much the deaths as all the knock-on and overload that happens to the medical and economic systems. The only reason the rate of death is currently 2% is that so many people are getting ICU-like treatment; otherwise deaths would be higher (alongside the 360 deaths, there was also something like 100+ in critical condition and another 100+ in serious condition)… and since nobody’s hospital systems can take on a big ICU load, I guess it’s in all our best interest to keep the transmission low, regardless of the actual, current death rate.
Exactly. Could we do any better? It seems to me that there are large advantages and large disadvantages that accompany a hierarchical, centralized system when it comes to dealing with pandemics.
I seem to remember large tents set up in California a few years ago to deal with a simple seasonal influenza epidemic. China built two large, reasonably-equipped hospitals in less than two weeks. They brought in their military medical personnel to help, who were in China and available. Our military medical personnel are spread out over 800 overseas bases.
Our seasonal flu has a death rate of 0.1%. The death rate of the novel coronavirus is unknown, but it’s currently estimated at 2%. That’s 20 times greater than our seasonal flu. If it is as contagious, and some think it is, we can imagine 20 times the number of deaths that we currently see during influenza epidemics.
What are our plans? What are we going to do with our massive homeless populations in the middle of our most densely populated cities? These are people who can’t be quarantined at home, who have no toilets or other sanitation facilities, and whose contacts can’t be easily traced. They could be a significant obstacle to containing an epidemic and, of course, in dire danger themselves.
China has to deal with a population density 4 times our own. Yet when they have instituted tough population control measures, we mercilessly attacked them for “human rights violations”. How would we manage an epidemic if we had 4 times the density of people; 4 times the number of homeless?
We should be supporting China in their efforts and giving encouragement and showing sympathy. I don’t see enough of that right now.
1. The US evacuated Americans earlier than many other nations. Russia just did so 1 or 2 days ago.
2. I haven’t read about it, but did Beijing order moving the sick to other provinces to be cared for, if stories of people waiting days to be examined are correct. Is that an option?
3. Did Beijing move some patients to military hospitals around China,?
4. 2 hospitals in Wuhan. I read of the need for ventilation machines. Is this the bottleneck, more than hospitals?
5. The mayor of Wuhan. His Wikipedia page seems to show his rise through being appointed, a series of them,, and not through being elected. How does this affect his performance, as far as responding to people of Wuhan is concerned?
6. There are stories of people angry at the city of Wuhan, and higher up. People might have criticized human rights, but can still be supportive in this case (while thinking critically about what has gone wrong, and what other countries like Japan, North Korea, the US, Russia, etc, would do).
7. Looking at List Of Epidemics at Wikipedia, for the 20th century, most originated not from the US/Europe. In the last 2 decades, there were 2 major ones from China. Is it just bad luck? People in China would naturally demand more of Beijing, as their personal well being is paramount, will ask questions.
8. If responding early, and reporting widely is important in cases like this, I believe that is something the US can address today. Maybe it is how Beijing works or maybe it is a lesson right there staring at us, I feel the US will do a better job in this area.
> What are we going to do with our massive homeless populations in the middle of our most densely populated cities? These are people who can’t be quarantined at home, who have no toilets or other sanitation facilities, and whose contacts can’t be easily traced. They could be a significant obstacle to containing an epidemic and, of course, in dire danger themselves.
Presumably what we’re already doing, but worse. Since what we’re already doing isn’t working, doubling down on it won’t help. One wonders also if there are synergies (I’m sure there’s a medical word for this but I don’t know what it is) between diseases already present among the homeless, and #2019-nCoV.
Saying that there could be a significant obstacle is almost like saying that the Sun might rise in the East tomorrow. Don’t forget all those people living in their vehicles. Just how would they be found, stopped, quarantined, questioned, and hopefully treated?
People were wondering what was the point of Trump’s ‘landmines are OK now’ thing.
Well, now we know.
I just noticed that Yves had made the same observation in an earlier comment — we’re looking at a death rate 20 times higher than our seasonal influenza.
Another way to look at this is to look at the influenza deaths during the 1918 influenza pandemic, which also had an estimated death rate of roughly 2%. Again, if the novel coronavirus is equally contagious, as some think it might be, the potential is scary. It’s estimated that 675,000 died in the United States from the 1918 flu. The population in the United States in 1918 was 103,208,000. If you scale that up to today’s population, we could be looking at over 2 million deaths in the United States from a novel coronavirus pandemic.
Here’s another useful tracker.
https://wuflu.live/
No idea of the genetics involved but apparently some Thai (and Chinese) doctors have been sucessfully treating it with flu and HIV medications:
https://www.businessinsider.com/coronavirus-treatment-cocktail-of-flu-hiv-drugs-2020-2
Reviewing the evidence for & against origin theories.
https://jameslyonsweiler.com/2020/01/30/on-the-origins-of-the-2019-ncov-virus-wuhan-china/
It looks like five attempts with pricey drugs. Notice of the group of three, they say “the patient”. One of that three looks to have had a dramatic improvement. The others appear to fall into mere “improved the condition”.
Of the other two, one had an allergic reaction and the other “showed improvement”.
Weiler is still CT, despite the camouflage of the neutral-sounding headline. The bioweapon meme is a pile of crap.
Fern, those are excellent questions as to how the U.S. would deal with thousands of people who contracted the novel coronavirus – honestly, I don’t think we’re anywhere near prepared for something like this. As you say, the massive amount of homeless people presents numerous medical/logistical issues – I don’t know how we would manage an epidemic like China is.
I have two questions regarding the virus (maybe some virologists or doctors would know this) – would the pneumonia vaccine given provide any protection? Since this is a virus, antibiotics won’t work against the virus, but if pneumonia develops would they be of any benefit? I have read that anti-virals are given, but what is the main type of treatment?
“would the pneumonia vaccine given provide any protection?”
No. It’s for a bacterial pneumonia.
“but if pneumonia develops would they be of any benefit?”
Only if it’s pneumococcus.
I have read that anti-virals are given, but what is the main type of treatment?
There is no treatment, now they are probably trying antivirals, and perhaps some of them work – but it’s hard to say without a double-blind study. What specific drug they are trying, I do not know.
https://www.cdc.gov/coronavirus/2019-ncov/hcp/clinical-guidance-management-patients.html
The pneumococcus vaccine may give some protection because it helps prevent secondary bacteria infections which are relatively common with the flu. However, it appears that the Wuhan virus can cause pneumonia directly from its own actions in the lungs, as well as helping trigger secondary bacterial infections. So the pneumococcus vaccine won’t be a panacea although it could very well help. http://theconversation.com/how-does-the-wuhan-coronavirus-cause-severe-illness-130864
The use of the pneumocccus vaccines over the past 20+ years appears to have reduced the incidence of pneumonia in general as there is beginning to be a herd immunity due to the number infants and seniors that have been given it. I got the PCV7 version in the late 90s after a nasty pneumonia triggered by a common cold or flu and it has largely eliminated my previously chronic sinus infections (same bug) as well as not having a pneumonia recurrence.
https://www.cdc.gov/vaccines/vpd/pneumo/public/index.html
Speaking as an MD: flu vaccine and pneumonia vaccine [eg Pneumovax 23] each contribute quite a lot to reducing your risk of having these largely preventable diseases superimposed on your pre-existing condition or on something like 2019-nCoV. You should for sure get both vaccines anyway, and in the current situation you should get moving on it right away.
Brass/copper are excellent antibiotics. I don’t think it was because that they were used in knobs and similar for centuries (since it was well before even microbes were discovered), but it does work a treat. Unlike the shiny stainless steel so belowed by modern architects which is a perfect surface for the viruses to last for long.. When I tried to get (becasue of the antibiotics properties) door/window handles few years back, I shot blank unless I wanted to scavenge some old ones which would not fit very well..
Anyways, on something different. The French evacuation plane that landed in France today had on board ~250 evacuees. Of which 36 had symptoms. Of course, no idea whether they were all (or even any) coronovirus infected, but that’s 10% of people who would most likely be trying pretty hard to avoid hazards and so in the last 10+ days. If even 20 of them are infected, it would suggest that the real infection rate in China is WAY more higher than even 10 times the official reported.
Also, there’s a story out (for example here https://qz.com/1793764/china-court-says-wuhan-coronavirus-rumors-might-have-helped/) that the initial reports of the ilnesses were supressed by the anti-rumour laws.
There is a video circulating widely on wechat from a bus in Wuhan showing a number of security officers arguing fiercely with an old lady who refuses to put on a mask. One even tries to give her money to buy one and she indignantly refuses.
The thing about the video is that all the security men and most of the passengers are not wearing gloves despite the cold weather. And of course the cash being pressed on the lady is a possible vector. I keep telling my Chinese friends that masks are of minimal use outside of a hospital environment – they are essentially a form of virtue signalling – the real risk is in hand contact via any hard metal surface. But that message just doesn’t seem to be going out in China.
Nasal infrastructure (did I just write this?) is amazingly adept at dealing with various stuff trying to infect us – assuming you have it functioning, and actually using (a lot of people I know breathes with their mouth even most of the time..).
Hand-to-mouth, or even worse, hand-to-eye, are on the other hand (no pun intended) pretty good infection vectors, both ways. The only good thing there is that hand skin is actually pretty bad for viruses (IIRC, the lifespan there is minutes), but still we use our hands a lot.