By Lambert Strether of Corrente.
My yellow waders got all yucky and corroded when I covered Hillary Clinton’s lunch with the FT back in June, and the repair guy is still coping with the damage. So I will not be able to give the Biden Administration’s latest “Fact Sheet” on BA.5 the full attention it so richly deserves. In policy terms, the “Fact Sheet” is not materially different from the Administrations “National COVID-19 Preparedness Plan” of March 2, with the exception of a focus on “equity,” a word that does not appear in the “Fact Sheet”, presumably because it has been achieved. There’s more specific content on both masks and ventilation in the “Fact Sheet” that in the “Prepareness Plan,” which would be a good thing were the content not wholly inadequate, not to say lethal if you follow the advice. (I can’t see that the White House Office of Science and Technology, which is good on both topics, had any input whatever, which would — hold onto your hats, here, folks — support the idea that the “Fact Sheet” is a mere public relations strategy.)
Reaction to the “Fact Sheet” has been extremely muted, not to say stifled. WaPo’s headline — “Biden officials urge use of booster shots, antivirals against BA.5” — suggests that the “vax and relax” mindset is still fully entrenched in WaPo’s readership, although the story is somewhat less limited:
White House coronavirus coordinator Ashish Jha said the administration’s strategy to manage BA.5 relies on vaccination, antiviral treatments, testing, masking and improved indoor ventilation, measures that have worked to keep people out of the hospital and from dying.
(Note the abandonment of the goal of controlling infection, to which we shall return.)
The Washington Times coverage — “White House COVID coordinator: Country can weather new BA.5 variant just fine” — is similar:
The Biden administration said the fast-moving BA.5 variant of the coronavirus is a stark but manageable challenge, unveiling a plan that relies on frequent testing, antiviral drugs and up-to-date vaccinations while stopping short of an immediate expansion of the booster campaign as drugmakers reformulate their shots.
Similar except, like the Guardian‘s coverage but not WaPo’s they leave out masking and ventilation altogether.
In this post, I’ll skip over the vaccination and booster controversies, and focus on the Biden Administration’s strategic goals, and also on masks and ventilation. I’m doing this for two reasons. First, I’m committed to policy of layered protection (“Swiss Cheese Model“), which I think would both subsume Biden’s vax-first policy and be more effective in preventing airborne transmission, especially given that the operational definition of Biden’s “Preparedness Plan” has turned out to be “Let ‘Er Rip,” turning the United States into a global reservoir for SARS-CoV-2 infection. Second, I believe that the Biden Administration’s guidance on both masking and ventilation is lethal, or to put matters more politely, won’t save as many lives as it could. (The “Fact Sheet” relies heavily on CDC content, so I’ll have to stumble into that gruesome morass as well, for which I apologize in advance.)
Let us now turn to “Fact Sheet: Biden Administration Outlines Strategy to Manage BA.5,” annotating passages in our usual way.
“Fact Sheet” Strategy: “Today, the White House COVID-19 Team is announcing its strategy to manage[1] BA.5. The strategy relies on ensuring that Americans continue to have easy and convenient access to the vaccines, treatments, tests, and other tools that protect against and treat[2] COVID-19. These tools – even in the face of BA.5 – work to prevent serious illness, keep people out of the hospital, and save lives – and we can prevent nearly all COVID-19 deaths with them[3].
[1] “Manage” how, exactly? Ed Yong asks the key question:
This is what “living with COVID” means—a continual cat-and-mouse game that we can choose to play seriously or repeatedly forfeit. The stakes of that game depend on a very simple question: Should we still care about preventing infections? If the answer is ‘not so much,’ which is the implicit and sometimes explicit posture that America’s leaders have adopted, then BA.5 changes little. But if the answer is ‘yes,’ as I and most of the experts I talk to still believe, then BA.5 is a problem.
In what follows, we’ll see that preventing infections is not a goal of the Administration. The metrics they “manage” by show this clearly.
[2] Notice the slipperiness between “protect against and treat” vs. “work to prevent serious illness” vs. “prevent nearly all COVID-19 deaths.” I think that, given the Biden administrations peformance on Omicron (record spike) and BA.5 (a guesstimated record spike, though CDC has butchered the case counts, so it’s hard to tell) plus the fact that the vaccines are not sterilizing and reinfection is frequent makes a claim to “protect against” weak, and the Administration is wise to slide away from it in the text that follows.
[3] As we see, the only metrics that matter are hospitalizations and (“from Covid”) deaths, and not infection. Long Covid, vascular damage, and neurological damage, all of which can come from “mild” infections, are not a metric that the Administration watches for.
“Fact Sheet” Mobilization: To confront BA.5, the Administration will continue mobilizing the full strength and capabilities of the federal government[1] and working with state and local leaders, health care workers, the private sector, and community- and faith-based organizations to ensure that the American people have easy and convenient access to and use vaccines, tests, and treatments[1].
[1] Well, maybe. Here’s a simple test you can apply yourself in the coming weeks. As readers surely know, the President’s time is the most valuable asset of any Administration. You would, therefore, expect to see “the full strength and capabilities of the federal government” embodied in the President’s presence, speaking to the issue. Now, Biden is a busy guy when not napping, so that’s probably too high a bar for this Administration. But what about President-In-Waiting Harris? Here is Harris’s schedule for the year from the Los Angeles Times:

Harris is obviously spending hardly any time on Covid at all (even when Omicron was peaking). If the Administration committed to the “full strength” bit, her schedule will fill right up with BA.5 events. However, this seems unlikely; if it were, Jill Biden would already be on it. I can’t find her schedule, but last I heard she was trying to salvage the Democrat midterms by appealing to the Hispanic Latinx vote. Of course, we can hope, but this doesn’t seem likely.
[2] “Vaccines, tests, and treatments” again shows that preventing infection does not matter to the Administration.
“Fact Sheet” Masking: Experts agree that masking in indoor, public spaces is an important tool to control the spread[1] of COVID-19. The CDC’s COVID-19 Community Levels provide individuals with clear recommendations[2] on when to consider masking in indoor, public spaces[3]. As BA.5 drives an increase in cases, the Administration continues to encourage Americans to visit COVID.gov to find the level of COVID-19 in their community and follow CDC’s recommendations on wearing masks in public, indoor settings[4].
[1] With “control the spread,” we finally get, conceptually, to transmission. However, the Administration doesn’t recommend a metric for transmission, unlike deaths and hospitalization (“You can’t manage what you don’t measure”), so the Fact Sheet’s remarks on masking are purely performative. (But don’t get me wrong: They’ll be “fighting for” them!)
[2] The CDC’s “Community Levels” metric — which has grown all over everything like kudzu — is indeed clear. It’s also wrong, and lethally so. See note [4] below.
[3] Private spaces are important too. Anecdotally — some of the best data we have, given the givens — there are many cases of households where one member became infected, but when the household adopted a layered strategy including masking, but also isolation of the infected, ventilation, and Corsi boxes, no other members were infected.
[4] Here, the Administration is recommending CDC’s Community Levels metric. Community Levels combines a leading indicator (cases) with a lagging one (hospitalization). The lag between infection and hospitalization can be as much as two weeks. Therefore, by the time Community Levels kicks in, infection in the community could already be high (important given that Covid exhibits doubling behavior. The CDC does have a map of transmission only (and explictly discourages dull normals like you from using it). That map has been solid red (dangerous) for a long, long time. However, CDC’s Community levels map, gamed as it is, has been green (safe) also for a long, long time. Eric Topol described CDC’s game-playing with metrics back in May, 2022:
[INTERVIEWER: ] But you look at the CDC’s [Community Levels] map, it shows the country where there’s a few hot spots, the orange up in New York and some yellow up in Minnesota and Michigan, but the rest of the country looks green, as if it — there isn’t a problem with this virus. What is the disconnect there?
[TOPOL: ] Well, I have called it a capitulation.
That is, the CDC is — frankly, it’s a deception, that the level of the virus is low, when the transmission is incredibly high. I mean, it’s starting to approach that of what we saw with the Omicron wave. And it’s continued — it’s rising quickly.
So this is really irresponsible of the CDC to give us this impression that things are copacetic, when they couldn’t be — that couldn’t be further from the truth.
In other words, if you follow the CDC’s Community Levels metric, you could be masking up two weeks too late. Don’t use it. Use the map of transmission only, the one that shows the real danger to you (scroll down to the red map with the “Community Transmission” dropdowns for Data Type and Map Metric. Ignore the CDC’s hectoring, immediately above the map, that “Community Transmission levels are provided for healthcare facility use only.”
“Fact Sheet” the Immunocompromised: The Administration has initiated a communications campaign to ensure that immunocompromised individuals and their close contacts are up to date with COVID-19 vaccination and boosters[1].
[1] Once again, anecdotes are what we have, but from what I hear, what the immunocompromised want most and don’t have is universal masking, so they can go out into the world like normal people and not worry about sharing air with the infected. (Yes, universal masking is safer than “one-way” masking.)
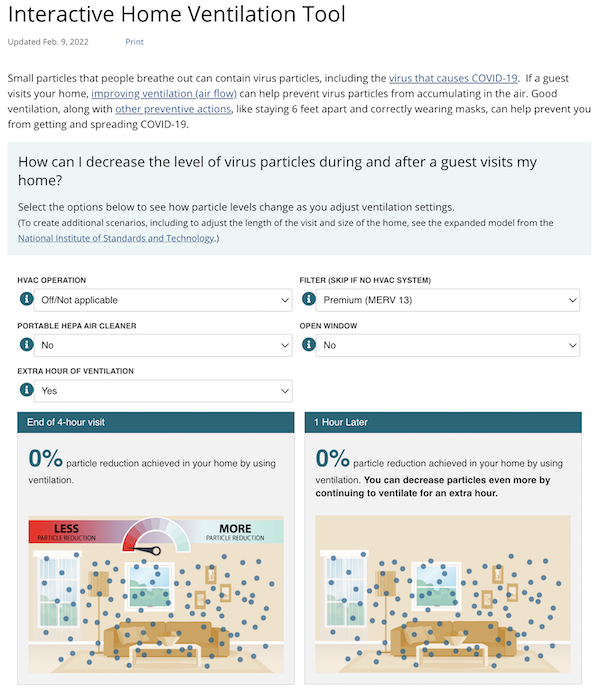
“Fact Sheet” Ventilation: Improving ventilation can[1] help prevent the spread of BA.4 and BA.5 indoors in buildings. The Administration has provided state and local leaders hundreds of billions of dollars in federal funds that can be used in schools, public buildings, and other settings to improve indoor air quality, and the Administration will continue to advance indoor air quality in buildings, including by increasing public awareness around ventilation and filtration improvements to reduce disease spread[2], as well as by recognizing buildings and organizations that have taken steps to improve indoor air quality. These efforts will expand on the Administration’s “best practices” guide for improving indoor air quality and reducing the risk of spreading dangerous airborne particles and the Clean Air in Buildings Challenge, which calls on all building owners and operators, schools, colleges and universities, and organizations of all kinds to adopt key strategies to improve indoor air quality in their buildings and reduce the spread of COVID-19. Additionally, CDC has released interactive tools to help individuals at home[3], in schools[4], and in other buildings to understand how air flows in their space and what they can do to help shore up air quality and improve ventilation indoors.”[5]
[1] I have helpfully underlined the Administration verbiage that indicates this is all voluntary, and there will be no demands for compliance with any sort of regulation (dread word).
[2] Here again we have a nod to tranmission, but with no metric and no enforcement, the Fact Sheet is merely performative.
[3] Naturally, the “Fact Sheet” doesn’t actually link to the interactive tools, but I think this is the guidance for homes:
I’ve got to assume that this is a tool, and not some kind of children’s toy (although the drawing style, especially the color palette, argues for the latter. The softness is designed to make it appear harmless, which it isn’t.) A good tool would take into account: The size of the room, the number of guests, and the duration of stay. Measures would include opening doors (not just windows ffs), turning on bathroom and kitchen fans, buying a box- or window- fan to really move the air, and Corsi-Rosenthal boxes as an alternative to portable air-cleaners (“DIY alternatives using single 1”, 2” and 4” MERV 13/14 filters compare favorably to commercially available systems in terms of estimated CADR and dBA but at five to ten times lower cost.”) Readers will doubtless have additional measures.
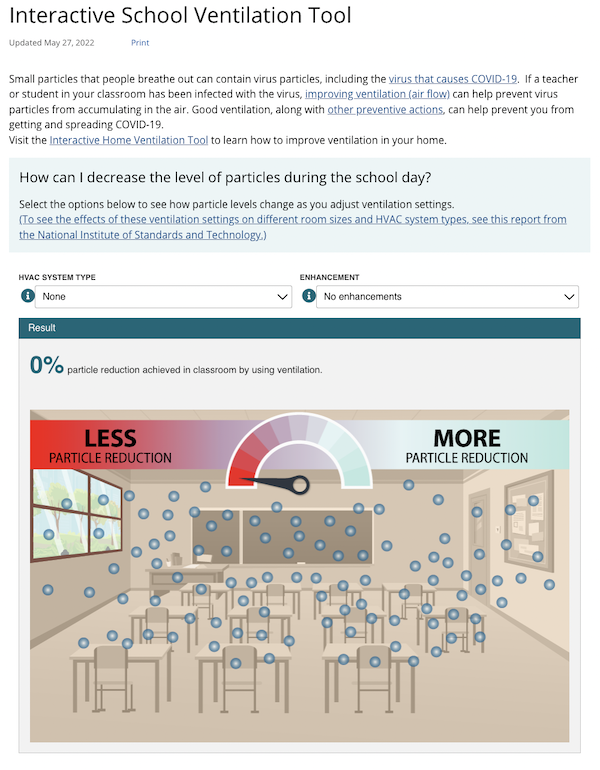
[4] The tool for schools is worse:
A good tool would take into account: The size of the classoom, the number of students, and the duration of class. Incredibly, CDC’s tool doesn’t mention opening windows or doors. Not incredibly, but even more lethally, they don’t mention Corsi-Rosenthal boxes, or even portable air cleaners. Finally, they don’t mention using CO2 meters as a proxy for shared air in the room, so parents could determine how much danger of infection their children were actually in.
[5] Throughout, although most obviously with the omission of CO2 meters, we see the Biden Administration’s wilful and crass evasion of measuring transmission.
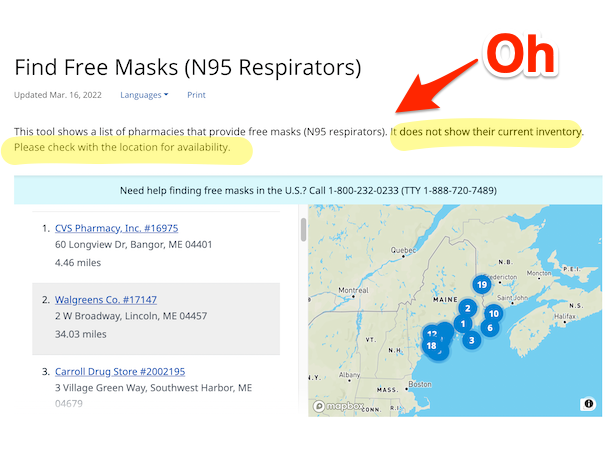
“Fact Sheet” Covid.gov: Earlier this year, the Biden Administration launched COVID.gov, a new one-stop shop website[1] to help Americans find where to access lifesaving tools like vaccines, tests, treatments, and masks[2]. People can also type in their county to find the latest updates on the level of COVID-19 in their community[3] and related guidance[4]. And, with a click of a button, people can access resources related to testing, ventilation, and other important COVID-19 topics.
[1] The site is not at all “one-stop.” In fact, it’s a thin layer of quasi-friendly redirections, primarily to the gruesome tangled mass that is the CDC’s website, but also to other sites.
[2] Here is the Covid.gov on masks:
Let’s just say this isn’t as helpful as it could be.
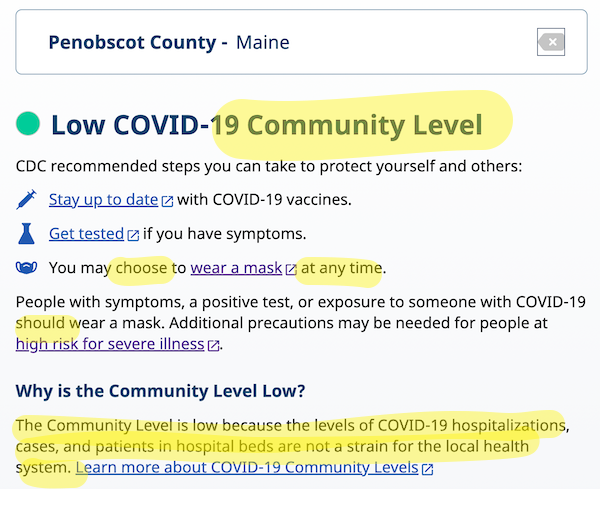
[3] By “level of COVID-19 in their community” the Administration means CDC’s “Community Level” metric, which Eric Topol (see above) rightly calls a “capitulation” and a “deception”:
Note the highlighted material at the bottom: “The Community Level is low because the levels of hospitalizations, cases, and patients in hospitlals are not a strain on the local health system.” In other words, transmission as such is not a relevant metric. If CDC were organizing a campaign against drunk driving, they’d be telling people it was OK to drive drunk when the ERs aren’t full.
[4] I tried travel:
What I would really like to know is whether my airports (leaving and arriving) are in “Rapid Riser” counties, because the air travel is one ginormous superspreading event, and so airports (as we saw in Manhattan in Spring 2020) are often epicenters of transmission spikes. (Therefore, a seven-day transmission average is not enough; I really want “rapid riser”). Unfortunately, CDC now only delivers “Rapid Riser” data twice a week, which is not fast enough, given the doubling behavior of the virus. Ah well, nevertheless.
Conclusion
What we see in the “Fact Sheet” is a willful refusal to create metrics or regulation for masking and ventilation, or for transmission generally. I can only conclude that the following meme (sorry) describes not only the policy of the Biden Administration but the future course of the disease:
Wave after wave after wave after wave after wave after wave after wave.
The Biden COVID plan. pic.twitter.com/Dj4TFiIEm5
— sachapie (💉➕ since March 2020) (@sachapie) June 15, 2022
Let ‘er rip!


It’s obvious that the globalists controlling Biden/Harris embarassment, and those bought out by Chinese money
want new pandemics for megaprofits, societal control and political advantage.
Occam’s Razor.
Why would ‘Chinese money’ be seeking new pandemics for any purpose? I trust you can provide some evidence to support the claim. That the globalists should seek new pandemics “for megaprofits, societal control and political advantage” is simply Neoliberalism 101 and thus axiomatic. Where and when has China pursued such a policy?
And slow stealthy mass murder. In fact the mass murder objective is the most important objective and maintaining some threadbare shred of plausible deniability for the fact that engineering the mass murder through the very careful fostering and acceleration of pandemics is the second most important objective.
After all, the rulers don’t want a critical tipping-point massload of people suddenly realizing the carefully engineered and fostered nature of the accelerationist response for fear of that tipping point massload of people rising up and seeking to physically exterminate every member of the rulership and enforcement-ship cadres.
Eggzactly – keepin’ the eugenics lowkey.
Yes, as clearly evidenced by the US ruling class (‘globalists’) having spent the last two years downplaying and minimizing the pandemic while doing the absolute bare minimum required to maintain a hair-above-failed-state-level of social and economic function. If this is the “plandemic,” I’d hate to see what “denialism” looks like!
I’m also sure the Chinese have been just ecstatic about being forced to act as the sole counterweight to US empire’s ‘global superspreader’ model, openly deployed for years to batter the PRC with an endless wave of cases from abroad. Get real.
Where’s the evidence for that? Not that I think it’s beyond the realm of possibility. I could say something hypothetical, but I want to make clear it’s hypothetical (because the reality is impossible to know right now). Even if the lab had really been a spy vs spy thing, there had to have been the appearance of cooperation on the surface. Which, if you look at where we are now, it’s almost beyond belief this “appearance” was so recent (probably one thing they don’t want us to ponder much). I take Yves’ point about the original problem causer being “wild,” mostly wild AFAICS but maybe passaged some? On purpose or not on purpose.
With regard to “dual use,” in Jacques Ellul’s technique world technique allows no real oversight. And it could be both PsTB thought it was just the trend to stack up weapons on the shelf (in the frig). And didn’t really look into the matter much! With really no serious plan to use them. I mean, who really thought they could conquer the world with F-35s? Defense contracts just multiply on their own. Like viruses, which some claim are not alive.
Well, part of looking into the matter is looking into how the bug moves, or (right now) how BA.5 variants could move. So I appreciate Lambert Strether helping us with this.
Perhaps US government is reluctant to implement more effective methods to control contagion out of fear of stimulating Russia to do the same. IOW, perhaps they hope that the CV reinfections and progressive debilitation of the population through multiple Long COVID sequelae will ravage Russia even worse than it does the US.
Perhaps the Rules-Based International Order can yet prevail, provided that the CV rules at home are not too effective.
I’ve been trying to persuade an older friend to keep using the N95s I previously provided. She is bombarded with contrary counsel from every direction. The medical facility staff she deals with periodically are using only the blue procedure masks, which she knows are ineffective — how dangerous can the situation be if medical people aren’t concerned?
I hope civilization lasts long enough for future historians to study this period and pass judgment on our rulers.
Looks like it’s more of the same old same old.
Me? I have a scrip for two meds that must not ever be mentioned* in polite company. It’s in the “just in case” part of my medicine cabinet.
I’m also doing a wide variety of things to strengthen my health and immunity. If you have an hour or two, I’ll tell you about them.
—–
*One of those meds begins with the letter “I” and has been widely reviled as horse paste. The other begins with “H” and was endorsed by a certain former POTUS who is orange and bad, very bad indeed.
> It’s in the “just in case” part of my medicine cabinet.
People with more knowledge of the chemistry might provide better counsel, but I wonder whether it might be better to refrigerate or freeze your stockpile of these meds. They probably have a shelf-life that could be extended at lower temperature, and one does not know what the regulatory regime will be in future (not to mention the state of supply chains) if they were past best-by date and one wanted to replenish them.
On the box it says “store in a cool, dry place (dark) under the temp of 30° C (86° F).
Slim, just a heads up. I don’t know if this is something new (for reasons) or a random thing. I, like you, stock the drug that cannot be named. I have bought 3 times from the same supplier (who has been great to deal with) who is overseas. Not an issue ever, but always got a notice from my credit card bank that there was an international purchase to my account. If you dispute this, please call customer service.
Last week I made another purchase. It was blocked by my bank. I got an e-mail from the supplier telling me I needed to authorize the payment. Never happened before. I could not find a way to do so on the banks website, even though I had an alert telling me there was “suspicious” activity, so there was no way to authorize it.
In the meantime, I got a text on my phone (nothing in my account) asking if I wanted to authorize this charge – yes – of course! Still nothing happened on the banks end.
To make a long (about 4 hours between two days) maddening story short, after talking to two different people (both seemed like they didn’t live in the US (accent was telling)) they told me to call the fraud dept. I did, they saw the charge, said it wasn’t blocked, but they couldn’t authorize it, I needed to call customer service (who I just hung up with). So another day, another 2 hours and finally, a guy who spoke good English fixed me up, and the payment finally went though.
I asked him why this happened when the last times it went right through? He didn’t have any idea, and said “sometimes this just happens.” OK, I guess it can just happen, but the cynic in me says different. This is a well known regional bank. I’m sure I’m not the only person doing this, and I’m sure they know what’s going on behind the order.
Maybe an anomaly, maybe not. I don’t trust any of them. And for the record, I have heard some shipments are being confiscated at customs by other buyers who do the same. We’ll see in a few weeks.
> I’m sure I’m not the only person doing this, and I’m sure they know what’s going on behind the order.
I guess that means it works, because Big Pharma wouldn’t be worried about it if it didn’t.
I’m a test dummy and so far, so good. I’ve been around all kinds of people who have gotten it. Closed classroom, no ventilation, students almost weekly missing because of COVID.
Just Monday, I talked to a buddy (fully vaxxed) who just spent 10 days in quarantine because he tested positive (and his wife (fully vaxxed) who he thinks got it from him). I asked him where he got it? Probably right here, which is a bar restaurant we both go to. Or at the golf course. I was at both at the same time as him.
He said he had a bad cough for 4 days.
I also do Vit-D, and have the iodine mixture Yves has spoken about here. I use that when I come home after being in a indoor place I think wasn’t ventilated very well.
> I also do Vit-D, and have the iodine mixture
Another way of saying “Swiss Cheese Model” is “more is more.” I strongly believe this…
Bleach begins with “B”. :)
> Bleach
If that’s a Trump reference, you do realize Pelosi faked it?
These days it’s difficult to determine what is genuine and what is fake. I was joking about bleach anyway. Public health has been abysmal in this country from the very beginning. We are all on our own, so I say try whatever you think will work for you. Best wishes to us all as this pandemic grinds on.
Minnesota Dept of Health completely stopped reporting case counts a few weeks ago, replaced by a link to the bafflingly useless CDC community spread charts. Capitulation is here, seems like the plan is to pretend it doesn’t exist until after the election. I keep an eye on the local biobot results, though it seems likely there will be another big surge when schools start again.
They did indeed successfully obscure their reporting to an astounding degree. To my knowledge, the closest they currently have to case count reports is now the Cases Over Time (7-Day Moving Average) graph at https://www.health.state.mn.us/diseases/coronavirus/stats/case.html. If the mouse is hovered over exactly the correct pixel on the graph, a pop-up for a given specimen collection date appears.
A small pulldown menu under that graph offers a csv file of this data (I have not tested using it).
Since their format change, the various permutations of their pages’ graphs can no longer be archived on Wayback (their data is also scattered amongst far more pages than it was for most of the pandemic).
Wayback also had a crash earlier this year which wiped out almost all of the archived MN Dept of Health daily updates over the course of the pandemic.
Walgreens seems to have the best available data for MN, though unfortunately it doesn’t break it out by county–a problem in a state with multiple geographic areas which have at times trended very differently from one another.
For the Twin Cities area, wastewater reporting at https://metrotransitmn.shinyapps.io/metc-wastewater-covid-monitor/ is helpful in addition to Biobot’s breakout of Hennepin and Dakota.
Not going to stop after the election. That’s when they move into the plan to put all pandemic healthcare into the private healthcare industry and make some moneeeeyyyyy.
The Biden administration has already admitted this is the plan. A
And long covid is a gold mine for companies.
Harvest people for money.
> Harvest people for money.
That really is it, and it’s not at all the same as classical “exploitation” as defined by The Bearded One. It’s a lot more like an addiction (waiting for Vaxxing as a Service, where you get your monthly booster as long as you’re fully paid up, which isn’t all that different from, say, opium addiction, at least structurally).
Does anyone know of any formal work that’s been done on this? (Capital has somehow figured out how to extract rent from the working class’s reproduction of its labor power. Amazing achievement!)
This is the kind of masterpiece I have come to expect from the administration of “THE NEW F.D.R.”.
We are blessed with leaders who have shown once again that stupidity has a genius of its own.
This policy will collide with reality soon, along with quite a few others this administration has been following,
Interesting times indeed.
It’s not just the good sunshine in summer, it’s also the fact that we open the windows to get a nice cross breeze. Not so much in winter.
FINALLY, NONS (Nitric Oxide Nasal Spray) treatment and preventative is making another appearance in the media:
https://www.msn.com/en-in/money/topstories/glenmark-says-its-nasal-spray-can-reduce-covid-viral-load-by-937-25-in-24-hrs/ar-AAZwdJo?fromMaestro=true
Other than a few of us commenting about it on this site, there’s been radio silence about it for many months.
Brandnames: Enovid in Israel and Sanotize in India. It’s a little pricey, but readily available online without a prescription.
I’ve just gotten mine from IsraeliPharm; It was quick and easy to get, no prescription was necessary. It must fly over on one of those many SARS-COV-2 transports that we call airplanes.
Bought Enovid as I have some intrusive dental procedures to weather thru next month. Easy to use, easy on the nasal passages… hope it works. I was using immunemist (povidone) but am concerned about overloading the thyroid with iodine so it’s good to have options.
As everyone should know by now, the vaccine is worthless as a prophylactic, tantamount to using a condom with a hole in it.
I used HOCL in a nose spray.
I sent corsi boxes and window exhaust fans to each of my kids’ classrooms. Teachers didn’t use.
> I sent corsi boxes and window exhaust fans to each of my kids’ classrooms. Teachers didn’t use.
Did they give a reason?
We could have used a little warp speed on getting nasal sprays approved in US, but I suspect they’re waiting to see how Pfizer can reverse engineer it without getting in patent trouble … UGH.
As always, thankful for the info here. I’m probably going to pull the trigger on ENOVID shortly, but I searched NC and found this interesting little thread (thx JB & PK) about the red algae based spray as well. Would probably like to try them both. We’ll see if I can source them.
> a nasal spray based on carrigalose
On Carrageenan (red seaweed; Irish Moss) and nasal sprays generally, see NC in 2021. I stan for nasal sprays!
Adding, when I hear “algae” I think green pond scum. But apparently seaweed is algae too! Learn something every day!
Thank you!
thanks to you Carla mine just arrived. But the labeling on the box is all in Hebrew, which I can’t read.
Any idea about directions for use?
I’d love to see a FOIA for the communications of relevant parties during the discussions that must ensure when creating these materials. Like, does anyone bring up whether we care about how many people are in a classroom, or look there are windows? Like some record that someone somewhere used a brain in the administration, and if so, how was it shot down? Bad optics, presumably bad science, no one actually thought of these things maybe (laziness, incompetence)?
It’s really astounding to behold!
Linus Pauling must be spinning in his grave. He does have a legacy group.
Orthomolecular.org has the complete story that has been ignored for what ever reason by our medical people. Vitamin C, hydrogen peroxide, tincture of iodine and the use of nebulizers are what we can do that the government is avoiding.
Just wanted to tell a brief story. This has basically been the only place on the web (aside from the folks at Death Panel who grasp the “macro truth” of the pandemic, and have from the beginning. My relatives, unfortunately, are very much not getting it, which isn’t entirely their fault; it’s not the responsibility of the citizen to be their own CDC and understand what you break down on epidemiological controls. But from the get-go, I realized I was talking to a wall based on the news they consumed. First, it was not listening to me about not going out the first week of March 2020, then ignoring me on going to restaurants or crowded events, or wearing masks. Now, even after getting three shots due to my insistence, they will not get a fourth shot despite being over 60. They have already gotten one confirmed infection in March 2020, and then another during the first Omicron wave (which they concealed from me). This now came to a head when one of them was diagnosed with kidney disease last week, which the doctor presumed was due to a viral infection. Perfectly healthy person with no other symptoms or risk factors, and while there are still tests to confirm, functions are something like 20%. 20%. Twenty. Percent.
I have been sitting in shock for the past week. I keep going over and over the life expectancies and life outcomes for people with this disease, and then going over and over the rates of long COVID per infection and the number of infections we are presumed to get in the future. It drives me mad. It is very literally driving me crazy now that it is finally, like a black cloud I felt a cool chill coming on for, coming to my door.
So first I just want to say thank you for sharing accurate and informed information on the pandemic, and how batshit insane the government’s policies are. I’ve just been grinding my teeth right now trying to understand and wrap my mind around the life-years that the government is ripping from our clutches, and there is no level of justice that can get it back. I truly hope a working class movement can hold people to account, maybe one day in the future. I would even settle for an ACT UP to force our government to act on these common-sense measures on ventilation and disease control. But knowing the truth is very literally the first step, so I just wanted to thank you for helping people get to that step. I can’t understate how important that is, and how it gives even a sprinkling of solace, of hope, in a world where people truly feel abandoned and forgot about, and where I feel increasingly isolated in a country where most people don’t “get it.”
The Trotskyists of the Fourth International have also been very good on the pandemic.
WSWS gets points for endorsing Zero Covid, but they’re basically Science™ liberals in all other respects.
They’ve been big shills for Western mRNA vaccines (plus the usual glowing deference to ghouls like Fauci, etc.) from the start, and have rather remarkably kept it up despite the mountains of evidence indicating the mRNA “miracle” is one of the worst public health disasters and Big Pharma frauds in history.
NC is the only place I refer anyone for pandemic analysis at this point.
> ACT UP
A movement we could learn from (and IIRC achieved some success?)
Yes, ACT UP did have a significant impact nationally and locally. It was due to the work of ACT UP that ‘compassionate release’ of experimental drugs became a thing, among other things. They succeeded because they were able to mobilize large numbers of people willing to undertake direct action to disrupt ‘business and usual’, and able to organize many more who had the backs of those who did potentially illegal things. The series of actions occupying FDA offices I believe had a real effect speeding compassionate release.
“ACT UP & ACT NOW Seize Control Of The FDA
“October 11, 1988 — ACT UP, joined by the national ACT.NOW coalition, shuts down the FDA headquarters in Rockville, Maryland. This historical demonstration against the FDA condemns the lethargy of this dysfunctional bureaucracy which is responsible for the testing and approval of possible AIDS treatments.”
https://youtu.be/s70aCOflRgY
“Direct action brings satisfaction.” As they say.
2022 is in an era quite different from 1988. The police are far more heavily armed, and they are far more of them. Attempts to shut down the FDA would not be successful now, unless protesters are willing to risk life and limb. Effective protests are difficult in a police state.
> unless protesters are willing to risk life and limb.
As they are doing in another Third World country, Myanmar. One reason I follow it, because it’s such an amazing natural experiment.
I hear you, MP. You are not alone.
you speak eloquently and for so many that I took the liberty of saving your comment.
there are many reasons to read NC but the shared experience of sanity and solidarity in a world gone mad is the most important right about now.
You may find this of interest: Christos Argyropolous, a nephrologist in New Mexico, has reported 2-3x increase of Chronic Kidney Disease consultations since the onset of delta and omicron
Biden has got to go…
They all have to go, a fate they are bringing on themselves, but not, perhaps, rapidly enough.
I can’t believe this — now it may be 30 days “immunity” before reinfection!!!
https://abc7news.com/ba5-covid-immunity-omicron-ba4-reinfections-how-long-are-you-immune-from-after-having-it/12047575/
don’t worry. “they” are already signalling that he should bow out next time and let Gavin Newsom or Mayor Pete take his place, or Hillary Clinton or some combination thereof.
“they” seem to have gotten the message that Harris is likely to be a failure on a second run.
and what will Newsom do? whatever his masters tell him to.
guess we should start asking the Gettys what they think should be done about Covid, as that is likely what Newsom will try to get across.
Newsom will do what Pelosi tells him what to do.
Well after all, she is his aunt…
You go Brandon!
As someone who remembers the wave after wave of funerals during the AIDS epidemic, this does have a certain resonance. Yes, AIDS without treatment is almost 100% lethal unlike Covid, but it is also much harder to get. Either way, two serious diseases with one taken seriously and the other not.
I am starting to fear the current pandemic much more than I ever did the previous one even though for years no one really had a clue about the first. But the adults were in charge forty years ago.
Well, jeez. As a “survivor” — day 8 and counting — of what I presume is the B.5 variant (symptoms differ from “traditional” Covid; mine correspond to b.5; and yes, I had a PCR test) — who got two shots, a booster, always wears a NIOSH-approved n95 in indoor public places and isn’t going to bars, theaters or restaurants and avoids outdoor crowds, I have to wonder if there are *any* tolerable and/or enforceable public health strategies which will be effective in societies larger than 2.
What has changed in recent weeks, in a high rent Manhattan neighborhood, is that more than half the supermarket patrons and many of the cashiers are unmasked — the presumed but unverifiable source of my own infection. Granted, quality masks should have been made available free (years ago), but people, even in the redoubts of limousine liberalism, will not wear them.
Public policy has its limits….
Hmm, I read that as “equality masks” — what could I possibly be thinking?
Well, there is the equality of the grave?
> more than half the supermarket patrons and many of the cashiers are unmasked
There’s one answer: Universal masking makes everybody safer than “one way” masking. (Who knew, altruism > selfishness.)
There is also the principle of “the dose makes the poison.” If all your measures reduced your level of exposure, then perhaps your case was less severe than it otherwise might have been.
> I have to wonder if there are *any* tolerable and/or enforceable public health strategies which will be effective in societies larger than 2.
Japan….
Exactly, Japan. But Japanese compliance relies on social taboos which have no force elsewhere, least of all in the U.S. Judging from current photos of Tokyo, there’s overwhelming pressure to wear masks even on the street, which virtually no one, including me, does here.
FWIW, the precautions noted above likely did [greatly] mitigate the disease: the course of it was mild. But based at least on this experience, there’s apparently no way to expect to avoid infection (and the odds of long Covid) if you leave the house without protective gear which will stop traffic….
To your point on improving those interactive models. The data on the volume of one human breath is easily available (without checking, i think it’s 500 mL/breath and 10-15 breaths/minute). It would be so easy to make the models better that the fact they aren’t better suggests it’s intentional.
Here’s a little story, a parable if you will. I do a lot of indoor mold investigations and one of the things I tell people is that mold spores are everywhere all the time. Sometimes I make a little “joke” about how the only way to not have spores indoors is if your HVAC system ran through a HEPA filter and then point out that nobody does that. Except this one time I was at a nursing home and the facility director said, “We did that.” Turns out they only have to change the HEPA once per year because it has cyclonic prefiltration, etc. He told me that while the install was more expensive than other options (they had to replace the HVAC anyhow), in the first year of use the incidents of cold/flu dropped by more than 60% with no other controls (this was long before Covid). It turns out that the community fireworks are launched from next door and in the past the smell of powder would just coat the whole facility. After the HEPA install nobody could tell the fireworks were launched.
While you couldn’t retrofit this to any old commercial or home HVAC system because the fan wouldn’t be speced to handle it, I’ll bet you could build a retrofit to those units where a separate fan pulled through the HEPA(s) and fed the make up air to the HVAC unit. It would require some balancing of fans, but modern commercial HVAC requires lots of balancing anyhow.
> It would be so easy to make the models better that the fact they aren’t better suggests it’s intentional.
You put better than I did. I mean, no open doors? Really?
> I’ll bet you could build a retrofit to those units
Sounds like a business model?
You can also carry your own HEPA filter with you.
My most prized tactical gear is an “Aurora AM99” powered HEPA filter/mask combo. $40 on Amazon. It’s a small metal box with a battery, HEPA filter, tube out to a mask of your choice. 8-hour charge on USB.
Re; “equity”
Translation: we’re all fvcked.
https://abcnews.go.com/US/dr-fauci-wear-goggles-eye-shields-prevent-spread/story?id=72059055
Dr. Fauci: Wear goggles or eye shields to prevent spread of COVID-19; flu vaccine a must
Anybody have any luck with goggles? I ordered some in two different sizes, but they don’t seem to fit.
Goggles may be overkill, unless you find yourself in an environment where the risk of disease contraction is very high. Day to day life is not that risky.
“… unless you find yourself in an environment where the risk of disease contraction is very high.”
I’m thinking airplanes.
Just point the overhead blowers at your face and you’ll be fine. Double mask til 20 minutes after takeoff and 20 minutes before landing and all through airport.
the airlane transmission debate is an interesting one, but I think this is ill-advised. I wouldn’t unmask on a plane,
which of course sucks.
This article is 2 years old.. while I realize its possible to get infected via the eyes I do not have reason to believe Fauci is still suggesting goggles
Was that one of Fauci’s noble lies?
> its possible to get infected via the eyes
The most likely way for that to happen would be if you rub your eyes with hands that have touched a contaminated surface. Back when fomite transmission was still a thing, and droplet goons ruled the earth, there was a lot of worry about this pathway. Now, in the world of aerosols, there isn’t. (That said, I’d still careful about rubbing my eyes, by the precautionary principle.)
I am not aware of any epidemiological studies showing SARS-CoV-2 infection through the eyes, and I do try to keep track.
I don’t believe this is the case. Eyes are constantly exposed to the air, although of course they do not create suction as the nose and mouth do. While less common than inhaled aerosol infection, aerosols would still be a concern vis à vis the eyes.
So this is an email I received at work this morning (slightly edited to anonymize things a bit) that pretty much has me desperately wishing I could retire:
————————
Hello, employees.
Later this morning, Our Public Health will announce it is recommending people here mask up indoors. This recommendation follows state health authorities and Centers for Disease Control guidelines. We have exceeded 200 cases per 100,000 people for two weeks in a row and hospital capacity is strained. This recommendation to wear masks indoors is especially timely as thousands of visitors are expected to arrive this week for many summer events.
We wanted to let you know first and to clarify what that means for you as employees.
Public Health’s recommendation includes our facilities. We will be providing masks at building entrances, along with signs about the recommendation, for employees and visitors to use [NOTE: I bet they will be surgical not N95 or KN95]. We are not requiring employees to mask up indoors.
We do ask that you respect the decisions of your colleagues when it comes to masking. [NOTE: both those who mask, and those who don’t. Of course.]
Visitors to our buildings are encouraged, but not required, to wear a mask. We will not deny anyone service if they choose to remain unmasked. Please note: masking requirements remain the same in healthcare settings.
In the community, we expect to see many privately owned businesses choosing to require masks.
Increased masking is one way we can all work together to keep our community safer. Thank you, as always, for continuing to be flexible as we try to keep people healthy and for considering this recommendation.
> We have exceeded 200 cases per 100,000 people for two weeks in a row and hospital capacity is strained. This recommendation to wear masks indoors is especially timely as thousands of visitors are expected to arrive this week for many summer events.
It”s not “timely.” It’s two weeks too late.
“Thank you, administrators, for continuing to be flaccid as we try to deal with an airborne pandemic….”
I think it may be appropriate to start looking for the real meaning of CDC:
– Communicable Disease Collaborators
– Critical Data Concealers
– Covid Doom Cult
any I missed?
Chamber D’Commerce
Now THAT… is on the money.
> Covid Doom Cult
I think Covid Death Cult would activate the right triggers. It also has the great merit of being true (see Rule #2).
Another data point here in north Iowa. Very few people are wearing masks. People go about their daily lives without ever thinking the pandemic is not over. What is truly shocking to me is the nursing homes have abandoned masking. The thinking is that everyone is vaxxed and boosted so no worries. Everyone in the hospital is wearing procedure masks. Someone told me we’re just tired of wearing masks.
NC is the only place that we can get ant decent info – the good, bad and the ugly – and it will get ugly. Thanks to all who makes information about Covid honest – sometimes brutally so. I’m sure you’ve saved lives.
The national strategy emphasizes “take the vaccine”. This NC post implies this is inadequate, i.e. more should be done to prevent infection. But how inadequate is the “take the vaccine” emphasis?
We know that vaccines significantly reduce serious infections (those requiring hospitalization).
I assume the concern expressed in this post is with the consequences of mild or asymptomatic infection among the vaccinated population. (I’m frankly not that interested or concerned about those who refuse to be vaccinated–they are free to gamble with their health and play the odds with post-infection anti-virals.)
We know from the veterans study that even the vaccinated can experience asymptomatic breakthrough infections, and these can also experience “long covid” consequences. In that study, of 2.5 million veterans who were fully vaccinated, only 34K vets experienced breakthrough infections, and of these, only around 10% experienced long covid, or around 3,000. That’s approximately one out of 1,000 vaccinated people.
Looking at these numbers, a “take the vaccine, damn it” strategy seems reasonable. Even if (as we now know) taking the vaccine does not reduce transmissability much, it’s the unvaccinated who bear most of the risk of lack of good anti-infection measures in the national policy.
Preventing infections is a good idea, but is not with cost. The costs include rigorous social distancing (of the kind seen in China), which also has health consequences (depression, suicide) and major investments (improved HVAC, etc.) that may not be politically or economically feasible given the level of risk reduction involved. All this to spare the few who are vaccinated from getting long covid? Or to alleviate risk to the unvaccinated?
I’ll be honest: I couldn’t care less about the risks being taken by willfully unvaccinated. This includes my own young (20 years), healthy, and very bright son. He’s done the research, and knows the risks he’s taking. He’s a conscientious objector to taking a vaccine. I respect that, even if I still (after much discussion with him) can’t understand the reasoning and values behind that commitment.
So, could you explain why preventing infection is a better (risk informed) and cost effective strategy?
I mean, we do have other priorities as a nation. Like helping the Ukrainians fight for their freedoms. /s
This is excellent quality information fire. It’s calm, organized, hits all the talking points paid for, celebrates values that flatter the reader, uses cagey qualifiers even though the costs are perfectly calculable and have been calculated (and are in any case irrelevant except as to material availability and production capacity), presumes the interests of others, compares apples and oranges, and glosses over their mendacious non-engagement with the dissident position with a perfectly delivered performance of the tone of reasonable discourse.
LOL … ::chef’s kiss::
@Karl, as someone who is vaccinated and double-boosted (Pfizer, Pfizer, Moderna, Moderna), I would like to point out that just as no one knows the extent of long-term vascular and neurological damage caused by (even mild) repeated Covid-19 re-infections, so too no one knows the long-term effects of MRNa vaccines. That concerns me, not for myself, because I’m old so the long-term is not very long in any case, but for all the middle-aged and younger people, and particularly for children. In the meantime, information about an effective and harmless preventative and treatment such as Nitrous Oxide Nasal Spray (NONs) is deliberately kept scarce. Why?
Thanks, Carla and hunkerdown
Karl: The veteran’s study you pointed to is from April 2020. That is 4? 4? 6? Hundreds? of variations ago. The increasing number of newer variants is partly a result of people believing in non-sterilizing vaccinations as a panacea. While your reinfection figure was small, it was only very early results from the earliest original disease.
Remember, the vaccinations do NOT prevent covid from spreading. the more people it spreads to, the more likely it is that one of those recipients, vaxxed or not, will generate a new variation, that will then spread by people who believe that all they need to do is vax, and the rest will take care of itself. Don’t forget vax “immunity,” if one can even call it that, begins to fall off rapidly, within weeks, and is virtually non-existent within a few months.
Now, with BA 5, we have, according to virtually all available information, bypasses the little immunity we might have. In that sense it is almost a new disease.
Now, add to that the lack of vaccination of most of the world, many of whose citizens are traveling to your home town, shopping in your grocery stores, and eating in your restaurants. And all because your country and mine, along with much of the so-called first world, have hoarded the semi-useless vaccines that two companies have earned billions from.
Thanks for your excellent comments. FYI, the Veterans study took place between January 1, 2021 and October 31 2021. It was received for review in January 2022, and published online May 2022. You can’t get much more current than that.
I think a lot of our differences of view concern risk tolerance, and the costs and benefits of taking more drastic measures at the tail end of the curve. Remember, the original goal of social distancing and other NPI’s was to “flatten the curve”, not flatten it all the way to zero. Also remember that there is such a thing as “long flu” and we’ve come to accept this phenomenon.
We have come to accept around 30K-60K deaths per year from flu. Granted, this is ~1/10 that of Covid, but national policy on flu is to emphasize vaccines, same as with Covid. Most survivors of each year’s flu strains are from ordinary exposure, not vaccine. Flu vaccines are often limited in effectiveness, but I take them anyway, because they help train my immune system, and I see little downside risk.
I predict that we as a society will come to accept endemic Covid-19 because we have somewhat effective vaccines (like flu), despite its ravages and the uncertainty about new strains. I don’t think we have much choice. Ten years from now, we’ll stop asking for proof of vaccination, masking, and other measures. We’ll let the chips fall where they may.
There’s also the issue of the United States — along with the UK and much of the Anglosphere — becoming a reservoir of Covid infection for the rest of the world. I’m about to break out my Canadian lapel pin, it makes me so ashamed of what we’ve become.
Sounds like your son assessed the risk of getting covid and compared it to the risks the vaccine presents for his age and health status. Makes sense.
There should never, ever have been a vaccine mandate. Now a masking mandate, on the other hand…
> The national strategy emphasizes “take the vaccine”. This NC post implies this is inadequate, i.e. more should be done to prevent infection. But how inadequate is the “take the vaccine” emphasis
A million dead, and we’re asking whether we did everything we could? Holy moley.
Do you really mean everything? We are already experiencing huge masking fatigue in this country. Our government and culture will resist more lock-downs, unless the severity of strains increases radically. I agree that this is a pitifully weak approach, because the best solution is to eradicate the virus and thereby eliminate the risk of new strains. But we’re past that point, unfortunately. We aren’t China. And eventually, the virus will vitiate all of China’s efforts because it will become endemic there too.
The one thing I would do that’s not being done is to enforce vaccine protocols and social distancing on airlines, cruise ships, etc. and require them to have UV ventilation systems. Long distance travel is the big spreader of new strains. Unfortunately, travel and tourism are just too important economically, apparently, to do this. Cruise ships are back up and running. Again, it comes down to risk tolerance. But I see no problem with vaccine/testing mandates for long distance travelers.
Why is fatigue reason enough to not bother with masking policies but not vaccine policies — especially in light of the limited downsides of masking?
If I were cynical I might think you were a Pfizer lobbyist
You mean? Why is fatigue reason enough to not bother with masking policies, while upholders of that say keep the jabs?
Ok, there is some fatigue with masks; but those who think well of jabs are not thinking about the few studies indicating thrice jabbed have currently [in some places] higher infection rates than the double jabbed?
I’m guessing sneezing/coughing is about 10% of the way you can get it. But I’m noticing more people sneezing more often. So, it’s a little measure but a sure measure. With a tight mask on a crowded sidewalk (no wind), they probably cut down on the tiny, tiny, tiny [at least the 10-30 micron “big”] water droplets bearing the bug?
I acknowledge mask fatigue, and I’m thinking the big issue of the future might be how not essential workers will not be grasping what essential workers are going through (an inequality issue). But their not grasping it on plastic gowns may end up ten times more of a policy challenging issue (if you think masks are a hassle, just try working in one of these sometimes necessary bad boys). There are other states of no-empathy-no-comprehension consciousness…in regard to many other matters…that center-orthodox-blue folks float around in. Way, way, way, way too often they don’t get the rhythm at all.
On the larger issue of the article, one wonders how Oliver Stone can endorse nuclear power stations when regulation/policy on something as serious as a pandemic ends up like what we’ve witnessed.
It doesn’t seem to be a big loss to me.
What can Kamala Harris even do? She seems to be totally incapable of doing anything. It’s not like her spending time on the pandemic can would help solve the problem.
She also does not seem to have surrounded herself with a competent team of professionals that is able to take a leading role. She’s also not a particularly good public speaker or capable of convincing skeptics.
Instead the fact that she was selected to be VP reflects very poorly on the Biden administration.
There seems to be a general incompetence in the Biden administration. They don’t seem to be able to handle any crisis with anything that could be described as effective leadership. Foreign policy, the economy, the pandemic, etc, have all been handled very poorly by the government.